
Abstract
Drowning is a leading cause of injury-related deaths among youth worldwide, often linked to inadequate supervision and ineffective guardianship. While paediatric studies have examined demographics and risk factors, little is known about how these variables interact to influence rescue likelihood. This study addresses that gap using a multivariate binary logistic regression model to assess the odds of not receiving a rescue attempt, using fatality records (n = 638) from coroners and medical examiners across Canada (2006–2016). This approach captures all known accidental fatal drownings but findings cannot be generalized to include incidents in which the individual survived. The best model explained 45.1% of the variance in rescue outcomes (Nagelkerke Pseudo R² = .451) with 84.6% accuracy. Findings revealed that age, sex, alcohol use, perimortem activity, water body type and urban/rural location significantly impacted rescue attempts. However, chronic medical conditions and general bystander presence showed no significant relationship at the bivariate level. When demographics and situational factors were considered, bystander type (with adult, minors only or alone/not witnessed) became a key model contributor for predicting rescue attempt likelihood. Teenagers (15–18 years) accounted for 33.5% of drownings, followed by toddlers (2–4 years, 21.9%) and children (5–11 years, 20.5%). Compared to infants, older children and teens faced greater risks of not being rescued, and bystander presence does not equate to capable guardianship. Open water environments posed the highest risk, with ocean drownings 7.9 times more likely to result in no rescue attempt, compared to domestic settings.
Introduction
Child drownings remain a significant public health concern worldwide, and according to the World Health Organization (WHO), drowning is the third leading cause of unintentional injury deaths worldwide. 1 In the Canadian 2024 Drowning Prevention Report, 2209 deaths were reported between 2015 to 2019 from Canada alone. 2 In North Carolina, a study of paediatric drowning injuries through emergency department intake information showed that drowning was proportionally higher among older-aged children, and COVID-19 pandemic-related changes (pool closures, fewer water safety training opportunities and lifeguard shortages) did not make a significant impact on paediatric drowning rates. 3 They also found that more drownings among younger children were occurring in pools, despite historically occurring in open fresh-water environments. Similar results were found in other studies, whereby younger children (ages 1–4) and teenagers (ages 15–17) were found to be drowning at higher rates than other age groups.4–6 New Canadian Tweens (aged 11–14) were five times as likely to not know how to swim compared to their classmates, despite participating in the same types and frequency of activities near and around water environments. 7 In a study of all paediatric drowning patients transported by emergency medical services in the United States in 2019 (n = 1160), patients were less likely to develop critical illness following drownings if they were rescued in an urban environment. 5 Several studies have pointed to timely intervention as an important factor in preventing critical illness after drowning.5,6,8,9 Among 1767 drowning deaths identified in the US Cardiac Arrest Registry to Enhance Survival (CARES) database, bystander-initiated CPR resulted in significantly higher odds of favourable neurological outcomes. 6 Xiong et al.'s 9 study on cardiac arrests resulting from drowning found that the survival group had a significant 57.1% bystander witness rate, as compared to the mortality group where only 17.0% were witnessed. Results further supported that bystander presence greatly improved survivability. In Australia, an average of 6.5 children drown each year in bathtubs – all of whom were left without adult supervision. 10
Despite advancements in water safety awareness and preventive measures, drowning incidents continue to occur, highlighting the need for more comprehensive understanding and targeted interventions. Utilizing Canada-wide fatal accidental aquatic death records, the objective of this research was to identify the demographic and situational risk factors that influence the likelihood of an individual being rescued. The assumption is that immediate interventions can greatly improve a person's chance of survival, thus, there is value in assessing factors relating to rescue attempts. By taking an Environmental Criminology approach to understanding risk mitigation and the differences between supervision and guardianship, we examined the current state of oversight of Canadian youth in drowning fatalities and in turn, identify gaps in knowledge and propose evidence-based recommendations for policy and practice aimed at reducing the incidence of drowning among children. Through a critical analysis that utilizes nation-wide medicolegal drowning data, we underscore the urgency of addressing this preventable tragedy and emphasize the importance of collaborative efforts among families, communities, and policy makers to safeguard the lives of children in aquatic environments. It is important to note that at the time of publication, Canadian health systems and databases remain highly fragmented, and are not integrated with their respective provincial medicolegal system, whether a coroner or medical examiner system. Without a centralized repository or data sharing agreements in place, data on successful rescues are largely inaccessible. It is probable that some successful rescues are not reported to government bodies, because those that survive may simply go home without sharing their experience with the police or EMS. As such, it is not yet possible to establish rescue likelihood – a study using only fatalities can only speak to whether rescue attempts were made in such fatalities.
In recent years, the social and parental expectations around child supervision have intensified, especially in settings involving water safety. Institutional policies have evolved to place greater responsibility on parents for water safety, aligning with the expectation of intensive supervision. National and local water safety guidelines, including the Canadian Drowning Prevention Plan (2022), include explicit recommendations for active supervision by parents at all times when their children are near or around water, regardless of the child's age or swimming ability. 11 This is further reinforced by public campaigns, such as the Lifesaving Society's tip cards and water safety materials that were translated into 10 common secondary languages. These programmes promote vigilance and endorse a zero-tolerance approach to unsupervised children near water. Public policy further reflects a preventative approach, as evidenced by increasing regulation around pool fencing in private residences, programming for equitable access to swimming lessons, and new policies around child supervision in public spaces. These policies, though potentially beneficial in reducing water-related incidents, can also intensify the expectations that parents can and will actively mitigate risks in all water-related environments; however, few studies have actually examined the impact of the presence of bystanders and potential guardians (minors included) on survivability.
Applying Crime Prevention and Social Control frameworks, Supervision refers to the presence of entities that actively monitor a particular space or people within a predetermined area. It can be an object or person that acts as a regulator of behaviours by virtue of its presence and serve as an intervener for social control. Supervisors can be further subcategorized into Place Managers, Controllers and Super Controllers12,13 Place Managers are assigned to a space such as lifeguards and security guards. Controllers include ambient surveillance like CCTV cameras that monitor public spaces as an informal social control, or even volunteer community members that have accepted a formalized role of authority. Super Controllers are the type of supervisors that oversee policies for a given region and are policy and decision-makers that oversee the governance of a given location or group of peoples. This includes regulatory structures and accountability that is place specific.
Guardianship involves individuals or elements within the environment that are capable and motivated to intervene for a specific individual. They may be formal such as designated family members tasked with overseeing children, or informal such as nearby neighbours or other legitimate space users and bystanders. Guardianship is not just about the presence of those with the responsibility to intervene but must also include an element of willingness. The key difference is that guardianship is about the protection and advocacy of an individual or specific community's health, whereas supervision extends to health systems, public safety programming and/or involve an element of formalized oversight (appointed individuals).
Methods
Data source
In partnership with the Canadian Drowning Prevention Research Centre and Lifesaving Society, all unintentional fatal drowning records from every coroner and medical examiner's office in Canada were collected for incidents that occurred between 1 January 2006 to 31 December 2016 (representing an 11-year period). This includes detailed information about the deceased individual's demographics (age, sex, medical conditions at the time of death), situational factors (drug/alcohol involvement, what the deceased was doing, location), and supervision and guardianship. Most importantly, we know if an attempted rescue at the time of death took place (i.e. received an intervention). The focus of this study is to examine what factors influence the likelihood of rescues being attempted in aquatic paediatric deaths, stratified by age groups based on expected stages of cognitive and physical development. A total of 638 cases involving victims ages 18 and under were included in this study. The manner of death was accidental in 99.5% (635) of these cases, and 0.5% (3) were undetermined. As there is no federal standard for what fields of data are collected by each provincial service, additional steps were taken when collating and cleaning data to ensure that cross-comparisons were possible. Information on data availability is noted in the descriptive statistics summary (Table 1). A combination of IBM SPSS (v.30.0) and Microsoft GeoNames were used to analyze and visualize data. Joint ethics approval between Simon Fraser University and Lifesaving Society was granted (SFU-2018s0742).
Descriptive statistics of unintentional fatal drowning incident factors in Canada from January 2006 to December 2016 (11-year period), including data availability scores (n = 638).
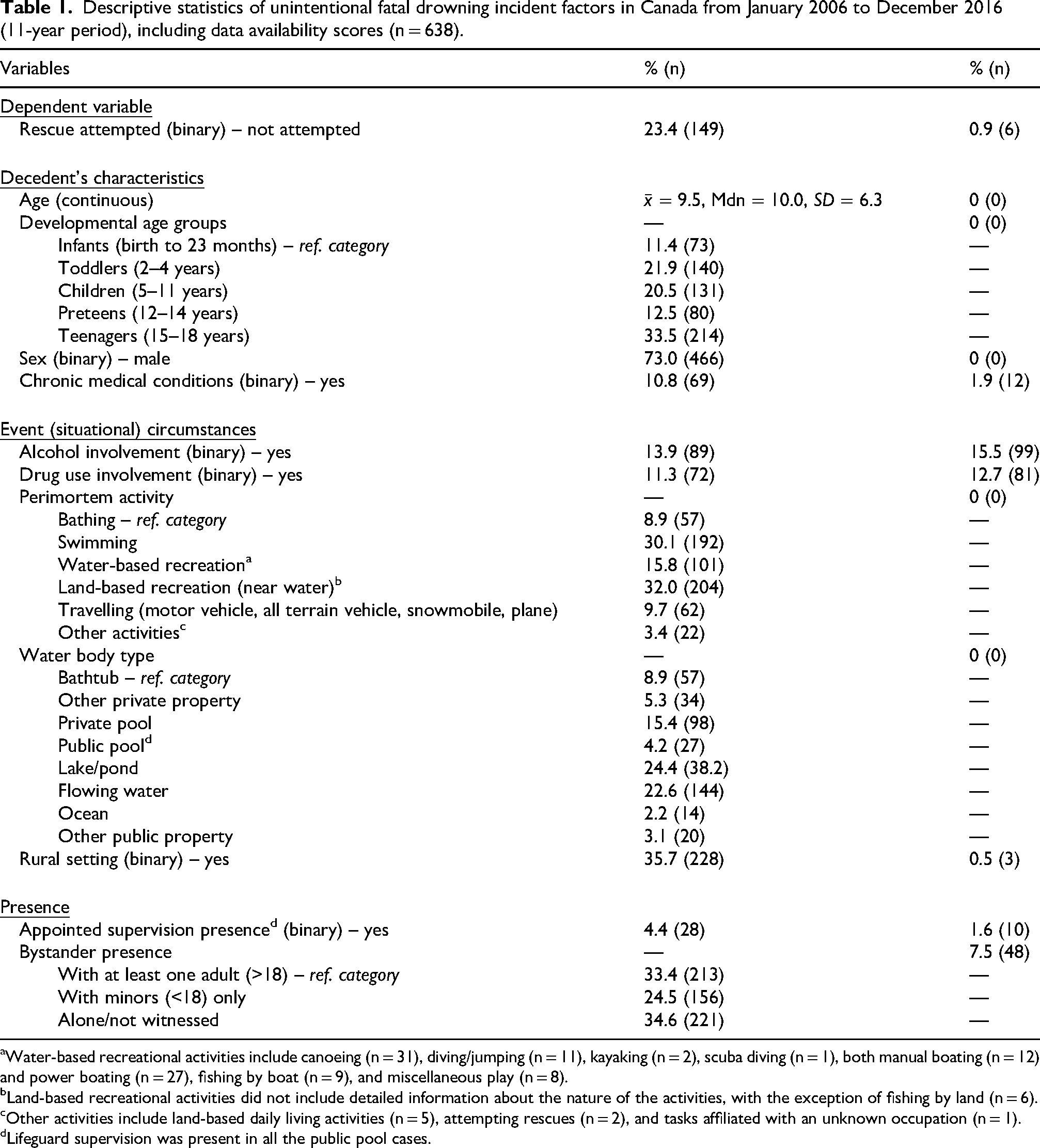
Water-based recreational activities include canoeing (n = 31), diving/jumping (n = 11), kayaking (n = 2), scuba diving (n = 1), both manual boating (n = 12) and power boating (n = 27), fishing by boat (n = 9), and miscellaneous play (n = 8).
Land-based recreational activities did not include detailed information about the nature of the activities, with the exception of fishing by land (n = 6).
Other activities include land-based daily living activities (n = 5), attempting rescues (n = 2), and tasks affiliated with an unknown occupation (n = 1).
Lifeguard supervision was present in all the public pool cases.
Measures of risk
It is not possible to capture information about successful rescues, given that parents, family and other interveners can rescue a person in distress without subsequently seeking medical attention. As such, the best measure we have of drowning risks is by fatalities, and to closely examine the circumstances that both preceded and followed the drowning incident. We can reasonably surmise that a person's chance of survival would improve if a rescue took place; when we say rescue, we are referring to immediate intervention at the time of the incident – not the rescue and recovery that takes place when search and rescue or emergency medical services personnel arrive to locate the body. There are a number of reasons why a rescue may fail, from delayed responses, pre-existing medical conditions, preceding blunt force trauma, distance travelled to reach a hospital, etc. – indeed, all of our cases are of fatalities (unsuccessful rescues). But this remains the best measure we have of risk, and thus, this study examines what co-factors influence the likelihood of someone being rescued (i.e. a rescue attempt taking place).
Analytical strategy
Bivariate analyses and binary logistic regression were used to discern the relationship between demographic and event variables with the likelihood that there would be an intervention (‘Rescue Attempted’). Because drowning occurs in unmonitored locations and there are few mechanisms to track non-fatal drownings, we are unable to ascertain the true number of rescues given that these data are comprised of deaths overseen by coroners/medical examiners. Statistical significance was calculated to a 95% confidence interval (α = 0.05), with significance being presented as either Cohen's d (dichotomous or continuous data) or Cramer's V (2 + levels). A two-step sequential model was chosen for the regression to assess how decedent characteristics, event factors, and supervision/guardianship presence impact the likelihood of an attempted rescue. Effect sizes were measured using Cramer's V, Phi coefficient, and Cohen's d, whereby the strength of association for V and Phi thresholds were < .10 very small, .10 small, .30 moderate and .50 strong and Cohen's d were < .20, .20, .50 and .80 respectively. Multi-factor categorical variables (developmental age groups, perimortem activities and locations) were dichotomized for secondary bivariate analysis and regression. Developmental age groups improved the model more than age (scale), thus, were chosen for the regression model. Despite manually entering all locations into the regression model, SPSS automatically removed ‘Other Public Property’ due to its lack of significance at both the bivariate and multivariate level of analysis. This is important to note, as despite there being no adjusted R2 function that penalizes models for including poorly contributing factors, it appears that the underlying logic and precautionary steps are now integrated.
Measures
The decedents’ ages were recoded into groups that reflect paediatric categories of development,14–16 which also coincide with health and safety guidelines for parents based on the expected level of development of the child 14 : data resolution did not discern between neonatal infants (birth to 27 days) and infants (28 days to 23 months). Biological sex was provided as a binary variable; there were no notes or indicators denoting gender non-binary affiliations. Although active bystanders may have lifeguard qualifications, the variable for Lifeguard Supervision Presence denotes professional lifeguards that were assigned or designated to be there as place managers. Regarding data normality, all variables were within accepted ranges (±2 skewedness and kurtosis) with the exception of drug involvement, chronic medical conditions, and lifeguard supervision. In a test of variance inflation factor (VIF score), the results for all predictor variables were < 2 and age was < 7, all of which indicate minimal concern about multicollinearity. Equal variances could not be assumed for the t-test, thus correct values were used.
Results
With 638 cases spanning 11-years, there were an average of 58 paediatric accidental fatal drowning cases per year in Canada (Figure 1). The highest counts were from Ontario (37.5%, 239), followed by Quebec (18.3%, 117), Alberta (10.7%, 68) and British Columbia (9.6%, 61). No rescue was attempted in 23.4% (149) of cases (Table 1). Deceased mean age was 9.5 years old, with the highest concentration being teenagers (aged 15–18 years old) at 33.5% (214), toddlers aged 2 to 4 (21.9%, 140) and children aged 5 to 11 (20.5%, 131). Linearly, age was found to be a significant predictor of rescues not attempted (t = −12.451, Cohen's d = 5.820, p ≤ .001) (Table 2). When age is conceptualized as developmental age groups, the effect size is significantly strong (Cramer's V = .408, p ≤.001) and contributes meaningfully to the regression model. In particular, when situational factors and presence of bystanders are also considered, being a teenager (15–18 years old) puts them at 7.8× times more risk of not being rescued in a drowning incident than an infant (Exp(B) = 7.775, p = .007) (Table 3). Teenagers are also drowning at higher rates than other age groups; in fact, one in three paediatric aquatic deaths are teenagers (33.5%, n = 214), making them a high-risk group. Children were at 3× times the risk (Exp(B) = 2.945, p = .150), and preteens at 4.5× times the risk of not being rescued (Exp(B) = 4.500, p = .056). With all other factors constant, the only age group that is at greater risk than infants are toddlers (2–4 years old) (Exp(B) = .489, p = .351) at the multivariate level.
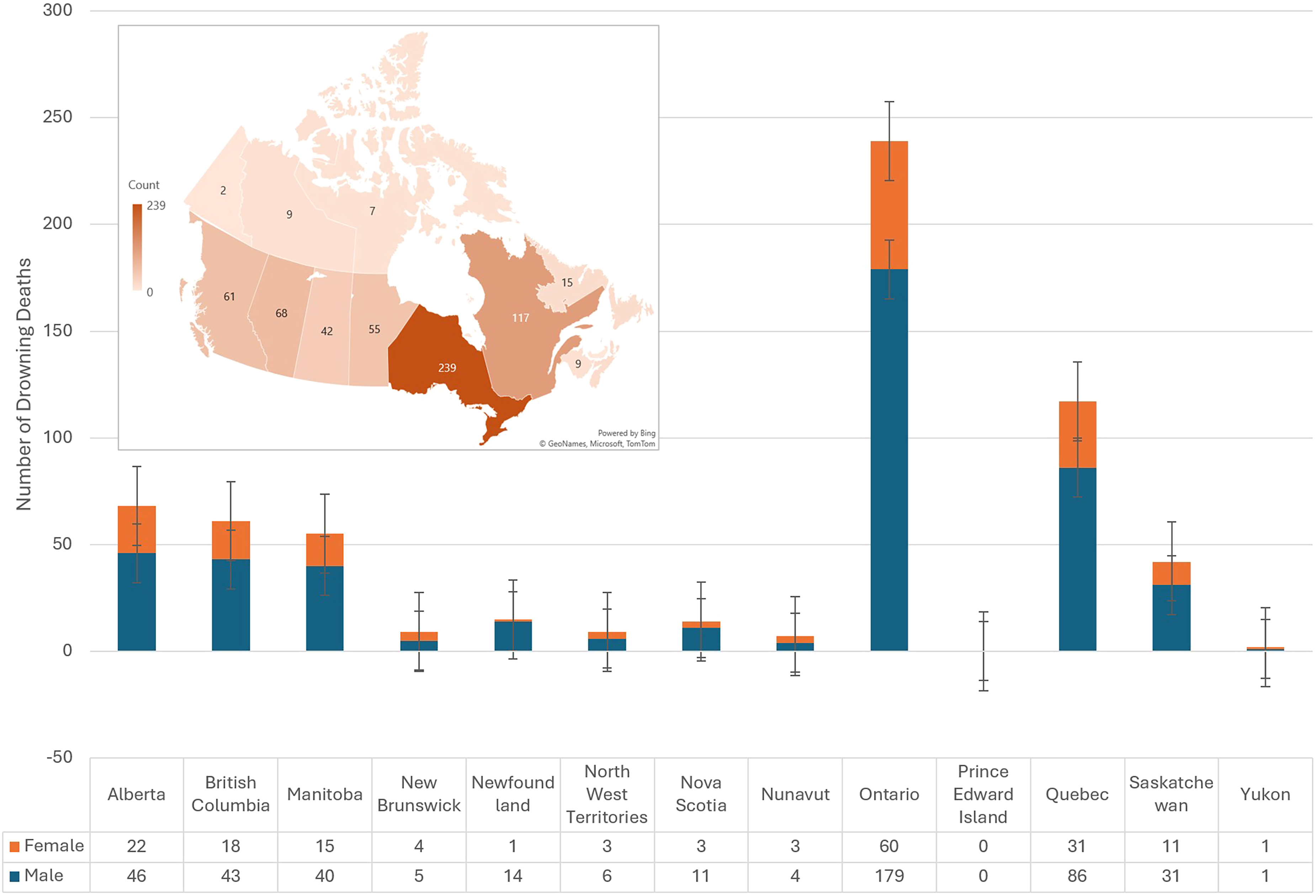
Boxplot bar chart and heat map depicting the distribution of cases of paediatric drownings across provinces and by biological sex (n = 638).
Bivariate associations between the rescue dependent variable and the independent demographic and event variables (n = 638).
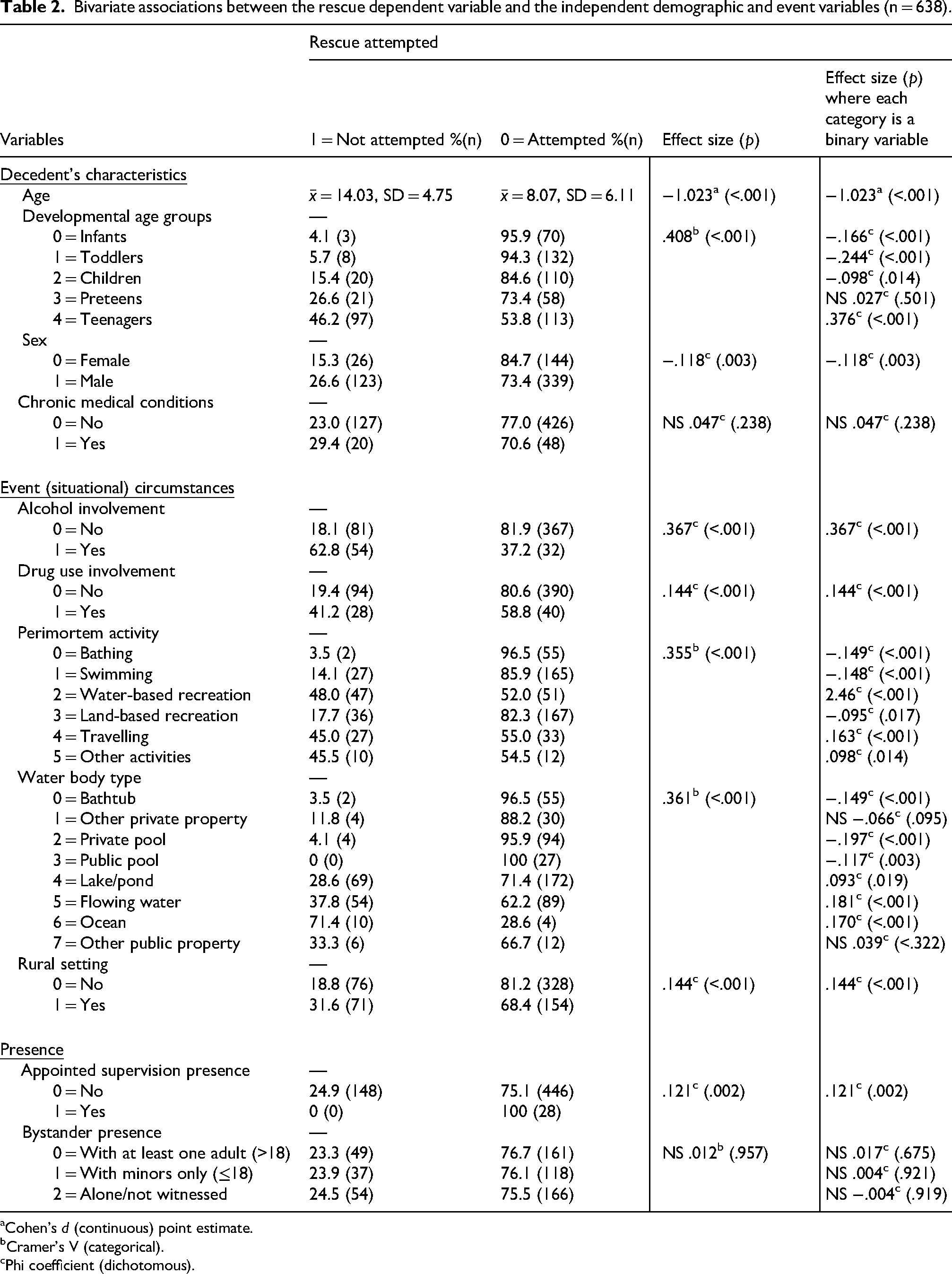
Cohen's d (continuous) point estimate.
Cramer's V (categorical).
Phi coefficient (dichotomous).
Multivariate binary logistic regression model of rescue attempts (lack thereof) in paediatric unintentional fatal drowning incidents in Canada (n = 638).
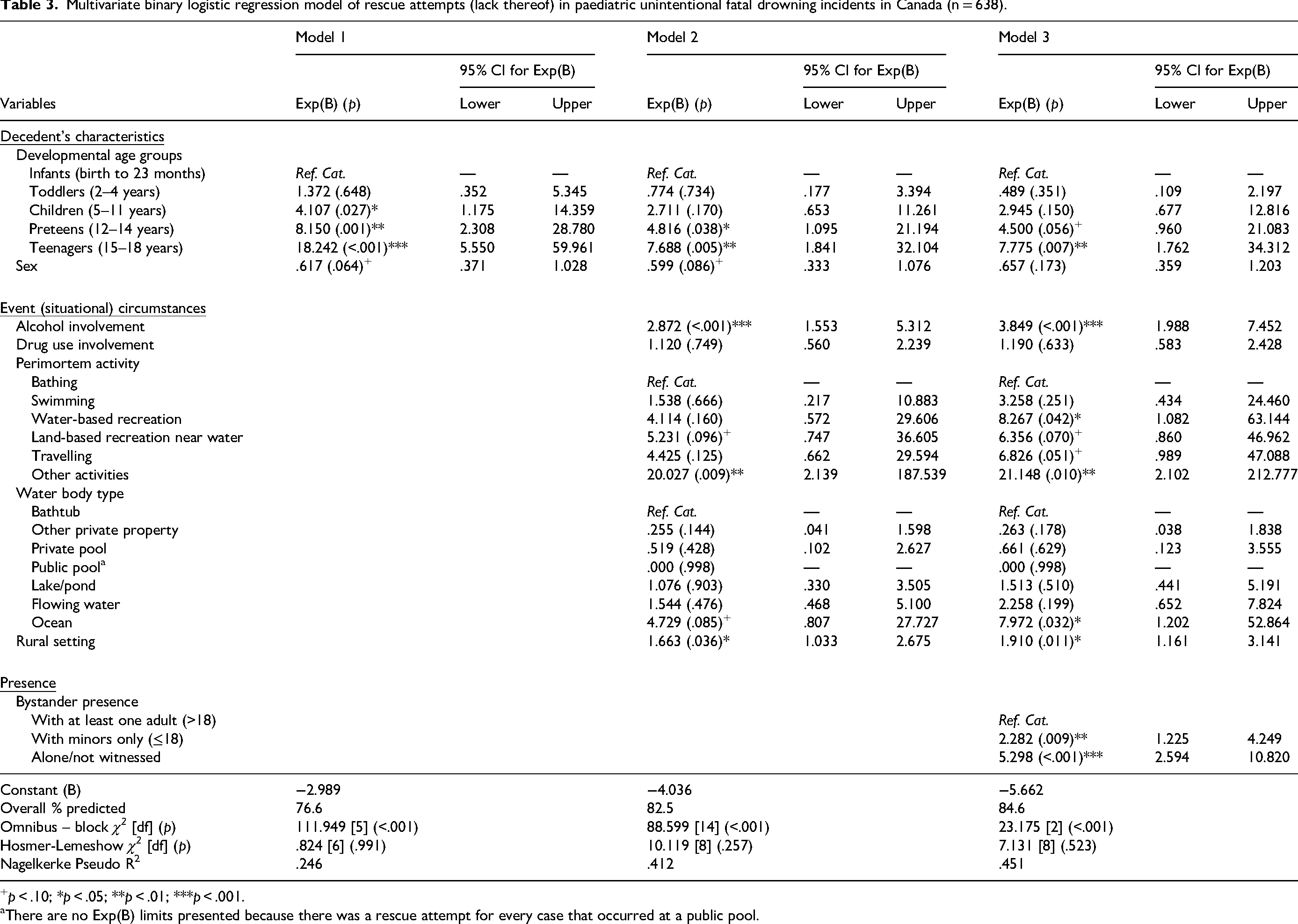
+p < .10; *p < .05; **p < .01; ***p < .001.
There are no Exp(B) limits presented because there was a rescue attempt for every case that occurred at a public pool.
Nearly three-quarters of the deceased were biological males (73.0%, 466). Although the group of females were smaller (172), 84.7% of them had a rescue attempt compared to 73.4% of the males. The presence of chronic medical conditions was only noted in 10.8% (69) of the death records. In cases where bystander presence was known, 66.7% of those with a known chronic medical condition drowned alone or not witnessed, as opposed to 34.6% of those that did not have a medical condition. This challenges our expectations that those with pre-existing conditions would more likely be rescued due to likely being under greater care and observation – our results show that they are just as likely to be rescued, and so presence of pre-existing conditions is, thus, non-significant for evaluating risk of not being rescued (p = .238). Chronic medical conditions were not significantly related to whether an individual would be rescued, and there were only marginal R2 gains (<.01) at the multivariate level, thus, it was excluded from the regression model (Table 2).
Regarding event (situational) circumstances, alcohol and drug involvement were flagged as being contributing factors to the drowning fatality in 13.9% (89) and 11.3% (72) of the cases, respectively (Table 2). Among teenagers, alcohol and drug involvement related primarily to the deceased's use and subsequent impairment, whereas in cases of infants to preteens, alcohol and drug involvement pertained to the cause of distraction of their primary caretaker. Alcohol and drug involvement were found to be significantly associated with the likelihood of being rescued, with alcohol having a moderate effect size and drugs a weaker one. Alcohol continued to be useful as a predictor of rescue attempts (Table 3), and when demographic and situational factors are considered, model 3 suggests that alcohol involvement puts the person at a significant 3.9× times the risk of not being rescued (Exp(B) = 3.849, p ≤.001).
Perimortem activities refer to what the decedent was doing right before the drowning incident occurred. A total of 8.9% (57) of the deaths occurred while bathing, of which, more than half were infants (54.4%, 31), toddlers (8.8%, 5) or children (14.0%, 8). All bathing activities occurred in a domestic bathtub, not pools, open water or other private property locations. A third of the deaths occurred while swimming (30.1%, 192), and 15.8% (101) during water-based recreational activities such as kayaking, canoeing, scuba diving and boating (Table 1). Another third unexpectedly occurred during land-based recreation activities near water (32.0%, 204), which represents hiking and play where there was unintentional water entry. The remainder of the activities were grouped into travelling by motor vehicle, all terrain vehicle, snowmobile or plane (9.7%, 62) and other activities (3.4%, 22). What the deceased was doing at the time of death was moderately significantly tied to their likelihood of being rescued (Cramer's V = .355, p ≤ .001), all of which contributed explanatory power to the predictive model. The ‘other activities’ category included those engaged in work related to daily living and occupation was found to place the individual at greatest risk (Exp(B) = 21.148, p ≤ .010) of not being rescued compared to the reference category, which might be attributed to how these activities largely pertained to unintentional water entry. Compared to bathing, the risk of not being rescued was 3.3× times higher while swimming, 8.3× times higher during water-based recreation, 6.4× times higher during land-based recreation (near water), and 6.8× times higher in cases where the deceased was in the middle of travelling.
Locations mirror the perimortem activities, in that the spatial characteristics of an environment is what allows the activity to take place; as such, it is not surprising that the location reflects a similar significant moderate effect on the likelihood of a rescue attempt (Cramer's V = .361, p ≤ .001). Open waters pose a greater threat, as in the case of oceanic locations with 7.9× times the risk of not being rescued (Exp(B) = 7.972, p = .032), flowing water (Exp(B) = 2.258, p = .199) or lakes/ponds (Exp(B) = 1.513, p = .510), with oceans being the only location that significantly contributes to model 3 – which is conversely true of enclosed locations like private property, public pools and private pools. Of note, there was a rescue attempt for all 27 drownings that occurred in a public pool. Using census boundaries, population density and distance to city centres as a measure of rural versus urban centres, 35.7% (228) of these paediatric deaths took place in a waterbody that was considered rural. Although significant, the effect size is weak (Phi = .144, p ≤ .001). When considered with all other constants, it becomes a significant contributor in model 3, and results suggest that an individual is 1.9× times more likely to not be rescued if they drown in a rural environment (Exp(B) = 1.910, p = .011). Of note, rural locations alone are not significantly related to being in the presence of a potential intervener (χ2 (2)= 4.865, p = .088), given that 31.6% (67) were alone, 38.2% (81) were with at least one adult, and 30.2% (64) were with minors only.
The presence of potential interveners in paediatric drowning deaths was assessed. When it comes to appointed supervisors (i.e. lifeguards), they were present in only 4.4% (28) of cases. This small number is not surprising, as the presence of lifeguards is assumed to greatly contribute to a person's survivability and this is a population of fatalities. Additionally, lifeguards are not expected in domestic settings or unsupervised open water ways that are frequented by Canadians. There was a significant but weak effect on the likelihood of rescue attempts (Phi = .121, p = .002). Appointed supervision as a factor was ultimately removed from the model due to skewing effects caused by being present in such small numbers (4.4%) and the variable's lack of explanatory power for the multivariable logistic regression models. The opposite is true of the bystander presence, in that at the bivariate level, it is not considered significantly related to rescue attempts (χ2 (2) = .087, p = .957) but becomes a significant contributor when other demographic and situational factors are considered. Its usefulness in improving the predictive model raises the Nagelkerke Pseudo R2 from .412 to .451, representing a 3.9% increase in model fit. Moreover, by transforming the categories into dichotomous variables, we are able to extrapolate the magnitude of risk and quantify that being with only minors increases risk of not being rescued 2.3× and being alone 5.3×, as compared to being in the presence of at least one adult.
Model 1 results show that demographics alone can reliably predict 24.6% of the variance in rescue attempts. The predictive value of this model increased to 41.2% when event factors are added to the computation and further increased to 45.1% when supervision and guardianship are considered – thus, making model three the best model for its predictive power. Despite these not being an adjusted R2 result, parsimony was achieved by eliminating erroneous variables, such as existing medical conditions and other public property locations from the model. Regarding overall model fit, the omnibus test of model coefficients in all three blocks was significant, indicating that the model fits the data significantly better than a null model with no predictors (block 1: χ2 (5)
Discussion
The results of this study highlight the importance of assessing the role of informal interveners in drowning deaths, such as caretakers, peers and active bystanders, as potential guardians. Lifeguards were present in only 4.4% of these accidental fatal drownings, which shows that accidental drowning cases are happening outside the purview of appointed supervisors. While lifeguard supervision continues to play a critical role in risk management of aquatic spaces, the risk factors identified in this study prompt a deeper discussion on how we can develop a more multi-faceted approach to drowning prevention. This starts with identifying who is actually drowning in Canada. When it comes to paediatric deaths, youth of all ages are drowning, but under very different circumstances. With infants, there is an expected layer of added guardianship, and there was an attempted rescue 95.9% of the time. Yet when we drill deeper, we see that both infants and toddlers were alone when the incident begins, and despite caregivers noticing the distress within a reportedly short interval of time, the intervention is not timely enough to prevent the death. Deceased preteens, on the other hand, died in the presence of other minors 46.5% of the time (Table 3), which suggests that despite being in the presence of others, their peers could not perform the function of an effective guardian. The same logic is applied to understanding why teenagers, despite being in the presence of another adult (>18 years old) more than half the time, are 7.8 times less likely to be rescued than infants. Alcohol and drug involvement were largely present in the teenager developmental age group, but despite there being at least one adult present in 61.0% of the time when alcohol is involved, the odds of being rescued were still low. To explain this phenomenon, we believe that it is possible that the other adults present were unable to perform the duties of a guardian because they too could have been inebriated/impaired. Thus, the simple presence of a bystander does not translate to them being capable guardians. This is an important consideration because results show that alcohol involvement puts a person at four times greater risk of not being rescued.
Echoing findings from other countries, three-quarters of Canadians that drown are males. Males were more likely to be alone at the time of the incident (43.1% compared to 35.5%) and not rescued as often (73.4% compared to 84.7%). Males remain at higher risk of aquatic deaths, possibly due to lifestyle factors, particularly at later stages of development beginning with their preteens. When other factors are considered, sex no longer significantly contributes to the overall predictive model, which suggests that rescues will take place independently of sex so targeted drowning prevention initiatives for this particular group should focus on introducing water safety education at ages 12 to 14, as opposed to improved intervention or target hardening techniques.
Regarding the locations of these deaths, it is also not surprising that the odds of someone not being rescued are similar across all the structured, built environments like bathtubs and pools. As compared to domestic baths, the risk increases by 1.5× times in lakes/ponds, 2.3× times in flowing water and 8.0× times in oceanic environments. Incidents in rural locations are also nearly twice as likely to not involve a rescue attempt.
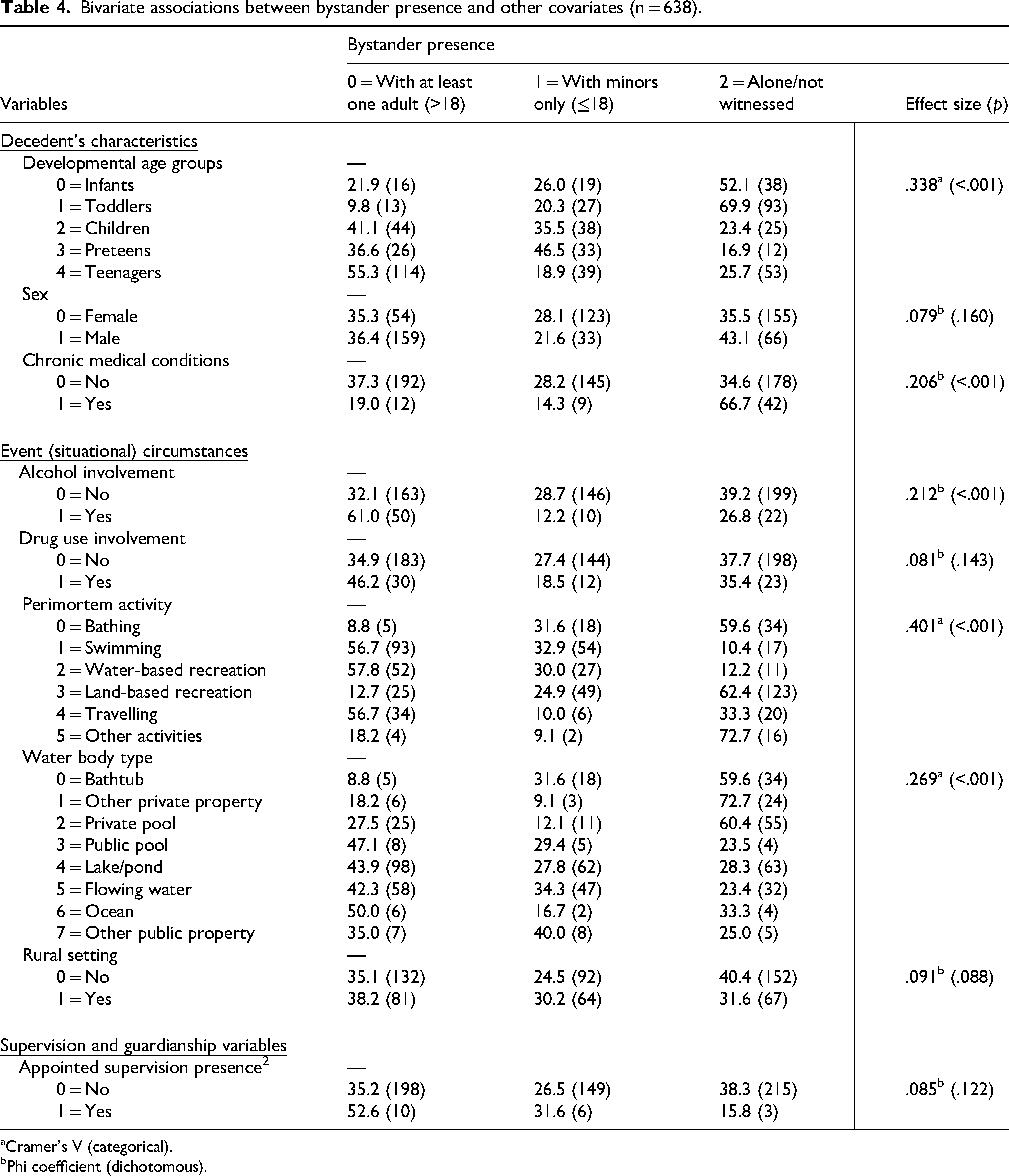
To further test whether it is the case that those drowning in rural environments have diminished bystander presence, covariates were evaluated (Table 4). Methodologically, this study points to the importance of running secondary analyses for model construction by demonstrating that, although factors alone may have an insignificant relationship at the bivariate level, they can become significant contributors to a regression model due to an underlying relationship with the other covariates. While cleaning and recoding these data, it became clear that Lifesaving Society has done a remarkable job in petitioning each province's coroner and medical examiner system to collect valuable information. These fields should be federally mandated, to ensure that the right types of information are being collected in a systematic and consistent manner across provinces. For instance, there is no federally mandated requirement for coroners or medical examiners to provide latitude and longitude data of the point of entry and point of recovery for such deaths. Having this information, particularly in open water environments, would offer very valuable spatial information that can be applied to identifying structural hazards and areas for improvement. More specifically, knowing the exact points of entry would allow for critical environmental assessments and better targeted intervention measures.
Bivariate associations between bystander presence and other covariates (n = 638).
Cramer's V (categorical).
Phi coefficient (dichotomous).
A federally mandated system for data collection would ensure long-term, cross-comparisons are possible. At face value, it appears that a lot of the rescue and recovery data in Canada exist in silos and are closely guarded by the presiding agency, whether that is the police, coroners or medical examiners, rescue societies, emergency management systems, or hospital pathology departments. Although some of this information is shared with death investigators, the type and amount of information shared is not consistent across every Canadian province and territory. This fragmentation makes it particularly challenging to identify which factors could improve survivability at different points of the incident timeline. For instance, it is currently difficult to evaluate whether delayed drowning could have been reasonably avoided if access to emergency medical services was improved. It is also unclear whether the length of time or distance between drowning incidents and health providers could have made a difference in such accidental drowning deaths. It is imperative that better sharing agreements are implemented for drowning prevention research.
Research on non-fatal drownings and effectiveness of existing drowning prevention programming continue to be an important endeavour. Without information on successful rescues, it is not possible to fully capture rescue likelihood, despite the use of fatality data being common place for such research. We believe that by examining other sources of data in future studies, we may be able to better grasp risk and what moderating factors may exist. For instance, a future study using lifeguard rescue data should further delineate their usefulness in thwarting fatal drowning incidents, and hospital intake data should help identify the true rates of drowning because these records can be a source of non-fatal drowning information. Quebec researchers have demonstrated successful integration of three major provincial databases from coroner, emergency departments and hospitals, each containing different fields of clinical and administrative data, 17 a model that can be emulated in other jurisdictions. Moreover, it will be important in coming years to assess the impact of remote, automated surveillance technology in open water-spaces, particularly the application of optical sensor artificial intelligence in detecting distress in water.
The Royal Life Saving Society of Canada's position is since drowning is silent and can happen in seconds, it is the parents and caregiver's responsibility to keep their eyes on their children and to be within arm's reach. Our research shows that even if there are other adults present, they may not be qualified and capable guardians. There are both developmental and sociological differences in how society treats and views youth in different age groups, with greater emphases for a need of care for those that are younger. Our results show that teenagers, despite being older and more physically capable, are at great risk of not being rescued should alcohol be involved, and simply being around others (adults and minor peers) provides an insufficient buffer. There are many benefits to early enrolment of toddlers in aquatic training for water familiarization, parents should remain vigilant because even if toddlers learn how to float or turn-over, they may not yet have the cognitive ability to recognize when they should do so – it is important to not give caretakers a false sense of security. 18
Both children and parents would benefit from the acquisition of water safety knowledge, and it is insufficient to offset caretaker duties to bystanders, as they may not be vigilant or capable of performing the duties of a guardian. A more effective preventative measure would be to focus on removing guardian distractions, promoting active attention, and ensuring that the caretaker is within arm's reach. Additionally, it is important to focus on targeting preteens for water safety training because their water-based incidents frequently occur in the presence of only their peers, who might not reliably be able to serve as capable guardians. Training through Lifesaving Society's Swim to Survive + (Plus) programmes incorporates both water safety, swimming, and assist-specific skills, such as deploying ring buoys for rescues and how to coach their friends in distress. 19 Developmentally, there is literature to suggest that preteens and teenagers are more likely to engage in risk taking behaviour, as a natural stage of maturation.20,21 Lifesaving Society programmes are also offer a wide array of water-safety and first aid programming, including the Junior Lifeguard Club, Swim Patrol and Bronze medals. 22
We expected to find that the presence of bystanders would increase the likelihood of rescue, with adults having a greater effect than minors. Shockingly, this was not the case; bystanders cannot be assumed to be capable guardians. The shift from community-shared responsibility over children's welfare to an individualized one also speaks to changes in society that need to be considered. Greater attention must be placed on creating safe environments, and training that can help facilitate both a parent and bystander's ability to intervene, particularly in open water spaces where sightlines can be obstructed. It is clear from this research that enhancing guardianship efficacy and the implementation of better safeguards are essential to improving the likelihood of a rescue during drowning incidents, and this is necessary for ensuring the safety of youth.
Footnotes
Acknowledgements
The authors would like to thank the many Lifesaving Society volunteers and members involved in collecting data from each coroner and medical examiner office in Canada over the years. Without their tremendous effort, this research would not be possible. The authors would also like to thank Dr. Robert Krausz for his statistics instruction and troubleshooting support.
Ethical considerations
Joint ethics approval between Simon Fraser University and Lifesaving Society was granted (SFU-2018s0742).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vienna C. Lam is supported in part by funding from the Social Sciences and Humanities Research Council Joseph Armand Bombardier Canadian Graduate Student Doctoral Award (767-2018-2671).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Please contact the Canadian Lifesaving society for these data. Due to the sensitivity of this information and with respect to the deceased, this information cannot be uploaded to an open public data repository.