
Abstract
While occupational health and safety scholarship has expanded in recent decades to include psychosocial hazards, there remains scant consideration of menstruation-related psychosocial hazards and harms, which women workers encounter at work. This article contributes to knowledge on menstruation-related workplace psychosocial hazards through examining the experiences of women working in the Bangladesh readymade garment industry. The article's purposes are threefold: first, to identify the psychosocial hazards that women workers experience during menstruation and the impacts on their physical and psychological health; second, to explain the prevalence of these psychosocial hazards; and third, to provide realistic regulatory and policy suggestions to eliminate these hazards in the emerging economy context. Using labour process theory, we argue that menstruation-related psychosocial hazards occurring in workplaces at the bottom of fast fashion supply chains where women workers continue to predominate are the product of systematic management strategies designed to secure capital accumulation through harnessing menstrual stigma in the organisational sphere. An understanding of the impacts of price and sourcing squeezes imposed on suppliers through global supply chains is crucial to informing practical policy interventions.
Keywords
Introduction
This article is concerned with the psychosocial hazards and harms women workers experience due to menstruation in developing countries. The occupational health and safety (OHS) literature has paid little heed to menstruation despite it being a regular natural health experience for most working women that contributes to workplace gender inequality (Sang et al., 2021). A growing policy attention on workplace menstrual health and hygiene issues, largely among public health and public policy experts in Western market economies, has led to the provision of industrial entitlements and other facilitative measures to assist women workers with menstrual health management (MHM) in many of these countries (Levitt and Barnack-Tavlaris, 2020; Patkar, 2020; Weiss-Wolf, 2020). However, these developments have largely not been mirrored in the Global South. To address this gap, this article sheds light on menstruation-related psychosocial hazards (MRPSH) in developing countries, through analysis of women workers’ experiences in Bangladesh readymade garment (RMG) factories. This study draws on labour process theory (LPT) (Braverman, 1974) to explain the dynamics of managerial control in relation to MRPSH in the garment manufacturing industry of Bangladesh. Using LPT, we examine how the menstruation-related bullying and harassment of women workers by managers are part of a systematic management strategy to meet the price and sourcing pressures imposed within global garment supply chains. Hence, we argue that the labour process has a direct influence on the formation of menstruation-oriented mistreatment in the workplace.
In recent decades, public health research and policy activism have highlighted how women's MHM is often impeded by limitations in access to health and hygiene facilities and the social and economic resources to effectively manage menstruation. Research and activism have centred mostly on Western market economies, leading to a range of public policy and, more recently, industrial relations, initiatives in many of these countries. These have included, for instance, promulgation of the ‘menstrual equity’ frame that has elevated recognition of the issue in the political sphere, advocacy campaigns to remove the ‘tampon tax’ in the USA, and subsequently Canada, England and Australia (Patkar, 2020; Weiss-Wolf, 2020), and the provision of menstruation-related industrial relations entitlements for women workers such as menstrual leave in some countries (Levitt and Barnack-Tavlaris, 2020; Sang et al., 2021). Menstrual equity agendas have extended from traditional health and hygiene concerns to highlighting the wider social and economic implications of menstruation through its role in gender discrimination and stereotyping (Weiss-Wolf, 2020). This policy momentum stands in stark contrast to the Global South, where such initiatives are not being considered. Nonetheless, in developing countries, recent research has drawn attention to menstrual health challenges related to the inadequate provision of safe and sanitary arrangements for MHM in many workplaces (Gaybor and Harcourt, 2022; USAID, 2019). Scholars and policy experts have largely attributed such challenges to the social stigma and taboos accompanying menstruation, women's poverty and limited public health investments (Hennegan et al., 2019; Sommer et al., 2016).
In contrast, our research among Bangladesh garment factory workers suggests that management deliberately harness and exploit socio-cultural menstrual stigma in their management of women process workers to minimise resistance and machine downtime and to maximise production. Utilising LPT as a conceptual framework, we argue that understanding MRPSH as management strategy is crucial to developing informed and realistic regulatory and policy responses.
Thus, this article contributes to conceptual understanding of why psychosocial hazards specifically related to menstruation commonly occur in the Bangladesh RMG workplace. To do so, we examine research findings on the perceptions and experiences of women workers in RMG factories concerning the nature of their work and the psychosocial hazards and harms encountered. The purposes of this article are threefold: first, to identify the MRPSH that women workers experience and their impact on workers’ physical and psychological health; second, to use a LPT lens to explain the prevalence of these psychosocial hazards; and third, to provide pragmatic suggestions for legislative and policy reform to reduce and eliminate the hazards and associated harms. The article begins with an analysis of the relevant scholarly literature on psychosocial hazards and MHM before examining conceptual approaches to understanding why the hazards arise in the work context. The subsequent sections of the article explain the research methods, the empirical findings and the implications for workplace psychosocial health and policy reforms.
Psychosocial hazards and MHM
Crucial concepts
This section examines the scholarly literature on psychosocial hazards and MHM with a focus on developing countries and the Bangladesh RMG sector. The term psychosocial hazards refer to a diverse and complex phenomenon arising from multiple sources in the workplace (Johnstone et al., 2011). According to the ILO, psychosocial hazards are those aspects of work design and the organisation and management of work, and their social and environmental context, which may have the potential to cause psychological or physical harm. (ILO, 1984)
A number of psychosocial hazards are associated specifically with MHM, including limitations in access to hygiene facilities and menstrual products (Sommer et al., 2016), and the social stigma and taboos that accompany the natural function of menses (Hennegan et al., 2019). Menstrual health is defined as a state of complete physical, mental and social well-being in relation to the menstrual cycle. Essential elements of menstrual health include that those who experience the menstrual cycle are appropriately informed, are able to care for their bodies during menstruation, can access timely treatment and care for discomforts and disorders, and experience a positive and respectful environment free from stigma and psychological distress in relation to menstruation (Hennegan et al., 2021).
Literature review on research in developing economies
To date, scholarly research on workplace psychosocial hazards has not dwelt specifically on hazards and harms associated with women's menstruation. This is, arguably, due to research and policy activism on MHM having developed largely through interdisciplinary work across the fields of public health and medicine, feminism and global development studies (Gaybor and Harcourt, 2022; USAID, 2019), rather than in studies of workplace and employment relations disciplines. Further, scholarly literature and research by non-government organisation on MHM in developing countries have focused mostly on the sanitation challenges of adolescent girls in school, rural and urban dwelling settings, rather than adult women (Sommer et al., 2016; USAID, 2019). The main identified challenges to MHM have included the stigmas and taboos around menstruation (Grandey et al., 2020; MacLean et al., 2020), inadequate societal infrastructure in terms of hygiene and sanitation (Rajaraman et al., 2013; USAID, 2019), and gender inequities in public health provision (Goldblatt and Steele, 2019; Patkar, 2020). While substantial research indicates a prevalence of poor MHM for schoolgirls and women in developing countries, a small but growing literature has looked at the challenges of women workers in managing menstruation at work (McCammon et al., 2020; Sommer et al., 2014, 2016). This research, again, has largely stressed the quality of water, sanitation, and hygiene standards and facilities as the key challenge for women workers, primarily in low- and middle-income countries (USAID, 2019). Key identified issues have pertained to the safety, privacy and cleanliness of hygiene facilities and inadequate provisions for MHM such as menstrual products, soap and water. For example, research has found that many women in the Indian construction sector experience poor MHM primarily due to the absence of toilet facilities on construction sites, and women garment workers in Cambodia fear being assaulted when walking outside to toilet facilities at night (Rajaraman et al., 2013; USAID, 2019). Similarly, research in Senegal has highlighted the inadequate provision of toilets and lack of privacy where toilets are mixed gender, unclean or unsafe (Speak Up Africa 2017 cited in USAID, 2019). Experts have argued these characteristics lead to both poor MHM and higher absenteeism among menstruating women (Speak Up Africa 2017 cited in USAID, 2019). Research has also found associations between poor MHM in factory settings, particularly where organisations do not provide access to menstrual products, and negative health outcomes such as stress and gynaecological disorders (Rajaraman et al., 2013; USAID, 2019). Further, Sommer et al. (2016) have observed that, even where adequate standards exist, without effective compliance mechanisms employers may not fulfil their obligations.
A significant gap in the existing literature on MRPSH in developing countries is research on how the practices of management may pose psychosocial risks to women workers. Some scholars have documented management practices as a source of menstrual health and hygiene challenges in the Global South. For instance, there are indications that where hygiene facilities exist, managers may prevent women workers’ access as required during menstruation (Rajaraman et al., 2013; Sommer et al., 2016). However, the reasons for the adoption of such management practices and their implications for psychosocial hazards and OHS, more broadly, remain largely unexplored. In this context, we argue, it is timely to examine psychosocial risks and hazards associated with menstruation in the workplaces of emerging economies.
Scholarly and policy discussions concerning how to improve women worker's opportunities for effective MHM in developing countries have concentrated on regulatory and public policy measures to increase the provision and safety of hygiene and menstrual health products, tackling the stigma associated with menstruation, and improving menstrual health literacy (Gaybor and Harcourt, 2022; Sang et al., 2021; Sommer et al., 2016; USAID, 2019). A key theme in policy discussions about improving MHM has been the entrenched nature of menstruation stigmas and taboos. As Sveinsdóttir (2017: 1391) has observed: Although menstruation is a shared experience for most women, it…historically has been surrounded with secrecy, shame, and lack of knowledge…[and] used to stigmatize and devalue women.
The Bangladesh RMG context
The Bangladesh RMG industry provides a fitting case study to research MRPSH because of the concentration of women workers in their reproductive years on the factory floor where the work is heavily machine-based. Since the industry's early decades, the main source of garment workers for low-grade work in factories has been and remains socially and economically disadvantaged young women, an estimated 90% of whom have migrated from rural areas (Afsar, 1994). Currently, women make up 60% of the RMG industry, with an average age of 25 years (Haque and Bari, 2020; Kanya, 2022).
RMG factories are typically characterised by a vertical gender segregation. While women are generally positioned as low-skilled workers, with absent or minimal career progression opportunities, men predominate in supervisory, middle, and senior management positions (Ahmed, 2004; Kabeer, 1991; Kabeer, 1994; Paul-Majumder and Begum, 2000). This spatial segregation by gender facilitates men's power concentration at the management level and reinforces women workers’ vulnerability and lack of voice and agency within organisations (Ahmed, 2004; Al Mamun et al., 2018; Gibbs et al., 2019). This vulnerability is compounded by the fact that only 5% of RMG factories are unionised and trade unions in Bangladesh remain heavily male-dominated, both in terms of members and leadership positions (Kabeer and Mahmud, 2004). Further, in organisations with a union presence, unions tend to have little workplace representation and few viable communication channels to the union leadership (Hossain and Akter, 2022).
While the Bangladesh RMG industry has sustained significant OHS reform in the past decade, largely in response to a series of industrial disasters, and particularly the 2013 Rana Plaza tragedy, which prompted the development of domestic legal reform, multi-stakeholder agreements and supply chain codes of conduct, change generally has centred on improvements to structural and building safety (Alamgir and Banerjee, 2019; Neve and Prentice, 2017; Prentice et al., 2018; Siddiqi, 2022). Historically, workplace psychosocial risks and hazards were overlooked in framing OHS law in Bangladesh. Thus, there is minimal regulation of psychosocial hazards, including those relating to menstruation, making the context both fertile and also challenging for regulatory and policy reform.
Drawing on empirical research among women workers in Bangladesh garment factories, this article argues that the MRPSH and harms that women workers encounter at work are rooted in systematic management practices. Using LPT, we argue that these management practices are part of a larger strategy of worker mistreatment designed to ensure a docile, compliant workforce to facilitate factories meeting the cost reduction and production deadline demands of global fast fashion supply chains. This article draws on a larger project that examined women workers’ experiences of psychosocial hazards in the RMG factories of Bangladesh (Author withheld, 2023). The project's broader findings on psychosocial hazards are consistent with previous research by scholars such as Siddiqi (2003), Ashraf (2017), Seneviratne (2019) and Pillinger (2016), which, while not using the concept of psychosocial hazards, found that management practices involving worker bullying and harassment and unrealistic work schedules and targets are ubiquitous in the factories of developing countries, including Bangladesh (Ashrah, 2017; Author withheld, 2023; Pillinger, 2016; Siddiqi, 2003; Seneviratne, 2019).
In analysing MRPSH in the Bangladesh workplace context, for reasons we discuss in the next section, we depart from the conventional conceptual approach to psychosocial hazards which has drawn on models of work-stress, such as Demerouti et al.'s job demands–resources (JD-R) model (2001), but neglect the socio-economic context of work and its influence on management practice. Instead, in response to scholars’ calls across various fields for a renewed focus on theory that has regard for the economic and social context of organisations and work, we use LPT as the conceptual framework for analysing the relationship between psychosocial hazards, management control strategies and the external environment of organisations (Hoel and Beale, 2006; Robinson and Rainbird, 2013; Wright, 2011).
Conceptual framework
Traditionally focused largely on structural and technical sources of OHS risk, the OHS field only expanded its scope to incorporate psychosocial hazards in the late 20th century. Recognition of psychosocial hazards emerged from a growing scholarly and public dialogue in developed countries on work stress, bullying, harassment and other mistreatments at work (Dollard et al., 2007; Johnstone et al., 2011; Niedhammer et al., 2008; Nielsen et al., 2009). Since then, conceptual discussion of psychosocial hazards has occurred largely in the public policy and organisational psychology disciplines, where different focuses emerged. In public policy, scholarly work centred on the need for organisations to identify and address hazards, facilitated by newly-developed risk inventories and audit mechanisms (Chirico et al., 2019; Kortum, 2011; Kortum et al., 2010, 2011; Kortum and Leka, 2014). In contrast, organisational psychologists focused on the causes of psychosocial hazards in organisations, their negative implications for well-being in terms of stress and burnout, and how employing organisations can eliminate such harms (Cox et al., 2000; Dollard et al., 2007; Nieuwenhuijsen et al., 2010; Salanova et al., 2014; van der Molen et al., 2020).
JD-R model
Arguably the most prominent conceptual framework used to analyse workplace psychosocial hazards has been Demerouti et al.'s (2001) JD-R model, as revised by Schaufeli and Bakker (2004). Due to consistent quantitative empirical evidence confirming the model's dual process of the interactions between job resources and job demands, this model has gained enormous scholarly popularity within organisational psychology (Ong and Johnson, 2023; Schaufeli and Taris, 2014). Perhaps because of its widespread acceptance in this field, scholars researching psychosocial hazards have tended also to utilise the model (e.g. see Dermovski and Mathison, 2023; Dollard and Bakker, 2010; Idris et al., 2012). In the JD-R model, job demands are those aspects of work that require sustained physical and psychological effort, and job resources are aspects that facilitate the achievement of work goals, reduce job demands and stimulate personal growth and development. The later revised model by Schaufeli and Bakker (2004) proposed two separate psychological process pathways through which stressors can interact negatively or positively and contribute, respectively, to the development of job strain or motivation (Bakker and Demerouti, 2007; Dollard and McTernan, 2011). For JD-R scholars, the presence and interaction of job demands and job resources may variously lead to motivational and/or health impairment outcomes, which impact on worker well-being and performance (Bakker and Demerouti, 2007; Schaufeli and Bakker, 2004).
Scholars researching the related concept of the psychosocial safety climate (PSC) have since used the JD-R model to show how an organisation's PSC relates to the psychosocial health of workers. PSC refers to shared perception regarding ‘policies, practices and procedures for the protection of worker psychological health and safety’ (Dollard and Bakker, 2010: 579). Therefore, PSC reflects the extent of management's commitment to safeguard the psychosocial health of workers in relation to job demands and productivity concerns (Cox and Cheyne, 2000). Some have argued that a low PSC is a precursor to poor job design, and by association high job demands, which in turn predicts stress outcomes leading to the ‘extended health erosion hypothesis of the JD-R theory’ (Dollard and McTernan, 2011; see also Dollard et al., 2019; Erwandi et al., 2021; McLinton et al., 2018). Studies also show the importance of a high PSC level in lowering the negative effects of job demands on psychosocial health through, for instance, reducing emotional job demands and workload pressure (Dollard and Bakker, 2010; Law et al., 2011).
As a tool for understanding the forms and occurrence of psychosocial hazards, however, we maintain that the JD-R model largely confines the explanation of the generation of job demands and job resources to internal organisational factors and individual worker characteristics, while neglecting external environmental influences. In this regard, while using the JD-R model, Dollard et al. (2019: 3) have argued that ‘work factors must be considered in their context’, including the socio-economic context of capitalism. This suggestion holds the promise of empirical work to come. However, JD-R adherents, generally still attribute psychosocial hazards to the interaction of job demands and resources in the immediate work environment and individual employees’ resources. The model accordingly suggests that once employers become aware of OHS hazards, they would implement appropriate HRM practices to improve workers’ well-being. This conceptualisation fails to take into account of external environmental influences over which employers may have little control. Within global supply chains, for instance, lead firm strategies in relation to the pricing and sourcing of goods by suppliers in developing countries, may exert considerable influence on management practices in relation to job demands and resources. Nor does the JD-R model consider psychosocial hazards a source of collective harm where either workers or managers may intend to harm and/or deliberately harm others for the purpose of responding to such external pressures. For these reasons, we have adopted from industrial sociology an alternative conceptual lens of LPT which brings an analysis of the broader socio-economic context to explanations of the nature of work within Bangladesh garment factories.
Labour process theory
LPT had its origins in classical sociology, and, particularly, in the scholarship of Marx and Weber (Thompson and Smith, 2009). A fundamental focus of LPT research has been to establish more precisely how employers extract surplus value from workers, given that labour is an indeterminate element of the capitalist production process embodied in the labour power of workers (Chai and Scully, 2019). From 1974, following the publication of Braverman's Labor and Monopoly Capital, many scholars studied the role of management control strategies in facilitating the extraction of surplus value from workers. Largely conducted in the Global North, much research centred on identifying the forms of management control strategies, with some scholars proposing typologies that included strategies that ranged from simple, direct and despotic to more sophisticated, embedded and hegemonic forms of authority (Braverman, 1974; Wright, 2011). They suggested that types of control strategies varied depending on the ‘logics of accumulation’ (Gandini, 2019: 1049) that shape capital-labour relations (Burawoy, 1983, 1985; Nielsen, 1980). Experts argued that management control strategies were implemented to stabilise work outcomes and to make the pace and outputs of production predictable and efficient. The typologies that LPT scholars developed to explain forms of control in work organisations in the Global North now appear to explain the prevalence of simple, direct and despotic management control strategies in many industries in developing countries, particularly at the lower end of supply chains (Anner, 2015). However, there remains little use of LPT in research on the nature of work and psychosocial hazards in developing countries such as Bangladesh.
Labour process research has continued unabated since the 1970s largely within industrial and organisational sociology. The theory has also informed the fields of industrial and employment relations for several reasons. First, LPT provides a critical perspective on workplace relations (Chillas and Baluch, 2019), in part because it provokes ‘empirical interest in the experience of work at the point of production and a theoretical concern with the contradictory relationships between capital and labour’ (Edwards, 2010: 42). In addition, LPT is utilised in employment relations because ‘its analysis of workplace issues within broader social and economic frameworks, [provides] a holistic model of the factors shaping, and being shaped by, ER’ (Harley, 2018: 81).
In recent years, some scholars in fields such as organisational psychology have argued for the use of a Marxist explanatory lens to gain a deeper understanding of phenomenon such as workplace bullying. For example, Hoel and Beale (2006: 249) proposed an interdisciplinary approach to conceptualising workplace bullying, having identified it as ‘part of a continuum of management behaviour aimed at establishing and maintaining management control’, a key LPT focus. In management research on global supply chains, some scholars have argued for research that uncovers the connections between the workplace and its political economy context (Coe and Yeung, 2019; Newsome et al., 2015; Wright, 2011). For instance, in examining global production networks, Coe and Yeung (2019) observed the value of considering labour process dynamics and interactions to analyse how work is experienced and the value obtained in global production pathways.
This article responds to such calls, in our analysis of MRPSH in Bangladesh RMG factories, by considering socio-economic influences on the formation of management control strategies. We argue that LPT facilitates an understanding of the dynamics of management control which underpin the menstruation-related psychosocial risks that women workers encounter in the developing economy context.
Methods and data analysis
As noted earlier, this study is part of a larger project concerning women's experiences and perceptions of psychosocial risks and harms in Bangladesh RMG factories (Author withheld, 2023). MHM was not a specific focus of the broader study. However, through participants’ responses, MRPSH emerged as an important issue for women workers and this article is based on the findings yielded from their comments. Given that the research sought to understand psychosocial phenomena through participants’ experiences and perspectives in their everyday work context, in designing the research, we adopted a qualitative case study method (Merriam and Tisdell, 2016; Yin, 2018). In this, we followed Pratt's (2009: 856) comment on ‘the value of qualitative research for understanding the world from the perspective of those studied’ in management research. As this study aims to contribute to the conceptual understanding of phenomena, in this case, menstruation-related psychosocial risks and harms, as opposed to testing an existing theoretical framework, we also employed an ‘inductive approach’ (Thomas, 2006) to data analysis. This bottom-up, inductive approach allowed us, as researchers, to immerse ourselves in contextual factors while exploring why menstruation is a psychosocial risk phenomenon and how associated hazards form and affect women workers’ health and well-being at work. As Bansal et al. (2018: 1194) observed in the Academy of Management Journal, ‘adopting qualitative inductive methods allows scholars to surface new insights and enable new ways of seeing’.
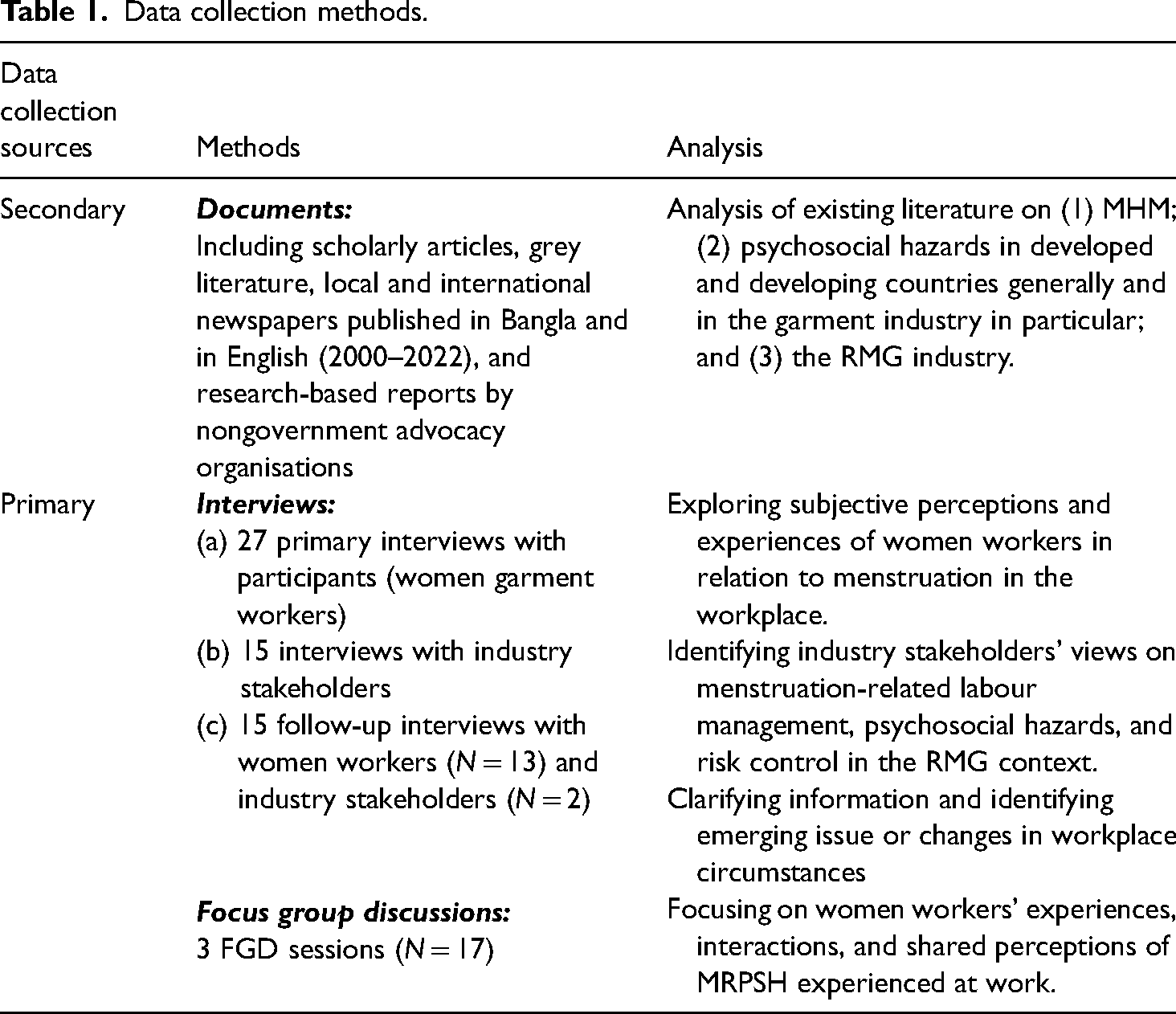
The project utilised the three principal data sources outlined in Table 1: secondary sources, semi-structured interviews, and focus groups (FGD). We used secondary sources to develop an overall understanding of the RMG industry in Bangladesh, including the socio-economic context in which firms operate, the nature of work in the sector, and possible psychosocial risks, hazards and harms. On a practical level, secondary data was also used to inform the development of interview and focus group protocols. Moreover, along with interviews and focus groups, the documentary sources provided a methodological triangulation useful for minimising potential bias and enhancing data credibility, as well as data richness (Bowen, 2009; Yin, 2003) in uncovering potential subtle or hidden psychosocial phenomena (Table 2).
Data collection methods.
Interviewee profile (women workers).
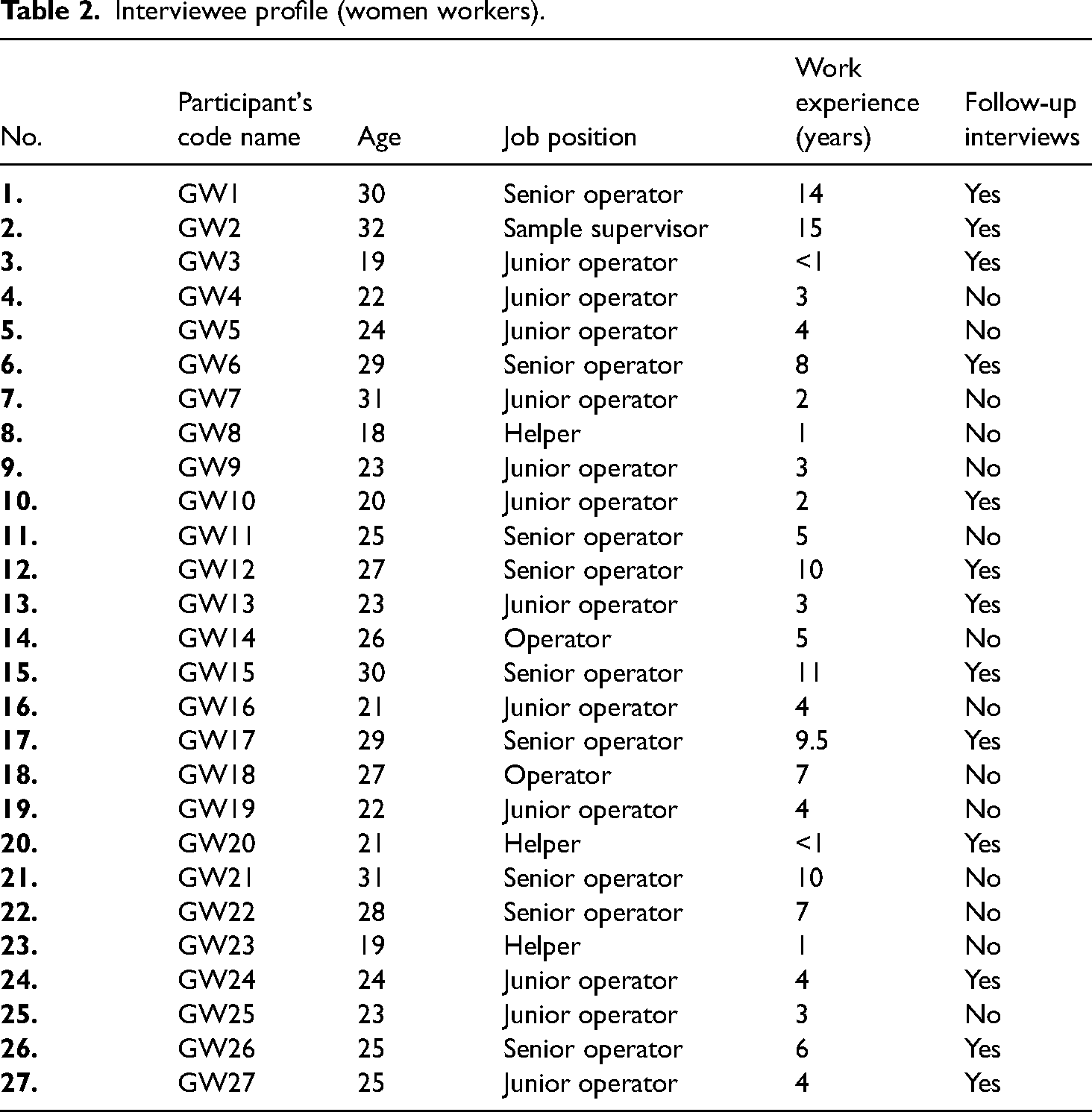
We conducted three stages of data collection. The first phase, which commenced in 2020 after obtaining Macquarie university ethics, involved conducting open-ended semi-structured interviews with two groups of participants: female garment workers (N = 27) and other industry stakeholders (N = 15). Interviews with industry stakeholders included trade union and employer association representatives, owners, apparel business consultants, senior managers and line managers working in RMG factories. Interviews with women workers not only gleaned their experiences and perceptions but also helped to inform the FGD questions and facilitated modifications to the interview protocol for industry stakeholders’ interviews. All interviews with women garment workers and industry stakeholders were conducted in the language of Bangla and lasted 60–120 min.
Interview participants were selected using a nonprobability and non-random sampling strategy. That is, initially, we used professional networks to connect with women workers and other industry stakeholders. The first author's professional collaboration with the Bangladesh industrial relations community helped to identify potential interview subjects to approach. Following the identification of initial participants, we relied on the snowballing method (Noy, 2008) to identify participants through referrals from existing contacts. In this respect, participants’ referrals were made on a voluntary basis and the research team provided the recruitment script containing the consent requirements, translated into Bangla, to the target contacts. The main criterion for including women workers as participants was their employment in a garment factory.
The participants were all located in Chattogram, the industrial capital of Bangladesh. Notably, all the women worker participants were approached individually, without any contact with employing organisations, to ensure their anonymity and confidentiality. The location of each interview was different. While some women workers (N = 5) chose to conduct the interview in a café, most selected their home. The locations for industry stakeholder interviews also took place according to their choice, generally in their workplaces or homes. Notably, most industry stakeholder participants either avoided responding to questions related to menstruation at work or denied it raised any issues.
In the second phase of data collection, we conducted three FGDs with additional women worker participants. The focus groups were used to obtain and clarify women workers’ shared perspectives on menstruation hazards in the workplace and to broaden and deepen the data both through exploring multiple and collective viewpoints and through observing degrees of consensus on matters discussed (DeMarrais and Lapan, 2004; Hesse-Biber and Leavy, 2011). The total sample size was 17, with six participants in two FGDs and five in the third. Considering the potential consequences of peer information disclosure, FGD sessions were designed with the purposive sampling criterion that participants must not work for the same or a shared organisation. Each session was conducted on a separate day and was around 120 min in duration.
The third data collection phase involved follow-up semi-structured interviews with 13 women workers and 2 industry stakeholder participants. These interviews lasted between 30 and 45 min. The follow-up interviews were conducted to clarify comments made and information revealed in the preliminary interviews and to ascertain emergent perceptions and changes in workplace circumstances. The identity of interview participants has been anonymised through the use of code names. In this article, women workers who participated in interviews and FGDs are coded as ‘GW’, and industry stakeholders as ‘IS’.
Before conducting data analysis, we translated and transcribed all recorded and documented interviews and FGDs into English. No third party was used to translate and transcribe the interview data because this would have risked losing both the linguistic context and the essence of the data so essential to an interpretive phenomenological research approach. We undertook a ‘thematic analysis’ (Braun et al., 2019; Braun and Clarke, 2021) approach to data analysis. Applying thematic analysis, we sought to identify patterns of data that were meaningful in answering the research questions. We used NVivo 12 to enable the flexible coding and recoding of data in an iterative manner and also to explore the interrelation between the codes and child nodes. Coding labels were evolved and redefined based on our development of new insights from the data. As well, this ‘organic coding process’ (Braun and Clarke, 2021: 9), a core aspect of thematic analysis, fuelled the emergence of major themes by identifying underlying relationships between nodes. It also facilitated developing interpretations of coding interactions that ‘underlie the data surface’ (Braun and Clarke, 2021: 5). Multiple themes emerged from this analysis including the presence of common MRPSH linked to both physical and psychological harms, and relationships between these hazards and management control strategies.
Empirical findings
In this section, we identify and discuss the types and prevalence of the MRPSH and the resulting harms that women workers experience in Bangladesh RMG factories. The research findings indicate that women experience psychosocial risks, hazards and harms from three forms of management practice which we discuss below. These include: first, the impeding of access to restroom facilities; second, demeaning and intimidating verbal harassment; and third, a lack of timely access to menstrual products at work.
Access to toilets: restrictions and fears
Restrictive supervisory decisions concerning the taking of toilet breaks emerged as a concern for most women, but a heightened concern during menstruation. While officially permitted to use restrooms during work hours, each worker must gain permission from their respective supervisor to leave their workstation for this purpose outside tea and lunch breaks. Women workers observed that they often require access to restrooms more frequently during menstruation to address menstrual hygiene. In this regard, it is important to note that women in garment factories usually work six days a week. Shifts are commonly ten hours a day or more, but often up to thirteen hours, and lengthy unscheduled overtime is common, particularly when supply deadlines are imminent. In the production areas, almost every women worker is of reproductive age.
Women respondents reported a reluctance to request toilet breaks for several reasons related to management responses. First, supervisors often rejected their requests in what they experienced as an arbitrary and unpredictable manner. Second, when women were questioned about requests to use restrooms and cited menstruation-related issues as the reason, supervisors commonly responded with humiliating, abusive language. Thus, participants said that typically they refrained from taking required toilet breaks during menstruation, despite the potential consequences, such as the humiliation of blood leakage on their clothes and physical health harms. As one worker explained: I knew I just got my period, and I wasn’t prepared for it; I told my supervisor I need a break from work, as I had no rags with me to save my clothes. He kept denying it. (GW10) Even though I can take a toilet break during work hours, I need my supervisor's permission. When I use the washroom break during menstruation, it might take five minutes. The supervisor will start asking about my lateness and yelling at me. So, I avoid toilet breaks at any cost. But yes, on days of heavy flow, I really get tensed about leaking and blood staining my clothes. (GW16)
Furthermore, women workers observed that asking male supervisors for toilet breaks during menstruation creates feelings of shame. This stems from the culturally ingrained menstrual taboos in Bangladesh society including the stigma associated with speaking openly about menstruation with men (see: McCammon et al., 2020). Women in other developing countries have reported similar societal expectations of silence and secrecy around menstruation and an intense fear of shame and distress when their menstruation is exposed publicly (Hennegan et al., 2019). As one participant commented: I can’t say to my male supervisor that I have got my period and I need more time on the toilet. How can I share this? It's a matter of my “izzat” (self-dignity). (GW31) … Often, we get so tensed and scared that we don’t take a proper lunch break just to make up missed hourly targets and save ourselves from the verbal torture. There are many women who bring their lunch back home without even opening it. Due to extreme production pressure, we often work while crying. (GW5)
Unscheduled requirements to work long overtime hours also caused significant concern, particularly when workers feel unwell. Twenty-nine out of forty-four interview and FGD participants reported being forced to continue working after their shift despite reporting symptoms of ill health to managers. When a worker reports being unwell, managers generally compel her to stay onsite until and unless her condition deteriorates to a critical point. As one recounted, One night I got headache since 1am and the headache was so severe that I didn’t even feel like keeping my eyes open. Then I kept insisting to my in-charge, please give me leave, I really can't work and I'm not feeling well at all. Shipment was due the next day, so my leave was not granted. (GW14)
Management bullying and harassment
A second major source of MRPSH for women is the intimidating verbal abuse managers inflict on them for taking toilet breaks. Workers discussed being tormented with bullying and sexualised language by supervisors and other managers, particularly during menstruation, for either visiting the toilet several times, or taking a slightly longer time. Participants described how the sexualised comments of male superiors distressed and scared them. If I go to toilet more than twice, the supervisor will start yelling and asking “What the hell are you doing in the toilet? I will give you chilli water to wash your private parts in the toilet.” This is such a matter of shame. That's why I try not to go to toilet several times. (GW18) My clothes were full of bloodstains by the time of lunchbreak. He (the supervisor) saw it and yelled at me: “you’ve contaminated my factory, bloody whore”. It was so embarrassing to me as everyone looked at me, he was so loud. (GW10) My co-worker was having heavy flow and she went to the medical room yesterday to get a sanitary napkin. She asked (medical officer/ nurse): “Madam, please give me a pad.” In reply, she said, “no pad will be provided. It's not a charity shop”. It's just a pad and she cried a lot once she went back to her station. I couldn’t do anything for her. (GW1)
Lack of access to menstruation products
Another key challenge for women workers is a lack of access to menstrual hygiene products. In some cases, this reflects women's menstrual poverty, but nonetheless, it makes them susceptible to supervisory harassment. As one reported: No, I can’t afford a sanitary napkin. Instead, I wear a thick cloth bandage, and I keep wearing the same rag till lunch break. I have no time to change before my lunch break. (GW26)
The inaccessibility of menstrual products in emergencies, such as when menstruation begins unexpectedly, also puts women workers at risk of harassment. The policy that workers are not allowed to leave their workstation during working hours without their supervisor's permission continues to apply when a worker has an urgent need for MHM resources. However, even when a supervisor permits workers to seek help from the in-house medical team, which exists in every medium to large factory, their problem may remain unresolved. Many women reported that medical units often lack MHM supplies. They also reported receiving humiliating responses from healthcare assistants when requesting these accessories.
The empirical research discussed in this section highlights that garment factory managers mistreat women workers during their menstruation in a variety of ways. Women participants in our study emphasised that, as almost all the women employed in these factories are of reproductive age, the effect is that most women workers encounter harassment and bullying, which demeans, scares, and mortifies them, because of the natural but stigmatised bodily function of menstruation. Through limiting the opportunities for women workers to engage in appropriate MHM, these management practices cause a range of physical and psychological harms.
Adverse physical and psychological health implications
The findings indicate that poor menstrual hygiene is a major psychosocial risk for women workers in Bangladesh garment factories. Women workers reported a range of sexual and reproductive health disorders which emanate from management practices. For example, ten (10) participants reported experiencing chronic vaginal yeast infections, itching, rashes, and/or urinary tract infections because of inadequate MHM at work. These findings are consistent with other research showing links between reproductive tract infections and the inadequate frequency of changing menstrual products (Hennegan et al., 2019; Sommer et al., 2016).
The menstruation-related management practices that women report also cause psychological distress, including fear, anxiety, embarrassment and humiliation. In some cases, the abuse and shaming by male supervisors and the fear of blood leakage and bloodstaining lead to recurrent, long-term psychological trauma. In this regard, some respondents discussed how disturbing experiences of early (unexpected) menstruation at work can become. Anticipating the management hostility to their requests for breaks to manage the issue, they tend to avoid the matter and continue to work despite inevitable blood leakage. Such experiences leave women workers feeling degraded, vulnerable and humiliated. Participants also reported that this management mistreatment adversely affects the mental health not only of the women directly affected but also of workplace onlookers. Our study suggests that these shame- and shock-inducing incidents are associated in some cases, with significant (undiagnosed) trauma akin to ‘post-traumatic stress disorder’ (Mayo Clinic, 2024). In analysing the psychological harms, associated with this management treatment, as well as the physical and psychological harms discussed above, it is important to consider the frequency and intensity of menstruation-driven stressful events. In garment factories, this natural and (generally) monthly condition of being a woman of reproductive age carries the potential for long-term health impairment due to ‘accumulative, recurrent and negative affective reactions’ (Sojo et al., 2016: 16). As well, the management mistreatment occurs in a socio-cultural context within which the breaking of taboos by women jeopardises their ‘izzat’ or honour which, in Bangladesh, may be their most valuable asset (Siddiqi, 2003). Indeed, Siddiqi (2003) has argued that, for Bangladesh garment workers, any harassment strikes at the heart of their honour, and by association, their dignity and self-worth. Thus, workplace MRPSH have the potential to cause significant, long-term physical, psychological and social harms.
Discussion
In the foregoing sections, we have explored how, in Bangladesh RMG factories, women workers are subject to psychosocial hazards based directly on their experience of menstruation. These MRPSH constitute a discrete set of gender-based dangers associated with the natural state of women. Our research has also shown that they cause a range of serious physical and psychological harms. Within developing societies, the implications of these management practices at work may also go well beyond the workplace. The practices we identified exploit existing socio-cultural taboos and stigma concerning menstruation, inflicting embarrassment, and shame on women workers. These experiences may reinforce broader socio-cultural experiences of stigma in relation to menstruation, perhaps compounding the psychological distress and barriers women face in maintaining effective MHM.
The development of realistic responses to reduce or eliminate these psychosocial hazards requires an understanding of why management engages in the practices. In this section, we argue that the LPT conceptualisation of management control mechanisms provides a valuable direction for analysing management utilisation of these practices in workplaces such as the Bangladesh garment factories at the bottom of global supply chains.
Significantly, our findings differ in a crucial respect from much recent scholarship on women workers and menstrual hygiene in developing countries. To date, public policy and public health experts have predominantly identified the frequent inadequacy of hygiene facilities, including the lack of safe, clean and private toilets with water facilities, and the difficulties women face in acquiring menstruation resources at work, as the core challenges for women workers in the least developed countries (Sommer et al., 2016). Scholars have also established an association between a lack of hygiene facilities and gender-based violence in urban and rural areas, arguing that even though access to hygiene facilities is not the root cause of gender-based violence, insufficient provision and location of facilities exacerbate women's vulnerability to violence (House et al., 2014).
However, our findings indicate that, in Bangladesh RMG organisations, the problem may not always be the lack of facilities as such. Rather, the problem can lie in the way management control is exercised in relation to women's MHM such that, in practical terms, women's timely access to facilities and menstrual products is curtailed and/or is accompanied by fear, humiliation, and a heightened apprehension of physical and psychological ill health.
The LPT conceptualisation of how managers develop control strategies to facilitate the extraction of surplus labour value (Burawoy, 1985; Quinlan et al., 2020; Wright, 2011) provides a valuable direction for analysing the association between management strategy and the MRPSH and harms that women workers experience in Bangladesh RMG factories. At the base of global supply chains, these factories are generally subject to heavy price and deadline-sourcing pressures from lead firms which flow down the managerial hierarchy to the lowest-level supervisors. As a woman worker said: Supervisor abuses workers, in-charge abuses supervisors and PM abuses the in-charge. It's a common practice … in every garment factory …At the end of the day when PM notices the gap of production output and expected production target, he becomes furious, often breaks the whiteboard and start yelling at us, ‘What are you doing? Are you all pregnant?’ (GW 27; Note: PM refers to Production Manager)
Drawing on the LPT lens, we argue that the management treatment has clear aims. One aim is to ensure that women workers do not leave their workstation, thus preventing machine downtime (see also: Seneviratne, 2019; Siddiqi, 2003; Quinlan et al., 2020). In addition, the menstruation-based bullying and harassment is part of a broader management strategy of mistreatment in garment factories, intended to demean, humiliate and scare women to ensure they remain a largely docile and compliant workforce. This interpretation is consistent with earlier research by Siddiqi (2003) and Seneviratne (2019) on workplace harassment in developing countries.
Thus, we argue that the labour process has a direct influence on the formation of menstruation-oriented mistreatment in the workplace. In this case, the gendered and capitalist power dynamics of the labour process consequently give rise to a low or poor PSC, high and recurrent workplace mistreatment, and coercive management control strategies leading to high job demands and also low job resources. This also reflects how management set the tone of a bullying and punitive work climate within organisations and undermine the value of psychosocial health and safety of women workers. Following Dollard and Colleagues’ viewpoint that PSC leads to a specific bullying mistreatment climate (Dollard et al., 2017: 845) we argue that the low PSC gives rise to the high and recurrent MRPHS which has a substantial adverse impact on workers’ psychosocial health outcomes. Using LPT, therefore, we argue that our findings highlight a distinctive management strategy by which employers seek to stabilise and maximise labour productivity through weaponising menstruation as a form of coercion-based control that specifically exploits feminised segments of the workforce. These menstruation-based management practices are part of the management control strategy in RMG factories designed to secure capital accumulation through harnessing menstrual stigma and gender-based power inequalities in organisations.
Given the regularity of menstruation in feminised workplaces, management's attack on menstruating women's ‘izzat’ or dignity through these control strategies is deeply embedded in the labour process. Arguably, when combined with the limited unionisation of female workers in the garment industry, the menstruation-related mistreatment, further enables the male-dominated management hierarchy to maintain worker compliance and to minimise possibilities for worker resistance and industrial disruption.
While the intention of these management practices is to prevent machine downtime and build a fearful and compliant workforce at the factory floor, however, there is no evidence that they actually result in the intended production benefits. The practices appear to be uninformed, blunt control instruments based essentially on gendered views among male managers about effective ways to control women workers. Given the negative impact of this strategy on women's physical and psychological health, arguably, it may backfire in terms of organisational performance, as research on the impact of workplace bullying has found (Mehmood et al., 2024).
However, the development of these management strategies is not driven entirely from within individual RMG factories. Drawing on LPT conception of the relationship between capitalism and the nature of work, it is vital to consider the influence of environmental factors, including the economic context in explaining the internal management practices of organisations. In the case of Bangladesh RMG factories, their location at the lower end of global supply chains, plays an important role. The highly competitive nature of the fast fashion industry leads to global buyers and leads firms imposing continued pressures on supplier factories through reducing prices and deadlines. In this economic context, senior managers in factories impose pressure downstream on supervisors to manage labour in ways that minimise reductions in profit margins (Anner, 2018; Kabeer, 2019). Yet, this often leads to hazardous work conditions being adopted (Alamgir and Alakavuklar, 2020; Anner, 2020; Bair et al., 2017; Kabeer, 2019; Schüßler et al., 2019). While many lead firms have imposed supply chain labour codes and standards, until they tackle the relationship between their pricing and sourcing demands and the management strategies adopted downstream, it is unlikely much progress will be made in eliminating menstruation-based management practices we have discussed here.
In sum, the empirical findings suggest that the weaponisation of menstrual health as a pervasive management strategy in Bangladesh RMG organisations poses significant threats to women workers’ psychosocial safety, health and dignity. The management harassment and bullying around menstruation reinforces cultural experiences of menstrual-related stigma, creates psychological distress for women, impedes effective MHM for women workers, and provides the conditions for substantial physical and psychological harms. Using LPT, our analysis has highlighted that menstruation-related management practices are used strategically to coerce and control women workers in ways that managers believe facilitate the achievement of production targets. This analysis presents an alternative to the arguments of other contemporary scholarly and policy experts that shortfalls in workplace MHM in developing countries are linked largely to the inadequate provision of hygiene facilities due to poverty, delayed national development and societal ignorance (USAID, 2019). Thus, we argue, eliminating MRPSH and harms cannot occur until management jettison these hazardous practices.
Policy proposals
In the final section of this article, we consider the current lack of policy and regulatory attention in Bangladesh to psychosocial hazards in general and MRPSH in particular. We then propose some policy approaches for reducing the prevalence of MRPSH in developing countries, focusing on the need for multi-level, multi-stakeholder involvement in tackling these embedded practices.
As noted earlier, in recent decades, policy attention to the improvement of MHM has grown, largely in developed countries, variously resulting in measures to improve the safety of menstrual health products, reduce (often) associated taxes on these products, and provide industrial entitlements such as menstrual leave (e.g. see Levitt and Barnack-Tavlaris, 2020). While research in developing countries, particularly on access to sanitation facilities has also grown, much of the policy activism conducted by NGOs has been directed at improving general societal knowledge and infrastructure (Sommer et al., 2016; USAID, 2019) rather than workplace-based interventions.
The situation in Bangladesh remains typical. Neither transnational stakeholders nor domestic legislators and regulators have considered psychosocial hazards, including menstruation-based mistreatment, and there remains an absence of political commitment at the local government level, and a lack of senior management commitment to, or even knowledge of, MHM issues. Notably, during stakeholder interviews, the male CEO of a group of garment companies, dismissed the subject, stating: it's not our business to look after their reproductive health. And it's completely a private matter of women, not related to our business (SI6).
A LPT analysis underscores the importance of policy interventions that address the reasons why management adopts particular control strategies. Given the economic and social context of garment factories such as those in Bangladesh, developing realistic strategies for eliminating psychosocial hazards will require a multi-level, multi-stakeholder approach. This is particularly the case in relation to MRPSH as broader socio-cultural patriarchal attitudes largely view menstruation as a subject of ‘shame, disgust, and abjection’ (Goldblatt and Steele, 2019: 298).
Further, the lack of significant women workers’ voice and agency inhibits the prospects for bottom-up influence on these management strategies. The voice and agency of women garment workers are low for several reasons including the narrow focus of Bangladesh law on labour rights (Al Mamun et al., 2018; Barnes and Kozar, 2008; Naved et al., 2018; Prentice, 2021); their low union density and the limited structures for workplace union representation; women's commonly low status in the production process; insecurity of employment in this sector due to easy labour replaceability; and patriarchal social attitudes (Goldblatt and Steele, 2019; Kabeer and Mahmud, 2004; Hossain and Akter, 2022).
Legislative reform is one method for building organisational responsibility to eradicate management mistreatment of menstruating women. A critical step for policymakers could be to impose a statutory legal responsibility on employers such as a duty of care to provide a safe working environment. This concept is utilised in common law countries such as Australia, New Zealand and North America, but rarely found in Asian countries. In relation to MHM, such a duty of care could be accompanied by codes or standards built into organisational OHS systems for monitoring employer provision of specific worker entitlements such as rights to unrestricted restroom breaks and guaranteed access to menstrual products at work. In this regard, we acknowledge Patkar's (2020: 502) recommendation that menstrual hygiene and health policies emphasising practical needs may provide ‘a stronger hook’ than more general calls for women's empowerment. Thus, for instance, shifting the allocation of menstrual products from the medical room to a designated dispensing machine in women workers’ toilets or restrooms may reduce distressing experiences and increase privacy. Specific provisions for dealing with menstruation-related harassment such as grievance processes could also assist in reducing management mistreatment.
We note, however, that recent scholarly work has urged caution concerning the growing resort to law to respond to menstrual injustice. Steele and Goldblatt (2020) have argued, for instance, that while provisions that legally recognise discrimination against women based on menstrual stigma in some countries may reduce the prevalence of some harmful practices and provide some remedies, the interventions may fail to eliminate injustices where they stem from transplanted ideas that fail to resonate in the local context where stigmas and taboos are particularly entrenched.
Arguably, therefore, a multi-pronged approach is needed, one which also includes a social dialogue among the various stakeholders in industries in which menstruation-related management strategies are prevalent to prevent psychosocial risks and to facilitate MHM at work. An important piece of this puzzle is to educate managers about the adverse impacts for such practices both for workers and productivity. Given the stigma attached to menstruation in Bangladesh society, and limitations in MHM literacy and knowledge, a broad dialogue is required not just to raise understanding but also legitimise the need for legislative reform and industry self-regulation.
The informed changing of management strategies in Bangladesh garment factories must be a crucial focus of reform efforts. However, the nature of management control, to a greater or lesser extent, is essentially constituted outside the workplace, at higher levels in the supply chain (Robinson and Rainbird, 2013). Thus, it is also essential that the lead firms in supply chains adopt a commitment to reducing MRPSH at the supply chain floor. In recent years, as part of their commitments to social values, global brands and retailers have addressed issues related to labour management in host countries, including wage levels, labour resistance, and the codification of supply chain norms and values (Cumbers et al., 2008; Feuerstein, 2013). According to Porter and Kramer (2006: 13), a responsive CSR approach can have a greater impact on ‘social good than any other institution or philanthropic organisation’. However, to date, lead firms in global supply chains have not recognised MHM as an OHS issue that is critical to establishing a safe garment industry workplace.
Global buyers could play a key role by demonstrating their own genuine commitment to such CSR initiatives as bearing the cost of menstrual products within suppliers’ organisations. By providing free menstrual products to women workers, lead firms could contribute to reducing menstrual poverty and improving MHM among women workers, while simultaneously strengthening their CSR portfolios and brand value. Such voluntary initiatives could also pave the way for lead firm intervention in menstruation-related management strategies causing psychosocial harm to women workers. Global brands and retailers are under intense competition to showcase CSR activities that are meaningful to target consumers. From this perspective, global buyers’ direct involvement in improving women workers’ health and well-being could add shared value to their core stakeholders.
Conclusions
This article has contributed to knowledge on workplace psychosocial hazards and harms, particularly in relation to menstruation-related hazards, through a case study of women workers in Bangladesh RMG factories. Using LPT, we have explained the prevalence of the identified hazards as management practices that form part of a systematic management strategy to reduce machine downtime and maintain a docile, compliant female workforce to facilitate employers in meeting the sourcing and price demands that lead firms impose through supply chains.
However, the findings also point to the need for future research on several topics to do with MRPSH. For instance, research on the long-term implications of the management practices we identified would be useful. In this regard, supporting Bond et al.'s (2010) call for research on the long-term consequences of traumatic events, such as bullying, we suggest that research on the enduring implications of menstrual harassment and shaming and of prolonged exposure to these practices, for longer-term trauma and post-traumatic stress syndrome would be valuable. This could, in turn, better facilitate public health advocacy on these psychosocial hazards. As well, empirical evidence on the effect of psychosocial hazards on worker performance and organisational productivity would be useful to inform realistic regulatory and policy changes. Currently, without evidence to the contrary, managers appear simply to assume these techniques contribute positively to production goals.
In explaining these management practices through the LPT lens, we are not rejecting the arguments of public health, global development, organisational psychologists and feminist scholars and policy experts that the sources of MHM challenges lie in broader societal, economic and cultural characteristics. Rather, we maintain that, in the workplace, MRPSH are also the product of systematic management strategies which harness socio-cultural taboos concerning menstruation to achieve managers’ production objectives. Improving psychosocial safety and MHM for women workers where such management practices prevail requires regulatory and policy interventions that recognise and respond to the relationships between stakeholders and the economic forces of production which underpin specific management strategies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.