
Abstract
A suicide where the deceased has employed more than one means of ending his or her life is defined as a complex suicide (CS). Forensic practitioners may face difficulties caused by the articulated mechanisms underlying this event. Among CS, the combination of hanging and gunshots is unusual. In this study, we present three unique cases of such planned complex suicides (PCS) that we have encountered in our 28 years of activity at the Bureau of Legal Medicine of Milan. Careful inspection of the death scene, precise analysis of the anamnestic-circumstantial data, and accurate medico-legal autopsy examination were the starting points for a better understanding of the causes and manner of death. In particular, the presence of vital reactions of tissues involved in the two different means used, the coherence of the areas involved with a self-inflicted wound, and the absence of signs of third party intervention allowed us to classify these events as suicides. As for the chronology of events, the lethality of the cerebral lesions caused by the gunshots in all cases, in accordance with the cervical lesions caused by hanging, led us to conclude that we were dealing with PCS and catalogue these three cases as unusually planned complex suicides avoiding incorrect and superficial classification.
Introduction
In contrast to simple suicides where death results from a single means usually characterised by “success” at first attempt, complex suicides (CS) are rare, self-suppressive forms. They involve more than one means; 1 in literature, up to six different modalities have been described. 2 Combining more than one method is aimed at achieving death with certainty, 3 avoiding a failure from any one chosen method. 4 A CS can occur with a series of more frequent methods of causing harm,3,5,6 with more unusual combinations,7 –14 or even with exceptional ones.4,7,15 –18 In particular, the combination of hanging and gunshot is considered particularly rare4,19 with only a few such cases reported. In these cases, hanging resulting in mechanical asphyxia was followed by gunshot using different weapons, such as a black powder derringer and, in one case, a manipulated bullet, 6 a captive bolt gun, 20 a muzzle-loading pistol, 21 and a pen gun. 22 There is only one case reported in the literature where a man who shot himself twice (to the chest and abdomen) subsequently hanged himself in the upper floor of his home. 23 This led to serious interpretation difficulties of the sequence of events. We present three cases of CS combining hanging and gunshot within a period of 28 years of forensic activity (1993–2020). We describe the characteristics and discuss the peculiar medico-legal aspects, with a brief review of the literature.
Case series
We retrospectively evaluated the records of 26,055 autopsy examinations assessed at the Bureau of Legal Medicine of Milan over a period of 28 years (1993–2020) and extrapolated all suicides. From these cases, we isolated all the complex suicides, and from these, all those that involved mechanical asphyxia by hanging and gunshot. From a total amount of 4,596 suicides, 55 CS were highlighted (1.19%; 0.2% of all autopsies). Only three (5.45% of all CS) showed an association between hanging and gunshots.
Case 1
A 66-year-old man with major depressive disorder was found hanging from a tree by a belt with a gunshot wound to the head. At his feet, on the ground, a wooden case was found. Beside it, not far from the crate, was a semi-automatic Smith & Wesson gun. External examination of the body did not highlight defence-type wounds that suggested another person had participated in causing the death. Exsiccated blood stains were observed on the right hand of the victim; at the right temporal-parietal region, a circular wound with introflexed borders and a blackish ring was documented; in the left parietal area, another X-shaped wound with irregular, everted, blood-infiltrated borders was observed. At the neck, in the supralaryngeal area, there was a bruised furrow with an intact region of approximately 1.5 cm (Figure 1A, 1B).
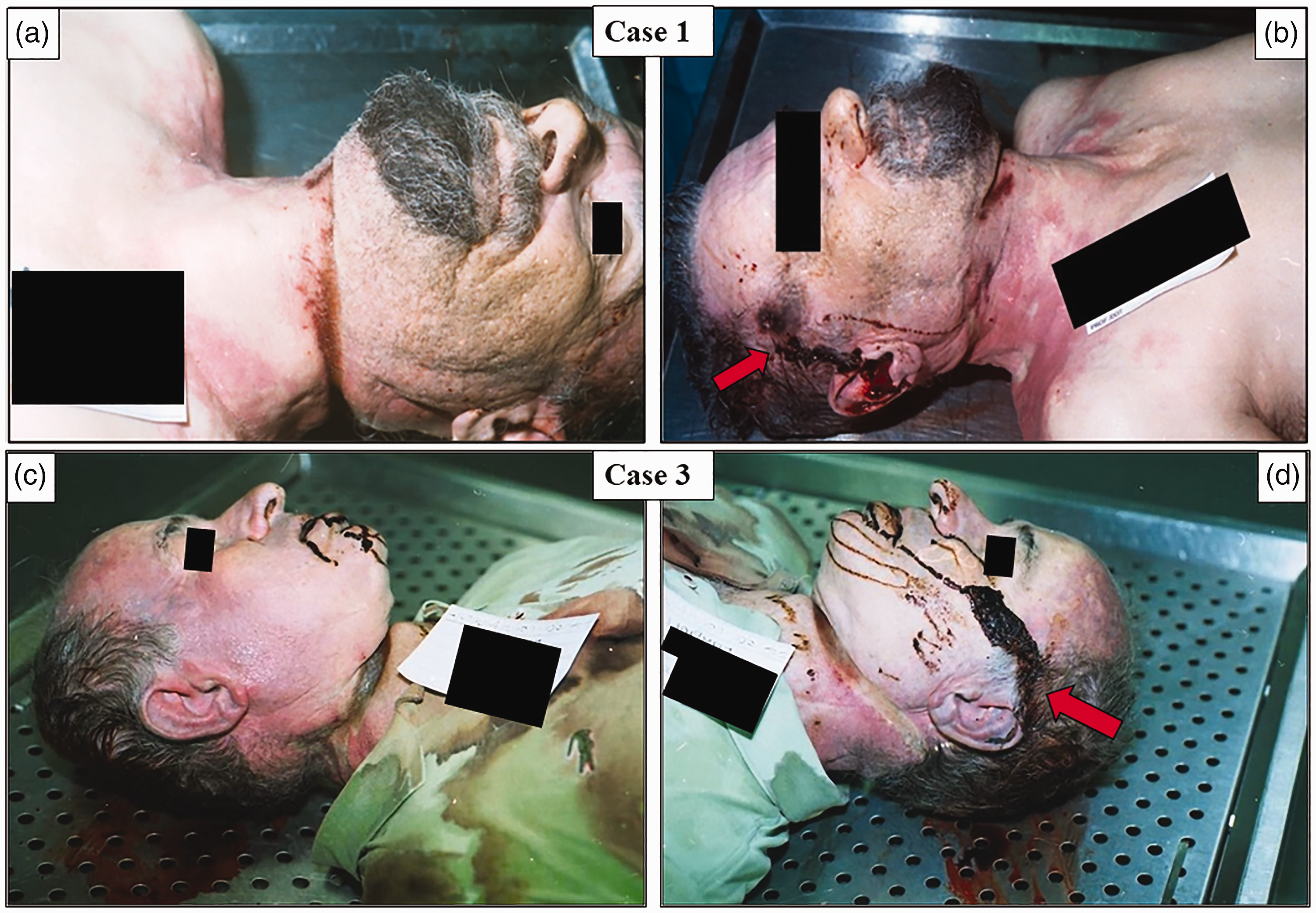
Macroscopic overview of the coexistent effects of hanging (a and c) and gunshot wounds (b and d) in cases 1 and 3.
Upon dissection, the vault and base of the cranium were observed to have several fractures and a disintegrated-haemorrhagic pattern. A diastatic fracture (C6–C7) with haematic infiltration was documented, in addition to a fracture of the thyroid cartilage with periwound haemorrhage. Subpleural petechiae, pulmonary oedema, and acute haematic stasis were observed in both lungs.
Case 2
A 74-year-old man with silicosis and oral neoplasia was discovered hanging from a rope in his vegetable garden with a gunshot wound in the head. The man suffered from generalised anxiety disorder and had indicated suicidal intentions previously. The rope was 4 m long, made of cotton and nylon, and secured with several coils to the branches of a tree, to some posts, and finally to the ground. At the victim's feet on the ground, there was a flipped stool and a semi-automatic Smith & Wesson. External examination revealed no defence-type wounds that might have been caused by a third party. Dried blood stains were observed on the right hand, as well as bilateral palpebral ecchymosis (spectacle-like). A circular skin wound with a blackish ring was observed at the right temporal-parietal region of the head. An ecchymotic-excoriated furrow was observed, with maximum width and depth (10 mm × 4 mm) in the right para-median supralaryngeal region, but which was barely visible in the nape. Upon dissection, the base of the cranium at the area of the anterior fossa showed several blood-infiltrated fractures. Bilateral fractures of the great horns of the hyoid bone and the superior horns of the thyroid cartilage with periwound haematic infiltration were detected. In the lungs, petechiae, pulmonary oedema, and acute haematic stasis were present.
Case 3
A 60-year-old man with major depressive disorder who was undergoing specific therapy was found hanging from the ceiling of his art conservator laboratory by means of a synthetic rope. He had a gunshot wound to the head. By his feet, on the floor, there was a flipped chair and a semi-automatic Beretta gun. External examination of the corpse revealed no defence-type wounds. On the right hand, several dry blood spots were observed; a gunshot wound with an ecchymotic-excoriated concentric ring was found in the right temporal area. An ecchymotic-excoriated furrow was observed at the supralaryngeal area, with the maximum depth in the left para-median area (Figure 1C, 1D). An interruption of the furrow was observed at the mastoid area of the right temporal bone, identifying the hanging point. Internal examination revealed a full metal jacket bullet in the left sub-epicranial aponeurosis. The calvarium and skull base showed several fractures, and some bone fragments were completely detached. Moreover, an extensive encephalic haemorrhage involving the entire ventricular system, a ventral pons haemorrhage, and cerebral oedema were also present. In the neck, a fracture of the thyroid shield and peri-lesion haemorrhage were observed, in addition to subpleural petechiae and acute haematic stasis.
Conclusive epicrisis
The cause of death in these three determined as suicide performed by complex means, resulting in cranial-encephalic lesions caused by gunshot and mechanical asphyxia from hanging.
Discussion
Complex suicides in forensic autopsies are rare with an occurrence of between 1.5 and 5.6% when compared to all suicides. 7 These events usually involve several body areas and have been known to forensic practitioners since 1974, when this classification was first created. 24 The literature differentiates between “primary events”, when the detrimental means are applied simultaneously, and “secondary events”, when the killing methods are applied in rapid chronological sequence. 7 The literature differentiates between “planned” and “expected or programmed” events when considering the perpetrator's intent. It depends on whether the chosen or actual means were established or were “unplanned” for cases in which the first method fails or is particularly painful, or is extremely slow in causing death, compelling the victim to use an additional improvised method.1,3,7,22 This latter case, however, requires a state of consciousness sufficient to commit such additional means of causing death that is within reach (Figure 2). 14
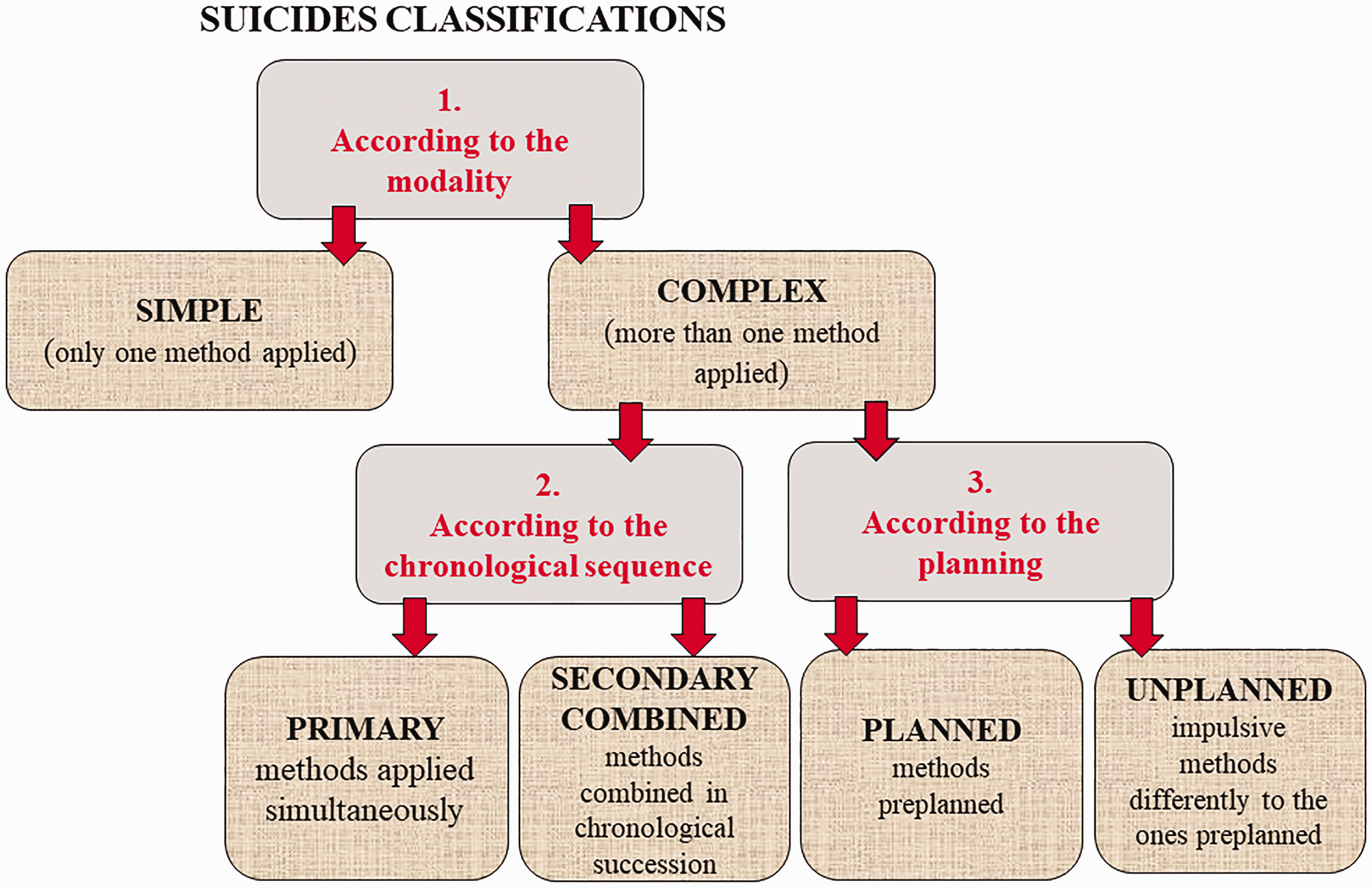
The recapitulatory schematization of suicides classification.
A third, very rare type of suicide, defined as “complicated”, 25 involves cases where the first method chosen by the victim fails to achieve its purpose, and death is caused by a secondary accidental trauma not foreseen by the victim. 26
CS in which victims decide to commit suicide by both hanging and gunshot is rare;4,22,23 as shown by our retrospective analysis of all the autopsy examinations performed over a period of 28 years, finding only three cases. Victims, all males between 61 and 74 years of age, were diagnosed with psychiatric diseases, and major depressive disorder in two cases (cases 1 and 3) and generalised anxiety disorder associated with end-stage cancer in another (case 2). This finding is in accordance with statements in the literature: psychiatric disorders are frequently documented in people committing suicide by complex means who are also often burdened by family, economic, or health problems. 26 Events occurred in external environments in two cases (cases 1 and 2); in the other (case 3) the event took place at home in a secluded room used as a laboratory.
External and internal examination of the corpses highlighted coherent lesions between what was observed on the bodies and the methods chosen by the victims (hanging and gunshot). The selection of two means was interpreted to avoid possible failure of achieving suicide, indicating determination to end their lives.
At the scene, all the tools necessary to perform the suicides were present. All the victims were equipped with adequate means to completely hang the body from the ground (crate, stool, chair) and something from which they could hang themselves (trouser belt, cotton and nylon rope, synthetic rope). By the victims’ feet, a legally-owned firearm was found in all cases: a Smith and Wesson handgun in two cases and a Beretta in one case. These guns fired just one bullet each; the gunshot wound was situated at either the right temporal-parietal area (cases 1 and 2) or the temporal bone area (case 3), a region that is highly lethal and particularly vulnerable, and as literature shows is frequently chosen in suicide events. 27
The lesions reported on the corpses demonstrated the involvement of two different but coexistent means (hanging and gunshot). In particular, all cases showed an excoriated or ecchymotic-excoriated furrow in the supralaryngeal area with fractures of the great horns of the hyoid bone and the thyroid cartilage, related to asphyxia. All the lesions had perilesional haemorrhage, proving that circulation was still active at the time death occurred. No haematic infiltration was reported in the airways in any case, consistent with the ligature around the neck that prevented aspiration of blood. In one case (case 1), a medial-distal cervical fracture was documented, a finding that has been observed in complete suspension hangings. In fact, these events, in extreme conditions, may end in complete or incomplete 25 decapitation of the subject, depending on the kinetic energy of the falling body, the endurance of the neck tissues, the diameter of the rope, and the elasticity of the detrimental means chosen by the victim. 28
The gunshot wounds, lesions situated at the entrance of the bullet, showed introflexed fringed borders with all the characteristics of a contact gunshot; internal bullet pathways led to the left temporal region (case 1), to the anterior cranial fossa (case 2), and to a blind ending with the bullet still in the body, just before the left sub-epicranial aponeurosis (case 3). These wounds were characterised by massive destruction, areas of haemorrhage, and comminuted fractures of the base of the skull. The two exit wounds had irregular and extroverted borders. In these cases, massive and diffuse haematic extravasation (cases 1 and 2), as well as ventricular haemorrhage associated with a ventral pons haemorrhage (case 3), proved the fatality of the lesions. Additional relevant data fundamental for the reconstruction of the events were the locations of the self-inflicted lesions which were all in areas easily reached by the victims. In particular, the victims’ right hands showed dried blood spots, a finding that was assessed as indicating the proximity of the hands to the entrance of the bullet. The lack of signs of potential interventions by other people on the bodies was also evaluated. There were no defence-type lesions, restraint marks, or fighting signs, which excluded the possibility of a homicide presented as suicide. 22 We believe that the timing was as follows: the victims first knotted the nooses around their necks and then shot themselves; the falling body allowed them to provoke mechanical asphyxia by hanging.
Examination of the corpses determined that the cause of death was cranial-encephalic lesions due to gunshot, associated with mechanical asphyxia due to hanging. Firearm wounds are considered immediately lethal, while asphyxia usually takes longer.
These three cases should be considered of great interest to the forensic scientific community. Careful observation of the scenes of the event, the circumstantial-anamnestic data collected, and the complete medico-legal autopsies on the bodies were the pivotal elements that enabled us to determine the cause and manner of death, the chronological order of the events, and the means chosen by the victims. The high lethality of gunshots to the head, in addition to the cervical lesions caused by hanging, led us to classify these as planned complex suicides, excluding the hypothesis of unplanned complex suicides and avoiding a more superficial classification.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.