
Abstract
Handwriting difficulties are frequently mentioned in descriptions of developmental coordination disorder (DCD). Recent studies have shown that children with DCD pause more and produce less text than typically developing (TD) peers. This temporal dysfluency indicates a lack of automaticity in handwriting production. One possible contributing factor is the accuracy and consistency of letter formation. The aim of this study was to gain a better understanding of handwriting dysfluency by examining the accuracy and consistency of letter production both within and across different writing tasks. A total of 28 children aged 8 to 15 years with DCD participated in the study with 28 TD age- and gender-matched control participants. They completed the alphabet writing and copy fast tasks from The Detailed Assessment of Speed of Handwriting on a digitizing writing tablet. The accuracy and consistency of letter production were examined. The DCD group had a higher percentage of errors within their letterforms than did the TD peers. Letter production was also less consistent between tasks. Children with DCD appear to have difficulties with the “allograph” (motor program) aspect of handwriting and may require explicit teaching of letter formation.
The skill of handwriting plays an important role in the overall task of writing as there is substantial evidence to support the relationship between transcription skills (handwriting and spelling) and the quality of written composition (Berninger et al., 1994). Handwriting speed (the number of letters or words written per minute) is thought to reflect automaticity of writing and has been shown to predict compositional quality in children who are developing typically (Berninger et al., 1994; Graham et al., 1997; Puranik & Al Otaiba, 2012) and atypically (Connelly et al., 2012; Prunty et al., 2016; Sumner et al., 2014). If a child has difficulties with producing handwriting that is fast and legible, it therefore may affect their academic performance (Graham et al., 2000).
One group known for their difficulties with handwriting are children with developmental coordination disorder (DCD), which is the term used to describe children who have motor coordination difficulties unexplained by a general medical condition, intellectual disability, or sensory or neurological impairment (American Psychiatric Association [APA], 2013). Handwriting difficulties are mentioned in the formal diagnostic criteria for DCD (APA, 2013) and are frequently reported as the most common reason for referral to occupational therapy services for this group (Asher, 2006). In the few studies that have examined handwriting in any detail in children with DCD, difficulties with both handwriting speed and legibility were reported (Barnett et al., 2018; Huau et al., 2015; Prunty et al., 2013; Rosenblum & Livneh-Zirinski, 2008; Smits-Engelsman et al., 2001). In addition, some studies examined the handwriting process using writing tablet technology to explore the real-time movements of the pen. These have found that children with DCD spend a greater percentage of time pausing during writing compared with typically developing (TD) peers (Prunty et al., 2013; Rosenblum & Livneh-Zirinski, 2008). In our previous work, we have attempted to characterize this pausing behavior by analyzing the location of pauses. We found that the children with DCD produced a higher percentage of within-word pauses compared with TD peers (Prunty et al., 2014). According to Kandel et al. (2006), within-word pauses are an indication of a lack of automaticity or “fluency” in handwriting. They argue that skilled writers have the ability to program the spelling and movement components for a word prior to commencing it, followed by an ability to execute the word without stopping (Kandel et al., 2006). Given that children with DCD do not seem to acquire this level of skill (Prunty et al., 2014), it is important to investigate the reasons for this to inform clinical practice. In addition, it has been well documented that DCD can co-occur with an autism spectrum disorder (ASD; Mari et al., 2003), attention-deficit/hyperactivity disorder (ADHD; Piek & Dyck, 2004), developmental language disorder (formally specific language impairment [SLI]; Gaines & Missiuna, 2007), and dyslexia (Kirby et al., 2008). These co-occurring difficulties are known to have an impact on the handwriting process in their own right. For example, children with dyslexia produce fewer words per minute compared with TD peers (Sumner et al., 2014) as do children with language impairment (Dockrell & Connelly, 2013). To understand the role of co-occurring conditions in the handwriting of children with DCD in future studies, we need to understand the unique role of motor difficulties in this group first.
According to Fitts and Posner (1967), a learner becomes automatic or fluent at a skill following extensive practice of movement patterns. From 2 to 3 years of age, children produce “writing” that is generally distinguishable from their drawing (Mortensen & Burnham, 2012; Treiman, 2017). At 3 years, they produce simple linear strokes, segment (often pretend) letterforms, and simple written units (small clusters of letters; Puranik & Lonigan, 2011). With the natural development of language and motor skill, together with formal instruction, these movement patterns become more refined to express meaning through specific letter shapes. According to Van Galen’s (1991) theoretical model of handwriting, the motor commands required to form a letter are referred to as “allographs.” This is where activation occurs for the motor program—which is a set of motor commands that define the essential details of the action. This requires knowledge about the movement patterns involved in a letterform, including where the letter starts, the sequence of the strokes, and the direction in which the strokes are formed (Van Galen, 1991). Problems with allograph selection may be a contributing factor to handwriting difficulties in children with DCD as poor letter formation and a tendency to overwrite or add elements to already formed letters have been reported in the literature (Rosenblum & Livneh-Zirinski, 2008). There is also evidence that children with DCD encounter difficulties when learning new motor patterns (Bo & Lee, 2013) including letterforms, which is manifested through variability and inconsistency in the velocity and trajectory length of pen strokes (Chang & Yu, 2010; Huau et al., 2015). Indeed, the real-time movement of the pen can be used to quantify the accuracy and consistency of letterform production, which may shed more light on allograph selection. By examining the patterns involved in letterform production, factors such as whether the child starts a letter in the correct place, moves in the correct direction, or executes too few or too many letter strokes can be analyzed. Analyzing handwriting in this way will help to establish a better understanding of the handwriting process in children with DCD.
Study Aim
Previous analyses of letterforms in children with DCD have tended to focus on the handwriting product with either a global description of handwriting legibility (spatial arrangement; Rosenblum & Livneh-Zirinski, 2008) or an analysis of the shape of individual letters (Chang & Yu, 2010). To date, no study has examined each of the individual letters of the alphabet by taking into account the process of letter production. This type of analysis would help determine whether children with DCD have difficulties with forming specific letters or letter groups (families) with similar movement patterns. It would also inform focused interventions and approaches to teaching in the classroom. The aim of this study was, therefore, to understand handwriting production in children with DCD through an examination of the accuracy of letter formation using the real-time movement of the pen. Two letter production tasks were used to allow for an additional analysis of consistency of letter formation. Our predictions were that children with DCD produce a higher percentage of errors in letterform production and are less consistent in letterform production compared with TD children. Our aim was to identify in this exploratory study which letters in particular were problematic to inform the teaching of handwriting.
Method
Research Design and Participants
A non-experimental between-group design was used to evaluate the accuracy and consistency of letter formation in children with and without DCD on two handwriting tasks. A total of 56 children aged 8 to 15 years participated in the study; 28 children with DCD (27 boys, 1 girl) were matched for age (within 4 months), gender, and handedness with 28 TD controls. To select participants for both groups, we used the same procedure as described in our earlier studies (Prunty et al., 2013, 2014, 2017). Children in the DCD group were recruited through advertising provided at parent support groups, given to schools, and posted on the research group website. The four criteria from the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) were used to assess children with DCD in line with the current European guidelines (Blank et al., 2012). All children scored below the 10th percentile on the second edition of the Movement Assessment Battery for Children (MABC-2; Henderson et al., 2007; Criterion A). These motor difficulties had a significant impact on their activities of daily living (Criterion B), as reported by their parents and evident on the MABC-2 checklist. Developmental, educational, and medical histories were taken from the parents, which confirmed that there was no history of neurological or intellectual impairment and no medical condition that might explain the motor deficit (Criteria C and D).
The control group was recruited through local primary and secondary schools in Oxfordshire, England. Teachers were asked to identify children who did not have difficulties with motor skill, reading, or spelling. All children were assessed to confirm that they had a score above the 16th percentile on the MABC-2 and no evidence of a reported physical, sensory, or neurological impairment. Children were included in the control group if they scored at the level expected for their age on all measures outlined below (no more than 1 SD below the mean).
Exclusion Criteria
Children from both groups with a diagnosis of dyslexia and/or those who had English as a second language were excluded from the study. This was to control the confounding role of language (Dockrell & Connelly, 2013) and spelling (Sumner et al., 2014) on handwriting performance and to ascertain a detailed understanding of handwriting difficulties in children with DCD only. As such, children with a physical, sensory, or neurological impairment were also excluded. This was to ensure that handwriting difficulties could not be attributed to other disorders.
Selection Measures
The MABC-2 was used to identify children with significant motor difficulties, with performance below the 10th percentile (24 below the 5th, 4 below the 10th) on the test component. The MABC-2 examines three components of motor competency: manual dexterity, aiming and catching, and balance in children aged 3 to 16 years. These motor difficulties had a significant impact on their activities of daily living, as reported by their parents and evident on the MABC-2. Reliability of the Total Test Score has been reported as good at .80 (Henderson et al., 2007).
The second edition of the British Picture Vocabulary Scale (BPVS-2; Dunn et al., 1997) was used to obtain a measure of receptive vocabulary that correlates highly with verbal IQ (Glenn & Cunningham, 2005). It is a standardized test with U.K. norms and is commonly used to examine the level of receptive vocabulary in children. Reliability of the BPVS-2 has been reported as good at .86 (Dunn et al., 1997). Performance on the BPVS-2 was in the average range for all children, confirming the absence of a general intellectual impairment.
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) was also used to note other parent-reported behavioral difficulties that commonly occur with DCD, such as attention deficits (Blank et al., 2012). The SDQ was designed for assessing the psychological adjustment of children aged 3 to 16 years. It consists of 25 attributes and uses a 3-point Likert-type scale to indicate how much an attribute applies to the child. The SDQ has been advocated as a useful measure in identifying emotional and behavioral difficulties and has good reliability (internal consistency α = .73) and validity (scores above the 90th percentile predict a substantially raised probability of independently diagnosed psychiatric disorders; Goodman, 2001). Seven children in the DCD group had a “slightly raised” profile in hyperactivity. However, no child had a diagnosis of ADHD.
The second edition of the British Ability Scales (BAS-II; Elliott, 1996) was used to examine the performance on single word reading and spelling tasks. The BAS-II has U.K. norms for children aged 5 to 18 years. The reading and spelling tasks have high internal reliability (α = .84–.95). The BAS-II revealed that eight children with DCD had literacy difficulties (one in reading, seven in spelling), as defined by a standard score of less than 85 on the BAS-II components, although none had a formal diagnosis of dyslexia or other language impairment (see Table 1 for performance profiles of both groups).
Means, Standard Deviations, Ages, and Performance Scores for DCD and TD Groups on Selection Measures.
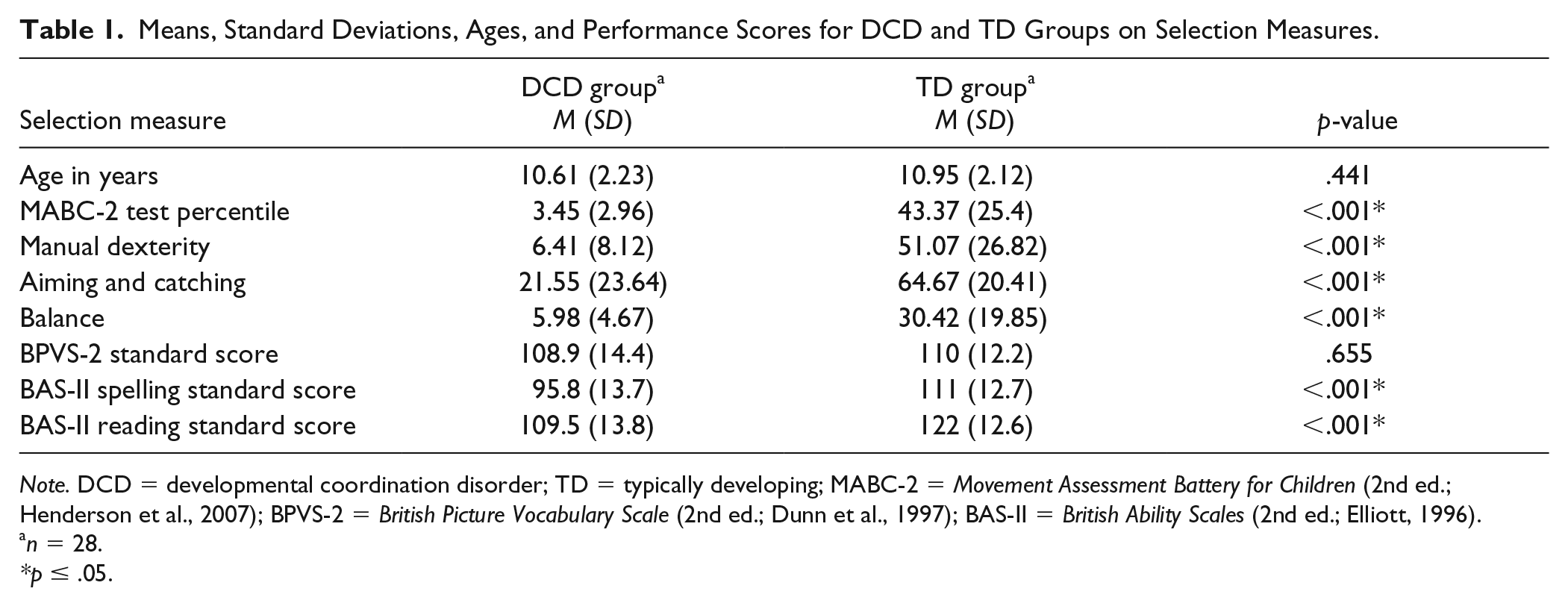
Note. DCD = developmental coordination disorder; TD = typically developing; MABC-2 = Movement Assessment Battery for Children (2nd ed.; Henderson et al., 2007); BPVS-2 = British Picture Vocabulary Scale (2nd ed.; Dunn et al., 1997); BAS-II = British Ability Scales (2nd ed.; Elliott, 1996).
n = 28.
p ≤ .05.
Handwriting Measures
The Detailed Assessment of Speed of Handwriting (DASH; Barnett et al., 2007) is a standardized handwriting speed test with U.K. norms for 9- to 16-year-olds. The product scores (number of letters/words per minute) for both groups were reported in Prunty et al. (2014). In this study, two tasks from the DASH were implemented, both of which were deemed appropriate for children aged 8 years and older. The interrater reliability for both tasks was .99. The tasks consisted of the following:
Task 1: Alphabet writing. The child wrote the alphabet repeatedly from memory as fast as possible for 1 minute. He or she was instructed to write it in the correct order using lower case letters, making sure that every letter was readable.
Task 2: Copy fast. The child copied the sentence “The quick brown fox jumps over the lazy dog” as quickly as possible for 2 minutes. This sentence includes all letters of the alphabet and thus provides an opportunity to examine each individual letterform.
Apparatus
When completing the two DASH tasks, the participants wrote with an inking pen on paper placed on a Wacom Intuos 4 digitizing writing tablet (325.1 mm × 203.2 mm) to record the movement of the pen during handwriting. The writing tablet transmits information about the spatial and temporal data of the pen as it moves across the surface. The data were sampled at 100 Hz through a laptop computer. Eye & Pen version 2 software (EP2; Alamargot et al., 2006) has a video function that allows researchers to replay the handwriting production in real time on a laptop.
Procedure
The handwriting component of this study took place during one 60-minute session. Each child was assessed individually by the first author (M.P.), who is a trained occupational therapist. During the handwriting tasks, the children were seated at a height-adjustable table and chair, with knees positioned at approximately 90 degrees and elbows approximately 2 to 4 cm above the table. The participants were encouraged to position their paper as they would normally do in the context of their natural environment; therefore, they were invited to maneuver the tablet to a position that was comfortable for them.
Coding Analysis
Accuracy of letter formation
In the United Kingdom, children may be taught different handwriting styles at school, which include variations of joined or unjoined letterforms. In this study, coding of errors in letter formation did not reflect handwriting style but focussed on universal aspects of letter formation that apply across all handwriting styles taught in the U.K. school system. The focus here was to examine the accuracy of the allograph (Van Galen, 1991); therefore, handwriting style did not have an impact on analysis.
The handwriting production was viewed by the first author and coded for accuracy and consistency of letter formation. Letter production was played and replayed in slow motion and was paused if needed to allow for accurate coding of the process. In order to classify the errors in letter formation, the following categories were used:
Incorrect direction of letter stroke. For example, a clockwise rather than anti-clockwise direction when forming the letter a or o (letters that may have appeared appropriate on paper but when production was replayed, incorrect letter stroke directions were revealed);
Incorrect start place. For example, the letters r, n, or i starting at the baseline rather than in the middle of the lines;
Letters with missing strokes. For example, the letters t and f written without the cross stroke or r, n, u completed with one stroke rather than two;
Letters with added strokes. For example, overwriting on strokes already formed;
Letter reversals. For example, the letter b appearing as d.
Using these categories, the following variables were calculated for the alphabet task for each child:
Percentage of letters with production errors;
Percentage of production errors in each category. It was also noted whether each child displayed production errors in more than one of the error categories.
Consistency of letter formation
The consistency of letter formation was established by comparing the performance on the alphabet task to the performance on the copy fast task. Only those letters produced in the alphabet task were examined in the copy fast task for each child. If a child only produced the first 14 letters of the alphabet (a to n), for example, the same 14 letters were examined in the copying task. As above, the letters were played and replayed in slow motion to allow for the categorization of errors. The consistency of letter formation was examined for each child by calculating the following:
The percentage of letters with production errors in the alphabet task that had the same errors recorded in the copying task;
The percentage of letters with production errors in the alphabet task that had different errors recorded in the copying task.
Production of letter groups/families
The letters of the Latin-based alphabet are sometimes grouped together into letter “families” for the purpose of teaching letter formation (Department for Education [DfE], 2001). The groups are usually defined by either the shape of the letters (ascenders and descenders) or the movements required in forming them (curves). While there are variations of letter families, this study applied those recommended by the DfE (2001), which are grouped according to movement patterns. Figure 1 illustrates the four letterform families: c, r, l, and z.
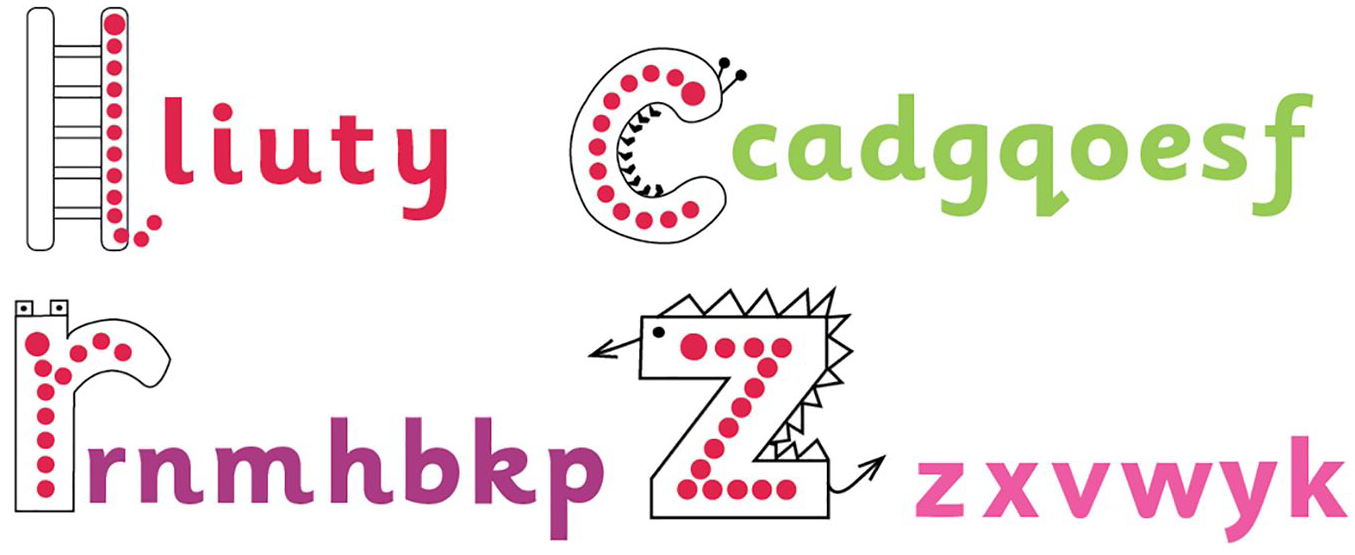
Four families of letterforms.
For the final analysis, each letter that was produced on the alphabet task was examined for accuracy, and the number of children in each group who made an error in each letter was calculated. The nature of the errors was categorized and the frequency of the error types was reported for any letter that yielded a significant group difference.
Interrater Reliability
Since the scoring criteria for identifying errors in the production of letterforms were novel, it was important to assess the reliability of scoring. An acceptable coefficient for interrater reliability would be above .70, but preferably above .80 (Landis & Koch, 1977). The first author initially scored all of the alphabet task files on EP2. To check the reliability of scoring, 10 files (5 DCD, 5 TD) were randomly selected and scored by an external rater (a psychologist with particular expertise in children’s writing). The rater was unaware of the group allocation of the scripts. The interrater reliability (intraclass correlation coefficient) for the number of letters in the alphabet task with a process error was .89.
Statistical Analysis
We used t tests or the Mann–Whitney U test to examine the differences between the DCD and the TD groups, depending on the normality of distributions. For categorical data, chi-square tests of independence were used to examine group differences in the proportion of production errors. Significance was set at p < .05 in all cases.
Results
Accuracy of Letter Formation
All children in the DCD group made production errors compared with (23/28) 82% of the TD group. As shown in Table 2, the DCD group had a higher median percentage of production errors in the alphabet task compared with the TD group (U = 141.0, Z = −4.13, p < .001, η2 = .30).
Median (Interquartile Range) Percentage of Errors in the Alphabet Task for DCD and TD Groups.
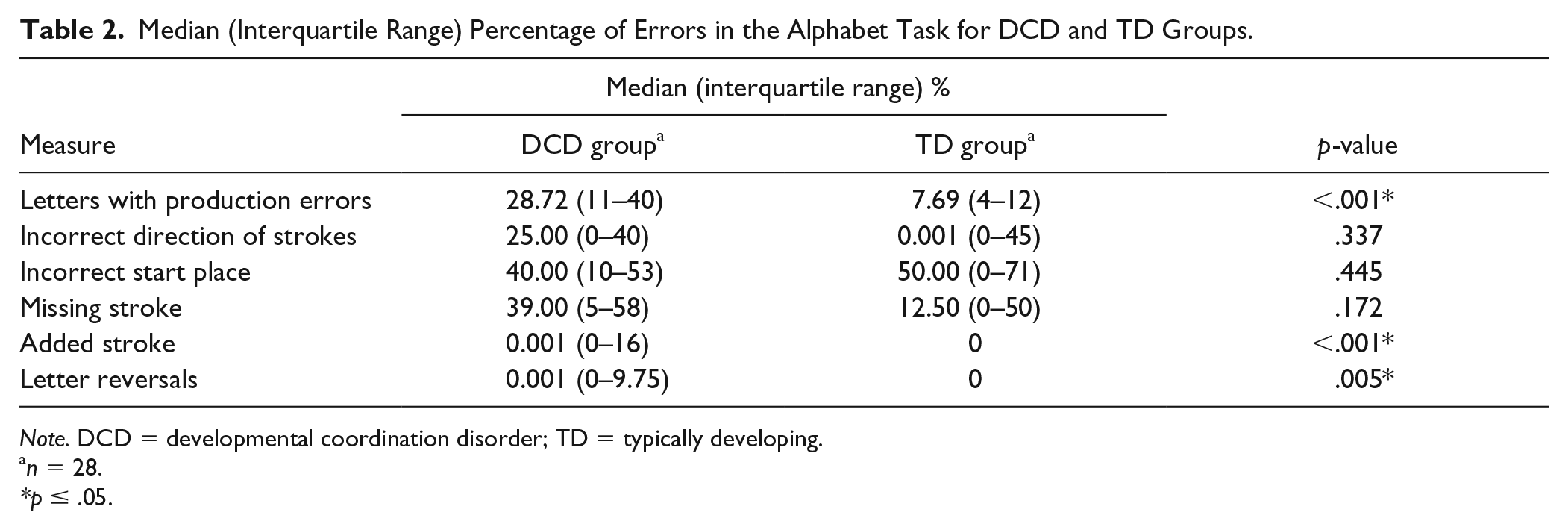
Note. DCD = developmental coordination disorder; TD = typically developing.
n = 28.
p ≤ .05.
Analysis of the error categories (see Table 2) showed higher median scores for the DCD group across all categories except for Incorrect Start Place, where the TD group exhibited higher median scores than the DCD group. However, the only significant group differences were for Added Strokes (U = 238.5, Z = −3.22, p <.001, η2 = .18) and Letter Reversals (U = 294.0, Z = −3.22, p =.005, η2 = .18). The percentage of these two types of errors in the DCD group was lower compared with other error types that they displayed. Also, no child in the TD group made Added Strokes or Letter Reversals. There was no effect of group for Incorrect Direction of Strokes (U = 335.5, Z = −.961, p =.337, η2 = .02), Incorrect Start Place (U = 346.0, Z = −.764, p =.445, η2 = .01), or Missing Strokes (U = 311.0, Z = −1.36, p =.172, η2 = .03). There was no effect of group for Incorrect Letters, with more than one error indicating that both groups (DCD, Mdn = 6.50; TD, Mdn = 0.001) made the same amount of errors within a letter (U = 299.0, Z = −1.75, p =.079, η2 = .05).
Consistency of Letter Formation
There was no effect of group when comparing the percentage of letters with errors in the alphabet task to the percentage of letters with the same errors recorded in the copying task (U = 299.0, Z = −1.75, p = .079, η2 = .05). This suggests that when both groups performed a letter incorrectly in the alphabet task, the same letter was still incorrect in the copying task. However, the DCD group had a significantly greater percentage of errors that were different in type between the alphabet and the copying tasks (U = 182.0, Z = −4.41, p < .001, η2 = .34). They had a tendency to produce inconsistent errors within the same letter, between the two tasks (see Table 3 for medians).
Median (Interquartile Range) Percentage of Production Errors on Both Tasks for DCD and TD Groups.
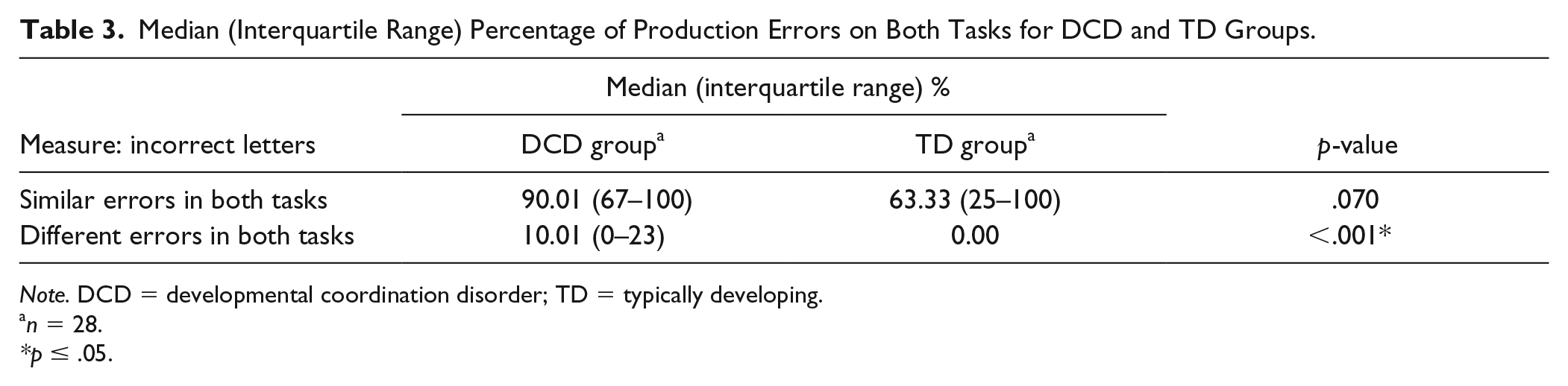
Note. DCD = developmental coordination disorder; TD = typically developing.
n = 28.
p ≤ .05.
Production of Letter Families
Table 4 reports the percentage of children in each group who made a production error in each letter. As can be seen, a higher percentage of children in the DCD group made errors in 11 letters across the four letter families. These were as follows:
l family i: χ2(1, N = 56) = 6.72, p = .010, η2 = .346 j: χ2(1, N = 56) = 4.08, p = .043, η2 = .270
c family a: χ2(1, N = 56) = 4.30, p = .038, η2 = .277 d: χ2(1, N = 56) = 16.04, p ≦ .001, η2 = .535 g: χ2(1, N = 56) = 5.49, p = .019, η2 = .313
r family r: χ2(1, N = 56) = 5.40, p = .020, η2 = .325 n: χ2(1, N = 56) = 7.52, p = .006, η2 = .377 m: χ2(1, N = 56) = 12.34, p ≦ .001, η2 = .478 h: χ2(1, N = 56) = 4.38, p = .036, η2 = .280 b: χ2(1, N = 56) = 6.17, p = .013, η2 = .332
z family z: χ2(1, N = 56) = 9.55, p = .002, η2 = .437
Percentage of Children in Each Group Who Made Production Errors in Individual Letters.
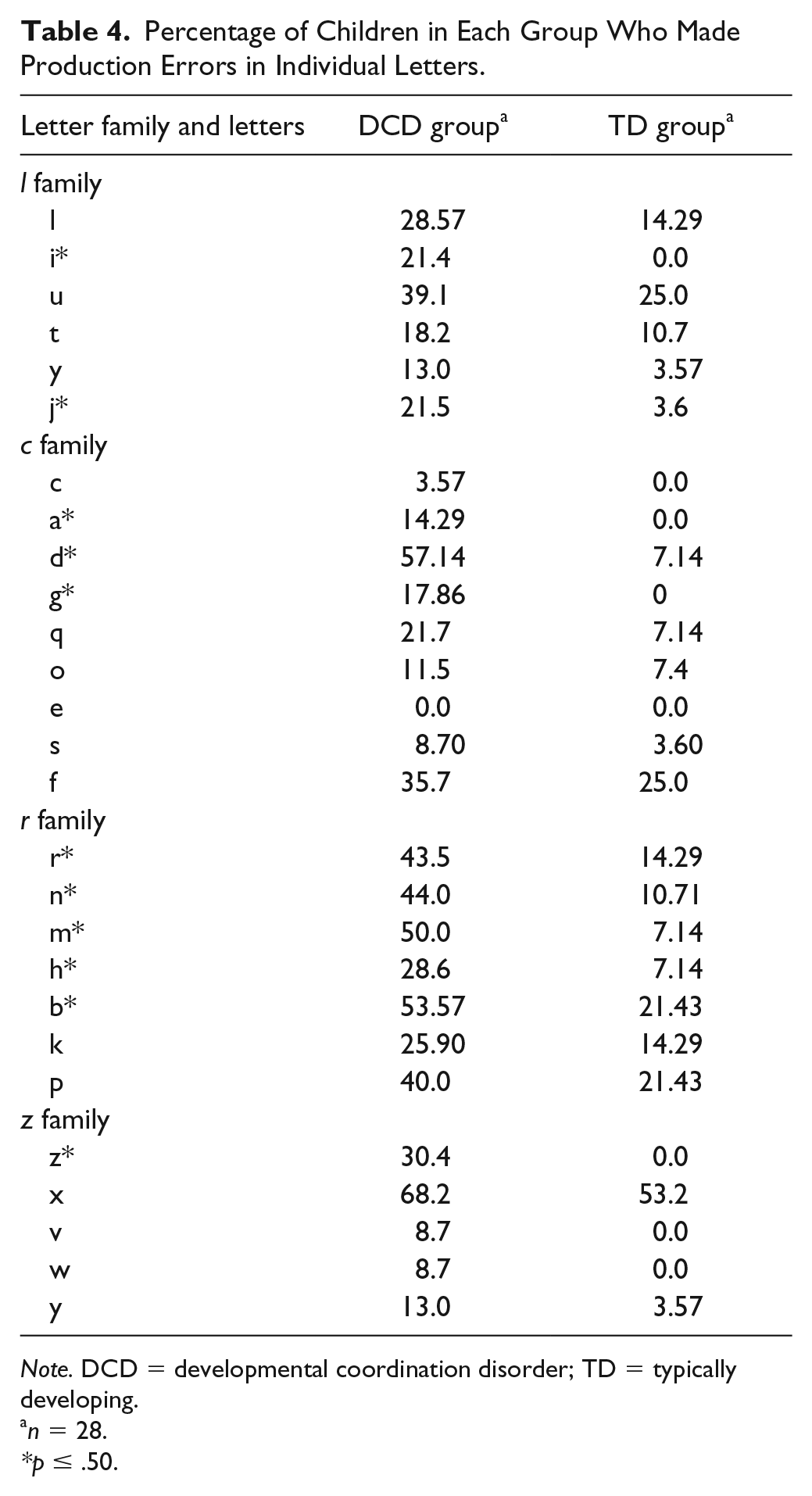
Note. DCD = developmental coordination disorder; TD = typically developing.
n = 28.
p ≤ .50.
From Table 4, it seems that it was within the r family that a greater proportion of children with DCD showed errors, with five of the seven letters more affected in this group compared with the TD group. Table 5 reports the percentage of error types within the 11 troublesome letters. The most common type of error was Incorrect Starting Place in nine of the 11 letters, followed by Incorrect Direction of Strokes and Missing Strokes in seven of the nine letters.
Breakdown of the Percentage of Errors Attributed to an Error Type for the DCD Group.
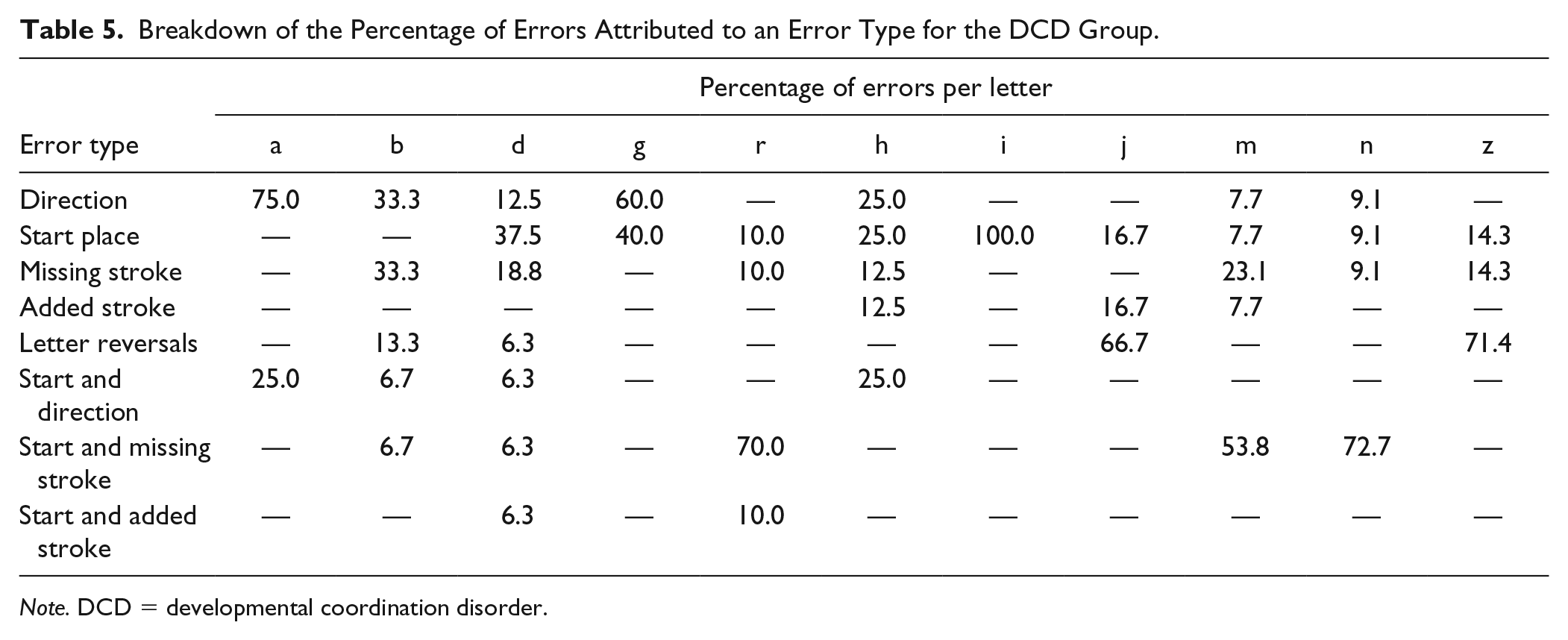
Note. DCD = developmental coordination disorder.
Discussion
In this study, we used a novel analysis to code and categorize errors in handwriting production through an analysis of the real-time movement of the pen. From a theoretical perspective, we were interested in examining the level of the allograph (the motor commands that define essential details of letter production) in Van Galen’s psychomotor model of handwriting in children with DCD. As predicted, our findings revealed that children with DCD produced a significantly higher percentage of production errors compared with TD peers. This indicated some difficulties with producing standard motor patterns required for letter formation. While this may not fully explain their difficulties with handwriting, it may contribute to some of the issues described in the literature, including poor letter formation and a tendency to overwrite on letters (Prunty et al., 2016; Rosenblum & Livneh-Zirinski, 2008).
We attempted to categorize the types of errors performed during the production of letterforms, which revealed a similarity in error types between both groups. The most common error made by both groups was the non-standard start position of a letter, while missing letter strokes was the second most common in the DCD group. Indeed, the issue of start position is interesting as it seems most of the errors in the TD group occurred in this category. One possible reason for this could have been attributed to the letter x where an error was coded if the participant started from the right side rather than the left side as outlined by the DfE (2001). On reflection, this criteria may have been too strict as the letter x appeared to pose the most issues for the TD group. Subsequently, this may have inflated the errors in start position reported for the TD group. However, an alternative explanation for this finding may relate to a possible lack of emphasis by classroom teachers on the correct starting position for letters. Although a description of classroom practice surrounding letter formation was beyond the scope of this study, it would be useful to explore this in future to help understand the influence of teaching practices on letter formation. In the United Kingdom, the statutory guidelines surrounding handwriting in the National Curriculum state that children should receive explicit teaching on handwriting. Therefore, future studies should take instruction into consideration to build a more complete picture.
An interesting finding in the DCD group was the high percentage of errors in the missing stokes category. It seems that some letters which started in the incorrect place (i.e., m) also contained fewer letter strokes. While this is not a method taught in schools (DfE, 2001), it occurred more frequently in the DCD group. This may have been related to difficulties in learning the correct sequence of the letters (Bo & Lee, 2013); however, it may have been an “economic” strategy employed by the DCD group to compensate for their movement difficulties. Future studies should examine this in more detail because it may have implications for the teaching and learning of handwriting in this group.
Another type of error explored in this study was letter reversal because there is anecdotal evidence that children with DCD produce reversals in their writing (Benbow, 2002). This was not one of the main errors seen in the current study, however. Although the DCD group appeared to make slightly more letter reversals and produce additional strokes compared with their TD peers, these errors did not occur frequently and not at all in the controls. This was an interesting finding because these two categories were the only two that yielded a statistically significant group difference but occurred less frequently than any other error type. As such, this raises a general point about the implications of our findings on practice: while high-frequency errors did not yield significant group differences, the errors that were statistically different might have been too infrequent to warrant attention in the classroom.
For determining consistency of letter production, we compared letter formation across the two writing tasks. Although not all children produced the full alphabet within the 1-minute time limit, it was evident that letters that were incorrectly formed on the alphabet task were also incorrectly formed in the copying task in both groups. However, the types of errors produced in the DCD group were not always consistent. For example, if a letter was performed in an incorrect way in the alphabet task, it was likely to remain incorrect in the copying task for both groups; however, the type of error made within the letter sometimes differed in the DCD group. This inconsistency may have implications for handwriting fluency given that acquiring automaticity in a skill requires that similar movement patterns be executed consistently (Fitts & Posner, 1967).
The reasons for the lack of accuracy and consistency of letter production in children with DCD are unclear. Proponents of one theory within the literature have suggested deficits related to motor sequence learning (Bo & Lee, 2013). Wilson et al. (2013) suggested that children with DCD can learn simple sequential movements, but handwriting involves 26 different letterforms of varying style (joined, unjoined, and capitalized); therefore, it may be more difficult for children with DCD to learn and retain such a variety of letterforms. This may be reflected in the types of errors that the DCD group made because they were more likely to perform errors associated with the initial pattern of letter formation (start position and missing strokes) rather than errors such as adding unnecessary strokes. It seems that they failed to learn the basic sequence of movements required for correct letter formation. Further investigation of the relationships among different errors may also help in understanding the characteristics of the errors seen. For example, it may be that once a letter is incorrectly started, there is a reduced likelihood of (or opportunity for) the addition of strokes, or that children with DCD are less likely to detect and/or correct errors. Huau et al. (2015) also reported difficulties with consistency in children with DCD when learning a new letterform. They found that despite a lengthy learning period, children in the DCD group exhibited more variability and inconsistency in performance (Huau et al., 2015). According to the authors, this instability of the motor program may be related to neuromotor noise in the system, preventing and disturbing the correct execution of motor patterns (Huau et al., 2015; Smits-Engelsman & Wilson, 2013). Further research is needed to explore this issue in more detail.
One important environmental factor to consider is the way in which children are taught handwriting in schools. Although handwriting is of growing importance in the U.K. educational system (DfE, 2013), the way in which it is taught can vary widely (Barnett et al., 2007). Given that practice and correct movement patterns are key elements in skills acquisition (Fitts & Posner, 1967), it is important to capture this when studying handwriting difficulties. Despite some emerging literature on difficulties with motor sequence learning in the DCD population (Wilson et al., 2013), it is not clear whether some of the issues explored in this study were linked to differences in teaching and opportunities for practice.
With regard to an applied perspective, we tried to ascertain whether specific letters were more problematic than others to inform intervention and strategies for teaching children with DCD. We found that children with DCD had particular issues with the r family of letters, with five of the seven letters affected. The main issue with these letters tended to be a combination of an incorrect starting place, missing stoke (letters n, m, r), or incorrect direction of strokes (b, h). The c family was the second most affected, with a, d, and g mainly affected. Here, issues with direction were most apparent in a and g followed by the correct starting place for d. This type of information may serve as useful guidance for teachers and therapists when deciding on where to focus interventions.
Study Limitations
One limitation of this study is the ability to generalize the findings to children with DCD who have co-occurring disorders. While this study controlled for factors such as reading ability, spelling ability, language, and attention, future research needs to consider children with co-occurring disorders, given the constraints of language on handwriting production (Connelly et al., 2012; Sumner et al., 2014). This study was also limited in terms of ethnic diversity and sample size and had a smaller proportion of females than reported in other studies (Rosenblum & Livneh-Zirinski, 2008). In addition, the lack of information surrounding how the children in this study were taught handwriting at school could be noted as a limitation. Finally, our focus here was on two short writing tasks from the DASH, limiting some aspects of the analyses and generalization of findings. The 1-minute alphabet task was not sufficient for all children to complete the full alphabet, and the 2-minute copying task had more constraints than a longer free writing task. In addition, the participants completed the handwriting tasks in a once-off session, which may not have been a true reflection of their handwriting performance.
Implications of Findings
One implication of this study relates to the importance of observation skills in educators and clinicians who work with children with DCD. While the use of digitizing tablets in this study allowed us to replay participants’ handwriting in real time, traditional measures of handwriting do not allow for this. It, therefore, is imperative that educators and clinicians observe children as they handwrite. By simply watching how a child produces letters, teachers could facilitate early identification and remediation of letter formation issues, which would support the development of handwriting speed later on.
This study also has implications for future research. While it revealed difficulties at the allograph level (Van Galen, 1991) in children with DCD, future research needs to investigate the levels of spelling, semantic retrieval, and syntax (language). Since DCD often co-occurs with difficulties in language, attention, reading, and spelling, additional studies are needed to provide insight into the role of these factors on the handwriting process of this group. A more comprehensive understanding of co-occurring conditions would go some way in informing more tailored interventions in the future.
Conclusion
Previous research has examined the quality of letter formation in children with DCD using the handwriting product, which is an approach widely used in practice both in the classroom and in the clinical settings. This exploratory study was the first of its kind to examine the accuracy of letter formation by analyzing handwriting production in real time. The findings went some way in categorizing issues with letter formation for children with DCD in a novel way. Further research is needed to refine and develop this method further. It does seems apparent that (a) this population demonstrates difficulties with particular letterforms and (b) explicit teaching of the skills should be considered in clinical and educational settings.
Footnotes
Acknowledgements
The authors would like to thank all of the families and children who took part in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.