Abstract

Our speaker tonight is Professor Mike Tipton. Professor Tipton is Professor of Human & Applied Physiology at the Extreme Environments Laboratory in the School of Sport, Health & Exercise Science at the University of Portsmouth. He has spent nearly 40 years working in the areas of environmental and occupational physiology. In that time, he has also worked at the Institute of Naval Medicine and was Consultant Head of the Institute’s Environmental Medicine Division from 1996 until 2004. He is a prolific author with over 750 scientific papers, reports and abstracts in his research areas which include drowning, thermoregulation and survival in the sea. He has been a trustee and director of Surf Lifesaving GB, he is a member of the Council of the RNLI, and a consultant in survival and thermal medicine to the Royal Air Force. As well as being a prolific writer, Professor Tipton also edits various scientific journals as well as being a visiting Professor at King’s College, London and a Fellow of both the Royal Society of Medicine and the Physiological Society. He was awarded an MBE for his services to physiological research in extreme environments, the Ireland Medal for saving lives from drowning worldwide and the H&L Swiftwater Rescue Lifetime Achievement award in the USA.
My researches tell me that his particular interests include the physiological, pathophysiological and psychological responses to adverse environments. I hope that the environment he is about to enter now will not test his knowledge any further.
Mike, thank you for agreeing to address us tonight and welcome to the Medico-Legal Society. (Applause)
The image that people have of Earth is of a blue oasis in the grey wasteland of space. But, in reality, the vast majority of our planet is covered in water and most of that water is dark because light only penetrates 50 to 80 metres into water and the average depth of the ocean is 4,000 metres. On the land, there is a lot of desert, ice, permafrost and mountains, leaving about 15% of the planet where most people live. For a tropical animal like humans, who evolved in 28°C low-altitude air, submersion in cold water represents a significant hazard.
At the Extreme Environments Laboratory at Portsmouth University we examine the physiological, pathophysiological and psychological responses of humans to extreme environments, and the protection, preparation and selection of those who enter these environments.
In this presentation I am going to concentrate on immersion; some of the reasons for this can be seen in Slide 1. Drowning is a pandemic that has claimed and changed lives, many of them young lives, for centuries. Climate change and its consequences (e.g. flooding, rising sea levels) are set to increase the risk of drowning. The 1000 deaths a day from drowning around the planet is probably an under-estimation, because a lot of them are in low-income countries where drownings go unreported. So, we think it may well be several times that number. In the UK we lose somebody about every 30 hours, one child a week.
The perceived problem associated with cold water immersion (CWI) was established by the Titanic disaster. One consequence of this accident was that people closely associated CWI with hypothermia. You still hear people saying, “You only have a few minutes in water this cold before you succumb to hypothermia.” It is physically impossible for an adult human to lose the amount of heat necessary to become hypothermic, even if naked in 0°C water, in less than about 30 minutes. We are too big, and we have too much mass and heat content to become hypothermic in minutes. Unfortunately, the preoccupation with hypothermia has, historically, driven: the kind of protective equipment that people are provided with; the protocols for search and rescue; and the expected resuscitation challenges of immersion casualties.
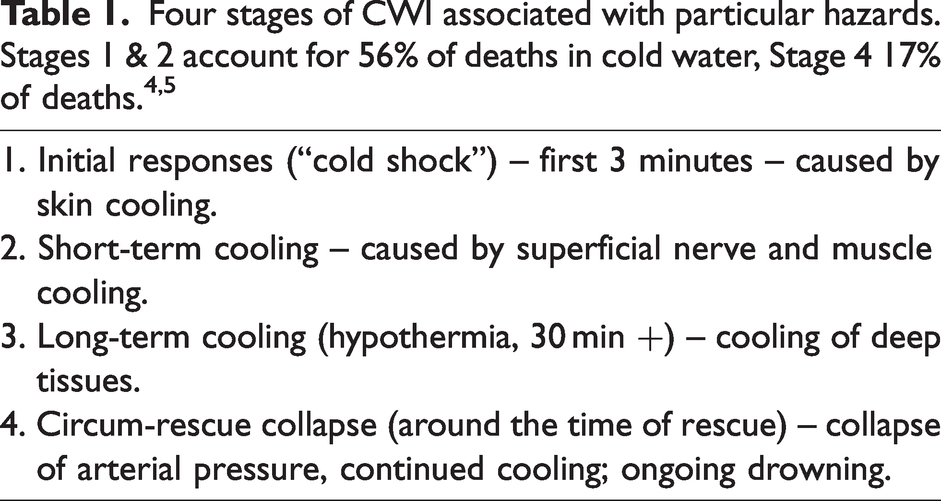
In the 1980s we spent quite a lot of time researching what kills people on CWI. My dear friend and colleague, Surgeon Rear Admiral Frank Golden RN OBE, identified four stages of CWI associated with particular risk (Table 1). We started to investigate these stages and identify their contribution to immersion deaths in cold water. I will review these stages and some of our work aimed at correcting the misconception that the primary problem on CWI is hypothermia.
Stage 1: Initial responses
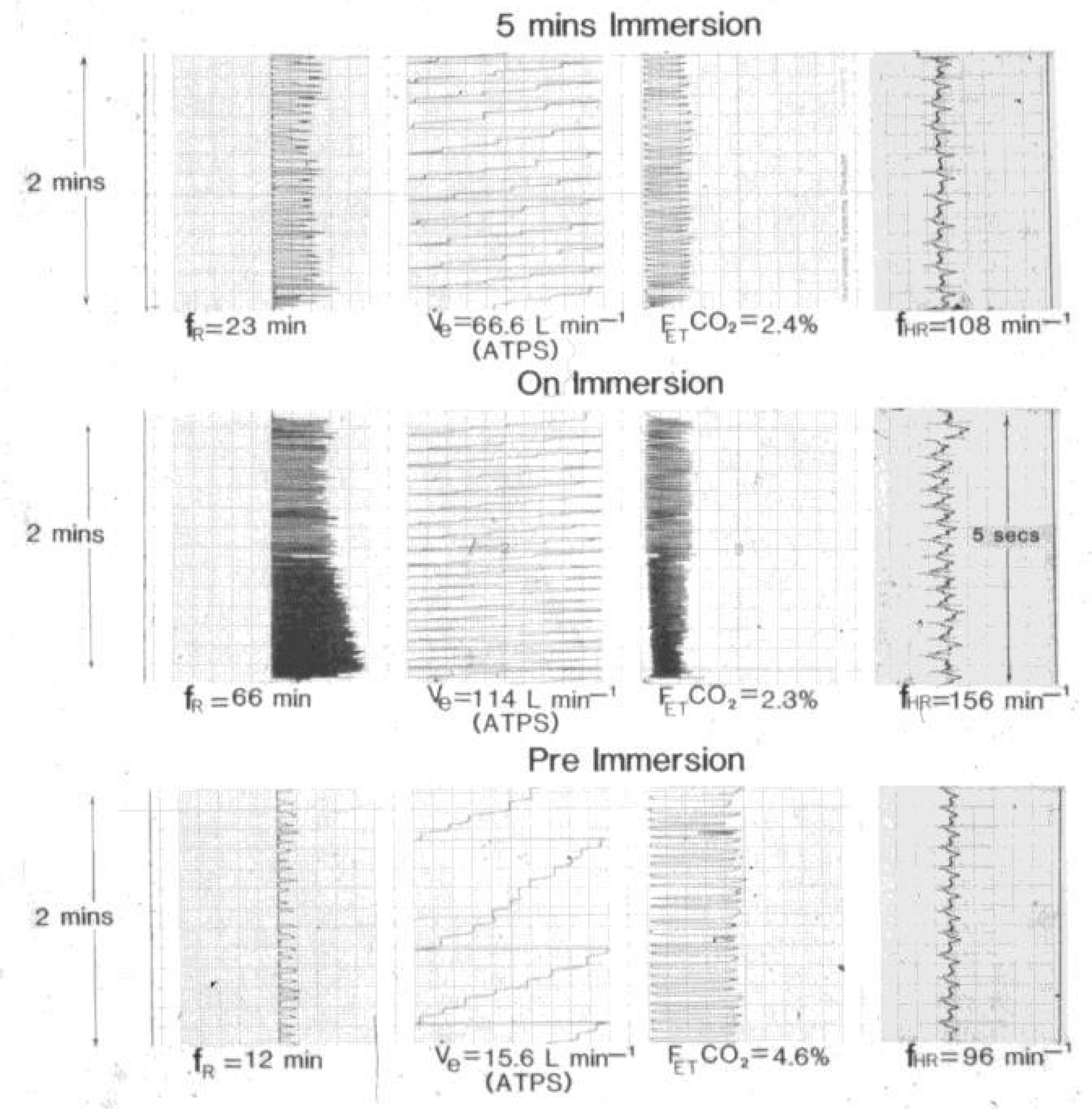
On CWI the first tissue to cool is the skin. This produces a set of responses we called “cold shock”; nothing to do with the medical definition of “shock”, but simply because sudden immersion in cold water is shocking. Slide 2 shows the physiological responses evoked by slowly immersing a young, fit healthy individual to the shoulders in 10°C water; the average temperature of open water around the UK is 10–12°C.
The cold shock response is evoked by the dynamic response of the cutaneous cold receptors. These receptors are about 0.18 mm below the surface of the skin, in a superficial subepidermal location, above the layer of subcutaneous fat (fat doesn’t protect against cold shock). The superficial location of the cold receptors means they are very responsive to changes in temperature, producing a “gasp” response of 2–3 L, uncontrollable hyperventilation, peripheral vasoconstriction, an increase in cardiac output, hypertension and an increase in the work demand placed on the heart. The gasp response evoked by CWI is probably the most dangerous of the responses seen on CWI because it prevents breath holding, so if it occurs when the airway is under water the prospect of drowning is significantly increased. Maximum breath-hold times of 45–60 s in air can fall to less than a second in cold water. 7
From Slide 2 you can see that the hyperventilation on immersion results in a minute ventilation (hyperventilation) of 114 L. To put this number into context, the lethal dose of salt water into the lung for drowning is about 1.5 L (about 3 L in fresh water) for a 75 kg adult. Often less water is aspirated during drowning. Thus, the gasp response at 2–3 L exceeds the lethal dose of aspiration for drowning.6,8 So, if you happen to have your head under water, or a wave breaks over your face on CWI, there is a good chance you will cross the lethal dose for drowning with your initial gasp.
Drowning is “the process of experiencing respiratory impairment from submersion in liquid” (“submersion” involves the airway going under the water, in “immersion” the airway is clear of the water). Drowning has three outcomes: death, morbidity, or no morbidity. Drowning to the point of cardio-respiratory arrest takes about two minutes.
8
The end-result of a drowning incident depends on the length of the anoxic period and the degree of secondary damage. The outcome of
Medico-legal cases involving drowning often seek information on the “experience” of drowning in terms of the time it takes, and the associated subjective sensations; this relates to the size of compensation claims. In response to a paucity of scientific papers in this area we published a review in the Medico-Legal Journal, 10 in which we examined the stages of drowning and the subjective reports of those who have drowned, but survived to recount their experience. The interest in this article (“most read” paper in the journal) suggests that it has provided information that is of use to the medico-legal community.
With regard to the experience of drowning, water going into the lung is reported to produce a “burning” sensation. Then, towards the end of the period of consciousness, people report a range of pleasurable experiences. Because drowning, in any type of water, is a form of suffocation, these late experiences in the drowning process are most likely related to changes in cognitive function caused by severe hypoxia. In our Medico-Legal Journal article, we quote Dr Frank Golden, who investigated many drowning incidents. He describes the process as: “a period of terror while struggling to breath hold, then feeling a tearing, burning sensation in the chest as water enters the airway, followed by a feeling of absolute calmness and tranquillity and a terminal period of stimulation of the CNS then CNS depression and unconsciousness.”
10
Struggle to keep the airway clear of the water. Initial submersion and breath holding. Aspiration of water. Unconsciousness. Cardio-respiratory arrest. Death – inability to revive.
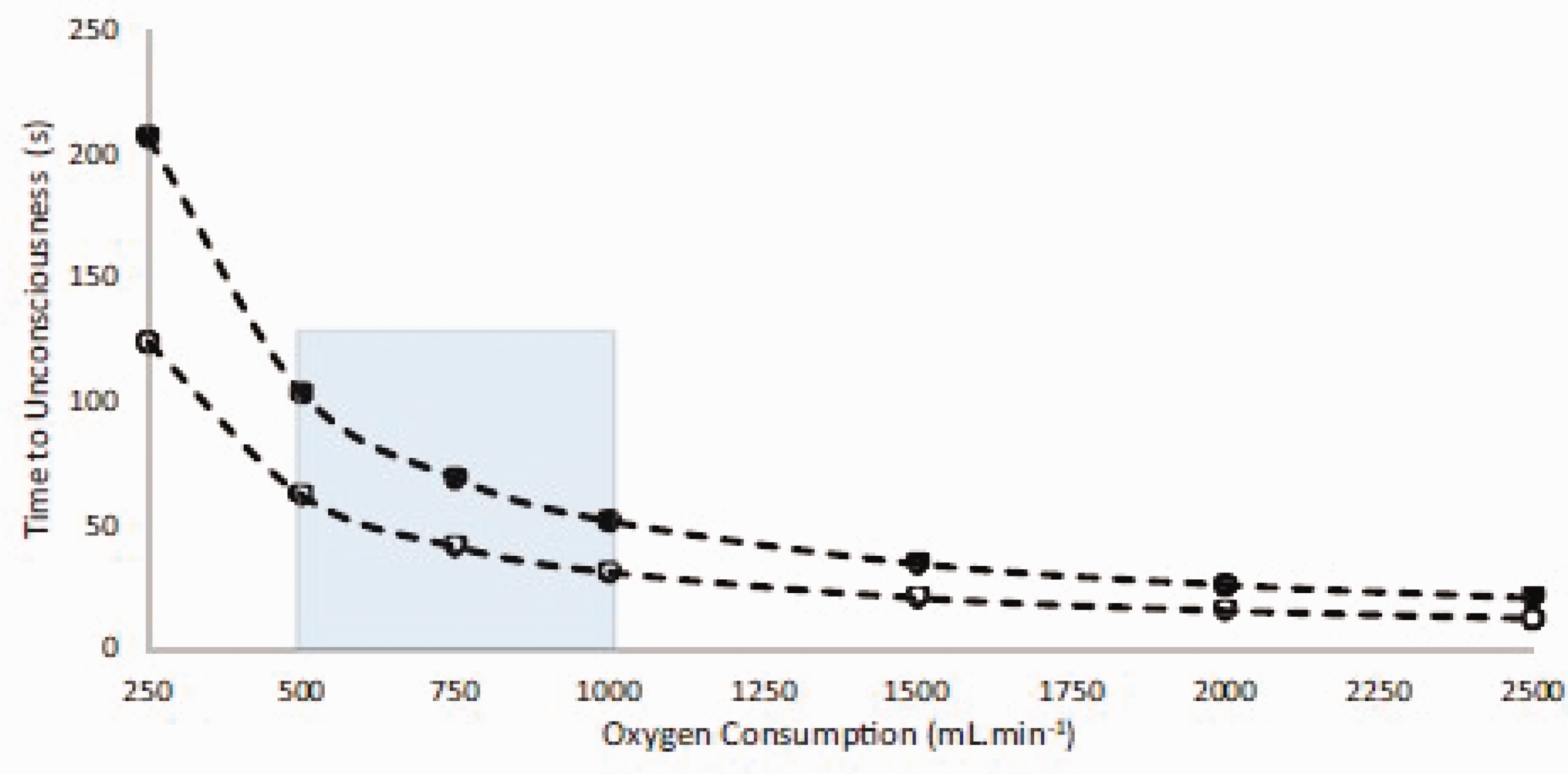
One question that comes up repeatedly in medico-legal cases is “how long does it take to become unconscious” during drowning? This depends on the oxygen available in the body when the airway is submerged, and the rate at which it is consumed when under the water. For an average individual, the oxygen available is a little under two litres, depending on lung volume and water aspiration, and the rate of oxygen consumption depends on the metabolic response when submerged, which itself depends on factors such as water temperature, clothing worn and effort expended trying to resurface (Slide 3).
When trying to address the global burden of drowning it is worth taking a holistic approach. That is, look at every link in the “drowning chain of survival”: 11 from education and information programmes in the community, to lifeguard fitness and function, to search and rescue, and out of hospital and in-hospital resuscitation. Some of us would argue that drowning is a process that starts with ignorance in the community about the dangers of water and how to mitigate them. For example, people often translate water temperature into air temperature, but 10°C water represents a very different stimulus and threat to 10°C air. The physical characteristics (conductivity, specific heat) of these two fluids are very different and produce different responses; air does not cool the skin fast enough to evoke cold shock. In water and air at the same cold temperature, people will cool about five times faster in water. Similarly, few people know about cold shock, rip currents and how tides can strand you, or what to do about these dangers.
Because it is driven by the dynamic response of the cold receptors, after a couple of minutes, the neurophysiological input that is producing cold shock adapts and breathing returns to conscious control. This is the neurophysiological correlate of “it’s okay once you’re in”. This can be seen in Slide 2 (upper block), where the responses are moderating after 5 minutes.
It follows that it is critical, in terms of avoiding drowning, to keep the airway clear of the water until breathing is back under control. Indeed, we use the information gained in the laboratory to help educate the general public not only about the dangers of CWI, but also how best to survive these threats: “From Lab to Lifesaving” (https://www.youtube.com/watch?v=6bLRr6OOhn0). In this context, Slide 2 has underpinned the Royal National Lifeboat Institution’s (RNLI) “Float to Live” campaign since its inception in 2014. From 2014 to 2017 the public were given information about cold shock (https://www.facebook.com/rnli/videos/10153870241583999/), it was then reported that about half of those who end up in the water had no intention of going in, so people needed to be told that the best thing to do during the first minute of immersion, when breathing is out of control, is to float: “fight your instincts and float to live” (https://www.youtube.com/watch?v=fgASxPh-xqU). So, we research to understand the basic physiology (https://www.port.ac.uk/news-events-and-blogs/news/lifesaving-float-to-live-campaign-launches-as-weather-warms), and then work with the RNLI and other talented people to produce public information films that we know, from unsolicited contacts with the RNLI, have saved lives in the UK and further afield as others follow this initiative (e.g. “Float to Survive” in Australia).
We are also lobbying to get this information and simple messaging on rips and tides onto the National Curriculum in the UK. As an island nation with thousands of miles of coastal and inland waterways, we have evidence 12 to suggest that a “Lesson for Life”, based on float first, what to do in a rip, and how to avoid getting cut off by the tide, will save many lives.
We named the “cold shock” response in the 1980s; during a head-out CWI it is this response that is evoked. During whole body submersion, including the face, the “diving response” can also be evoked by stimulation of receptors around the nose and mouth (ophthalmic division of the trigeminal nerve). This was first described by Paul Bert in 1870; 13 it includes a bradycardia, apnoea and selective vasoconstriction.
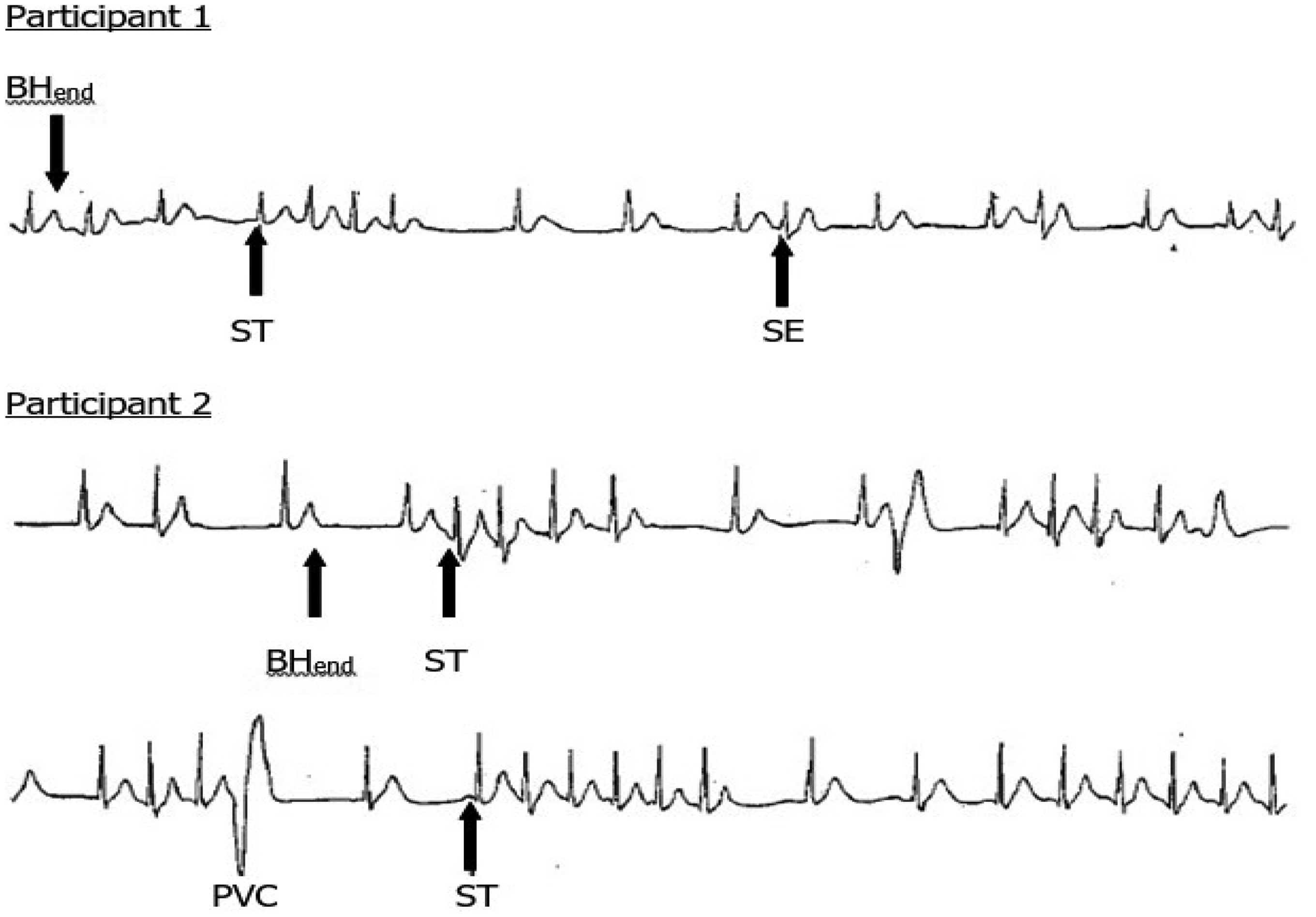
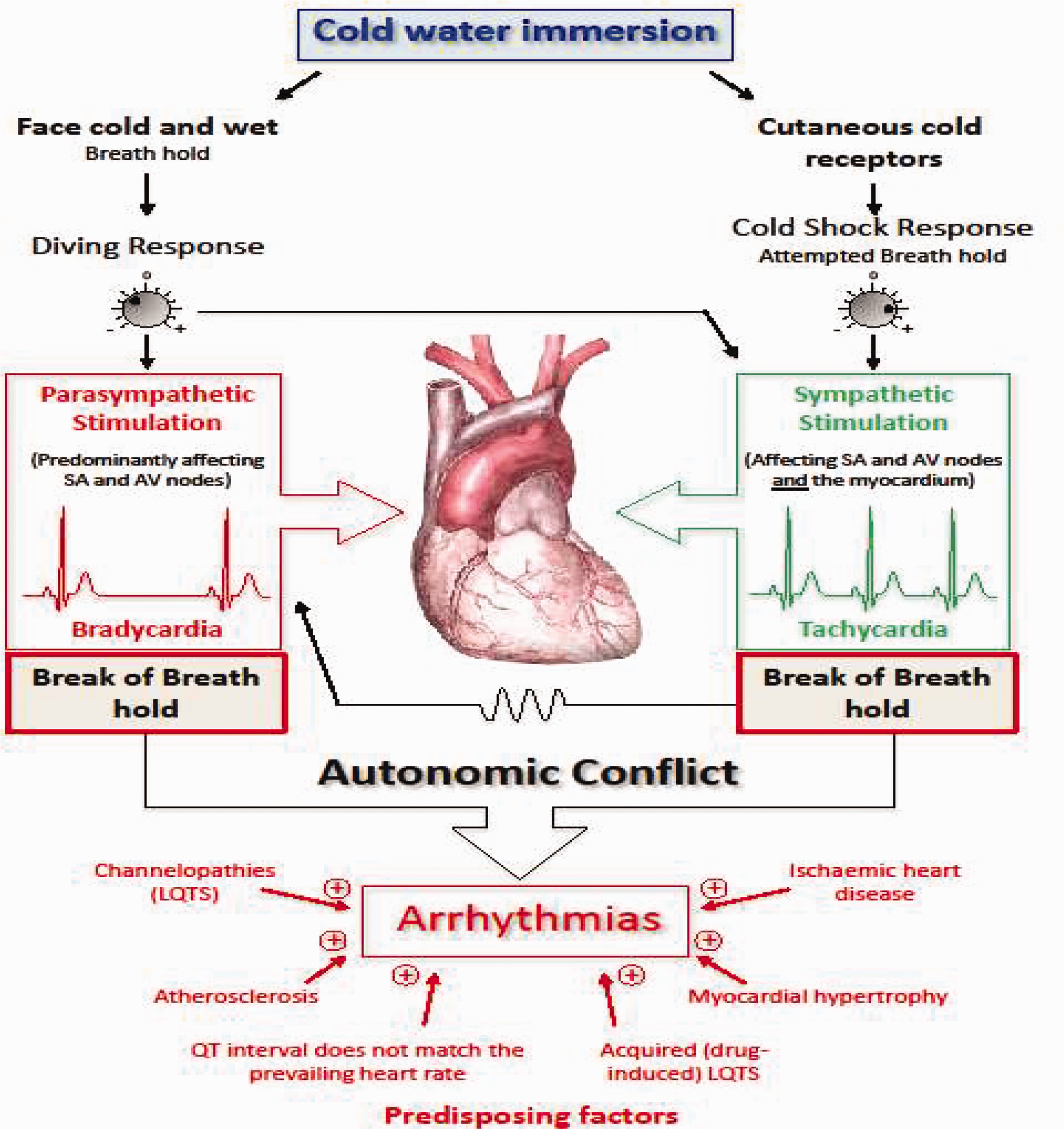
Various factors influence the relative strength of the cold shock and diving responses; these include: fitness, clothing worn, age, acclimatisation. In several ways these responses are opposed to each other, and when they are both evoked there is competition between them, with cold shock trying to increase heart rate (tachycardia) and the force of contraction via the sympathetic branch of the autonomic nervous system, and the diving response trying to slow it (bradycardia) and reduce the force of contraction via the parasympathetic branch of the autonomic nervous system. These coincidental competing inputs to the heart result in variations in cardiac rhythm, fluctuating between tachycardia and bradycardia. Where these rhythms switch, and particularly in the presence of the end of breath holding, arrythmias occur, normally supraventricular but occasionally ventricular. In the right circumstances, these arrythmia are common, even with young, fit and healthy participants. For example, the incidence of cardiac arrythmias increases from 1–3% during head out CWI, to 63% during head out CWI with maximum breath holding, to 82% during head in CWI with breath holding. 14 The arrythmias are reproducible and idiosyncratic in an individual (Slide 4).
Professor Mike Shattock from King’s College London and myself have called this response “autonomic conflict”, 16 because the arrythmias arise due to conflicting inputs to the heart from the two divisions of the autonomic nervous system. It is a very effective way of producing arrhythmias that then can descend into something more dangerous if an individual has any of a variety of predisposing factors (Slide 5). Amongst these is Long QT Syndrome, I mention this because there are a variety of commonly taken drugs that can lengthen the QT interval. 16
Just occasionally, an extraordinary case of survival is reported in which an individual, normally a child (67% of incidents) or small adult, survive an extended period of submersion under icy cold water. The current “record” being 66 minutes by a two-and-a-half-year-old in the US. These incidents are rare; in the review that we did, 17 there were 43 cases of prolonged survival underwater amongst thousands of lethal drowning cases. But our rescue services know that these extraordinary survivals can occur, and it is therefore important to give them some guidance.
We think the protective mechanism at work is rapid and selective brain cooling as a result of the flushing of cold water in and out of the lung during drowning, thereby cooling the heart and blood supply to the brain. Counter-intuitively, therefore, the hyperventilation of the cold shock response may actually be part of a protective mechanism in the special circumstance. With cooling comes protection as the hypoxic survival time of the brain is extended by hypothermia: cerebral activity, and therefore oxygen demand, fall close to minimum levels at a brain temperature of 22°C. For this protective mechanism to function, water temperature appears to have to be colder than 6°C. There is evidence from the work of Conn et al 18 to support this theory; they found reductions in carotid artery temperature of 7.5–8.5°C during the first two minutes of submersion before cardio-respiratory arrest. Much slower rates of cooling were seen after arrest when the lung could no longer act as a heat exchanger.
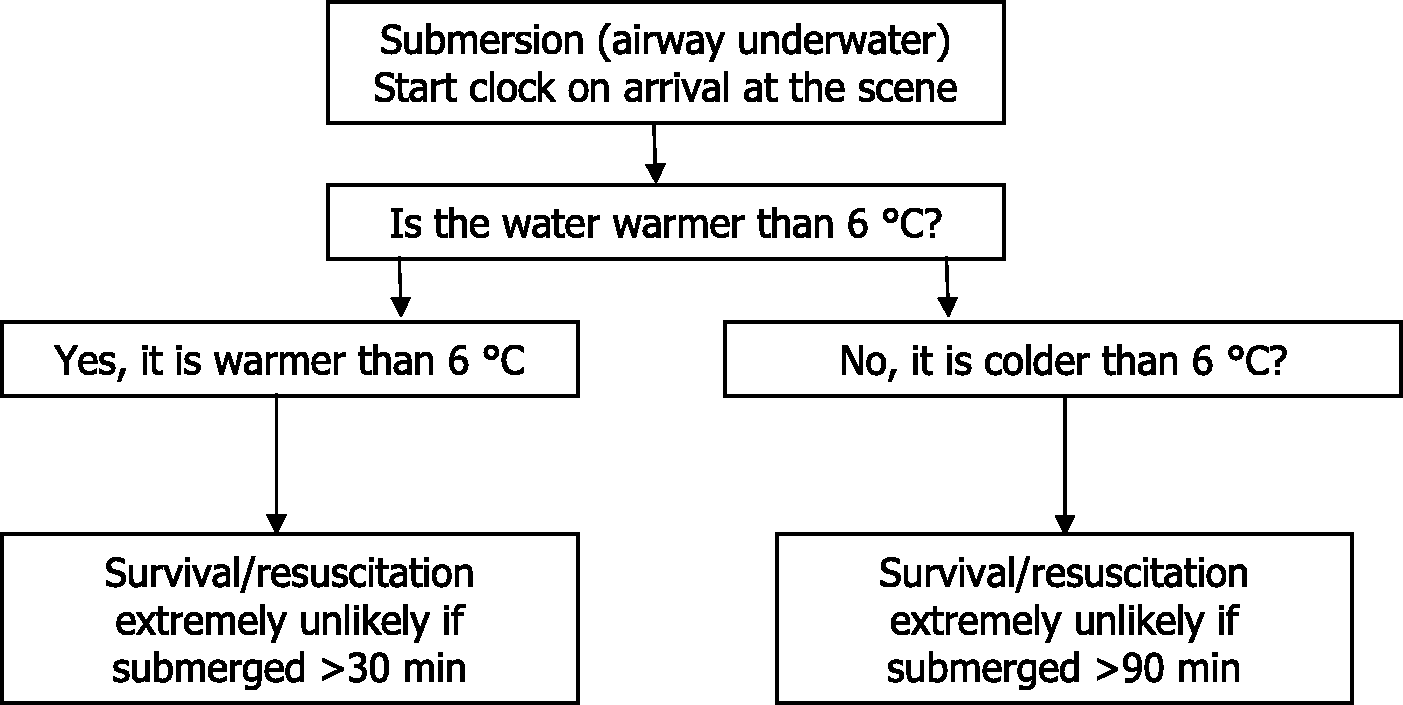
With this understanding we can provide advice (Slide 6) to rescue personnel. This is incorporated into the National Operational Guidance used by the rescue and ambulance services: another example of “lab to lifesaving” applied physiology.
Because the protective mechanism selectively cools the brain, any other measure of deep body temperature is of little prognostic value in this situation. Indeed, many problems in medico-legal cases arise because of the improper or inaccurate measurement of deep body temperature; it is incredibly difficult to obtain an accurate measurement of this temperature in a natural environment, even if you have a thermometer!
Stage 2: Short term CWI: superficial cooling
After the skin, the superficial tissues of the body are the next to be cooled. The arms are particularly susceptible to cooling, being long, thin cylinders with superficial nerves and muscles. It can take as little as 10 minutes in 5°C water to cool these nerves and muscles to about 27°C, the temperature where they cease to function, and loss of proprioceptive feedback and physical incapacitation occur. 19 This can result in swim failure, the inability to self-rescue and drowning. 10 It takes about 20 minutes to reach the same point in water at 12°C. This is why we recommend that the rapidly growing band of open cold water swimmers should not stay immersed for more than 10 minutes.
Once again, despite misconceptions, the problem in this stage is not due to hypothermia, but local cooling leading to incapacitation. 19
Stage 3: Long term CWI: hypothermia
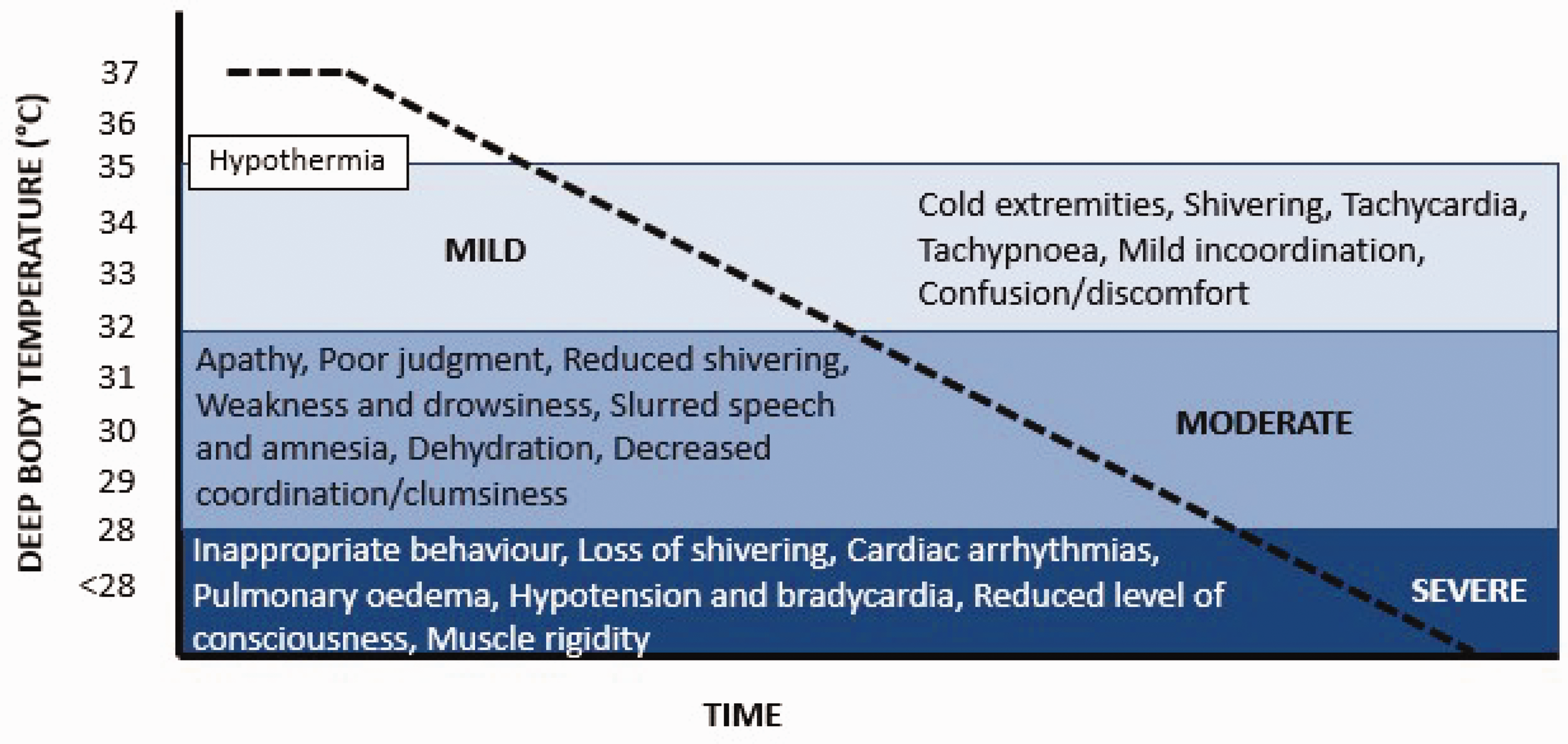
After at least 30 minutes, hypothermia can start to become a problem. The clinical signs and symptoms of hypothermia are presented in Slide 7.
The first major organ to be affected is the brain. Unconsciousness occurs at a deep body temperature of around 30°C; drowning occurs at this time if the casualty is not wearing a lifejacket to keep the airway clear of the water. 10 Hence, again, the cause of death is drowning not hypothermia per se.
There are no units of time on the X-axis of Slide 7 because the time to different states varies enormously in different situations and with different people. For example, the lowest deep body temperature from which a person with accidental hypothermia has been resuscitated with neurologically intact survival is 11.8°C (two-year-old boy). But, for the search and rescue community, an accurate prediction of survival time and consequent search time is critical to their operations. For prolonged CWI, this requires knowledge of both the lethal deep body temperature, and rate cooling to this temperature. Data for these estimations comes from actual events, laboratory studies and mathematical models based on these inputs. 22 However, large variations exist; for example, deep body temperatures ranging from 25–34°C have been regarded as “lethal”. This source of variation is compounded by a wide range of thermal and non-thermal factors that influence the rate of cooling in water (Table 2).
Some thermal and non-thermal factors influencing longer-term survival time in cold water.
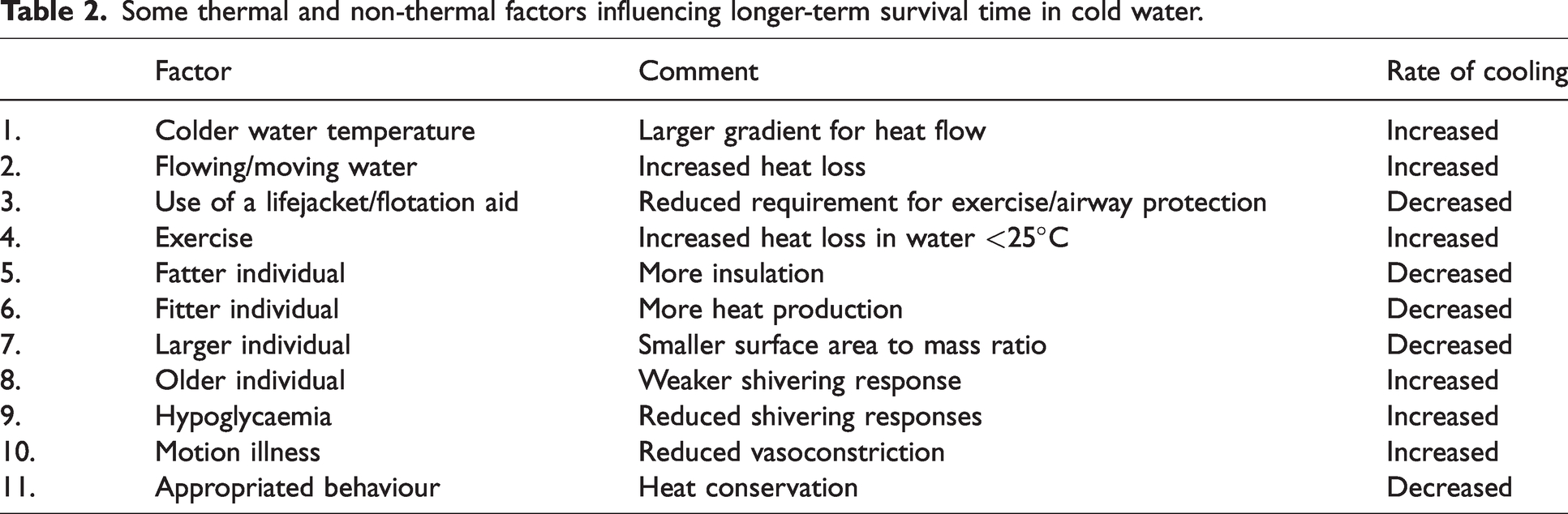
These factors explain why the prediction of survival time in cold water is difficult, and improved with increasing amounts of information about the casualty and an understanding of the physiology in operation. A case study will help emphasise this point and the complexity associated with determining accurate survival times in cold water.
Medico-legal case study
Five males were fishing, water temperature 10°C; sea state – choppy; wind – Force 3. The small vessel they were on board flooded and they were immersed. Sadly, there were three fatalities (younger individuals) and two survivors (older individuals). Why did the younger individuals die and the older survive; this is not what might be expected from Table 2 (Factor 8)? A second question was, would those who died and were found after 5 hours 15 minutes have been alive at 4 hours 25 minutes?
To address these questions accurately one must consider and understand the physiology underpinning the factors in Table 2. Although the survivors were older (Factor 8) they were found sooner, they were of large build (Factors 5 and 7) and had lashed themselves to the hull of the boat preventing them from having to exercise to keep their airways clear of the water (Factor 4). The younger individuals had a variety of factors working against them, including: ineffective flotation aids (Factor 3); the need to exercise (Factor 4); small individuals (Factor 7); motion illness prior to the accident (Factor 10); hunger prior to the accident (Factor 9).
The immersion time in 10°C water associated with “likely death”, from a wide range of sources, is estimated to be between 2.5 and 4 hours. 23 Given that all of the factors in this unfortunate incident were tending to reduce rather than extend survival time, it is likely that those that died did so before 4 hours and 25 minutes.
This incident is presented to help demonstrate the complexity involved in the estimation of survival time. We have helped develop decision-making aids for those having to determine search and rescue times internationally. One of these is the “Realistic Upper limit of Survival Graph” in The International Aeronautical and Maritime Search and Rescue (IAMSAR) Manual, jointly published by two United Nations agencies: International Civil Aviation Organization (ICAO) and the International Maritime Organization (IMO). 24 The graph guides all search and rescue activity of the 193 member States. In addition, we have collaborated with the US Army and US Coastguard to help them produce an advanced “Probability of Survival Decision Aid” which allows, in addition to water temperature, some of the factors in Table 2 to be included in the predictive model assisting the search and rescue coordinator. 22 We are currently working with the UK and US Coastguards to evaluate this aid for use in the UK.
Other medico-legal cases involving cold water immersion range from murder, through child abuse, to compensation claims against different groups for loss of life. For resolution, all require the application of an understanding of the physiological responses described above.
The benefits of voluntary cold water immersion
I know that we have some open cold water swimmers in the audience, and this is an increasingly popular pastime at the moment, so I thought I would finish with some comments on voluntary cold water immersion. The claimed benefits generally fall into three categories:
“Activation, feeling alert and ready for the day.” Immune function improvements. Improvements in conditions involving inflammation.
25
The “activation”, “feeling alive” responses associated with cold water immersion are related to the stress of the cold shock response, including the release of stress hormones.
The evidence for the benefits to immune and anti-inflammatory responses is mixed, and largely anecdotal at this time. We have reported a case study of the benefits of cold water immersion as a treatment for major depressive disorder. 26 We can propose potential mechanisms for these benefits, but they have not been rigorously tested and the “active ingredient” in the experience of cold water immersion (e.g. going somewhere nice, floating, hydrostatic squeeze, exercising, meeting friends, “defeating” cold, getting cold?) has not been isolated. To some extent this doesn’t matter for those claiming benefits from CWI, but if we can isolate the mechanisms underpinning any benefits, we may be able to evoke these in ways (e.g. partial immersion, cold pressor test) that avoid the risk of whole-body cold water immersion, or make them available to those who cannot undertake a full CWI.
Associated with the rapid increase in the numbers taking up CWI for therapeutic reasons has, inevitably, come an increase in the number of problems. In 2020, HM Coastguard recorded a 52% increase in incidents related to open water swimming and cold water dipping in the UK. In the same year swimming was responsible for 28% of accidental/natural coastal fatalities. The increase in those undertaking cold water immersion has also been associated with an increase in the incidence of previously relatively rare conditions such as swimming-induced pulmonary (o)edema (SIPE) and transient global amnesia (TGA).
SIPE is caused by cold vasoconstriction, hypervolaemia, restrictive wetsuits, intense exercise, and can be fatal. The symptoms include coughing, shortness of breath, chest pain/tightness and, occasionally, haemoptysis. These symptoms lessen after exiting the water and are normally gone within 48 hours. The risk factors are: hypertension, being female, swimming more than 1.2 miles (which we would not normally recommend), and a history of SIPE. Out of hospital treatment is to sit up and remove wetsuits, engage in pursed lips breathing and evacuate to medical care. At hospital, tell staff you think you might have SIPE because it is not that well recognised or understood.
TGA is, again, very rare, about one in 10,000, and is unpredictable. Major risk factors include a history of migraines and being an older man. Common triggers include CWI, other exciting experiences like big sporting occasions, and sex. TGA is short-lived, with episodes lasting eight to ten hours.
In an attempt to maximise the benefits of cold immersions and minimise the risks, we have published guidelines 27 for those wanting to undertake this activity. These include: get a medical check-up; swim with experienced people; wear a wet suit; enter the water slowly; avoid prolonged breath holds; stay in your depth; limit your immersion to a maximum of 10 minutes (2 minutes is probably sufficient), no matter how good you feel; float on your back if in difficulty; rewarm thoroughly on leaving the water and before driving. The guidelines also include suggestions for those providing an open water swimming “experience”, and those providing a medical assessment prior to participation. 27
I would like to finish by thanking and acknowledging my friends and colleagues from the Extreme Environments Laboratory, in the School of Health, Exercise & Science at the University of Portsmouth, for their support, friendship and hard work over the years.
Thank you for your attention.
Discussion
We were tasked with producing a system that was easy to use, would extend underwater survival time and would not introduce any additional dangers. This last requirement precluded the use of mini-scuba sets (due to the possibility of pulmonary barotrauma). Based on earlier work 28 on the determinants of maximum breath hold time, we knew that the reason you break your breath hold in air is the need for respiratory movement. In cold water, as you have heard, you break your breath hold due to cold shock, you then hyperventilate. It occurred to us that an empty plastic bag would allow you to capture the breath lost with the gasp response, and rebreathe that breath thereby extending underwater survival time. Studies followed to prove this concept and the award-winning helicopter underwater emergency breathing aid “Air Pocket” was born and included in the personal protective equipment provided for those flying offshore in the oil industry. 29
“I represented a mother at an inquest. She and her family had been on a boating trip abroad with another family. The boat overturned and the families did not know that it was equipped with lifejackets. I have never forgotten her harrowing evidence as she described how her family died one by one but she survived until rescuers found them the next day. I think the family survived because they got on top of the boat. What struck me was the length of time the family including small children survived and how the order in which they died was not that which I would have predicted. In those circumstances, how important is the will to survive? What other relevant survival factors are there between individuals with seemingly the same susceptibility?”
The other thing that we know is that the condition of a significant number of people deteriorates just before being rescued, they can even die at this point. The number of people this happens to is beyond coincidence. The casualties have not been touched, all that has happened is that help has arrived. This has been reported in immersion and avalanche survival cases, and it is really devastating for search and rescue communities. We cannot research this in the laboratory, but we think it is the wave of relief that comes over people as they realise salvation is at hand. It may be represented physiologically by an alteration in the balance of the autonomic nervous system (a little like autonomic conflict). It can be made worse by rescuers saying things like, “Relax, we’ve got you, you’re safe.” So, we recommend that rescuers say, “We are here to help but keep fighting for your survival.”
Habituate the cold shock response: as few as six, three minute CWIs can halve the response, and it is still reduced by 25% 14 months later.
30
The habituation occurs more centrally than the cutaneous cold receptors (you can habituate one side of the body and get a reduced cold shock response from the other, unexposed side).
31
But, note, it is not possible to adapt to the incapacitation caused by cooling of peripheral tissues (Stage 2 above). Be a large person with a combination of fatness, muscle mass and fitness. Be a strong swimmer and fast enough to be able to swim one kilometre in less than 30 minutes.
Lewis Pugh has all of these attributes and can therefore achieve great things for important causes.
The cold shock response evoked by slow (0.8 m.s−1), seated immersion to the shoulders into water at 10°C (reproduced with permission
6
). The time to unconsciousness during drowning depending on lung volume and metabolic rate (oxygen consumption – blue region). Estimations based on a 70 kg human with a lung capacity of 5.5 L at one atmosphere. The maximum volume of oxygen available is set at 1724 mL, loss of consciousness assumed when 50% of available oxygen has been used. Solid circles = all air in lung available. Open circles = no air in lung available.
10
ECG of two individuals during submersion (head under) wearing an immersion dry suit. BHend = end of breath holding; ST = supraventricular tachycardia; SE = supraventricular extrasystoles; PVC = premature ventricular complex (adapted from Tipton et al
15
). Autonomic conflict (reproduced with permission).
16
Recommendation for the search and rescue of submerged (airway underwater) casualties (adapted from Tipton et al.
17
).