
Abstract
Objectives: This study aims to parse out the effects of childhood head injury (HI) as an acquired neuropsychological deficit that impacts adolescent delinquent behavior, while accounting for other early-life risk factors and potential temporal ordering. Methods: Nationally representative prospective data from the UK Millennium Cohort Study (MCS; N = 13,287) and a series of logistic and binomial regressions are used to examine the relationship between early-life risk factors, HI, and adolescent delinquent behavior. Methodological considerations from clinical HI research, such as the use of an orthopedic injury comparison group, are incorporated. Results: Findings are consistent with the conceptualization of HI as an acquired neuropsychological deficit, in that childhood HI increases the risk of early- and adolescent-onset delinquency, sustained delinquent behavior from childhood to early adolescence, and participation in a greater variety of delinquent behavior. Conclusions: Childhood HI is relatively common, as over 27% of the sample reported at least one HI. The importance of HI as an acquired neuropsychological deficit and its relevance as a risk factor for later criminal behavior is reiterated. Future research should examine the importance of developmental period effects and mechanisms underlying this relationship.
The psychological, emotional, and behavioral complications that arise after experiencing a head injury (HI), such as a concussion, are numerous and potentially detrimental across the lifespan (Crowe 2008; Eslinger, Flaherty-Craig, and Benton 2004; Karver et al. 2012; Yeates and Taylor 2005). Damage to the brain during childhood may disrupt neural and psychosocial development, which developmental and biosocial theories of crime suggest would influence later criminal behavior (Farrington 2006; Moffitt 1993; Moffitt and Caspi 2001). Research consistently finds associations between HI and criminality (Durand et al. 2017; D. Fishbein et al. 2016; Huw Williams et al. 2010; Kaba et al. 2014; Luukkainen et al. 2012; Schofield et al. 2015; Schwartz, Connolly, and Brauer 2017; Schwartz, Connolly, and Valgardson 2018; Vaughn et al. 2019), but the vast majority of these studies examine this relationship among either adults or incarcerated adolescents. Little is known about the effect of childhood head injury on onset of antisocial behaviors. While HI at any point in the lifespan has the potential to change brain functioning and subsequent behaviors (see Schwartz et al. 2019 for review), animal models suggest that HI during childhood or adolescence may be even more detrimental to normative development (Guilhaume-Correa et al. 2020; Zhao et al. 2018). During this time, the brain goes though marked changes in both structure and function, making it more susceptible to environmental influences (Karver et al. 2012).
Based on biosocial theories of crime, individuals who experience some sort of early-life trauma, such as a HI, should be more likely to initiate delinquent behavior early and engage in more serious delinquent behaviors (Moffitt 1993; Moffitt and Caspi 2001). As early onset of criminal or delinquent behavior is predictive of frequent, serious, and persistent behavior throughout the life-course, an in-depth exploration into HI is warranted (LeBlanc and Loeber 1990, 1998). Part of this increased likelihood of serious delinquency could be due to the acquired neuropsychological deficits that follow a head injury. Previous literature has established neuropsychological deficits—and specifically HI—as important risk factors for impulsivity, aggression, and substance use (Beaver et al. 2010; Bonow et al. 2019; D. Fishbein et al. 2016; Huw Williams et al. 2010; Kennedy, Heron, and Munafò 2017; Perron and Howard 2008; Schwartz 2019; Schwartz et al. 2017, 2018; Vaughn et al. 2014), all of which could lead toward onset or acceleration of criminal behavior (LeBlanc and Loeber 1990, 1998).
Research on the behavioral correlates of HI tends to fall under the purview of either clinical or criminological research. These two fields offer relatively different perspectives and foci on the study of HI, sometimes to the detriment of further progress in HI research. Clinical literature tends to focus on moderate to severe HIs, which are much less common than mild HIs (Frost et al. 2013), while criminological literature tends to focus on offenders with a history of HI, which introduces selection issues (Schwartz 2019; Schwartz et al. 2017; see Connolly and McCormick 2019 for exception). While clinical samples provide useful insights on the potentially severe effects of HI, they are not representative of the general population that experiences a HI. It has been estimated that up to 50% of young adults with mild HIs—which are far more common than their more severe counterparts—do not seek medical attention (Demakis and Rimland 2010), leaving much of the population with HIs outside of the scope of clinical studies. On the other hand, criminological studies of offender populations shed light on the prevalence of head injuries among incarcerated populations, which ranges from 46% to 60% (Durand et al. 2017; Farrer and Hedges 2011), but do little to address whether HI has any influence on initiation and persistence of criminal behavior or whether HIs occur as a consequence of involvement in criminal and potentially dangerous behavior. Additionally, the use of convicted samples in criminology research excludes those who have a history of HI but have not come into contact with the criminal justice system.
Furthermore, methodological complications exist in the study of HI, many of which involve the operationalization of the injury variable itself. Most clinical studies use diagnostic scales, which allow for relatively precise measures of HI severity (Bonow et al. 2019; Light et al. 1998; O’Sullivan et al. 2015; Yeates and Taylor 2005), while criminological research tends to rely on self-reports of HI history, which introduces potential issues with construct validity across studies (Kennedy et al. 2017; Perron and Howard 2008; Vaughn et al. 2014). Another major area of discrepancy between clinical and criminological research is the operationalization of control groups. Clinical studies often use a measure of other orthopedic or bodily injury as a control group, while criminological studies tend to compare those with HI to their non-injured peers. The use of the orthopedic injury (OI) reference group has been recommended for future studies on HI, as its use should account for omitted variables that might simultaneously influence the risk of experiencing any sort of bodily injury and the risk for the antisocial behavioral outcomes of interest (Karver et al. 2012; Milders et al. 2008; Yeates and Taylor 2005).
In the present study, nationally representative, prospective data from the UK Millennium Cohort Study (MCS) are used to examine the effect of childhood HI on onset and persistence of adolescent delinquent behavior. The MCS follows the lives of over 18,000 children and their families to gain insight on their physical, social, cognitive, and behavioral development throughout the new millennium (Connelly and Platt 2014; Joshi and Fitzsimons 2016). At the initial wave, cohort members were 9 months of age. Subsequent waves of data have been collected at ages 3, 5, 7, 11, and 14 years, all of which are used in the present study. The focal analyses of the current study examine the effect of HI on age of delinquent behavior onset and patterns of delinquent behavior, while accounting for early-life risk factors consistent with DLC theories of crime. Parent reports of cohort members’ experiences of HI at multiple ages provide a unique non-clinical sample, while self-reports from the cohort members provide information on delinquent and antisocial behaviors. This study aims to contribute to the field of biosocial criminology by parsing out the effects of childhood HI on adolescent delinquent behavior, while accounting for other important early-life risk factors and incorporating relevant methodological considerations from clinical studies of HI in a nationally representative sample. In doing so, the present study will further our knowledge of risk factors for early-onset of delinquent behavior and shed light on possible mechanisms that facilitate persistence of delinquency throughout adolescence.
Theoretical Perspectives
Developmental and biosocial perspectives generally posit that early life risk factors influence later antisocial behaviors, specifically delinquency (Farrington and Loeber 2012; Gottfredson and Hirschi 1990; Jolliffe et al. 2017; LeBlanc and Loeber 1998; Moffitt 1993). Moffit (1993) posited that serious delinquency during adolescence could be attributed to what Schwartz (2019)would later call “acquired neuropsychological deficits” that arise from perinatal head injury, among other environmental and biological risk factors. As an acquired neuropsychological deficit, HIs uniquely span the gap between environmental and biological risk factors, in that they tend to occur as a function of the environment but largely affect behavior on a neurobiological level (Beaver et al. 2010; Fishbein et al. 2016; Guilhaume-Correa et al. 2020; Schwartz et al. 2017; Schwartz 2019; Zhao et al. 2018). Recent biosocial research has further opened the door to incorporating neurobiological mechanisms, such as executive functioning and self-regulation, as influential in the emergence of delinquent behavior (Beaver et al. 2010; Beaver, Wright, and Delisi 2007; Schwartz et al. 2017, 2018). These neuropsychological deficits may then distinguish those who begin their delinquent behavior earlier and persist throughout the life-course from those who do not do so (LeBlanc and Loeber 1990, 1998; Moffitt and Caspi 2001; Nagin, Farrington, and Moffitt 1995).
While Moffitt (1993) originally focused on disruptive events that occur early in life as risk factors for later delinquency, increasing evidence from developmental research suggests that risk factors can and do occur throughout childhood and into adolescence (Beaver et al. 2010; Miller, Malone, and Dodge 2010; Moffitt and Caspi 2001; Pepler et al. 2010). Indeed, there are critical points in development throughout childhood and adolescence when vulnerability to both environmental and biological risk factors is accentuated (Casey, Giedd, and Thomas 2000; Eslinger et al. 2004; Karver et al. 2012). For instance, the “latent deficit” hypothesis suggests that early childhood traumas will produce worse and longer-lasting cognitive deficits than adult injuries of the same magnitude due to heightened sensitivity of the brain (Barker et al. 2010; Eslinger et al. 2004). It is possible that neuropsychological deficits acquired during childhood will have more impact on psychological and behavioral outcomes (Benz, Ritz, and Kiesow 1999), which may then lead to earlier onset of delinquent behavior. Studies of mice with mechanically induced head injuries provide support for this hypothesis, as neuropsychological deficits are more severe in adolescent than adult mice (Guilhaume-Correa et al. 2020; Zhao et al. 2018), suggesting that timing of the injury is an important determinant of observed outcomes. Therefore, HI that occur during these critical periods of development—such as childhood and adolescence—may pose greater risk than HI at other time periods. This enhanced risk is then likely to translate to longer lasting and more deleterious behavior outcomes, such as earlier and more serious criminal behavior, as well as earlier criminal justice contact (LeBlanc and Loeber 1990, 1998).
One of the proposed mechanisms through which HI could increase the risk of delinquent behavior is via impacts on executive functioning (Schwartz et al. 2017), and a hallmark of executive dysfunction is impulsivity or lack of self-control (Beaver et al. 2007). Neurological deficits that arise as a result of damage to the brain during childhood have potential to negatively impact the development of an individual’s self-control, and consequently, their propensity for delinquent behavior (Beaver et al. 2010, 2007; Cauffman, Steinberg, and Piquero 2005). On the other hand, Gottfredson and Hirschi’s (1990) theory of self-control argues that low self-control also increases the likelihood of accidents or injuries. Therefore, early levels of self-control might have an impact on an individual’s likelihood of getting a HI—or any injury, for that matter—throughout childhood. Individuals who are more impulsive may be more likely to exhibit behaviors that could lead to both delinquency and any type of injury.
It is then important to consider how low self-control—and many of the social factors that are theorized to influence self-control—may render the relationship between the risk of injury and the risk of delinquency spurious. There are a number of other possible confounding influences that are typically unobserved in studies of HI, such as experience of abuse or victimization, parental supervision and attachment, extraversion, and participation in sports to name a few. Clinical studies of head injury often use a negative control injury group to implicitly control for these possible spurious relationships. Those who have sustained bodily injuries, but not head injuries, act as a negative control injury group, which should implicitly account for unobserved factors that may lead to both injury and delinquency (Karver et al. 2012; Yeates and Taylor 2005). For these reasons, a measure of bodily injury sustained over the time period of interest is used as a proxy for these unobserved and potentially confounding characteristics.
HI and Crime
HI is consistently associated with impulsivity, aggression, and substance use, as well as criminal behavior (Crowe 2008; Fishbein et al. 2016; Huw Williams et al. 2010; Perron and Howard 2008; Schwartz et al. 2017; Vaughn et al. 2014). Damage to the brain can occur even after a relatively mild concussion (Crowe 2008) and often impacts executive functioning, which includes abilities such as inhibition, decision-making, and emotional regulation (Barker et al. 2010). Executive function deficits, especially increased impulsivity and aggression, are often implicated in criminal behavior, which provides a potential link between HI and criminal behavior (Moffitt 1993; Moffitt and Caspi 2001; Perron and Howard 2008; Vaughn et al. 2014). Other deficits have been proposed, such as emotion regulation and moral reasoning, both of which can be impacted by the experience of an HI (Eslinger et al. 2004; Schwartz, Fitter, and Jodis 2020; Tonks et al. 2009)
Although the connection between HI and crime is well-established, past studies have predominately focused on the high prevalence of HI in offender populations, rather than the predictive validity of HI for criminal behavior (Durand et al. 2017; Farrer, Frost, and Hedges 2013; Farrer and Hedges 2011; Huw Williams et al. 2010; Perron and Howard 2008). Several studies have established that the prevalence of HI in adult incarcerated groups is significantly higher than that of the general population, with estimates ranging from 46% to 60% for incarcerated populations (Durand et al. 2017; Farrer and Hedges 2011; Fazel et al. 2011). Among juvenile offenders, the prevalence of self-reported HI ranges from 18-75% (Farrer et al. 2013; Huw Williams et al. 2010; Perron and Howard 2008). However, there is comparatively little work considering HI as a risk factor for the onset of delinquency.
Schwartz, Connolly, and Brauer (2017) examined the link between head injury, self-control, and delinquency in adjudicated adolescents and found that self-reported TBI was associated with lower levels of self-control, as well as higher rates of aggression and delinquent behaviors. However, this study was not adequately able to determine whether HI affected the initiation of criminal behavior or whether HI occurred as a consequence of involvement in criminal and risky behavior. Fishbein et al. (2016) examined the relationship between childhood HI, substance use and aggression in a sample of incarcerated adults. Childhood HI was associated with earlier initiation into illicit substance use than those without HI or with HI occurring later in life. However, since both of these studies utilize sample of known offenders, associations between HI and antisocial or delinquent behaviors might be underestimated, as the variation in outcomes of interest is reduced.
While it is generally proposed that damage to brain tissue can precede criminal behavior, few studies have examined this relationship longitudinally. Only recently have studies attempted to delineate the causal ordering of HI and delinquent behavior. Timonen et al. (2002) and Fazel et al. (2011) both reported increases in reported criminal behavior following a head injury; however, their estimates may be biased upward by comparing severe clinical samples to uninjured individuals. Kennedy, Heron, and Munafo (2017) examined a similar relationship in a longitudinal birth cohort but found that, when comparing to those with orthopedic injury, the association between HI and criminal behavior was not statistically significant. Schwartz et al. (2018) found that head injury was not associated with increases in later delinquent behavior in a sample of adolescent offenders but did find that it was associated with increases in impulsivity, which may, in turn, increase the risk of delinquent behavior. In the same sample of adolescent offenders and using multilevel, within-person models, Schwartz (2019) found that head injury led to prolonged periods of persistence in criminal behavior, suggesting that head injury does have a potentially causal effect on sustained delinquent behavior, but was unable to determine the effect of HI on delinquency onset. In a sample of high-risk adolescents, Connolly and McCormick (2019) identified a positive association between head injury and future delinquency, net of previous delinquent behavior.
The aforementioned studies tend to provide support for HI as an important predictor of criminal behavior, but much is still unknown about HI as an acquired neuropsychological deficit. Given the importance of sensitive developmental periods in childhood and adolescence, it stands to reason that head injury during those sensitive periods in childhood may lead to significant detrimental outcomes, including onset of delinquent behavior. However, prior studies have largely been unable to assess the influence of childhood head injury on delinquency onset, in addition to persistence, especially in general adolescent populations.
The Current Study
While much of this literature points to HI as influential in the initiation of criminal behavior, very few studies have been able to assess this relationship longitudinally and in samples of non-incarcerated individuals (Bonow et al. 2019; Kennedy et al. 2017; Connolly and McCormick 2019). To address several of the limitations identified above, as well as to extend previous findings to an adolescent population, the current study seeks to examine the relationships between early-life risk factors, HI, and delinquent behavior. The first step of the analysis determines whether certain early-life risk factors predict whether a child will experience a HI or OI. Although OI is used to control for unobserved injury-related characteristics—such as low baseline self-control—it is possible that some early-life risk factors are more predictive of one type of injury than the other. The second step of the analysis examines whether childhood HI is a significant predictor of onset and typology of adolescent delinquency, even when compared to individuals with other bodily injuries. To my knowledge, no other study has addressed onset and typology of delinquent behavior, while also controlling for the pre-morbid injury-related factors that could confound the relationship between crime and HI. The use of the Millennium Cohort Study allows for in-depth analyses of these relationships in a nationally representative and non-clinically defined sample of adolescents. Furthermore, the longitudinal nature of the data allows for analyses to be restricted to head injuries that occurred prior to delinquent behavior.
Consistent with prior research, a history of childhood HI should predict higher levels of delinquency, compared to those who have been uninjured. In contrast, the effect of childhood HI on adolescent delinquency should be attenuated when compared to those with childhood orthopedic injury (OI). As an acquired neuropsychological deficit, HI is likely to predict both delinquency onset at age 11 years and onset at age 14 years. Additionally, HI should still be predictive of more serious delinquent behavior, such as consistency in behavior from age 11 to age 14 and participation in a greater variety of delinquent behavior at age 14.
Methods
Data
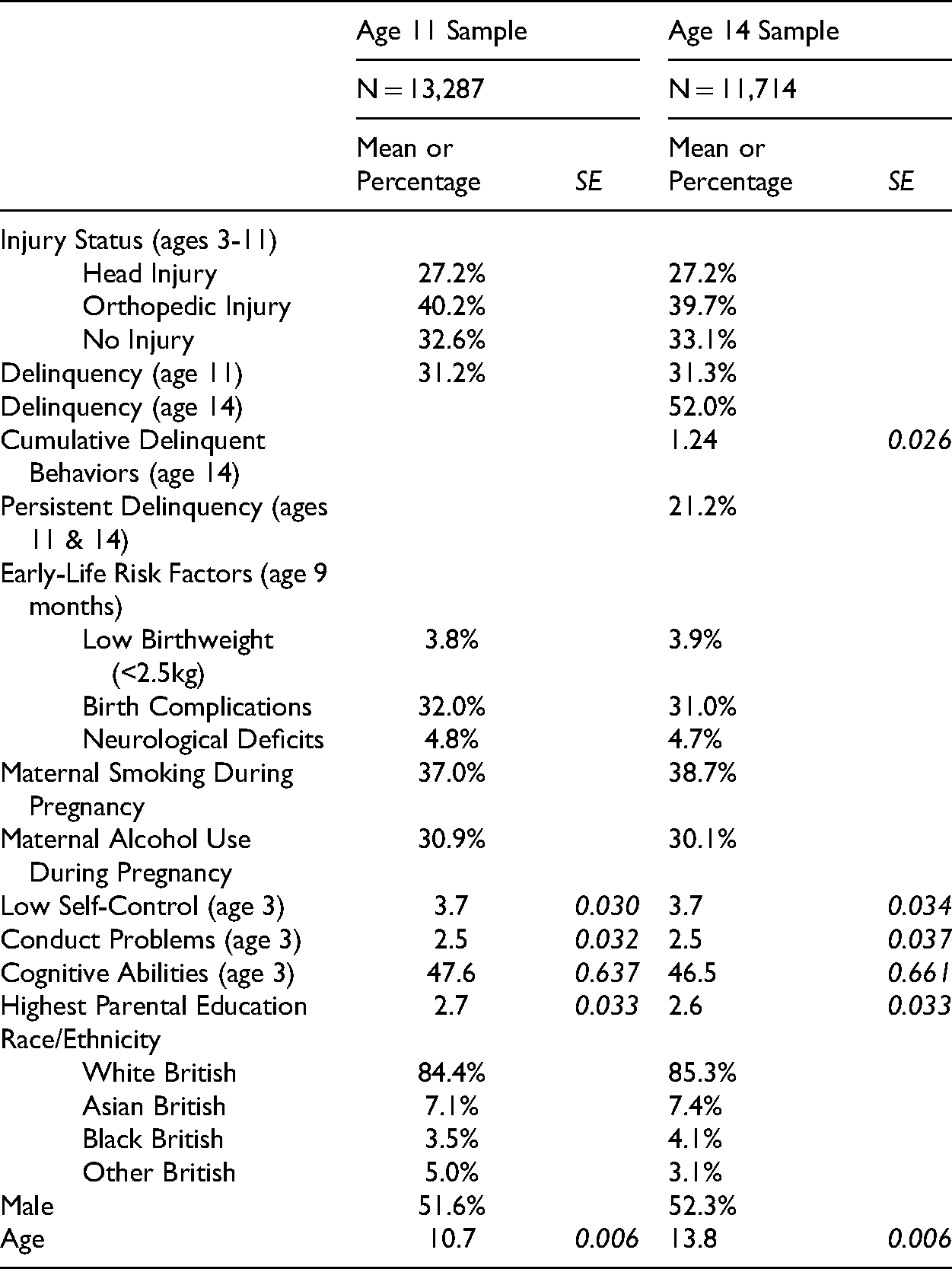
The Millennium Cohort Study (MCS) is a longitudinal and nationally representative study of children born in the UK from 2000 to 2002 (Plewis 2007). Infants included in the survey were living in either England, Wales, Northern Ireland, or Scotland at the time of the initial wave (Joshi and Fitzsimons 2016). The MCS oversampled children exposed to higher levels of disadvantage, including electoral wards with high levels of poverty (Connelly and Platt 2014). At the initial wave, which occurred when cohort children were modal age 9 months, parents from 18,552 families participated in questionnaires and in-person interviews, producing a total sample of 18,818 children (Plewis 2007). Data were collected when the children were modal ages 9 months, 3, 5, 7, 11, and 14 years old. In 98% of cases, the main caregiver was the cohort member’s natural mother (Fitzsimons 2017). At ages 11 and 14, the MCS cohort members were administered confidential surveys to assess their attitudes and participation in risky behaviors. Descriptive statistics for the variables of interest in the present study are shown in Table 1. Analytic samples for both age 11 (wave 5) and age 14 (wave 6) are presented. By age 14, about 76% of MCS children were still able and willing to participate. Attrition 1 was more likely among boys, Whites, children of parents with lower levels of education, and children in single-parent households (Mostafa and Ploubidis 2017).
Weighted Descriptive Statistics.
Injury Status
At ages 9 months, 3, 5, 7, 11, and 14 years, primary caregivers of the MCS children are asked what serious injuries their child had experienced since the last wave, such as a “broken bone” or a “cut needing stitches”. Children were coded as experiencing a HI if either “loss of consciousness/knocked out” or “bang on the head/injury to head without being knocked out” were reported. These criteria for head injury remained constant across all waves. Caregivers were able to report multiple injuries within a given wave. Injuries that were reported between the ages of 3 and 11 are included in the analyses in order to isolate this predictor to injuries that would have primarily occurred before the reported delinquent behaviors. However, it should be noted that there is some overlap between the age 11 delinquency measure and this measure, and, as such, causal identification is not possible.
Following previous clinical literature, individuals with a history of Orthopedic Injury (OI) are included as a comparison group to those with HI (Kennedy et al. 2017; Milders et al. 2008; Yeates and Taylor 2005). Whether an individual experienced an OI or not was determined from all of the other injury-related responses to the same question(s) used to determine experience of a HI. OIs were reported more frequently at each wave than HIs, which is to be expected. By using OI as a foil, other pre-morbid effects or injury-related factors that might be contributing to the relationship between HI and delinquency are considered and accounted for implicitly (Kennedy et al. 2017). Therefore, compared to OI, we could assume head injury leads to delinquency above and beyond whatever spurious mechanisms, including social factors, lead to both bodily injury and criminal behavior.
Individuals were coded as having No Injury (NI) if no injuries were reported at any of the waves from ages 3 to 11. If an individual had reports of both OI and HI at either the same wave or different waves, they were coded to belong in the HI group, as is common in other studies (Bonow et al. 2019; Kennedy et al. 2017). Individuals within the HI group may have experienced both HI and OI, but the use of the OI group as a control should account for any of the injury-related factors that are present in both groups. As shown in Table 1, approximately 27% of children experienced an HI from ages 3 to 11. Approximately 40% experienced an OI from ages 3 to 11, and approximately 33% never experienced either an HI or an OI.
Delinquency Onset 2
Age 11 delinquency is used to obtain an indicator of early onset of delinquent behavior (Staff et al. 2015). The average age of initial formal contact with the justice system in the UK is 15.2 years of age (Ministry of Justice 2016), and, as such, the age 14 measure is used to capture more normative delinquency. Items from the age 11and 14 questionnaires ask about cohort members’ own delinquent behaviors; however, the age 11 questionnaire measures any previous delinquent behavior, while the age 14 questionnaire is restricted to those behaviors that occurred in the 12 months prior. Delinquency at age 11 was coded as a binary measure of whether the respondent had ever exhibited any of the following behaviors by the time of the survey: “had an alcoholic drink,” “tried a cigarette,” “damaged anything in a public place that didn’t belong to [them],” “spray painted on a building,” “taken something from a shop without paying for it,” or “been noisy or rude in public so that people complained.” By wave 5 (modal age 11), 31% of cohort members had engaged in delinquent behavior.
The binary delinquency onset measure at age 14 included those same measures (i.e., drinking alcohol, smoking cigarettes, damaging and defacing public property, shoplifting, and public disturbance) as well as whether or not the cohort members “missed school without parents’ permission.” At this survey wave, all behaviors were restricted to those that occurred in the 12 months prior to the survey to assess recent onset. By wave 6 (modal age 14), 52% of cohort members had engaged in some form of delinquency in the past 12 months.
Cumulative Delinquent Behaviors
A variety score of delinquency was coded to represent the summation of positive responses to participation in each of the delinquent behaviors at age 14 listed above. Additionally, lifetime use of cannabis and ever having been stopped or warned by the police were included in this measure. 3 The delinquency variety score ranged from 0-10, with a mean of 1.24 delinquent behaviors. Prior research has indicated that binary coding schemes may not be sufficient for assessing delinquent behavior (Sweeten 2012), so the variety score for delinquent behavior should provide a more nuanced picture of delinquent behavior accumulation at age 14. Additionally, the variety score helps to account for breadth of delinquent behavior, rather than treating any participation in delinquent behavior as equally serious.
Persistence of Delinquency
Persistence of delinquency over time was coded as a binary measure based on whether respondents indicated that they had persisted in their delinquency at both the age 11 and 14 waves. All respondents who did not indicate delinquency at both waves were coded as 0. Approximately 21% of cohort members engaged in delinquent behavior at both age 11 and 14 years.
Low-Self Control
Hyperactivity was measured as part of the Strengths and Difficulties Questionnaire (SDQ) at age 3 (Goodman 1997; Goodman, Lamping and Ploubidis 2010; www.sdqinfo.com). Items from the hyperactivity scale are used to operationalize low self-control in the MCS cohort. The measure for low self-control includes items of whether the child is “constantly fidgeting,” “easily distracted,” “restless, overactive, or cannot stay still for long,” “thinks things out before acting” (reverse coded), “see tasks through to the end” (reverse coded). Responses to these items range from 0 “not true” to 2 “certainly true” (Cronbach’s α = 0.71). Scores range from 0-10 (mean = 3.7), with higher scores indicating substantial problematic behaviors (Goodman 1997; Goodman, Meltzer and Bailey 1998; Goodman et al. 2000).
Conduct Problems
Conduct problems were also measured as part of the SDQ at age 3 through parent’s reports. Items from this scale are used to indicate aggressive childhood behaviors. This scale includes items such as “often has temper tantrums,” “generally obedient” (reverse coded), “fights with or bullies other children,” “often argumentative with adults,” and “can be spiteful to others” (Cronbach’s α = 0.68). Responses to these items range from 0 “not true” to 2 “certainly true.” As with low self-control, scores range from 0-10 (mean = 2.5), with higher scores indicating substantial levels of conduct problems at age 3 (Goodman 1997; Goodman, Meltzer and Bailey 1998; Goodman et al. 2000).
Cognitive Abilities
Cognitive abilities were measured at age 3 through the use of the British Ability Scales II (BAS II). The BAS II is a cognitive battery assessing ability and educational achievement (Elliot, Smith, and McCulloch 1996). At age 3 years, the BAS II primarily tests expressive verbal ability. Percentile scores adjust for the test item difficulty and the cohort member’s age, while also indicating relative ability in comparison to the rest of the sample (Connelly 2013).
Prenatal & Perinatal Risk Factors
Based on Moffitt’s dual taxonomy theory, all models include controls for several prenatal and perinatal risk factors that could influence future delinquency. Each of these risk factors were reported by the primary caregiver at either wave 1 (modal age 9 months) or wave 2 (modal age 3 years), which in the vast majority of cases (98%) is the birth mother. Low birth weight is measured as any weight less than 2.5kg, which is the standard threshold (Cutland et al. 2017). Less than 4% of MCS children fell under this threshold. Birth complications refer to a binary measure for any medical complications that arose during labor, such as “breech birth” or “foetal distress”. Approximately 32% of caregivers reported complications at birth. Neurological deficits refer to a binary measure of whether any central nervous system disorders were diagnosed by age 3, such as “epilepsy,” “convulsions,” or “blackouts.” Less than 5% of the sample reported one of these neurological deficits. Maternal smoking behavior is coded as a binary measure reflecting whether or not the cohort member’s biological mother used nicotine during pregnancy. Approximately 38% of caregivers reported maternal smoking during pregnancy. Maternal drinking behavior refers to a binary measure of whether the cohort member’s mother ever drank alcohol during her pregnancy. 31% of caregivers reported maternal alcohol use during pregnancy.
Sociodemographic Controls
A variety of sociodemographic characteristics were utilized as controls for all analyses. Parent(s’) highest educational level is based on the European national vocational qualification (NVQ) scale ranging from NCQ0 to NVQ5. NVQ0 is equivalent to not having a diploma, while NVQ5 is equivalent to postsecondary academic credentials. Race/ethnicity is coded as a categorical variable of White British, Black British (“Black or Black British”), Asian British (“Pakistani and Bangladeshi” and “Indian”), and Other British (“Mixed” and “Other Ethnic Group”). White British is used as the reference group for all models, as this group makes up the vast majority of the sample. Age of the cohort member was measured during either wave 5 (modal age 11 years) or wave 6 (modal age 14 years) and was included as a control in every model. The focal wave for the outcome of interest determined whether wave 5 or wave 6 age was used (i.e., wave 5 age would be used in a model predicting delinquency at wave 5). Finally, sex is present in all models (male = 1). Approximately 52% of the sample is male.
Analytic Strategy
As previously mentioned, the MCS is a longitudinal and nationally representative survey of youth in the UK born at the turn of the century. The population was stratified at both the country level and the electoral ward level. In all analyses, survey weights, provided by the investigators, were used to account for the complex survey design and sampling procedures by using the “svy” command in Stata 15 (StataCorp 2017). To account for missing data, multiple imputation strategies that relied on chained regressions were used. In order to account for the variety of outcomes and operationalizations of variables, several imputations were carried out. All multiple imputations were run using the “mi estimate” command in Stata 15 (StataCorp 2017). Previous studies have used multiple imputations with the MCS data and retained accurate estimates (Staff et al. 2019).
For the age 11 analytic sample, 25 imputations were run to achieve a final analytic sample of 13,287 cohort members with valid statistical weights. All variables of interest were missing less than 10% of cases, except for two—low self-control and cognitive abilities at age 3 years, which were missing 13.0% and 14.4%, respectively. Delinquency at age 11 was missing on less than 3% of cases, and the injury status variable was only missing on 27 (0.2%) out of the 13,287 cases.
Data were imputed 25 times to achieve a sample of 11,714 cohort members with valid statistical weights for the age 14 analytic sample. Similarly, all variables were missing less than 10% of cases, except for low self-control (12.3%) and cognitive abilities (13.5%) at age 3 years. Delinquency at age 14 was missing on 3.0% of cases, and the injury status variable was missing on 0.3% out of the 11,714 cases. For models predicting delinquency onset by age 14, those who reported delinquent behavior at age 11 are excluded, producing an analytic sample of 8,377.
The analysis will proceed in five primary steps. First, I examine whether early-life risk factors are associated with selection into one of the injury categories. Multinomial logistic regressions are used to compare risk factors associated with NI, OI, and HI. Second, the relationship between injury status and early-onset delinquency is examined using logistic regressions. Multiple models are estimated, using either NI or OI as the reference category, to show how results vary depending on the foil to HI. Third, the relationship between injury status and adolescent-typical delinquency onset is examined using logistic regression. Similarly, these models will be tested with varying reference categories. Fourth, logistic regression will be used to examine the relationship between childhood HI and persistence of delinquent behavior. Finally, binomial regression will be used to examine how childhood HI affects the count of delinquent behaviors exhibited at age 14. Since the variety score for delinquency is bounded (max = 10), binomial regressions are used, which provide more accurate estimates than traditional regression models for count outcomes (Britt, Rocque, and Zimmerman 2018). Additional supplementary analyses with alternate specifications of the injury variable and delinquency outcomes are available online.
Results
Early Life Factors as Predictors of HI by Age 11
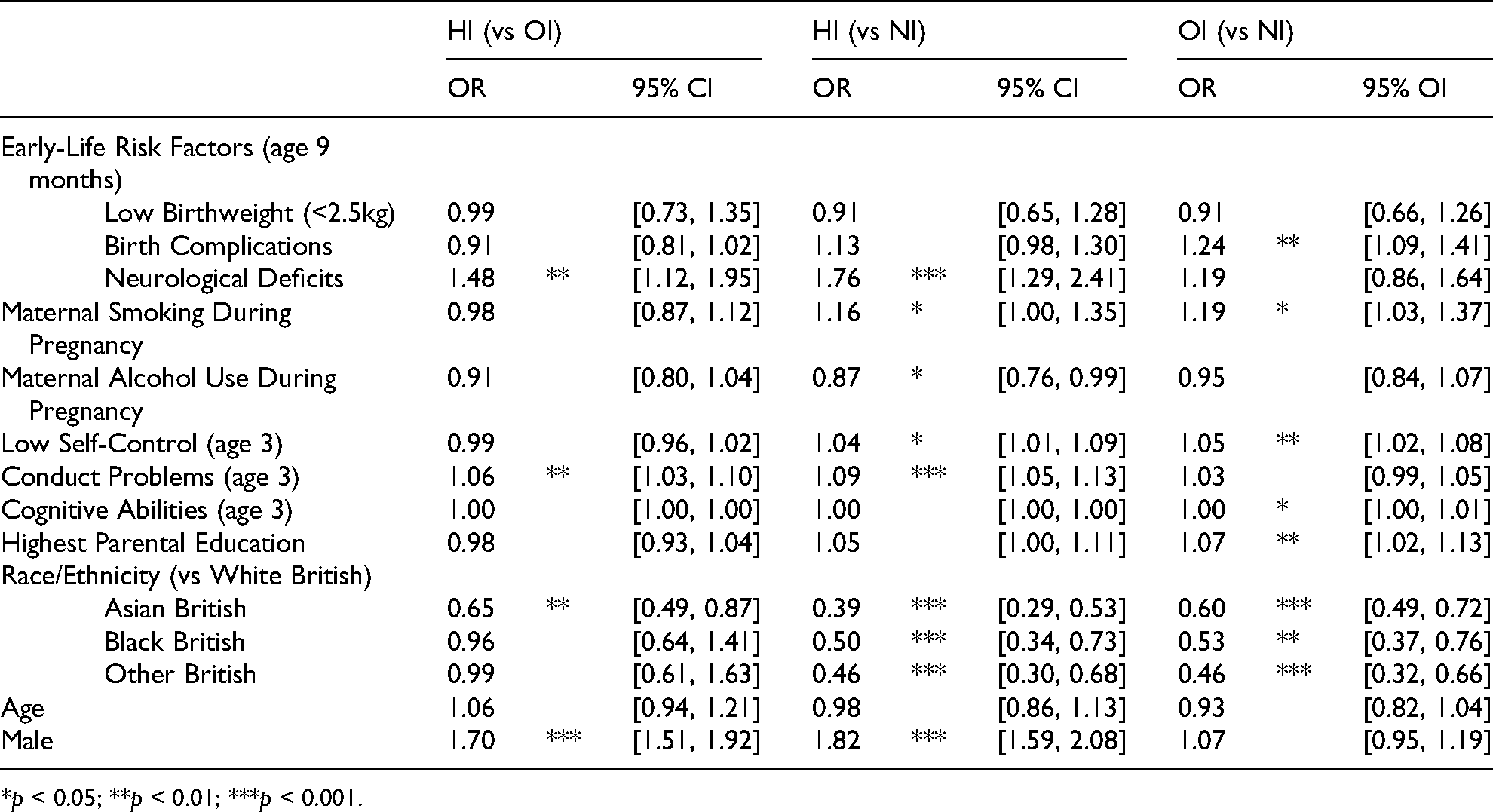
The results from the multinomial logistic regression examining how early-life risk factors predict injury status by age 11 years are presented in Table 2. Notably, several of the risk factors that are significant in distinguishing HI from NI are not statistically significant in distinguishing HI from OI. None of the measures of maternal substance use during pregnancy are predictive of HI when compared to OI. On the other hand, higher levels of conduct problems by age 3 years increases the odds of having HI versus OI (OR = 1.06, 95% CI [1.03, 1.10]), as does being male (OR = 1.70, 95% CI [1.51, 1.92]). In contrast, many of the risk factors identified are significant predictors of OI compared to NI, suggesting that there is something inherently different about people who are injured—regardless of where the injury occurred—and uninjured individuals. For instance, maternal smoking during pregnancy does not predict whether an individual is more likely to receive an HI over an OI, but it is a significant predictor of both HI and OI compared to NI. However, there are also covariates that appear to distinguish between those who incur an HI and both of the other reference groups, such as higher levels of conduct problems at age 3 and being male.
Multinomial Logistic Regression of Early-Life Risk Factors Predicting Injury Status Category (N = 11,714).
*p < 0.05; **p < 0.01; ***p < 0.001.
Injury Predicting Age 11 Delinquency
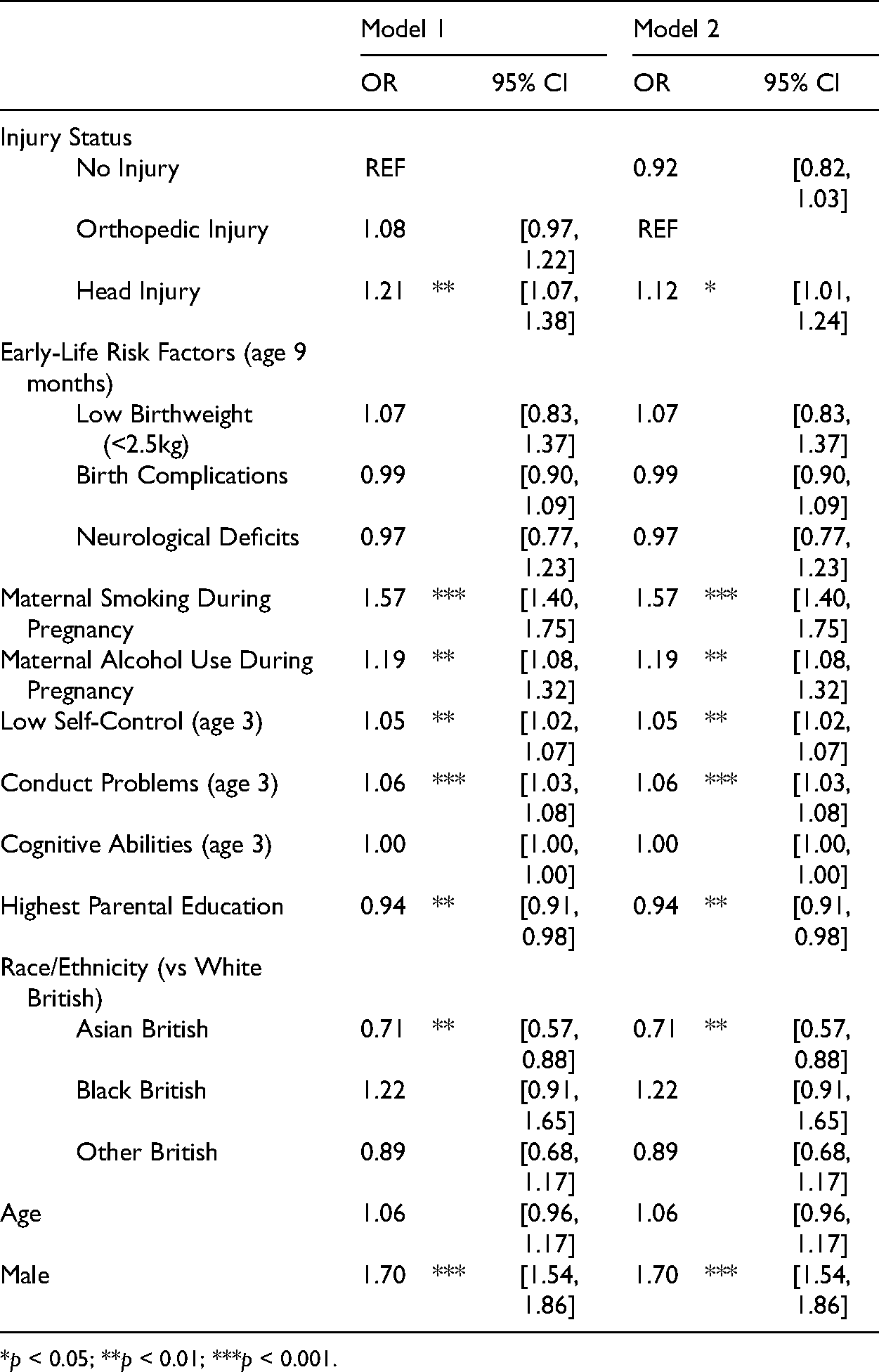
Table 3 displays the estimated odds ratios from the multivariable logistic regression of injury status predicting early-onset delinquency. Model 1 uses NI as a reference category, while Model 2 uses OI. As the only change between Models 1 and 2 is the reference category, the coefficients for model covariates are merely repeated. In Model 1, the effect of HI on early-onset delinquency is statistically significant (OR = 1.21, 95% CI [1.07, 1.38]). When using the more conservative test with OI as a reference category, HI is still significantly associated with early-onset delinquency, although the effect is attenuated. 4 Childhood HI increases the odds of being delinquent at age 11 by 12% (OR = 1.12, 95% CI [1.01 1.24]). Both maternal smoking and alcohol use during pregnancy increase the odds of early-onset delinquency. Being male drastically increases the odds of early-onset delinquency, compared to females (OR = 1.70, 95% CI [1.54, 1.86]).
Logistic Regression of Injury Status Category Predicting Delinquency at Age 11 (N = 13,287).
*p < 0.05; **p < 0.01; ***p < 0.001.
Injury Predicting Age 14 Delinquency
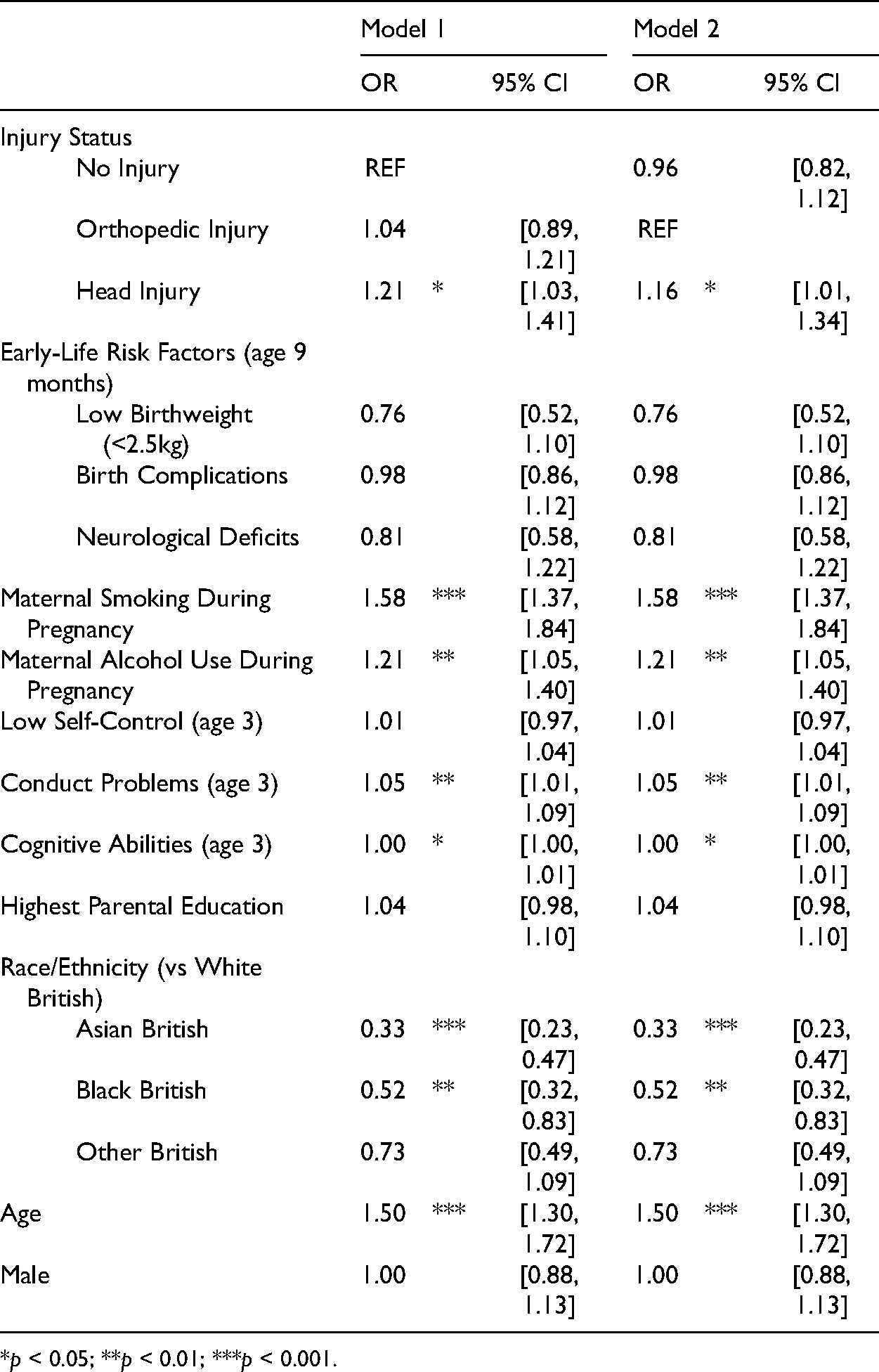
Table 4 displays the results from the multivariate logistic regression of injury status predicting adolescent delinquency. The sample size is reduced to 8,377 cases, as the model excludes those who have already reported delinquency onset by age 11. Similar to the previous results, childhood HI is a significant predictor of adolescent delinquency, regardless of whether it is compared to NI or OI. When comparing to OI, the estimated effect of HI is attenuated but is still statistically significantly associated with increased odds of delinquency onset (OR = 1.16, 95% CI [1.01, 1.34]). All other risk factors that were associated with age 11 delinquency onset are still statistically significant, with the exception of lower levels of self-control.
Logistic Regression of Injury Status Category Predicting Delinquency at Age 14 (N = 8,377).
*p < 0.05; **p < 0.01; ***p < 0.001.
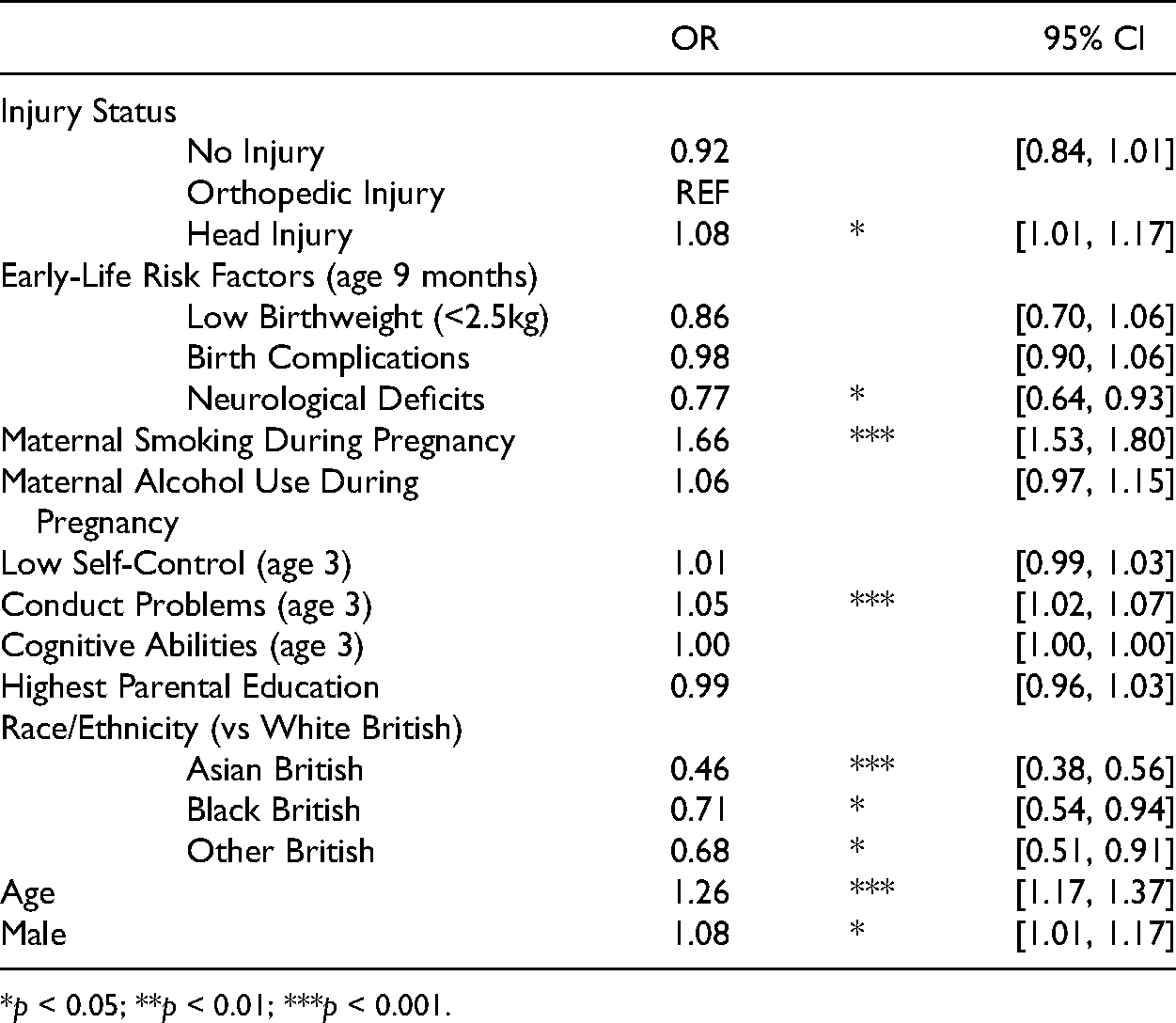
Injury Predicting Cumulative Delinquent Behaviors
Table 5 presents the estimates from a binomial regression of injury status on variety of delinquent behaviors exhibited by age 14 years. For this and the following models, OI is used as a reference group to obtain the most accurate and conservative estimates. When compared to OI, a history of HI is significantly and positively associated with variety of delinquency behavior. Those who have a childhood HI have an 8% increase in the odds of committing an additional delinquent behavior than those who have OI (OR = 1.08, 95% CI [1.01, 1.17]). Unlike previous models, neurological deficits are significantly associated with decreased odds of exhibiting additional delinquent behaviors (OR = 0.77, 95% CI [0.64, 0.93]). Maternal smoking during pregnancy increases the odds of additional delinquent behaviors at age 14 (OR = 1.66, 95% CI [1.53, 1.80]); however, maternal alcohol use during pregnancy is not a statistically significant predictor in this model. It is possible that these particular covariate estimates are due to suppression, as there is likely an underlying relationship between maternal alcohol use during pregnancy, diagnoses of neurological deficits, and delinquent behavior (van Hazebroek et al. 2019; MacKinnon, Krull, and Lockwood 2000).
Binomial Regression of Injury Status Category Predicting Cumulative Delinquent Behavior at Age 14 (N = 11,714).
*p < 0.05; **p < 0.01; ***p < 0.001.
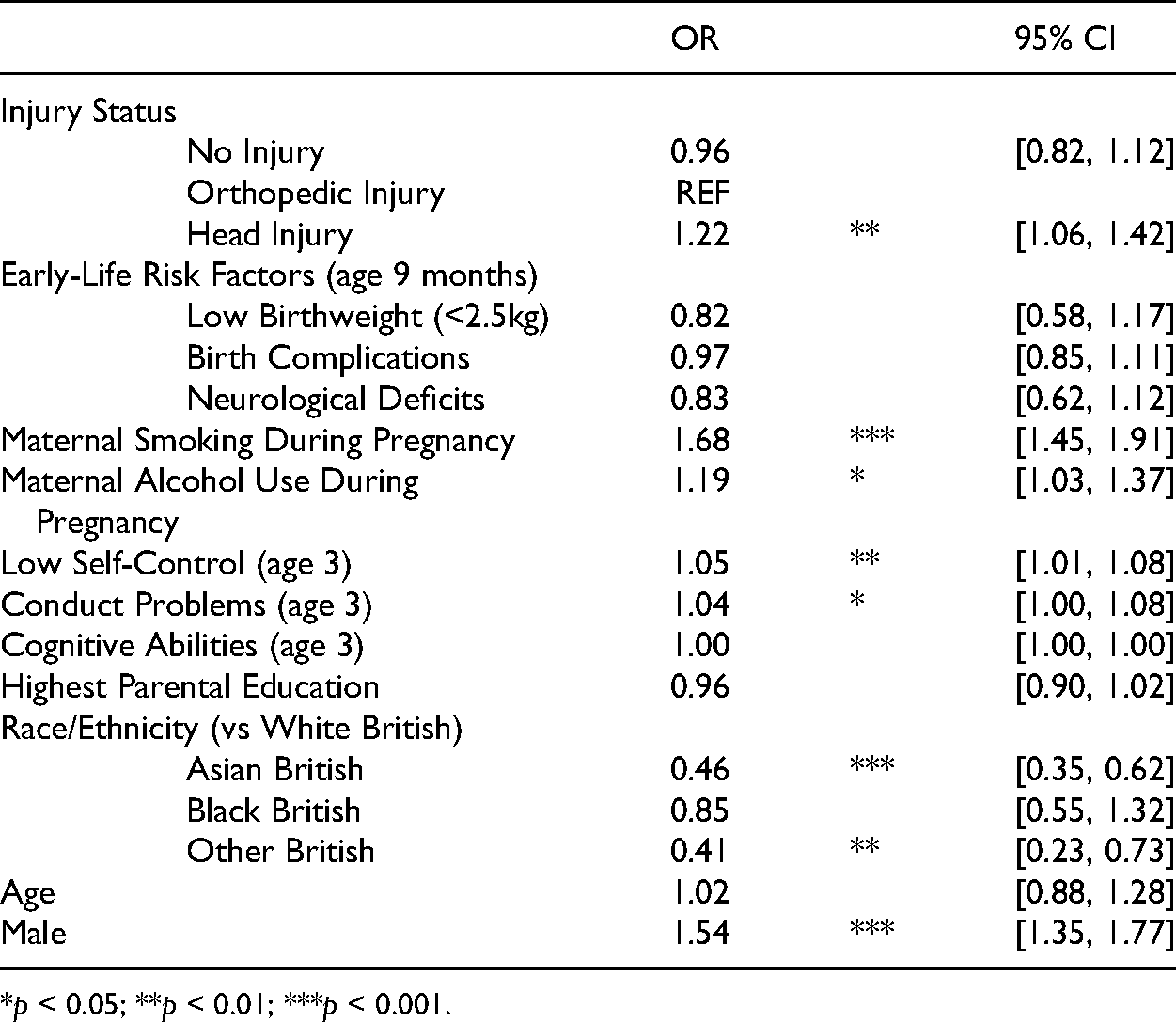
Injury Predicting Persistent Delinquent Behavior
The results from a logistic regression of injury status on persistent delinquent behavior from age 11 to age 14 years are shown in Table 6. A history of childhood HI is significantly associated with a 22% increase in the odds of sustained delinquent behavior (OR = 1.22, 95% CI [1.06, 1.42]), even when compared to those with OI. Once again, both maternal smoking (OR = 1.68, 95% CI [1.45, 1.91]) and maternal alcohol use (OR = 1.19, 95% CI [1.03, 1.37]) during pregnancy are significantly associated with persistent delinquent behavior over time.
Logistic Regression of Injury Status Category Predicting Sustained Delinquency at Age 11 and 14 (N = 11,714).
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
Developmental and life course theories have historically placed importance on early-life traumas as risk factors for later criminal behavior (Cauffman et al. 2005; Farrington 2006; Moffitt 1993; Moffitt and Caspi 2001; Staff et al. 2015), but the consideration of childhood head injury as one of these risk factors, or as an “acquired neuropsychological deficit” (Schwartz 2019) is a relatively new area of study. While increasing attention has been given to the relationship between HI and criminal behavior, a vast majority of studies examine this relationship in samples of adults or incarcerated adolescents (Connolly and McCormick 2019; Kennedy et al. 2017; Schwartz 2019; Schwartz et al. 2018), rather than in the general population. Much is still unknown about the influence of childhood HI on delinquency onset and persistence in adolescence, as well as potentially influential mechanisms. The relative dearth of studies on childhood HI is especially concerning, since they are likely associated with worse outcomes later in life than HIs that occur during adulthood, as is predicted by the latent deficit hypothesis (Benz et al. 1999; Fishbein et al. 2016; Guilhaume-Correa et al. 2020; Zhao et al. 2018). Additionally, consideration of HI as an “acquired neuropsychological deficit” (Schwartz 2019) offers further elucidation of its influence on later criminal behavior by introducing possible mechanisms that can be explored in future work, such as self-control and emotional dysregulation.
The present study explores the relationship between childhood HI and adolescent delinquency, while accounting both for other early-life risk factors identified by DLC theories and for methodological recommendations from clinical studies. Data from the MCS, a cohort study from the UK, are used to obtain prospective reports of HI throughout childhood and self-reports of delinquency in adolescence. DLC theories of crime provide reason to expect that childhood HI, as a neuropsychological deficit, would increase the likelihood of adolescent delinquent behavior onset—especially onset at an early age. Consistent with these expectations and prior research, the findings indicate that childhood HI is a consistent predictor of delinquency onset in early and mid-adolescence. Specifically, childhood HI is predictive of delinquency onset at both age 11 and 14 years, as well as persistence of and variety in delinquent behavior throughout these years. Together, these findings indicate that childhood HI is a theoretically and empirically relevant risk factor for initiation and persistence of criminal behavior, even when controlling for self-control and other early-life risk factors that could have rendered the relationship spurious. Additionally, the temporal restrictions of HI to those that occurred primarily before delinquency onset provides preliminary support for HI as a potential cause of delinquency, even in a general adolescent population. While the prevalence of HI within prison and jail populations is steep and concerning (Farrer and Hedges 2011; Frost et al. 2013; Kaba et al. 2014), an understanding of how HI might impact adolescents without prior criminal justice contact is equally important, especially if that HI might lead to increased risk of early-onset delinquent behavior (LeBlanc and Loeber 1990, 1998).
Unlike other studies of HI and delinquency, the present study explicitly examines childhood HI in relation to onset of delinquent behavior in a general population sample of adolescents. Connolly and McCormick (2019) examine a similar relationship in a sample of high-risk adolescents and find that mild traumatic brain injury is associated with increases in aggression and delinquency; however, the study is limited by its ability to assess the timing of these experiences, as well as the lack of a suitable comparison group. As studies on the effects of HI become more commonplace within criminology, it is important to incorporate theoretically relevant methodological considerations from clinical literature. The use of the OI group as a negative control represents one such methodological consideration. This negative control group is used to account for unobserved early-life risk factors that may influence the occurrence of both an injury and delinquent behavior, such as self-control (Gottfredson and Hirschi 1990), parental attachment, experiences of victimization, and participation in contact sports, to name a few.
The results reported in Table 2 indicate that the risk factors of experiencing an HI or an OI are relatively similar but tend to be distinct from those that would predict NI. As such, it is likely that there is something inherently different between those who remain uninjured and those are experiencing some form of injury (Bonow et al. 2019). Despite these similar risk factors, HI and OI have the potential for very different behavioral outcomes. However, it should be noted that these are not empirically derived control groups. In fact, there are certain risk factors, such as neurological deficits and being male, that appear to be uniquely associated with experiencing an HI. While the use of the OI group allows the statistical models to retain cases that might be lost in an empirically driven matching strategy, it does provide more conservative estimates than those that might be gleaned from either an empirically driven or an uninjured control group. Previous findings may then have overestimated the effect of HI when those who are injured are compared to uninjured peers. Following other recommendations (Kennedy et al. 2017; Milders et al. 2008; Yeates and Taylor 2005), the use of a negative injury control group is strongly recommended for future studies of head injury.
Although this study makes progress in expanding our understanding of acquired neurological deficits in childhood and their relation to delinquency, it is not without limitations. As is common in studies of HI within criminology, the sample used is not clinically defined. That is, those who report HI or OI have not necessarily been diagnosed by a physician or assessed according to a standardized scale. Instead, the sample is based on parent-reports of their child’s injuries, which cannot indicate the extent of neurological damage. Unlike clinical samples, severity cannot be assessed with the current data. Therefore, all HIs are treated as equifinal, as opposed to variable depending on injury severity. However, as previously mentioned, the use of the non-clinical sample does offer benefits in terms of generalizability, especially since, within this US, about half of individuals with mild HIs do not seek medical attention (Demakis and Rimland 2010). However, within this sample, over 90% received medical attention for their injuries, and this stark difference in estimates of medical treatment may be due to differences in the healthcare systems of the US and the UK. Additionally, because the overwhelming majority of individuals received some form of medical attention, the estimates presented in this study may be conservative, as proper treatment may mitigate negative consequences of HI.
Furthermore, this sample differs from many others in that the injuries are reported by parents. Parent-reports of injuries may suffer from social desirability bias, as parents may refrain from reporting injuries their child experiences in order to seem like more competent parents. Injuries might also not be reported by parents if the parents themselves were the cause of the injury, as is the case in abuse. On the other hand, parent-reports of early childhood injuries may be more accurate than retrospective self-reports. Forward telescoping and forgetfulness may plague self-reports of injury that occurred during childhood, especially at early ages. As the prevalence rates of HI are higher than those in similar studies (Connolly and McCormick 2019; Kennedy et al. 2017), it does not appear that parents were refraining from reporting the majority of injuries due to social desirability. On balance, these estimates presented here should not be biased by parent-reporting.
The nature of the data itself presents a couple of limitations. Notably, the ages utilized to illustrate early and normative delinquency onset are a product of the survey administration and not necessarily indicative of hard and fast cutoff points in distinguishing adolescent delinquency. Furthermore, as only two waves of data regarding delinquent behaviors were available, the measure of persistence of delinquency is limited. Ideally, future work may be able to better assess how HI impacts trajectories of delinquent behavior over time.
Additionally, the phrasing of the age 11 delinquency questions does not allow for causality to be firmly established, as the behaviors reported could have occurred prior to the HI in question. In one set of supplementary analyses (available online), the HIs were restricted to only those that occurred between the ages of 3 and 7 years, and the resulting estimates were actually greater than those shown in Table 3. However, even this restriction does not necessarily allow for causal identification, as it is still possible that some of the delinquent behaviors reported at age 11 occurred prior to 7 years of age. Yet another set of supplementary analyses estimates the relationship between HIs from ages 3 to 7 and cigarette use initiation after age 8 years, as this was one delinquent behavior with additional nuanced information available. Once again, these estimates indicate that HI during childhood is associated with onset of delinquent behavior and help further establish temporal ordering.
Lastly, this study is currently limited in its ability to assess mechanisms underlying possible behavioral changes after HI, something that future work should continue to explore. The neurological damage and subsequent changes in function that can arise after HI are not explicitly included in the present analyses. There is reason to believe that changes in self-control (Schwartz et al. 2017; Schwartz et al. 2018), moral reasoning (Schwartz, Fitter, and Jodis 2020), and emotional regulation (Milders et al. 2008) are more proximate causes of criminal behavior than the injury itself, which suggests that mechanisms underscoring the relationship between HI and delinquency are of importance for future studies. Although HI may be a precipitating factor, it is likely to be a more distal cause of delinquent behavior. To some extent, this might explain why the effect sizes for these estimates are relatively weak. 5 Additionally, the effect sizes of the present estimates may be smaller than expected due to the use of the OI comparison group (see Bonow et al. 2019 for a similar case) and due to the wide variety in severity of HI.
Overall, the present study implicates HI as a somewhat robust early-life risk factor for delinquent behavior. The majority of prior criminological studies of HI focus on prevalence rates and correlates of injuries within offender samples (Perron and Howard 2008; Schwartz et al. 2017, 2020; Vaughn et al. 2014). While much of this literature points to HI as influential in the initiation of criminal behavior, very few studies have been able to assess this relationship longitudinally and in a sample of non-incarcerated individuals (Bonow et al. 2019; Connolly and McCormick 2019; Kennedy et al. 2017). Others have examined how HI might impact the persistence of criminal behavior and the likelihood of recidivism, with conclusions pointing to repetitive criminal justice contact following an HI (Ray and Richardson 2017; Schwartz 2021). The present study contributes to biosocial and DLC criminology in finding that HI can and should be considered an acquired neuropsychological risk factor for the initiation and persistence of adolescent delinquent behavior, even among the general population. Those who experience a childhood HI are at increased risk of early-onset delinquency and are likely to be subject to many of the deleterious outcomes that follow early-onset delinquent behavior (Farrington 2006; LeBlanc and Loeber 1990, 1998). Additionally, the temporal restriction of HI to those that occur prior to delinquency lends support for a potentially causal relationship, something that other work is beginning to explore further (Schwartz 2021). Regardless, childhood HI does appear to be a meaningful and important risk factor for onset of adolescent delinquent behavior,
The present findings only scratch the surface in uncovering the nuance within the relationship between HI and criminal behavior. Future research should continue to explore the mechanisms underscoring this relationship, as well as the possible moderating effects of injury timing during childhood, in order to capture some of the vast variation in the behavioral outcomes following HI. Furthermore, the roles of these possible cognitive mechanisms may lead to developments in DLC and biosocial criminological theory, as we gain increasing insight into the neuropsychological risk factors for delinquent and antisocial behavior. Uncovering more of the nuance in this relationship may help shed light on how HI acts as a precipitator for criminal involvement and how we might intervene—either before or after injury—in order to mitigate the deleterious outcomes that could follow these adolescents throughout the life-course.
Supplemental Material
sj-docx-1-jrc-10.1177_00224278221081140 - Supplemental material for Childhood Head Injury as an Acquired Neuropsychological Risk Factor for Adolescent Delinquency
Supplemental material, sj-docx-1-jrc-10.1177_00224278221081140 for Childhood Head Injury as an Acquired Neuropsychological Risk Factor for Adolescent Delinquency by Jessica Mongilio in Journal of Research in Crime and Delinquency
Footnotes
Acknowledgments
I would like to thank Jeremy Staff, Tom Loughran, Pam Wilcox, and Denni Fishbein for their support and suggestions throughout the duration of this project. Additionally, I would like to thank the anonymous reviewers for their feedback on earlier versions of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is based on analysis of data from the UK Millennium Cohort Study (MCS), which receives core funding from the Economic and Social Research Council UK (ESRC) and a consortium of UK government departments. Measures of alcohol use at age 11 in the MCS were supported by grant AA019606 from the National Institute on Alcohol Abuse and Alcoholism. The study sponsors played no role in the study design; collection, analysis, nor interpretation of data; the writing of the report; nor the decision to submit the manuscript for publication.
Notes
Supplemental material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.