
Abstract
Forced psychiatric medication, administered without consent, is one of the most ethically contested practices in mental health care. While often justified through risk management and biomedical models, the voices of those subjected to it are frequently marginalised. This scoping review synthesises findings from 21 qualitative studies to explore individuals’ experiences of forced medication. The review identifies recurring themes of violence and dehumanisation, epistemic exclusion, protest and survival strategies, powerlessness, retrospective reframing, and a desire for alternatives. Interpreted through the Power Threat Meaning Framework, the review frames forced medication as a manifestation of systemic power that shapes emotional responses, meaning-making, and lived experience. Provisional psychopharmacological considerations are also proposed for future research to empirically examine, suggesting that coercive contexts may alter subjective drug responses. Taken together, these findings call for an epistemological shift towards rights-based, relational, and trauma-informed care surrounding medication use.
Introduction
Forced psychiatric medication, defined as the non-consensual and coercive administration of psychotropic drugs, is one of the most ethically contested practices in mental health care (Sashidharan & Saraceno, 2017). In England and Wales, the Mental Health Act 1983 permits individuals to be detained and treated without consent if they are considered to have a mental disorder and pose a risk to themselves or others (Ogunwale, 2019). Between 2022 and 2023, more than 53,000 people were involuntarily admitted in the United Kingdom, representing an increase of over 40% since 2000 (National Health Service, 2023; Smith et al., 2020). Individuals detained under the act may experience various coercive interventions, including physical restraint, seclusion, and the administration of medication without their agreement. These practices are widely recognised as harmful to autonomy, dignity, and psychological well-being (Aguirre et al., 2023; Sashidharan & Saraceno, 2017).
Although often justified on clinical or legal grounds, forced medication is experienced by many service users as traumatic. It is strongly associated with dissatisfaction and disengagement from psychiatric care (McLaughlin et al., 2016). Reports frequently highlight loss of trust, emotional distress, and deterioration in therapeutic relationships (Knight et al., 2023; Szmukler & Appelbaum, 2008). Under current legal frameworks, psychiatrists are granted authority to enforce treatment based on capacity assessments and risk evaluations. These decisions often rely on the biomedical model, which views mental distress as rooted in biological dysfunction and prioritises medication as the primary and at times only intervention, facilitating its administration by force (Lavelle & Tusaie, 2011). Recent qualitative work within National Health Service (NHS) inpatient teams has shown that many clinicians still perceive the biomedical model and medication treatment to hold dominant explanatory power, especially under resource pressure and within biological training norms (Barnes et al., 2022).
Service users who resist medication or question their prescribed treatment are often labelled as “lacking insight,” a designation that could provide the basis for both legal and ideological justification for forced administration on the grounds that it serves the individual’s best interests (Johnstone et al., 2018). Although some clinicians argue that forced medication may lead to symptom reduction, remission, and eventual discharge into the community, its long-term effects on therapeutic relationships, medication adherence, and overall well-being remain highly contested (Gøtzsche, 2022; Katsakou et al., 2011). Ethical concerns are significant too, as the practice challenges the principles of informed consent and bodily integrity. The United Nations has called for the global abolition of involuntary psychiatric treatment, citing its potentially discriminatory impact on people with disabilities (Corderoy et al., 2024). As a signatory to the Convention on the Rights of Persons with Disabilities, the United Kingdom is obligated to support decision-making, prevent arbitrary detention, and uphold respect for physical and mental integrity (UN General Assembly, 2008; Waddington & McSherry, 2016). These obligations demand careful consideration of how coercive interventions are justified and implemented in practice. Continued use of forced medication raises legal and moral questions regarding human rights compliance with international conventions, while some view it as an unwillingness within psychiatry to relinquish epistemic authority (Johnstone et al., 2018).
From a clinical perspective, questions remain about the effectiveness of forced medication (Bauer et al., 2016). Psychotropic drugs, particularly antipsychotics, are tested in controlled conditions with consenting participants (Lally & MacCabe, 2015). In contrast, forced medication typically occurs during high-stress incidents, often following restraint or seclusion, which are profoundly different to the controlled conditions of randomised controlled trials (RCTs; Gøtzsche, 2022). These conditions introduce both physiological and psychological stress responses that may affect how medications are subjectively experienced (Bauer et al., 2016; Konstandi et al., 2014). RCTs rarely capture subjective and service user-centred outcomes, highlighting the need for pragmatic approaches to psychopharmacological research that better reflect real-world clinical practice, including coerced treatment (Chevance et al., 2022).
Coercive treatment can also generate “psychological reactance,” a response that arises when individuals feel their autonomy is threatened (Brehm & Brehm, 2013). This may manifest as protest, resistance, and disengagement from services (De Las Cuevas, 2023). In some cases, the experience of coercion may also produce nocebo effects, where negative meaning and expectations are assigned to a medication (Rief et al., 2011; Tracey, 2010). Meynen and Swaab (2011) suggest that the distress inherent in forced administration increases vulnerability to such nocebo responses. Similarly, Mintz (2011) emphasises the symbolic and emotional meaning attached to psychotropic medication, proposing that these contextual and experiential factors directly influence how drugs are subjectively processed. These interpretations remain provisional and theory-informed but point to important considerations.
There may be situations where forced medication may be required to manage acute risk to self or others, though the nature of such situations varies depending on services and individual care plans. While safeguarding individuals can at times necessitate urgent pharmacological intervention, clinicians are encouraged to prioritise the least harmful options and involve service users in decision-making wherever possible. Benzodiazepines, for instance, may provide short-term relief for agitation without the longer-term risks of antipsychotics (Gøtzsche, 2022). Evidence from Germany, where court restrictions on forced medication initially prompted staff to adopt alternative strategies and manage distress without coercion despite safety concerns, indicates that coercion-free care is possible, but when the law was later reversed, services largely reverted to previous practices (Jaeger et al., 2019). Taken together, this suggests that while forced medication may occasionally be unavoidable, it is sometimes employed to meet institutional needs rather than purely to deliver therapeutic benefit.
In attempting to understand how individuals experience and respond to forced medication, it becomes essential to engage with personal meaning-making. To explore these issues in greater depth, this review adopts the Power Threat Meaning Framework (PTMF) as its theoretical and interpretative foundation (Harper, 2022). The PTMF conceptualises psychological distress as a response to social and relational threats. It shifts the focus from diagnostic or biological determinism to the meanings individuals assign to their experiences, especially in contexts shaped by unequal power, social and personal adversity (Johnstone et al., 2018). The PTMF offers an evidence-based framework for understanding how institutional power, subjective meaning, and embodied threat responses intersect to shape lived experiences of forced medication, while also laying the groundwork for an epistemological shift. This shift moves the focus away from whether the medication “works” in a clinical sense to how it is experienced in the real-world contexts of compulsion, trauma, and resistance. In doing so, this review contributes to a more humanistic and social justice-oriented understanding of forced medication.
While several reviews have explored coercive practices more broadly, none has comprehensively focused on the subjective experience of forced medication. Existing reviews tend to rely on quantitative studies, include smaller samples of qualitative research or detract by including staff experiences (Aguilera-Serrano et al., 2018; Ford et al., 2015; Jarrett et al., 2008; Muir-Cochrane & Oster, 2021). There remains a striking absence of a comprehensive synthesis into the rich subjective experience of forced medication. Bringing together these first-person accounts not only addresses this gap but also offers a foundation for developing provisional psychopharmacological considerations that future empirical work can explore.
Aim
The current scoping review aims to synthesise qualitative research that explores how individuals experience forced psychiatric medication using the PTMF as an interpretative guide. In doing so, the review contributes to a more person-centred, ethically informed, and rights-respecting understanding of psychiatric intervention, while also aiming to generate provisional considerations and propositions regarding possible psychopharmacological responses in coercive contexts for future empirical study.
Method
Rationale for Conducting a Scoping Review
This study employed a scoping review methodology to explore how individuals subjected to forced psychiatric medication describe their subjective experiences. A scoping review was selected to accommodate the exploratory nature of the topic and the heterogeneity of relevant literature. In line with Arksey and O’Malley’s (2005) framework and enhanced by Levac et al. (2010), scoping reviews are particularly suited for mapping the extent, range, and nature of research in underdeveloped areas, such as the intersection of coercive treatment and subjective experience. This approach allows for the inclusion of diverse qualitative studies, including peer-reviewed literature and grey sources, thereby expanding the scope of understanding and identifying critical knowledge gaps. Consistent with the scope, all statements about psychopharmacology are presented as tentative inferences to guide future empirical work rather than as empirical findings.
Eligibility Criteria
Inclusion Criteria
Qualitative in methodology or containing a standalone qualitative component.
Focused on subjective, first-person experiences of forced or coerced psychiatric medication.
Published in English.
Peer-reviewed articles or doctoral theses.
Primarily inpatient and crisis settings, with community contexts included where forced or coerced medication is described.
Exclusion Criteria
Solely reported on clinical outcomes without first-person data.
Used only quantitative self-report tools without qualitative elaboration.
Papers on coercive measures that do not include forced medication experience; purely legal or ethical commentary without first-person data; treatments unrelated to psychotropic medication.
Search Strategy
A comprehensive literature search was conducted using EBSCOhost across the following databases: PsycINFO, PsycARTICLES, Academic Search Ultimate, Academic Search Complete, and the Psychological and Behavioural Sciences Collection.
Search terms included combinations of:
“Forced medication” OR “involuntary treatment” OR “coerced treatment” OR “compulsory treatment”
AND “subjective experience” OR “lived experience” OR “experience”
A time restriction was applied, limiting studies to those published between January 1, 2000 and July 15, 2025. This decision was made to reflect contemporary psychiatric practice, policy, and medication regimes. As Peters et al. (2015) note, time limits can be appropriately applied in scoping reviews when justified by shifts in clinical or social context. Older studies were excluded to maintain relevance to current coercive practices, institutional cultures, and psychopharmacological standards.
Selection Process
All identified records were imported into a citation management tool for de-duplication. Titles and abstracts were screened against the inclusion criteria. Full texts were then retrieved and assessed for eligibility. Screening and selection were conducted by the author.
Data Extraction and Synthesis
A reflexive thematic analysis, as outlined by Braun and Clarke (2021), was used to synthesise the data. While thematic analysis was applied systematically, it was employed in a descriptive and inductive manner consistent with the exploratory aims of a scoping review (Arksey & O’Malley, 2005). The process followed six iterative stages: familiarisation with the data, generation of initial codes, searching for themes, reviewing themes, defining and naming themes, and producing the report (Figure 1).
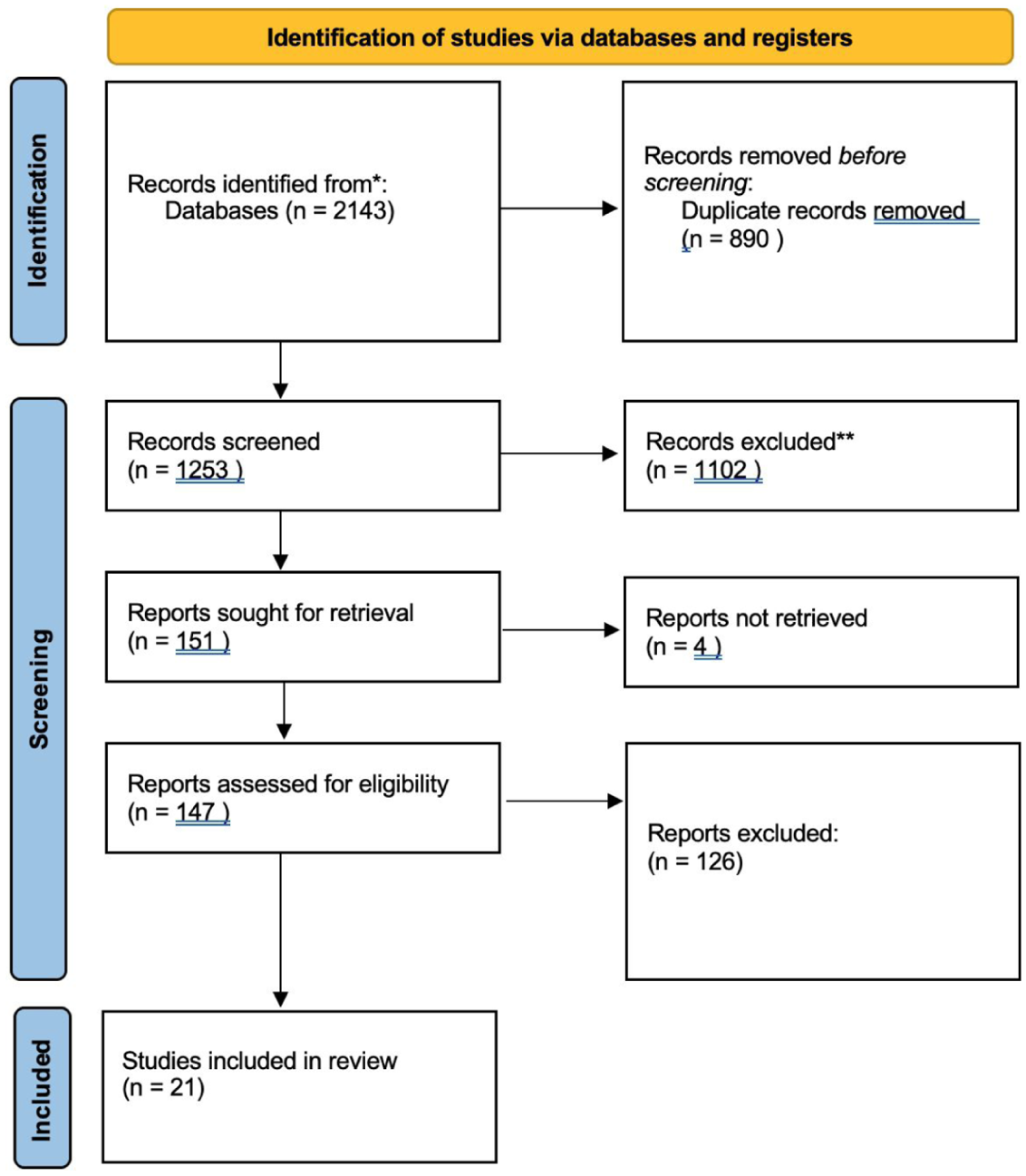
PRISMA 2020 flow diagram of study selection (Page et al., 2021).
Results
Study Characteristics
Studies employed qualitative methodologies, with semi-structured interviews being the predominant method of data collection. Two studies utilised focus groups (Mayers et al., 2010; Rose et al., 2015), one relied on written self-reports (Looi et al., 2015), and another analysed secondary data from complaints submitted to a national health board (Gøtzsche & Sørensen, 2020). The studies were primarily conducted in the United Kingdom and Sweden, though several were also based in Canada, Norway, Ireland, Austria, Switzerland, South Africa, and Denmark. Further study characteristics, including method, setting, and sample size, are detailed in Table 1.
Characteristics and Summary of Included Studies.
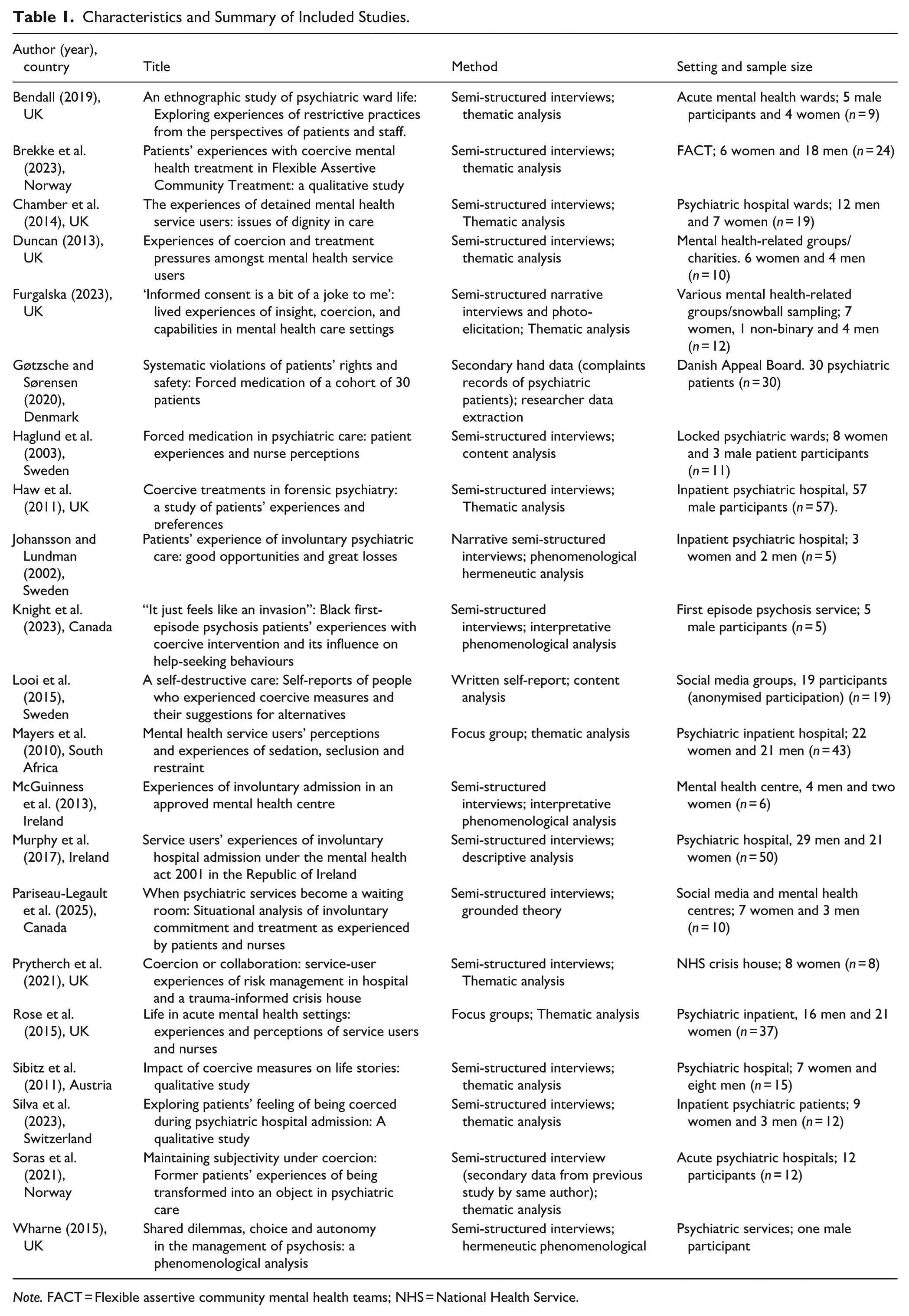
Note. FACT = Flexible assertive community mental health teams; NHS = National Health Service.
Across the 21 studies included in this review, six key themes were identified regarding the subjective experience of forced medication: The violence of forced medication, lack of communication and epistemic exclusion, from protest to survival, powerlessness, retrospective reframing and acceptance, and desire for alternatives.
Theme 1: Forced Medication as an Act of Violence
Across studies, participants described forced medication as a violent intrusion, often experienced as dehumanising, coercive, and traumatising. Terms such as “assault,” “torture,” and “violation” were used to convey the physical and psychological impact (Chambers et al., 2014; Haw et al., 2011; Prytherch et al., 2021). The administration of medication was frequently associated with staff behaving as enforcers (McGuinness et al., 2013), and in some cases, participants were retraumatised by parallels with past abuse (Duncan, 2013; Sibitz et al., 2011). The violence perceived in the administration of forced medication led many participants to describe it as feeling like being “killed,” symbolising a profound erosion of autonomy (Gøtzsche & Sørensen, 2020; Knight et al., 2023).
Beyond immediate effects, participants reported long-term consequences, including emotional blunting, fear, and a perceived erosion of identity (Brekke et al., 2023; Knight et al., 2023). Some viewed the employment of forced medication as an act to silence and suppress expression (Mayers et al., 2010). Finally, some individuals reported unwanted feelings of drowsiness, weakness, and feelings of paralysis (Haw et al., 2011).
In summary, forced medication is experienced as a tool to subdue, control and at times threaten participants to comply and promote behaviour change. The physical and psychological impact of forced medication was described as undermining, leaving participants feeling more vulnerable and, at times, more inclined to comply with the expectations of psychiatrists or nursing staff (Sibitz et al., 2011).
Theme 2: Lack of Information and Epistemic Exclusion
A recurring theme was the lack of adequate information provided before the use of forced medication, resulting in confusion and fear (Knight et al., 2023; Silva et al., 2023). Some participants expressed that they may have consented voluntarily had they been properly informed. However, others felt deliberately excluded from decision-making processes, leading to feelings of devaluation and stigma (Johansson & Lundman, 2002; Silva et al., 2023). Participants’ concerns about medication were often ignored, invalidated, and pathologised, by being attributed to “delusions,” reinforcing power asymmetries (Gøtzsche & Sørensen, 2020; McGuinness et al., 2013).
The epistemic exclusion created a sense of helplessness and insecurity in some participants as they did not know what to expect of the medication and wider coercive measures, and some believed this to be a deliberate act to limit awareness and ability to defend themselves (Johansson & Lundman, 2002; Pariseau-Legault et al., 2025).
Theme 3: From Protest to Survival
Initial reactions to forced medication frequently involved protest and anger, with individuals attempting to regain agency through verbal resistance, formal complaints, or physical expressions of defiance (Duncan, 2013; McGuinness et al., 2023; Silva et al., 2023). At times, individuals resorted to aggression as a means of reclaiming autonomy and expressing opposition to forced medication (Johansson & Lundman, 2002; Rose et al., 2015). One individual attempted to commit suicide as an act of protest against being forcefully medicated (Brekke et al., 2023). Individuals often resorted to arguments, complaints, and physical acts such as stripping to protest the use of forced medication but were met with no success (Duncan, 2013). However, such actions were frequently misinterpreted as symptoms of illness, further justifying coercion.
Feelings of resignation begin to dominate as individuals realise any sign of resistance provides justification for further acts of forced medication (Bendall, 2019; Brekke et al., 2023). Over time, many individuals adopted strategies of compliance or “performative insight” as a survival mechanism to avoid further coercive interventions and secure discharge (Furgalska, 2023).
Theme 4: Powerlessness
Forced medication was consistently linked to a profound sense of powerlessness. Participants described feeling legally entrapped and silenced, with no genuine opportunity to influence treatment decisions (Knight et al., 2023; McGuinness et al., 2013). This was exacerbated when family members endorsed forced treatment, deepening the sense of betrayal and isolation (Looi et al., 2015). Resistance was routinely medicalised, and the erosion of autonomy led to disruptions in participant’s sense of self and interpersonal trust (Duncan, 2013; Sibitz et al., 2011). Some sought empowerment post-discharge by engaging in advocacy and activism (Sørås & Snipstad, 2021).
Theme 5: Retrospective Reframing and Acceptance
Several studies reported that some individuals later reassessed these experiences with greater acceptance. Knight et al. (2023) showed a transition from confusion and disapproval to acceptance as individuals began to improve with the use of medication. McGuinness et al. (2013) also display the transition to acceptance amongst their participants as improvement occurred in self-reported wellbeing. Haglund et al. (2003) highlighted how some survivors of forced medication accepted medication voluntarily in future hospitalisations and prevented forceful administration when professionals adopted a more respectful approach. Finally, some individuals attributed their initial disapproval of forced medication due to a “lack of insight” into their “illness” and provided retrospective approval of staff actions and saw the necessity in them (Johansson & Lundman, 2002).
Theme 6: Appetite for an Alternative
Embedded within the subjective experience of receiving forced medication was the deep sediment that services and professionals relied far too heavily upon medication. Many participants expressed a strong desire for less invasive, more dialogical approaches to treatment (Haglund et al., 2003; McGuinness et al., 2013). Pariseau-Legault et al. (2025) found a desire for further dialogue with nursing staff and doctors as individuals sought to make meaning out of their experience and express their frustrations. Some individuals viewed the over reliance on forced medication as absurd due to viewing the act as unnecessary as they believed dialogue can produce an equally desirable therapeutic effect (Looi et al., 2015; Prytherch et al., 2021). Finally, individuals advocated for greater consideration of talking therapies, social approaches, and the use of crisis teams/ safe rooms to manage risk before resorting to forced medication (Chambers et al., 2014; Sibitz et al., 2011).
Discussion
This scoping review set out to map the subjective experiences of individuals who have undergone forced psychiatric medication and to consider how those experiences might inform our understanding regarding the phenomena. Across the 21 included studies, participants described forced medication as emotionally and existentially distressing, with implications for how such medications are processed and experienced psychologically. This discussion summarises the key experiential findings and interprets them through the PTMF, while also outlining provisional implications for psychopharmacology, practice, and the methodological boundaries of the review.
A dominant theme was violence and dehumanisation. Participants often described forced medication in starkly traumatic terms, where physical restraint and the imposition of psychotropic drugs ruptured bodily integrity, eroded trust in services, and undermined the perceived legitimacy of psychiatric care. These accounts align with critiques that frame coercive practices as re-enactments of social and epistemic violence (Johnstone et al., 2018; Sashidharan & Saraceno, 2017). Many individuals reported fear, loss of autonomy, and a sense of being controlled by staff. Interpreted through the PTMF, these responses can be understood as survival strategies in the face of systemic power, which operates through legal, ideological, and physical mechanisms to threaten dignity and identity. The assault on personal agency and bodily autonomy further erodes therapeutic trust and reinforces perceptions of medication as a tool of control rather than a therapeutic intervention.
Another dimension of power evident in the findings was epistemic exclusion. Many participants were not only denied informed consent but also denied recognition as experts of their own bodies and lived experience. As Silva et al. (2023) and Knight et al. (2023) describe, individuals often felt patronised, silenced, or ignored when asking questions or offering feedback about medication. These experiences reflect a structural silencing of service user voices and mirror broader critiques regarding the suppression of first-person knowledge in psychotropic drug prescribing (Duncan, 2013; Stupak & Dobroczyński, 2021). The employment of structural and ideological power by prescribers can lead to the exclusion of service users from decision-making and produce ruptures in the therapeutic alliance (Johnstone et al., 2018). In some cases, this produced negative psychological responses towards the medication and prescriber as the individual adopted internalised survival strategies and personalised meaning-making to regain agency in the form of a threat response (Johnstone et al., 2018; Mintz, 2005). This allows individuals to hold onto a sense of coherence and stability even when subjected to operations of power (Johnstone et al., 2018).
Another core theme was protest and performative survival, where individuals attempted to resist coercion through self-advocacy, performative insight, or even suicidality. These coping responses are frequently pathologised in clinical settings as symptoms of illness, thereby reinforcing the cycle of force. The PTMF offers a helpful lens here, viewing these behaviours as adaptive survival mechanisms to systems of power and threat (Johnstone et al., 2018). These survival strategies reflect an inner psychological response to oppressive power, producing threat reactions often misinterpreted as negative, when in fact they represent attempts to resist and counter harmful operations of power (De Las Cuevas, 2023; Johnstone et al., 2018). Importantly, the systemic attribution of dissent to “lack of insight” allowed professionals to override personal meaning and preferences, reducing individuals to passive recipients of care. This disempowerment fosters mistrust and resistance as various operations of power ranging from ideological, interpersonal, and legal, are enforced upon the individual (Johnstone et al., 2018). They collectively invalidate the individual’s right to refuse medication, and any such attempt is viewed as a “lack in insight” (Stupak & Dobroczyński, 2021).
Some individuals retrospectively reappraised forced medication as necessary and beneficial. This can be an indicator towards the utility of medication in fostering positive therapeutic outcomes for individuals. Yet even in these narratives, acceptance was often conditional on later recovery, improved relationships with staff, or reframing their own experience as one of “lacking insight” at the time. Such narratives reflect the complex and non-binary nature of coercion, where perceived therapeutic benefit can coexist with psychological harm and loss of trust. The PTMF views these accounts as post-hoc meaning-making strategies, in which individuals reconcile the violation of autonomy with later outcomes to restore coherence and agency (Johnstone et al., 2018). Notably, participants did not report experiencing benefit from the medication at the time of administration. Retrospective approval was often based on symptom remission, which may or may not have been causally related to the intervention. While psychiatrists often attribute improvement directly to the effects of the medication, this framing risks dismissing the individual’s subjective understanding and the broader psychosocial context in which change occurred (Gøtzsche & Sørensen, 2020).
Participants consistently expressed a preference for alternative models of care that are less coercive, more dialogical and empowering. Suggestions included psychosocial interventions, crisis houses, talking therapies, and greater relational continuity. These preferences resonate with international models such as Open Dialogue, which builds collaborative responses to crisis through shared decision-making with the individual and their network (Mackey, 2022; Seikkula et al., 2001), and Soteria houses, which delay medication in favour of supportive, relational care (D’Ambrozio et al., 2022). In Norway, medication-free treatment units have also shown that safe and effective care is possible without coercion, while increasing satisfaction and autonomy (Standal et al., 2024). These alternatives demonstrate that consensual and relational approaches to psychiatric crisis care are not only feasible but effective.
The PTMF offers a framework for services to reframe distress as a response to power and adversity, legitimising personal meaning-making and enabling the creation of validating, service user-led medication narratives that reduce reliance on externally imposed interpretations. For clinicians, this means beginning the epistemological shift toward First-person Psychopharmacology through the creation of shared narratives that prioritise asking service users how medications actually feel, exploring the symbolic and emotional meanings attached to them, and recognising the relational context in which they are administered. As Stupak and Dobroczyński (2021) note, psychotropics are better understood as psychoactive substances whose effects are shaped by subjective experience rather than solely as symptom-targeting drugs. This orientation encourages shared decision-making, reduces epistemic exclusion, and promotes therapeutic trust.
Finally, these findings highlight the growing ethical and legal tensions surrounding forced psychiatric treatment. Coercive medication increasingly conflicts with the principles of the Convention on the Rights of Persons with Disabilities, which emphasises autonomy, bodily integrity, and non-discrimination (UN General Assembly, 2008; Waddington & McSherry, 2016). As Evans et al. (2024) note, coercion can undermine therapeutic relationships and risks retraumatising those already in crisis. Although legal systems based on substituted decision-making do safeguard individuals, they often also silence the most vulnerable and can perpetuate structural injustice (Johnstone et al., 2018). Psychiatric advance directives represent one constructive alternative, enabling people to express treatment preferences in advance, reduce the use of coercion, and preserve agency during periods of acute distress (Amering et al., 2005; Johnstone et al., 2018). This would align psychiatry with its ethical obligations and help transform care from something imposed onto individuals into something co-created with them.
Provisional Psychopharmacological Considerations
As this review synthesises qualitative accounts regarding the experience of forced medication, it cannot establish the direct and clear consequences related to the psychopharmacological response’s individuals may undergo. The inferences below are provisional and offered to articulate plausible pathways by which the lived context of coercion may shape how psychotropic drugs are felt and evaluated, and to outline testable propositions for future empirical work.
The use of coercive power and force threatens bodily autonomy and may activate stress responses that alter neurotransmitter levels and liver enzyme activity, thereby affecting medication metabolism (Konstandi et al., 2014; Mora et al., 2012). These conditions differ markedly from RCTs that typically involve informed consent and low-arousal sterile settings, which limit the direct translation of trial findings to coercive contexts (Bauer et al., 2016). In such high-stress circumstances, altered pharmacokinetics and pharmacodynamics may yield effects that deviate from a drug’s intended profile.
Participants’ accounts of heightened sensitivity to adverse effects align with nocebo phenomena, where negative expectations and threat appraisals intensify side effects or diminish perceived benefit, partly via dopaminergic deactivation and related expectancy pathways (Meynen & Swaab, 2011; Rief et al., 2011; Tracey, 2010). These expectancy-driven effects are rarely considered in routine prescribing decisions, yet they are integral to understanding how context and meaning shape medication outcomes.
Negative emotional states reported in the included studies, such as fear, humiliation, and shame, may further skew subjective drug experiences, amplifying the perception of adverse effects (Mintz, 2002; Silke et al., 2014). In parallel, psychological reactance to perceived loss of autonomy can foster resistance and nonadherence, which in turn inhibits subjective integration of psychotropic drugs over time (Brehm & Brehm, 2013; De Las Cuevas, 2023). This disempowerment may itself alter how psychotropic medications are felt, evaluated, and incorporated into an individual’s narrative, contributing to a sustained adverse psychopharmacological appraisal.
Future Directions
Taken together, these signals suggest that forceful administration interacts with bodily stress and meaning-making in ways that may systematically shape psychopharmacological response. To evaluate these propositions, future studies should compare forced, coerced, and voluntary administration, embed trials in real-world settings with broad inclusion, prioritise service user-important outcomes (e.g. emotional responses, agency, withdrawal), and use pragmatic clinical trial (PCT) designs (Chevance et al., 2022). PCTs can illuminate how psychopharmacology unfolds, offering insights that conventional RCTs cannot provide by evaluating forced medication in real-world clinical settings. The use of qualitative methodologies can also deepen understanding by capturing lived experiences, subjective drug effects, and symbolic meanings, thereby complementing quantitative data. Integrating these approaches would generate more person-centred, clinically relevant, and ethically informed evidence to guide practice.
Limitations
This review is, to our knowledge, the first to bring together qualitative first-person accounts of forced medication. A scoping approach was well-suited to a fragmented field and enabled inclusion of diverse study types across countries and settings.
Several constraints should be noted. Included studies were heterogeneous and often examined coercion more broadly than forced medication while typically using small samples concentrated in Europe, which limits transferability. Only English language reports were included, and so other relevant studies may have been missed. As is common in scoping work, no formal quality appraisal was undertaken, and screening plus extraction was completed by a single reviewer, which may introduce bias. Jurisdictional differences in law and service models reduce comparability. Given the limited scope of this review, it cannot establish psychopharmacological effects but can only suggest tentative possibilities that warrant further investigation.
Conclusion
This review shows that forced psychiatric medication is frequently experienced as an act of institutional violence, producing psychological distress, damaging therapeutic relationships, and shaping individual reactions towards medications. The PTMF illuminates these experiences as coherent responses to power, threat, and meaning-making, shifting attention away from narrow biomedical framings. These insights challenge psychiatry’s prevailing focus on symptom reduction and instead call for trauma-informed, rights-based, and relational approaches to care. First-person psychopharmacology offers a way forward by centring lived experience and exploring not only whether drugs achieve clinical effects but how they are embodied and interpreted. Reconceptualising psychotropics as psychoactive substances rather than purely biological correctives may support more cautious, intentional, and person-led use (Stupak & Dobroczyński, 2021). Future research must engage directly with subjective experiences of medication, combining in-depth qualitative methods with pragmatic clinical trials to produce evidence that is clinically meaningful, and reflective of real-world practice.
Footnotes
Acknowledgements
In the name of Allah, the Beneficent, the Merciful. All praise belongs to the Beloved for granting me the opportunity to undertake and complete this project as part of my spiritual endeavours to serve His creation. I also wish to express my deepest gratitude to my fellow trainee counselling psychologist, Marie Hayes Vigerust, whose wisdom, generous insights, and thoughtful conversations were instrumental in bringing this manuscript to completion.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.