
Abstract
Dying in the United States is characterized as: medicalized, depersonalized, high technology, fragmented with frequent transitions among care settings, burdensome to patients and families, driven by efficiency and effectiveness, and lacking in key areas, for example, access to palliative care and adequate pain and symptom treatment. Patients and families are often left with a choice of two extremes: vitalism or utilitarian pessimism (utilitarianism). The Catholic Church, however, rejects both of these extremes, and Catholic social teaching (CST) at end of life focuses on ordinary-extraordinary treatments/means, a culture of life and human dignity, accompaniment and community, and caring for whole persons through the end of life. The Catholic tradition of ordinary-extraordinary means is helpful to guide complex end-of-life decisions, regardless of one's religious beliefs, and offers a middle ground between vitalism and utilitarianism that can inform end-of-life care and decision-making for all patients in Catholic health care. While it does not provide answers, it offers guidance and enables conversations that are crucial for the dying and their families to make autonomous, informed decisions about end-of-life care. It provides an opportunity for the dying to let the care team, loved ones, and decision-makers know what a life with meaning, purpose, and passion is for them—and how they want to live and die. This article will summarize the problem, describe end-of-life Catholic teaching, and discuss how it offers a middle-ground. Arguments for and against vitalism and utilitarianism will be explored, including a discussion of CST's response to those receiving care in Catholic health care facilities who are outside the Catholic tradition and do not believe in the teaching. The last section describes a model of collaborative partnership where local parishes and Catholic health care come together to tackle the challenges of caring for and ministering to the seriously ill and those facing death.
Keywords
Introduction
A report by the Institute of Medicine (2015) characterizes dying in the United States (U.S) as: medicalized, depersonalized, high technology, fragmented with frequent transitions among care settings, burdensome to patients and families, driven by efficiency and effectiveness, and lacking in access to high-quality palliative care and adequate treatment of pain and distressing symptoms. Patients and families are often left with a choice of two extremes: vitalism or utilitarian pessimism (utilitarianism). Vitalism focuses on preserving biological life, irrespective of other values such as loss of dignity, independence, preventing pain, or stewarding resources (CHA ND; D. Kelly 2006, 4–5). Utilitarianism values life for its social usefulness and supports the option to intentionally end one's life when they perceive their life is burdensome, frustrating, useless, or futile (CHA 1993b; Jordan 2017; Kelly 2006, 5–7; Paris 2015; Singer 2003). The Catholic Church, however, rejects both of these extremes, and Catholic social teaching (CST) focuses on ordinary-extraordinary treatments/means, a culture of life, accompaniment and community, and caring for whole persons through the end of life (CHA 1993b; CHA ND; D. Kelly 2006, 6; USCCB ERDs 2018). The Catholic tradition of ordinary-extraordinary means is helpful to guide complex end-of-life decisions, regardless of one's religious beliefs. While it does not provide answers, it offers guidance and enables conversations that are crucial for the dying and their families to make autonomous, informed decisions about end-of-life care (Sullivan 2007). It provides an opportunity for the dying to let the care team, loved ones, and decision-makers know what a life with meaning, purpose, and passion is for them—and how they want to live and die.
Catholic teaching offers a middle ground between vitalism and utilitarianism that can inform and guide end-of-life care and decision-making for all patients in Catholic health care. This article will summarize the problem, describe end-of-life Catholic teaching, and discuss how it offers a middle-ground. Arguments for and against vitalism and utilitarianism will be explored, including a discussion of CST's response to those receiving care in Catholic health care facilities who are outside the Catholic tradition and do not believe in the teaching. The last section describes a model of collaborative partnership where local parishes and Catholic health care come together to tackle the challenges of caring for and ministering to the seriously ill and those facing death.
Summary of the Problem
Dying is a universal and personal human experience. About half of Americans think end-of-life care is fair or poor, and that they have too little control over their own medical decisions at the end of life (Hamel, Wu and Brodie 2017). One's perceptions and beliefs about death and dying are influenced by a variety of factors and experiences. Factors that are important to Americans when thinking about their own death include: (1) ensuring their care is not a financial or emotional burden to their families, (2) making sure their wishes for medical care are followed, (3) being surrounded by loved ones, (4) being at peace spiritually, (5) ensuring their family is not burdened by tough decisions about their care, and (6) being comfortable and without pain (Hamel, Wu and Brodie 2017). At the bottom of the list is living as long as possible. This is a significant disconnect, given the prevalence of aggressive, intensive, life-prolonging treatments and the significant expenditure of resources in the last six months of life (Aldridge and Bradley 2017).
Advances in science and medicine and the availability/deployment of modern medical technology may provide cures and life-saving interventions, may palliate symptoms, or may slow the process of chronic, progressive illnesses. This same technology often results in “technological lives” where the dead are kept alive in the ICU with machines and tubes that may be burdensome and provide no benefit (Bishop 2011, 118). American society is fascinated with the results and efficiency that science and technology offer, and health care professionals also strive for efficiency in their work. The investment by the United States in health care, continued rising costs, estimates of waste, fraud, and abuse, and perceived gaps in quality, safety, access, affordability, equity, and experience warrant efforts in efficiency and effectiveness. Further, the costs (monetary and others) that occur with life-prolonging treatments for chronic illness are staggering (Aldridge and Bradley 2017; Fraser, Encinosa and Glied 2008)). However, efforts in efficiency and effectiveness and use of technology should not be at the expense of other pursuits in health care.
If the drive for efficiency and use of technology results in care that is primarily or solely transactional and leaves little time for goals of care conversations, shared decision-making, and personalized, relational care, then the essence of health care may be lost. This may impact how end-of-life decisions are made. The drive for efficiency and technology in health care may also threaten religious and family traditions that are important at the end of life (CHA 1993a). Technology and efficiency can unintentionally prevent engagement between the patient and others around end-of-life conversations (Hamel, Wu and Brodie 2017). Though patients desire such conversations, challenges remain in providing quality, compassionate end-of-life care that is sustainable and affordable, uses technology for the benefit of the patient, and offers a range of choices. Society, including the Catholic community, has failed to deliver on the promise of excellent, compassionate end-of-life care, resulting in a dichotomy of the extreme choice of vitalism and utilitarianism.
Dichotomous Choices
Most people want to be in control of decisions about their care at every age and stage of life, but fear that they cannot control every decision (Dugdale 2020, 100; Hamel, Wu and Brodie 2017). The dichotomy of end-of-life choices is often described as medical vitalism versus pessimistic utilitarianism (D. Kelly 2006, 4–5; Jordan 2017; Paris 2015; Singer 2003). Physician author, Lydia Dugdale, describes the dichotomy at the end of life as “fight or flight” similar to the biological reaction to fear or threat (Dugdale 2020, 100). Fighting death, or vitalism, often results in highly medicalized dying in an institution with non-beneficial treatments and technology, and the consequent “ethically controversial” conflicts between the interests of patients/families, care team, and society (Bosslet et al. 2015, 1319). The ultimate form of flight or escape from the fear of dying is intentionally ending one's life through physician-assisted death (PAD) 1 (Dugdale 2020, 100). PAD is sometimes described as the solution to the problem of dying badly; however, it is a symptom of the problem (or another example of the problem) of highly medicalized death, that is, the failure to teach and support dying well and provide excellent end-of-life care, so people have confidence in their end-of-life decisions and the care they will receive while dying.
The Church teaches that life does not need to be preserved at all costs and should be focused on the whole person, not just the body: “Without health of the spirit, high technology focused strictly on the body offers limited hope for healing the whole person” (O’Rourke and Boyle 2011; USCC 1981 §IVA1, 12). Likewise, the Church forbids intentional killing or hastening death through PAD (Congregation for the Doctine of the Faith, Samaritus bonus 2020; Sacred Congregation for the Doctrine of the Faith, Declaration on Euthanasia 1980). CST around end-of-life is founded in the rich tradition of the Church, which has always cared for the ill and dying until their death (CHA 1993b, CHA ND). Death is the inevitable outcome of human/earthly life and from death comes eternal life. The Church's teaching on end of life offers a middle ground to the binary extremes that so many find themselves facing at the end of life.
Catholic Teaching on End-of-Life Care
Attentive care for the seriously ill, suffering, and dying is an essential part of the Church's mission. The Church community has long provided “hospitable places of care and comfort for those in need of healing” (USCC 1981 § IIB, 5). The Catholic tradition around end-of-life flows from Scripture, the moral tradition, Magisterial and other teaching documents, and the values of CST (Hamel 2006, 12–14). The Church's role in the founding of the first hospitals/hospices in the fourth century and the formation of religious orders to care for the sick and dying is also part of this tradition that led to Catholic-sponsored health care organizations that continues today (Carney et al. 2017).
Life is a sacred gift from God, and from this principle, flow two obligations: 1) to nurture and support life, and 2) not to harm or destroy life (CHA 1993b; DE 1980). The duty to preserve life, however, is not absolute if it poses excessive burdens without hope of reasonable benefit (John-Paul II 1995). Values from CST and the moral tradition that guide medical decision making affirm that human life is a basic good to be cherished, preserved, and not abandoned prematurely. Dying well with dignity rests on the ideals of living well, caring for whole persons in accordance with their wishes through the end of life, and the loving accompaniment of the community to the end and beyond (den Hartogh 2017; Kopfensteiner 1996). The Church's teaching and decisional framework in the form of ordinary-extraordinary means of preserving life informs and guides complex end-of-life decision-making and offers a middle-ground. The teaching on ordinary-extraordinary means as a moral distinction versus a medical distinction is best codified in The Ethical and Religious Directives for Catholic Health Care Services (ERDs) and has ancient roots and a rich history (USCCB ERDs 2018, Part Five Directives 56, 57).
History and Development of the Ordinary-Extraordinary Means Teaching
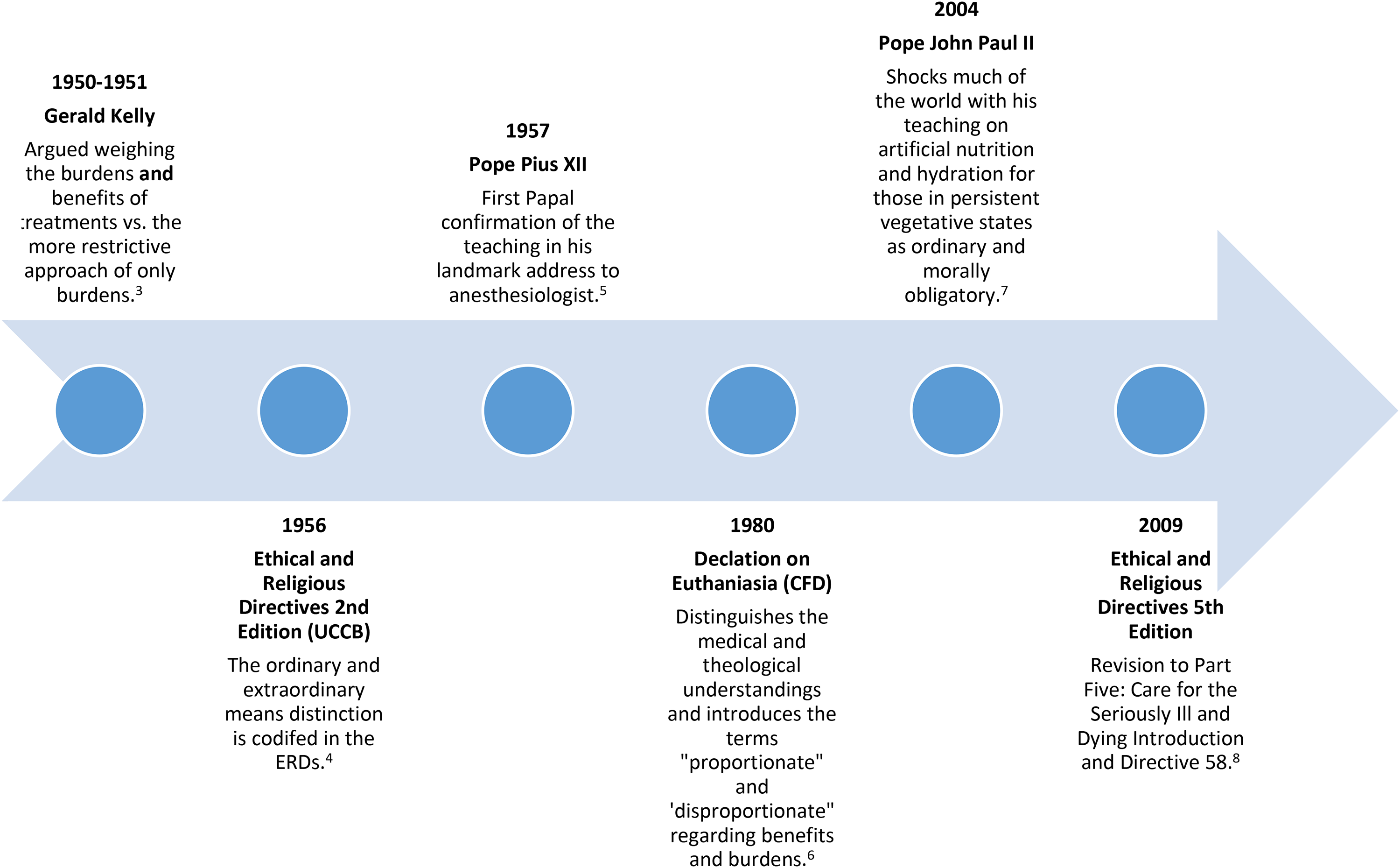
The seeds of the ordinary-extraordinary means were in the writings of St. Thomas Aquinas in the thirteenth century, and further developed the late sixteenth century from three Spanish Dominicans: Francisco De Vitoria, Domingo Soto, Domingo Bañez, and Spanish Jesuit, Juan Cardinal de Lugo (Cronin 1956 1958 reprinted 2011). By the mid-sixteenth century, the ordinary-extraordinary means distinction was established in the Catholic moral tradition, and with the exception of St. Alphonsus Liguori's teaching in the eighteenth century, remained “fairly well standardized” until the mid-twentieth century when it was examined in the context of rapid advances in science, technology, and health care (Cronin 1956 1958 reprinted 2011, 93; G. Kelly 1950; 1951). Significant contributions during this period came from Gerald Kelly (1950; 1951), the Second Edition of the ERDs (1956 in O’Rourke, Kopfensteiner and Hamel 2001), and Pope Pius XII (1957 reprinted 2009). Additional development came from the Congregation for the Doctrine of the Faith in Declaration on Euthanasia (SCDF DE 1980), Pope John Paul II (2004), and a revised Directive 58 in the ERDs (Hamel and Nairn 2010). It has remained unchanged and confirmed by each pope since 2009. Please see Figures 1 and 2 for detailed timelines and contributions in the development of the tradition. Figure 1 highlights the ancient origins and development through the eighteenth century. Figure 2 shows the development from the twentieth century on, highlighting the enduring relevance of the ordinary-extraordinary means distinction.
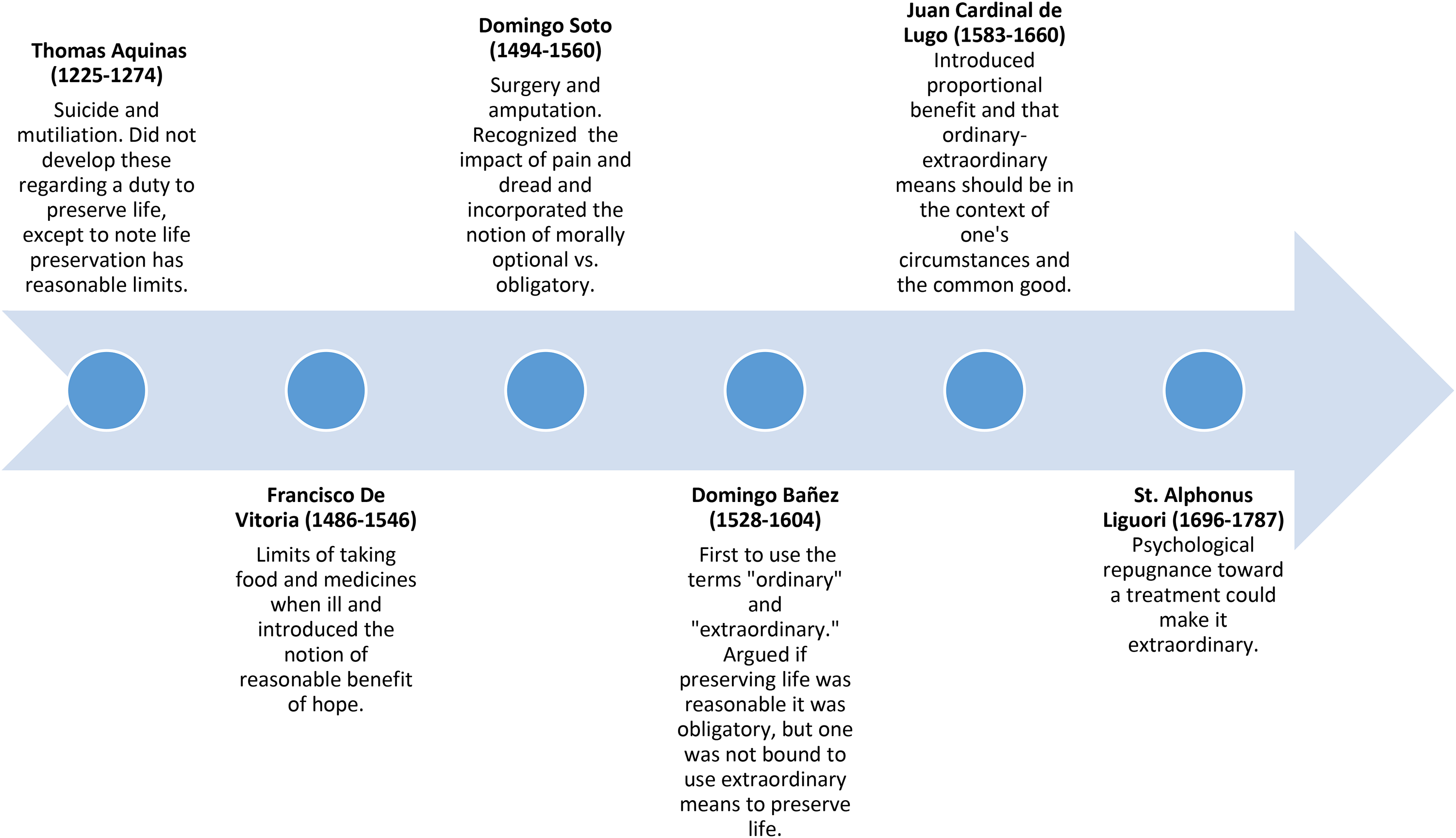
Ordinary and extraordinary means tradition development thirteenth century-eighteenth century. 2
Ordinary means offer significant human benefit in one's pursuit of spiritual goods without disproportionate burden, are morally obligatory, and include four elements: reasonable hope of benefit, common means, proportionate according to status, undemanding means (the difficulty must be proportionate) (Cronin 1956, 1958 reprinted 2011; Henke 2005; G. Kelly 1950, 1951; Panicola 2001; Pius XII 1957 reprinted 2009; USCCB ERDs 2018; Wildes 1996). Ordinary does not refer to medical care that is normal or frequently used; rather, it is used in the context of whether the intervention offers reasonable hope of benefit and is not excessively burdensome. Excessive burdens include something impossible, something requiring great/grave effort or hardship, unbearable/excessive pain, excessive/unreasonable expense, and/or repugnance/severe dread (CHA ND; Cronin 1956, 1958 reprinted 2011; Clark 2006; Henke 2005; Panicola 2001; Sullivan 2007). On the other hand, extraordinary means are morally optional. They promise little significant human benefit in one's pursuit of spiritual goods or impose disproportionate burdens relative to the expected benefit. Forgoing ethically disproportionate life-sustaining treatments (LSTs) acknowledges the human condition, limits of medical science, and finitude of human life—it is not the moral equivalent of euthanasia or suicide (Dugdale 2020; Pope John-Paul II 1995, §65).
The same treatment/intervention can be considered medically ordinary, but ethically disproportionate/extraordinary. For example, antibiotics to treat pneumonia is ordinary medically, but for someone who has terminal cancer with weeks to live, it may be considered morally extraordinary/disproportionate (D. Kelly 2006, 8–9). Likewise, the same treatment/intervention can be ordinary in one clinical scenario and extraordinary in another, depending on the benefits/burdens of each. For example, a ventilator for a reversible, acute, or temporary condition may offer high benefit with relatively low burden and would be considered ordinary (and obligatory); that same ventilator in someone dying from COVID-19 pneumonia or metastatic lung cancer would not produce expected benefit proportionate to the burden and would be considered extraordinary (and non-obligatory) in that case. The ordinary-extraordinary means teaching is useful in navigating the tension between the value of temporal goods and spiritual goods: “The present life is to be treasured, but it is not all there is” (D. Kelly 2006, 5).
The ordinary-extraordinary means distinction as a framework for decision-making clarifies values, priorities, and preferences; addresses questions of meaning and purpose; and supports discerning what one defines as burden or benefit. Understanding these and incorporating them into the care and treatment plan ensures goal-aligned care for whole persons.
Caring for Whole Persons
As a ministry of the Church, Catholic health care is called to restore health (wholeness) to the individual and community through healing (USCC 1981 §IIB, 4). “Health in the biblical perspective means wholeness—not only physical…but also spiritual and psychological wholeness; not only individual, but also social and institutional wholeness” (USCC 1981 §IIA, 4). Treating a disease/condition well but not treating the whole person well is possible. Providing excellent care/cure for a disease or condition but providing bad care at the end of life for the same condition is also possible. Caring for whole persons at the end of life addresses the person's physical, psychological, emotional, social, and spiritual needs and ensures that treatments align with what matters most to patients and families. This results in personalized care that is often less medicalized (Dugdale 2020; Sulmasy and Mueller 2017). The current pressures in health care do not leave much space to enable personalized care for whole persons, as that requires (1) engaging people in conversations around what matters most to them—their values, preferences, priorities, goals, and desires, and (2) shared decision-making that aligns those values/goals with available treatment options to ensure care and treatments are in accordance with the goals and values of the patient/families. If, through efficiency, love and compassion are lost, then the opportunity to care for whole persons may also be lost. The agent for end-of-life decision-making is the individual, and whole person care requires that healing and care for the individual be in the context of the community and its loving accompaniment (Brungardt 2017; Sachs 1991, 9; USCC 1981; USCCB ERDs 2018, Part Five Introduction).
Accompaniment and Community
No one should be abandoned near the end of their life. The trust, love, and support vital for living well is also necessary to die well (Kopfensteiner 1996; Sullins 2014). The Church teaches that illness and dying should take place in the context of the community's accompanying presence that bears one another's illness, suffering, and dying (Callahan 1993; Kopfensteiner 1996). The inherent dignity of human life can only be understood in the context of community with others, which is the heart of the gospel message (Sachs 1991, 10). Accompaniment seeks to reconstitute whole persons so they can discern the existential questions of meaning, value, and purpose of one's life (Brungardt 2017). This has important implications for the individual, the community, and health care.
Stanley Hauerwas (1986b, 82), a Protestant theologian and ethicist, states, “The hospital is, first and foremost, a house of hospitality along the way of our journey of our finitude.” This calls health professionals to accompany and not abandon the ill, suffering, and dying. If the hospital becomes a place of isolation from the community, then this is a failure to ensure that the individual remains constitutive of the community. Catholic health care has a unique obligation to create communities of love and compassion, welcome the communities of patients wherever care is received, be signs of God's presence, bear witness to suffering, and ensure that end-of-life decision-making is in the context of the individual, family, and the community (Hauerwas 1986b, 82; Powers 2013; USCCB ERDs 2018, Part Five Directives 56, 57). Catholic teaching on end of life is normative and theological, and it offers insights, wisdom, and a middle ground for all who are discerning end-of-life decisions, whether or not they believe or follow the Catholic teaching (McCarthy and Kuczewski 2014).
Catholic Teaching and Those Considering Vitalism and/or Utilitarianism
One could argue that based on autonomy, the dignity of human life, and personalized care where a person's values, priorities, and preferences are to preserve life at all costs or to control when one dies that vitalism and utilitarianism are options. Fear of the unknown of the dying process, lack of decisional confidence, a health care system that continues to offer options that are non-beneficial and places autonomy as a preeminent value, and parishes that do not teach, preach, and minister to their parishioners around end-of-life care and decisions ensure that PAD is growing in acceptance, and vitalism is alive and well in American culture.
Arguments for and Against Vitalism
The primary argument for vitalism is the duty to preserve the inherent dignity of human life as a sacred gift from God (USCCB ERDs 2018, Part Three Directive 23). Those considering this extreme often fear that forgoing LST is ethically the same as intentionally ending one's life, or that the clinical team will give up on them (Coulter, Snider and Neil 2019; D. Kelly 2006, 5). Arguments against vitalism include that: (1) the duty to preserve life is not absolute, (2) forgoing LST is ethically distinct from intentionally ending life and does not mean no treatment—ongoing compassionate care will be provided, (3) the primary focus on the biologic in vitalism is inappropriate in that it does not ensure care for the whole person, (4) while patient wishes are important, their discretion is not unlimited, (5) the costs of vitalism, e.g., economic, family caregiving, resource utilization, and distress (physical, emotional, moral) in patients, families, and professionals warrant consideration, especially if it limits access to another's ordinary means, (6) there are limits to human life (human finitude) and medical science, and (7) for believers, this earthly life is not all there is—eternal life comes from our death (Daly 2013; Kearns, Emmerich and Gordijn 2020; C. Kelly 2019; McCarthy and Kuczewski 2014; SCFD 1980; USCCB ERDs 2018).
Arguments for and Against PAD
PAD is legal in ten countries, including the United States in eleven states (Death with Dignity 2021; ProCon.org 2020). The primary reasons for requesting PAD include loss of autonomy (91%), inability to engage in activities that make life enjoyable (89%), loss of dignity (68%), loss of control over bodily functions (48%), and burden on family and friends (41%) (Emanuel at al. 2016). Only 25% expressed concerns about pain or control of pain (Emanuel et al. 2016). Public and physician support for, and legalization of PAD have increased over the last two decades; however, PAD is utilized rarely and mostly in patients with cancer (Emanuel et al. 2016; Hetzler et al. 2019; Quill and Brody 1996).
Those in favor of PAD argue: (1) it is an act of compassion as some patients will benefit from death (an end to pain and suffering when death is evitable), (2) there is no ethical or moral difference between PAD and withholding or withdrawing LST, and the overall intent between the two is the same, (3) there may be cases of pain that cannot be relieved, and (4) the preeminent values of liberty and autonomy (Brock 1992; Emanuel 1994; Goligher et al. 2017; Hardwig 1997; McKhann 1996; Quill, Cassel and Meier 1992; Rachels 1975; Rodriquez 2001; Singer 2003). Proponents argue medical or physician aid in dying is distinct from suicide, assisted suicide, or euthanasia, and with proper safeguards it is a safe medical practice (Compassion & Choices 2018; Death with Dignity 2021; Statement of the American Association of Suicidology 2017).
Arguments against PAD are summarized as: (1) the slippery slope, (2) the erosion of trust in the physician-patient relationship, (3) PAD has a different intent than forgoing LST and is ethically distinct, (4) pain and suffering can usually be relieved, (5) the benefit of death is unknown and unknowable to medicine, (6) the goals of forgoing LST are achieved whether person dies or not, whereas the goals of PAD are achieved only if the patient dies, (7) PAD may alleviate biologic pain/physical suffering in the short term, but it may increase existential suffering in the long term, and (8) PAD is the opposite of compassion. Compassion from its Latin root means “to suffer with” or “endure with” and is the antithesis of prematurely ending or abandoning life (Goligher et al. 2017; Kuczewski 1998; Sulmasy and Mueller 2017; Traina 1998). Understanding the arguments for and against each extreme provides insight into how patients in Catholic health care facilities—those who believe in the tradition and those who do not—view these issues and how the Catholic end-of-life teaching might appeal to them to consider the middle ground it offers.
Catholic Teaching's Response to the Counterargument
Catholic health care should draw on both its longstanding tradition and American preferences at end of life to engage patients and families in their facilities who do not believe in the tradition and/or may request the extremes. American preferences at the end of life, regardless of beliefs, argue for a middle-ground. Americans do not want to live as long as possible, do not want to expend disproportionate resources or be a burden at the end of life, want a say over what happens with end-of-life decisions, and want to be listened to and understood (Hamel, Wu and Brodie 2017; Lelorain et al. 2012). All human beings seek meaning in life, and the majority of Americans, including atheists, find meaning in family (Pew 2018; Weir 2020). About one-fifth say they “do believe in some kind of higher power”. (Lipka 2019, 2). The majority of religious Americans (94%) believe their physicians should ask about their religious beliefs should they become gravely ill, and 45% of nonbelievers still agree that physicians should ask about spiritual beliefs in grave illness (Ehman et al. 1999). Further, proponents of PAD suggest options for those who live in states where it is not legal that are similar to the ethically permissible middle-ground alternatives offered by CST (Death with Dignity FAQs ND).
The Catholic tradition views dying not as a medical problem, but as a natural part of life that can be meaningful and peaceful (D. Kelly 2006, 5; Callahan 1993). The hallmarks of Catholic teaching at end-of-life are dignity and human flourishing, whole person care, the ordinary-extraordinary means distinction for decision-making, and accompaniment and community. The ERDs inform and guide the choices made in Catholic health care to help address the challenges of vitalism and utilitarianism faced at the end of life (USCCB ERDs 2018).
Catholic end-of-life teaching argues that personalized, compassionate whole person care should be the standard approach to care for everyone at every age and stage of life. Studies show this type of care improves outcomes, increases patient/family and provider satisfaction, and decreases costs and resource utilization (Mittelberger ND; Oshima and Emanuel 2013). Although this approach is not routine in American health care, it is imperative at the end of life to ensure patients have a say in their decisions and focus on what is meaningful for them (CAPC ND; Hamel, Wu and Brodie 2017; Sulmasy and Mueller 2017).
Likewise, Catholic teaching argues that the ordinary-extraordinary means as framework in shared decision-making is broad, flexible, and applicable as a framework for all patients and families to determine disproportionate burdens relative to benefits and allows the forgoing of LST when they no longer offer a reasonable hope of benefit. It ensures autonomy and dignity by weighing relative benefits and burdens of treatments from the perspective of the individual, family, and community—not the specific disease(s) involved. Further, the Church supports advance care planning (ACP) in the form of advance directives and physician orders for life sustaining treatment (POLST) to legally document these wishes and decisions for those who will care for them and for surrogate decision-makers (USCCB ERDs 2018, Part Five).
Catholic teaching also argues that the community to which the patient belongs provides companionship and reassures the dying that they will not be abandoned at the end of life, and they should not seek to end life prematurely to avoid their suffering and natural death. PAD tears the fabric of the community, erodes the flourishing of common good, and negatively impacts family, health care professionals, caregivers, and the poor and vulnerable (Bascom and Tolle 2002; Finlay and George 2011; Goldberg et al. 2021; O’Rourke and Boyle 2011). The companionship of their loving community offers healing presence and allows those at the end of life to experience relationship to self, family, others, community, society, nature, and the significant or sacred—all of which are identified as providing meaning in life for Americans (Brungardt 2017; Pew 2018).
Reassurance that one's life and death have meaning, that they will have a say in their end-of-life decisions, that their dignity will be honored, that they will not be isolated or abandoned, and that they and their family will not suffer unnecessary burdens i.e., that they will not die badly is especially important when facing the end of one's life (Hamel, Wu, Brodie 2017). Only one in three of those who fill the lethal prescriptions for PAD use them—the reassurance from simply having the prescriptions is enough (Death with Dignity FAQs ND). Studies show that empathy, listening, and compassionate care provide reassurance by lowering fear, anxiety, and distress, which results in higher satisfaction in those with serious illness (Lelorain et al. 2012; Puchalski et al. 2014). Requests for either non-beneficial, extraordinary treatments (vitalism) or for PAD (utilitarianism) are typically pursued less when compassionate and supportive care is provided (Bascom and Tolle 2002; Hamel 1998; Sulmasy and Mueller 2017). Patient requests for either extreme are opportunities to explore the beliefs, fears, and suffering of the patient and to thoroughly and compassionately explore all options to address these issues (Bascom and Tolle 2002; Goligher et al. 2017; Sulmasy and Mueller 2017). Avoiding these discussions or ending them prematurely contributes to the sense of isolation that those who are ill, suffering, and dying experience (Sulmasy and Mueller 2017). Compassionate, high quality end-of-life care takes time and reflection and does not occur often enough; however, failing to provide such care may drive patients to one of the extremes (Death with Dignity 2021; Dugdale 2020; Sulmasy and Mueller 2017).
Although the Church's end-of-life tradition is distinctly Catholic, its appeal and application in Catholic health care is not reserved for only those who identify as Catholic. Several models of care for the dying exist that resonate with all patients and families, regardless of beliefs. Notably the tenets and principles of these align closely with the Church's teaching around end of life. These include the medical specialties of palliative care and hospice, the American College of Physicians’ model of compassionate care to those at the end of life, and a Catholic model offering a better approach to care for the dying (CAPC ND; Hamel 1998; Powers 2013; Sulmasy and Mueller 2017). See Appendices 1–3 for more detailed descriptions that show similarities between the models and alignment with end-of-life CST.
Providing high-quality, compassionate end-of-life care should be a priority for all health care organizations, but Catholic health care as ministry of the Church has a special duty to do so (USCCB ERDs 2018). By partnering with other Catholic ministries, for example, parishes, Catholic health care can ensure excellent end-of-life care and decision-making, which is more effective when faith communities and health care partner (Hamel 1998). Engaging religious communities in conversations about death and end-of-life care provides an opportunity for these conversations to occur earlier and within the context of religious and ethical teaching and spiritual support from the community; however, this may be insufficient to resolve the problem. Patients who have high spiritual support from religious communities tend use hospice less, have more aggressive end-of life care, and die in the ICU more frequently (Balboni et al. 2013). However, those with high spiritual support from religious communities who also received spiritual support from the medical team and an end-of-life conversation had significantly increased use of hospice, less aggressive end-of-life care, died less frequently in the ICU, and reported higher acceptance and spiritual peace in dying (Balboni et al. 2013).
This suggests that resolution of the problem requires both medical care and theology/religious communities, each drawing on the other to complement/reinforce the other. Each is necessary, and neither is sufficient on its own. The challenge to the Catholic Christian community is to mitigate the dichotomy, wherein one need not choose either extreme for their life and death to have meaning.
The Role of Religion/Spirituality in End-of-Life Discussions
Half of U.S. adults say that their religious and spiritual beliefs play a significant role in how they think about their own wishes for end-of-life medical treatment (Hamel, Wu and Brodie 2017). Catholic parishes play a significant role in the local community and the health care ministry and are called to have these conversations with their parishioners (USCC 1981 §IIIC, 8). Catholic parishes and other faith communities ought to develop ministries to the dying and their families that go beyond prayer and the sacraments. Greater education for parishioners and Church leaders in the theological teachings and basic biomedical processes involved in dying is needed. Likewise, hospitals need to provide better spiritual care training for clinicians and optimal spiritual care support to patients, families, and employees. It is not realistic to expect end-of-life care to be the sole responsibility of either the Church or health care; therefore, parishes and Catholic health care together should lead the way to develop models that serve as a source of guidance and support for all those seriously ill and dying. Recent innovative models borne from collaborative partnership between faith communities and health care provide hope for improved care at the end of life.
Enlightening Models/Experiences
A Pew study showed that faith communities can complement health care systems as sources of information and support as people consider decisions for end-of life care (Avellino, Barnett and Goldberg 2017). They studied geographically and theologically diverse religious and health care communities across the United States, and these experiences offer important insights about the role faith communities can play in society to facilitate ACP and end-of-life conversations for all. There were differences in the approach, tools used, and foundational theology in these experiences; however, there were four common themes: (1) faith communities are a natural place for ACP discussions; (2) for people of faith, ACP can be simultaneously a personal, theological, medical, and legal process, and be seen as a gift to their families, an expression of their faith and beliefs, and an opportunity to document their wishes/decisions; (3) most faith communities theologically distinguish between actions taken to directly hasten death (e.g., suicide, PAD, or euthanasia) and the decision to forgo or withdraw LST when death is inevitable; and (4) faith communities are open to a variety of tools and media for ACP (Avellino, Barnett and Goldberg 2017). These experiences provide thought leaders in religion and in health care with examples to innovate and develop similar collaborative models in their own communities.
One such example is an initiative in California, which is a collaboration between the California Conference of Catholic Bishops and the Alliance of Catholic Health Care and their partners (CWPI 2016–2022a). This statewide initiative, “Caring for Whole Persons: Finding Peace and Support During Serious Illness” (CWPI 2016–2022a), began in 2016 and is based on CST about caring for whole persons and accompaniment, which are key concepts that resonated in focus groups (CWPI 2016–2022a; EMC Research 2018–2019). CWPI's aspirational statement states in part, “…we are committed to developing together… a medical and pastoral approach to care that provides alternative[s]…our intent is to create a Church and Catholic health care collaborative model that serves our California parishioners and patients well…” (CWPI 2016–2022b, 9).
This initiative brings together California parishes and Catholic health care to develop tools, resources, guidance, and training programs to develop a ministry focused on the seriously ill and dying in parishes and ensuring compassionate, personalized care in Catholic health care institutions (CWPI 2016–2022a). The parish program (versus health care) launched first in February 2020, with the first trainings in May 2020. A comprehensive toolkit for parish leaders was developed and is available on the website (CPWI 2016–2022b). The toolkit includes an overview of the CPWI, a self-assessment to determine the potential level of parish engagement, and various resources and checklists by tier of engagement (CWPI 2016–2022b). Figure 3 illustrates the CPWI tiers and the training/resources in each tier.
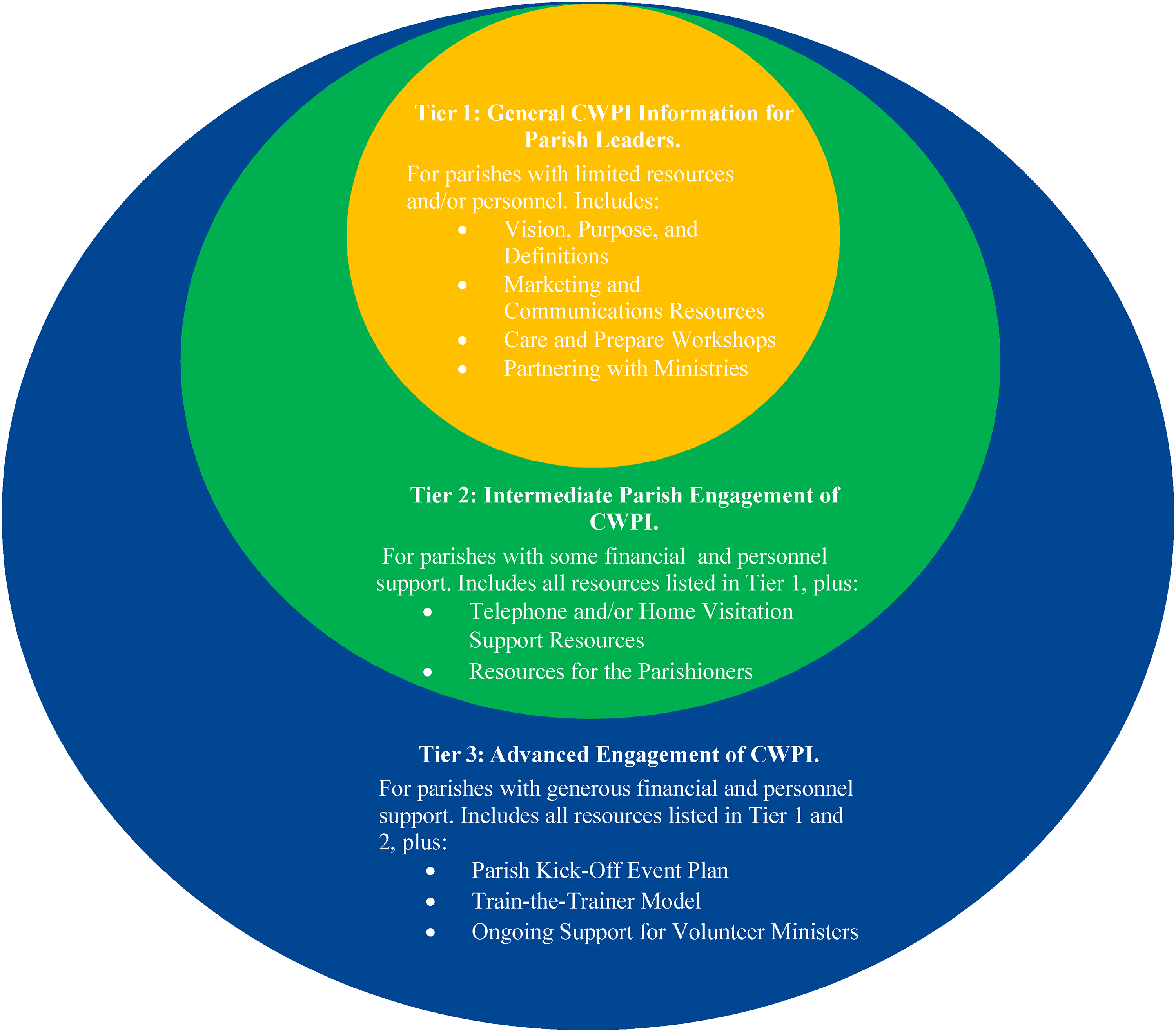
Three-Tiered overview of resources. Caring for the Whole Person Toolkit (CPWI 2016–2022b, 2).
The CPWI education and training curriculum for parishes was developed in consultation with moral theologians, ethicists, and experts within Catholic health care, and deploys a variety of media/teaching methods, e.g., didactic, group discussion, role playing (CWPI 2016–2022a). Figure 4 shows a summary of the modules; Appendix 4 provides more detail on the core curriculum.
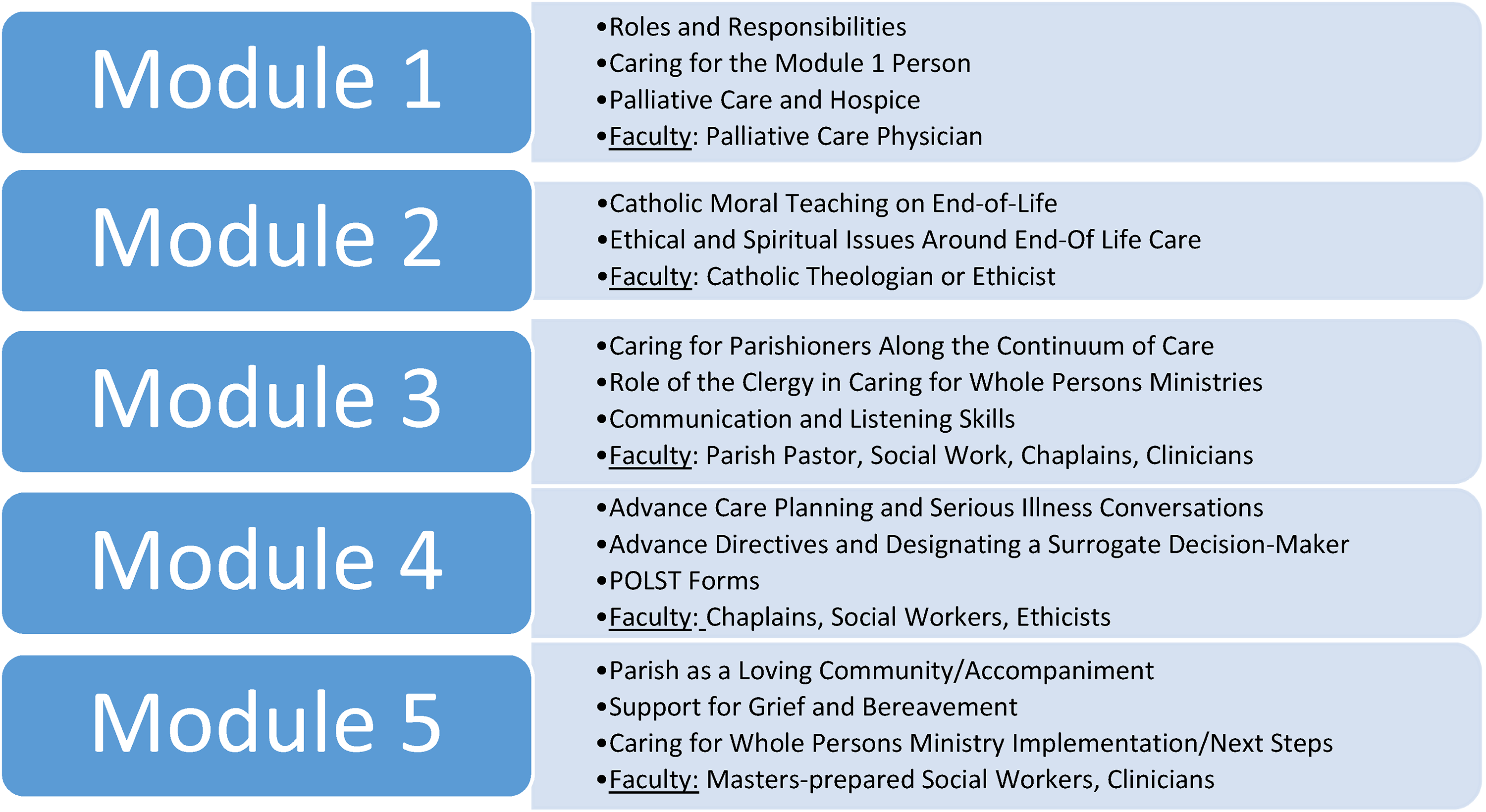
Summary of caring for whole persons Parish education curriculum (CPWI 2016–2022c).
The parish program framework includes (1) one two-hour session weekly for five consecutive weeks, (2) accompaniment training supporting parishioners with serious illness at the end of life, (3) recruiting volunteers to visit and minister to the seriously ill and their families within the parish, and (4) assessing and planning for community needs. Through June 2022, seven dioceses have committed, seventy-five parishes have active CPW ministries, 173 parish leaders have committed, and 444 parish leaders have been trained (CWPI ND).
The evaluations from the training programs are high and note the importance of including both the medical and theological content in the training, as well the value of the parish community to accompany those with serious illness (CWPI ND). A similar modular training and implementation program could be envisioned for Catholic health care, including training for Catholic health professionals on Catholic moral teaching at end-of-life, including the ERDs, whole person care, end-of-life care and decision-making, goals of care conversations, goal-aligned care, shared decision-making, and the role of accompaniment on the journey of human finitude. This model in California holds significant promise in the care of the seriously ill and dying to combine the best of theology and the best of medical science/ health care.
Conclusion
Decisions at the end of life are incredibly complex and often occur far too late in the process. While advances in medical science may allow us to live longer, they create complex decisions for patients and families. Technology and efficiency in moderation are important pursuits to ensure that health care financing and delivery are sustainable; however, when taken to extremes or as sole pursuits, they result in a dichotomy of extreme choices at the end of life: vitalism or utilitarianism. CST provides a middle-ground between these extreme choices as well as a framework that supports excellent end-of-life care and decisions for individuals, families, and communities.
The Catholic community can be a powerful and prophetic voice in serious illness and dying. Drawing on its ancient tradition, it must inform and guide end-of-life care and decisions and teach, preach, and show what it is “for,” rather than exclusively mounting campaigns on what it is against, for example, PAD. Before discussions around PAD occur, the Catholic community must do a better job in demonstrating alternative approaches to serious illness, death, and dying. It must also provide as excellent care to the dying as to those who may recover. Further, Catholic leadership should preach and teach the ERDs to ensure greater understanding of this ancient tradition in the practical application of decisions at the end of life. To the extent that Catholic health care provides mediocre end-of-life care and parishes fail to preach, teach, and minister to parishioners around end of life, the Catholic community is complicit in the growing social and moral acceptance of PAD and the continued prevalence of vitalism.
The Catholic teaching on end of life enables dying well according to our natures that not only brings peace and happiness, but it also happens to be morally preferrable (McCarthy and Kuczewski 2014). Additional study in three key areas will further address some of the greatest ethical challenges posed by the extremes of vitalism and utilitarianism at the end of life and improve the quality of serious illness and end-of-life care for all, regardless of beliefs or sponsorship of the facility: (1) understanding how this tradition might be relevant and more broadly applied in all health care settings; (2) understanding the gaps in awareness and understanding of patients, families, and health care professionals on the role of palliative care and hospice and how to remove barriers to access these specialty services in secular and faith-based health care; and (3) better understanding of the relationship between religion and spirituality and end-of-life attitudes/preferences, especially among those who identify as nonbelievers.
A patient-centered, family-oriented approach to care for the seriously ill and dying resulting in compassionate, dignified, loving, affordable, and efficacious care is achievable through personalized whole person care, access to palliative care and hospice, the accompaniment and healing presence of the community, and good ACP decision-making using the ordinary-extraordinary means framework. By drawing on its ancient end-of-life tradition and developing innovative partnerships between its parish and health care ministries, the Catholic community is uniquely positioned as an antidote to the crisis of dying badly in America—leading the way as a prophetic example of how to honor the dignity of and care for whole persons, and restore, heal, and accompany those at the end of life.
Footnotes
Acknowledgments
The author would like to acknowledge and thank the Neiswanger Institute for Bioethics & Healthcare Leadership, Loyola University, Chicago, most especially Dr. Michael McCarthy for his encouragement, wisdom, guidance, and moral theology expertise in this area of study and Dr. Nanette Elster for her encouragement, keen eye, and for teaching me to be a better writer. The author would also like to thank and acknowledge William Cox, Lori Dangberg, and Edward Dolejsi, their teams, especially Tue Nguyen, and all the partners from the Caring for Whole Person Initiative in California for their vision, leadership, and exemplar model. This article would not be possible without them all.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Biographical Note
Appendix 1. Palliative Care and Hospice
Source:CAPC ND; Mittelberger ND; Powers 2013.
Appendix 2. American College of Physicians Twelve Things Physicians Should Do for All Patients Nearing the End of Life
Source: Sulmasy, Lois Snyder and Paul S. Mueller. 2017, Appendix 7.
Appendix 3. Ron Hamel's Principles for Excellent End-of-Life Care for All in Catholic Health Care Facilities.
Source: Hamel, Ron. 1998, 55–59.
Appendix 4. Caring for the Whole Person Core Curriculum
General overview of the initiative What is Palliative Care and how can I receive that type of care What is the difference between Palliative Care and Hospice Ethical and Religious Directives related to end of life Common Misunderstandings of Catholic Teaching on Ethical Decisions about Treatment How clergy can support parishioners and families towards the end of life Resources from our faith tradition How to support parishioners and families towards the end of life Physical, emotional, spiritual changes and how to address them Physician Assisted Suicide guidelines and how to respond Communication and Listening Skills Boundaries and confidentiality Volunteer Guidelines Overview of Advance Care Planning Advance Directive POLST Misunderstandings about POLST Advance Directive vs. POLST A Day in the Life of a Caregiver Burdens of caregiving Family dynamics around caregiving How to provide emotional support to caregivers What is grief and mourning Stages and types of grief Signs of grief Spiritual care for the bereaved How to manage and maintain a CWP Ministry Recruiting and screening Identifying speakers for presenting Identifying parishioners in need and assigning CWP ministers Documenting and reporting visits Keeping volunteers engaged—ongoing education and support Source: Caring for the Whole Person Core Curriculum (CWPI 2016–2022c). https://wholeperson.care/sites/default/files/2020-09/CWPI%20Core%20Curriculum.pdf. Accessed September 30, 2022.
MODULE 1
Introduction to the (CWPI) and to Palliative Care and Hospice
Faculty: Palliative Care Physician
MODULE 2
Catholic Moral Teaching Around End of Life Care
Faculty: Catholic Moral Theologian or Ethicist
MODULE 3
Caring for Parishioners along the Continuum of Care
Faculty: Parish Pastor, Ethicist, Clinicians, Social Workers, Chaplains
MODULE 4
Advance Care Planning, Communication and Taking Care of Business
Faculty: Chaplains, Ethicist, Clinicians
MODULE 5
Parish as a loving community, Caring for one another
Faculty: Masters-Prepared Social Workers, Project Managers, Chaplains