
Abstract
Many people are living in prison with a range of social care needs, for example, requiring support with washing, eating, getting around safely, and/or maintaining relationships. However, social care for this vulnerable group is generally inadequate. There is uncertainty and confusion about who is legally responsible for this and how it can best be provided, and a lack of integration with healthcare. We used realist-informed approaches to develop an initial programme theory (IPT) for identifying/assessing social care needs of, and providing care to, male adults in prison and on release. IPT development was an iterative process involving (a) an initial scoping of the international prison literature; (b) scoping prison and community social care policy documents and guidelines; (c) full systematic search of the international prison social care literature; (d) insights from the community social care literature; (e) stakeholder workshops. Information from 189 documents/sources and stakeholder feedback informed the IPT, which recommended that models of prison social care should be: trauma-informed; well integrated with health, criminal justice, third-sector services and families; and person-centred involving service-users in all aspects including co-production of care plans, goals, and staff training/awareness programmes. Our IPT provides an initial gold standard model for social care provision for people in prison and on release. The model, named Empowered Together, will be evaluated in a future trial and will be of interest to those working in the criminal justice system, care providers and commissioners, local authorities, housing authorities, voluntary groups, and service-users and their families.
Introduction
There is mounting recognition that social care needs in and on release from prison are poorly identified and that when they are detected they are often inadequately met.1–5 Some people living in prison struggle to dress/bathe, get to the toilet, collect meals, or engage in rehabilitative activities, and some have inadequate help with incontinence and personal hygiene.3,6–8 This is a universal problem 9 and provision largely remains fragmented with many people in prison left underserved.9,10
Moreover, given the increasing number of older people living in prison, the level of social care needs in this setting is increasing not only in the UK but in most high-income countries.11,12
According to international policy, care for people living in prison should equate to that in the community and there should be continuity of care upon release.11,13,14 However, social care in prison has been described as inconsistent or in some cases non-existent, exacerbated by unclear lines of responsibility.11,15 In England, before the 2014 Care Act 16 it was unclear where responsibility lay for meeting social care needs in prison. This meant inadequate support or unmet needs, 17 for example, people with mobility problems unable to shower regularly 18 ; those with incontinence not being provided with pads/clean bedding. 8 The Care Act clarified that responsibility for provision lies with local authorities (LAs), but there is no clear guidance on how services should be delivered, leaving this at the discretion of individual LAs. 19 Adequacy of provision varies considerably between and across prisons and LAs, and no overarching model of best practice has been identified. 19 It is unclear how much the situation has improved since the Care Act's inception and there is evidence of ongoing failings. 6
There are examples of good social care practice in prison settings including sociable activities to overcome isolation of older adults in prison 20 ; ‘light work’ activities for this group 5 ; and well-supported/trained peer supporter systems.10,19,21 While these initiatives are encouraging, there is no consistency or guarantee of equivalence of care for people in prison compared to people living in the community, with inspectors reporting a ‘mixed picture’ despite the Care Act. 10 Advocates are calling for people living in prison to have access to the same level of care as their community-dwelling counterparts,4,20,22 thereby meeting human rights obligations.4,8
Considering the insufficient guidance and inconsistent provision of social care in prisons, we aimed to develop an initial programme theory (IPT) and model for identifying, assessing, and providing for these needs (for individuals meeting Care Act eligibility criteria), with a view to evaluating in a future trial.
Methods
Realist approach and synthesis
Systematic literature reviews are often the first ports of call when informing policy or evidence-based guidelines. 23 Our preliminary investigations found an absence of systematic literature reviews on provision of social care in prison and on release, however, and traditional systematic reviews do not lend themselves to learning from alternative settings or exploring what works, for whom, and why. 24 Therefore, a realist approach and synthesis were adopted to explore the literature in prison and community settings.
Realist synthesis is an iterative, qualitative, theory-driven approach to synthesising qualitative, quantitative and/or mixed-methods data and is appropriate when considering complex interventions across different settings.25,26 It brings together evidence and insights from multiple sources, promotes stakeholder engagement, and optimises learning across policy, disciplinary and organisational domains. 26 Programme theories are sets of assumptions about how and why a programme/intervention contributes to specific outcomes.27–29 A key concept is the context-mechanism-outcome (CMO) configuration: context is the ‘background environment’, and mechanisms are resources created by interventions/programmes, and people's response to them. 30 Realist synthesis can explore insights from a diverse range of material including policy documents/guidelines/grey literature whereby insights may include authors’ interpretations/recommendations, and helps us to understand how interventions might work and why (rather than simply ‘does it work?’).30–32
As recommended by the RAMESES (Realist And MEta-narrative Evidence Syntheses: Evolving Standards) group, we adopted an abductive reasoning approach: information gathering and synthesis were iterative processes involving continual reviewing/refining to facilitate and fine-tune our evolving IPT.28,30
Research questions
What works for social care in prison and on release, in what circumstances, and why?
What works for social care in the wider community, in what circumstances, and how can this be translated into prison settings?
Process
The overall process for developing and refining the IPT, including development of the search strategy, was multi-staged. Each of these stages is summarised in Figure 1 and described in more detail below.
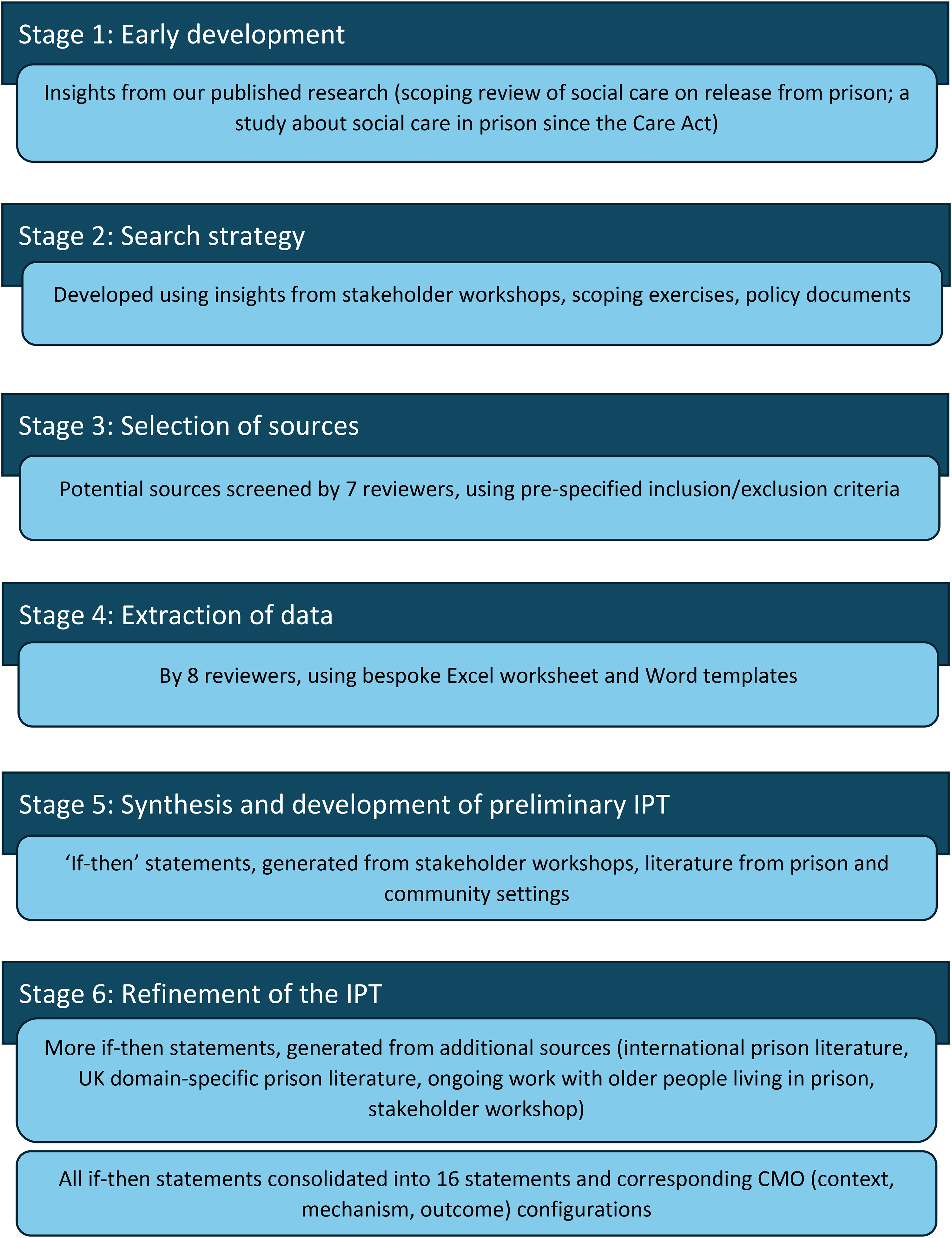
Multi-staged process for developing and refining the IPT using a realist synthesis approach.
Stage 1: early development of IPT
We began developing our IPT based on findings from our previous research including a scoping review of social care on release from prison 33 and a study about social care in prison since the Care Act. 19 These provided an initial structure for our IPT, focussing on four aspects of social care: identification, assessment, provision in prison, provision on release.
Stage 2: literature search strategy/process
In line with the realist approach,30–32 the search process involved several stages to inform, develop and refine the search strategy before conducting a full systematic search. This included stakeholder workshops, scoping exercises, and examination of key policy documents. We also examined specific aspects of the literature identified as important by stakeholders, namely literature concerning strengths-based assessment approaches and community good practice. Full details of the overall process are included in Table 1. Lists of the search terms used are provided in Supplementary Table S1. Snowballing methods 34 were used to identify additional sources.
Iterative process for developing initial if-then statements and preliminary IPT framework, and refining IPT framework.
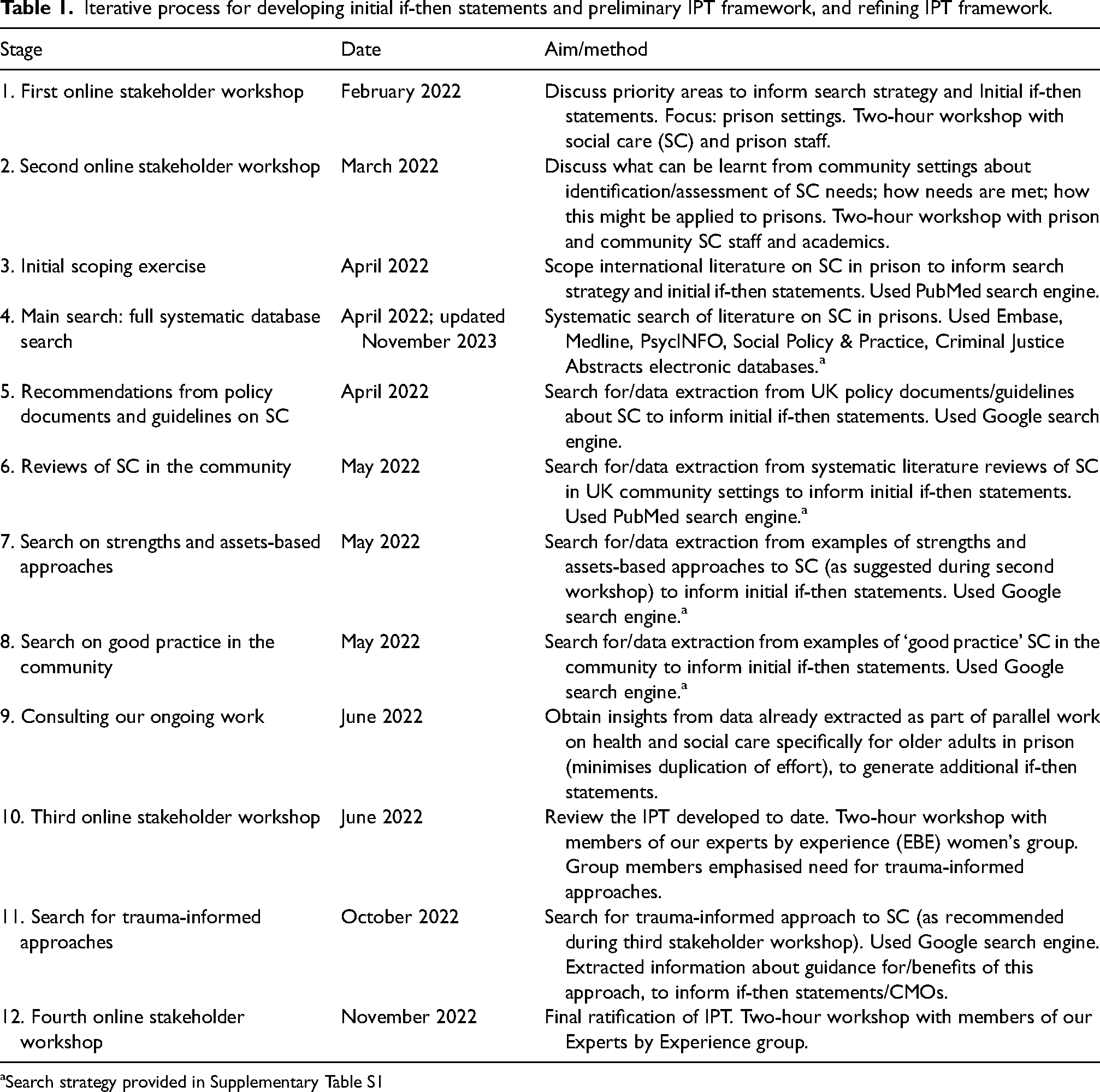
Search strategy provided in Supplementary Table S1
Stage 3: screening/selection of literature
Articles were screened by abstract/title by seven reviewers using pre-specified inclusion/exclusion criteria (Supplementary Table S2). In total, 20,975 records were retrieved and 189 were retained. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (flow diagram (Figure 2) displays full details of the sources and numbers of records retrieved/retained.
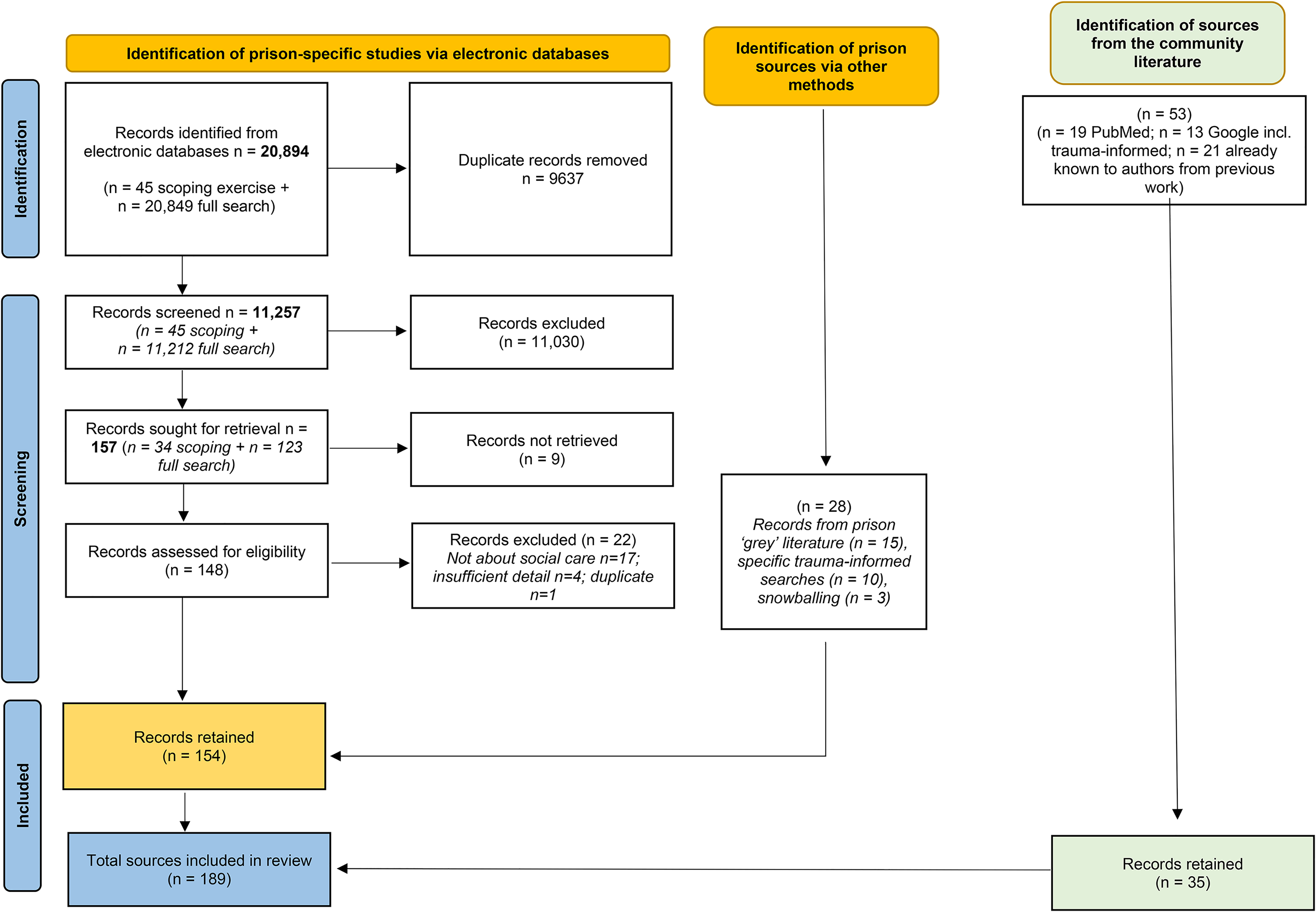
PRISMA flow diagram.
Stage 4: data extraction from literature
Data extraction was conducted by eight reviewers using bespoke Excel worksheet and Word templates. Information extracted included the population/sub-group, stages reported (e.g., identification/assessment/provision/release), type of social care, findings, examples/facilitators of good practice, and author recommendations. Data extraction templates are provided in Supplementary Table S3.
Stage 5: synthesis and development of the preliminary IPT
The preliminary framework for the IPT (Supplementary Figure S1) was informed by if-then statements which were generated from a variety of sources including stakeholder workshops and literature from prison and community settings (full details are provided in Figure 3). If–then statements help structure ideas and identify how an intervention might be linked to outcomes. 25 Insights for these ‘scenarios’ can be gleaned from any section of the document. Generation of initial statements involved theorising how particular ‘resources’ (e.g., life skills training) may result in particular outcomes (e.g., successful reintegration). The statements were organised by theme into a single word document. This ‘working’ document was refined over several iterative steps through team discussions and updated during subsequent stages of IPT refinement (see below). The final version contains all statements, CMOs, and ‘nuggets’ of information, 29 together with sources/references, and forms Supplementary File S1.
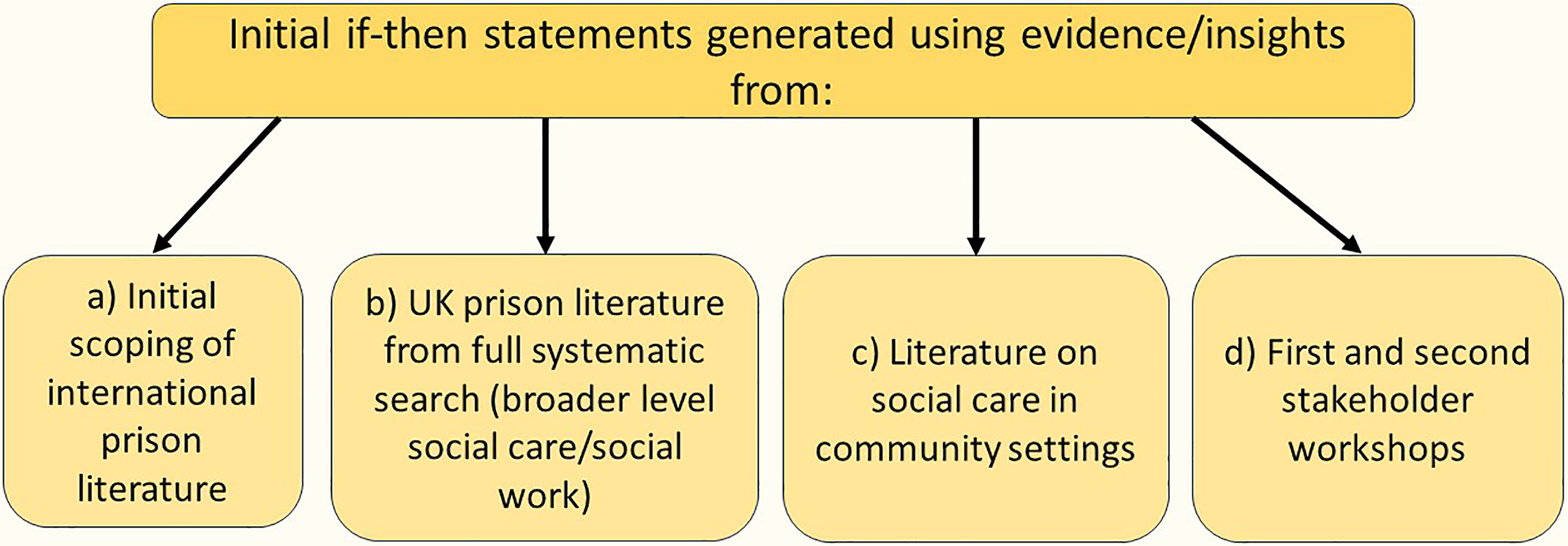
Developing the preliminary IPT - summary of the research process.
Stage 6: refinement of the IPT
Further if-then statements were generated based on additional sources as outlined in Figure 4. In total, 263 if-then statements were generated alongside 245 additional ‘nuggets’ of information (Supplementary File S1). Together with the initial statements, these were reformulated into 16 consolidated statements over several iterative steps to produce richer, more detailed accounts while minimising overlap/repetition. 35 We used these 16 statements to develop 16 corresponding CMO configurations, theorising about expected responses to proposed interventions/resources. The theoretical elements were based on evidence/insights from the literature and reviewers’ hypotheses and were discussed/refined by the team as part of the iterative process, with mechanisms subdivided into ‘resource’ and ‘response/reasoning’ components. These help to explain how resources work to change individual or group reactions/reasoning which achieves the outcomes.36,37 After several further phases of CMO development, including creative mind-mapping sessions with the review team and reflecting further on the data, we distinguished three categories of CMO as outlined in Figure 5, and 11 CMOs concerning identification, assessment, provision, and release which were combined into four consolidated CMOs.
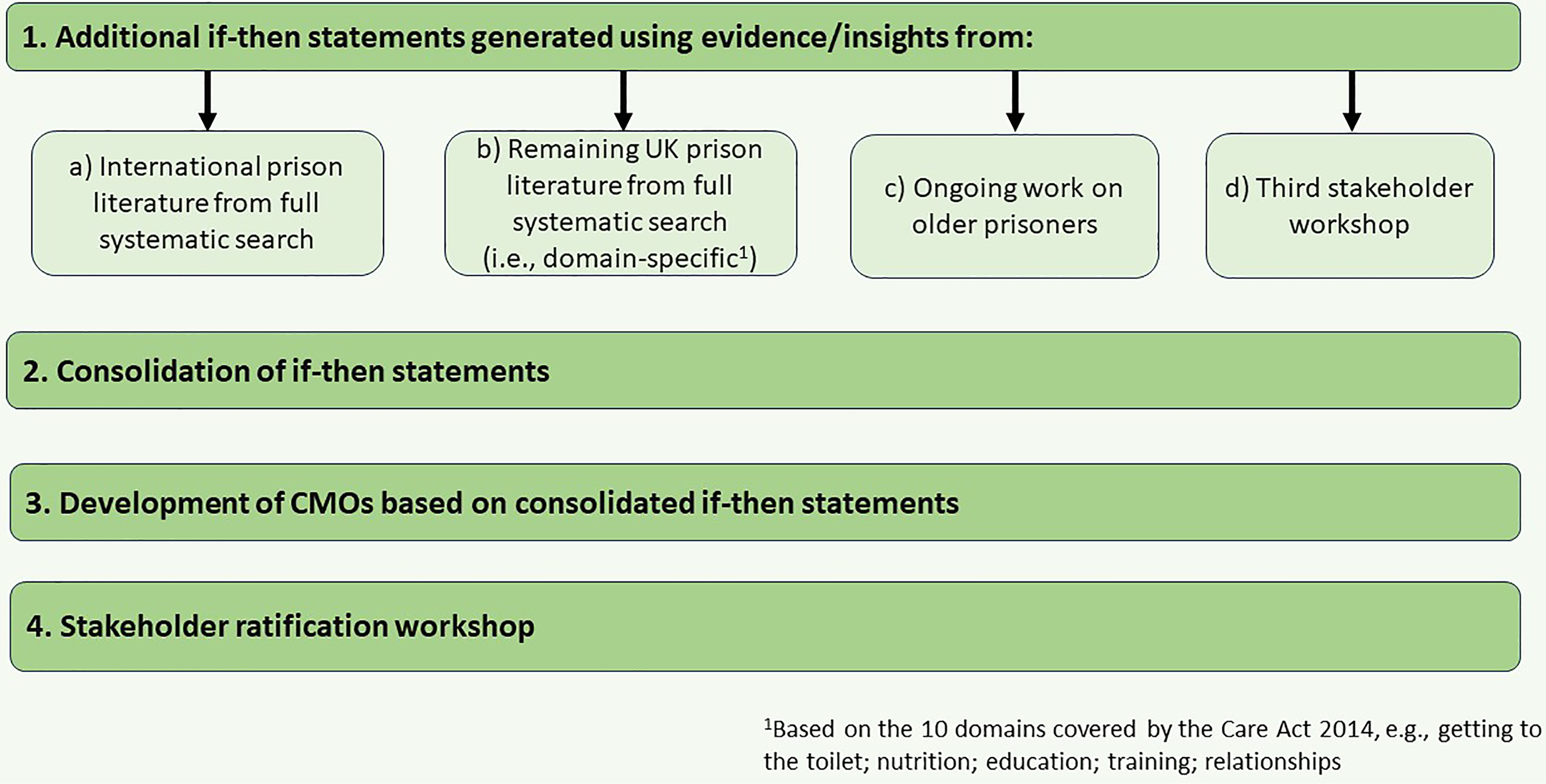
Refining the IPT - summary of the research process.
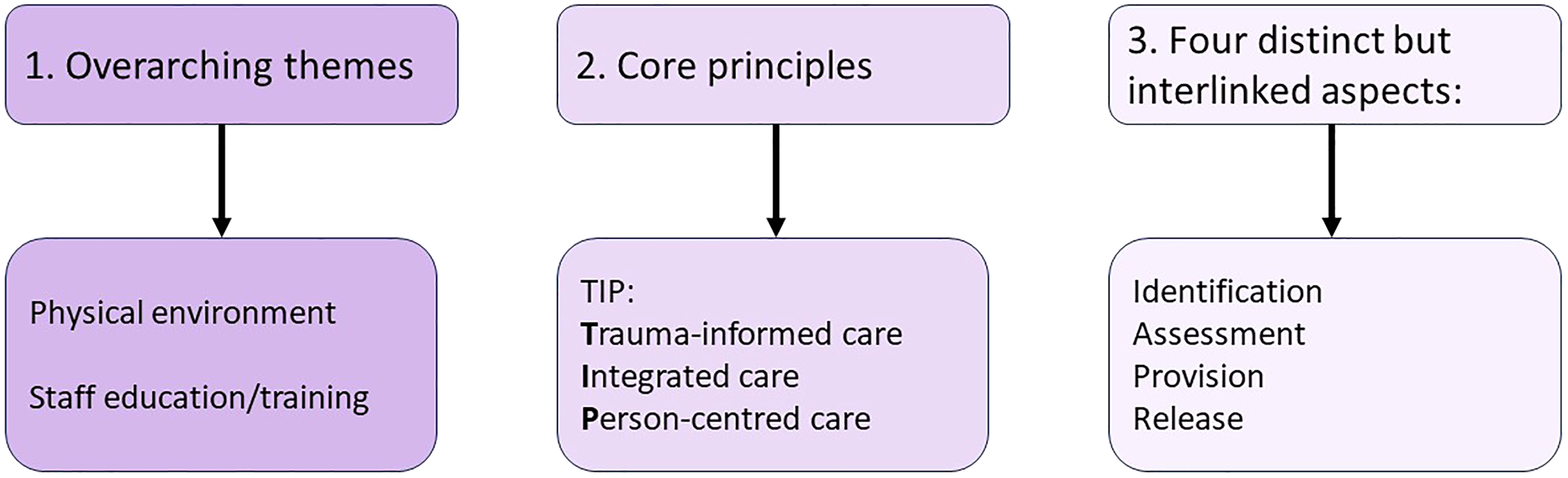
Three categories of CMO guiding the IPT.
Results
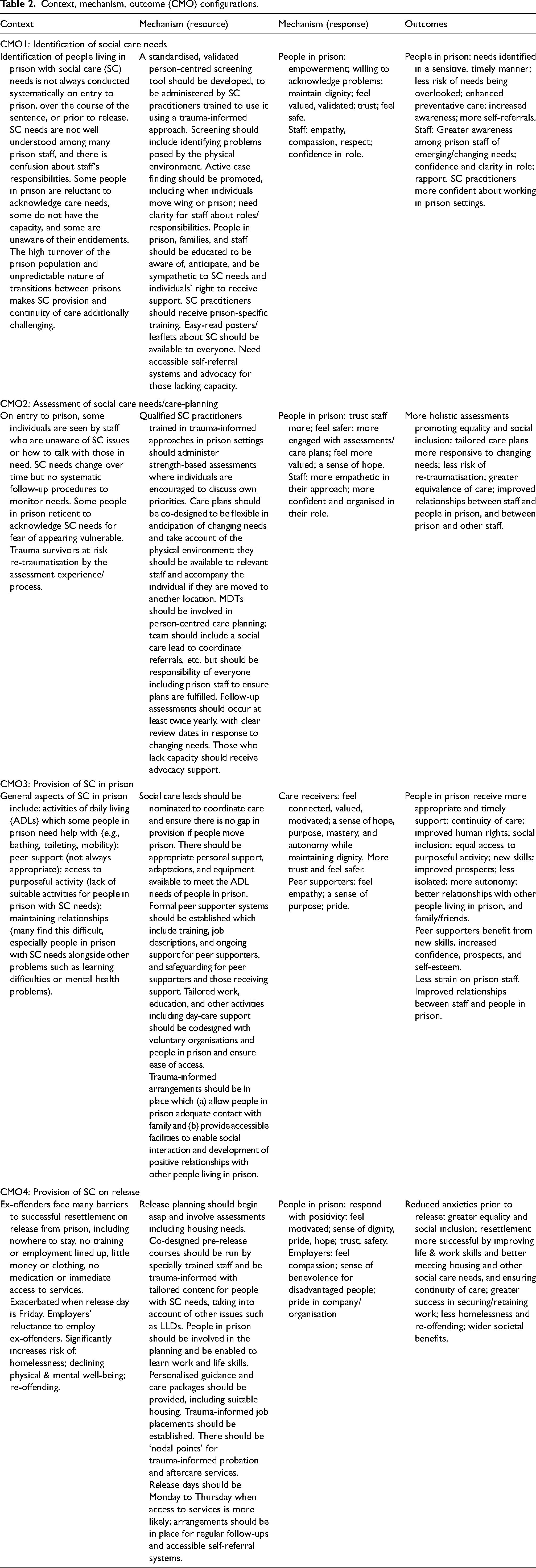
This section presents a narrative summary of the four consolidated CMOs, which are outlined in Table 2 and visually in Supplementary Figure S2. Thus, this section encompasses a description of the model of social care that our expert-by-experience group has named ‘Empowered Together’. An extended version of the findings is available (Supplementary File S2). The content of the CMOs is based on evidence and insights from sources as described In the Methods. The complete list of if-then statements, CMOs, and ‘nuggets’ of information are included in Supplementary File S1.
Context, mechanism, outcome (CMO) configurations.
Identifying social care needs
Before social care needs can be addressed they need to be identified on arrival and, for emerging needs, at any point during an individual's stay in prison.
A key resource needed to ensure accurate and timely identification of needs is a standardised but flexible, person-centred screening tool capable of detecting ‘harder to see’ needs. This should include open-ended questions, enabling/encouraging individuals to acknowledge difficulties they have with mobility, self-care, relationships, or other elements of social care, with social care practitioners trained to screen in a sensitive, trauma-informed way. The identification process should include screening for mental health problems, learning difficulties, dementia, mild cognitive impairment, and trauma alongside general health and social care needs.
Active case finding is fundamental to ensure social care needs are identified, particularly those that may not be apparent on arrival from the community or when individuals move to a different prison. This should involve repeating the formal identification process twice yearly after arrival and enabling suitably trained staff to proactively talk to people, asking questions about their ability to get around safely, take care of themselves, and participate in activities, with a robust route into assessment. This should involve liaison between care staff and prison officers who may identify/refer people with additional support needs if these become apparent.
The identification of social care needs must happen within an integrated care system which includes clarity for staff about respective roles/responsibilities. Awareness of issues relating to social care is vital for this to work. While all people living in prison, their families, and staff should be educated about social care issues, staff should receive formal training to recognise/understand these needs, drawing on the tenets of equality, diversity, and inclusion. Training programmes should be co-designed with people with lived experience of prison and voluntary organisations, further promoting person-centredness and ensuring pertinent issues are addressed. While some social workers receive training around social work in prisons, many do not feel suitably equipped or confident to work in this setting or with particular groups such as people with substance misuse problems. Well-advertised, accessible self-referral options should be available together with user-friendly informational posters/leaflets, such as ‘The Care Act and You’ leaflet, with the option of advocacy to ensure the information is understood by the individual or, where necessary, make decisions on their behalf.
Assessing social care needs
Individuals should be empowered to be actively involved in their assessments and in co-designing care plans, which must be timely and take the limitations of the physical environment into account. Care plans should be available to relevant staff and accompany the individual if they are moved to another location. Advocacy should be offered to people with insufficient capacity to meaningfully participate in their assessments/care plans. Advocates could be informal and internal to the prison (peers, prison staff, healthcare staff) with the person's consent, or formal independent advocacy services including LAs or other staff who must be approved by the LA (e.g., the third sector). All staff should be educated about trauma-informed approaches. The assessment process itself will be traumatising for some individuals, so formal assessments should be conducted by suitably qualified practitioners.
Strengths and assets-based approaches to assessment and care-planning focus on people's capabilities, explore help available from wider support networks, and take account of issues of importance to the individual. Care needs change over time, therefore regular follow-up assessments should be conducted, with changes to care plans being jointly agreed. It is important that everyone has user-friendly information about social care rights and the option to self-refer in response to changing needs.
Provision of social care/support
To optimise social care in prisons it is vital that collaborative, integrated working is implemented whereby prisons, LAs, healthcare, social care, and voluntary organisations develop joint working arrangements with multidisciplinary teams (MDTs), co-designed goals, shared aims, and agreements on information sharing. Pivotal to this is the nomination of a social care lead in each prison to facilitate the co-ordination of care. Social care leads should be embedded within the integrated care system to coordinate referrals and ensure continuity of care if people move prison. MDTs should be involved in care-planning with the social care lead, but it is crucial that there is clarity regarding roles and responsibilities and that all stakeholders are accountable for implementing these plans, which could be expedited by co-designed memorandums of understanding.
Services should be co-designed with people who have social care needs and experience of living in prison. Tailoring to individual needs, this should include safe access to purposeful activities and fully integrated, meaningful day-care support where appropriate. Support should be available to help people build/maintain relationships with family and peers.
Peer support systems are seen as a major resource. It is evident, however, that peer supporters must be suitably assessed, trained, safeguarded, and supported themselves. Where possible, the peer supporter and support receiver should be matched to take account of cultural, religious, communication and support needs. Training and support for peers could involve third-sector organisations (such as RECOOP), while group peer mentoring programmes could be run by ex-offenders with social care needs. A professional could be employed to support peer supporters who could be encouraged to obtain recognised qualifications. Peer supporters should not be involved in providing personal care.
Individuals should be supported to maintain contact with family/friends, and arrangements made to encourage family visits. This is particularly important for certain groups such as people with learning difficulties. The duration/frequency of visits may be more than the standard amount if this is what individuals want/need to maintain social networks. This could include online visits/video visitations, which should not be a replacement for in-person visits. It is important to ensure facilities within prison are accessible to enable social interaction and development of positive relationships with peers. Accessible activities include tailored clubs and buddying systems. Positive staff relationships are important, particularly for those with no other contacts.
Social care on release from prison
People living in prison should be offered tailored pre-release planning and courses, and planning should begin as early as possible, with the individual's engagement, to enable assessment of predicted needs, and covering, at the very least, housing, training/education, employment, food provision, and social and healthcare. People should be enabled to maintain or learn life skills, with other issues such as language and learning disorders (LLDs) being considered. Courses should be co-designed, trauma-informed, and run by staff who have been specifically trained. Employment training should focus on basic work/life skills. Employment placement programmes should ideally be developed with input from employment specialists. Individuals should be provided with personalised guidance notes prior to release, and a care package (if applicable) and personalised pathway document upon release. A single point of contact should be established for those returning to the community, providing trauma-informed probation, counselling, and aftercare services, continuing-care packages, and joined-up support including suitable housing, employment, and access to benefits. There should be arrangements for regular follow-up and ongoing support, and self-referral options to address changing needs.
Discussion
Summary of findings
Our IPT proposes that social care in and on release from prison should be trauma-informed, integrated, and person-centred (TIP). To effectively identify social care needs there needs to be a standardised but flexible systematic screening tool, alongside active case finding and training to increase awareness. Assessments should be strengths-based resulting in co-produced care plans with advocacy provided where needed. Care should be coordinated by a social care lead. Peer support should be provided where appropriate, by trained, well-supported and supervised peers. Early coproduced pre-release courses should be provided, alongside personalised guidance notes and an identified single point of contact should be provided for individuals with social care needs on release.
Comparisons to the literature
TIP principles are increasingly encouraged in community settings,38,39 and are becoming relatively well-established in the criminal justice systems of the UK and USA. 40 However, in the UK this applies only to high secure male prison estates. 40 Our programme theory/model focuses on social care in and on release from prison and applies to all categories of male prisons. This is important because people living in prison are among the most vulnerable, marginalised and excluded in society. 41 Providing TIP care/support to this group will help reduce inequalities, improve well-being, prevent/delay further social care needs, and improve post-release outcomes.
Reintegration is difficult for most people on release from prison who face challenges such as limited family support, stigma, no employment links, and no stable housing.42,43 These challenges tend to be amplified for people with social care needs. Our IPT offers solutions to these challenges, including skills training, co-designed pre-release courses, and personalised guidance and care packages,4,44–46 set within TIP approaches.
Strengths and limitations
To the best of our knowledge, this is the first realist-informed synthesis to determine how the social care needs of men in prison and on release may be best identified, assessed, and met. Whilst the current study included international literature, sources were restricted to English language: it is possible that valuable insights have been omitted. We acknowledge that the framework is predominantly England-focused but believe many other jurisdictions could take some valuable insights from this. Financial implications were not considered, and while some new or improved services would entail financial input, it is likely that the longer-term benefits from preventative care and more successful reintegration into the community would negate this financial cost. Our IPT does not cover people living in the female prison estate, as it is widely held that many of the social care needs of this group differ to those in male prisons. However, we are currently undertaking a study focusing specifically on this group.
Implications for policy and practice
The need to formalise agreements between LAs, healthcare providers and prison staff for the provision of social care in prison is evident. The Care Act stipulates that this should be in the form of a memorandum of understanding; however, such formal understandings are lacking or poorly implemented. This is the first step for improving social care provision in prisons. The need for a designated prison-based social care lead to coordinate service provision is a further aspect of the management structure that requires implementing to enable the development of effective, integrated prison health and social care.4,10,47 Cultural change is also required to ensure that the principles of trauma-informed, integrated, person-centred care are embedded within health, social care, and custodial organisations.9,48 More pragmatically, thorough screening and active case finding is required to ensure individuals with social care needs are not missed. 19 Strengths-based assessments, appropriate peer support, and coproduced care plans should also be implemented. Finally, to prepare for release, early coproduced pre-release courses, personalised guidance and a single point of contact should also be provided.
Discernible barriers to be addressed include lack of awareness among staff and people living in prison, 49 challenges in training entire workforces characterised by high turnover, 42 silo-working (stakeholder workshop, February 2022), and uncertainty around legal responsibilities, roles and accountability.50,51 How to eventually achieve a ‘gold standard’ will vary between prisons and across LAs, depending on current systems and presence/absence of existing agreements, and the characteristics of individual prison estates. While legislation has clarified who is responsible for social care in England's prisons, provision remains inconsistent and until now there was no proposed programme theory aiming to address this. A strength of our IPT is that it is accompanied by examples of how this may be achieved.
Future research
There is a dearth of empirical evidence relating to models of social care in prison since the introduction of the 2014 Care Act. We have developed an IPT and logic model for social care in and on release from prison, based on available information. The next steps are to implement this systems-level ‘Empowered Together’ model and conduct a feasibility study. The model will need further refinement and customisation for different prison settings before a full evaluation can be conducted.
Conclusion
In conclusion, our IPT provides a sound initial framework indicating how social care in prisons can be developed to achieve equivalence of care while preserving dignity, preventing/delaying deterioration, improving prospects and in the long-term improving outcomes and benefiting the wider community.
Supplemental Material
sj-docx-1-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-1-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-pdf-2-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-pdf-2-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-docx-3-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-3-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-docx-4-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-4-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-docx-5-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-5-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-docx-6-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-6-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Supplemental Material
sj-docx-7-msl-10.1177_00258024241264762 - Supplemental material for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach
Supplemental material, sj-docx-7-msl-10.1177_00258024241264762 for Developing an initial programme theory for a model of social care in prisons and on release (empowered together): A realist synthesis approach by Deborah Buck, Lee D Mulligan, Charlotte Lennox, Jana Bowden, Matilda Minchin, Lowenna Kemp, Lucy Devine, Joshua Southworth, Falaq Ghafur, Catherine Robinson, Andrew Shepherd, Jennifer J Shaw and Katrina Forsyth in Medicine, Science and the Law
Footnotes
Acknowledgements
The authors would like to thank all the participants (service-users, prison and probation staff, and social care practitioners) who attended the stakeholder workshops.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health Research [grant number NIHR202610].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.