
Abstract
2019 has been the most violent year on record for health workers in the Democratic Republic of the Congo. Attacks on healthcare coincided with the first-ever Ebola outbreak in an active conflict zone. Many of the attacks on the Ebola response were perpetrated by civilians who intended to disrupt the response, which in turn contributed to the spread of the virus. Why would communities attack the very people trying to protect them from disease? This mixed-method study examines the case of violence against Ebola responders during the Democratic Republic of the Congo’s tenth Ebola outbreak from 2018 to 2020. First, an ‘explaining-outcome’ process tracing reconstructs key events that led to the violent resistance of the population. I find that – contrary to popular belief – distrust alone was not the main driver. Rather, I argue that the politicization of the response provoked violent popular resistance. Second, an interrupted time-series model shows that the exclusion of three regions from the presidential election due to Ebola led to a significant increase in attacks on Ebola responders. The analysis demonstrates that the behavior of healthcare responders has limited ability to build trust when other political dynamics are at work. The article illustrates how combining process tracing with quantitative causal inference methods enables the simultaneous inquiry of cause, mechanism, and effect.
Keywords
The paradox of popular violence against healthcare
2019 has been the most violent year on record for health workers in the Democratic Republic of the Congo (DRC) (WHO, 2020). Attacks on healthcare coincided with the first-ever Ebola outbreak in an active conflict zone. Many attacks against the Ebola response were perpetrated by civilians and aimed at disrupting the response, which in turn contributed to the spread of the virus (Wells et al., 2019). For example, on 15 September 2019, civilians reportedly set four medical facilities and 18 houses for Ebola responders on fire. The local community accused the Ebola responders of killing people and disguising their deaths as resulting from Ebola so that they could continue to receive humanitarian funds (Insecurity Insight, 2019).
Why would communities attack the very people who were trying to protect them from a deadly virus? This mixed-method study examines the case of violence against Ebola responders during the DRC’s tenth Ebola outbreak from 2018 to 2020. My main argument is that popular violent resistance is not solely the result of distrust. Rather, political exclusion served as a tipping point. In the midst of the Ebola outbreak, presidential elections were held in December 2018, with some Ebola-affected provinces barred from voting. According to the government’s official statement, it was a health measure to contain the virus. However, the affected regions were an opposition stronghold. After the election exclusion, local elites and media framed Ebola as a political tool of the government, resulting in popular resistance to Ebola responders.
Section two presents an overview of explanations for popular resistance to healthcare. Health policies that target the population unequally can become politicized, leading to violent resistance. Section three proceeds with a brief background on the DRC and the tenth Ebola outbreak. In section four, I begin my search for an explanation with an ‘explaining-outcome’ process tracing. The ‘shoe-sole’ work reconstructs the sequence of key events and perceptions during the Ebola response. I find that, contrary to popular belief, distrust alone was not the main driver of violence against Ebola responders. I propose that the politicization of the health emergency provoked large-scale violent popular resistance. In section five, I test the correlation of the novel mechanism in an interrupted time-series model. The analysis shows that in the weeks after the election exclusion, violence against Ebola responders increased sharply. Section six provides a brief discussion of how the response became depoliticized over time and gives concluding remarks.
This article makes several contributions. First, it advances debates about aid and healthcare politicization by illuminating the link between repressive regimes and public perceptions. Seemingly neutral health measures can become politicized when they cannot be distinguished from other repressive government measures. Second, the article adds to the literature on micro-dynamics of violence by demonstrating when not only armed groups but also civilians become perpetrators. Finally, the article shows how combining process tracing with quantitative causal inference methods allows for the simultaneous inquiry of cause, mechanism, and effect.
Explanations for violence against healthcare
Popular resistance to healthcare workers during emergencies is not a new phenomenon; it has been observed during previous epidemics in response to restrictive healthcare measures. The best-documented cases are the European cholera outbreak of the 1830s and the 2013/14 West African Ebola epidemic.
During Europe’s first cholera epidemic in the 1830s, riots raged across the continent, destroying entire cities and torching healthcare facilities. Doctors and nurses were required to implement strict government health measures, such as isolating the sick and quarantining people. The surveillance-based healthcare strategies instilled public distrust and fueled the spread of conspiracies (Cohn & Kutalek, 2016). People in France believed that the wealthy elite had ordered doctors to poison the water supplies of the poor (Evans, 1988). The professionalization of surgeons in Britain increased the demand for human cadavers. Fear gripped the populace that doctors were conspiring against the poor to preserve their bodies for experiments (Tognotti, 2013).
During the 2013/14 Ebola epidemic in West Africa, violent mobs protested and attacked aid workers, burning down healthcare facilities and destroying provisional treatment facilities. Due to the risk of infection, the dignified burial of disease victims was a source of contention. Fears that the state had poisoned or buried the patients alive provoked riots and protests, including attacks on health workers and the burning of treatment facilities (Cohn & Kutalek, 2016).
These previous resistance movements demonstrate that government-imposed healthcare strategies, even when well-intended, can become politicized when they disproportionately affect certain groups. The riots were sparked by distrust of the government’s intentions behind the healthcare measures, not by the epidemic itself.
Literature on violence against aid workers during humanitarian emergencies looks at the individual behavior of humanitarians (Fast, 2014), criminal violence driven by economic motivations (Buchanan & Muggah, 2005; Naylor, 1997) and political motivations of organized armed groups (Anderson, 1999; Lischer, 2006; Narang & Stanton, 2017; Sauter, 2017; Stoddard, Harmer & DiDomenico, 2009). The explanations are mostly based on structural factors that could explain why the phenomenon occurs more frequently in some contexts than in others. However, they do not specifically address violence against healthcare or the circumstances in which civilians are the prevalent perpetrators. In contrast, the literature on violence against healthcare is driven by medical and health researchers who analyze the lived experiences of healthcare personnel. The majority of these studies identified frustrations and misunderstanding with medical services as the causes of this violence (Haar et al., 2021; ICRC, 2020). These studies cannot explain why violence against healthcare is more widespread in some cases.
An epidemic can be used to violently manifest state power. Health security, defined as protection from threats to health, is often blurred with national security, defined as threats to sovereign power (Benton, 2017: 32). Securitization is a discursive process that declares a specific issue to be an existential threat. Securitizing an issue gives a government the authority to take emergency measures that may violate legal constraints and democratic principles (Buzan, Wæver & De Wilde, 1998).
The United Nations (UN) Security Council Resolution 1308 on HIV/AIDS, passed in 2000, was the first UN document to frame a health issue as a threat to international security (Davies, 2008). Ebola was first securitized during the West African outbreak, due to its deadly nature and fast cross-border spread. In September 2014, the UN declared the outbreak ‘a threat to international peace and security’. 1 Framing a disease in security terms allows governments to impose health measures that limit individuals’ rights through curfews and lockdowns. These measures, often aimed at restoring state power, hit the poor disproportionately. Resistant communities that do not comply become a threat to national security (Caremel, Faye & Ouedraogo, 2017; Enemark, 2009).
Healthcare measures aimed at containing the spread of a virus can resemble repressive governments’ policies aimed at suppressing opposition. Healthcare policies become ‘observably equivalent’ to other forms of repression. As a result, the public is unable to differentiate between health policies and political repression (Barceló et al., 2022). At the same time, healthcare emergencies enable governments to engage in ‘opportunistic repression’, limiting civil liberties for ostensibly legitimate reasons. During the COVID-19 pandemic, for example, repressive states imposed more violent lockdowns, and repression in opposition areas intensified (Grasse et al., 2021).
The public’s perceptions matter. Persistent economic or political inequalities can undermine trust in the state and exacerbate violent conflict (Horowitz, 2001; Muller & Seligson, 1987). During the West African Ebola outbreak, health measures restricting individual liberties sparked civil unrest in areas where trust in the state was low (González-Torres & Esposito, 2020).
People’s trust is strained in conflict-affected areas (Kijewski & Freitag, 2018), and trust towards out-groups is generally lower than towards the in-group (Cassar, Grosjean & Whitt, 2013). Identity politics combined with discrimination or oppression fuels violence (Gurr, 2000; Horowitz, 2001). When some groups are politically excluded from state authority, group-level grievances can facilitate mobilization and fuel violent conflict (Cederman, Gleditsch & Buhaug, 2013; Gurr, 2000; Østby, 2008; Stewart, 2008). Excluded groups resort to violence when their grievances are strong enough. Local leaders can mobilize deprived groups through an ‘injustice framing process’. When injustices are attributed to a particular actor, negative emotions can turn into violence (Benford & Snow, 2000). During this framing process, disinformation campaigns play an important role in mobilizing the masses (Snyder, 2000). According to the backlash hypothesis, people respond to repression in the short or long term with violent or nonviolent civil resistance (Carey, 2006; Khawaja, 1993). This article contributes to the discussion by demonstrating that a violent backlash may emerge, not against government agents, but against those who have to enforce the healthcare measures.
If healthcare policies have a negative impact on a certain part of the population, a vicious cycle of distrust of the state and the virus emerges. Humanitarians are mostly outside actors and need government permission to do their work. As a result, the public may believe that healthcare responders are government agents seeking to enforce repressive policies. When health policies cause already disadvantaged parts of the population to be further disadvantaged, conspiracy theories about government intentions and the realities of the health emergency can quickly emerge. Rumors portray the health emergency as a political tool of the government. Local leaders can incite the populace, leading to an escalation of violence. As a result, I expect that discriminatory health policies are a source of conspiracies and thus a potential danger to healthcare respondents.
The tenth Ebola outbreak in the DRC
On 1 August 2018, the Ministry of Health declared the tenth Ebola outbreak in the country (WHO, 2018a). The virus extended across North Kivu and Ituri provinces and later spread into South Kivu province (Oxfam, 2018). By the end of the outbreak in March 2020, 3,462 cases had been recorded, including 2,262 deaths, making it the second deadliest outbreak in the world after the 2013/14 West African outbreak.
The Ebola outbreak was not only the first in an active conflict zone, but it was also located in the country’s most violent region. The Kivus are an opposition stronghold that has been subjected to extreme violence. In 2018, the two Kivu provinces were home to over 130 different armed groups with varying political and ideological agendas. The conflict’s main hotspot is in Beni territory where more than 31% of all civilian casualties were recorded in 2018, the majority of which were committed by government forces (Congo Research Group, 2019: 10). The conflict and the virus were mutually reinforcing. More violent regions were more vulnerable to the disease, and the spread of the virus further destabilized already fragile regions (Kraemer et al., 2020).
The conflict in the eastern DRC is based on group identities rooted in unequal access to citizenship and related landownership rights (Autesserre, 2010; Bøås & Dunn, 2014). Decades of violent conflict, including grave human rights abuses by the government, led to political and social grievances. Throughout the last century, Western powers have led numerous humanitarian interventions, making the local population suspicious of outsiders. The ‘peacekeeping culture’ ignored local bottom-up approaches, failing to recognize the link between distrust and colonial legacy, land tenure, and citizenship issues in the eastern provinces (Autesserre, 2010; Kabemba, 2013). Although there are ethnic tensions in eastern DRC, the conflict is not exclusively ethnic. Persistent economic and political inequalities undermine trust in the state and exacerbate violent conflict.
During the tenth Ebola outbreak, 566 violent incidents took place against Ebola responders, 525 of which occurred in 2019 alone (see section five for data sources). The perpetrators ranged from organized armed groups to popular mobs. Since many of the attacks were carried out by civilians, it can be assumed that the incidents were not mere crossfire events in the conflict. The high level of violence directed at Ebola responders makes the 2018–20 Ebola outbreak an extreme case on the outcome that can be used to explore a novel mechanism (Seawright & Gerring, 2008: 302).
Resistance by individuals and families was typically targeted against prevention activities, such as isolating sick patients, vaccination campaigns or removing corpses. For example, on 11 January 2019 in Marabo town in Ituri province, local taxi drivers and other residents threw rocks at health workers because they opposed the construction of an Ebola isolation center. On 17 May 2019, two burial teams were attacked by mobs throwing stones in Butembo and Bunia (Insecurity Insight, 2020a). In Beni town in June 2019, residents threw stones at vehicles for the Ebola response. They were enraged at the politicians and health workers in the cars for not stopping at the checkpoints to wash their hands (Maxmen, 2019b).
Communities targeted not only Ebola responders but also those cooperating with the response, prompting the World Health Organization (WHO) to change its vaccination strategy. Initially, vaccination centers were set up as close as possible to the homes of the contacts of a sick person. After neighbors murdered a vaccinated man and accused him of ‘helping bring Ebola to our area’, a new system allowed the vaccine to be obtained in nearby towns to avoid being observed by neighbors (Maxmen, 2019a).
Explaining the popular violent resistance
This section proposes a novel mechanism explaining why violence against Ebola responders was so common during the DRC’s tenth outbreak, and why so many attacks were perpetrated by local communities. First, I provide an overview of the method, data, and operationalization, followed by the results of the process tracing analysis.
Method and data
Following Wight (2004: 290), I define mechanisms as a ‘sequence of events and processes that lead to the event’. Beach & Pedersen (2019: 284) state that ‘providing a full account of an outcome requires including reasons that are complex and case specific’. This means that mechanisms, or their parts, can be unique and are not necessarily generalizable to other cases. While the findings as such cannot be generalized, some elements of the explanation may be more general and can ‘point outwards’ (Beach & Pedersen, 2019: 285).
The bottom-up shoe-sole work of explaining-outcome process tracing begins with the outcome and works backward in an iterative research strategy. In contrast to theory-testing process tracing, which seeks to unravel a causal mechanism of an already established correlation between cause and outcome, explaining-outcome process tracing seeks to find a cause to an outcome through the mechanism. It can be understood as a ‘minimally sufficient explanation’ accounting for the main aspects of an outcome (Beach & Pedersen, 2019: 282–283).
I use three main public sources. The first are Situation Reports (SITREPs) from international organizations. During humanitarian emergencies, international organizations usually publish monthly, bimonthly or quarterly updates. Due to the scale of the world’s second-worst Ebola outbreak, the WHO issued 92 SITREPs between August 2018 and May 2020. The weekly updates provided an unusual wealth of information and allowed the unfolding of the humanitarian response to be tracked in detail. The reports not only described the latest epidemiological developments and updates from the response but also analyzed sociopolitical events and sentiments in the population.
Causal mechanism
Thirdly, SSHAP also provided irregular updates from media monitoring. Messages in popular messenger channels, but also public statements from local or national politicians and civil society organizations were collected. The media monitors unveil the messages of local and national leaders to the population. I triangulate the relevant information with resources that were less systematic (neither standardized nor periodic) such as local newspaper articles, practitioner accounts from the field, and less frequent SITREPs from other organizations involved in the response. The process tracing sources are cited throughout the document, but the bibliographical overview is in the Online appendix for space reasons.
Although interviews and other interactive research methods are currently the preferred standard for process tracing, relying on documents produced during the crisis does have several advantages over other data types. Since the Ebola outbreak is over, it would not have been possible to research the issue first-hand. SITREPs document events and rapid surveys grasp perceptions in real-time. This is more reliable than retrospective memories of selected actors (Schwartz & Straus, 2018).
These sources have some limitations. International organizations have their own interests and are dependent on donors or member states. Hence, they may attempt to portray their own actions in a more favorable light. However, I am more interested in the events surrounding the response and less in the actual actions. Furthermore, rapid surveys in the field may not follow rigorous research standards. Random sampling may not be possible due to access restrictions. Communities may have their own reasons for responding to the survey; for example, they may answer questions more positively in the hope of receiving humanitarian aid. Still, the regular iterations of both document types provide insights on how the response and perceptions changed over time.
Process tracing analysis
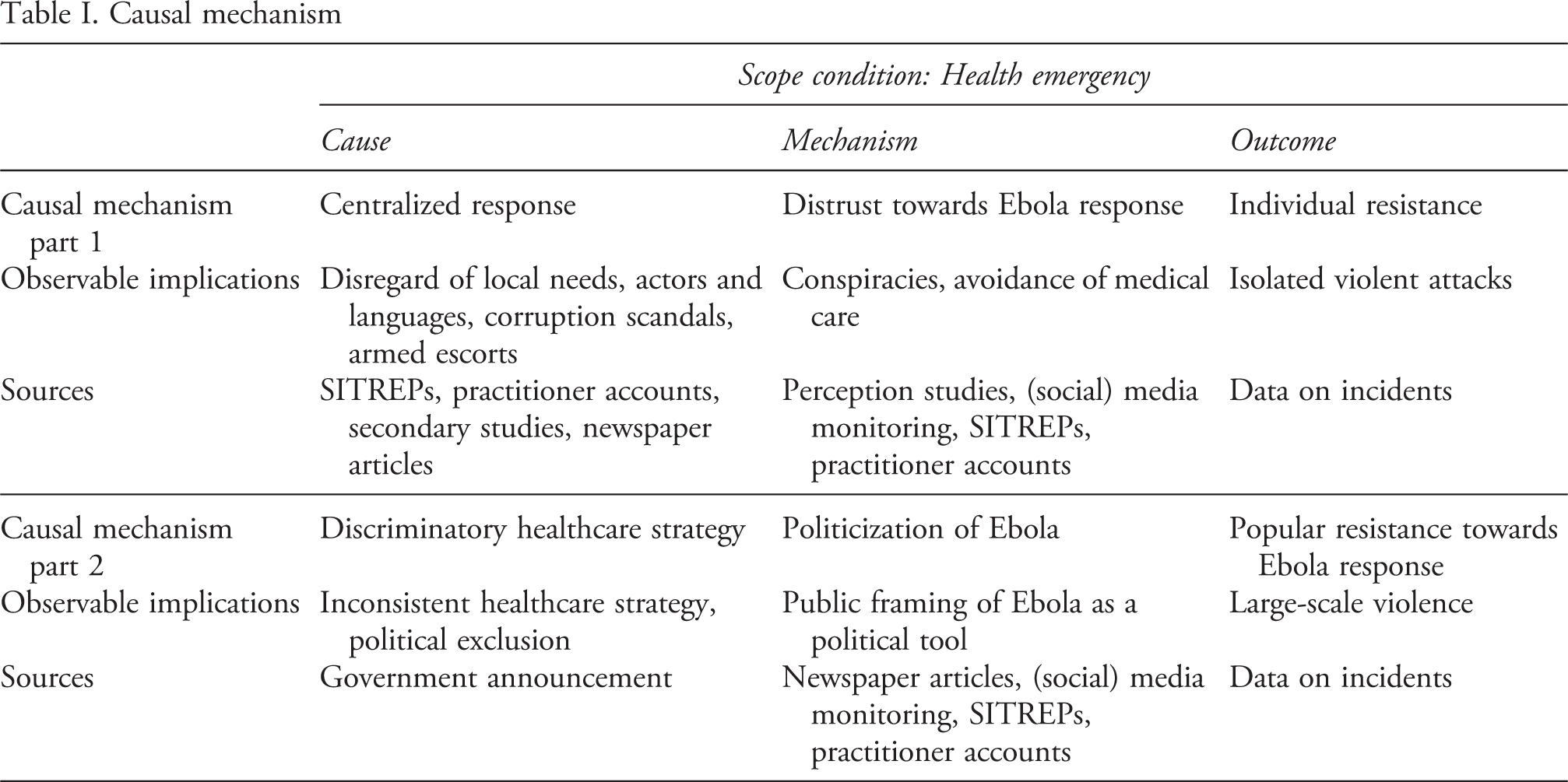
Table I presents the causal mechanism, divided into two parts, leading to popular resistance against Ebola responders. For each part, the first row outlines the causal mechanism, the second row illustrates the observable implications of the causal mechanism, and the third row shows the sources used to trace the observable implications.
I began the process tracing analysis by looking into the narrative of distrust. The upper part of Table I outlines the first part of the proposed mechanism. The spreading of rumors and conspiracies about Ebola and the response are empirical observables suggesting that a significant part of the population distrusted the response. This is also manifested in the widespread avoidance of Ebola Treatment Centers (ETCs). The content of the rumors makes it clear that the lack of trust was related to how the response was organized. Local actors were not involved in the planning and implementation of the response, communication materials were not translated into local languages, and medical staff were from other regions or countries. These empirical observables point to a centralized response that was detached from local communities. In addition, Ebola responders were often accompanied by armed escorts who had a track record of abusing the local population, and some high-ranking national politicians embezzled Ebola money. These actions and approaches linked the Ebola response to an unpopular government regime. However, the following empirical analysis will make clear that the distrust mechanism can explain isolated incidents but is insufficient in explaining widespread popular violence.
I propose a second cause, namely the discriminatory healthcare strategy of the government, which acted as a tipping point and politicized Ebola, as outlined in the lower part of Table I. Local elites publicly framed Ebola as a political tool after the government had excluded some Ebola-affected regions from voting in the presidential elections. This agitated the population against Ebola responders, which resulted in large-scale popular violent resistance. In line with what the literature on ethnic mobilization and group-based grievances suggests, the horizontal inequality of disenfranchised regions mobilized civilians to attack what they deemed as enforcers of a repressive political agenda. The injustice framing process of local leaders and media helped mobilize the masses.
In short, distrust can account for isolated incidents. However, it is insufficient to explain widespread popular resistance. The politicization of the response was the necessary tipping point for popular violent resistance.
A matter of distrust?
Several newspapers (Al Jazeera, 2019; Freudenthal, 2019), as well as humanitarian organizations involved in the Ebola response (Kleijer, 2020; Newport, 2020), argued that attacks on Ebola responders were motivated by ‘distrust’. A lack of community engagement, according to the argument, resulted in negative local perceptions. This fueled mistrust in the Ebola response, leading to violence.
The spread of wild rumors and conspiracy theories implies that large parts of the population did not trust the virus and the response. According to surveys conducted in September 2018 in Beni and Butembo, more than 30% of respondents believed that Ebola was fabricated for financial or political gain, while about 25% did not believe in Ebola at all (Vinck et al., 2019). What caused these rumors? Furthermore, is distrust a sufficient mechanism in explaining the upsurge in popular resistance against Ebola responders?
Centralized response
Immediately after the announcement of the Ebola outbreak in August 2018, international medical teams deployed swiftly to support the national Ebola response, which was co-led by the government and the WHO (WHO, 2018a). The actors involved were in silent agreement that speed was more important than other factors such as community engagement. The specific needs or cultural customs of affected populations were not taken into consideration (WHO, 2019).
One manifestation of this centralization and the disregard for local needs was the issue with language. Regular updates on the state of the outbreak were only published in French, English, or formal Swahili; these are languages that were not understood by locals (Farrar, 2019). Translators without borders (2020) found that in September 2019, more than one year after the outbreak was declared, most Ebola communication material was still produced in English, French, or formal Swahili.
The sudden influx of vast amounts of international money, combined with a system that needed to act quickly, created the ideal environment for nepotism and corruption. National and regional politicians competed for well-paying positions. The term ‘Ebola business’ arose, referring to how some people made a lot of money as a result of Ebola, while the majority of the affected communities suffered. For instance, officials in Butembo charged between $1,800 and $3,000 a month to rent their private car to the response while working for the same organization. A WHO adviser said: ‘You don’t need a degree in finance to realize that [it’s bad] to rent a vehicle from someone who works in the response […] When other people see this, it creates distrust’ (Freudenthal, 2020).
Three Congolese doctors from the Ministry of Health were arrested in spring 2019 on suspicion of ordering the murder of a WHO epidemiologist. David Gressly, the former UN Ebola emergency coordinator, assumed that ‘the attack on the WHO doctor may have been motivated by a desire to divert resources to local health workers’. Furthermore, the then Minister of Health, Oly Ilunga, was accused of embezzling Ebola money and had to resign from his post (Freudenthal, 2020). The corruption scandals were reported in the local media and led to public outrage (Sengeya, 2019). The corruption business not only led to a negative perception of the Ebola response but also linked it directly to the ruling party.
Another factor was fear of state abuse. The Kivus have a history of grave human rights abuses on the civilian population by state actors. Due to the insecurity in the Kivu regions, armed escorts often accompanied medical staff, for example to enforce ‘safe’ burials (Bedford et al., 2018). Instead of explaining to the community why they could not touch the bodies of the diseased, police would shoot in the air to clear away gatherings during burials (Freudenthal, 2019). Several aid organizations released statements protesting the use of armed escorts. MSF described the practice as ‘militarization’ of the response (Miles, 2019), and the Red Cross explained that armed escorts ‘may aggravate the tensions that already exist between communities and responders’ (IFRC, 2019). The national response strategy focused on strengthening surveillance, active case-finding, and contact monitoring. Enforcing this strategy with armed guards made the population feel that they were being hunted by the government.
The nature of the virus and the conditions of the healthcare system exacerbated negative perceptions. Firstly, most medical centers treated Ebola patients only even though most care-seekers were sick from other serious illnesses. Non-Ebola patients were rejected from accessing treatment. The population was wondering why all the money was limited to Ebola patients only, while people suffered from all sorts of grievances related to the conflict, economic deprivation, and other health problems (Nguyen, 2019).
Precarious conditions in the healthcare system led to infections among healthcare personnel, creating a vicious cycle. Patients seeking care for other illnesses got infected by nurses or doctors. Medical facilities were associated with inevitable Ebola death. Despite the availability of vaccines, around 60–70% of infected patients died (Nguyen, 2019). People believed that whoever ‘gets taken’ into ETCs would disappear or die and that this was orchestrated by the government. Due to the deadly nature of the virus, the rumors were not unfounded and expressed a real fear. However, they evolved into conspiracy theories that claimed healthcare workers were collaborating with the government to infect people and wipe out the Kivu population (Bedford et al., 2018, 2019). Advocacy campaigns were ineffective in countering the distrust narrative because most healthcare workers were not from local communities and communication materials were not available in the local languages. But the narrative cannot answer why popular resistance turned violent, for two reasons. Distrust was more likely to lead to avoidance, and Ebola responders increased community engagement over time.
Firstly, if you distrust doctors, you simply stay away from them. Many communities preferred seeking advice from traditional bush doctors or fled ETCs despite having symptoms of Ebola. Regional governments began providing free health services to encourage the population to seek professional medical care. The free services, while well meant, had an unexpected negative response. People believed that healthcare workers needed to make up for lost income by sending more people to the ETCs. These beliefs in a government conspiracy led people to stay away from state institutions (Carter & McKay, 2019). A field doctor found that communities were less cooperative with public health measures where Ebola responders were accompanied by armed guards. ‘The lesson is clear: guns and public health don’t mix. Epidemics thrive on fear – when they are frightened, patients flee hospitals, sick people stay away to begin with, and affected communities distrust groups trying to respond to the epidemic’ (Nguyen, 2019: 1299). This suggests that people may have distrusted the response, but distrust led to avoidance rather than violence against Ebola responders.
Secondly, SITREPs document how over time the response has become more local and the communities more involved. The WHO first reported on resistance in the community on 23 October 2018 and recommended adapting ‘strategies to the context of insecurity and high community resistances’ (WHO, 2018: 5). Beginning in January 2019, the WHO published weekly key indicator surveys tracking all response activity, demonstrating that community engagement significantly improved week after week (see Online appendix B.1). If suspicion of the centralized response was the main driver behind the attacks, the number of incidents should have decreased in early 2019. However, Figure 2 shows that the violence increased dramatically in the first half of 2019.
Past Ebola outbreaks indicate important cross-case variation. During the West African outbreak, the response was similarly centrally organized as in the DRC, fueling distrust (Benton, 2017). In Guinea, for example, people believed that Ebola was planted by the state to regain control, win elections, and legitimize the use of armed force (Caremel, Faye & Ouedraogo, 2017: 68). While isolated attacks against Ebola responders occurred, it was never a widespread phenomenon. The comparison with past cases demonstrates that distrust alone does not necessarily lead to large-scale violence.
Discriminatory healthcare strategy
What happened in early 2019 that suddenly increased violence against Ebola responders? In the midst of the outbreak, the presidential elections took place in December 2018, from which more than a million eligible voters were excluded. The electoral commission argued that due to the rapid spread of the virus, it would be too dangerous for large crowds to gather in polling stations (Le Point Afrique, 2018).
The presidential election was originally planned for 2016 but had been postponed to 26 December 2018. In Map of provinces in the DR Congo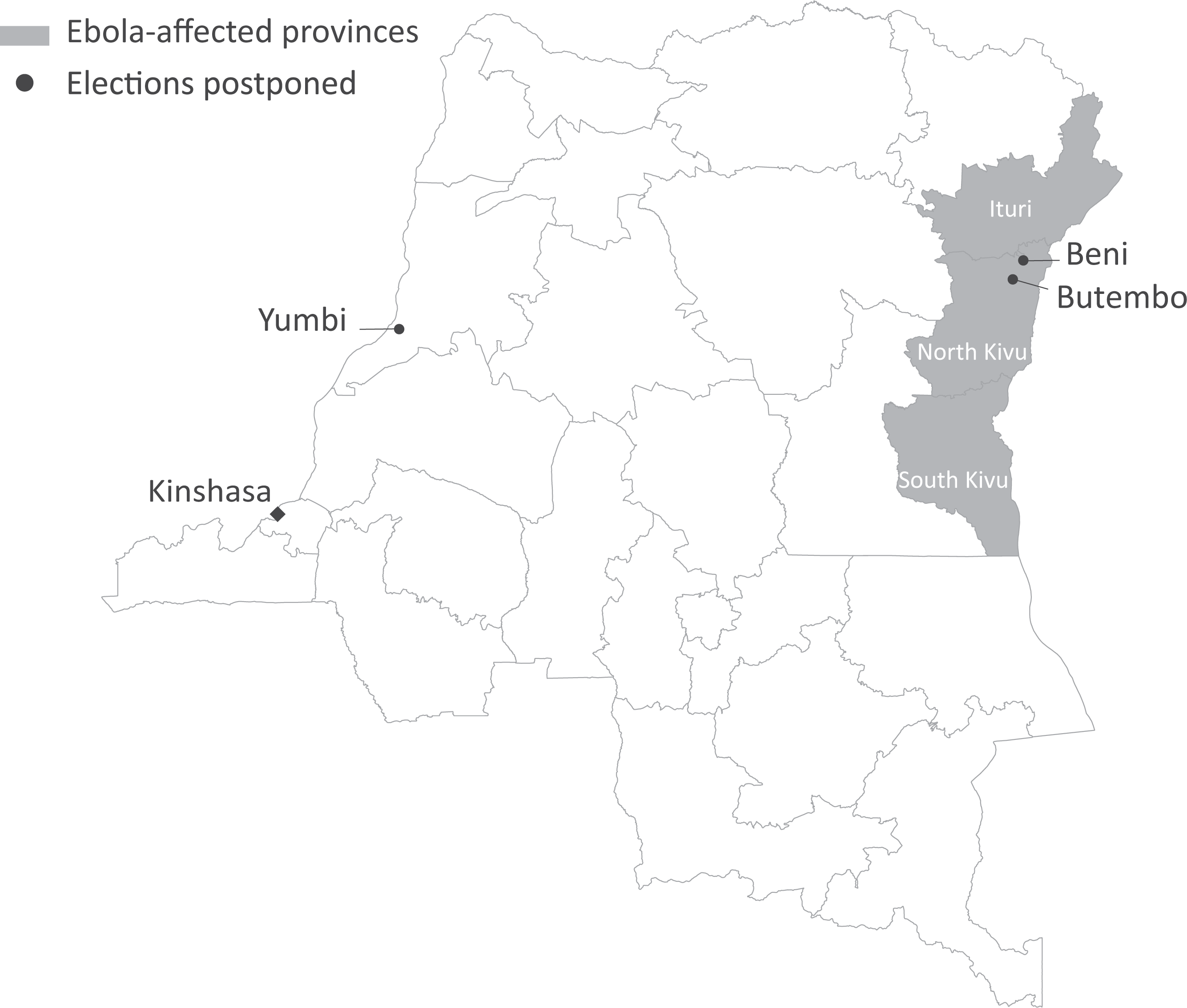
Due to the prior securitization of Ebola, the Congolese government needed little effort to securitize the 2018 outbreak. The government was therefore unrestricted in implementing emergency measures to contain the virus. The international community did not condemn the decision to exclude the three regions from voting. The rationale that this was a healthcare measure to avoid large gatherings and contain a highly infectious virus was an easy sell to election observers.
Surprisingly, the opposition candidate with the worst pre-election polls, Félix Tshisekedi, won the election. Tshisekedi was accused of having made a deal with Kabila, the former longstanding president, to win the election. The fraud could not be proven, and Tshisekedi was sworn in as president on 24 January 2019. Exclusion from voting in the elections affected the regions with little support for the central government. The candidate that came in second, Martin Fayulu, had his main support base in the Kivu regions. Some election observers testified that Fayulu should have won by a landslide. The shady deal between Kabila and Tshisekedi made the political exclusion of people in Beni and Butembo even more sour (Salihu, 2019).
The national government had little authority over the Kivus to introduce restrictive healthcare measures. Instead, international organizations tried to focus on screening, surveillance, and contact tracing. The rationale to ban only two regions from a wider area affected by Ebola raised questions. It was particularly controversial that no other restrictions were imposed on freedom of movement or on social gatherings, such as school or church visits (The Lancet, 2019). A further controversy was that large election campaign events were held in all the regions affected by Ebola until one week before the election (Ndaye, 2018). For epidemiological reasons, it made little sense to only restrict political rights on election day, and to do so in just two areas of a whole region that had been ravaged by the virus.
Politicization of Ebola
Local elites already played a critical role in disseminating misinformation and conspiracies before the election. For example, in September 2018, Crispin Mbindule Mitono, an opposition politician, claimed on local radio that a government lab had manufactured the Ebola virus ‘to exterminate the population of Beni’ (Spinney, 2019: 214). A common narrative was: ‘First the kidnappings [2010–14], then the massacres [2014–present], now Ebola’ (Sweet, 2018: 1). Only one month after the start of the outbreak, Ebola was already viewed as the latest ‘weapon of war’ used by the government against the Kivu population. In the weeks after the election, Sylvain Kanyamanda, the mayor of the city of Butembo, publicly stated that the people felt neglected by Kinshasa for a long time and were waiting to sanction power at the ballot box, but that they were stripped of this right (Ciyow, 2019). These statements show that local elites enhanced distrust of the Ebola response by framing it as yet another oppressive and violent government tool. As such, they used an injustice framing process to mobilize the population.
The election event fueled this narrative with statements directly accusing the government of excluding the regions from voting for political rather than epidemiological reasons. A regional activist group called ‘Lutte pour le changement (Lucha)’ publicly incriminated the government, claiming that their votes were not canceled because of the virus but because the region did not support the political majority (Le Point Afrique, 2018). Residents in Beni organized a fictitious vote with three ballot stations in town to demonstrate their reservations about government health measures and to prove that the ballots were safe (RTBF, 2018).
The corruption scandals were also publicly denounced. In an open letter, civil society members from Butembo accused the leader of the response, Dr Djokolo Tambwe Bathé, of being motivated by political interests in the region and of appointing political supporters to well-paid jobs during the response. They also criticized the cancellation of the elections as an inconsistent health strategy and stated that they had prepared adequate sanitary precautions for election day (Sweet, 2019: 4, 10).
After the election, opposition candidate Martin Fayulu held political rallies in several cities across the country, including Butembo, Beni, Goma, Kinshasa, and Matadi. He continued to dispute the election result and called on the population to take part in peaceful demonstrations. Public statements made by local elites incited the population against the government. Protests against the election result raged across the country for several months. As of April 2019, more than 1,000 lawsuits had been filed contesting the election results (MONUSCO, 2019).
The election confirmed many people’s fears that Ebola served political ends. Media monitoring shows that after the election, conspiracy theories stating that Ebola was being deliberately spread by the government and health workers to harm local people had grown in prominence (Bedford et al., 2019). Several perception studies based on surveys throughout the outbreak show that the regions excluded from the election had considerably higher levels of disbelief in the virus or believed that the virus served political or economic goals (SSHAP, 2019, 2020).
Ebola responders were suddenly at the center of a repressive government act and were the enforcers of a new national security agenda. Supposedly nongovernmental humanitarian organizations were perceived as being part of the government conspiracy due to the jointly coordinated response. Humanitarians working in the field named the December election a ‘definite turning point’ (Aizenman, 2019). A day after the election postponement was announced, protesters stormed an Ebola triage center in Beni and set it on fire (Freytas-Tamura, 2018). The grievances from the politically disenfranchised fueled popular mobilization and violence. It is critical to note that the election per se did not result in violence. Rather, the government used Ebola to justify the exclusion from the election. Along with other inconsistent health measures, this left an ‘observably equivalent’ impression between health policies and state repression. As a result, Ebola responders were seen as enforcers of a repressive government agenda, leading to a violent backlash against them.
Process tracing: Summary and results
The shoe-sole work of the ‘explaining-outcome’ process tracing showed that distrust can explain isolated violent incidents against Ebola responders, but it fails to account for the large-scale popular resistance. When the government excluded some regions affected by Ebola from voting, Ebola became politicized. The political exclusion was a tipping point, and local elites agitated the population by publicly framing Ebola as a political tool of the government.
While the causal mechanism could only be established based on qualitative case evidence, the link between cause and outcome can be tested in a quantitative analysis. The timing of the election exclusion in the midst of the outbreak allows the following hypothesis to be tested in an interrupted time-series (ITS) design: Interrupted time-series plot of the weekly number of attacks against healthcare responders and civilians, protest events, and Ebola cases, January 2018–March 2020
H1: After the exclusion of three regions from the presidential election, attacks against Ebola responders sharply increased.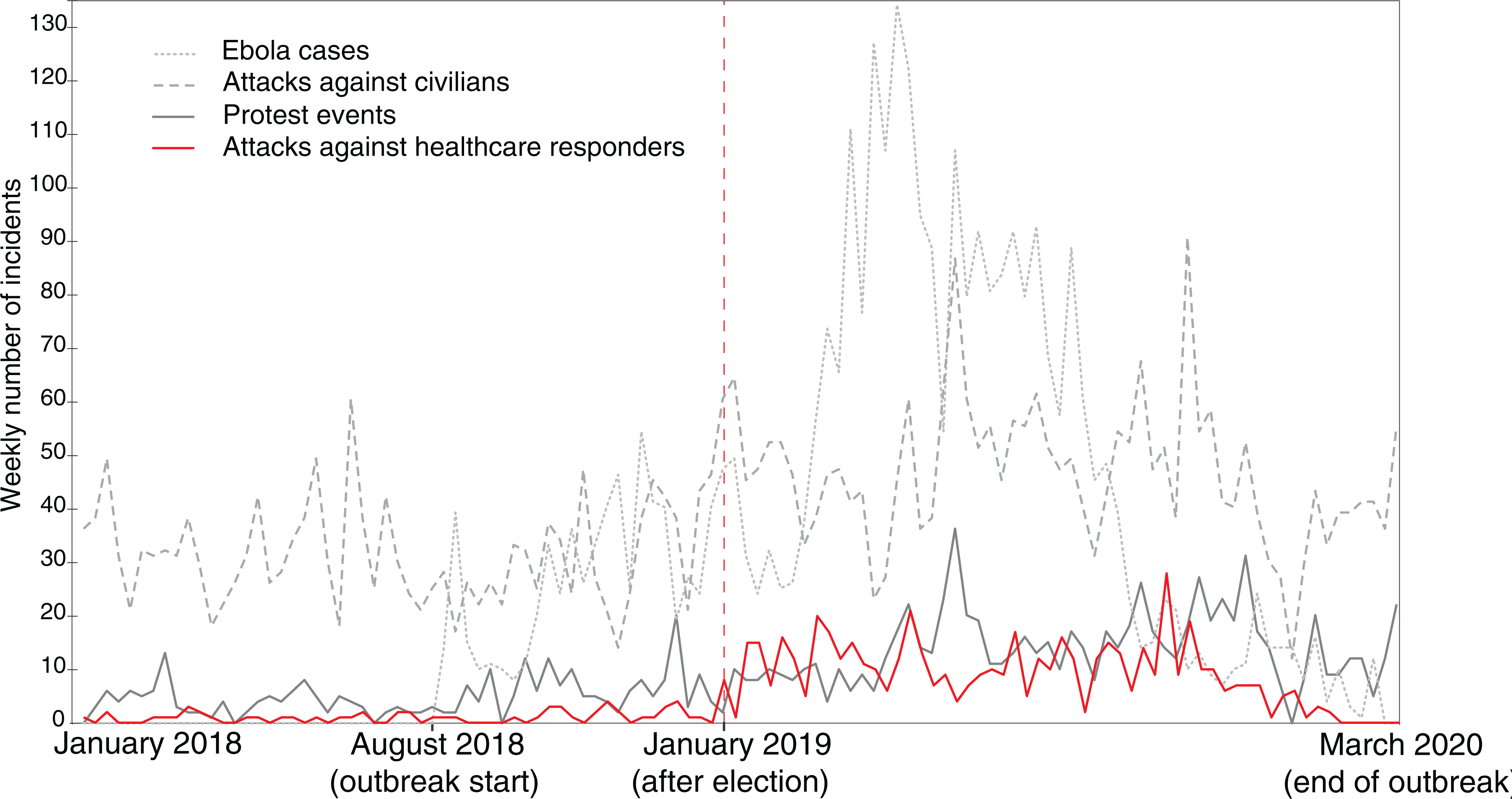
The effect of the election on violence against Ebola responders
Data and methods
This section looks at the temporal trend of the outcome – the number of violent incidents against Ebola responders – in light of a particular event of interest – the election postponement – in an ITS Model. The interruption event of an ITS Model takes place at a known point in time. The Model estimates the average treatment effect of the interruption event by comparing it with the counterfactual (the hypothetical scenario under which the interruption event had not taken place) (Bernal, Cummins & Gasparrini, 2017).
Several events related to the election took place within five weeks: the postponement of the election in three regions on 26 December 2018, the actual election in the remaining regions on 30 December 2018, the announcements of the results on 15 January 2019, and the new president taking office on 25 January 2019. It may be that these events had separate effects on how Ebola responders were perceived, but it may also be that the accumulation of events led to violent resistance. I determine the interruption event as the fifth calendar week starting on 28 January 2019. To have a meaningful time unit the data is aggregated to calendar-weeks.
The definition of Ebola responders is not clearcut. On the one hand, it must include all healthcare personnel working for government facilities, international organizations, and NGOs, as well as additional administrative personnel. On the other hand, most NGOs and international aid agencies have more than one mandate. They may be responding to the Ebola crisis but at the same time, they might be supporting food distribution or engaging in educational activities. This not only poses a definition problem for research, but also for the local population, which has a hard time knowing which individuals from the same organization work for an Ebola-related program or not. As a result of this, I combine data from attacks against healthcare and aid workers from Insecurity Insights (2020a), the aid work security database (AWSD) (Humanitarian Outcomes, 2021), and the surveillance system for attacks on healthcare from the WHO (2020). The data collection is described in further detail in the Online appendix.
Conditional means before and after the election event
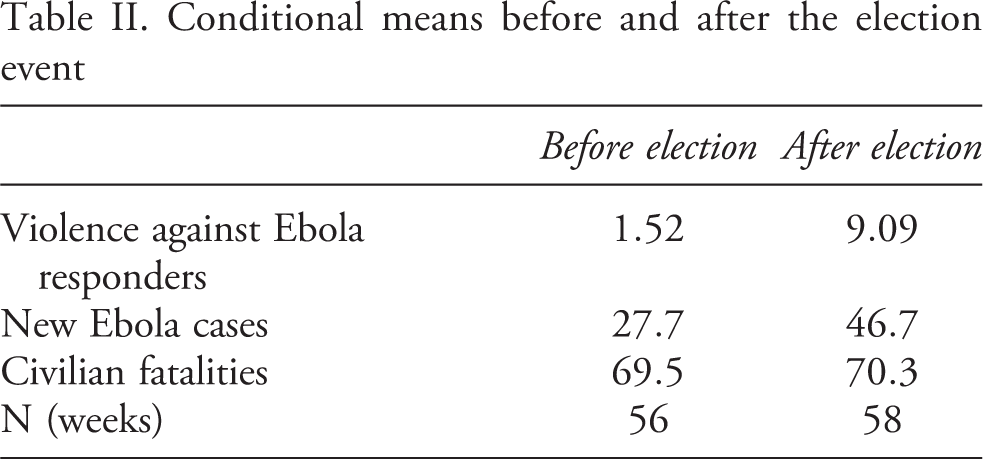
A weekly unit of analysis is unaffected by variables that can only change over the course of months, such as most socio-economic indicators (Bernal, Cummins & Gasparrini, 2017). Two time-varying confounders may impact the model, namely the number of new Ebola infections and the overall level of violence related to the conflict. Regarding the former, a sudden and stark increase in Ebola cases may heighten the distrust against the Ebola response and induce violence against Ebola responders that is unrelated to the election event. The spread of the virus also proxies for the number of Ebola responders in the field. The data from the DRC’s ministry of health is aggregated to measure the number of new Ebola infections per calendar-week. Regarding the latter, an overall outbreak in violence may explain an increasing number of attacks against Ebola responders as crossfire events. While the causal mechanism does not favor this explanation, qualitative case evidence could not rule out this explanation. To take the level of violence into account, I aggregate the number of civilians killed from the Armed Conflict Location & Event Data Project (ACLED) (Raleigh et al., 2010). I cleaned the data from all events affecting violent incidents, riots, or protests involving NGOs, Ebola responders, or healthcare workers to avoid a double count of events in my control and outcome variable.
Table II shows the means of all variables before and after the election event, as well as the number of observations. Attacks against Ebola responders before the election count 1.52 compared to 9.09 after the election. The number of new Ebola cases was clearly lower before the election with an average of 27.7 cases, and 46.7 after. The number of civilian fatalities was only slightly lower before the election event with 69.5 weekly fatalities on average compared to 70.3 after the election.
Results ITS
*p

where Y represents the count of dependent events; T the weeks elapsed since the start of the study; Xt
a dummy variable indicating the pre- or post-election period; and
Results
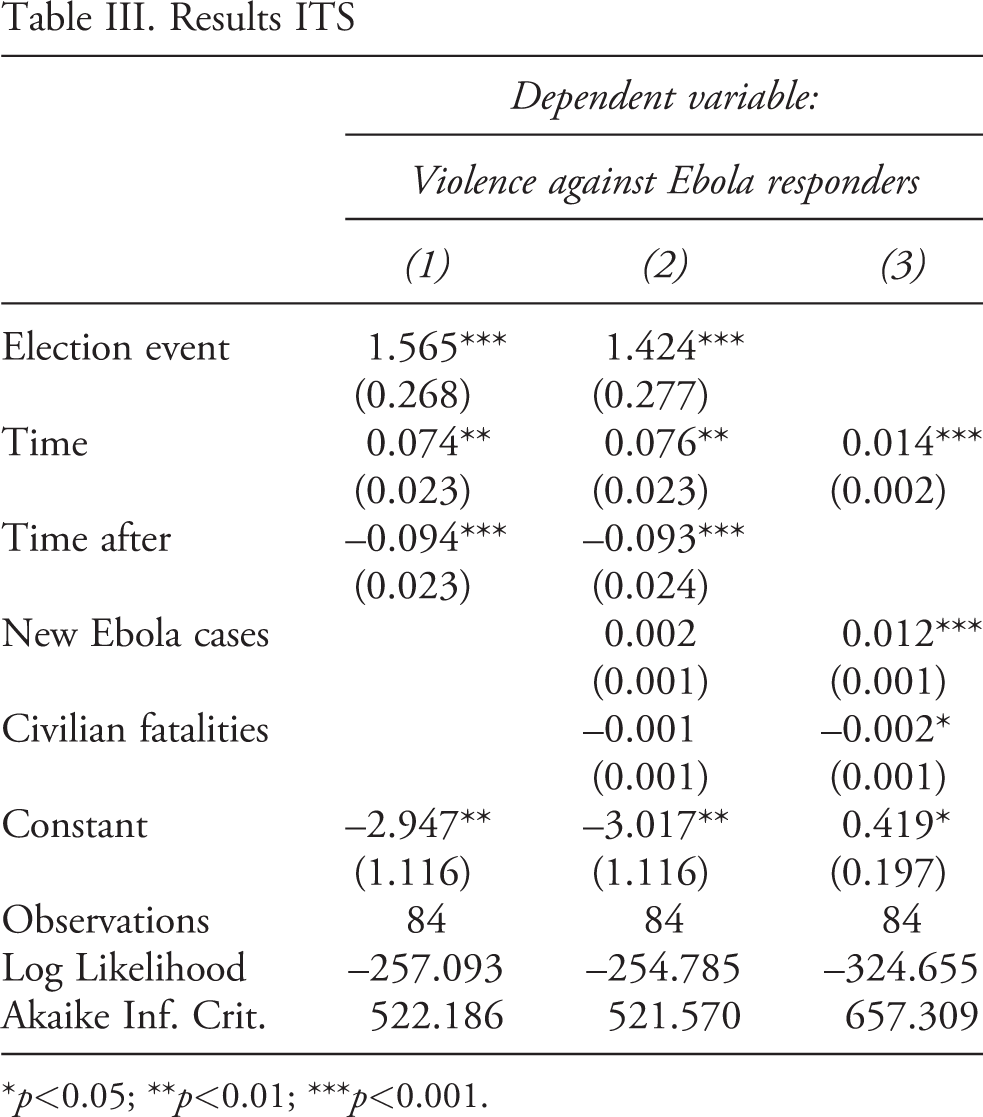
The results, shown in Table III, confirm what the causal mechanism suggests. Column 1 shows the simple model, Column 2 shows the full model, and Column 3 shows the counterfactual model.
In both Models 1 and 2, the election event has a significant positive effect on violence against Ebola responders. The time variable (number of weeks) further shows a slight but significant increase in the number of violent incidents over time. However, the time-after Predicted trend and counterfactual model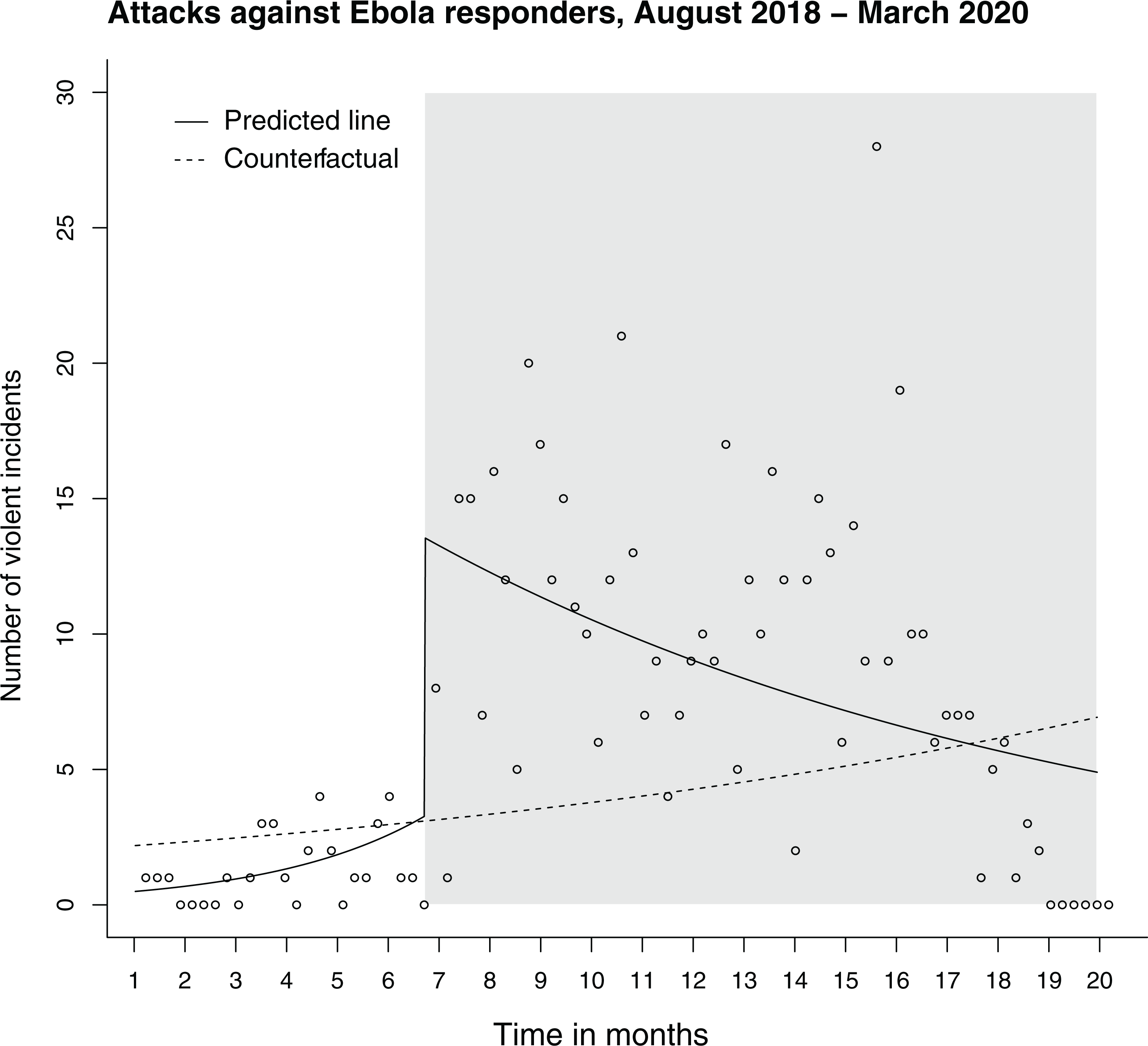
The counterfactual model in Column 3 shows what the trend looks like without the election event. In this model, new Ebola cases have a significant positive effect on violence against Ebola responders. Further, the effect of violence against civilians becomes slightly significant. The model cannot account for a slope change.
Figure 3 shows the predicted trends of the full model (solid line) and the counterfactual model (dashed line). The grey-shaded area marks the time after the election event. The counterfactual model shows that without the election event, the predicted trend is gradually increasing over time. The election model clearly shows that this is only due to a stark level change immediately after the election, and after the event the trend decreases again. However, even more than a year after the election, the predicted weekly number of incidents is still above the average from before the election. This indicates that although the trend decreases over time, the election has a long-lasting effect on violence against healthcare and aid workers.
Ebola responders were already attacked before the December election. However, the quantitative analysis shows that attacks increased in frequency after the election, indicating that popular resistance against Ebola responders increased.
In the Online appendix, several robustness checks of the main model can be found. Firstly, I test the same model with the log of total Ebola cases instead of the total number of new Ebola cases to account for the exponential growth in new cases. Moreover, different time windows for the election event are chosen. I also extend the data to start in January 2018 to include months prior to the Ebola outbreak. I further simulate a placebo test using data from January 2018, with the outbreak declaration serving as the interruption event.
Results control series
*p
Alternative explanations
Alternative explanations relate to a generally high level of violence after the election in which healthcare workers were crossfire victims.
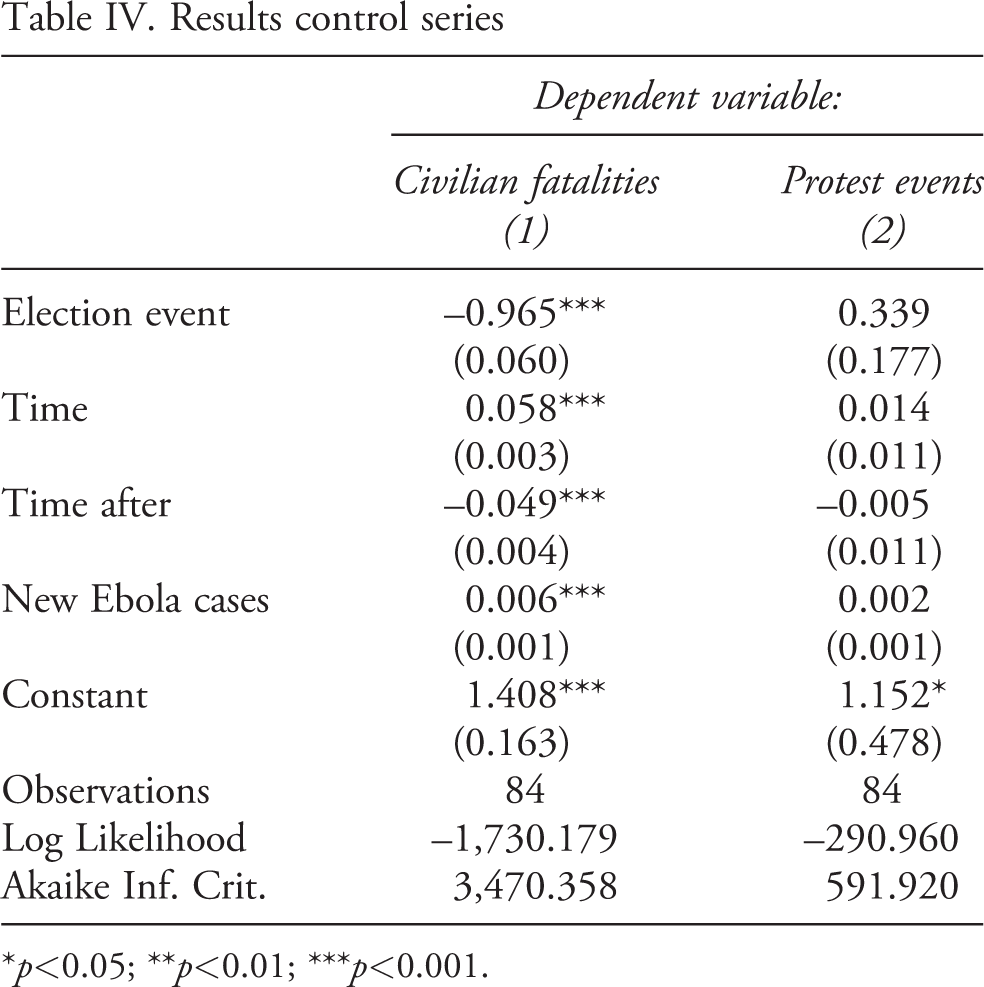
Table IV presents a control series with two different outcomes on violence against civilians and protest events. Column 1 shows that the election event has a significant negative effect on violence against civilians. This is somewhat surprising as there were several violent protests in the aftermath of the election. This strengthens the main analysis, making clear that the increase in violence against Ebola responders was not driven by a general increase in violence against civilians after the election. The second column shows that the election event has no effect on the number of protests. Hence, the sudden increase in violence against healthcare responders after the election, with an effect that lasted for more than 12 months, cannot be explained by election-related protests.
Discussion and conclusion
This article explains why healthcare respondents can become a target of violent attacks. The common narrative during the tenth Ebola outbreak in the DRC was that distrust of the centralized and international response was the primary cause. This article shows that while this served as a precondition, violence only spread after Ebola-affected areas were politically excluded. The government, in the eyes of the public, politicized the Ebola response by barring three regions from voting in the December 2018 presidential election. This explains why 2019 was not only the most violent year for healthcare workers but also why the DRC’s tenth Ebola outbreak was the most violent.
The mixed-method approach makes it possible to explain a complex phenomenon that purely quantitative or qualitative methods alone could not. The ‘explaining-outcome’ process tracing reconstructs the events and dynamics leading up to the outcome – violence against Ebola responders. An interrupted time-series model is then used to test the novel mechanism, showing that a significant increase in attacks on Ebola responders began immediately after the election exclusion. Strikingly, the peak of Ebola infections occurred in spring 2019. Figure 3 illustrates that attacks decreased over time, albeit remaining higher than before the election. How can this decreasing trend be explained if not by containment of the virus?
Firstly, on 23 May 2019, the UN appointed an Emergency Ebola Response Coordinator (United Nations, 2019). This appointment strengthened advocacy, allowing for a greater emphasis on community engagement (UNICEF, 2019b: 3). Because of this momentum, humanitarian organizations were able to gain the support of local leaders, who began publishing encouraging messages about the Ebola response (Sweet, 2019: 10).
Secondly, the new government’s consoling efforts depoliticized the response. As part of President Tshisekedi’s 100-day emergency program, around 700 political detainees, including some prominent opposition leaders, were pardoned. He also fired several corrupt ministers and bureaucrats. Tshisekedi held townhall meetings in Ebola-affected areas. The opening of the political space alleviated regional tensions (MONUSCO, 2019).
The study contributes to the literature on violence against aid workers by providing a novel theoretical framework explaining when and why not only armed groups but also civilians become perpetrators. Using a public health emergency to restrict the political rights of a section of the population can lead to conspiracy theories about the intentions behind the health measures. Thus, the argument connects to previous research on how aggrieved group identities can lead to conflict and how public framing can exacerbate tensions.
In authoritarian regimes, health emergencies open the door to opportunistic repression (Grasse et al., 2021), rendering healthcare and repression ‘observably equivalent’ (Barceló et al., 2022). This article adds to the literature on health emergencies in repressive states by demonstrating that this may result in a violent backlash against those who have to enforce the measures. The article contributes to knowledge on how governments can better manage health measures that limit individuals’ rights and freedoms.
There is a widespread belief in the aid sector that ‘all security is local’ (Cunningham, 2017: 3). Recent initiatives, such as the Grand Bargain and the Charter for Change, argue that localizing aid increases aid workers’ security (Fairbanks, 2018). The argument ignores the political context, resulting in ineffective anti-violence measures. Humanitarians may want to stay away from politics, but politics does not always stay away from them. Understanding the sources of popular discontent is necessary for defusing tensions. While it is certainly beneficial to localize aid and engage communities, it is not always the best or only way to respond to security incidents.
An Italian proverb says ‘Sparare sulla Croce Rossa’ [Shoot at the Red Cross]. The phrase refers to those who take advantage of an apparent weakness in others. It is based on the premise that unarmed health workers, clearly marked with a red cross, are easy targets. In this case, Ebola responders were undoubtedly an easier target than armed government actors.
Footnotes
Replication data
Acknowledgements
Special thanks to Jeffrey Checkel for his advice on the process tracing section and to the anonymous reviewers for their comments. I would also like to thank Lucas Schramm and Adam Kamradt-Scott for their feedback on the draft article. This article also benefited from input from participants at several conferences and workshops, including the IR Theory Working Group and Sparks Group at the EUI, the Workshop on Conflict Dynamics at Oxford University, the Empirical Peace and Conflict Research Workshop at Hertie School, and the Swiss Political Science Conference.