
Abstract
Alfaxalone is a neurosteroid with anaesthetic effects and it has been used successfully in several animal species. However, there are no data, to our knowledge, about its efficacy and safety in ferrets (Mustela putorius furo). We evaluated a variety of anaesthetic regimens in ferrets, namely, alfaxalone at 20, 10 and 5 mg/kg (n = 1, 10 and 9, respectively; intravenously); medetomidine at 20 µg/kg (n = 3; intramuscularly); medetomidine (20 µg/kg, intramuscularly) plus alfaxalone (2.5 mg/kg, intravenously; n = 7); and tramadol (5 mg/kg, intramuscularly) plus alfaxalone (5 mg/kg, intravenously; n = 2). Two animals treated with alfaxalone at 10 mg/kg and 20 mg/kg, respectively, died. At 5 mg/kg alfaxalone produced anaesthesia with a similar onset but a shorter duration of anaesthesia and analgesia than alfaxalone at 10 mg/kg. The medetomidine–alfaxalone combination produced anaesthesia and analgesia of a longer duration than alfaxalone administered alone at 5 mg/kg (P < 0.0001 and P < 0.001, respectively). Under this anaesthetic regimen, there was a progressive decrease in pulse rate during the first 30 min before the pulse rate stabilized. Respiratory parameters were maintained at acceptable levels. When tramadol was administered, all the animals exhibited a strong excitation reaction and in no case was the toe-pinch reflex clearly abolished. Thus, alfaxalone plus medetomidine provided safe and effective anaesthesia in ferrets. Alfaxalone, alone or in combination with tramadol, did not produce satisfactory results for use as an anaesthetic for this species.
The ferret (Mustela putorius furo) is a useful animal model for biomedical research, and is also a popular pet. For many procedures, such as a complete physical examination, radiography or blood sampling, sedation or anaesthesia is required.
Some drugs currently used for anaesthesia and analgesia in dogs and cats have been used similarly in ferrets, with dosing extrapolated, on occasion, from cat veterinary medicine. 1 However, doses should be specific to the species, without direct extrapolation, because ferrets have a higher metabolic rate, smaller size, and lower body weight than cats.
Inhalant anaesthesia (isoflurane or sevoflurane) is often administered to ferrets. 2 However, the development of safe and effective injectable anaesthetic procedures would enhance ease of administration and environmental and personal safety, without requiring complex equipment. Various parenteral protocols have been reported, including combinations of ketamine and xylazine/diazepam/medetomidine, 1 propofol or tiletamine/zolazepam, 3 all of which have been described as acceptable in terms of sedation and anaesthesia.1,3–6
Alfaxalone has been widely used as an anaesthetic agent in dogs and cats for more than 40 years,7,8 mainly in combination with alphadolone (Saffan®). 9 However, this combination has been discontinued in some countries because of safety concerns in dogs. In cats, this formulation can produce side-effects such as hyperaemia, peripheral oedema and urticaria and, even, death. 10 In both species, these effects seemed to be related to the solubilizing agent (Cremophor EL), a polyoxyethylated castor oil-based surfactant. It has been reported that intravenous injection of Cremophor EL in humans can result in hypersensitivity reactions, mediated by the release of histamine. 11
The more recent formulation of alfaxalone alone (Alfaxan-CD®) contains, as a solubilizing agent, 2-hydroxypropyl-beta cyclodextrin, a chemically modified cyclodextrin that forms reversible complexes with many drugs. This formulation does not induce the release of histamine and it has been used successfully in dogs and cats.12–14. In cats, alfaxalone produces good to excellent anaesthesia, with rapid induction, excellent muscle relaxation, unresponsiveness to noxious stimuli, and smooth, uneventful recovery from anaesthesia. 13 In addition, it has been reported that hypoventilation and apnoea are uncommon at clinically relevant doses, but become the most important adverse effect when larger doses are intravenously administered rapidly. 13 In dogs, alfaxalone anaesthesia has also been judged to be good to excellent, with hypoventilation and apnoea being the most prominent dose-dependent side-effects. 12 Moreover, it has been reported that alfaxalone is a clinically acceptable anaesthetic in dogs with moderate to severe systemic disease. 15
To our knowledge, Alfaxan-CD® has not been widely used in ferrets and there are no data in the literature about its efficacy and safety. The objective of the present study was to assess the effects of alfaxalone in ferrets, alone and in combination with medetomidine or tramadol, and to evaluate the cardiorespiratory effects of the most effective anaesthetic combination.
Animals
Male castrated ferrets, aged 1.5 years and weighing 1.3 ± 0.2 kg (mean ± SD), were used. The animals were not used for any other procedure and were originally purchased from a commercial breeder (Marshall BioResources, North Rose, NY, USA) and housed at the facilities of Almirall SA (Barcelona, Spain) throughout the study. They were kept in polycarbonate double-decker cages (Tecniplast SpA, Varese, Italy), with a basal surface area of 5000 cm2 each. Cages were connected via PVC tubing that allowed the animals to move from one cage to another. The animals were housed in groups with a maximum of eight animals per group and were maintained under controlled ambient conditions (temperature, 20–24℃; relative humidity, 40–70%). The light/dark cycle was 12/12 h: lights were turned off at 19:00 h and turned on at 07:00 h. Care of the animals complied with European Community Directive 86/609/CEE for the use of laboratory animals and local regulations. Experimental procedures were approved by the institutional Animal Care and Use Committee of Almirall SA.
All the animals were examined and weighed at the start of the study and always had unlimited access to water and standard ferret diet (2072 Teklad Global Ferret Diet; Harlan Laboratories, Barcelona, Spain).
Materials and methods
Design of the study
Alfaxalone (Alfaxan®; Vétoquinol, Madrid, Spain) was administered alone or in combination with an alpha-2 adrenoceptor agonist (medetomidine, Domitor®; Pfizer, Madrid, Spain) or an opioid (tramadol, Adolonta®; Grünenthal Pharma, Madrid, Spain). The following anaesthetic regimens were employed and in the following order: (1) alfaxalone alone at 20, 10 and 5 mg/kg (intravenously, n = 1, 10 and 9, respectively); (2) medetomidine alone at 20 µg/kg (intramuscularly, n = 3) or plus alfaxalone at 2.5 mg/kg (intravenously, n = 7); and (3) tramadol at 5 mg/kg (intramuscularly) plus alfaxalone at 5 mg/kg (intravenously, n = 2). The ferrets were randomly assigned to the treatment groups. Each animal received only one anaesthetic regimen; except for eight ferrets, which received two treatments, with at least one month between each treatment.
The initial sample size of each group was estimated by extrapolation of previous studies focused on alfaxalone in other species12,13,15 and/or on medetomidine in ferrets. 1 The final sample sizes were established according to the homogeneity of the results and the severity of the adverse effects, when such effects occurred.
Procedures
The animals were randomly taken from their cages to an adjoining experimental room. The intramuscular administration of drugs was performed via the hindlimb, with injection into the semimembranosus and semitendinosus muscles using a 25 G needle from a 1 mL syringe. For intravenous administration, a small area of the forelimb was shaved with a clipper to provide a clear view of the cephalic vein, which was punctured with a 24 G catheter. When alfaxalone was administered without prior medication, topical lidocaine (Xilonibsa® aerosol 10%; Inibsa, Barcelona, Spain) was applied to the surface of the skin to facilitate the painless insertion of the catheter. One caretaker held the animal firmly but carefully while the veterinarian administered drugs via a 1 to 2 mL syringe. The injections were given slowly, always over the course of more than one minute, to avoid respiratory depression and apnoea. After the injection, the catheter was removed.
When anaesthetics were administered, the following parameters were recorded, starting immediately after administration of the second drug (if more than one was used): time to lateral recumbency; time to regain sternal recumbency; and time to loss and to recovery of the toe-pinch reflex. This reflex was tested at one-minute intervals by pinching the interdigital fold with the anaesthetist’s fingernails. Side-effects, such as unwanted movements, excitation, sialorrhea and apnoea, were recorded. The feasibility of endotracheal intubation was also assessed using a straight #1 blade laryngoscope and an uncuffed 2.5 mm endotracheal tube.
Duration of anaesthesia was taken as the time during which the animals were laterally recumbent, before they regained sternal recumbency. Duration of analgesia was taken as the time during which the toe-pinch reflex was absent.
Monitoring
All the animals that were anaesthetized with medetomidine plus alfaxalone were intubated and attached to recorders of cardiorespiratory parameters.
Once the animals lost toe-pinch reflex, they were intubated and placed on an electric blanket to prevent hypothermia. Body temperature (BT) was measured with an electronic rectal thermometer. The endotracheal tube was connected to a capnograph (Capnomac Ultima; Datex, Helsinki, Finland), which allowed the recording of the end-tidal fraction of CO2 (EtCO2) and the respiratory rate (RR). When swallowing reflex was recovered, the animals were extubated, and from that moment on, RR was measured by watching movements of the chest. For the monitoring of oxygen saturation of haemoglobin (SatO2) and pulse rate (PR), the base of the tail was shaved and covered with an adhesive probe (Nellcor sensor; Covidien, Mansfield, MA, USA) connected to a pulse oximeter (Nonin-8800; Nonin Medical Inc, Plymouth, MN, USA).
After the administration of alfaxalone, all the above-mentioned parameters (BT, EtCO2, RR, SatO2 and PR) were recorded at 5 min intervals for the first 20 min and then at 10 min intervals for another 50 min, except in the case of EtCO2, which was recorded until the animal was extubated.
Statistical analysis
We compared the means of duration of anaesthesia and analgesic effects produced by all the anaesthetic regimens. Monitored parameters were registered every 5 min and compared with the respective baseline values.
Comparisons of means were made by Student’s t-test for normal distributions and by the Kruskal-Wallis test for non-normal distributions. Hartley's f-test for equality of variance was applied. A P value of less than 0.05 (two-tailed) was accepted as evidence of statistical significance.
Statistical analyses were performed with Open-EPI, version 2.3.1 (OpenEpi: Open Source Epidemiologic Statistics for Public Health, version 2.3.1; www.OpenEpi.com) and StatPlus 2007 (AnalystSoft; http://www.analystsoft.com/es/)..
Results
Effects of alfaxalone alone
Anaesthethic effects of alfaxalone and medetomidine, alone and in combination.
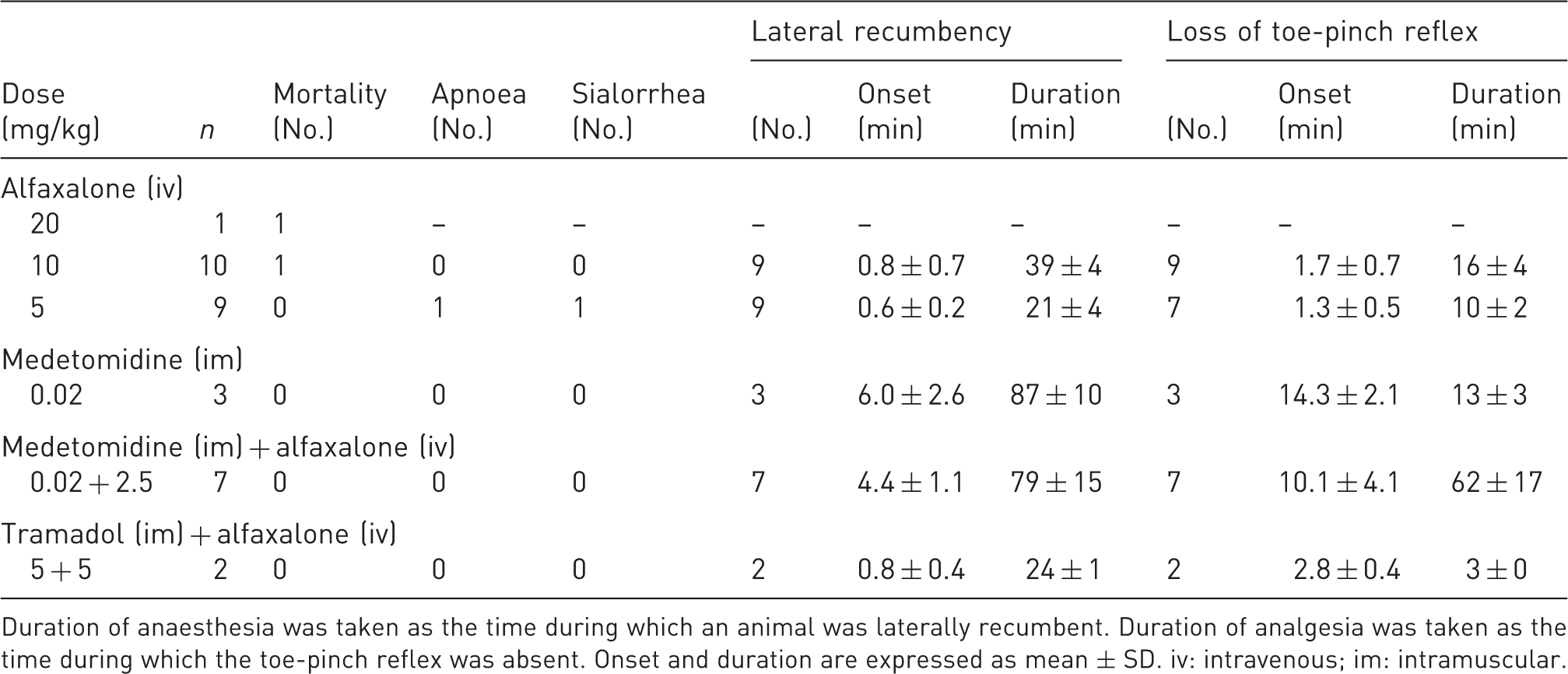
Duration of anaesthesia was taken as the time during which an animal was laterally recumbent. Duration of analgesia was taken as the time during which the toe-pinch reflex was absent. Onset and duration are expressed as mean ± SD. iv: intravenous; im: intramuscular.
In all the animals in which the toe-pinch reflex was abolished, endotracheal intubation was successful, indicating that the swallowing reflex had also been lost.
The duration of anaesthesia and the duration of the analgesic effect produced by alfaxalone at 5 mg/kg were shorter than at 10 mg/kg, with the difference being statistically significant (P < 0.0001 and P < 0.001, respectively; Table 1).
Effects of medetomidine alone
A pilot study was performed to determine a suitable dose of medetomidine. We examined the effects of 80, 40, 20 and 10 µg/kg, using one animal per dose (data not shown). A dose of 20 µg/kg was the lowest that induced lateral recumbency and loss of the toe-pinch reflex. Therefore, we increased to three the number of animals treated with this dose. The variability of results among these animals was low and, thus, we did not consider it necessary to increase the number of ferrets in this group. The durations of anaesthesia and analgesia are shown in Table 1.
The mean duration of anaesthesia without analgesia produced by medetomidine at 20 µg/kg was 74 ± 10 min (n = 3).
Effects of medetomidine plus alfaxalone
The addition of medetomidine allowed us to reduce the dose of alfaxalone to 2.5 mg/kg. This combination prolonged the duration of both anaesthesia and analgesia as compared to alfaxalone administered alone at 5 mg/kg (P < 0.0001 and P < 0.001, respectively; Table 1). All the animals lost their swallowing reflex between 13 and 25 min (20.1 ± 4.1 min; n = 7) after administration of the drugs.
The duration of anaesthesia without analgesia was reduced to 18 ± 8 min (comparison with medetomidine alone: P = 0.002).
The initial values of BT ranged from 36.0 to 36.5℃. BT increased progressively to a mean rectal temperature of 37.3 ± 0.7℃ (n = 5) at the end of the anaesthetic period (Figure 1). In two animals, heat was inadvertently not supplied via the electric blanket and the BTs of these animals were excluded from the analysis. Pearson’s linear correlation indicated that there was a statistically significant relationship between BT and PR (P = 0.01). Thus, these two animals were also excluded from the analysis of PR values. The other measured parameters were not significantly correlated with BT and, therefore, results from all the animals were analysed.
Graphic representations of changes with time of the parameters monitored during the anaesthesia of ferrets with medetomidine (20 mcg/kg) plus alfaxalone (2.5 mg/kg). As explained in the text, n= 7, except for body temperature and pulse rate in which n= 5. Values shown are means ± SD.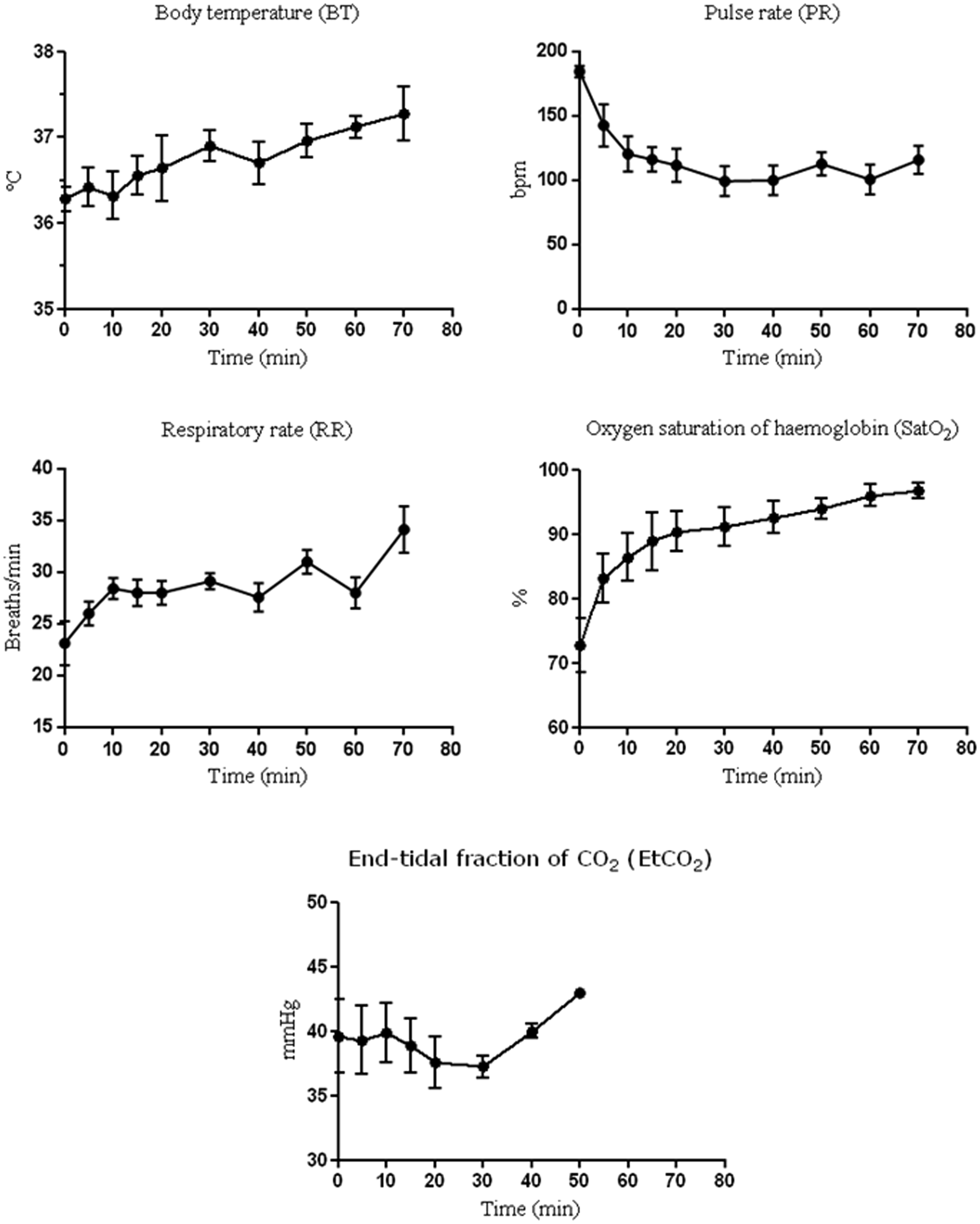
The initial values of PR ranged from 170 to 202 bpm (mean, 185 ± 11 bpm; n = 5). During the first 30 min of the experiment, there was a progressive decrease in PR to a minimum of 109 ± 25 bpm at 30 min, and this mean value was maintained, approximately, until the end of the experiment (116 ± 29 bpm; Figure 1).
Baseline RR, measured previously by direct observation of the respiratory movements of 17 conscious ferrets in our colony, was 28 ± 5 breaths/min. In the present study, immediately after administration of the two drugs, the mean RR was 23 ± 6 breaths/min (n = 7) and the rate gradually increased to 29 ± 2 breaths/min at 30 min (Figure 1). When all the animals were extubated (at 60 min) RR was 28 ± 4 breaths/min.
The initial SatO2 level was low (73 ± 11%; n = 7), then it increased gradually to 91 ± 8% at 30 min and to 97 ± 3% at the end of the anaesthetic period (Figure 1).
Values of EtCO2 were measured in all the animals until they were extubated. Specifically, from the beginning of the experiment to min 20, values from all the animals were recorded; at 30 min, values from four animals were recorded; at 40 min, from three animals; and at 50 min, from one animal. Mean of EtCO2 values ranged from 37 ± 2 mmHg to 40 ± 7 mmHg (Figure 1).
Effects of tramadol plus alfaxalone
Tramadol at 5 mg/kg produced a marked excitatory reaction, which was characterized by licking and self-biting, and the toe-pinch reflex was unaffected. Therefore, alfaxalone at 5 mg/kg was administered to only two tramadol-treated animals. In these animals the duration of anaesthesia was 23 and 24 min, while that of analgesia was 2.5 and 3 min, respectively (Table 1). Cardiorespiratory effects were not examined for this anaesthetic regimen.
Discussion
To evaluate the effects of anaesthetic regimens based on the use of alfaxalone in ferrets, we injected alfaxalone intravenously alone or with other drugs, namely, the alpha-2 adrenoceptor agonist medetomidine and the opioid tramadol.
When administered alone, alfaxalone induced a relatively brief anaesthesia and analgesia effect (Table 1), which might be adequate for clinical explorations and handling but not for complex experimental procedures. The analgesic effect was briefer than that reported in cats 13 and than that reported in dogs treated with alfaxalone at 6 mg/kg, in which the duration of analgesia was more than 30 min. 12 Apparently, dogs are more resistant than ferrets to the respiratory depression provoked by the drug at 20 mg/kg since no deaths have been reported in dogs. 12 Moreover, such previous results in dogs led us to choose 20 mg/kg as the starting dose. However, this dose proved to be lethal for ferrets.
In the present study, endotracheal intubation was possible when the animals had lost the toe-pinch reflex. In cats, the mean dose of alfaxalone, without prior medication, that allowed endotracheal intubation was 4.3 mg/kg (range: 2.7–5.8 mg/kg). 14 However, in ferrets, higher doses are clearly needed, since alfaxalone at 5 mg/kg was not sufficient to allow intubation of all animals (specifically, 7 out of 9).
Our results indicate that alfaxalone, administered alone, is not a good anaesthetic for ferrets, and its use should be restricted to the induction of brief sedation for simple and non-painful procedures (nail trimming, ear cleaning, oral prophylaxis, etc.). In addition, intravenous administration without prior medication can be challenging because the bolus has to be administered slowly in order to avoid adverse effects, such as respiratory depression and apnoea. Rapid intravenous administration (within less than one minute) of a variety of anaesthetic agents induces depression of the respiratory centres and skeletal muscle relaxation in both cats and dogs.16–18
Difficulties associated with percutaneous venepuncture in conscious animals can be avoided by using a local anaesthetic, such as lidocaine, applied topically prior to the venepuncture. In the present study, we performed percutaneous venepuncture in the forelimb of ferrets, whose skin is very thick, and we sprayed the area first with a lidocaine aerosol to prevent the pain reflex in animals that had led, initially (in preliminary assays), to extravasation and incorrect administration of drugs. Using lidocaine, administration of drugs intravenously to conscious animals was successful in all cases. Lidocaine might be absorbed through the skin. Thus, some of the anaesthetic effects seen in our study animals might have been related in part to the effects of this drug. However, assuming such effects to be negligible, we found that the application of lidocaine was essential for correct administration of alfaxalone, with less stress for both the animal and the handler. When we used the combination of medetomidine and alfaxalone, it was not necessary to apply lidocaine to the site of venepuncture because the animal was already unconscious as a result of the medetomidine and, thus, handling was easier.
Despite the difficulties of intravenous administration in the ferret, injection of alfaxalone via the intramuscular route was discarded, since this drug has been marketed at a concentration of 10 mg/mL. Therefore, with the doses tested, it would have required the injection of unacceptably high volumes.
Medetomidine is an alpha-2 adrenergic agonist that is widely used as an animal sedative and hypnotic with variable analgesic effects. It has been reported that medetomidine produces light to heavy sedation in ferrets, 5 but combination with other agents, such as ketamine, butorphanol or both, has been recommended. 1 In our study, the administration of medetomidine alone resulted in a long interval between recovery of the toe-pinch reflex and recovery of the sternal position. In other words, the anaesthetic effect was of a much longer duration than the analgesic effect. Thus, the recovery period was rather long. The combination of medetomidine, at a relatively low dose, and alfaxalone produced analgesia of a longer duration than that obtained, in ferrets, with medetomidine alone, and even of a longer duration than that reported for a high dose of medetomidine (80 µg/kg) alone and in combination with ketamine in the same animal.1,19
In previous studies of ferrets treated with a high dose of medetomidine (60 µg/kg) plus ketamine, the mean duration of sedation without analgesia ranged from 48 to 64 min, depending on the dose of ketamine. 19 In the present study, the use of a reduced dose of medetomidine (20 µg/kg) plus alfaxalone (2.5 mg/kg) yielded the closest correlation between the duration of anaesthesia and that of analgesia.
This combination produced a marked decrease in PR, relative to the initial value (Figure 1). We did not measure the basal value in conscious animals, but the range of the first values in anaesthetized animals (170–202 bpm) was slightly lower than the range of heart rates reported in the literature (200–250 bpm). 20 The lowest mean value was recorded 30 min after the injection of alfaxalone (109 ± 25 bpm; n = 5) and, even when animals had recovered some of their reflexes, PR remained low. Ko and coworkers reported similar mean values after 30 min of anaesthesia with medetomidine alone (80 µg/kg) and in combination with butorphanol, whereas combinations with ketamine and with ketamine plus butorphanol yielded higher values. 1 In cats, alfaxalone causes decreases in heart rate, arterial blood pressure and cardiac output in a dose-dependent manner. 13 If we extrapolate this observation to ferrets, we can postulate that the administration of medetomidine prior to alfaxalone might help to avoid dangerous changes in haemodynamic parameters since it allows a reduction in the dose of alfaxalone that is required to achieve the desired effect.
The RR hardly changed with time, increasing only slightly at the end of the experiment. In addition, EtCO2 also remained constant and SatO2, which was low at the beginning of the experiment (probably because we did not pre-oxygenate the animals), increased during anaesthesia until it reached normal values. The EtCO2 levels were not confirmed by arterial blood gas analysis, and we are aware that real values might have been higher, since our system (sidestream capnography) might theoretically lead to erroneous measurements in very small mammals. Nonetheless, RR and SatO2 values pointed to absence of respiratory depression. By contrast, depression of respiratory functions and increases in EtCO2 were reported in ferrets that had been anaesthetized with other medetomidine-based combinations (medetomidine plus ketamine and/or butorphanol). 1 Alfaxalone in cats and dogs produced respiratory depression.12,13 Moreover, respiratory depression was dose-dependent and was the clinically most relevant adverse effect in dogs. 12 In ferrets, the combination of medetomidine and alfaxalone allowed us to reduce the dose of each drug and, in this way, to minimize their potential negative side-effects on respiration.
Tramadol is an opioid agonist that appears to offer some advantages in anaesthesia since it has a second mode of action, independent of the opioid-agonist mechanism, namely, the inhibition of the reuptake of serotonin and noradrenaline in the spinal cord. 21 In addition, it is inexpensive and, in many countries, it is not classified as a controlled substance. These potential advantages, together with the good results reported previously in some species,22,23 led us to examine its effect, as a premedication, in ferrets since, to our knowledge, there are no published data about the use of tramadol in the ferret. However, ferrets in the present study showed a strong excitation reaction after the administration of tramadol, which was mainly characterized by self-biting and which was probably associated with pruritus and/or a reaction at the site of the injection.
Prior to testing the tramadol–alfaxalone combination, we performed a small pilot experiment to select a suitable dose of tramadol. Specifically, we tested 5 and 10 mg/kg (n = 1 each; data not shown) and we found excitatory reactions, which were more marked in animals injected with the higher dose. For this reason we selected the lower dose to be used in combination with alfaxalone.
When the condition of an animal allowed subsequent intravenous injection of alfaxalone, the duration of analgesia was shorter than that obtained with alfaxalone alone (Table 1) and endotracheal intubation was not possible. Thus, tramadol might not be analgesic in ferrets and/or might not potentiate the effects of alfaxalone. However, we cannot ignore the possibility that the intravenous administration of alfaxalone was defective as a consequence of the excited state of the animals. In fact, we cannot discard the possibility that subsequent higher doses of alfaxalone might have given a better anaesthetic performance. However, due to the excitatory status of the animals, it was not possible to administer additional doses intravenously, neither was it considered ethically acceptable to include more animals because of the apparent discomfort they would have experienced.
In conclusion, alfaxalone administered to ferrets as a single anaesthetic drug, at the doses tested, produced a short-term anaesthesia and had a brief analgesic effect, without noticeable adverse effects. At higher doses, the drug was lethal. When alfaxalone was combined with the opioid tramadol, the anaesthetic and analgesic effect was not improved and excitation was observed. However, the combination of alfaxalone and medetomidine had an anaesthetic effect that might be suitable for short- or medium-term experimental procedures in ferrets. The alpha-2 adrenoceptor agonist medetomidine potentiated the analgesic effect of alfaxalone and allowed us to reduce the dose of the latter drug.
Footnotes
Acknowledgements
The authors thank Ms Vanessa Panadés, Ms Alexandra Cordón and Ms Rosa Gaya for their invaluable technical assistance during the course of this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.