
Abstract
Science and practice seem deeply stuck in the so-called stage theory of grief. Health-care professionals continue to “prescribe” stages. Basically, this perspective endorses the idea that bereaved people go through a set pattern of specific reactions over time following the death of a loved one. It has frequently been interpreted prescriptively, as a progression that bereaved persons must follow in order to adapt to loss. It is of paramount importance to assess stage theory, not least in view of the current status of the maladaptive “persistent complex bereavement-related disorder” as a category for further research in DSM-5. We therefore review the status and value of this approach. It has remained hugely influential among researchers as well as practitioners across recent decades, but there has also been forceful opposition. Major concerns include the absence of sound empirical evidence, conceptual clarity, or explanatory potential. It lacks practical utility for the design or allocation of treatment services, and it does not help identification of those at risk or with complications in the grieving process. Most disturbingly, the expectation that bereaved persons will, even should, go through stages of grieving can be harmful to those who do not. Following such lines of reasoning, we argue that stage theory should be discarded by all concerned (including bereaved persons themselves); at best, it should be relegated to the realms of history. There are alternative models that better represent grieving processes. We develop guidelines to enhance such a move beyond the stage approach in both theory and practice.
Theoretical models of bereavement should serve the function of increasing understanding of grief and grieving, particularly given the physical and mental health ramifications of this severe life event (Parkes, 1972/1996), which may require professional intervention (Shear, 2015). Among these approaches, so-called stage theories, postulating that grief progresses through specific emotional stages, have remained highly influential. Indeed, such adoption of a stage approach follows a long tradition in psychology (e.g., in developmental, health, social, and clinical domains) as well as in psychiatry and medicine. A stage theory can offer new ways of understanding complex systems of human behavior, ways that may be helpful for diagnostic purposes and to guide intervention (McGorry, 2007). However, those stage theories that have proven valuable show the evidence of scientifically based principles (e.g., postulating discrete changes in the nature of underlying stage-related processes or cognitive levels, providing empirical evidence for a sequential progression/for efficacy in treatment). Does the stage theory of grief meet such criteria? Is it a valid and useful model of grief and grieving? Answering such questions requires evaluation of both its scientific and practical value. Therefore, the aim of this article is to review and assess the contribution of the stage theory of grief.
To this end, in the next section, we trace how stage theory emerged historically, documenting its remarkable, persisting popularity in the face of ongoing opposition. Then we focus on emergent lines of argument against stage theory, covering conceptual concerns, lack of empirical validity, its failure to assist in identifying those at risk or with complications, and the potentially negative consequences for bereaved persons themselves. As we show, the stage theory of grief falls short in all these respects. There is no scientific foundation, and decades of research have shown that most people do not grieve in stages. Using stages as a guide in work with bereaved is unhelpful and may even cause harm. Our critical assessment leads to the conclusion that stage theory should be relegated to the past and eliminated from contemporary clinical practice. We discuss what actions can be taken to move on, suggesting an alternative approach and providing initial guidelines for health-care professionals and bereaved persons.
Stage Theory in Historical Perspective: Claim and Refutation
The emergence of stage theory is usually ascribed to Elisabeth Kübler-Ross’s (1969) monograph “On Death and Dying,” which documented her observations of adjustment among dying patients. In essence, Kübler-Ross’s stage perspective held that dying people go through five stages of grieving: denial, anger, bargaining, depression, and, finally, acceptance (sometimes called the DABDA model). Each stage was described in a separate chapter, with “stage” in the heading of these, strongly suggesting that they were distinct and sequential, even linear (although minimal acknowledgment of fluctuations between stages, individually varying time sequences, and coexisting stages can be detected on close reading). Later, in reintroducing the stages and focusing more on the bereaved (Kübler-Ross & Kessler, 2005), this was contested (though separate, sequential descriptions remained).
It is important to note that Kübler-Ross herself extended the application of the stages of dying to the situation of (anticipatorily) bereaved persons already in her 1969 book. Excerpts from her chapter “The Patient’s Family” make this clear: Family members undergo different stages of adjustment similar to the ones described for our patients. At first many of them cannot believe it is true. They may deny the fact that there is such an illness in the family. . . . Just as the patient goes through a stage of anger, the immediate family will experience the same emotional reaction. . . . When anger, resentment, and guilt can be worked through, the family will then go through a phase of preparatory grief, just as the dying person does. (Kübler-Ross, 1969, pp. 168–169)
Other formulations of stages or phases appeared over the following decades (Bowlby, 1980; Horowitz, 1976; Jacobs, 1993; Sanders, 1989; Shuchter & Zisook, 1993), varying in labels (e.g., various combinations of disbelief, numbness, yearning, shock, and guilt), numbers of stages (e.g., 3, 4, and 7), and general guidelines (e.g., emphases on fluidity vs. rigidity). It is beyond our scope to review all, but our arguments can be considered in the context of these approaches.
It was Kübler-Ross’s volume which became an international bestseller, even, according to Friedman and James (2008), reaching the status of “one of the most influential books in the history of psychology” (p. 37). Indeed, Kübler-Ross succinctly both formulated and popularized stage theory, promoting it throughout her life. She was also a charismatic person, much admired and loved by her followers, even described as “legendary”; in 1999, Time Magazine named Kübler-Ross as one of the “100 Most Important Thinkers” of the past century (from her obituary); in 2007, she was posthumously inducted into the United States Women’s Hall of Fame. Already by 1982, Kübler-Ross estimated that her stages had been taught in 125,000 courses in colleges, seminaries, medical schools, hospitals, and social work institutions (Rosenbaum, 1982; Wortman & Silver, 1987). By 2016, On Death and Dying reached a remarkable figure of well over 11,000 citations in Google Scholar.
Contributions of both Parkes and Bowlby, around the time that Kübler-Ross’s monograph was published, avoided some of the pitfalls of stage theory, going on to become major contributions to understanding of the course of grief and grieving. 1 These researchers incorporated the notion of phases in a theory-based manner (following attachment theory principles; Bowlby, 1980; Parkes, 2006). More cautiously than Kübler-Ross’s (1969) presentation of stages, Bowlby (1980) stated: “these phases are not clear cut, and any one individual may oscillate for a time back and forth between any two of them” (p. 85).
Looking across the decades, a highly influential source of opposition to stage theory came from Wortman and Silver (Silver & Wortman, 1980; Wortman & Silver, 1987, 1989, 1992), who drew attention to the alarmingly widespread adoption of stages among health-care professionals, with disastrous consequences for the bereaved, despite lack of solid evidence. Their classic article of 1989, “The Myths of Coping With Loss,” criticized Kübler-Ross’s expectation of recovery through to the final, acceptance stage of grieving, pointing to longer, varying courses of grieving among many bereaved people (without indications of pathology). Their conclusions were echoed in the Institute of Medicine’s authoritative review, which cautioned: The notion of stages might lead people to expect the bereaved to proceed from one clearly identifiable reaction to another in a more orderly fashion than usually occurs. It might also result in inappropriate behavior toward the bereaved, including hasty assessments of where individuals are or ought to be in the grieving process. (Osterweis & Green, 1984, p. 48) suspiciously simplistic models, such as stage theories of grieving that have been largely repudiated by contemporary theorists and researchers … grief counseling … rarely draws on the best available theories regarding the nature of bereavement and its facilitation. (p. 547) Although it is sometimes instructive to conceptualize the manifestations of grief in this manner, it is important to emphasize that the idea that grief unfolds inexorably in regular phases is an oversimplification of the highly complex, personal waxing and waning of the emotional process. (p. 18)
Neither these nor other criticisms impacted on Kübler-Ross’s adherence to stages. The title of her 2005 monograph with Kessler, On Grief and Grieving: Finding the Meaning of Grief Through the Five Stages of Loss, leaves little doubt about that. This volume, like its 1969 forerunner, continued to strongly divide opinion among readers (it was positively reviewed by Bolden (2007). The authors responded to the criticisms from previous years in the opening lines of Chapter 1: The stages have evolved since their introduction, and they have been very misunderstood over the past three decades. They were never meant to tuck messy emotions into neat packages. They are responses to loss that many people have, but there is not a typical response to loss, as there is no typical loss. Our grief is as individual as our lives. (Kübler-Ross & Kessler, 2005, p. 7)
To this day, stage theory is still widely known, taught, and used in clinical practice. Konigsberg’s book (2011), entitled The Truth About Grief: The Myth of its Five Stages and the New Science of Loss, though accessibly reviewed by Balk (2011) and Neimeyer (2012), has remained apparently unheeded and relatively uncited. As a final illustration of perseverance, the stages approach has recently been claimed state of the science of bereavement theorizing in an article by Jurecic (2015). According to Jurecic, what is “emblemic of modern loss and grief” in medicine is a progression through Kübler-Ross’s five stages (1969), which “encourage an orderly process of bereavement,” that contemporary (medical) approaches propose that “mourning progresses in predictable stages” and that there is a “right way to mourn.” This misrepresentation of current scientific understanding in the bereavement field (elaborated below) does our field—to say nothing of bereaved people themselves—no good. Worryingly, her claims may even promote the use of stages. Again the enormous resistance to moving beyond the stages approach is demonstrated. There are compelling arguments to be made as to why this situation must change.
Criticisms and Assessment of Stage Theory
From the claims and refutations traced earlier, five main categories of criticism emerge:
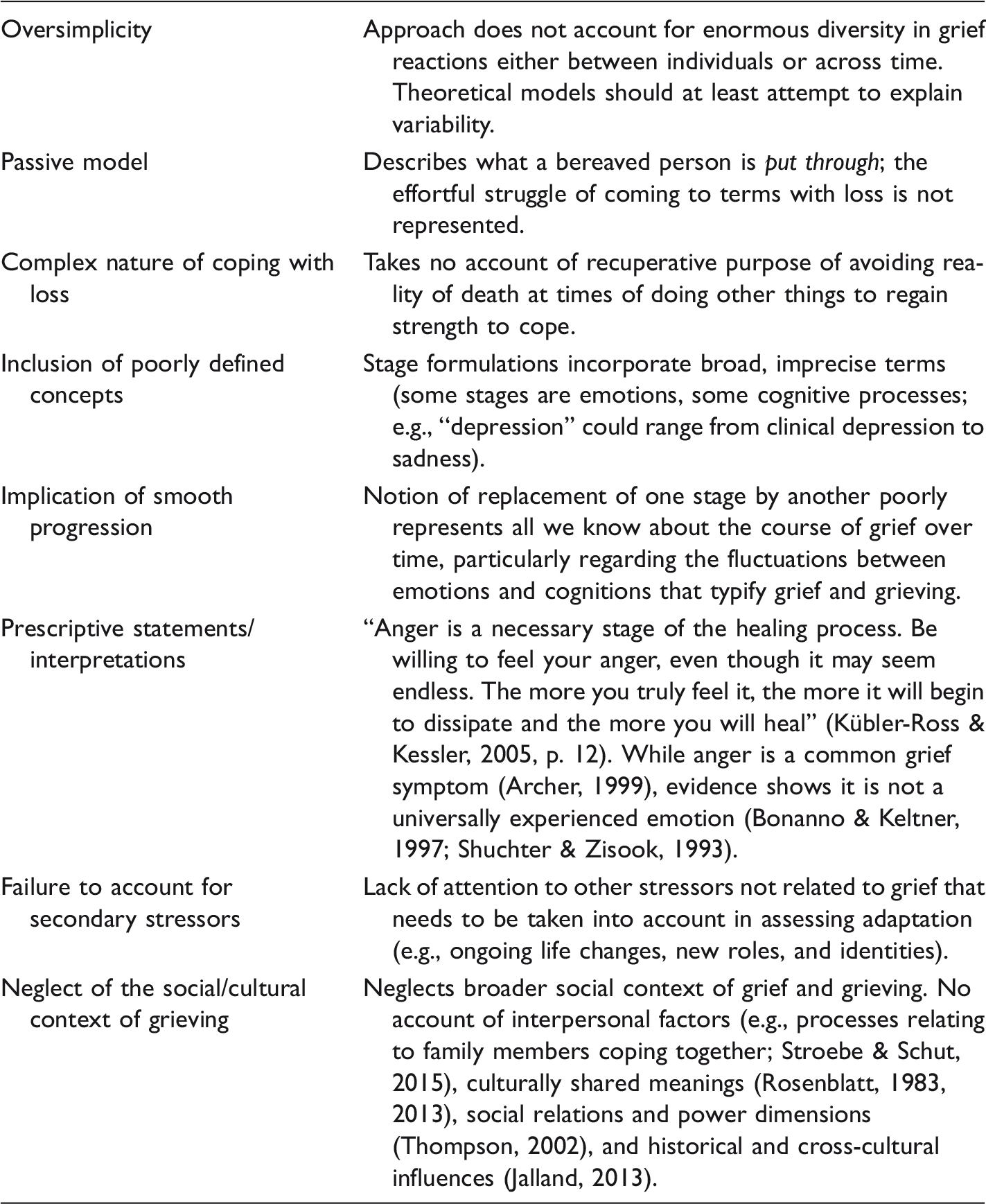
Lack of theoretical depth/explanation. In contrast to Bowlby’s phases, Kübler-Ross’s stages (1969) were not derived from theoretical principles. As Archer (1999) pointed out, the approach “does not address the issue of what might be the principles underlying this organization” (p. 100). This therefore fails to address the question: What is the function of grief? In Bowlby’s (1980) case, the phases were related to attachment phenomena, serving the purpose of regaining proximity to the person from whom the separation had occurred. No such underlying principles were postulated for the stages. Bonanno and Boerner (2007) expressed their doubts as follows: Grief stages tell us little about how people might cope with the loss; why they might experience varying degrees and kinds of distress at different times; and how, over time, they adjust to a life without their loved one. Considering the evidence from other studies that contradicts the idea of an “average” normal response to loss, this is a misguiding message. (p. 2693) Conceptual confusion and misrepresentation of grief and grieving. Among this class of critical comments, the following stands out: It is unclear what the sequential stages (i.e., denial, anger, bargaining, depression, and acceptance) really are and what they represent. Some denote affective states, others cognitive processes. So there is a mixture of different types of constructs which do not fit coherently or sequentially together. There is no theoretical rationale for this particular arbitrary use of dividing lines between states. Further examples of conceptual concerns are given in Table 1. Taken together, rather than providing us with “the knowledge of grief’s terrain” (Kübler-Ross & Kessler, 2005, p. 7), it becomes clear from the points listed that stage theory misrepresents phenomena associated with bereavement. Lack of empirical evidence. Kübler-Ross’s (1969) knowledge was not derived from systematic, empirical investigation (of bereaved persons) but through the contact of “over two hundred dying patients” (p. 38). Despite this number, in Parkes’ (2013) view, there was lack of scientific rigor: On Death and Dying was simply “a collection of case studies in the form of conversations with dying patients” (p. 94). Surprisingly little empirical testing of stage theory has been subsequently undertaken—as Archer (1999) pointed out, this is difficult to do. Table 2 reviews relevant studies, indicating little support and quite some refutation of the stages. In conclusion: While there is empirical evidence that people experience (some of) the emotional and cognitive reactions some of the time, there is little to support the sequential development of these in stages. The availability of alternative models. The stages approach has been supplanted by finer grained, sometimes theoretically based, more-representative-of-the-grieving-process models of grief and grieving (see Table 3; for reviews, see Boerner, Stroebe, Schut, & Wortman, 2015; Doka & Tucci, 2011; Stroebe & Schut, 2001). These alternative perspectives, developed over the years, are well known but received no acknowledgment or discussion by Kübler-Ross and Kessler (2005). The devastating consequences of using stage theory. Last, but certainly not least, it is important to recognize that using the stages approach as a guideline in supporting bereaved persons may raise undue expectations, even presumptions about the course that grief should take. Naturally, some bereaved people may feel affirmation from reading about incorporation of emotions such as anger or despair in stage theory: If they fit one’s personal experience, they provide verification. Kübler-Ross received a large fan mail confirming this. However, such positive appraisal does not provide evidence for the sequence of stages in general, nor does it follow that the stages should be taught or used in therapy. Silver and Wortman (2007) stated: A mistaken belief in the stage model . . . can have devastating consequences. Not only can it lead bereaved persons to feel that they are not coping appropriately, but it also can result in ineffective support provision by members of their social network as well as unhelpful and potentially harmful responses by health care professional. (p. 2692) Misrepresentation of Grief and Grieving in Stage Theories: Major Concerns. Empirical Investigation of Stage Theory: Claim and Refutation. Moving Beyond the Stages of Grief and Grieving: Suggestions and Guidelines.
Such fears were endorsed by Friedman and James (2008) who expressed concern about the “horror stories . . . heard from thousands of grieving people who’ve told us how they’d been harmed by them.”


Many writers have also drawn attention to the dangers for bereaved people of prescriptive interpretation. The stages, it was often said, were meant to be descriptive. However, they have been taken to be prescriptive (browsing the Internet provides ample evidence). Caregivers mention clients worrying because they are not experiencing the stages in “the right order” (and that a not-uncommon reason for seeking professional help is a failure to experience one or more of the stages of grief). Whatever the intention, the theory promotes the idea of an orderly progression through distinct periods of grief and grieving, ones which can be identified and described by particular features.
Conclusions
Where do these criticisms leave us? Certainly, Kübler-Ross’s enormous impact must be acknowledged. Her writing (indeed, her whole extraordinary career) drastically altered the care and treatment of dying patients (see, e.g., Friedman & James, 2008). Her work brought death and dying out of the closet. Furthermore, bereaved people stand to benefit from her compassionate, easily accessible writing and teaching. However, such merits are on a completely different level from evaluation of the actual stages; it does not follow that the stages are adequate representations of what grieving people go through.
Why has stage theory been so impossible to dislodge from its favored position among many teachers, clinicians, and clients? The abiding appeal is perhaps its simplicity. In the midst of such emotional complexity as characterizes the bereavement experience, the stages offer something to hold on to, both descriptively and prescriptively. Bereaved people want to know what to expect and how long the upset will last (Friedman & James, 2008). As Hall (2014) expressed, “Stage theories have a certain seductive appeal—they bring a sense of conceptual order to a complex process and offer the emotional promised land of ‘recovery’ and ‘closure’” (p. 8).
What we need, then, is not a plethora of alternative perspectives but an accessible, easily comprehensible, informative, single substitute for stages (but one that at least attempts explanation at a theoretical level). In our view, we should aim for further theoretical integration. Having a range of alternatives presents a weak, nonunited front to stage theory. That is perhaps a major next step for researchers to take: to work toward developing a theory that explains the process of dealing with loss and ongoing life, reflecting the experience of bereaved persons, their thoughts, and feelings. Indeed, some of the perspectives [e.g., trajectories, Dual Process Model of Coping with Bereavement (DPM), meaning making] are compatible in important ways (e.g., in their focus on both loss and change; Marris, 1974; Parkes, 1971; Stroebe & Schut, 2015). Furthermore, concrete steps must be taken to encourage the move beyond stages in practical as well as in such theoretical terms (see Table 3).
In summary, the critical points outlined earlier provide a strong case for abandoning the stage theory of grief and grieving. We have argued that, while it is the nature of the endeavor that scientists try to identify regularities, the regularities of stage theory are too simplistic and limited; they fail to represent the complex emotions and processes of grief and grieving. They also lack empirical foundation. Using stages in practice is potentially harmful, and yet an (perhaps the) ultimate goal of theory construction in our field is to enable health-care professionals to provide tangible help to those who need it.
Therefore, our urgent appeal is for the stages to be relegated to the shelves of history. They are, after all, only “manmade”: As Rosenblatt (1983) puts it, “The stages are, of course, mental constructions of researchers, clinicians, and theoreticians. They are not real, quite abruptly delineable sets of events that are obvious to any observer” (pp. 38–39). It is our sincere hope that this article will help eradicate adherence to stage theory and promote discussion of alternatives, in the best interests of bereaved people and those who endeavor to support them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.