
Abstract
Contact centre workers experience disproportionately low physical activity levels and high sedentary behaviour levels, as well as an increased risk of negative occupational health outcomes such as anxiety and depression. Organisational culture factors such as strict work schedules and pressure to maintain productivity often impede the effectiveness of programmes to reduce these health risks. Despite its significance, organisational culture is often overlooked during the development and implementation of workplace health programmes due to its conceptually complex nature. The COVID-19 pandemic further complicated organisational culture-related associations to workplace health programmes in contact centres. This study investigated how organisational culture influences the existence and effectiveness of workplace health programmes in contact centres and if/how COVID-19 disrupted these associations. Fifteen interviews were conducted with contact centre managers and workplace health experts between February and June 2021. Findings indicate that employee well-being is increasingly being prioritised within contact centres, especially post-pandemic, and that there is a legacy of COVID-19 to learn from the spotlight that was placed on employee well-being during the pandemic to improve workplace conditions for contact centre employees. Further, to maximise effectiveness and support positive organisational culture change, these findings should be considered during well-being programme planning, delivery, implementation and evaluation.
Keywords
The workplace is a key setting for implementing health interventions, which can benefit both employee and employer outcomes (Ryan et al., 2021). In 2022, full-time UK workers worked an average of 36.4 h per week, averaging 7.3 h per day (Office for National Statistics, 2023). As working hours take up such a large portion of the day, work time forms crucial periods of the day that can positively or negatively impact one's health and well-being.
The work context changed significantly during the COVID-19 pandemic, which shifted business operations and organisational priorities for most employers. Many workers experienced an increased digitalisation of work and office organisation to allow for remote working and adhere to pandemic restrictions through the implementation of new health and safety policies as per government directives (Amankwah-Amoah et al., 2021). As the place of work (including commuting) has such a significant influence on day-to-day life and health, these shifts in working practices played a crucial role in how people's lives were impacted by the pandemic and their sense of well-being during that time, including increased stress, anxiety and depression (Giorgi et al., 2020).
There is evidence of how these new ways of working can negatively impact on the mental and physical health of desk-based workers in particular (Oakman et al., 2020). For example, working from home during the pandemic was associated with increased levels of sedentary behaviour, and decreased levels of physical activity (Ráthonyi et al., 2021; Thivel et al., 2018) and self-reported health across a number of mental and physical health measures (Oakman et al., 2020). Depending on the demands of the home environment, culture of organisational support and social connections outside of work, homeworking could have either a positive or negative impact on mental health (Oakman et al., 2020) and physical health (Nijp et al., 2016). Factors related to increased digitalisation during the pandemic could also have a negative impact on employee well-being, for example where digital working leads to a culture of greater surveillance, which increases stress by decreasing trust and control (Amankwah-Amoah et al., 2021).
During the pandemic, factors such as furlough and sectors of the economy closing and opening again resulted in increased turnover and job-changing in the UK labour market (Jon Boys, 2022). Following on from the pandemic and the effects of Brexit, there are also high employment vacancies and fewer people in most sectors of the labour force (Jon Boys, 2022). It has been hypothesised that this may be due to an exodus of immigrants coupled with a decrease in UK nationals participating in the UK labour market (Jon Boys, 2022). Given this, it is no surprise that one of the UK Government's priorities as part of the Spring Budget 2023 is to increase workforce retention (namely by incentivising workers over 50 to continue working) (UK Government, 2023). According to the Chartered Institute of Personnel and Development (UK), aside from salary and benefits, organisations aiming to improve retention should have flexible working practices, treat people fairly, support well-being, enable career development and ensure employees have a say in work systems (The Chartered Institute of Personnel and Development, 2023). This, in conjunction with the challenges associated with post-pandemic working, suggests that organisations looking to attract and retain workers need to improve working conditions by creating a culture that supports well-being, encourages flexibility, career development and employee consultation.
Pre-pandemic contact centres (previously called call centres) are an example of traditionally office-based organisations frequently cited as having sub-optimal working conditions, often resulting in poor health outcomes and increased turnover. Contact centres handle large numbers of phone calls, normally providing customer service or other business functions within organisations across various sectors (Marr and Parry, 2004). Work is mostly desk-based, and often involves repetitive and monotonous computer-based tasks (Faghy et al., 2022; Toomingas and Gavhed, 2008). Contact centre work can be highly sedentary and stressful, with limited opportunities to engage in physical activity, all of which can increase the risk of long-term health conditions (Chau et al., 2013; Cho et al., 2012; Dempsey et al., 2020; Owen et al., 2010; Proper et al., 2011; Rezende et al., 2014; Thorp et al., 2011). Contact centre staff face several environmental and organisational barriers which prevent them from breaking up their sitting and engaging in physical activity during the work day (Morris et al., 2018; Thorp et al., 2012). For example, low autonomy, strict work schedules and supervision, limited breaks, high workloads with pressure to maintain high levels of productivity and emphasis on individual performance (sometimes commission-based) can all implicitly or explicitly reinforce the individual priority of workload/performance over well-being (Kazi et al., 2014). Contact centres often take a command and control approach, as opposed to a person-centred one where leaders motivate and support staff, rather than control them, to perform (Plas and Lewis, 2000). These barriers are still relevant for work completed outside of the traditional office environment (from home), as was the case for many organisations during the COVID-19 pandemic. High levels of sedentary behaviour and low levels of physical activity in adults can increase the risk of all-cause, cardiovascular and cancer mortality, as well as incidence of cancer, cardiovascular disease, Type-2 diabetes and depression (Chau et al., 2013; Cho et al., 2012; Dempsey et al., 2020; Owen et al., 2010; Proper et al., 2011; Rezende et al., 2014; Thorp et al., 2011). The organisational factors noted above can also create stressful work environments (Kazi et al., 2014). Workplace stress is linked to negative health consequences such as high blood pressure and sleep disturbances (Shirom, 2003) and creates further barriers to engaging in health behaviours such as physical activity and healthy eating (Mazzola et al., 2019). Call handlers, the highest proportion of contact centre staff, have higher levels of job-related depression and anxiety compared to other desk-based workers who are not physically public facing (Sprigg et al., 2003).
Implementation of health promotion programmes at work is a common organisational strategy to improve employee well-being (Ryan et al., 2021), however, they often have mixed success in achieving their aims (Dewitt et al., 2019; Hadgraft et al., 2018; Mackenzie et al., 2019). One reason for this is that many programmes focus solely on individual health behaviours (Ribisl and Reischl, 1993), without consideration of the organisation's underlying culture. Organisational culture is a unique set of values, beliefs and norms which are shared by its members (Buchanan and Huczynski, 2016), and interact with organisational structures, operations and policy (Such and Mutrie, 2017). Factors tied to an organisation's culture, such as tangible objects, and more subtle beliefs, values and assumptions are often neglected (Schein, 2017), despite the fact that they can reinforce or lead to some of the barriers that contact centres face. As organisational culture can influence workplace health and well-being through mechanisms including job satisfaction, work and family balance and job performance (Pronk, 2010), failing to consider these factors can impact effectiveness and long-term sustainability of health programmes (Macdonald et al., 2018; Mackenzie et al., 2019). Cultural barriers and facilitators, such as a supportive or unsupportive work environment and (lack of) social support from management have been shown to be critical to successful workplace health programme implementation (Chau et al., 2014; Hadgraft et al., 2017a; Jepson et al., 2022). There is a need to explore organisational culture factors in workplace settings such as contact centres, where such factors present barriers, and how to incorporate them into health programme design, especially within the new post-pandemic work context.
Health promotion programmes are often designed and understood from an ecological perspective which investigates behavioural influences from multiple levels (e.g. individual, social, environmental, and organisational) (Sallis et al., 1998). The use of the ecological model during health programme development is known to have an impact on workplace health and the success of workplace health programmes (Pronk and Kottke, 2009). The model suggests that, for example, sedentary and physical activity behaviours during the workday will be influenced by a variety of factors (Sallis et al., 2015) including personal factors, workplace social norms, workload (De Cocker et al., 2014; Hadgraft et al., 2017b) and the built environment (Chu et al., 2016). Factors tied to organisational culture are considered broadly as part of the organisational level within the ecological model. However, ‘organisational culture can be conceptually complex and extremely difficult to assess accurately and to change’ (Gifford and Wietrak, 2022: 4). As such, there is often a lack of in-depth consideration of these organisational level factors during programme design and implementation and many workplace health studies conclude that more research or efforts are needed to address them (Macdonald et al., 2018; Mackenzie et al., 2019; Shrestha et al., 2018). This suggests that the ecological model alone may not be enough to break down complex organisational culture factors and understand how they relate to health and health programmes in the workplace.
The incorporation of organisational culture theory has the potential to provide a more complete approach to ensure efficacious workplace health programmes. Such theories prompt an investigation into the interaction of values, beliefs and norms within the specific context of an organisation, and its external environment. Thus, the uniqueness of an organisation is understood from all angles and applied to programme development, delivery and implementation, and evaluation. This allows for the development of a more in-depth understanding of organisational culture and factors at the broader organisational level than previous research or existing protocols.
Schein's (1990) model of organisational culture looks at how cultural artefacts create and shape an organisation's culture in conjunction with absolute and espoused beliefs. The model outlines three bidirectional levels of organisational culture; artefacts, espoused beliefs and values and basic assumptions. Artefacts represent the most superficial, overt and observable elements of an organisation (e.g. the physical environment of the office or home working environment) (Schein, 2017). Changes to artefacts tied to the work environment are particularly relevant post-pandemic given the shift to remote working (i.e., less face-to-face time with colleagues, increased sitting, home working setup, etc.). Espoused beliefs are one step deeper; a company's declared set of values or norms (e.g. a contact centre's employee handbook) (Schein, 2017). Finally, basic assumptions are the core of an organisation's culture; they represent a set of beliefs that are associated with actual behaviour and used to make decisions. In order for a basic assumption to be true, artefacts and espoused beliefs must align. For example, an organisation has a policy whereby, all employees are treated equally (espoused belief) and exemplify this by offering all employees an ergonomic desk assessment (regardless of their role or if they work from home) (artefact). In this example, the espoused belief and the artefact align, and thus we can say that employee equality is a basic assumption (at least with regard to desk environment) of the organisation. However, models of organisational culture can be complex to apply in practice. ‘In Schein's model, the [basic] assumptions and [espoused] beliefs that underpin behaviour are profound, usually invisible to the casual observer and even unconscious to people in the organisation’ (Gifford and Wietrak, 2022: 5). This may explain why such models are seldom used in workplace health programme research. As such the application of Schein's model requires further investigation in different work contexts and provides a novel approach to addressing how organisational responses to COVID-19 disrupted the existence and efficacy of workplace health programmes. Combining Schein's model with the ecological model allows for an investigation of factors related to health programmes and health behaviours from different levels (levels which are proven to influence health behaviours and health programmes) in the context of an organisation's unique culture (artefacts, espoused beliefs and values, and basic assumptions). A similar combination of models was used to understand how culture can influence sedentary behaviour programmes in a workplace setting (Such and Mutrie, 2017). The study indicated that workplace health programme development would benefit from identifying contextual factors within the domains first outlined by Schein (1990) and the ecological levels to better understand health behaviours in the workplace (Such and Mutrie, 2017).
This article draws on the principles of Schein's organisational culture model and the ecological model to investigate existing organisational barriers and conduits to workplace health programmes and how COVID-19-related changes to work may have impacted these. Few studies to date have investigated the novel combination of the challenges and opportunities associated with these new ways of working in the context of organisational culture, and how this might apply to workplace health programmes. The study setting (contact centres) adds an additional level of novelty to this study, especially considering the significant and pre-existing organisational culture barriers these organisations commonly display. Through this unique angle, the current study extends prior literature on behavioural and social factors in the workplace by placing them in the current work context, and applying them to an industry with pre-existing and enduring challenges.
The aim of this article is to identify and understand how organisational culture influences the existence and effectiveness of workplace health programmes in contact centres and how the COVID-19 pandemic disrupted these associations, from the perspective of contact centre leaders (managers) and workplace health experts. The research questions are as follows:
What impact have current external drivers (COVID-19 and digitalisation) have on organisational adaptations and cultural changes within the UK contact centre workforce? What are the existing and post-COVID-19 organisational barriers and conduits to long-term implementation and sustainability of workplace health programmes?
Methods
Study design
This article draws on qualitative, semi-structured interviews. This design allowed for an in-depth exploration of ideas and perceptions about factors related to organisational culture, workplace health programmes and the impact of COVID-19 in UK contact centres. This was motivated in part by Schein's assertion that organisational culture should be assessed qualitatively through studies that observe actions and interactions and by talking with participants, exploring lived experience of the organisational context (Gifford and Wietrak, 2022).
Participants, setting and sampling
Participants consisted of employees working in and alongside the UK contact centre industry. A total of 15 interviews, involving 16 individuals, were conducted and ranged between 30–60 min (average of 46 min). See Table 1 below for detailed participant and organisation characteristics. As noted in Table 1, Participants 4 and 6 were interviewed together upon request due to logistical reasons.
Participant and organisation characteristics.
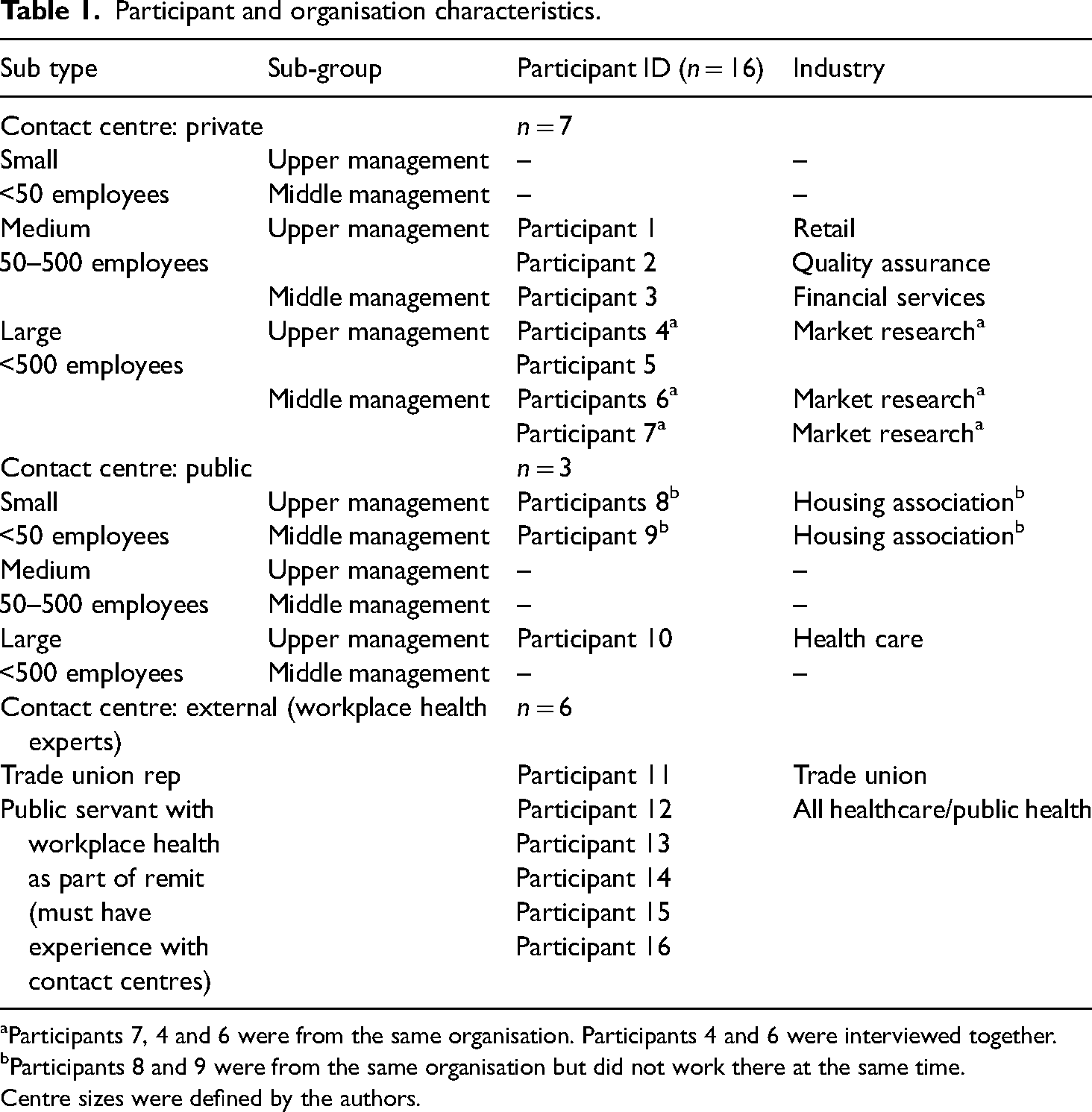
Participants 7, 4 and 6 were from the same organisation. Participants 4 and 6 were interviewed together.
Participants 8 and 9 were from the same organisation but did not work there at the same time.
Centre sizes were defined by the authors.
The sampling strategy used a combination of purposive (stratification) and convenience sampling (snowball recruitment) (Braun, 2013). We recruited upper and middle managers from a mix of private and public contact centres, as well as individuals who worked alongside contact centres (we aimed for at least one trade union representative and one public servant with workplace health in their remit). This allowed for perspectives across various types of contact centres and organisational levels, and from individuals helping to improve employee well-being from outside the contact centre environment. All participants and organisations were UK based. At least one employee from upper management and one employee from middle management was recruited from each size of centre (small <50 employees, medium 50–500 employees, and large >500 employees).
The final sample consisted of: (a) seven upper and middle managers from five private contact centres (industries included: retail, quality assurance, financial services, market research), (b) three upper and middle managers from two public contact centres (housing and healthcare industries), (c) one trade union representative, and (d) five public servants from five health care/public health-related organisations. See Table 1 for details.
The aim of the study was to understand the perspectives of managers and workplace health experts, and as such data from frontline staff was not collected. It was felt that managers and workplace health experts would have a better grasp of the culture and more importantly capacity for change in their respective organisations and the contact centre industry. At least seven of the contact centre managers who were interviewed worked their way up to their position. This meant that they had served more time in the organisation/industry, and had an understanding of what it was like at all job levels, and in some cases from multiple organisations. Also, organisational culture, in part is heavily influenced by senior management (Buchanan and Huczynski, 2016) and middle managers were able to provide unique perspectives as they worked between frontline staff and senior management. Finally, much of the existing literature on workplace health interventions includes perspectives from front-line staff (e.g. Jepson et al., 2022) and this literature is referenced throughout the article and was used in developing the study protocol.
Recruitment
To initially identify and recruit participants, the first author circulated the information among professional networks and invited individuals to participate via email which included an information sheet. Fifty per cent of participants were recruited via email through a UK contact centre association. Participants volunteered and were not financially incentivised to participate.
Data collection procedures
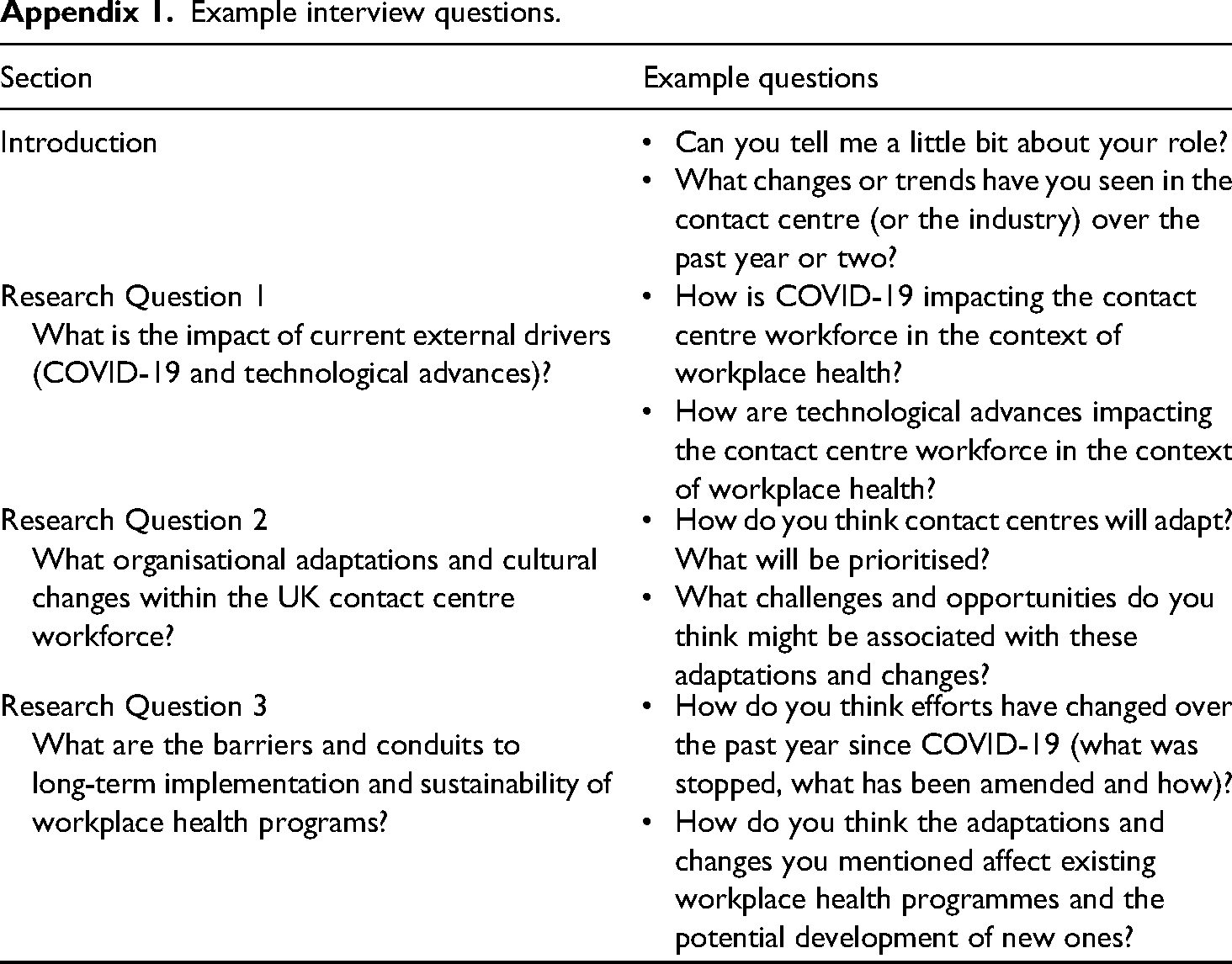
Interviews took place online using Microsoft Teams between February and June 2021. They were audio and video (optional) recorded on the software and transcribed anonymously by the first author. An iterative semi-structured topic guide was developed to address the study research questions based on previous research in this area. The topic guide facilitated discussions around a number of cultural factors to workplace health programmes (level of organisational support in the workplace) and health behaviours (workplace social norms and the work environment) (Macdonald et al., 2018; Mackenzie et al., 2019) and explored their impact on health within the participant's organisation and the contact centre industry. In line with recent studies on the impact of COVID-19 on the well-being of office workers, there were several questions on how COVID-19 impacted working practices, employee well-being and well-being programme implementation, engagement and participation. To understand general trends in the contact centre industry, questions around current external drivers other than the COVID-19 pandemic, and how they affect workplace health programmes were also included. See Appendix 1 for example questions. The semi-structured nature of the topic guide allowed for participants to raise issues that were unanticipated, thus generating a broader picture of organisational culture factors. The first author took field notes during and after interviews in order to adapt the guide as needed to ensure the research questions were adequately answered and that participants were able to bring any additional experience to the discussions.
Data analysis
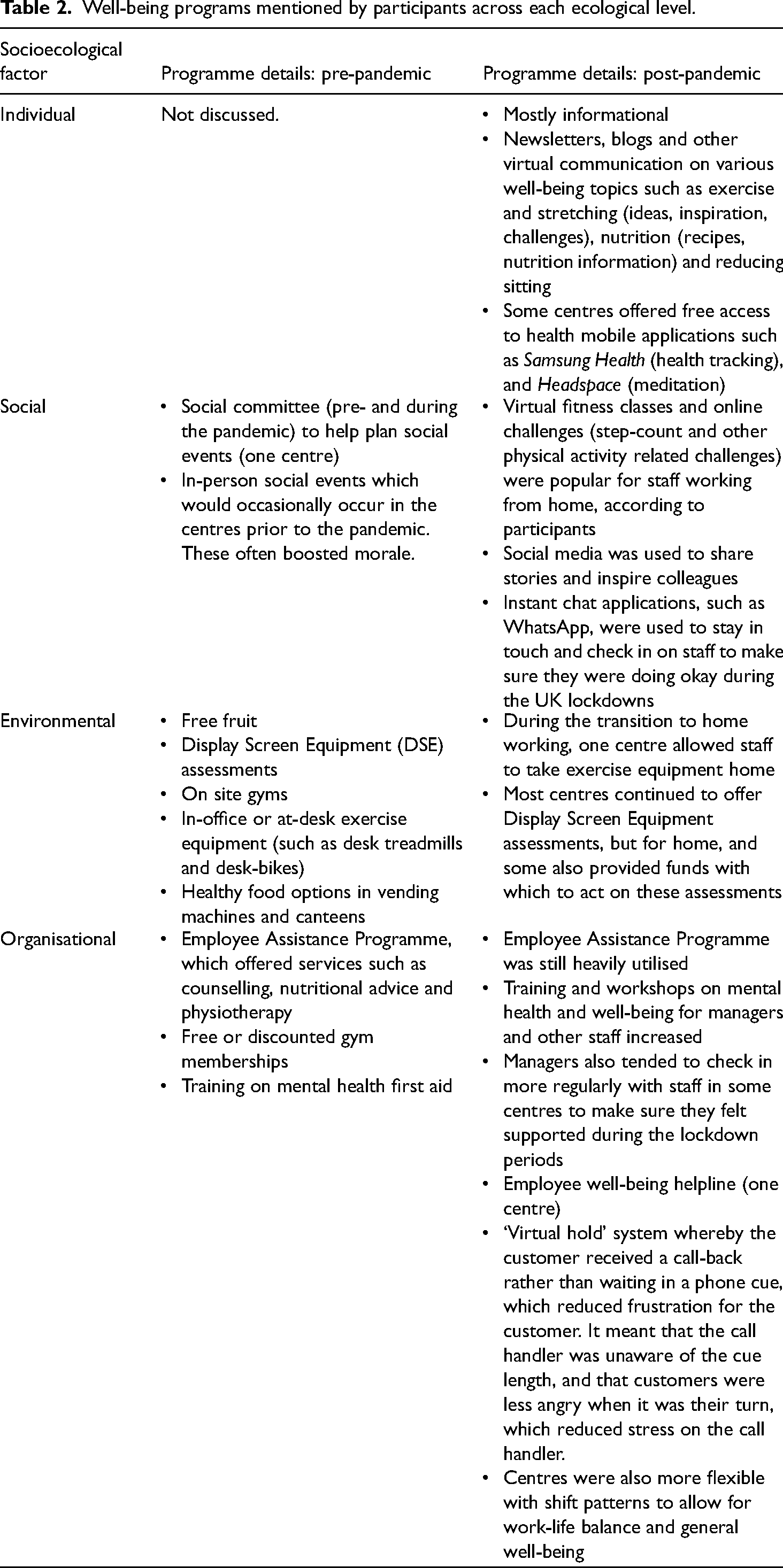
Interviews were analysed using a codebook thematic analysis approach, drawing on the reflexive principles of reflexive thematic analysis (Braun and Clarke, 2021). As the overall study aim was exploratory, an inductive analysis approach was used to allow for unanticipated themes to develop organically, although examples of workplace health programmes were coded deductively by ecological level (see Table 2; well-being programmes mentioned by participants across each ecological level for examples of existing programmes) to capture data on different well-being programmes offered by contact centres. One transcript was triple coded by three of the authors to ensure initial coding related to the study aims and to consider different perspectives. Triple coding was not conducted as an attempt to increase reliability of the coding process. In fact, it is argued inter-rater reliability does not demonstrate rigor as it does not necessarily produce theory-free knowledge, and makes it difficult to identify the appropriate unit of analysis (Smith and Mcgannon, 2018). Furthermore, inter-rater reliability contradicts the reflexive nature of thematic analysis. As such, single coding is considered good practice as it utilises the reflexivity of reflexive thematic analysis (Braun and Clarke, 2022). Following triple-coding, the first author developed an interative codebook with preliminary themes which captured all relevant codes identified by all three authors. The first author coded the remaining transcripts in NVivo using the codebook, which evolved as relevant codes and themes were added, in order to capture the prominent codes and themes of the collective dataset. This iterative approach allowed for data-driven codes to develop (Braun and Clarke, 2021). Transcripts were coded completely and a latent approach to theme development was used to enable underlying patterns and ideas which underpin participant experience to be captured (Braun and Clarke, 2006). Themes were named in an attempt to showcase to the reader why the theme is important and interesting while capturing ‘the “essence” of what the theme is about’ (Braun and Clarke, 2006). Relevant themes were further analysed in the context of Schein's model of organisational culture (Dauber et al., 2012; Schein, 2017). This allowed the authors to make deeper connections between the developing themes and the influence of Schein's three levels of organisational culture. The model was not incorporated into the initial analysis for the reasons above; the initial phase used an inductive approach to allow for organic theme development. Initial theme development for both stages of analysis (before and after the application of Schein's model) was conducted by the first author and then discussed and clarified amongst all authors.
Well-being programs mentioned by participants across each ecological level.
Ethics and informed consent
Ethics approval was received from the Moray House School of Education and Sport Ethics Committee, University of Edinburgh (Ref: JM08122020-1). Participants received an information sheet and were encouraged to ask questions prior to their interview. Participants provided written informed consent using an online form on Qualtrics (Qualtrics, 2021) prior to the interview, which was reaffirmed verbally before recording.
Findings
Findings are presented in three parts. First, we found that management's response to organisational challenges of COVID-19 highlighted gaps in employee well-being support and ongoing initiatives. Second, we identified gaps in management's awareness of the wider organisation determinants of well-being. Third, we evidence lessons learned from the impact on employee well-being of homeworking during the pandemic. These findings are then discussed in the context of Schein's organisational culture model.
Organisational attitudes towards employee well-being and support provided
Shifting organisational attitudes towards employee well-being, catalysed by COVID-19 provided conduits for well-being support in contact centres. Upper and middle management in contact centres were more focused on supporting their employees during the pandemic than they had been previously. In some centres, this shift in thinking began pre-pandemic (see Participant 2 quote below), whilst others were prompted to consider the importance of supporting employees and adapting to their needs during and post-pandemic. These perceptions were reported by all participants, most of which were contact centre managers themselves. Participant 2 (upper management) explained when this shift started to happen in his organisation: … there's a far better understanding now that we [the industry] need to look after people, than we ever have done in the past. Certainly … maybe five years ago, things started to change for the better.
There was a ‘recognition that they [contact centres] need to do more to support employees, not just because it is a good thing to do for the individual, but also business wise’ (Participant 13, public servant). The pandemic appeared to act as a catalyst for upper and middle management to improve employee well-being support, or as Participant 1 (upper management) put it, ‘accelerated’ improvements in such support. During the pandemic, organisations were more inclined to attend to the individual needs of employees, which varied greatly from employee to employee depending on their personal and living circumstances and ability to work from home.
Changed management behaviour resulted in asking employees what they want and need to support their well-being and to do their job well. Support needs were mostly collected through staff surveys, however, some centres encouraged staff to come forward on an ad-hoc basis. Centres were more open to flexible working and work-from-home requests (even when offices re-opened), shift changes, and shortening of hours to support work-life balance. Some participants also felt that in some centres most employees were ‘trusted more just to get on with their job’ (Participant 5, upper management) which increased autonomy and empowered homeworkers. It was perceived that this change in management behaviour served to keep staff happy and working effectively, and as a result ’people have been more productive’ (Participant 1, upper management). While seemingly motivated by business continuity, the change in management practice had the additional benefit of maintaining job satisfaction through the personal and organisational challenges of the pandemic.
During the pandemic, most centres were quick to develop new well-being programmes (e.g. see Table 2 ), however, there were barriers to engaging staff (such as perceived lack of time) and a lack of consensus on their effectiveness. Although contact centres ‘traditionally had high turnover of staff’ (Participant 13, public servant), a few participants mentioned that some contact centres are now looking to attract and retain talent through well-being support, appearing socially responsible and enabling growth within the business. Participant 2 (upper management) noted, ‘[it] was becoming challenging to get skilled people [leading up to and since COVID-19]. So more had to be offered. And if it wasn’t around necessarily salary, it was more about culture, environment, showing up on things that people care about far more than they ever used to’. This supports the sentiment behind the Great Resignation, and the idea that organisations must create better working conditions to reduce turnover in the post-pandemic context (Hirsch, 2021; Serenko, 2022; Sheather and Slattery, 2021; Sull et al., 2022). See Table 2 below for a list of the different activities offered pre and post-pandemic among contact centres that participants worked with or alongside. These are divided into factors (levels of analysis), which have been adapted from ecological models of behaviour change (McLeroy et al., 1988); individual, social, environmental and organisational.
It was acknowledged that consistently measuring staff well-being was important in (a) determining their needs and what health programmes might be helpful and (b) understanding the effectiveness of existing programmes. However, successfully measuring programme impact was ‘a big gap’ (Participant 10, upper management) in understanding effectiveness and thus the ability to improve employee well-being. The act (artefact) of employee well-being and health programme evaluation was lacking in contact centres because of organisational barriers such as lack of staff time and expertise.
Specific perceptions on attitudes and support around mental and physical health are provided below.
Unintended consequences of prioritizing mental health during the pandemic at the expense of physical health
All participants noted that there was a focus on and a ‘recognition of the importance of mental well-being and what employers can do to support that’ (Participant 13, public servant) prior to and during the pandemic. For example, centres were encouraging informal virtual communication as a means of ‘checking in’, providing apps, offering the Employee Assistance Programme and mental health first aid training.
Due to the stressful and repetitive nature of some contact centre roles, some participants mentioned that staff often burnt out, and this was exacerbated by the stresses and anxieties caused by homeworking, and of changes to living and personal circumstances as a result of the pandemic. A few participants mentioned an absence of support and training for middle management which created barriers in being able to effectively support employees who were struggling. There was also a lack of acknowledgement of the pressure felt by managers to support these employees, both individually and as part of mental health programmes. Participant 1 (upper management) described this in the following quote: … there's a lot of blame placed on bad leadership for people's mental health issues. … these guys aren’t set up for this, to manage this stuff. So, no wonder they are getting it wrong, or they don’t know what to do … for those first level leaders, it's difficult because we expect them from a mental health perspective to be counsellors.
Although it was believed that organisations were more focused on mental well-being during the pandemic, it was felt that some centres were making efforts (and/or had done so pre-pandemic) to improve physical well-being in addition. As mentioned in Table 2, centres offered programmes such as newsletters, apps, and online challenges. Pre-pandemic (and for centres who kept staff in-office during the pandemic), some employees had access to things like on-site gyms and fitness classes. However, this varied between centres and their unique cultures.
The contact centre environment often presented barriers to well-being. Participants identified a need for centres to pay more attention to the environment of employees working from home and to offer more long-term solutions to reduce the risk of developing musculoskeletal issues due to poor setup and lack of movement during the workday. Homeworking environments varied among staff, many of whom did not have an appropriate working environment (desk, ergonomic chair, etc.). The offer of a homeworking ergonomic assessment varied among organisations and this was noted by both contact centre managers and workplace health experts (i.e., Participants 11–16). For example, managers from three organisations (Participants 1, 3 and 9) mentioned the use of Display Screen Equipment (DSE) ergonomic assessments for home workers. For staff who did receive ergonomic advice, only some were provided with, or received financial support to purchase, appropriate equipment. For example, Participant 3 (from a large financial services organisation) and Participant 9 (from a small public housing association) said that their organisations provided equipment, and Participant 1 said his (medium-sized retail organisation) offered funds to purchase equipment to certain staff but not others. Additionally, some staff did not have space for new equipment, so it was not possible to follow DSE assessment recommendations. This led to inequalities between centres and among staff. … now that so many people are working from home there isn’t enough focus being placed on have people got the right working environment. Physically are their homes actually suitable for their physical health long term, and those are then linked into mental health because the two are, in many ways intrinsically linked from my experience. (Participant 1, upper management)
Sedentary behaviour, although high in contact centre staff, was rarely mentioned, and programmes which target this behaviour were limited. Most of the workplace health experts (Participants 12, 14, 15 and 16) felt that sedentary behaviour needed to be addressed independently of support for physical activity and mental health, which were the primary factors targeted in contact centres. Participant 4 (upper management) said that sedentary behaviour ‘did go by the wayside’ as a well-being-related priority during COVID-19.
As implied above, well-being support varied greatly among centres. Participant 11 (trade union representative) noted that, ‘[in] a lot of the non-unionised workplaces, employers don’t have that option [of employee assistance programs and alike]’. Although managers may have changed their thinking around well-being support, this highlights one of the more significant barriers related to implementation of such support.
Overall, contact centres were good at acknowledging the importance of mental and physical health (pre and post COVID), and tailoring support to the needs of individuals, however there were sometimes barriers related to putting this knowledge into practice in a practical and sustainable way.
Gaps in management's awareness of the wider determinants of workplace well-being
Organisational buy-in
According to many participants, having buy-in and well-being champions at every level of the organisation was a key conduit. However, participants reported that ‘a lot of the culture really is set by the individuals at the top’ (Participant 14, public servant). Participants also believed that changes to the culture of an organisation require financial investment in well-being programmes (e.g. buying staff equipment to work from home), but also staff time and resources, to develop and implement such programmes using a top-down approach. Participants felt that sometimes senior managers did not acknowledge the need for investment in well-being programmes, and they believed that ‘as long as the ROI is okay, what's the issue?’ (Participant 2, upper management). To overcome this barrier, it was felt that some top-level contact centre managers (chief executive officers, directors) would benefit from education around the wider organisational determinants of well-being. This would provide incentive to look past short-term ROI indicators and understand the longer-term business benefits to investing in sustainable well-being solutions. However, participants expressed difficulties in capturing the attention of busy senior managers and in providing captivating evidence to create a business case for investment. It was also felt that senior management should lead by example (e.g. by participating in well-being programmes).
Support for middle management
Engagement of middle management was viewed as key to the success or failure of well-being programmes. However, there was often a contradiction between what they were asked to do to support staff well-being, and what they needed to do to fulfil their remit (normal work tasks such as ensuring staff hit targets). This shows conflicting espoused beliefs of senior management, and supports the notion mentioned above that organisational culture must be changed top-down. Middle managers were normally expected to spend time implementing well-being programmes, while continuing to juggle their regular workload and meet performance expectations. These challenges were exacerbated by the pandemic, as organisations rushed to implement new well-being programmes whilst transitioning to a new work context. For example: … it's really difficult for those [middle] managers because presumably they’re getting that message [about supporting wellbeing programs] saying this is important, you need to do these things but equally another message saying, but you got to hit the targets. (Participant 15, public servant)
It was suggested by a number of participants (from both upper and middle management) that middle management should be provided with the resources and support to carry out well-being programmes, and for them to be explicitly told if they would be receiving this when being asked to do so. Participant 13 (public servant) explained the need for this: I think that's where the change needs to happen, between the middle and senior management, for senior management to demonstrate, yes, we will support you to do this. And then middle management to be able to confidently say, ‘we realise these are the impacts it could have on short term productivity, or releasing staff to attend different things’.
This lack of consideration of staff time and resources (particularly for middle management) during well-being programme implementation was seen as a major barrier to the success of well-being programmes.
Effective communication of available support
Many participants acknowledged the efforts contact centres were making to improve the type and frequency of well-being communication with staff. Since the pandemic, many centres were engaging in two-way communication, listening to staff needs and taking them on board, and encouraging them to prioritise their well-being. Some centres began to act this way prior to the pandemic, and it was felt that this behaviour was tied to a shift in culture and would remain in the long term. However, participants felt there was a need for some centres to explicitly give staff permission to make choices in line with this, such as allowing staff to take breaks when needed. Participant 1 (upper management) described the need for this below: It's probably all a bit superficial because a lot of it was sending out newsletters with: stand up, take a break, walk around, get some fresh air, take regular screen breaks, do this that and the other … we need to almost empower them, give them permission, tell them it's okay to do it.
Difficulties in engaging homeworkers in well-being-related communication was noted as a barrier and participants felt it was more difficult to cascade communication around well-being policies, procedures, and education down the business. This was especially challenging if there were bottlenecks created by middle management, for example if managers lacked time and resources as mentioned above, or were not supportive.
A paradoxical culture of productivity and time pressure and time spent on employee well-being
All participants described contact centres as numbers-driven businesses, with most staff needing to adhere to strict targets, which presented barriers to well-being and well-being programmes. Depending on the nature of the centre, call handlers were often subject to stressful calls by service users and roles were sometimes commission-based, which added to an already pressurised work environment. One of the major challenges identified by participants was contact centre senior managers’ reliance on numbers (e.g. meeting targets) to determine business success without regard to their context. A lack of interpretation and questioning of such numbers filtered down to middle management, which perpetuated a numbers-driven culture onto front-line staff. Participant 1 (upper management) said, ‘… your headline number might be read on a dashboard each week … the context that sits behind that could be an absolutely brilliant result because of 300 other things that have influenced it’. He also expressed that things may be changing, noting, ‘there has been a real shift in terms of more flexible and more progressive thinking over what good looks like’.
Participants reported that some contact centre senior managers were too driven by organisational performance metrics to consider investment in well-being programmes. Senior management often thought that such programmes might have a negative impact on business. For example, Participant 3, a senior manager, felt that ‘… a lot of organisations, especially now, are really concerned about productivity being reduced, and losing money if staff are doing things other than being at their desk’. It was largely accepted that the emphasis on organisational performance was a key (and inherently logical) basic assumption of contact centre businesses and was therefore unlikely to change. However, participants indicated that well-being programmes could actually improve performance by increasing employee engagement, decreasing absence and turnover and increasing productivity. It was suggested that, in order to make a case for investment and buy-in from senior management, contact centre managers, union reps, public servants and researchers needed to make clear connections between investment in well-being programmes and potential business benefits, particularly around productivity. Following on from her comment above, Participant 3 noted, ‘it really just goes back to productivity and ROI and, and really evidencing how workplace health programmes or initiatives or things like that are good for the business’. Participant 11 (trade union representative) echoed this in saying, ‘it's all about educating the employer about how they can get more from the staff [by supporting their wellbeing]’. This further outlines the importance of providing appropriate support for middle management who are the first point of contact and support for staff. It also exemplifies a positive shift in how numbers and targets could be communicated by and to middle managers differently despite their perceived permanence.
Centres were described as ‘command and control’ environments where management dictated strict rules about what staff could and could not do. This type of culture further increased perceptions of time pressure. However, some participants perceived that things were changing in some centres, where staff were managed as peers rather than subordinates. For example, Participant 1, a senior manager, said, ‘How you work with people and how you motivate them is more sophisticated because if you just keep telling people eventually they just switch off. So irrespective of the leadership role you are in, you have to just make sure that you’re managing everybody as your peer’. This cultural shift in leadership style, including the interpretation and communication of targets mentioned above present perceptions of how to improve employee motivation, engagement and overall well-being without sacrificing organisational performance. However, Participant 1 (upper management) reinforced the need for middle management support and training in saying, ‘first level leaders [i.e., middle managers] find it the most difficult to adapt’, and, ‘change their style of leadership away from just looking at numbers’. As mentioned above, it was felt that middle managers had difficulty balancing the need for their staff to be productive whilst supporting their well-being.
It was felt that the rigid and stressful contact centre environment increased the need for well-being support, while simultaneously presenting barriers to participation. Lack of time (or perceived lack of time) was the most cited barrier resulting from this organisational rigidity and this point was mentioned in some form by every participant. Factors such as limited break times and pressure to hit numbers were seldom considered when developing and implementing well-being programmes. This resulted in programmes that, although beneficial, emphasised individual responsibility and were seen as more ‘superficial’ (such as newsletters). Furthermore, if employees did not perceive that they had the time to take part in well-being programmes or health behaviours more broadly, such efforts (regardless of type) had little or no impact on their well-being.
Participant 12, a public servant, said ‘I really don’t think that they’ve got it yet. They’ve really not’. This illustrates that, although organisational attitudes around well-being are shifting (especially since the pandemic), many efforts to support employee well-being might still be superficial due to the focus on numbers and metrics.
Impact of homeworking on a post-pandemic future of ‘contact centre’ work
The COVID-19 pandemic forced many organisations to adopt a homeworking approach, which shifted the physical artefacts of the workplace. Participants sensed that this trend would continue indefinitely in some form based on their perceptions of how the industry adapted during the pandemic. Homeworking was perceived to support both work-life balance, productivity and an increased level of service provided by employees. Transitioning to online working offered a ‘huge amount of operational flexibility’ (Participant 5, upper management) and allowed organisations to continue to operate using homeworking models during the UK's lockdown periods. However, there were challenges in engaging virtually with staff for the purpose of work management and well-being support. Centres tried to utilise informal virtual communication such as WhatsApp and desktop instant chat functions, some for social purposes and to help support employee well-being. As mentioned previously, a few ran online health challenges, provided health applications, and sent newsletters which facilitated health behaviours and social interaction.
Homeworking also limited social contact among colleagues, which reduced opportunities to engage in activities that support well-being, such as the ability to switch off, go for a walk or prompt a much-needed screen break. The inability to read body language and tone (if written communication) made it challenging to communicate and develop relationships, especially among colleagues who had rarely or never met in person. Mental exhaustion from excessive use of virtual platforms (in particular video calls), sometimes referred to as ‘Zoom fatigue’ (Bailenson, 2021) was frequently mentioned in interviews as detrimental to online working. Some homeworkers, including the participants themselves, felt a blurring of work and home life, which sometimes led to longer working hours, and a difficulty in disconnecting from work. Many call handlers were also subject to increases in the volume and urgency of calls during the pandemic. This exacerbated an already tense working environment, especially for those working from home. Participant 9, a middle manager, describes this challenge below: COVID has been mentally draining on everyone. And our work, it's actually very stressful. We’ve got strict procedures to follow in certain circumstances because of the nature of the calls and when you’re isolated working from home, you’ve not got a team to bounce off as quick … you’re in that spot where you’re making those decisions yourself. You’re not in that office space environment and it is stressful.
In summary, as demonstrated above, an analysis of the organisational culture of a contact centre as defined by Schein (1990) indicates that employees sit for most of the day, their work environments are varied, most communication is online, and breaks are often short and rigid. As a result of these artefacts employees do not always have the time and support to act or engage in health programmes or health behaviours. Yet, contact centres espoused values often tell a different story. They outwardly acknowledge the importance of mental and physical well-being through their internal communication with employees. They also make efforts to promote the well-being programmes and initiatives they offer, and task middle management with their implementation. Despite this, the artefacts often indicate that a contact centre's true beliefs (basic assumptions) might not necessarily prioritise employee well-being. This paradox between espoused values and artefacts can be attributed to metrics-driven cultures; the prioritisation of business success over employee well-being.
COVID-19 led to new physical workplace artefacts; an increase in the variability of work environments (for those who began to work from home) and online communication. However, it appears to have acted as a positive disruptive force with regard to organisational attitudes, and stronger espoused values, around the importance of workplace well-being. Attending to the individual needs of employees, including allowing more flexible working has shifted some of the artefacts of contact centre work, more closely aligning them to these stronger values. Despite the continued existence of artefacts which indicate a lack of time and resources to engage in and support well-being behaviours and programmes reveal somewhat unchanged beliefs (basic assumptions). Employee well-being may be higher up on the priority list, but business outcomes are still number one.
Discussion
This article provides new insight into how COVID-19 disrupted and is likely to continue to disrupt organisational practices of workplace health and well-being programs in contact centres. Building on existing research, which identified contact centre workers as at risk of lower physical and mental health outcomes (Chau et al., 2013; Dempsey et al., 2020), we provide three key and novel insights for a post-COVID-19 organisation context. Contact centre management response to organisational challenges of COVID-19 highlighted gaps in employee well-being support and ongoing initiatives. We also identified gaps in management awareness of the wider organisation determinants of well-being, and of employee lived experience of workplace well-being. We conclude by evidencing lessons learned around the impact on employee well-being of homeworking during the pandemic, and how call centres might address the paradoxical cycle of productivity and employee well-being. Despite the fact that the study included a range of contact centre industry employees, participants shared similar perceptions and experiences increasing the relevance of the findings.
COVID-19 and the resulting move to homeworking appear to have shifted management attitudes toward the importance of workplace health programs. However, the novel application of Schein's theory (Schein, 1990) to the findings reveals a contradiction between espoused values around health and well-being programs and not always providing employees the time and space to act or engage in such programs and in health behaviours more broadly. This suggests that business performance still supersedes employee well-being as a basic assumption of contact centre organisations. It was acknowledged that this was not going to change, which indicates a need for the development of solutions which optimise both. Using Schein's levels of organisational culture, we identified specific cultural barriers and proposed potential ways to address them based on our analysis and interpretation of participant perceptions and existing well-being initiatives across the various ecological levels. Although Schein's model has frequently been used in other studies (e.g. Such and Mutrie, 2017), this is the first instance, to our knowledge, of the model's application to examine the impact of the disruptive nature of COVID-19 on organisational culture in contact centres in the context of well-being programs. The unique contribution here demonstrates that the crisis situation brought about by the pandemic has also resulted in positive changes regarding how contact centres approach employee well-being.
One of the major challenges identified by participants was contact centre senior managers’ reliance on performance metrics to determine business success, and the fact that the sometimes rigid and stressful contact centre environment increased the need for well-being support, while simultaneously presenting barriers to engage in such support (particularly perceived lack of time). This supports existing literature on the negative impact of productivity pressure on mental health and engagement in health behaviours such as physical activity and reducing sedentary time (Renton et al., 2011). Acknowledging that the emphasis on targets and metrics is unlikely to change, shifting leadership style away from command and control, and communicating targets in a more positive and supportive manner could help reduce some of this pressure without discounting organisational performance. This could be achieved through a more person-centred leadership style where leaders motivate and inspire staff to perform whilst creating a positive and supportive work environment (Plas and Lewis, 2000). This type of leadership is flexible and adaptable to the specific organisational context as it ‘tends to operate somewhat differently from organisation to organisation because its’ successful execution depends on the specific individuals who implement it and the unique culture in which it is developed’ (Plas and Lewis, 2000: 35). Evidence suggests that person-centred leadership can work well in high-pressure systems (Plas and Lewis, 2000) of which contact centres are an example of. This leadership style may also be ideal for hybrid working, as it fosters employee motivation, engagement, and adaptability even in virtual work environments.
Leadership style is particularly important for managers, who have the potential to help their organisations reduce and overcome the identified barriers through setting a positive example, communicating effectively and taking into account the individual needs of employees. Middle management specifically had the potential to help implement and engage with well-being programs and support the well-being needs of their teams, but only if they were provided with the training and support to do so, indicated by a top-down approach to well-being. Evidence suggests that middle managers have the capacity to be change agents if they are adequately supported to do so (Buick et al., 2018). However, middle manager experiences and how they can contribute to change are often overlooked in the literature (Balogun, 2003). As such, the lack of middle management support and training with regard to employee well-being (including how management style can benefit both well-being and performance) is a significant finding from this study, and an important issue for contact centres.
Assessing and changing an organisation's culture is incredibly challenging, especially considering basic assumptions and espoused beliefs are often difficult to identify (Gifford and Wietrak, 2022). Despite the need for this consideration, as indicated in previous studies (Macdonald et al., 2018; Mackenzie et al., 2019), contact centres lacked strategic planning around well-being programme implementation that considered organisational culture factors. Furthermore, there was a lack of evaluation of well-being programs, which limited knowledge of effectiveness and opportunities for enhancement. Although productivity may always be the highest organisational priority, aligning well-being with business outcomes (such as productivity and turnover) by demonstrating how these two sets of outcomes are intrinsically linked through mechanisms such as increased engagement and motivation to hit targets as well as decreased sickness absence would help make the case for future investment in health and well-being programs.
According to participants, homeworking and the increased utilisation of technology were perceived to increase operational flexibility, work-life balance and productivity. However, the literature on homeworking indicates a number of issues associated with this (Amankwah-Amoah et al., 2021; Giorgi et al., 2020; Hayes et al., 2021; Nijp et al., 2016; Oakman et al., 2020; Ráthonyi et al., 2021). For example, challenges with communication, collaboration and time management while homeworking during the COVID-19 pandemic were noted in one US study (Hayes et al., 2021). Similarly, participants in the current study reported that homeworking during the pandemic presented challenges to effective communication and engagement. Participants also expressed that perceived lack of time was a major (pre-existing) barrier to health behaviour participation, arguably exacerbated by the effects of the pandemic and homeworking. Previous evidence also indicates that homeworking and challenges with time management can contribute to higher levels of perceived stress and burnout, both related to work, and balancing work and home roles (Hayes et al., 2021). Participants in the current study echoed these findings, while also describing the positive changes to organisational attitudes with respect to employee well-being brought on by COVID-19.
Overall, in response to COVID-19 most centres were quick to recognise the importance of employee well-being and to develop helpful programs to support this. However this support varied among centres and there were often issues with implementation, engagement and evaluation. Creating a person-focused culture where the individual needs of staff and their well-being are considered and they are managed as peers in a positive and supportive manner from the top-down would help alleviate these issues and benefit both employees and their organisations. A number of practical implications have been noted at the end of this section, which outline how this could be achieved.
Strengths and limitations
This study contributes unique insight into the efficacy of workplace health programs through a period of crisis and organisational instability, namely the COVID-19 pandemic, from an analysis of qualitative data from a diverse set of employees working in or alongside contact centres of different size and sector. Further, this study brings together both ecological and organisational culture theories, which few articles have done despite the significant overlap in concepts within them. The ecological model allowed for an investigation of workplace health programs and health behaviours across different levels, and Schein's model allowed for this to occur in the context of organisational culture to understand how it impacts workplace health programs. This angle provides a new way of investigating why some workplace health promotion programs fail to deliver expected benefits. The study's design takes into account findings from an ecological perspective and acknowledges its limited ability to break down organisational culture factors and understand the relationships between them. The novel application of Schein's model (Schein, 2017) to the findings fills this gap, and allowed for the identification of the pre and post-COVID-19 artefacts, espoused values and basic assumptions of contact centres and how these three levels of culture could be used to optimise both well-being and business performance. Given these strengths, the findings could be applied to the development of health programs in contact centres and other desk-based working environments in the post-pandemic social and economic context.
As some participants were recruited via convenience sampling or through a contact centre association, it is possible that these participants, and their organisations may have already been motivated to improve well-being programs in their organisation or had already made efforts to do so. Furthermore, if Participants 4 and 6 were interviewed separately (rather than together) it may have produced different data. The study could have also included frontline staff (such as call handlers) and more trade union representatives (as we were only able to recruit one) to capture perspectives from participants within a broader range of job roles and perspectives. Justification for the exclusion of frontline staff was included in the methods section. Additionally, the impact of the COVID-19 pandemic on organisational culture in contact centres, and on the culture of office work more broadly is still in its infancy. Organisations are often required to significantly shift their culture during times of social and economic change in order to position themselves within a new context (Meyerson and Martin, 1987). Therefore, it is possible that organisational culture will continue to change as organisations recover and recalibrate from the pandemic. Despite these limitations the study makes an important theoretical contribution to the literature on the effectiveness of workplace health programs and a practical contribution to future workplace health programme development.
Implications for practice
Although organisational culture can be difficult to assess and change (Gifford and Wietrak, 2022), doing so may help improve employee well-being in a way which encourages, but does not necessitate the reduction of targets or performance metrics which are unlikely to change (especially given the current economic climate). Contact centres would benefit from routinely speaking to staff and management in order to identify and address organisation-specific barriers to health programme and health behaviour participation by staff, using the ones identified in this article as a guide. An example of this could be leveraging homeworking to support well-being by considering individual needs such as flexible working and ergonomic support at home. More broadly, organisations may want to consider adopting a person-centred leadership style. The reason being that this style is culturally-dependent and allows managers from all levels to motivate their staff to achieve desired targets whilst making them feel they are adequately supported in doing so (including well-being-related support). It is also important for organisations to ensure that there are adequate support and resources for middle management to effectively lead in this way and support the well-being of their staff. Addressing these and other cultural barriers may benefit employee well-being and well-being programs in the first instance. However, in some cases, although beneficial, cultural changes alone may not be enough to enable staff to achieve targets in a feasible, sustainable and healthy manner. In these circumstances adjusting targets may still be required. Additionally, stakeholders (researchers, centre managers etc.) need to make clear data-driven connections between well-being programs, improvements to employee well-being, and business outcomes such as productivity and turnover to make the case for investment in well-being programs. Consistently evaluating the effectiveness of well-being programs alongside health and business outcomes could help make this case, while supporting the ongoing design and implementation of programs.
As we write about the future of work and lessons learned for supporting workplace health, we are mindful that regulatory bodies, such as the Health and Safety Executive (HSE) in the UK are prompted to review their regulatory frameworks for a post-COVID world of work (Davies and Rodgers, 2023). Specifically, there are calls for much higher recognition for health and safety processes and protocols to be focused on ‘every person in the workforce’ (Davies and Rodgers, 2023). This shift is an opportunity for employers to be more engaged in health and safety, which we suggest should be incorporated into broader workplace culture (Davies and Rodgers, 2023).
Conclusion
Our findings highlight the need for employee well-being to be increasingly prioritised within contact centres. There is a need for contact centres to gain an increased understanding of their organisational culture during the various stages of well-being programme planning, development, implementation, and evaluation, to increase effectiveness and sustainability and support positive organisational change. This may require re-evaluating an organisation's espoused values and engaging in strategic planning of well-being programs and programs which not only consider the behaviour of employees and their environment (artefacts), but also the basic assumptions of the organisation which create barriers to well-being (such as prioritisation of numbers and leadership style) to optimise both business success and employee health. These findings could potentially be applied to other industries that employ desk-based workers, as working conditions and job roles may be transferable to similar barriers and conduits to well-being programs. Subsequent studies should focus on developing an understanding of how to address the identified organisational barriers in the context of homeworking.
Footnotes
Acknowledgments
The authors would like to thank the Call Centre Management Association (CCMA) for their support and assistance with recruitment of participants. They also thank Dr Sally Brown for her input during the initial manuscript drafting.
Availability of data
Anonymised participant data available upon request to
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded as part of a PhD studentship by the School of Health in Social Science, University of Edinburgh.
Biographical notes
Appendices
Example interview questions.
| Section | Example questions |
|---|---|
| Introduction |
Can you tell me a little bit about your role? What changes or trends have you seen in the contact centre (or the industry) over the past year or two? |
| Research Question 1 What is the impact of current external drivers (COVID-19 and technological advances)? |
How is COVID-19 impacting the contact centre workforce in the context of workplace health? How are technological advances impacting the contact centre workforce in the context of workplace health? |
| Research Question 2 What organisational adaptations and cultural changes within the UK contact centre workforce? |
How do you think contact centres will adapt? What will be prioritised? What challenges and opportunities do you think might be associated with these adaptations and changes? |
| Research Question 3 What are the barriers and conduits to long-term implementation and sustainability of workplace health programs? |
How do you think efforts have changed over the past year since COVID-19 (what was stopped, what has been amended and how)? How do you think the adaptations and changes you mentioned affect existing workplace health programmes and the potential development of new ones? |