
Abstract
Following a mass fatality incident, the assessment of survivability and preventability is essential, yet current methodologies remain inconsistent both within the UK and internationally. The 2024 UK Home Office report ‘The Patronising Disposition of Unaccountable Power: Independent Review of Forensic Pathology’ evaluated learning from the Hillsborough disaster and the Manchester Arena bombing inquests, highlighting the urgent need for clearer, standardised processes in determining survivability and preventability. This paper critically reviews existing techniques in use to address the question of survivability and preventability and makes recommendations for a national best practice framework to improve this process for future inquiries.
Introduction
The ability to review deaths form a significant part of any branch of medicine seeking to learn and improve. 1 For in-hospital deaths, reviewers can consider a plethora of data, however, for patients who die prior to reaching hospital, the absence of this data makes the review of deaths challenging.
Prehospital services within the UK commonly review prehospital deaths via the traditional case review process, in addition to Clinicopathological Correlation (CPC), 2 a process developed by the authors in response to the National Confidential Enquiry into Patient Outcome and Death report, ‘The Coroner's Autopsy: Do We Deserve Better?’. 3 The CPC meetings bring together forensic pathologists and experienced prehospital clinicians to discuss and debate the cause of prehospital deaths alongside potential opportunities for learning and improvement in care. 2
Despite these advancements, the assessment of an ‘isolated’ prehospital death following injury remains challenging. 4 This difficulty is amplified in mass-fatality incidents, due to complex injury patterns, limited documentation for each patient, and data sharing difficulties between clinical and non-clinical organisations. However, the review of prehospital deaths within a mass-fatality incident is crucial; not only from a legal and medicolegal perspective but also as part of the inquiry and as an important stage in the deceased's loved ones’ healing process. A question commonly asked during this process is ‘was this death preventable?’.
Preventability and survivability assessments
The question of preventability and survivability is increasingly considered internationally as part of the inquiry or inquest into mass fatality incidents. However, there is significant international variation in how this question is addressed, with no universal guidelines or best practices available. A systematic review collating 27 civilian and military studies (incorporating data from Europe, Asia, Canada, Australasia and the USA) found 11 distinct approaches to survivability/preventability assessments with inconsistent terminology; where the terms ‘survivability’, ‘preventability’ and ‘avoidability’ were used in 15 different combinations, and often synonymously. 4
The commonest approach, and the one recommended by the World Health Organisation's (WHO) ‘Guidelines for Trauma Quality Improvement Programme’, 5 was the use of a multidisciplinary panel to reach a majority consensus on whether the death was preventable, potentially preventable or not preventable. To achieve this, many studies utilise a two-phase approach consisting of a survivability assessment and a preventability assessment. 6
The first phase presents post-mortem data to the panel, who consider the question ‘under optimal conditions, has this pattern of injury ever led to a survivor’? If, despite optimal conditions, a patient has never survived their specific injury pattern, then the death is classified as ‘non-preventable’. Some studies rapidly screened patients using a pre-determined list of non-survivable injuries, whereas others sought consensus panel agreement or a combination of both approaches. 7
If the pattern of injury has previously led to a survivor, the death is then reviewed in the second phase, the preventability assessment. The preventability assessment considers the injuries sustained in addition to the individual patient's co-morbidities, age and frailty alongside scene factors (e.g. location/accessibility), available resources and pre-hospital interventions offered. As part of this phase, the question is then asked, ‘What could have been done for this patient to survive?’ Patients are then classified as ‘preventable’ or ‘potentially-preventable’, based upon majority consensus.
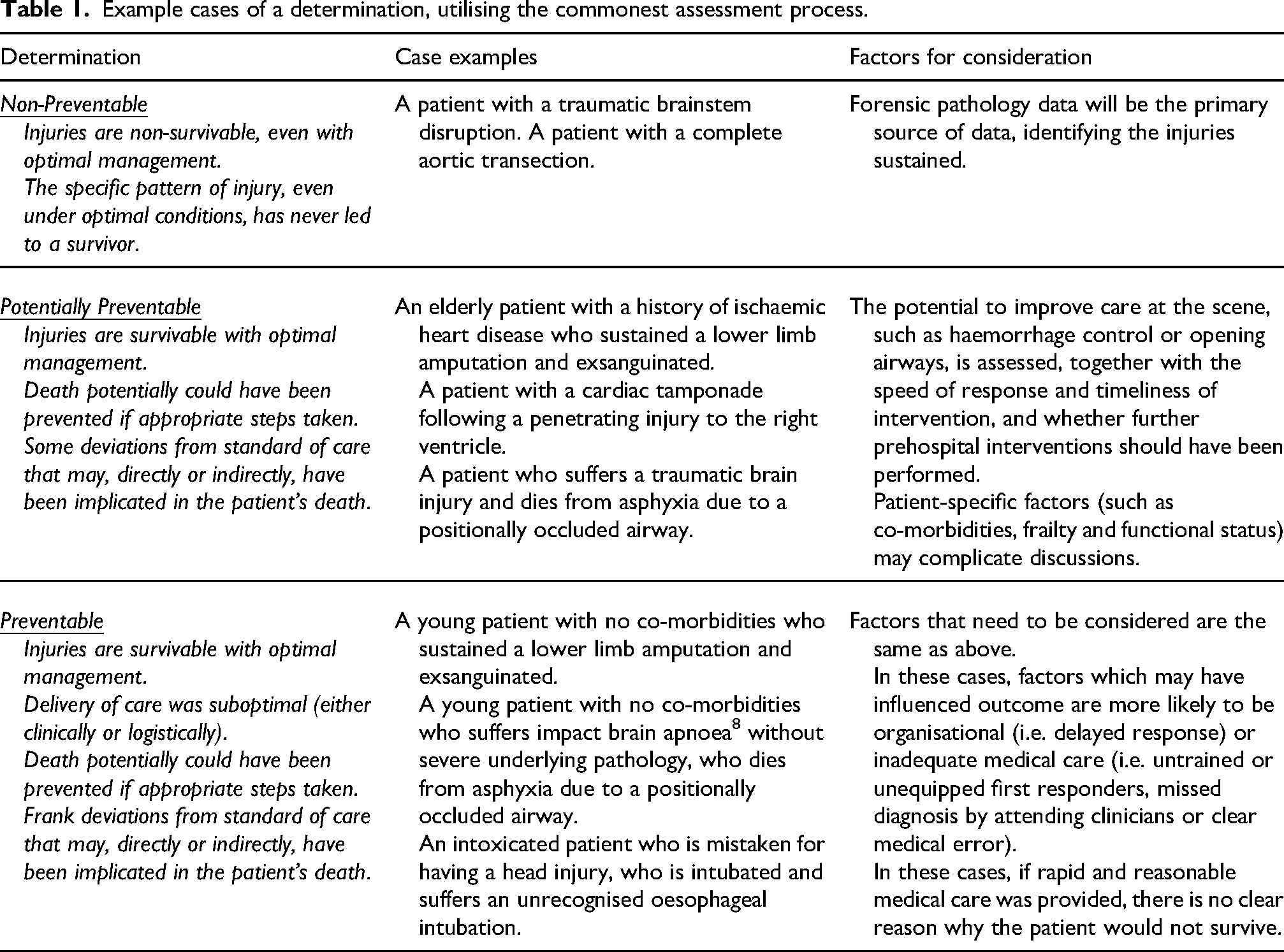
The potential outcomes of this process are illustrated in Table 1.
Example cases of a determination, utilising the commonest assessment process.
England’s experience
The review of prehospital deaths in mass fatality incidents has been necessary within the inquests of recent English events (Box 1).
The Hillsborough Stadium Disaster Inquests
36
(Initial inquest 1991, independent inquest 2012 and new inquests 2016)
Coroner's Inquests into the London Bombings of 7 July 2005
9
(2011)
Inquests arising from the deaths in the Westminster Terror Attack of 22 March 2017
37
(2018)
Inquests arising from the deaths in the London Bridge and Borough Market Terror Attack of 3 June 2017
38
(2019)
Inquests arising from the deaths in the Fishmonger's Hall terror attack of 29 November 2019
39
(2021)
The Manchester Arena Inquiry (Manchester Arena Bombing of 22 May 2017)
10
(2022)
Whilst survivability and preventability were considered at each inquest, addressing this question has become more pertinent in recent years. Following the July 7th London bombings in 2005, invasive post-mortem examinations were not conducted, with deaths recorded as ‘injuries consistent with explosion’. This limited understanding of internal injuries prevented meaningful assessment of survivability or preventability and restricted the ability to learn lessons from the emergency response. The inquest addressed survivability only superficially, concluding that ‘on the balance of probabilities each of the deceased would have died whatever time the emergency services had reached and rescued them’. 9 In contrast, the Manchester Arena Inquiry used modern forensic techniques to assess survivability on an individual basis, allowing better clarity of each patient's individual injury burden and thus potential interventions. Furthermore, the question of survivability was addressed by multidisciplinary expert panels and discussed in detail. 10
In the Manchester Arena Inquiry, a determination of ‘unsurvivable’ was offered for twenty of the twenty-two who died and ‘survivable’ for one of the cases. In one case, a narrative was offered in relation to potential survivability, where the Hon Sir John Saunders stated ‘it is highly unlikely that she could have survived her injuries. There was only a remote possibility that she could have survived with different treatment and care’. 10 For the latter two cases, a narrative specified what could or should have been done to alter the outcome.
It is worth noting that the terminology used within these inquests (survivable) is inconsistent with the commonest nomenclature used internationally, and the terminology recommended by the WHO (preventable). It is not clear why the term ‘survivable’ was used, rather than ‘preventable’.
In September 2024, the independent review ‘The Patronising Disposition of Unaccountable Power: Independent Review of Forensic Pathology’ was published. This report was commissioned by the Home Office in response to the Hillsborough inquests, but was also able to incorporate experiences relating to the Manchester Arena bombing. 11 It sought to explore the family's perspective of the inquest process, but also ways to improve the process. The review identified six key actionable areas, including clearer processes in addressing survivability/preventability, and the need to include families throughout.
These key action areas, in combination with the inconsistent approaches between inquests (both within the UK and internationally), highlight the urgent need for a national best practice framework to be established. However, to achieve this, several current gaps need to be urgently discussed, which have not been defined within the international literature, such as:
Is the multidisciplinary panel the best methodology to review deaths? Which professionals need to be involved in this process? What nomenclature should be used? What is meant by survivable? What data should be reviewed? What should the burden of proof be for determinations? What logistical challenges should be planned for?
Current gap: is the multidisciplinary panel the best methodology to review deaths?
The commonest approach to reviewing deaths following mass fatality incidents is the use of a multidisciplinary panel. 4 Panels review post-mortem findings alongside available clinical data, including the patient's presentation, observations, interventions and the patient's response to these. A consensus determination of survivability/preventability is then reached, either through discussion or blind voting. 4 Although widely used, alternative methodologies warrant consideration, including Injury Severity Scoring (ISS) and probability of survival (Ps) calculations.
Injury Severity Scoring-based approaches are well described within the literature, with thresholds defined for preventable, potentially preventable and non-preventable deaths (or other determinations). Several authors classify deaths with an ISS < 24 as preventable, 25–49 as potentially preventable and >49 as non-preventable.12–17 However, thresholds vary. For example, Ashour et al. (Australia) defined unsurvivable deaths as ISS > 50, with an ISS < 50 considered preventable. 18
Probability of survival-based approaches similarly vary. Ryan et al. (Australia) used Bull's Probit (incorporating ISS and age), defining Ps 25–50% as potentially preventable and Ps > 50% as preventable. 19 In contrast, Motomura et al. (Japan) defined Ps > 50% as preventable and Ps < 50% as non-preventable.20. McDermott et al. (Australia) classified Ps < 25% as non-preventable, 25–75% as potentially preventable and >75% as preventable.21–24
Whilst quantitative scoring offers consistency and reproducibility, it has intrinsic limitations, including underscoring multiple injuries within the same body region 25 and reliance on outdated injury classifications that do not reflect modern medical capability. 26 Quantitative methods also fail to account for the complexity of prehospital environments, particularly in mass fatality incidents.
This viewpoint is supported by UK case law, where Clerk & Lindell on Torts states ‘Care has to be exercised when relying on statistics as a means of establishing causation. The court must look at a claimant's individual circumstances rather than general statistics’. 27 In an often-cited summary judgement in which the consideration of possible survival is discussed, Justice Pepperall noted ‘general statistical evidence alone is, however, unlikely to be sufficient. For example, even where the rate is over 50%, a raw survival rate for the group into which (without the relevant event or omission) the deceased is said to fall is unlikely to be sufficient because, without evidence supporting the proposition derived from the population data, a jury could not safely conclude that he or she would have fallen into the category of survivors. As Croom-Johnson LJ put it, being a figure in a statistic does not of itself prove causation’. 28
Therefore, our view (supported by the findings of a 2025 Dutch Delphi study addressing the same question) is that multidisciplinary panel review represents best practice, with quantitative data used as an adjunct where available. 29
However, we propose refinements to the multidisciplinary panel methodology based on learning from previous inquests. Traditionally, panels convene once all data are available. Experience from the Manchester Areana Inquiry suggests it may be advantageous to establish the panel at the earliest opportunity, ideally before the post-mortem examination. This would support a focused multidisciplinary approach to inform and direct the post-mortem examination, including joint consideration of ancillary techniques such as post-mortem imaging, with angiography where appropriate. 10 Such an approach would help ensure adequate injury assessment in cases that may later become contentious.
During discussions relating to Saffie-Rose Roussos at the Manchester Arena Inquiry, expert opinion diverged on the preventability of thigh injuries identified on non-contrast CT but not examined invasively. 10 Had the multidisciplinary panel met prior to the invasive post-mortem examination, these injuries could have been identified as relevant, enabling targeted examination and potentially reducing deliberation time and uncertainty for the family. 30
Current gap: which professionals should be involved in this process?
Common panel participants described within the literature are summarised in Box 2. 4
Prehospital physicians now represent the expected standard of care within the UK, typically with backgrounds in Emergency Medicine, Anaesthesia or Intensive Care. 31 It is therefore logical to include prehospital physicians from each core specialty, as their experience enables input on the pathophysiology, available interventions, anticipated patient trajectories, prehospital challenges and resource restraints. Alongside forensic pathologists, forensic radiologists and surgeons; this would create a well-rounded expert panel.
Trauma surgeons Forensic pathologists Emergency physicians Anaesthetists Intensivists
Trauma surgeon (with experience in damage control surgery) Intensivist (with prehospital experience) Anaesthetist (with prehospital experience) Emergency Physician (with prehospital experience) Forensic Radiologist Home Office Registered Forensic Pathologist Patient and Family Liaison Clinician
We strongly believe the process would benefit from including patient and family liaison clinicians. Typically drawn from nursing or paramedic backgrounds, these clinicians are employed by UK air ambulance charities to provide aftercare and family support. Their national network is well placed to support families throughout the inquest process. Whilst this role is traditionally undertaken by police family liaison officers; patient and family liaison clinicians offer the additional advantage of clinical expertise, enabling them to sensitively interpret clinical discussions and act as a conduit between families and inquest participants, ensuring family views and perspectives are heard. 32
The introduction of patient and family liaison clinicians would support a key recommendation made in ‘The Patronising Disposition of Unaccountable Power’ regarding family engagement and communication throughout the inquest process. 9
Current gap: what nomenclature should be used?
There is inconsistency internationally in inquest nomenclature, with deaths classified as ‘survivable’ or ‘preventable’, often without explanation for the chosen term. One explanation may be the perception of these terms, meaning it is essential we consider the impact that these terms may have upon a patient's loved ones.
Eastridge (USA, military) acknowledges this and states: ‘analyses in the civilian trauma literature denote these as ‘preventable’ deaths… we chose not to use this language because it invokes the perception of wrongdoing or blame’. 7 Whilst understandable, it is important to consider that Eastridge is discussing the review of military deaths, where families may learn of the determination in writing, without the contextual discussion typical in civilian inquests.
When choosing terminology, it is important to recognise differences between military and civilian practice, while also noting potential similarities, particularly in mass fatality incidents such as terrorist attacks or interpersonal violence. Holcomb (USA, military) states, ‘The classic terminology encountered in the civilian literature when conducting a similar analysis is “preventable death”, “potentially preventable death” and “nonpreventable death”. However, delivery of care on the battlefield is dictated as much by the tactical situation as by traditional medical necessity. While a casualty may sustain an injury that is considered treatable and from which the soldier should not have died, if this same injury occurs during a fire fight that prohibits a medic or soldier from reaching the casualty, then to categorize the death as “preventable” is erroneous. The term “preventable” implies that something could have or should have been done to alter the final outcome of the patient’.
In the context of a mass-fatality inquest, if a patient dies from survivable injuries, but care was delayed due to scene hostility, this should be explicitly discussed in the determination. While Holcomb argues this is why the term ‘preventability’ should not be used, we disagree. If a death could have been prevented through non-clinical interventions (i.e. had armed police arrived sooner or used different tactics), this must be identified to support learning. Conversely, if nothing could have been done differently due to non-modifiable factors, a death from survivable injuries may reasonably be classified as non-preventable, provided the determination explains the circumstances. Separating survivability (based on injuries) from preventability (considering co-morbidities, care and scene factors) allows deeper analysis and more detailed learning.
With these arguments in mind, we recommend using ‘preventable’, ‘potentially preventable’ and ‘non-preventable’ as part of a two-phase approach to promote international consistency, recognising that UK mass fatality inquests occur in open forums attended by families. The points raised by Holcomb and Eastridge further underscore the importance of presenting each determination as a narrative, providing context and specifying how outcomes might have been altered to support learning and institutional development. It also highlights the importance of including patient and family liaison clinicians, who can sensitively explain and contextualise medical discussions for loved ones.
Current gap: what is meant by ‘survivable’?
The first part of the two-phase approach considers ‘survivability’ (in ideal circumstances, has this pattern of injury ever led to a survivor?). However, ‘survivor’ remains undefined. One might assume survival means the patient did not die at scene (i.e. reached hospital), but this is not always meaningful – for instance, a child may only be pronounced deceased upon hospital arrival, despite never showing signs of life. Does this count as survival or merely delayed legal recognition of death?
There is no clear definition of survival in the literature. Trauma and resuscitation research often uses time-based outcomes, such as survival to hospital, 24 or 96 h, 30 days or hospital discharge.33,34 Whilst standardised in medical research, using timepoints beyond hospital arrival weakens the assessment of prehospital care, as outcomes are influenced by multiple in-hospital professionals and interventions. For best practice, we recommended defining survival as a patient arriving at hospital with sustained, spontaneous cardiac output. Beyond this point, in-hospital variables make it difficult to isolate the effect of prehospital management.
Current gap: what data should be reviewed?
Data available for each death will vary, making a minimum dataset difficult to describe, and may include the post-mortem report, clinical notes from the attending team and any recorded observation data.
Digital media, such as CCTV and Body Worn Video (BWV), is rarely discussed in the literature. The Manchester Arena Inquiry showed that police were often first at patient's sides, and BWV footage allowed reviewers to observe the patient's presentation earlier than clinicians or clinical records. 10 Such media provides context and insight into injury severity, showing dynamic signs such as complexion, behaviour and work of breathing. It also enables construction of a timeline from injury to likely cardiac arrest, highlighting potential intervention opportunities.
Previous studies have defined a minimum dataset, but available data will vary depending on the professionals and services involved. All available data should be presented to the review panel, with particular emphasis on using digital media to construct a timeline from injury to death, to identify opportunities for intervention.
Current gap: what should the burden of proof be for these judgements?
The standard of proof within the law is a concept not discussed within the preventable death literature. Oliver and Walters found that every study utilising a multidisciplinary panel achieved a determination through a majority consensus, equating to a determination of “on the balance of probabilities” within England and Wales. 4 This represents the lower of the two thresholds of proof (the higher being ‘beyond reasonable doubt’) and would accord with the standard required for civil matters, including coroner's verdicts and professional tribunals, and thus is considered the most appropriate threshold for mass fatality inquests. 35
In cases where a determination may infer negligence or unlawful killing, this may have downstream criminal implications, not to mention the emotional impact this may have upon the patient's loved ones. 35 However, the challenge with a higher burden of proof lies in the intrinsic uncertainty associated with prehospital deaths and the large volume of ‘unknowns’. The sheer complexity of human physiology may mean that it becomes impossible to judge, beyond all reasonable doubt, whether a death was preventable or not from a given injury pattern, considering an individuals’ co-morbidities, fitness and physiological reserve.
At the outset of an inquiry, legal clarification would be beneficial to ascertain whether the balance of probabilities is an appropriate threshold when labelling a death as ‘preventable’, or whether the higher burden of proof is required.
Current gap: what logistical challenges should be planned for?
It is accepted that rapidly convening a multidisciplinary panel comes with challenges. The overall direction will be from the coroner or presiding judge, however, we suggest a registry of suitable experts be created and held by a central government agency (within the UK, this would be the National Crime Agency), where members can be pre-screened for eligibility. This would allow timely convening, using members external to the locality of the event, to enable prompt screening of cases and to focus the forensic pathology strategy for each. This registry may also facilitate the creation of an independent oversight group, to provide governance.
As part of the inquest, families may appoint independent representation. Consideration needs to be given to how these representatives are best integrated within the process. Our view is that independently appointed representatives act as advisors to the review panel, with their input facilitated through the patient and family liaison clinician.
The next steps
Future reviews of deaths following mass fatality incidents are inevitable. To be prepared, we must learn from past inquiries and establish recommended best practices. A UK-specific best practice framework is urgently needed to address recognised issues. 9 The closest guidance is the WHO Guidelines for Trauma Quality Improvement Programmes, which focus on isolated in-hospital deaths and are generalised for global applicability. Despite being published in 2009, notable UK inquests have diverged from both these guidelines and broader international methodologies.
There is a need to define best practice for reviewing prehospital deaths after mass fatality incidents, including an agreed glossary of terms and a standardised multidisciplinary review process. We therefore propose the following recommendations for a best practice framework:
Use the terms ‘preventable’, ‘potentially preventable’ and ‘non-preventable’ for international consistency. Apply a two-phase approach: first, assess survivability – in ideal circumstances, have these injuries ever led to a survivor? If no, the death is non-preventable. If yes, assess preventability by asking what could or should have been done to alter the outcome. This allows for consideration of both injuries and broader circumstances, including co-morbidities, scene factors (such as access and hostility) and the emergency response. Convene the multidisciplinary review panel as early as possible to allow guidance of the forensic pathology strategy. Establish a registry of qualified, vetted clinicians willing to participate in the multidisciplinary review process, to allow rapid convening following a mass fatality incident. Develop governance processes for oversight and refinement of survivability and preventability assessments. Ensure multidisciplinary panels include greater representation of prehospital clinicians and patient and family liaison clinicians to support families through the process. Provide the determination (preventable, potentially preventable or non-preventable) alongside a narrative, clearly justifying the rationale for the determination and if applicable, specifying what could or should have been done to alter the outcome.
A suggested framework, developed from expert opinion and our working group discussions, is included (Appendix 1), supported by the international literature.
Developing and implementing an agreed framework offers several advantages. A standardised approach allows the UK to demonstrate best practice that can be replicated internationally and refined after each inquest, rather than reinventing methods each time. International adoption enables mutual learning, promoting rapid, collective improvement. Finally, a defined process facilitates better preparation and a more streamlined approach, as recommended in ‘The Patronising Disposition of Unaccountable Power: Independent Review of Forensic Pathology’. 11
Any framework must ultimately be refined with input from the relevant Royal Colleges, legal experts and the families of those who have lost their lives, to ensure future emergency responses acknowledge and embed the learning obtained from these terrible incidents.
Footnotes
Funding
Funding was kindly provided for open access publication by Queen Mary University of London.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Appendix 1: Suggested best practice for the review of a death following a mass fatality incident.
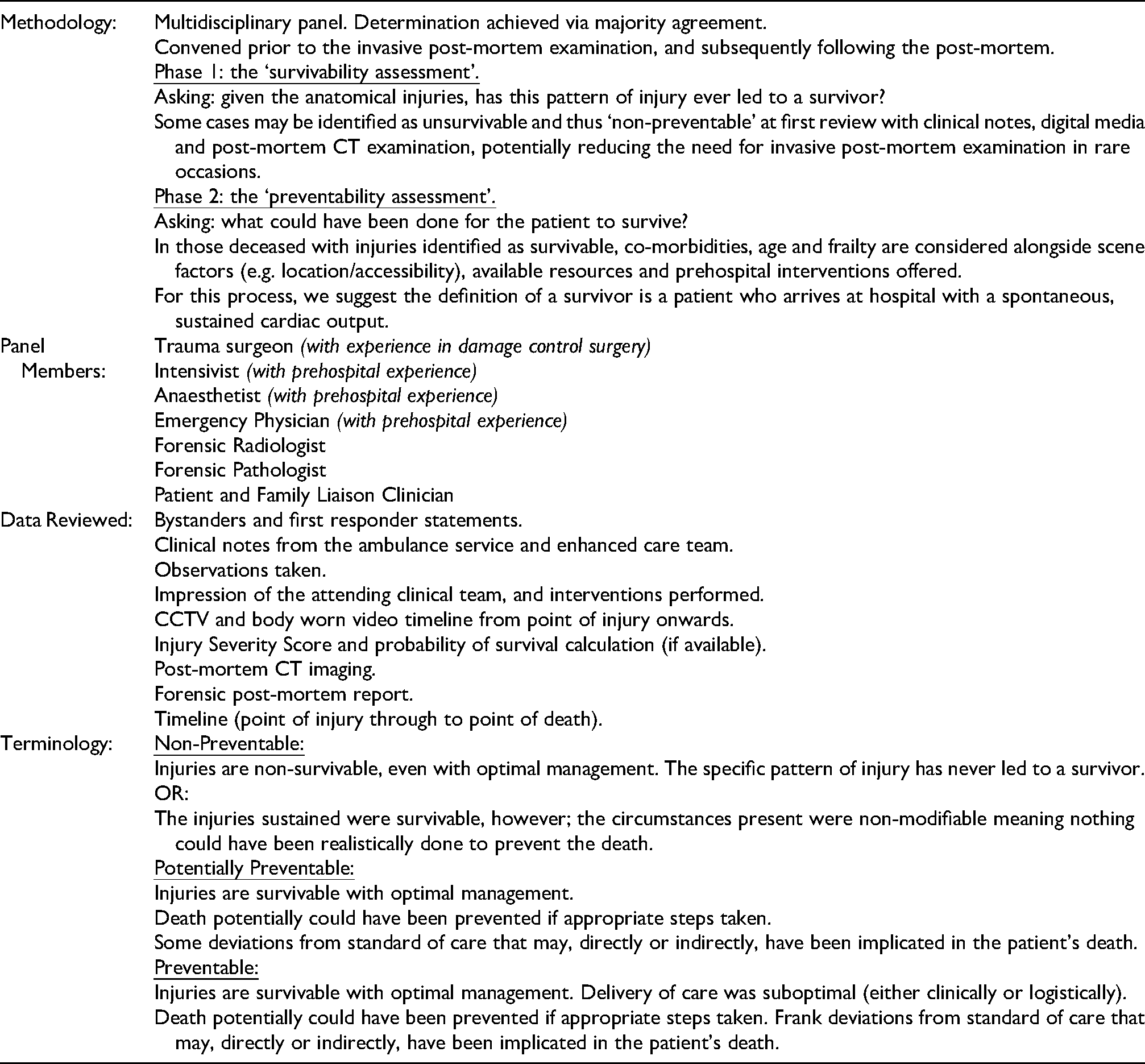
| Methodology: | Multidisciplinary panel. Determination achieved via majority agreement. Convened prior to the invasive post-mortem examination, and subsequently following the post-mortem. Asking: given the anatomical injuries, has this pattern of injury ever led to a survivor? Some cases may be identified as unsurvivable and thus ‘non-preventable’ at first review with clinical notes, digital media and post-mortem CT examination, potentially reducing the need for invasive post-mortem examination in rare occasions. Asking: what could have been done for the patient to survive? In those deceased with injuries identified as survivable, co-morbidities, age and frailty are considered alongside scene factors (e.g. location/accessibility), available resources and prehospital interventions offered. For this process, we suggest the definition of a survivor is a patient who arrives at hospital with a spontaneous, sustained cardiac output. |
| Panel Members: |
Trauma surgeon (with experience in damage control surgery) Intensivist (with prehospital experience) Anaesthetist (with prehospital experience) Emergency Physician (with prehospital experience) Forensic Radiologist Forensic Pathologist Patient and Family Liaison Clinician |
| Data Reviewed: |
Bystanders and first responder statements. Clinical notes from the ambulance service and enhanced care team. Observations taken. Impression of the attending clinical team, and interventions performed. CCTV and body worn video timeline from point of injury onwards. Injury Severity Score and probability of survival calculation (if available). Post-mortem CT imaging. Forensic post-mortem report. Timeline (point of injury through to point of death). |
| Terminology: | Injuries are non-survivable, even with optimal management. The specific pattern of injury has never led to a survivor. OR: The injuries sustained were survivable, however; the circumstances present were non-modifiable meaning nothing could have been realistically done to prevent the death. Injuries are survivable with optimal management. Death potentially could have been prevented if appropriate steps taken. Some deviations from standard of care that may, directly or indirectly, have been implicated in the patient's death. Injuries are survivable with optimal management. Delivery of care was suboptimal (either clinically or logistically). Death potentially could have been prevented if appropriate steps taken. Frank deviations from standard of care that may, directly or indirectly, have been implicated in the patient's death. |