
Abstract
Clinical outreach is a crucial but understudied health care service delivery model. Physicians staffing rural outreach clinics must allocate a limited resource (i.e., their time) between caring for patients at their main sites and outreach locations. Using a unique 30-year data set of decisions made by cardiologists, the authors estimate a constrained utility maximization model of time allocations across home and outreach locations. The results show that travel distance, potential competition, and patient demand for cardiology services significantly influence allocation decisions. This structural model is used to simulate the impact of a predicted reduction in cardiologist supply. The expected impacts are unevenly distributed, with some rural locations experiencing large decreases in access. The authors evaluate two policies to restore rural access: targeted immigration and a subsidy program. A subsidy program with an estimated annual cost of $406,000 can restore outreach after a 10% reduction in cardiologist supply. This option should be preferred to recruiting and supporting five additional cardiologists under a targeted immigration strategy. This research demonstrates the value of marketing modeling in addressing limited access to health care services and evaluating alternative policies for maintaining access in the face of coming physician shortages.
Keywords
Cardiovascular disease is the leading cause of death in the United States (Xu et al. 2022). However, the supply of cardiologists is failing to keep up with growing demands owing to the aging of the U.S. population and the aging of the cardiology workforce (Dall et al. 2013; Fry 2022; Sauer 2020). This shortage has persisted for decades (Aneja et al. 2011) and is expected to only worsen over time.
The current shortage of cardiologists in the United States is an especially serious issue facing over 60 million rural residents who suffer from higher levels of heart disease, hypertension, and stroke (Harrington et al. 2020). Between 2010 and 2015, the death rate from coronary heart disease was significantly higher in rural areas (i.e., 118.2 per million) than in urban areas (i.e., 106.2 per million) (Singh et al. 2019). Furthermore, people living in rural areas have a 30% higher risk for stroke mortality (Howard et al. 2017). Reflecting concern over rising death rates for heart disease and stroke in rural areas, the American Heart Association (AHA) and American Stroke Association (ASA) issued a “Call to Action” to address the rising inequities in cardiovascular health of rural populations (Harrington et al. 2020). Fortunately, regular access to specialist care can have a positive effect on patient health. Indeed, rural Medicare patients with at least one specialist physician visit per year had significantly fewer preventable hospitalizations and lower mortality (Johnston, Wen, and Joynt Maddox 2019).
Since most rural communities are too small to support a full-time cardiologist, outreach clinics increase access to cardiologists for underserved rural patients (Gruca, Pyo, and Nelson 2016). Bringing cardiologists to the local community reduces the need for patients to travel inconvenient distances and can lead to more timely diagnoses and treatment, resulting in better patient outcomes. Unfortunately, how cardiologists decide where and how often to staff rural outreach clinics is little understood. For hospitals, policy makers, and insurance providers, understanding outreach decisions and how they may be impacted by the coming cardiologist shortage is a prerequisite for any plans or policies directed at ensuring equitable access to these vital health care services (Harrington et al. 2020).
Physicians offering clinical outreach in rural locations must allocate a valuable yet highly limited resource—their time—while considering various trade-offs. Cardiologists choosing outreach have multiple goals, such as expanding access to cardiology care for rural patients in their own communities and solidifying their patient referral base (Drew et al. 2006; O'Sullivan, McGrail, and Stoelwinder 2017; Tracy, Saltzman, and Wakefield 1996). Whereas rural areas are underserved by cardiologists, urban areas seem to be in a state of oversupply. In Iowa, the setting for our study, our data show that the number of cardiologists per 100,000 people is 10.6 in urban counties compared with 1.5 in rural counties and 6.5 nationwide (American Association of Medical Colleges 2019). The level of competition for patients in urban locations provides further motivation for engaging in rural outreach. Therefore, we employ the lens of an allocation problem to account for factors including patient demand, geography, and competition in our analysis.
The outreach allocation decision is complex, as it includes both whether and how often to visit a location. In particular, a cardiology group practice must weigh direct travel and opportunity costs against the immediate and future benefits associated with a given site since outreach sites differ with respect to their demand for cardiology services. In addition, practices are likely to take competitors into account when deciding where and how often to staff an outreach site that lies in proximity to more than one cardiology practice.
In this article, we use a utility model to study outreach decisions by cardiology practices as almost all specialists are part of a multiphysician organization. These decisions include the locations of rural outreach clinics and the frequencies with which cardiologists staff these sites. Specifically, outreach allocation is treated as a constrained optimization problem in which each physician group practice decides how much time to allocate to different locations, including its home location. As noted previously, the practice must consider local demand for cardiology services, travel costs, and potential competition (from other practices near outreach sites). We rely on economic models of allocation (Bhat 2005; Kim, Allenby, and Rossi 2002) to estimate the main drivers of outreach incidence (i.e., whether to staff an outreach clinic at a given location) and frequency (i.e., how often the clinic is staffed). We use a unique 30-year data set of cardiology outreach decisions across Iowa.
We identify several important drivers of outreach activity. Demand for office-based cardiology care at outreach locations is positively related to incidence and frequency of staffing outreach clinics. Proximity to other practices (potential competitors) and travel distance are negatively related to outreach being offered at a given location. Outreach is also negatively related to community median income. Although these relationships are intuitive, by placing them within a model of constrained allocation, we can assess their relative weights and interpret their significance to cardiologists making these decisions. Furthermore, unlike a reduced-form model (e.g., Nam, Gruca, and Tracy 2010), a structural model can be used to simulate counterfactual situations to evaluate the impact of coming changes that will affect rural heart patients’ access to cardiology care in their own communities.
We use the model to predict the impacts of the coming cardiologist shortage on outreach across the state. For a key counterfactual analysis, we simulate the impact of a 10% decrease in the supply of cardiologists, distributed across practices in proportion to average physician age and practice size. Because most practices are located in urban areas, having fewer cardiologists reduces the level of competition disproportionately within urban population centers. This results in cardiologists reducing their outreach activities in many rural locations. Of the rural areas expected to be hardest hit, three are located far from any potential providers. These rural locations depend on outreach from cardiologists in urban centers who will experience reduced competition at their home site as the supply of cardiologists available for outreach declines. We call this “asymmetric dependence” because the rural location depends more on the urban center than the reverse.
We simulate the effects of two mitigation strategies to restore access to local cardiology care for rural patients: targeted immigration of physicians and a subsidy program. We find that the subsidy is a cost-effective way to restore access through outreach. To replace the outreach clinic days lost due to a 10% reduction in cardiologists would require a total statewide subsidy of $406,000. This modest figure (i.e., less than the cost of a single full-time equivalent [FTE] cardiologist) would fully restore rural access to cardiology care to its current level. Targeted immigration of new physicians (using the J-1 visa waiver program) requires a median of five new cardiologists to restore outreach after a 10% overall decrease in cardiologists. We estimate that the costs of attracting and supporting five new cardiologists would be substantially higher than the amount required by direct subsidies.
The major contribution of this article is that by estimating a structural model of practices’ outreach decisions, we can perform counterfactual analysis to yield important policy insights for the health care sector. To do so, we use a model developed in marketing (Kim, Allenby, and Rossi 2002) and later refined in the transportation literature on consumer choice (Bhat 2005, 2008). Under this constrained utility maximization approach, outreach decisions result from optimizing a utility function subject to a resource constraint. The model readily incorporates “hard” economic factors (i.e., compensation, time constraints) alongside “soft” or subjective factors (i.e., mission-driven service, individual fulfillment). Using this approach, we show how key marketing decisions made by physician group practices affect patient access for an underserved population (i.e., rural patients). To motivate our modeling framework, considering the context of cardiologists choosing to pursue rural outreach is critical. Therefore, we discuss this setting in the next section.
Background and Institutional Setting
Rural areas tend to be sparsely populated and, therefore, lack the population necessary to support a specialist physician practice. Also, clinical research suggests that for many procedures, better patient outcomes are associated with hospitals having a high volume of procedures (Kastrati, Neumann, and Schömig 1998). For these reasons (among others), specialist physicians are unlikely to have their primary practice locations in rural areas (Aneja et al. 2011; Fordyce et al. 2007), requiring patients from rural areas to travel to urban areas to receive the specialized medical care they need. But many rural residents are reluctant (or unable) to travel long distances for medical and surgical care (Rodriguez 2023). As a consequence, they see specialist physicians less frequently than their urban counterparts (Chan, Hart, and Goodman 2006). This occurs despite rural residents having significantly more frequent and serious health problems than people living in cities (Harrington et al. 2020). This lack of access to specialist care is consequential: rural patients not receiving adequate specialist physician care are likely to experience preventable hospitalizations and higher mortality rates (Johnston, Wen, and Joynt Maddox 2019). Furthermore, regular access to specialist care accounts for almost 90% of the variation in preventable hospitalizations between rural and urban Medicare patients (Johnston, Wen, and Joynt Maddox 2019).
One long-standing approach to increasing access to specialist physicians in rural areas is the visiting consultant clinic (VCC) model (Drew et al. 2006; Gruen et al. 2004). A VCC is a formal arrangement between a rural hospital (or clinic) and a specialist physician, usually from a nearby urban area. This collaboration involves the specialist physician traveling to the outreach site on a regular basis to see patients in their own rural communities. Depending on the type of visiting specialist, the rural hospital provides examination rooms and other necessary support (e.g., lab testing, imaging). In the case of cardiology, VCCs are limited to office-type visits and noninvasive procedures (e.g., Holter monitors, stress tests, treadmill tests, electrocardiography, echocardiography). For more complex procedures, the rural patient is usually treated by the same physician in a larger (most often urban) hospital with the appropriate level of staffing and specialized equipment (see Tracy, Saltzman, and Wakefield 1996; Wakefield, Tracy, and Einhellig 1997).
A review of the clinical literature shows that specialist physician outreach improves access to care for rural patients, increases the quality of care in rural areas, and leads to better patient outcomes (Gruen et al. 2004). Cardiologist rural outreach is documented in studies outside the United States (e.g., O'Sullivan, Stoelwinder, and McGrail 2015) and in multiple cross-sectional U.S. state-level studies (e.g., Gruca, Pyo, and Nelson 2016; Kellerman et al. 2001). However, little is known about how cardiology practices allocate their time between their home locations and rural outreach sites. We advance knowledge through better understanding of a rural cardiology service delivery model that is effective and sustainable, a key priority identified in the AHA–ASA call to action on urban–rural disparities in cardiovascular outcomes (Harrington et al. 2020).
Cardiology VCCs are crucial as people in rural areas are more likely to have cardiovascular disease (i.e., heart disease, hypertension, and stroke) than those in urban areas, in addition to having higher levels of key risk factors such as smoking, obesity, and diabetes (see review in Harrington et al. [2020]). Because very few cardiologists practice in rural areas (Barreto et al. 2021), rural heart patients rely heavily on their rural primary care physicians for most of their medical care (Chan, Hart, and Goodman 2006). However, the clinical literature suggests that many cardiac patients markedly benefit from continued care from a cardiologist (e.g., Czarnecki et al. 2014). Thus, regular access to cardiologists should improve outcomes for rural heart patients. VCC outreach provides access to specialist care on a regular basis in the patient's local hospital or clinic, which can prevent poor outcomes for patients (Johnston, Wen, and Joynt Maddox 2019).
Generally a patient is first referred by a primary care provider (Barnett, Song, and Landon 2012) before meeting with a cardiologist (whether in a home location or an outreach clinic). The referral relationship between the primary care physician and cardiologist is crucial to the success of any cardiology practice. A cardiologist must establish and maintain working relationships with primary care physicians, a task made markedly more difficult when the primary care physician is in a rural area. An additional concern is the concentration of cardiologists in urban areas (Fordyce et al. 2007). As noted previously, there are 10.6 cardiologists per 100,000 people (2019 data) in urban areas of Iowa compared with 1.5 in rural areas (nationwide, the ratio is 6.5 per 100,000 people). Thus, competition between cardiology practices for patient referrals—including those associated with more complex procedures—adds motivation for engaging in rural outreach (Drew et al. 2006). So, to gain access to patients from rural areas, cardiologists often engage in outreach, thereby meeting with patients in their local communities (Tracy, Saltzman, and Wakefield 1996).
There can be major benefits for all parties involved in VCC outreach. First, patients are able to see their cardiologist without the concomitant travel burden (Tracy, Saltzman, and Wakefield 1996). Second, local access increases the likelihood that a patient will make and keep an appointment when compared with a referral to a more distant urban population center (see, e.g., Pierce 2007). Third, rural hospitals can supply some diagnostic services locally (e.g., lab, imaging); this retains revenue from those services in the rural community (Tracy, Saltzman, and Wakefield 1996). Fourth, for participating cardiology practices, VCCs represent opportunities to expand and maintain their referral bases in rural communities (Drew et al. 2006; O'Sullivan, McGrail, and Stoelwinder 2017). Fifth, providing regular contact with cardiologists helps primary care physicians more easily coordinate care for their patients with complex heart conditions (Wakefield, Tracy, and Einhellig 1997).
The decision to undertake rural outreach involves complex trade-offs for the cardiologist. Notionally, outreach is intended to improve the lives of rural patients. By reducing barriers to access, rural outreach can decrease delays in diagnosis and treatment, leading to better patient outcomes (e.g., SCOT-HEART Investigators 2018). Because heart disease is a chronic condition, improved coordination of ongoing care helps primary care providers better support rural heart patients. Furthermore, rural patients seeing a specialist regularly are less likely to be hospitalized (Johnston, Wen, and Joynt Maddox 2019).
Although outreach is beneficial to rural patients, participating cardiologists have to take into consideration various costs and benefits. The most obvious costs are travel costs associated with driving to the rural outreach site. During this time, the physician incurs opportunity costs owing to the inability to see patients in the office or treat them in the cardiac catheterization laboratory (“cath lab”), where more advanced diagnostic and treatment procedures are done (Loh et al. 2013). This time is essentially lost and is, in aggregate, significant. The estimated total cost of time lost from physician travel to rural outreach sites in Iowa (i.e., “windshield time”) exceeds $1.8 million annually (Gruca, Pyo, and Nelson 2016). In addition, cardiology practices incur other direct travel costs (e.g., mileage and payments to accompanying nursing staff).
A second kind of opportunity cost is a function of the outreach setting as the patient encounters are limited to office visits and certain on-site diagnostic and imaging procedures. The cardiologist’s compensation for these encounters—whether meeting with patients or interpreting test results—is low compared with the compensation for providing advanced diagnostic procedures or treatments. This limitation is keenly relevant as a substantial proportion of a cardiologist's compensation is frequently linked to productivity. Indeed, individual productivity has some role in compensation for 94% of cardiologists (MedAxiom 2020). Moreover, 46% of cardiologists report that all or almost all of their compensation is linked to individual productivity (Walter 2022). Furthermore, cardiologists achieve their performance goals with a combination of office visits, advanced diagnostics, and invasive procedures. Depending on the practice, office visits account for 44% to 60% of total activity (MedAxiom 2019).
To quantify the opportunity costs associated with outreach, we assess physician productivity with the work relative value unit (wRVU). This measure, established by Medicare, is used to account for differences in physician time and effort, clinical staff, and specialized equipment across different types of patient encounters including office visits and cath lab procedures (Wann 2014). Medicare uses wRVUs to set reimbursement rates for various treatments and procedures. In 2018, the median productivity of a full-time cardiologist was 9,642 wRVUs (MedAxiom 2019). Based on a 300-day work year, this requires an average production of 32.14 wRVU per day. Comparing wRVUs across contexts is especially revealing. For example, a 22-minute office visit with an existing patient has a value of .93 wRVU. In comparison, an angiogram—a diagnostic procedure done in a cath lab to discern how blood flows through the patient’s heart—has a value of 4.54 wRVUs or more depending on other procedures performed at the same time. Treating a blocked blood vessel in the cath lab via a coronary balloon angioplasty, moreover, has a value of 9.85 wRVUs (Blankenship et al. 2019; MedAxiom 2020).
Prior research suggests that the operating hours of an outreach clinic are between three and five hours (Tracy, Saltzman, and Wakefield 1996). Using a five-hour clinic day and assuming an average 30 minutes of total time (i.e., physician preparation and face time) per patient, a typical day in an outreach clinic will result in ten office visits with patients. Because most of these office visits are with established patients, the number of wRVUs generated will be at or near 10, well below the daily average of 32.14. In comparison, for the same day in a clinic at the urban home location, a physician could be expected to generate an additional two wRVUs of production per hour of total travel time. This shortfall in wRVU production during outreach clinic days reveals one important trade-off inherent in rural outreach.
Although procedures in the cath lab are more remunerative, they generally do not happen without accompanying initial office visits, diagnostic tests (e.g., electrocardiography, stress tests), and/or imaging (e.g., echocardiography) as well as follow-up office visits. Therefore, the compensation for the visiting cardiologist extends beyond payments for office visits at an outreach site. Patients initially seen in an outreach site often are candidates for more advanced diagnostic and treatment procedures, usually performed by the same physician. For some medical conditions, though, the visiting cardiologist may refer a rural patient to a subspecialist in the same practice. For example, a patient with an arrhythmia (i.e., an irregular heart beat) would be referred to an electrophysiologist for treatment using medicine, cardiac ablation, or other alternatives. In short, many outreach office visits are related to an upcoming procedure or a follow-up to a recent procedure.
In evaluating a rural location for an outreach clinic, a cardiologist must consider the impact of competition. Urban areas are often home to multiple competing cardiology practices, each of which is interested in expanding its referral base. In addition, cardiology practices from other urban areas may be interested in rural outreach in the “backyard” of another cardiology practice.
Also, the demand for care from specialist physicians is not completely supply driven. The mere presence of cardiologists in a rural town will not create more patients with heart disease. Therefore, cardiology practices have to balance the rewards of a given VCC relationship with the knowledge that other cardiologists can (and often do) enter relationships with the same rural hospital or clinic (Tracy, Saltzman, and Wakefield 1996). With the number of patients limited by population size of the local hospital service area, the marginal benefits decrease as the number of clinic operating days at the outreach site increases.
Taken together, patient benefits, travel and opportunity costs, and current and future reimbursements from payers affect cardiologists’ decisions to establish and staff VCC outreach sites. The key reason for explicitly modeling the VCC decisions of cardiology practices is that rural outreach in the United States is noticeably different from that in most of the rest of the world. In many other countries, health planners at the national or regional level organize and fund outreach by visiting specialists (Gruen et al. 2004). In contrast, cardiology VCCs in the United States are “market-driven,” arising due to agreements between independent entities, that is, cardiology practices and rural hospitals/clinics (Tracy, Saltzman, and Wakefield 1996). As mentioned previously, changes coming to the cardiology workforce will affect the ability of physicians to staff rural outreach clinics (Aneja et al. 2011; Dall et al. 2013; Fry 2022; Sauer 2020), so the potential impact on outreach should be assessed to preserve access for underserved rural heart patients (Harrington et al. 2020).
Data
Data Sources
As previously noted, rural outreach by cardiologists has been documented in international reviews (Gruen et al. 2004) and state-level studies in the United States (Drew et al. 2006; Kellerman et al. 2001). However, that work is cross-sectional and has usually used survey data. Our VCC data are derived from a unique 30-year longitudinal data set collected in Iowa. The Office of Statewide Clinical Education Programs (OSCEP) at the University of Iowa Carver College of Medicine continuously tracks all physicians and their work locations using multiple methods. One is a twice-yearly census of all locations that employ health professionals, including physicians. From these data, the OSCEP compiles an annual report on Iowa's visiting medical consultant activity. This report includes the locations and frequencies of all cardiology VCCs as well as the names and affiliations of the physicians involved with each outreach site. Iowa's statewide data collection on VCCs began in 1989. Several snapshots of typical VCC activity statewide are shown in Figure 1. Presented are the VCC relationships in Iowa documented by the OSCEP in 1989, 1996, 2004, 2012, and 2019. As is evident from the maps, a large number of rural outreach locations are staffed from a small number of larger cities, most of which are in Iowa.

Rural Outreach Clinic Maps.
In addition, the OSCEP provided the locations of all cardiologists and cardiology practices in Iowa for 1990–2019. Combining the data on the number of cardiologists in each practice location with the VCC activity associated with each practice, we could determine the allocation of practice days between the primary practice location and rural outreach sites. We also know the age, gender, and specialty of each cardiologist at each practice. Data at this level of detail, including all outreach activity, are only available for cardiologists in Iowa. Therefore, we limit our modeling of allocation decisions to Iowa-based cardiology practices that had staffed an outreach site at some point during the last 30 years. This comprised approximately one-half of cardiology practices in the statewide database of all cardiologists.
We measured distance in minutes of travel time. In our model, time is the constrained variable (as opposed to, say, miles). To estimate driving times, we used the urban city centroids for practices conducting outreach and the rural community centroids for VCC clinic locations. Driving distances from primary practice locations to VCC locations were estimated using the Google Distance Matrix API. Although some approximation error resulted from using the city centroids as opposed to exact locations, the error for population centroids is lower than for other nonexact approximations (Berke and Shi 2009).
We used the Area Health Resource Files (AHRF) for county-level data on population, age distribution, and median income. The AHRF data contain the number of people in each age group, which can be used to compute demand for office visits. The National Ambulatory Medical Care Survey reports the number of cardiology office visits per 100 people for each age group (Centers for Disease Control and Prevention 2010). Combining these data, we computed the demand for cardiology office visits for every rural county for each year. For example, consider a hypothetical location with 1,000 people between ages 65 and 74 and 1,000 people over age 75. The number of visits per 100 people 65–74 years of age is 37. The number of visits per 100 people over age 75 is 54. This hypothetical population of 2,000 people would be expected to need 37 × 10 + 54 × 10 = 910 total office visits. These figures provide our measure of patient demand for cardiology services in rural counties.
Our sample covered the entire state of Iowa. The variables differed in level of aggregation. Our dependent variable—time spent—is defined at the community level, where the community was the home location of the cardiology practice or a small to medium-sized rural town. AHRF data were reported at the county level. We aggregated data on individual cardiologists to the practice level.
Our unit of analysis for the decisions on staffing and frequency of outreach clinics was the cardiology practice. Some cardiology practices also employ subspecialists, including heart surgeons (who perform such procedures as open heart surgery and transplants) and electrophysiologists (who specialize in heart rhythm problems). Heart surgeons do not engage in outreach, and electrophysiologists rarely staff an outreach clinic. However, their colleagues who do so can generate referrals that benefit the practice as a whole. In addition, when a cardiologist is staffing an outreach clinic, the other doctors in the practice are usually responsible for being “on call” for problems arising with patients at the home location. 1 Call coverage is a major point of stress for many physicians (Mitchell 2018). Therefore, the decision to undertake rural outreach impacts more than the participating cardiologist.
Our final data set consisted of 30 years of allocation decisions made by cardiology practices. We summarize some key statistics in Table 1. On average, there were 84 unique VCC relationships between Iowa cardiologists and rural hospitals/clinics per year. The number of rural communities hosting a cardiology VCC averaged 67, which means there were two or more competing VCCs in a substantial number of rural locations every year (these are indicated by the numbers in parentheses in Figure 1). Most clinics (64%) were offered one or two days a month. The average driving time for cardiologists staffing these clinics was 60.6 minutes, but more than 40% of the one-way trips were more than 60 minutes.
Data Overview.

On average, 18.5 Iowa-based cardiology practices staffed an average of 4.6 different outreach clinics per month. The practice sizes ranged from 1 to 44 physicians. The average cardiology practice had 41 alternative rural outreach locations within a 130-minute (one-way) drive time. Cardiologists in practices that staff outreach clinics tended to be male and Doctor of Medicine (MD) degree holders. The average physician age in these practices was 49 years. In the next section, we discuss the time allocation data.
Description of Time Allocation Data
Our dependent variable was the number of days per month allocated by each practice to each location (both home and outreach) in a given year. Each year, all practices decided where and how often to staff outreach clinics. While clinic days occurred monthly, the agreements with the hosting rural location were made annually and fixed the schedule for the year. Therefore, the decision time frame was consistent with our annual data.
The distribution of allocations was extremely skewed, to the degree that a histogram of the values was uninformative without a transformation. Of the 23,901 values in the data set, 20,798 (87%) were zero. This is due to the fact that each cardiology practice had many alternative outreach locations (hospitals and clinics) within a 130-minute driving time 2 (i.e., 41 on average). Figure 2, Panel A, shows the natural log of the 13% (N = 3,103) of allocations having positive values. As revealed in Figure 2, Panel A, a modeling challenge became evident. The distribution for home locations differed distinctly from that for outreach, but the two were interdependent. Furthermore, they were range bound as well as sum constrained and thus could not be treated separately (Bultez and Naert 1975). Instead, we construct a single, unified model that can reproduce the characteristics of both distributions. If we were to model our VCC data as a simple binary outcome—rather than an allocation problem with continuous variables—we would have to omit critical features of the data. Another benefit of continuous data was that the variation in time spent at rural outreach locations enabled identification of some of the key model parameters, such as the coefficients on patient demand and travel time.

Time Allocation Distributions.
In the Web Appendix, we present a case study of market share dynamics near Johnson County, where the only academic medical center in Iowa is located. The key takeaway from this case study is that allocations tend to vary every year, and that rural hospitals/clinics do switch between different outreach providers. This variation is beneficial for more precisely estimating model parameters.
Presented in Figure 2, Panel B, is how practices typically allocated time between home and outreach locations. For most practices in most years, 60% or more of the time was spent at the home location. The mean share is 90%. The distributions look similar when split at the median practice size of five cardiologists. With a few exceptions, large and small practices seem to allocate time similarly between home and outreach locations.
As noted previously, the cardiology practices ranged in size from 1 to 44 physicians, with a median of 5. The size of each practice formed the basis for the time constraints. We assumed that each cardiologist worked 25 days per month. The practice decided how to allocate the days of each cardiologist from the total time “budget”: the practice size multiplied by 25.
Figure 3 gives key context for our focal counterfactual analyses. After increasing from 1990 to 2000, the total number of days of outreach per year in rural communities has stayed relatively constant. The number of days demanded in rural counties, 3 in contrast, continues to increase throughout. This reflects the current shortage of cardiology care in rural areas.

Actual Versus Demanded Days of Outreach.
Figure 4 shows the basic associations for nonzero rural outreach allocations of physician days over years (N = 2,532). Outreach activity at a location was positively related to patient demand in that rural county (see, e.g., Centers for Disease Control and Prevention 2010). The allocation of days was negatively related to travel time to the rural site. Other relationships were ambiguous. Consequently, a formal model would help reveal the impact of these and other driving factors.

Outreach Drivers.
Model and Variables
As described previously, the decision to staff an outreach location is complex. Multiple goals are in play with every choice of location and number of days per month committed to patients in that community, whether at the home location or at a rural hospital or clinic. Improving care for patients and developing a medical practice are but two of many considerations. There are trade-offs between the needs of rural patients lacking access to cardiology care in their own communities and the reality that needed specialized facilities and personnel are limited to a cardiologist's home location. Moreover, traveling to outreach locations incurs opportunity costs and yet provides the basis of referrals for more complex treatments in the future.
When evaluating potential rural outreach locations, the practice can readily discern its distance from its home location as well as locations of other cardiology practices. This is an important factor if the other cardiologists are contemplating their own outreach options or may have already established a regular schedule of outreach clinic days. Furthermore, demand for cardiology office visits tends to be driven by the number of residents over age 65. Also, less financially well-off patients in rural areas could have increased difficulty traveling to nearby urban areas due to the lack of affordable transportation options (Syed, Gerber, and Sharp 2013). These aforementioned observable factors influence the benefits and costs—both current and future—of allocating days to a given rural outreach location.
The presence of such varying and potentially conflicting considerations means that a day of rural outreach represents the distillation of many factors, some observable and some hidden. For this reason, we characterized the objective function governing outreach decisions as a utility function. Specifically, we assumed that cardiology practices maximize utility subject to a time constraint as there are only so many days and too many demands.
Utility Function and Constraint
Each cardiology practice
4
maximizes utility by choosing where and how often doctors visit each location (including the home location). The core logic of a practice's decision to staff a rural outreach clinic is embedded in the utility function. Practices decide once a year on an allocation that holds for the next 12 months. Practices are indexed by m = 1, …, M; locations, by l = 1, …, L; and years, by t = 1, …, T. The decision variable is the number of clinic days to allocate to location l in year t by practice m, denoted by amlt. Note that since the decision applies for each month of the year, the annual and monthly allocations always differ by exactly a factor of 12. We employ a family of translated utility functions introduced in Kim, Allenby, and Rossi (2002) to represent the utility for practice m at location l in year t:
The preference parameter (ψmlt) reflects the attractiveness of each location for a given practice. Because preferences vary across locations and times, we introduce six covariates (Xmlt), which influence ψmlt. The covariates capture both supply-side factors such as inertia, travel time, and competition and demand-side factors such as patient population and income level. We also include the year in case of a time trend. We also add an error term (
Variable Definitions.
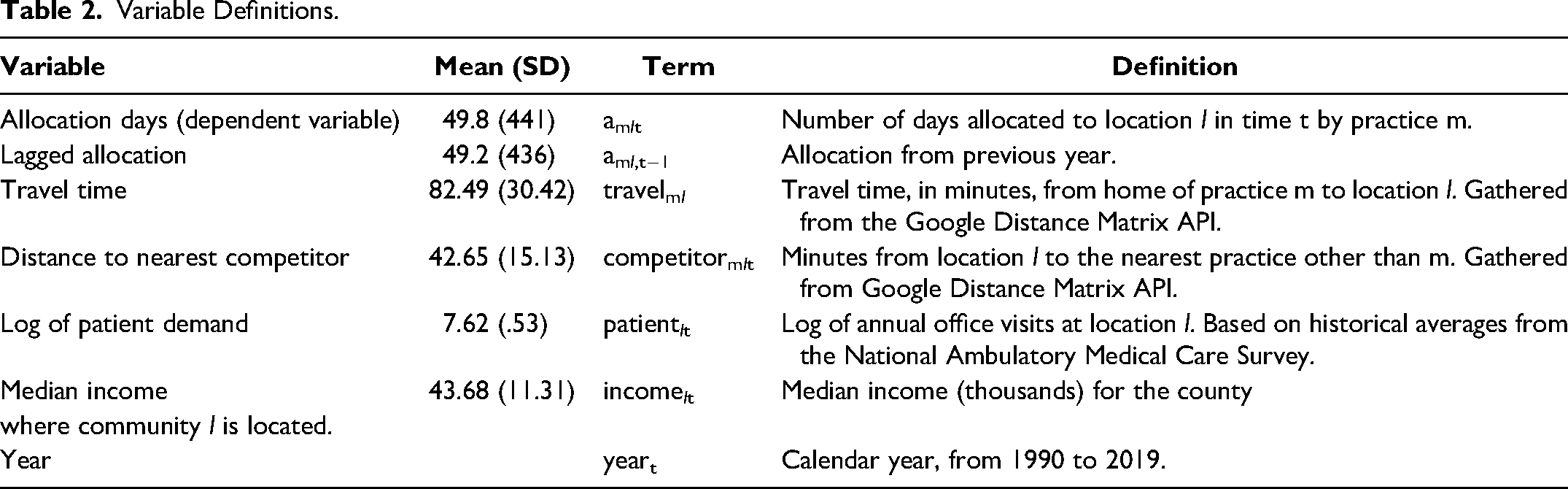
The diminishing returns parameter (γ l ) controls the rate at which utility falls as more days of physician time are allocated to a location. 6 Constrained within the range of 0 to 1, γ l influences the concavity of the utility function. Concavity implies that the incremental gain in utility diminishes as the days allocated to the location increases. A smaller value of γ l indicates a stronger tendency toward diminishing returns, leading to lower allocations. Conversely, a large value of γ l implies a slower decrease in marginal utility, leading to a higher allocation of clinic days. If diminishing returns are not supported by the data, the diminishing returns parameter will approach 1, and utility becomes approximately linear in allocation (constant returns). Note that diminishing returns apply over repeated visits to the same location over the year. For the visiting physician, outreach has multiple benefits including providing timely patient care in rural towns and providing referrals for more complex procedures in their home locations. However, due to the low population density of rural areas, there is a limit on the demand for cardiology office care at any one location. Rural hospitals and clinics draw from the local population of patients needing specialized cardiology care. As the number of outreach clinic days staffed at any one location increases beyond a certain point, the marginal benefit to the visiting cardiologist eventually decreases.
The translation parameter (τ l ) either causes indifference curves associated with the utility function to cross the axes if τ l = 1, which allows for corner solutions, or enforces an interior solution if τ l = 0. We set it to 0 for the home location based on the observed fact that every practice always allocated more than zero days to its home location. It is set to 1 for away locations, accommodating both zeros and positive allocation days.
We anticipate significant differences in both the baseline preference (β0l) and the degree of diminishing returns (γ l ) between home and away locations. This is because practices offer comprehensive services, such as procedural care, at their home location, whereas clinic days at outreach locations are exclusively dedicated to office visits. Theoretically, it might be possible to allow for these parameters to be location-specific if we had a substantial historical record of allocation decisions among a small set of locations. However, our data are limited to relatively short time series for each practice (median of 8.5 years) while the number of outreach locations considered is large (median of 45 locations). Therefore, we simplify our model by differentiating these parameters just between home versus away locations (i.e., for the home location, denoted by h: β0l = β0h, γ l = γh; for away locations, denoted by a: β0l = β0a, γ l = γa).
We assume that practice m optimizes the allocation of its finite resource (namely, physician time) to achieve maximum overall utility. The objective of the practice is to maximize
Given the characteristics of practices and locations, and conditional on the known values of the error terms (
Without loss of generality, suppose the first K locations are allocated positive time, and the rest are not visited. Then the model likelihood for an observed optimal allocation 
Practices might place different weights in evaluating the utility of their allocation decisions. To incorporate practice heterogeneity, we allow for the baseline preference and diminishing returns parameters, which determine the shape of utility function, to be practice-specific. We use a random-effects specification for the practice-level parameters as follows:
Note that θm does not include the baseline parameter for the home location (β0h). Because one of the baseline parameters is required to be fixed for model identification, we fix the baseline for the home location to be zero (i.e., β0h = 0). In addition, to ensure the diminishing returns parameters fall between 0 and 1, we reparameterize γh as
Estimation Results
Given the hierarchical structure, we estimated the model using Bayesian Markov chain Monte Carlo methods with proper but relatively diffuse priors (details in the Web Appendix). We ran the chain for 500,000 iterations, with the first 100,000 draws discarded as burn-in. We thinned the chain by retaining every tenth iteration, thus leaving 40,000 draws to summarize the posterior distribution.
Model Fit
To show that the model recovers the moments of the data, we compare the empirical cumulative distribution function (ECDF) from realizations of the model against the ECDF of the observed data. Using the simulation procedure in the Web Appendix, we produce predicted allocations (
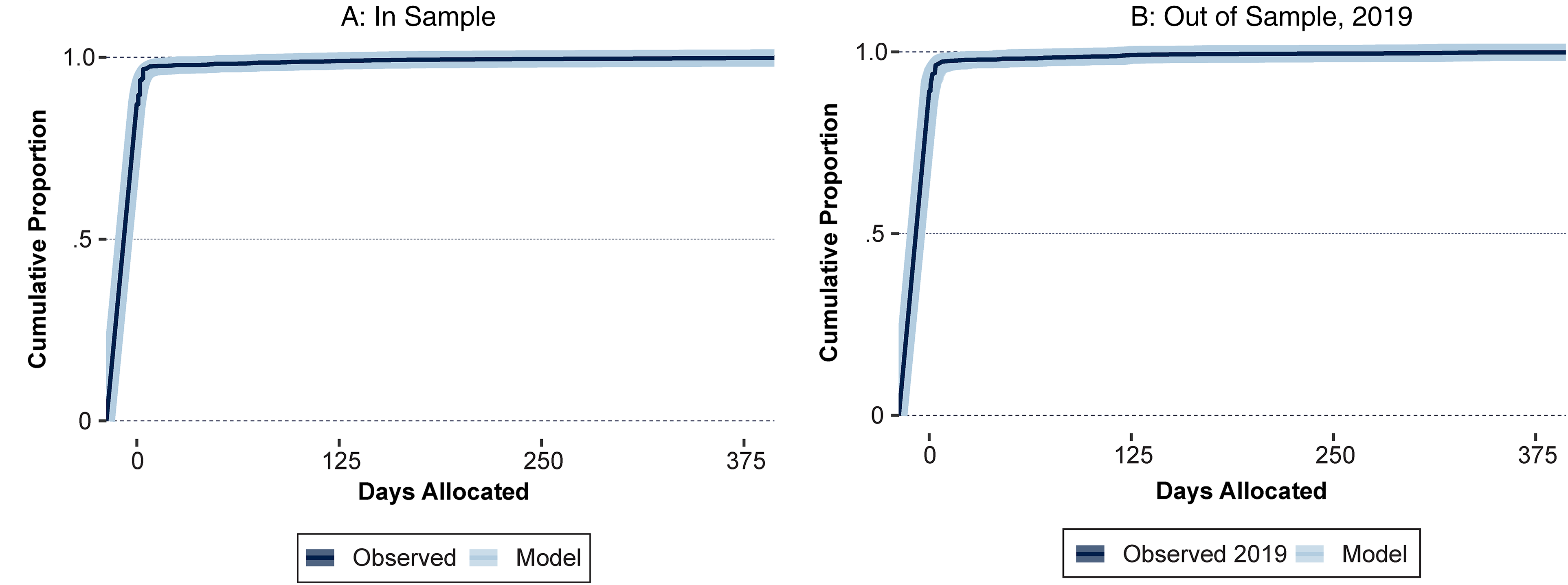
Structural Model Fits the Data Distribution.
In addition, Table 3 compares specific moments between the data in sample and with 2019 as a holdout. The model recovers the first four statistical moments well, along with the incidence of zeros and the mean and standard deviation when excluding zeros.
Structural Model Captures Data Moments.

Parameter Estimates
Table 4 presents the estimation results of our model. For each of the heterogeneous parameters in Equation 5, we report the posterior mean and standard deviation for the average of practice-level parameters. We summarize the posterior distributions of the homogeneous parameters shown in Equation 2 using means and standard derivations. We first discuss the homogeneous parameters, which reflect the effects of covariates. Then we delve into the implications of the heterogeneous parameters that characterize the utility structure of each practice.
Parameter Estimates.

95% credible interval excludes 0.
Notes: N = 23,901. Log marginal density = −2,929.
The baseline preference parameter cannot be directly compared between the home and away locations because their translation parameters are set differently (i.e., τh = 0, τa = 1). Therefore, we measure the baseline marginal utility by computing the increase in utility resulting from the first clinic day allocation, while holding all covariates at zero (i.e.,
Figure 6 illustrates the differences in the baseline marginal utility between home and away locations. First, Panel A shows the baseline marginal utility of away locations compared with that of the home location. The baseline marginal utility of away locations is significantly lower (paired t-test: t = 19.71, p-value < .001), indicating the increased benefits of working at the home location. These benefits include the availability of specialized staff, equipment, and facilities necessary for providing procedural care. Panel B compares the rate of diminishing marginal return between home and away locations (i.e., γh vs. γa). The diminishing marginal returns parameter is significantly smaller in away locations (paired t-test: t = 7.64, p-value < .001), implying a faster decrease in marginal utility. It reveals that practices experience diminishing marginal returns with respect to time allocation at the home location, which prompts them to consider staffing outreach clinics. However, most practices face more pronounced diminishing returns at away locations due to small patient populations. Consequently, practices allocate a majority of their time to the home location, where the baseline marginal utility is high but diminishes slowly. As the incremental gain from the home location becomes smaller, practices extend their reach to rural locations with low baseline but quickly diminishing marginal utility, by providing a small number of clinic days at multiple locations.

Home Versus Away Utility Parameters Across Practices.
The effects of covariates on outreach allocations are also found in Table 4. The positive coefficient on lagged allocation suggests the presence of inertia, possibly due to switching costs associated with forming or dissolving VCC relationships with a rural hospital (Tracy, Saltzman, and Wakefield 1996). As anticipated, the negative coefficient on travel time reflects the presence of opportunity costs. Additionally, the positive coefficient on distance to the nearest competitor, measured in minutes like the travel time variable, suggests a negative impact of potential competition on the allocation of outreach clinic days in certain rural areas. Specifically, outreach activities are more likely to be allocated to rural locations that are farther away from competitors, indicating that these locations are considered more attractive for outreach efforts. This competition variable also applies to home locations, as practices that do not have other practices in the same city are likely to spend more time at home (rather than away at outreach locations) due to the absence of local competition.
Location-specific characteristics also play a significant role in outreach decisions. As anticipated, the coefficient on the log of patient demand is positive, indicating that practices tend to offer more outreach clinic days to rural areas with higher demand for cardiology services. Interestingly, the negative coefficient on income suggests that practices prioritize lower-income counties. It is possible that lower incomes represent a barrier in terms of transportation costs, leading practices to focus on areas with lower income levels for their outreach efforts. The coefficient on year is not significant, suggesting there is no clear time trend in the pattern of allocations.
Practice Heterogeneity
As noted previously, previous research has suggested four possible sources of heterogeneity in outreach decisions: physician age, physician degree, physician gender, and practice size. The hierarchical Bayes framework enables us to understand how the variations in practice-level parameters (i.e.,
Practice Heterogeneity Estimates.

Notes: N = 50. Only significant results reported (95% credible interval excludes 0). Full results are available in the Web Appendix.
Practices with a higher average age have sharper diminishing returns on time allocated to the home location. This may be due to older cardiologists cutting back on call coverage and reducing the amount of procedural care they provide (Fry 2022). For larger practices, the value of additional time at the home location is lower than for smaller practices. A smaller practice may more easily balance the conflicting demands of office visits, call coverage, and procedural care. In contrast, there may not be sufficient local demand for procedural care for all of the physicians in a large practice, hence the need for rural outreach. However, the utility of any single outreach location is lower for the larger practice. Thus, making up the shortfall for the entire practice is likely to involve multiple outreach sites. Finally, the marginal utility of time allocated to outreach sites is lower for practices with a larger proportion of female physicians. This reflects the observed tendency for lower participation in rural outreach by female physicians (O'Sullivan, Stoelwinder, and McGrail 2015).
Impact of the Coming Shortage of Cardiologists
A structural model has the ability to simulate counterfactual scenarios of importance to rural patients, cardiology practices, and policy makers. Of particular interest in this study is the impact of a potential decrease in the availability of cardiologists to participate in rural outreach activity. The aging of the U.S. population is greatly increasing the demand for care from the current cardiology workforce. Moreover, the aging of the cardiology workforce and limits on the number of cardiology fellows being trained suggests there will be a reduction in the number of cardiologists in the near future. A study by MedAxiom (a consulting company associated with the American College of Cardiology) examined the impact of the aging of the cardiology workforce (Sauer 2020). Due to retirements and lower productivity among physicians older than age 60, the workforce loses the equivalent of 2,000 FTE cardiologists each year. Due to past restrictions on the numbers of cardiology residents and fellows, fewer than 1,500 new cardiologists enter the workforce each year. This results in a net loss of more than 500 FTE cardiologists per year. This reduction comes on top of a growing need for cardiology care due to an aging population. As these changes shape the cardiology workforce (and physician workloads), the attendant effects on patient care will be consequential, especially for rural patients. Therefore, ascertaining which locations might face significantly decreased access to local care provided by visiting cardiologists is of paramount concern. To gain insight into this potential future scenario, we used the posterior distribution of the model to simulate the impact of a counterfactual scenario in which the population of cardiologists in Iowa is reduced by 10%.
We focused on 2019, the final year in the data sample for the counterfactual analysis, as it represented the most current conditions in our data. First, we simulated from the fitted model, without changing the original data set. The result is a set of fitted allocations (
We used 375 draws from the posterior to simulate 375 outcomes under the counterfactual scenario, and computed the impact as the difference between model predictions under observed data and counterfactual data. The units of this difference were days per year, so −20 meant that a county received 20 fewer clinic days a year under the counterfactual scenario compared with the original data. Results are shown in Figure 7. The home locations are labeled. The counties most affected by a reduction in cardiologist supply were Johnson, Linn, Black Hawk, and Story (indicated by darker colors). Unlabeled locations are outreach counties, with darker shades indicating a larger decrease in days allocated under the counterfactual situation relative to the current conditions. Of special note is that, as competition decreased in Johnson, Linn, and Black Hawk counties, practices allocated more time to their home locations and, consequently, less to outreach locations. This was especially true of the rural counties that border Linn and Johnson counties.

Impact of 10% Reduction in Cardiologists on Days Allocated.
Shown in Table 6 are the predicted number of days per year of outreach under the counterfactual analysis for these communities. Under the 10% reduction in cardiologists, several rural locations were likely to lose most or all of their cardiology outreach care. For five of these rural locations, there was virtually no probability of receiving any outreach. For an additional two locations, the median outcome was near zero, and for most there was a 95% posterior probability of receiving less than one day a month. This low level of VCC frequency was rarely observed in our data (6 out of 2,839 observations or .2%). In fact, the trend for rural outreach in other medical specialties (e.g., medical oncologists) has been moving toward staffing fewer locations but visiting more often (Gruca, Inwoo, and Tracy 2014). If this trend generalizes to cardiology, rural patients in these communities are likely to face decreased local access to cardiologists.
Communities with Less Than One Day of Outreach Care per Month.

Notes: The counties in this table are each allocated less than one day per month, total, under 50% or more of the counterfactual simulations.
Shown in Figure 8 is a map of Iowa counties predicted to have less than one outreach day per month based on our model. Eleven of the 17 counties directly border a county with a practicing cardiologist. Four of the remaining six are in the middle-south of the state. The region in which each of these locations falls is relatively more accessible to practices in the center of the state, especially in Polk County, and has a large number of less populous locations. In the event of a decrease in the number of cardiologists, some locations were less attractive because of a combination of declining competition, short travel distances for patients, and low patient demand. Fayette County is in a similar situation, as it is dependent on outreach from urban counties that have many alternative rural locations to choose from.

Counties of Communities with Predicted Allocations of ≤1 Day Per Month.
As noted previously, the reduction in outreach supply creates “asymmetric dependence.” This phenomenon describes the vulnerable locations that depend on physicians from urban centers to provide outreach more than those physicians depend on these vulnerable locations for additional revenue. The important distinction between the most vulnerable three locations (in Clarke, Lucas, and Fayette counties) and the rest is the lack of substitute providers for these rural locations, paired with abundant outreach location options for the visiting physicians.
Mitigation Strategies
Using the model, we evaluated different strategies to mitigate the negative impact of a 10% reduction in the supply of cardiologists. We consider two approaches: subsidies and targeted physician immigration. These policy options have precedents in the Australian health care system, which also faces a limited physician workforce in rural areas of the country (O'Sullivan, McGrail, and Stoelwinder 2016; O'Sullivan et al. 2019).
The first strategy is a direct subsidy paid to a physician for participating in rural outreach. About 20% of all specialist physicians participate in rural outreach in Australia (O'Sullivan, Joyce, and McGrail 2014). However, only a small percentage (i.e., 16%) visited more remote locations. (In comparison, 45% of Iowa's cardiologists regularly participated in rural outreach in 2014; see Gruca, Pyo, and Nelson [2016].)
A national program of subsidies—the Australian government’s Rural Health Outreach Fund (RHOF)—was established in 2000 to motivate specialist physicians to engage in rural outreach (O'Sullivan, McGrail, and Stoelwinder 2016). The purpose of this system is to ensure regular access to specialists for patients living in outer regions and remote towns. A survey of outreach physicians in 2014 found that nearly half of all participating physicians received some sort of subsidy. The subsidy split between the RHOF and other sources was 40%:60%. We focused on the type of subsidy offered by the RHOF as this program centers on national priority areas of concern, including chronic diseases such as cardiovascular disease. The RHOF subsidy is based on cost of travel including loss of income from being away from one's home practice.
The second strategy is targeted immigration, whereby qualified cardiologists are offered positions in rural areas. In its call to action to remedy inequities in heart health outcomes for rural residents, the AHA mentions using targeted immigration to increase the availability of cardiologists in rural areas (Harrington et al. 2020). Health planners in Australia have used targeted immigration to meet the needs of rural patients for access to specialist physicians (O'Sullivan et al. 2019).
In Australia, rural areas often rely on overseas-trained doctors (O'Sullivan et al. 2019). A recent study examined the relationship between the location of training and the practice location for medical specialists. Overseas-trained doctors beginning their careers in Australia after 2000 were almost twice as likely to practice in a large regional area (<50,000 people) or in a small regional/remote area than in an urban area (O'Sullivan et al. 2019). However, the number of specialist physicians per capita practicing in nonurban locations remains roughly one-half to one-fifth of the number in urban areas.
The path for an international medical graduate (IMG)—someone who attended a medical school outside the United States—to practice cardiology in the United States is markedly different from that in Australia. In Australia, some physicians who have completed residency can become licensed without additional training. In the United States, though, regardless of prior training and experience, IMGs are required to complete the full residency and fellowship training to qualify to hold a license and become board certified (Zoghbi et al. 2004).
Despite these hurdles, approximately one-quarter of U.S. physicians were trained in a non-U.S. medical school (Ranasinghe 2015). The comparable figures for cardiology are even higher, with 31% of cardiologists having graduated from a non-U.S. medical school. Recent research on cardiology residency programs found that nearly 40% of adult cardiology trainees fall into the IMG category (Shahid et al. 2021). Nearly two-thirds of all IMGs entering practice after completing a residency are not subject to immigration restrictions as they are U.S. citizens, permanent residents, or refugees with permanent status (Zoghbi et al. 2004).
Employment options for the other one-third of IMGs depend on their visa status. For example, an IMG cardiologist holding an H-1 visa can use an offer for employment to apply for permanent residence. In contrast, those holding a J-1 visa are usually required to return to their country of origin for two years after completing training in the United States (Zoghbi et al. 2004). Under the J-1 exchange visitor visa program, this requirement is waived if the physician serves for three years in a rural or underserved urban area (Maree and FitzGerald 2009). The number of waivers is limited to 30 per state, and less than 25% of the waivers can be allocated to specialist physicians (Zoghbi et al. 2004). To evaluate the feasibility of subsidies versus targeted immigration, we conducted separate simulations.
Subsidy
For a subsidy to motivate physicians to undertake more outreach despite the reduction in the overall supply of cardiologists, we have to consider the primary impediment: the opportunity costs associated with time lost due to travel. In 2019, the average cardiologist's salary was $430,000. Based on a typical 2,080-hour work-year, this translates to a per-minute cost of $3.45. We used this figure to estimate the cost of fully mitigating the negative impact of a 10% decrease in cardiologists.
Our aim was to determine the amount of money that would close the outreach gap, starting from the counterfactual of a 10% reduction in cardiology supply. We assumed each practice had access to a subsidy awarded for each minute of outreach travel time throughout the year.
7
To simulate the impact of this subsidy on behavior, we modify the coefficient on travel time (β2). The intuition is that each minute of travel time is made less costly by the subsidy. The travel time coefficient is not scaled to U.S. dollars, nor is it on the utility scale (because of the exponential in Equation 2). To convert money into the scale of the time coefficient we start by observing that, according to the preceding calculation, a minute for a cardiologist is worth $3.45. At the same time, each minute in travel time has an impact of β2 on marginal utility. A per-minute subsidy of ϕ, then, is worth the fraction of β2 given by
The simulation procedure takes the following steps, for 375 postconvergence parameter draws:
Set ϕ at $.05, and compute Using Check whether the number of days of outreach is at least as large as actual 2019 outreach.
If yes, stop. Calculate the subsidy cost given simulated outreach. If no, increment ϕ by $.05 and start at Step 2.
The annual subsidy amount is computed in Step 3a using the following formula, where

Recall that we assumed a binding constraint. This means that the total amount of time spent across all locations and practices is necessarily 10% lower than that observed in 2019, regardless of the subsidy amount. The subsidy only reallocates time to rural locations and thus results in the same level of rural access to care as observed in 2019, albeit with fewer doctors overall in the state.
As a plausibility check, we compared $406,000 to a “back-of-the-envelope” calculation. The observed total number of outreach days offered in 2019 is 3,264. Assuming a 10% decrease in outreach from the reduction in supply leaves a gap of roughly 326 days. If we assume eight-hour days at hourly rates of $207 ($430,000/2,080), the value of a day is $1,654. Then our back-of-the-envelope estimate of the dollar value of a reduction in supply is $540,000. This suggests that the estimate of $406,000 is on a reasonable order of magnitude.
The fact that the subsidy figure generated by our model is lower may be the result of two factors. First, the back-of-the-envelope calculation does not account for practice heterogeneity, whereas the subsidy simulation model did. Practices that are better placed to take advantage of the subsidy would likely do so, which increases efficiency in terms of outreach impact per dollar. Because our model is estimated on detailed data about long-term behavior, it is better placed to predict which practices are likely to take advantage of the subsidy more intensively. The second factor is that the back-of-the-envelope calculation assumes that a 10% reduction would have proportionate impacts on home and away locations. However, our simulation predicted that a 10% reduction in cardiology supply would disproportionately impact time spent at home. Specifically, the simulation predicted that the total decrease in time spent was split roughly 40:60 between outreach and home, respectively. This means that the back-of-the-envelope calculation may have overstated the size of the outreach shortfall in the first place. These reasons together suggest that $406,000 is a plausible figure.
The subsidy's simulation results are reported in Table 7. Also shown are the findings for the targeted immigration simulation (discussed next). These findings are presented together to facilitate comparison.
Mitigation Strategy Comparison.

Targeted Immigration
The counterfactual for targeted immigration used a similar approach to the subsidy simulation: the starting point was an outreach gap caused by a 10% decrease in the number of cardiologists. The goal was to completely close the outreach gap. A key distinction, however, is that targeted immigration actually increases the total supply of cardiologists, unlike the subsidy, which reallocates time from some cardiologists' home locations to rural outreach locations.
A constraint on targeted immigration was that most rural locations could not feasibly host a new cardiology practice. To select plausible locations, we limited our focus to those that had a full-time cardiologist at some time between 1990 and 2019. The hospitals in these rural cities presumably had, at one time, the requisite staff to support a local cardiologist. The four locations were Bettendorf, Cresco, Marshalltown, and Onawa. The simulation procedure follows, for 375 postconvergence parameter draws:
Find the rural location with the largest outreach shortfall (“hardest hit”). Find the closest feasible community location (among the four listed previously) for a new cardiologist. Resimulate with a new cardiologist located in the community selected in Step 2. Check whether the number of days of outreach is at least as large as the actual 2019 outreach.
If yes, stop. If no, start again at Step 1.
We set a minimum outreach percentage of 10% for each newly recruited cardiologist (i.e., the cardiologist must allocate at least 10% of time away from the home location). Our justification was that a policy intended to increase outreach would presumably come with this attendant condition attached. This threshold ensured that a new IMG cardiologist would staff outreach locations as this is the ultimate goal of the targeted immigration program.
We found that in almost all 375 simulations (98%), the outreach gap was closed by adding three to six new IMG cardiologists. The average is 4.4, so we round up to five to ensure that all outreach is restored. The recruiting and setup costs associated with bringing five new cardiologists to the state are not straightforward to compute. However, we note that the cost per cardiologist at which the subsidy and targeted immigration costs break even was $81,000 at the mean. In other words, for targeted immigration to break even with the per-minute travel time subsidy program, it must be possible to attract and retain five cardiologists for $81,000 or less on average per year.
We could not determine the required level of support to fully compensate cardiologists in these rural locations, but the break-even figure cited previously is likely to be greatly exceeded. Consider a situation in which one of three rural hospitals mentioned previously (Cresco, Marshalltown, Onowa) recruits a new, full-time cardiologist. This cardiologist would not perform invasive procedures as these rural hospitals do not have cath labs (nor does Bettendorf, but there is a remote possibility of providing procedural care in a competing hospital in an adjacent city). In an ideal situation, this new rural-based cardiologist would see patients full time in the local community (and in outreach locations), thus eliminating the need for these patients to travel to an urban location for office-based care. Assuming a schedule of 15 patients per day and a 300-day work year, this would result in a total wRVU production of 4,500. There would also be additional wRVUs for diagnostic test interpretation. This could raise the wRVU total by 25%–30%, thus resulting in a total wRVU of 5,850. However, this is approximately 60% of the median 9,642 of wRVU production for the typical cardiologist. The shortfall in wRVU production would mean that the hospital would have to subsidize this position at a level of $172,000 per cardiologist per year. This figure greatly exceeds the break-even values noted previously. Although more office-based cardiology care would be available in a small number of selected rural hospitals, it comes at a very high cost especially when compared with widespread impact of the travel cost subsidy strategy.
Furthermore, additional practical considerations would argue against the strategy of recruiting a new cardiologist for a rural location. Any rural location with a single cardiologist would most likely not be practicable, as a single physician could not provide call coverage for every night and weekend. A second cardiologist would need to be recruited for each rural location. Thus, the incomes of two cardiologists would have to be supplemented to provide expanded access to patients from these rural hospitals.
Discussion
Rural patients in the United States tend to have worse outcomes regarding cardiovascular disease than people living in urban areas. The AHA and ASA have asked their members to address this persistent disparity that affects 60 million people nationwide (Harrington et al. 2020). The AHA and ASA have identified three major forces driving the inequity of outcomes for rural patients: individual factors (e.g., obesity, smoking, inactivity), social determinants (income, education), and health delivery system issues.
Among the health delivery system solutions proposed are new models and sites for delivery of cardiovascular care. One such option is the focus of this article: provision of rural-specific care delivery sites where patients receive specialty office-based care in their own communities (Harrington et al. 2020). By leveraging existing medical infrastructure, outreach clinics can ensure that cardiology care is more widely available and delivered efficiently. In this study, we model the site location and clinic frequency decisions by cardiologists staffing outreach sites across Iowa, an area encompassing more than 55,800 square miles. We center on this cardiology care delivery system as it has been operating successfully for over 30 years (Tracy, Saltzman, and Wakefield 1996) and has been shown to markedly improve patient access to local care (Gruca, Pyo, and Nelson 2016).
Our empirical results suggest that several major factors determine whether a cardiologist will host an outreach clinic at a given location. First, both direct and indirect costs for the physician are increased owing to travel distance. Second, because the payoffs of outreach also include revenue from future patient procedures and follow-up visits, the size of the patient pool has a significant influence. Third, the proximity of an outreach location to a competing cardiology practice affects its attractiveness. We also find that practices exhibit inertia in their allocations.
Competition and Patient Access
Our results show that, in some ways, competition can reduce the availability of cardiology care via rural outreach. This is a surprising outcome. Research on competition in health care suggests that increasing competition among practices reduces fees and/or increases access (e.g., Rivers and Glover 2008). In the case of rural outreach, two simultaneous competitive effects are present. First, cardiologists are predominantly located in urban areas, which increases the level of competition for urban patients. Thus, specialist physicians have an incentive to shape the decision making of rural patients in order to secure their procedural revenue. Therefore, high levels of competition within urban areas motivates cardiologists to offer rural outreach clinics. The net effect is to enhance access to routine cardiology care for rural patients. This is the expected positive impact of competition that benefits patients.
The second, and unexpected, effect suggests that competition among practices inhibits the establishment and staffing of some rural outreach clinics. Cardiology practices from the same urban area may wish to offer outreach in the same nearby rural town. In addition, cardiologists from a completely different urban area may find that rural site attractive. Given that the future payoffs of rural outreach are uncertain whereas the direct and opportunity costs are immediate, the presence (or potential presence) of a rival can inhibit creation of a VCC arrangement with a rural site that would otherwise be attractive. Therefore, competition between cardiology practices may also reduce access to care for some rural patients.
Policy Alternatives and Implications
We used the model to investigate potential effects of the expected decline in the number of cardiologists (Fry 2022; Rodgers et al. 2009; Sauer 2020). Simulating a 10% reduction, we found that the negative impacts fall unequally across rural outreach sites. Specifically, those rural locations that draw from only one urban area are less likely to retain their outreach clinics than those that may be reasonably staffed from multiple urban centers. This is an important insight for policy makers and insurance providers (including Medicare). Rural patients that do not receive adequate specialist physician care are more likely to have preventable hospitalizations, which unnecessarily increase spending (Johnston, Wen, and Joynt Maddox 2019). Moreover, rural patients without regular access to specialist care have higher levels of mortality; such losses ripple out from their families to their communities and ultimately society as a whole. One suggested intervention to close this gap is the “creation of opportunities for specialists to provide intermittent care for rural areas” (Johnston, Wen, and Joynt Maddox 2019, p. 2001). This is exactly the role of rural outreach by VCC cardiologists today. However, this successful health care delivery system may be undermined as the supply of cardiologists decreases.
We simulated two counterfactual policies for mitigating negative impacts of a cardiologist shortage: a subsidy program and targeted immigration. Targeted immigration requires a mean of five new cardiologists to restore outreach. However, to break even with a subsidy, the total cost of supporting a new cardiologist must average below $81,000, annually. The actual costs may be over two times that level. In contrast, a subsidy can restore outreach efficiently by providing incentives for cardiologists to allocate more time away from their home location.
In this study, we focused on in-person outreach by specialist physicians. Another option for expanding access for rural heart patients is telehealth. However, few rural hospitals have a telehealth program in cardiology. Indeed, a 2013 study found that only 6.2% of rural hospitals had a cardiology, heart attack, or stroke telehealth program (Ward, Ullrich, and Mueller 2014). Overall, less than one-third of all rural hospitals had any operational telehealth program of any type. Furthermore, there are issues regarding reimbursement for cardiac telehealth consultations (Thomas and Capistrant 2015). In addition, telehealth requires reliable, high-speed internet access, which can be a problem in many rural areas.
A final barrier to telehealth involves patient attitudes toward it. A pre-COVID survey in Montana—a largely rural state served by multiple telehealth systems—found that more than 40% of respondents were “unequivocally averse to telemedicine” despite the reduction of travel time and other costs for patients (Call et al. 2015). During the COVID-19 pandemic, many states relaxed their restrictions regarding telehealth, but whether these changes will persist is uncertain. Moreover, a recent study of cardiac patients in Los Angeles County examined their use of telehealth during the COVID-19 pandemic (April 1, 2020–December 31, 2020). The study shows that, despite the availability of telephone and video appointments, more than 80% of clinic visits were in-person (Yuan et al. 2021). Intriguingly, these patients had better access to high-speed internet and lower travel burdens than rural patients; nevertheless, they chose to see their cardiologists face-to-face, despite the risks of contracting COVID-19. These findings are consistent with those from McKinsey showing that less than 10% of cardiology office visits during the pandemic utilized telehealth (Bestsennyy et al. 2021). Although these data do not directly provide insights into rural patients and their propensity to use telehealth services, they suggest that cardiac patients prefer to see their cardiologist in person.
In terms of longevity (more than 30 years) and physician participation (45% of cardiologists in 2014), the system of cardiology VCCs in Iowa is a success. However, the rapid aging of the U.S. population and projected reductions in the supply of cardiologists will present new challenges to this method for providing outreach to rural patients. As our counterfactual analysis shows, outreach provision is sensitive to supply reductions. Rural towns located far from urban centers or serving a small number of patients will likely lose local cardiology care. However, our results reveal that such changes may be modeled and anticipated in advance, and at least one solution for mitigation—direct subsidization—seems promising.
Limitations and Future Research
This study has certain limitations. We included lagged terms in the model, and decision makers were assumed to treat separate years independently (conditional on the lagged term) and were not forward-looking. Therefore, in the spirit of Frick, Iijima, and Strzalecki (2019), future research could explore forward-looking versions of the model. In addition, we mainly focused on rural outreach in our analysis. Modeling physician activity in the home market could prove useful, but it would require detailed data on time allocations between procedural care and office visits. Also, modeling the role of outreach on the referral patterns of primary care physicians could be interesting since not all rural towns have access to local cardiology care. Despite its importance in medical care, the referral process between physicians is an understudied topic.
Future empirical research is needed on many fronts. These include collecting data on VCCs in other states, as well as for other key specialist physicians affected by the aging population and provider shortages (e.g., medical oncologists). Moreover, researchers should further examine patient attitudes toward telehealth and its impact on usage/compliance. The problems of providing access to care in rural areas are long-standing, and thus more research that focuses on the issue is needed.
Our study models decisions by physicians that are, at the same time, intended to build their practices (a typical marketing objective) and have a major effect on health care access for a chronically underserved market (a major public policy challenge). Future research on health care markets needs to move beyond the usual focus on merely improving provider outcomes to advancing our understanding of the implications for patients. We provide a novel way to view the problem of patient access, as we show how it is influenced by the competitive marketing decisions individual providers make. We expect that using these two focuses (provider behavior and patient outcomes) will enable marketing scholars to provide valuable insights into other important and vexing health care problems.
Supplemental Material
sj-pdf-1-jmx-10.1177_00222429231207830 - Supplemental material for Bringing the Doctor to the Patients: Cardiology Outreach to Rural Areas
Supplemental material, sj-pdf-1-jmx-10.1177_00222429231207830 for Bringing the Doctor to the Patients: Cardiology Outreach to Rural Areas by J. Jason Bell, Sanghak Lee and Thomas S. Gruca in Journal of Marketing
Footnotes
Special Issue Editor
Harald van Heerde
Associate Editor
Pradeep Chintagunta
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.