
Abstract

A meeting of the Medico-Legal Society was held on 13th October 2025 at the Medical Society of London (and also remotely by Zoom) with the President, Dr Sarah Galbraith in the Chair.
We welcome Dr Michael Biggs who is going to talk to us about the history and evidence for puberty suppression as an intervention for children experiencing gender dysphoria. He is an Associate Professor of Sociology at the University of Oxford and Fellow of St Cross College, Oxford.
Dr Biggs is a leading, and often pioneering, researcher in the complex and sensitive field of gender dysphoria treatment in young people. He has dedicated his work to understanding the evidence surrounding puberty suppression as a treatment for children presenting with gender dysphoria.
Dr Biggs’s contributions to this field are substantial. He was the first to discover the experimental use of puberty blockers at the Tavistock Clinic’s Gender Identity Development Service, bringing to light critical data that has significantly shaped the ongoing debate. His research, exploring the effects of puberty blockers and the complex relationship between gender identity and adolescent mental health, including the risk of suicide, has been published in numerous prestigious journals.
Beyond his academic contributions, Dr Biggs has played a crucial role in legal proceedings related to gender dysphoria treatment. He served as an expert witness in the landmark case of Keira Bell and Mrs A v Tavistock NHS Trust [2002] at the High Court, as well as in cases in Australia and the USA.
Dr Biggs’s work has often challenged conventional thinking, prompting crucial conversations about the long-term impacts of medical interventions for gender dysphoria. He has been a vocal advocate for rigorous research and open discussion, even when faced with the challenges that can arise when questioning established practices.
We are honoured to have him with us today to share his expertise and insights with us. Thank you.
Thank you very much for this invitation. I’m very happy to be here particularly since just over 4 years ago Dr Bernadette Wren gave a talk on ethico-legal issues arising in the care of gender-variant children and adolescents. She was a consultant clinical psychologist at the Tavistock & Portman NHS Foundation Trust. I did try to find out if I could see exactly what she said here because I think we take quite different views but, unfortunately, that talk wasn’t published.
She wouldn’t allow it.
That explains why I couldn’t find it.
The Dutch protocol
Let me begin with the Dutch protocol. I’m reporting my research that was published in an article on the ‘Dutch Protocol for Juvenile Transsexuals’ and I use that word, that very unfashionable terminology, for reasons which will become obvious in a second. 1
I begin with a psychologist called Peggy Cohen-Kettenis who founded the Children’s Gender Clinic in Utrecht in 1987; it was the first gender clinic for children in Europe and one of the first, of course, in the world. She was very enthusiastic about transitioning adolescents at younger ages; she thought that if you did it younger you would get better results. The key pharmacological breakthrough was this new drug, Gonadotropin-Releasing Hormone agonist (GnRHa), originally used to treat prostate cancer and precocious puberty in children. The idea was that this could actually be used to halt puberty in children suffering from gender dysphoria. This is the reason why I use the words ‘juvenile transsexuals’ as this was the title of the first article that was published in the scientific literature by Louis Gooren and Henriette Delemarre-van de Waal, an endocrinologist and a psychologist at the Amsterdam Medical Centre, ‘The Feasibility of Endocrine Interventions in Juvenile Transsexuals’ and I think that phrase is worth underlining. 2
The key article was in 1998 by Cohen-Kettenis and van Goozen, a case study of a patient who we know as B. 3 She had always been a classical tomboy in her play activities, her choice of toys and so on; she liked to hang out with the boys, she wanted to be a boy, but the father was from Italy and he wanted a girly-girl and this led to family conflict. So what Delemarre-van de Waal thought was, we’re going to experimentally prescribe GnRHa, which we call ‘puberty blockers’ when they’re used for gender dysphoria, for B when she was aged 13. Then she endured 5 years without sex hormones and then, when she reached 18, very quickly went through the whole transition process: testosterone, mastectomy, oophorectomy (removal of ovaries), hysterectomy, genital surgery, and change of legal sex.
As a result of all this, according to the article, B had no gender dysphoria at all; ‘he’ had found adjustment to the male role very easy. So here we have a case study of a kind of miracle cure, obviously, B can now continue living as a man and live a happy and contented life. That was the promise of puberty suppression. You can see the rationale behind the Dutch Protocol.
The Dutch Protocol, which was formally institutionalised in the early 2000s, starts at Tanner Stage 2 or age 12, whichever is the oldest. The child starts with puberty blockers, then at age 16 they get cross-sex hormones and at 18 they have surgeries. The Dutch are very keen and it really is a conveyor belt: as soon as you reach 18, they want the adolescent to get all the surgeries done as quickly as possible so they can get on with their life.
The eligibility criteria are (1) gender dysphoria from childhood which became worse at puberty; (2) the adolescent has to be psychologically stable and (3) have support from the family. The key selling point of the Dutch Protocol, as we saw with B, is it results in a high proportion of individuals who more easily pass into the opposite gender role than with treatment commenced well after the development of secondary characteristics. Really the emphasis is on appearance – B looked like a man at the age of 20 – and you find this throughout the Dutch publications. I repeat, the emphasis is on appearance, not on sexuality or fertility. For example, they’re obsessed with height. Was B tall enough? B was actually quite short for a Dutch bloke, having a Mediterranean background and being female, so they were very worried about whether B was tall enough.
Reading the literature on the Dutch Protocol, there were two interesting rhetorical devices used to justify this technology. The first is the claim that puberty blocking is reversible, ‘no lasting undesired effects are to be expected’. 2 Their phrasing is revealing: we don’t have evidence that there are no lasting effects but we don’t expect there to be any lasting effects. Of course, this justifies starting under the normal age of medical consent of 16. The reason why they started cross-sex hormones at 16 was that this was age in the Netherlands at which you could ask a patient to consent to permanent intervention, but if they said that puberty blockers are reversible, then that’s okay, they didn’t have to worry so much about consent.
The second rhetorical device was the notion that it wasn’t just a treatment, it was a treatment and diagnostic tool rolled into one. It’s a very helpful diagnostic aid; it allowed the psychologist and the patient to discuss problems that possibly underlie the cross-gender identity. Even in the same article where they say it’s a diagnostic aid, they say that none of the patients selected for pubertal suppression had decided to stop taking GnRHa. So it’s a diagnostic tool that always gives the same results: the kid is a ‘juvenile transsexual’ and they need to proceed to cross-sex hormones and surgeries.
These rhetorical devices lead to the common description of puberty blockers as ‘hitting the pause button’. It’s often said by clinicians and I’m sure Bernadette Wren said that same thing here in 2018, we’re just pressing the pause button; it’s completely reversible.
Then there are silences in this literature on the Dutch Protocol. The first and maybe the most puzzling is the disappearance of homosexuality, because it is well known that there was a strong association between same-sex attraction and people who have a cross-gender identity. Even Gooren and Delemarre-van de Waal in this first article say, ‘Not all children with gender atypicality will turn out to be transsexuals later in life. Several prospective studies of gender atypical boys show that this childhood behaviour correlates considerably stronger with future homosexuality than with transsexualism’. 2 One study published as The Sissy Boy Syndrome followed young prepubescent boys who were identified as prospective transsexuals, but almost all of them ended up as gay. 4 Gooren and Delemarre-van de Waal assert, ‘Some of the youngsters will turn out to be genuinely transsexual in their mid-teens’, but of course they started puberty suppression at 12, so I don’t know how they squared that circle.
The other problem is a problem for males only. If you suppress puberty young enough, their male genitals won’t develop and so you have the penis and testicles of a pubescent boy which makes it much more difficult to get the vaginoplasty later because a vaginoplasty uses the skin of the penis and testicles to create the new neovagina as it’s called. So, as a result, they had to use much less satisfactory techniques which included using some of the bowel to line the neovagina. Weirdly enough, they only admitted this in 2008 even though it should have been obvious all along to an endocrinologist – but that was the first appearance of that problem in the literature.
So this was the Dutch Protocol and how it was justified. The Amsterdam Gender Clinic is the most prolific in terms of scientific output and it was very influential. The numbers of adolescents subjected to puberty suppression increased over time. At the beginning in the 1990s it was about one per year. As the Dutch Protocol was formalised in the early 2000s it was a couple per year, but then the numbers just keep growing and growing. By 2017, they were doing 170 per year. At that point they could no longer do them all in Amsterdam and they had to create satellite clinics all over the country. In 2023 the forecast was we will see 900 patients going through puberty suppression each year. So you can see growth on three orders of magnitude, from 1 to 10 to 100 to almost 1000. Their thinking about puberty suppression has not changed at all despite that massive increase in the number of patients.
Even at the same time as Dutch clinicians were publishing the first scientific articles there was a very widely-watched documentary from Channel 4 called The Wrong Body. It was a British documentary that took three young females who were suffering from gender dysphoria, including one young kid about the age of 13, to Amsterdam to see the miracle taking place. This was watched by 3 million viewers and I think had a big impact in spreading the word of this new ‘miracle cure’. There was a very revealing interview with Cohen-Kettenis in the documentary when she said, ‘It’s very difficult to give exact criteria, in some cases you have the feeling that the adolescent has thought about and knows pretty well what she or he is doing’, so a rather intuitive approach to diagnosis. Also what is interesting is what Gooren, who is the endocrinologist, does after interviewing this young girl from England who identifies as a boy. The parents take her back to London, she goes to what is the precursor of the gender identity clinic at the Tavistock where the psychiatrist says, we’re not going to prescribe anything until you’re 16. So the mother rings up Gooren and asks him to prescribe puberty blockers and he agrees. He prescribed Triptorelin for 3 months, which is allowed under EU law and could be collected at the local pharmacy. Wasn’t that a cavalier approach to prescribing?
After just one case study was published, the new Dutch Protocol was incorporated in the World Professional Association of Transgender Health’s Standards of Care. As the Protocol was adopted outside the Netherlands the minimum age was removed. The Netherlands are pretty strict on 12 years of age (sometimes lowered slightly to 11.5), but when this Dutch Protocol was taken outside the Netherlands clinicians just said whenever Tanner Stage 2 starts – the beginning of puberty so this could be as young as nine – that’s when we can start puberty blockers.
All of this has happened without any real evidence, but in 2011 – this is the evidence that will provide the foundation for this practice – an article is published on 70 adolescents in the Amsterdam Gender Clinic, the first cohort that has gone through the Dutch protocol. After spending some time on puberty blockers, ‘Behavioural and emotional problems and depressive symptoms decreased, while general function improved’. 5 So this seems good evidence for this treatment.
The Tavistock’s early intervention study
Now I will pause and go across the channel from the Netherlands to England. The Tavistock’s Gender Identity Development Service, as we saw in The Wrong Body, even up to 2010, they were not offering any medical intervention under the age of 16. It was purely therapy, talking therapy with psychologists, until you reached 16. Obviously they came under increasing pressure from the parents of transgender kids who would say they could go to the Netherlands or even to America to get private treatment. As a result, the Gender Identity Development Service at the Tavistock (the GIDS) say, we’re going to do a research study which will use puberty blockers early. In fact, just as Bernadette Wren was giving her lecture to the Medico-Legal Society, I was digging round trying to find out about this study: I emailed the Tavistock in early 2019 and asked, ‘What happened to the study?’ because I had discovered the initial press release on their website. They never replied to my email. I thought that was odd, because researchers are usually very keen to share their research, that’s what we want to do, and by that time it was 7 years after the study was publicised, so what happened?
What we know now is that there were 44 patients involved in the study, starting in 2011; they were aged 12–15. 6 The last was recruited in 2014. That same year Polly Carmichael, who was the Director of the GIDS, says, ‘Now we’ve done the study and the results thus far have been positive we’ve decided to continue with it’ and in 2015 NHS England then made puberty suppression from Tanner Stage 2 – no age minimum – the national standard. So what had before been a sort of experimental treatment done at one particular clinic now becomes the standard that everybody in England has the right to get. This is ‘healthcare’.
What I discovered is that in 2015 the results from 30 of the patients, the first two-thirds of those patients, after 1 year on puberty blockers were presented to the Tavistock’s Board of Governors and they were actually more negative than positive, but nobody had taken any notice of that. In 2016, Carmichael had given a presentation to the European Professional Association of Transgender Health and I tracked down the video of it – there’s no paper but there is a video – and she says, ‘Our results have been different to the Dutch’. So, clearly they weren’t replicating. They obviously set up the study quite legitimately to replicate the Dutch findings but they weren’t finding the results they expected.
This graph (Figure 1) is actually from my analysis, the first time that these results for the 30 patients were properly analysed. 7 There are several different scales of psychological functioning. Improvement is on the right-hand side, decline is on the left-hand side. The black bars show the original Dutch results. 5 You can see that on all the scales, the Dutch kids are getting better. The grey bars show my calculation from the presentation to the Tavistock Board of Governors and you can see that they are much more mixed. It’s a small sample, and so the estimates are very uncertain, but you can certainly see worrying results for the girls. Internalising problems like self-harm and negative thoughts are getting worse; this is from the Child Behaviour Checklist, where parents have described problems their kid is having. That scale is significantly worse even with this small sample.
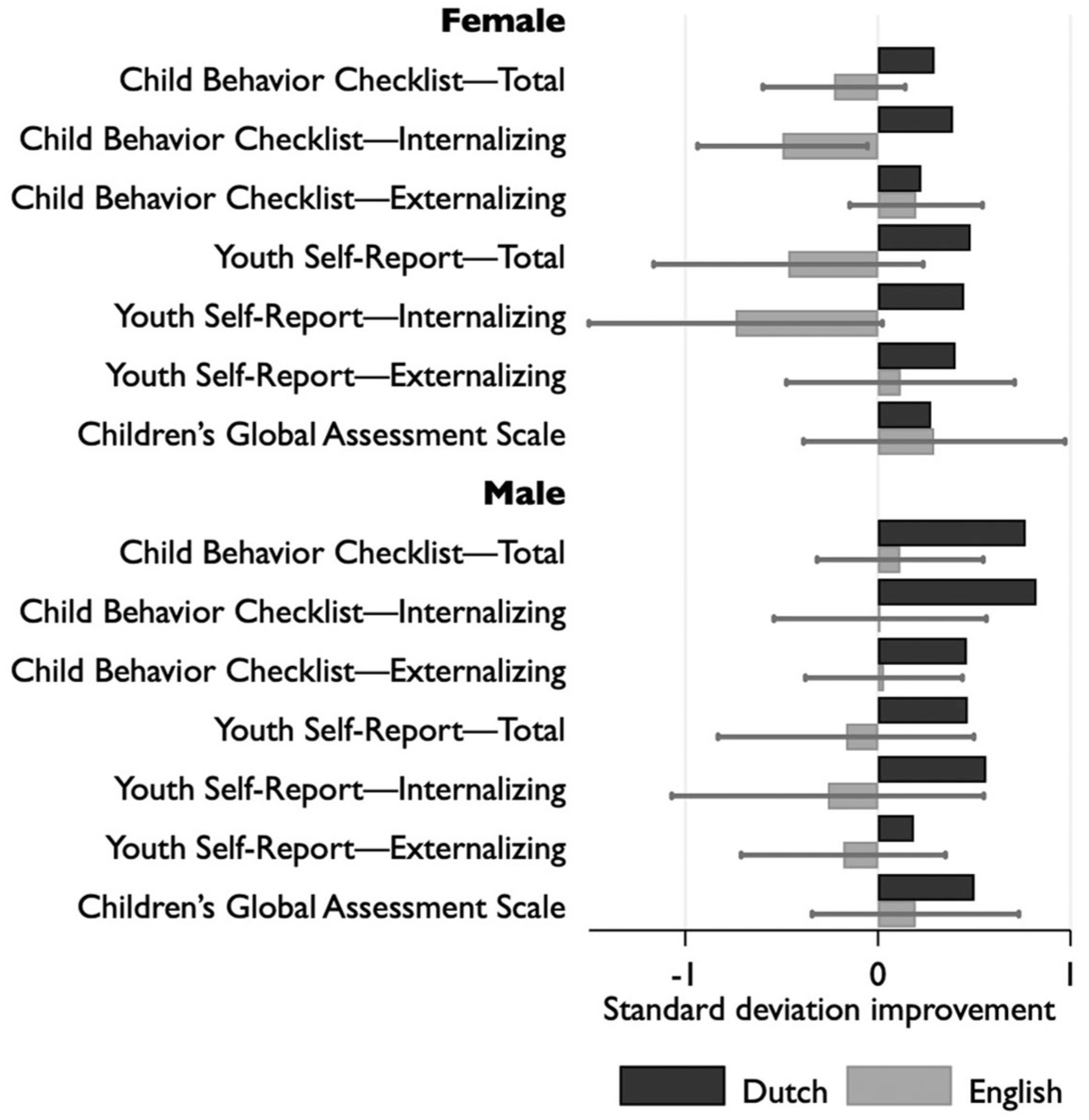
Change in psychological functioning after puberty suppression. The magnitude of the bar represents change after treatment divided by standard deviation at baseline; for the English sample, the line traces the 95% confidence interval. Positive values indicate better functioning. (Reproduced from Biggs 2020).
After digging round and getting what I thought were negative results or at least unfavourable results, I presented my research on Stephanie Davies-Arai’s blog Transgender Trend. 8 Then we managed to get it into the mainstream media. The Telegraph was the first paper to run the story, ‘NHS Transgender Clinic accused of covering up negative impacts of puberty blockers’ (7 March 2019). I was interviewed by BBC’s Newsnight and then it became more of a story.
The next landmark is this case brought by Keira Bell, who had gone through the transition process at the Tavistock clinic, and Mrs A, who was the mother of a child who identified as trans, and who was worried about her child getting these interventions. This was a landmark judicial review case. The judgment came out at the end of 2020, and it’s worth quoting some of the judgment. 9
First of all, the judges said there was a real ‘lack of clarity over the purpose of the treatment: in particular, whether it provides a “pause to think” in a “hormone-neutral state”’ – that is the diagnostic tool – ‘or is a treatment to limit . . . the need for greater surgical and chemical intervention later’.
So they put their finger on that ambiguity, and they emphasised just how difficult it would be for a young person to consent, given the range of different things you would have to consent to if you were a 12-year old or even a 10-year old. In the extreme cases you would have to understand the immediate consequences of the treatment in physical and psychological terms; the fact that the vast majority who take puberty blockers go on to cross-sex hormones, so therefore, you are not just consenting to puberty blockers but you’re actually consenting to a very high probability of the next stage, a pathway to being a lifelong medical patient. You would also need to understand the relationship between cross-sex hormones and subsequent surgery (and obviously vaginoplasty is the most salient concern); the fact that it might result in a loss of fertility; the unclear impact on sexual function; the impact of this on future relationships; and of course the fact that the evidence for this treatment is highly uncertain.
The judges pointed out that the GIDS always assessed children even as young as 10 as being able to consent. There was not a single case where the GIDS said, ‘Actually, this kid wants puberty blockers and maybe they are medically indicated but, unfortunately, they lack the competence and maybe they lack the understanding or maturity to consent’. Everybody always consented and, in fact, the Care Quality Commission in the subsequent year when they tried to track down the records of consent found that the records of young people who began medical treatment before January 2020 did not include a record of their capacity, competency and consent. Why do they suddenly start filling in these forms in January 2020? As Keira Bell and Mrs A launched their legal case in January 2020 maybe the date is more than a coincidence.
It was also very clear – I attended the trial as well as presenting written evidence – that the judges were astounded that the Tavistock could not supply basic information. For example, they asked what proportion of the GIDS patients were autistic. The Tavistock said they did not know, and when the judges asked whether they could provide the information tomorrow, the Tavistock stated baldly that they just didn’t have the information. The judges also noted, as I pointed out, that the results of the 2011–2014 study had still not been published. Some of the witness statements from the Tavistock stated that they were almost ready to publish, but they used COVID as the excuse.
Surprisingly enough, the very day after the judgement was handed down, the study’s results were posted on medRxiv. 10 To quote from the preprint, ‘GnRHa [puberty blockers] brought no measurable benefit nor harm to psychological function in these young people. . . . Gender dysphoria and body image changed little’. So what they’re saying is, we didn’t see an improvement, and we also didn’t see any decline. In fact they hypothesised that they wouldn’t find any improvement in the statistical analysis plan which was given to the Health Research Authority 2 days before the Health Research Authority emailed me the result of their investigation of my complaint in 2019. So I think it’s very clear that a statistical analysis plan was created as a result of my complaint and, of course, if you compare the statistical analysis plan in 2019 with the protocol that they put forward to get ethical approval in 2010, of course the protocol said, we expect this to reduce gender dysphoria and improve psychological functioning. That was the result of the first Dutch study and so of course they thought they’d find the same thing here. But when they didn’t find that, they then retrospectively decided, we didn’t really expect to find any improvement anyway.
The judgment in Bell and Mrs A was a humiliation for the Tavistock. The Tavistock then appealed and they won on appeal. The judges now said that the High Court in the judicial review had not found the Tavistock’s Policy and Practices to be actually illegal. Note that these Policy and Practices were dated 31 January 2020, just after the Keira Bell judicial review proceedings were initiated. But the Appeals Court found that the High Court shouldn’t have been providing guidance on Gillick competence. The High Court had found that it was really very unlikely that a child under 16 would be able to consent to this, but the Appeal Court said they had no business in making that sort of claim. It really is for clinicians to exercise their judgment about competence and this has been debated, there is medical evidence around puberty blockers, it’s not for judges to weigh in.
So the High Court judgment was no longer in force. However, the key thing is that this first judgment had a huge impact in opening up the debate. Before it had really been just a few ‘cranks’ who were questioning this. Some radical feminists, Stephanie Davies-Arai, some worried parents, some crazy sociologists – but in 2020 it seemed that scepticism had the support of some important members of the establishment. So even though the initial ruling was overturned, it had a huge impact not just in Britain but in other countries as well.
Subsequent evidence
Now I’m going to do a very quick run-through of the subsequent evidence.
The first Amsterdam cohort, these ones that apparently did well on puberty blockers, were followed up subsequently and most of them were surveyed after their surgery in their early 20s, and, again, seemed to show very positive results. ‘Gender dysphoria had resolved, psychological function had steadily improved, and well-being was comparable to same-age peers’. 11 So the Dutch were finding apparently good results. However, there were only a relatively few observations. The headline figure was 55 but the actual number of observations for some statistics were as low as 32, quite a small sample.
The authors also did something which is a bit odd: they switched the gender of the Utrecht Gender Dysphoria Scale. 12 So if I’m male and I go to the gender clinic and say that I want to be a girl, they give me the scale for males. It’ll ask, for example, whether ‘I dislike having erections’ and I’ll say yes because I want to be a girl. Then after transition, they give me the women’s scale which asks me whether ‘I hate menstruating because it makes me feel like a girl/woman’. Of course I would say no because I don’t menstruate. Comparing the scales before and after suggests my gender dysphoria is resolved – but, of course it is partly an artefact, not entirely, but partly an artefact of changing the sex of the dysphoria scale.
The other thing that the Dutch mention but don’t actually explain is that one patient was killed by the vaginoplasty. This was the result of puberty blockers preventing the genitals from growing, and so rather than using the penis for the vaginoplasty, the surgeons had to use part of the patient’s intestines instead. That caused an infection and this patient quickly died in the hospital. That means the clinic started off with 70 healthy Dutch kids, and had a death rate of over 1% which is actually quite significant.
We still only have favourable data from the Netherlands. There have been quite a few American studies which are really poor because they used different measures, they used tiny samples, inconsistent recording of results, and very high attrition rate. So they’ll follow kids over a year or 18 months and then 50% of them have disappeared over the course of that time, so you’ve got no idea what happened to the rest. Maybe the ones who stayed on medication were doing better but what happened to the ones who dropped out? This is very bad scientific practice because they should have used the same measures that were used by the Amsterdam Gender Clinic, just as the Tavistock did. I have a lot of criticism of the Tavistock research but at least it was properly designed to replicate the Dutch research.
Then to overcome all these problems, the U.S. National Institutes of Health gave millions of dollars for a multi-site prospective study of puberty suppression. Ninety patients (or slightly over 90 patients) were recruited from 2016 to 2018 and the results have never been published. A few months ago Olson-Kennedy finally came out and said why she was not publishing the results: she said, ‘I do not want our work to be weaponized’ by the transphobes. ‘The kids are in really good shape when they come in, and they’re in really good shape after two years’. 13 This is very odd because they did report the baseline results in 2019 and the kids aren’t in good shape, so that is obviously extremely misleading – and also of course the whole point is that they are meant to improve. 14 Again, it seems to be a repeat of what happened at the Tavistock: you expect improvement, you give the kids the puberty blockers, they don’t improve – they don’t get worse but they don’t improve – and then you say, well, that doesn’t matter because we didn’t expect them to get better anyway. I think it’s a travesty that somebody could take public money from the NIH, and have this data available now, the results for these kids. You had 2 years on puberty blockers by 2021 and 3 or 4 years later there is no publication, and I think that is scientific misconduct.
In terms of the long-term outcomes, the very long-term outcomes, we have precisely one case study and this is the guinea pig, the tomboy B, who was followed up at the age of 35. 15 B says he had no regrets about his treatment, that the negative side effects are limited, so that’s good, and Cohen-Kettenis and the co-authors present this as a good result except they’re obsessed about the height, that he’s not tall enough. But if you read the text closely it says he’s split up with his girlfriend because of shame about his genital appearance and has feelings of inadequacy in sexual matters. So, actually, it does seem not quite as good as it seems in the abstract of the article and, moreover, if you’re ashamed about your genital appearance, isn’t that gender dysphoria? So there were much more equivocal results. Also, I should have pointed out when I mentioned B at the start that B is a tomboy who hangs out with the boys and plays with boys’ toys. Have a guess at their sexual orientation and, of course, we find out later that B has a girlfriend.
The only fragmentary evidence that we get of what has happened to that Dutch cohort now is there was a conference presentation which I’ve seen a transcript of, but they only get a 50% response rate. 16 So, for some reason, they can’t follow up enough of these kids and journalists have heard that there have been at least one or maybe two suicides.
Again, we come back across the channel to Britain. The GIDS won $1.8 million to follow the longitudinal outcomes of the Gender Identity Clinic. They have not published anything from the study and, in fact, Gary Butler, who is the endocrinologist who used to work with the GIDS, admitted in 2018 that basically they can’t track people beyond the age of 18. The problem is that they will change their NHS number in order to conceal their previous sex and that means – though I’m sure it’s technically possible – according to Butler, ‘to date they have not been able to be followed up’. 17 They have no idea whatever happened to any of their patients as adults.
Dr Hilary Cass did try to commission research on this but she said, ‘I’ve received significant opposition from all but one of the adult GDCs [Gender Development Clinics]’. 18 The great thing about having an NHS is that we should have all the records and we should be able to have bona fide researchers following up to find out what has happened, but that is not happening in gender medicine.
We know that there is one negative side effect which is bone density. Even the gender clinicians will admit this, but I don’t think they’ve quite admitted just how bad it is. Figure 2 shows my re-analysis of data that was presented by Butler and colleagues from the early intervention study. 19 The data were only available because I made that complaint to the Health Research Authority. The authors say that if you look at the bone density of kids after 2 years on puberty blockers, well, it goes down – relative to the norm for their sex and age – but it’s not really a big deal. In fact, they conclude that we shouldn’t be wasting money on expensive bone density scans. 20 In fact, when I analysed the data, you can see that, actually, a significant minority of these kids have really low bone mineral density. The bell curve is what you’d expect for this age and sex and the grey bars are what we actually find after 2 years of puberty blockers. You can see a significant number of kids below −2 which is a risk of osteoporosis. Even in this small sample (24 for the spine and 21 for the hip), you can see that there are quite a few who are below −3 for the spine, so that is really extreme lack of bone density for their age and sex. In terms of the longer-term consequences of that, we know now that a Swedish adolescent who was taking puberty blockers suffered from severe osteoporosis and indeed there were a number of kids who were having problems with bone density which led the Swedish authorities to say, we’re no longer going to offer this as a regular treatment. 21
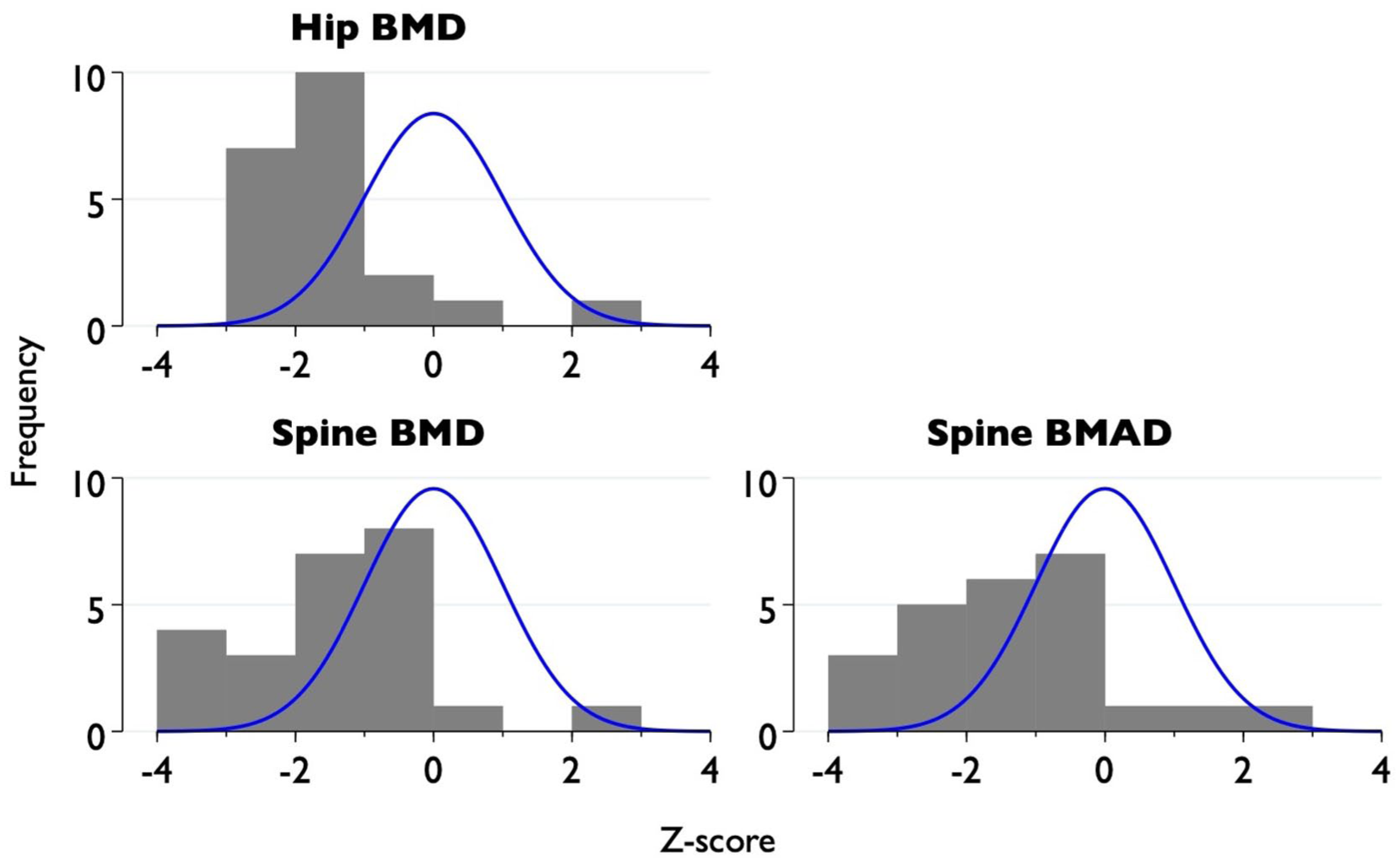
Bone density after 2 years on puberty blockers. Z-score shows the individual’s bone density standardised relative to the population of the same age and sex (shown by the blue curve). (Reproduced from Biggs 2021).
What is probably more worrying are the unknown effects. Finally, many years after this was used to treat children with gender dysphoria, we actually have some good studies, proper randomised control trials in non-human animals. So we do find in experiments on sheep that their spatial memory is impaired after taking puberty suppression and the effect is not reversed after the treatment stops.22,23 So the idea that this was reversible turns out to be wrong. We know that mice have increased stress response, anxiety and despair-like behaviour when they’re given puberty blockers; with macaques the effects of experimental delay of puberty on brain development were broad and profound.24,25 The curious thing about this is that the endocrinologist in Amsterdam, Delemarre-van de Waal, actually had a whole laboratory full of rats, so she could have actually done some testing on animals herself. Instead, she just chose a human guinea pig, B, to experiment on.
More recently, the President of the World Professional Association of Transgender Health, Marci Bowers, who is a surgeon who does vaginoplasties, was caught on video saying, ‘Every single child . . . who was truly blocked at Tanner stage 2 has never experienced orgasm. I mean it’s really about zero’. 26 I think that is probably an exaggeration but clearly, even among gender clinicians, there’s a worry about the effect of early puberty suppression. De Vries’s comment when she was asked about this by a journalist was that orgasm is ‘a very interesting and so far not studied question’. 27
Conclusion
Let me draw to a conclusion and summarise what you’ve seen. I’ve argued that there’s really scanty evidence for the benefits of puberty suppression. All the evidence relies on these 55 Dutch adolescents. Replications outside the Netherlands in England and America have failed to show favourable results. There is literally only a single patient in the published medical literature for whom we know the long-term outcome and that was mixed. There is a continual pattern of failure to collect long-term outcomes, despite the absolute requirement for scientists and clinicians to publish results even if they are not favourable to the treatments that they are advocating.
One final speculative reflection. It’s true that only a small number of adolescents who are going through a transition or identify as transgender undergo early puberty suppression. Even if you look at the ones who go for medical intervention, the typical patient would be a 17-year-old girl who thinks she’s non-binary or thinks she’s a boy, and of course puberty suppression is irrelevant in that case. However, even though only a small number of children have undergone early puberty suppression, they dominate media portrayals and they help to construct the image of the transgender child. It’s very telling that all the media-friendly trans kids have had early puberty suppression: Jazz Jennings in America and Jackie Green in the UK; there was also a trans boy called Leo who was featured on BBC Children’s television; and Valentijn de Hingh, a very famous transgender woman in the Netherlands. So actually they have an outsized role in constructing this idea of a transgender child. Moreover, the availability of puberty blockers becomes a kind of self-fulfilling prophecy because it makes social transition feasible. Before puberty blockers, it was not really possible to socially transition in school because, obviously, your emerging sex characteristics would become visible to everyone. But the availability of puberty blockers makes social transition in school possible; consequently, social transition becomes a self-fulfilling prophecy because it locks in the transgender identity.
I think the final broader cultural ramification of puberty suppression is that you begin to conceive puberty not as a crucial life stage that we all have to go through in order to become adults – but as literally a disease or almost like a disease. As de Vries, the most published Dutch gender clinician, says, ‘Disallowing puberty suppression, resulting in irreversible development of secondary sex characteristics, may be considered unethical’. 5 This is why she said we can never have a randomised control trial because it’s actually unethical not to stop puberty. So the broader social and cultural implications of puberty suppression are very wide.
Thank you. (Applause)
Discussion
I found it all fascinating, but what I found particularly fascinating is your comment about the recent funding of a longitudinal study because, to extrapolate, as the NHS number changes, does that mean you could never follow up long-term people who had transitioned?
I am sure there is a way of doing it but I think there was a lot of objection from transgender advocates. I am sure that technically there must be some way of mapping the numbers but I think it was considered that there were legal and ethical obstacles to matching the numbers.
And yet they were happy to accept the money for the study.
Yes, exactly. Whether they were going to try to match the numbers or whether they were just thinking that long-term means up to the age of 18 is not clear.
Diana Brahams, retired barrister, Editor of the Medico-Legal Journal. I’m curious to know how it is that the Dutch study had results that seemed to be so different from everybody else’s. It does make me wonder whether we should have looked a little more closely at the Dutch study itself. Have you any information on that?
In some ways you might think it strange but, actually, it’s very, very common in medical research and scientific research. The first researchers who have a hypothesis or a new drug, they test it in their hospital or in their research laboratory. There are great results, they publish it in Nature or The New England Journal of Medicine or whatever and then other hospitals try to replicate it and the effect goes down. I think it’s very, very common and it could be for various reasons: it could be placebo. I don’t think it’s dishonesty, I think you are very, very excited about this new technique and you convey that excitement to the patient. Maybe you choose the patients who you think are most likely to respond. It could be that they were much more cautious in which patients they were putting on it. It could be that some of the missing data was maybe less favourable. I think it’s just in the nature of things and that’s why we need replication.
There could be one other reason and that is that the kids who come in, Dutch kids, are much healthier in mental health than English kids. It’s a much healthier society for bringing up children. The kids who come to the gender clinic in the Netherlands are generally better on these psychological measures, they’re already better than kids going to clinics in Switzerland, Belgium, and England – the English kids are the worst off. It could just be that maybe it works if you’re already doing quite well. That’s conjecture but you can’t rule that out, but if you’re doing very badly, then of course you don’t respond positively. That’s a possibility. I think it’s very common for very good results to end up not being replicated elsewhere or at least to have a much lower magnitude elsewhere.
One other point, you talked about non-human studies, but the usual way round in medical research is to try things out on animals before humans, but here it seems to me that they tried them on humans first. Is that right?
Exactly, yes. I think what they said was, well, we know that it’s been tested – I’m sure GnRHa was tested on animals before being given for prostate cancer – and we know it works because, ultimately, what they’re saying is, we know these drugs stop puberty, that is not a debate, the question is what are the other implications of that. As I said, Delemarre-van de Waal actually had rats in her lab, so she could have easily started out doing the experiment on animals but she didn’t. So, yes, it’s very puzzling to me and I’m just as puzzled as you are about that.
That raises another profound point. Sue Evans was a nurse at the Tavistock who left in 2005 – she was actually the first whistleblower – and one of the things she said when giving a talk recently really stuck with me, which is that sometimes the clinician is medicating not just to remove the children’s distress but to remove the clinician’s distress. So here you’d have the child coming in very, very distressed and you think, I have this drug, I can give it to the kid and the kid will feel better and I won’t feel so upset after seeing the kid. So I think there is some sense of you have this apparently good medication, why wait 5 years before you do the animal study and publish it? The kid is suffering now. Let’s give the kid this apparently great cure.
Geoff Simpson-Scott, I’m a solicitor at Hodge Jones & Allen. Thank you very much for your lecture. Please say if this is an unfair question. Do you feel there’s a top three set of misconceptions or maybe cognitive biases which influence treatment decisions and, if so, what can we do to avoid making them in practice?
That’s a tough question! The top three and you’re talking about work for the clinician. I think one is that in some sense when you’ve got a hammer the whole world looks like a nail. So if you’re in a gender clinic, you do gender treatment, you do cross-sex hormones and puberty blockers. So there is a lack of understanding of maybe there are other issues going on with the kid’s life and you just see it as, let’s focus on the gender because that’s what we’re specialists in. In fact, I think there is a phrase in the literature about this, ‘The name of your clinic is what you give the diagnosis for’. The kid comes to a gender clinic and you give them a diagnosis of gender dysphoria and if they went to the autism clinic, you’d diagnose them as autistic and so in some sense you diagnose the name of your institution. I think that’s one thing, there’s a lack of joined-up thinking and that’s been very clear for many years and Sue Evans herself put that argument forward very early on. She was, as I said, the first whistleblower and the Cass review obviously makes that point again. These are obviously kids with many different problems, often very high rates of autism, depression and eating disorders, and the very fact that they have eating disorders is one of the reasons why their bone density is so bad after puberty blockers. I think a lack of understanding of lots of co-morbidities.
Secondly, selecting. I think you become invested in the treatment you’ve given. So obviously once you’ve given puberty blockers for quite a few years to many dozens or hundreds of patients, it becomes very hard to say, actually, maybe now that we’re looking at the results or being forced to look at the results and to admit that the results weren’t good, now can you really say that was all maybe dubious. It’s very hard because then of course is the question, am I going to become liable? Now that I’m admitting that I gave this treatment without good evidence, now maybe I’m liable for people coming to me and saying, ‘I want compensation’.
What would be the third? I think the third would be focusing on these positive results. There’s a very famous article by John Ioannidis, that most published medical research is wrong. So just because something has a flashy result in a journal, don’t trust that result until you see replication in studies that are not done by the original authors. So I think kind of an optimism bias in thinking, oh, there’s a latest treatment, apparently it gives good results here, therefore it must be great. Be a bit more cautious about adopting the latest what seems to be a miracle cure.
Gina Weston-Petrides and I am a surgeon. You talked about the long-term follow-up. Even if the hospital number isn’t changed within the NHS, long-term follow-up is actually really difficult in a lot of studies. So the loss to follow-up number is really high in all studies like this. On that point, you mentioned about the researchers being happy to receive the money. I wonder what’s the accountability of the body that awarded the grant. I think that’s quite significant because they made the final decision based on the presentation given to them about the grant application. There must have been quite a few holes in that initially to start with but even before the study was started and you’ve brought up a few points already. I’m just wondering what that looks like.
That’s an excellent point and I think they should be accountable, but I found that when I went to the Health Research Authority which ultimately gave ethical approval for the first early intervention study, they were actually quite reluctant to get involved even though the researchers had breached their terms in terms of submitting annual reports and so on. I think they tend to give the money and don’t do anything. The one experience I have had in trying to get some changes is actually a different grant. The National Institute of Health Research gave a grant to the University of Oxford – about £700,000 – just to interview trans kids and parents about what sort of care they wanted. Unfortunately, they actually put up on the Healthtalk website all these transcripts from these trans kids who praised GenderGP for giving drugs like puberty blockers at competitive prices. It was very odd, why are you advertising this company that’s registered in Singapore using the Oxford logo and the NHS logo? I was able, through a lot of complaint and writing an article in The Critic, to actually get them to redact that commercial advertisement. The researchers had originally asked GenderGP to help recruit kids for the study. 28
The doctor running it was erased from the Medical Register, or suspended.
Yes, there were two doctors, a husband and wife, and the husband was struck off for dishonesty and breaches of medical ethics. The wife, Helen Webberley, was suspended though later her suspension was overturned on appeal. But it’s incredible that the National Institute of Health Research funded the project that put that advertisement up with an Oxford logo on it. Unfortunately, the quality of medical research in this area is not high.
We have to leave it there because we’ve come to the end of our time. Thank you once again, Dr Biggs, for talking to us. (Applause)