
Abstract
The current article aims to investigate the effects of pandemics of varying severity on death-thought accessibility in two studies while controlling for health anxiety. Study 1 (n = 203) examined the effect of standard mortality salience (MS), severe pandemic, mild pandemic, and dental conditions on death-thought accessibility as assessed by the death word fragment task (DWFT). Study 1 did not find significant effects of MS and delay on death-thought accessibility, which could be attributable to the less-sensitive nature of the DWFT. Thus, Study 2 (n = 163) was conducted with more sensitive death-thought accessibility measures. Results from Study 2 found that response time toward death and positive words on the lexical-decision task was significantly faster than in standard MS and dental conditions. Both studies recruited predominantly Americans (Study 1) and Europeans (Study 2), which limits the generalizability of the results to other populations. Future studies can consider replicating the studies in other populations.
Introduction
Critical incidents, such as terrorist attacks and pandemics, have demonstrated MS effects on attitudes and behaviors (Arrowood et al., 2017; Das et al., 2009; Maki et al., 2019). These studies on critical incidents have consistently maintained that exposure to life-threatening events such as pandemics, natural hazards, terrorist attacks, and wars has led to the activation of the tripartite anxiety buffers (i.e., worldview defense, self-esteem enhancement, and seeking close relationships) of the terror management theory (TMT) (Plusnin et al., 2018). While TMT research regarding MS effects of pandemics is growing, there are a few research gaps that need to be addressed. First, very few TMT studies exploring MS effects of pandemics have also examined the role and the presence of death cognitions (Arrowood et al., 2017; Goodwin et al., 2011; Hu et al., 2020). Also, no studies have investigated the MS effects of pandemics of varying severity (Leung et al., 2022). As highlighted in crisis management resources (Pfeifer & Roman, 2016; Sapriel, 2003), different critical incidents’ severity may require varying levels of intervention. Thus, it will be helpful to examine whether MS effects of pandemics will change according to severity, which would have downstream impact on resource utilization. Finally, pandemics, being a health-related incident, could have triggered health anxiety, which has been hypothesized to trigger responses similar to those observed in TMT (Taylor, 2019). This overlap between health and death anxiety will need to be examined to clarify the unique MS effects of pandemics. Hence, this study hopes to address these gaps by investigating the effects of pandemics of varying severity on death-thought accessibilities.
TMT
TMT proposes that individuals recognize that their lives are finite, which triggers death-thought accessibility, and in turn anxiety. To cope with this anxiety arising from a salience of one’s mortality, individuals seek ways to reduce death thoughts by extending their mortality in symbolic ways; in particular, by defending their worldview, enhancing self-esteem, and/or seeking close relationships (Plusnin et al., 2018).
When reminded about their mortality, the dual process system would be activated to guide individual responses depending on whether death thoughts are within or outside of focal attention (Kosloff et al., 2019). This dual process system suggests that if death thoughts are in the forefront of individuals’ awareness, individuals are more likely to actively suppress these death thoughts to regulate the triggered anxiety. Nonetheless, when death thoughts recede into the background after a time delay and are less prominent in the individual’s awareness, these previously suppressed death thoughts would rebound, making death thoughts more accessible and triggering the tripartite anxiety buffers (Steinman & Updegraff, 2015). Hence, in many TMT studies, death-thought accessibility tends to increase significantly after a time delay when death thoughts rebound as individuals stopped the active suppression of death thoughts (Hayes et al., 2010; Steinman & Updegraff, 2015).
There had been some studies suggesting that death thoughts appeared immediately following death reminders and weakened with time delay (Trafimow & Hughes, 2012). In a series of five experiments, Trafimow and Hughes (2012) consistently found that death-thought accessibility was elevated on the DWFT or the lexical-decision task immediately after death reminders. The effect of the delay was absent despite various manipulations of the lengths of delay. In their final experiment, the authors instructed participants to consciously avoid thinking about death in an attempt to mimic death-thought suppression/delay rebound effect. Instead of the established delayed TMT effects on death-thought accessibility, the authors found that the death-thought accessibility was significantly higher in the suppression condition, which asked participants to consciously track and avoid death thoughts whenever they arise, thus disconfirming the thought suppression/delay rebound effect. Nevertheless, these studies had not been replicated at the time of writing and research indicating a delayed rebound of death-thought accessibility has been more robust and well-documented (Hayes et al., 2010; Steinman & Updegraff, 2015).
To alleviate the death thoughts arising from death reminders, individuals would defend their worldview, enhance self-esteem, and seek close relationships to reduce death-thought accessibility. These pathways, also known as the tripartite anxiety buffers, have been widely researched and established (Rosenblatt et al., 1989; Tam et al., 2007). For instance, as compared to control groups, individuals who were asked to write about their personal deaths were more likely to provide less resources (Tam et al., 2007) or mete out harsher punishment (Rosenblatt et al., 1989) to those who represent or uphold a different worldview from themselves. They are also more likely to bolster their self-esteem following reminders of death by buying items that are endorsed by celebrities (Arndt et al., 2004) or seeking out interpersonal intimacy (Birnbaum et al., 2011; Lam et al., 2009; Mikulincer et al., 2003). Other studies have shown that death reminders act through death thoughts to trigger these tripartite anxiety buffers (Vail et al., 2012). When being reminded of death through pictures of buildings destroyed by war or natural disasters, Vail et al. (2012) found that individuals reported higher death thoughts and showed more intensified support for their political orientation as compared to those in control conditions. These death reminders, also known as MS, are likely to trigger death anxiety and consequently activate the tripartite anxiety buffers (Plusnin et al., 2018).
MS Effects of Pandemics
Over the years, infectious diseases and pandemics have led to numerous fatalities (Saunders-Hastings & Krewski, 2016). The Spanish flu, which occurred in 1918, killed at least 50 million worldwide. Between 2014 and 2016, Ebola had accumulated more than 11,000 deaths in Guinea, Liberia, and Sierra Leone. The ongoing coronavirus 2019 (COVID-19) pandemic has caused close to seven million deaths worldwide since December 2019 (John Hopkins University, 2023). This association with deaths insinuates the ability of pandemics to trigger MS.
Indeed, terror management studies have utilized pandemics as MS inductions. Ebola, swine flu, and COVID-19 have been studied as a form of death reminder in TMT studies (Arrowood et al., 2017; Bélanger et al., 2013; Goodwin et al., 2011; Jutzi et al., 2020). For instance, Arrowood et al. (2017) conducted two studies to investigate the MS effects of Ebola virus on death cognitions and adherence to religious teachings. Participants were instructed to pen down thoughts and feelings of contracting Ebola virus before completing the word fragment task, which assessed death thoughts, and the religious fundamentalism scale. Both studies found that the Ebola condition yielded significantly more death-related words than the control condition. The death cognitions also mediated the relationship between Ebola salience and individuals’ commitment to religious teachings, indicating the process through which death reminders trigger worldview defense.
Similar patterns of the MS effect on death cognitions were observed in TMT studies using swine flu. Bélanger et al. (2013) and Goodwin et al. (2011) both reported elevated death-related thoughts when their participants were being reminded of the swine flu such as writing significantly more death-related words after reading about contracting swine flu or thinking about their deaths more frequently since the swine flu outbreak.
More recently, researchers have begun investigating the MS effects of COVID-19. Some assessed the MS effects of COVID-19 by collecting data during the COVID-19 peak periods (Tomaszek & Muchacka-Cymerman, 2020; Wong & Yang, 2020) while others have tried to induce MS by asking participants to rate their perceived threat of COVID-19 (Nanni & Ulqinaku, 2021; Song et al., 2020). Su and Shen (2020) induced MS by asking participants to consider the chances of someone contracting COVID-19 in their community. They found that those who perceived a higher likelihood of infection in their community showed more support for a nationalistic policy (i.e., international travel ban). Jutzi et al. (2020) also found MS effects on ingroup bias, an example of worldview defense, when they manipulated the COVID-19 threat. Specifically, when participants were led to believe that COVID-19 was incurable, they exhibited more ingroup bias than those in the control group. Individuals also behaved in ways which boosted their self-esteem in the face of COVID-19 threats. For instance, individuals who perceived technology as central to their self-esteem were more accepting toward virtual tours of museums (Nanni & Ulqinaku, 2021) when the perceived COVID-19 threat was high. This evidence converged to highlight the MS effects of pandemics on worldview defense and self-esteem enhancement.
Studies have also found MS effects of pandemics on death-thought accessibility (Arrowood et al., 2017; Grover et al., 2010). To explore the MS effects of the AIDS pandemic, Grover et al. (2010) compared number of death-related words completed in a word fragment task by participants randomized to the standard MS (i.e., thinking about death in general), AIDS, or dental pain conditions. They found that both standard MS and AIDS conditions yielded significantly more death words, and hence higher death-thought accessibility, than the dental pain control condition. Arrowood et al. (2017) also assessed significantly higher death-thought accessibility in the Ebola condition than the control condition. These results demonstrated that pandemic situations had similar MS effects as thinking about death in general and both heightened death-thought accessibility significantly than control conditions.
Anxieties During Pandemics
Pandemics like COVID-19 have triggered elevated levels of psychological distress, such as depression and anxiety. In a nationwide study assessing anxiety, depression, avoidant and compulsive behaviors, and physical symptoms during COVID-19, Qiu et al. (2020) found that 35% of their 52,000 samples reported significant psychological distress. In the United States, Twenge and Joiner (2020) found that as compared to the National Health Interview Survey conducted in 2018, American adults were at least three to eight times more likely to meet criteria for severe mental distress, as represented by depressive and anxiety symptoms, when surveyed during the COVID-19 pandemic. This pattern of heightened psychological distress during COVID-19 was evident across the world (Bäuerle et al., 2020; Bigot et al., 2021; Özdin & Bayrak Özdin, 2020; Vahedian-Azimi et al., 2020), reflecting the increased fear and anxieties during pandemics and their possible relationships to health behaviors in pandemics.
Other studies have examined the relationship between psychological distress and health behaviors in pandemics. For instance, researchers have reported that state anxiety predicted handwashing behaviors, but not adherence to social-distancing measures, in Koreans during the swine flu pandemic (Kim et al., 2011). Others have found health anxiety was related to higher frequency of handwashing, better indoor ventilation, and more frequent disinfection of households during COVID-19 (Ko et al., 2020).
The COVID-19 pandemic, being a health-related scenario, could have triggered a health anxiety-related response other than TMT responses. From a health anxiety perspective, individuals are more likely to misinterpret bodily symptoms as disease, triggering anxiety, which eventually can lead to behaviors such as seeking medical attention and adherence to infection control measures. It was also suggested that individuals who breached social-distancing measures could be low in health anxiety, held an “unrealistic optimism bias,” where individuals felt that they would not contract the disease, or probably coped with stressful events, such as a prolonged crisis like a pandemic, by seeking social closeness (Taylor, 2019). Extrapolating evidence related to health anxiety, Taylor (2019) and Asmundson and Taylor (2020a, 2020b) hypothesized that people adopted many of the health behaviors observed in the COVID-19 pandemic, such as stockpiling, more adherence to infection control measures and xenophobic sentiments as a means to protect and maintain good health, thereby alleviating health anxiety. Coincidentally, these behaviors were also similar to those observed in TMT (Courtney et al., 2020; Pyszczynski et al., 2021).
Health Anxiety and TMT
These responses triggered by health anxiety were similar to the defenses depicted in the TMT. As illustrated by Courtney et al. (2020) and Pyszczynski et al. (2021), health-related behaviors could also be appreciated through the lens of TMT. Specifically, these responses serve as defense mechanisms to regulate anxiety arising from an innate need for self-preservation in the face of death threats (i.e., pandemics). Thus, one major difference between the two approaches is the individual’s preoccupation. In TMT, preoccupation with death thoughts has been shown to mediate the relationship between death threat with behavioral and attitudinal outcomes such as adherence to religious practices and political preferences (Arrowood et al., 2017; Vail et al., 2012). Alternatively, individuals with health anxiety could be preoccupied with health or other catastrophic consequences of illnesses such as physical suffering, loss of mobility, and enjoyment in life (Salkovskis et al., 2002).
Hu et al. (2020) examined the relationship between COVID-19 threat and anxiety. They found that perceived COVID-19 threat was related to general anxiety and death anxiety, suggesting that COVID-19 could bring about TMT-related outcomes. Tomaszek and Muchacka-Cymerman (2020) found that individuals’ post-traumatic stress symptoms were related to their existential anxiety during the peak of COVID-19. Further analysis in their study concluded that existential anxiety mediated the relationship between COVID-19 and post-traumatic stress disorder symptoms. On the contrary, Ko et al. (2020) and Bigot et al. (2021) examined the relationships between worries and health anxieties during COVID-19, and their relationship to health behaviors. These suggested that the COVID-19 pandemic also triggered health anxiety, which motivated behaviors which overlapped with the defenses of TMT. Therefore, this study controls for health anxiety, to isolate the effects of death anxiety in pandemics (Arrowood et al., 2017; Goodwin et al., 2011; Hu et al., 2020).
Addressing Research Gaps
Despite evidence pointing to the MS effects of pandemics, several research gaps still exist. First, although most studies have shown that pandemics trigger worldview defense and self-esteem enhancement (Jutzi et al., 2020; Nanni & Ulqinaku, 2021), few have assessed death-related cognitions, an important component of TMT (Leung et al., 2022). As Hayes et al. (2010) pointed out, unconscious preoccupation with death, which triggers death anxiety, forms the basis of TMT. These implicit death thoughts could be assessed through measures such as word fragments and implicit attitude tests (Naidu et al., 2020; Vail et al., 2012). Indeed, some studies have observed increased death cognitions in standard MS and Critical Incident (CI) conditions (Fairlamb & Cinnirella, 2020; Suzuki et al., 2022), but others have not been able to replicate these findings (Dewa et al., 2014; Luke & Hartwig, 2014; Lyall & Thorsteinsson, 2007). Furthermore, these studies were conducted in the context of terrorism and wars, and not specific to pandemics. Thus, there is a need to investigate the relationship between pandemics and death cognitions.
Another research gap to be examined would be the MS effects of pandemic conditions of varying severity. Although some studies have explored a specific pandemic (e.g., swine flu and COVID-19), they have not compared the MS effects of CIs of varying severity. As far as the current researchers are aware, MS effects of pandemics of varying severity have not been the focus of studies to date. The differentiation between the varying severity might refine crisis responses and maximize utility of resources for intervention. As recommended in crisis management guidelines, tiered responses based on severity and the nature of CIs will help to deploy resources in an efficient and effective manner (Pfeifer & Roman, 2016; Sapriel, 2003). Thus, exploring the MS effects and designing interventions based on these differences would ensure timely deployment and utilization of resources.
Finally, the pandemic, being a health-related critical incident, could have triggered health anxiety, which in turn triggered behaviors observed in pandemics (Asmundson & Taylor, 2020a). However, these behaviors could also be a product of the death anxiety triggered by the infectious nature and fatalities of COVID-19. To isolate the MS effects of the pandemic, it will be important to acknowledge and control the potential contribution of health anxiety.
Thus, Study 1 aims to address these research gaps. In summary, this study hypothesizes that the severe pandemic condition and the standard MS condition will yield significantly higher levels of death cognitions than the mild pandemic and dental conditions after a time delay and will continue to do so when controlled for health anxiety.
Study 1 Method
Participants
An a priori power analysis for a two-way analysis of variance (ANOVA) with medium effect size of 0.25 (Steinman & Updegraff, 2015, α = .05, 1–β = .8) revealed that a minimum of 179 participants would be required for a sufficiently-powered test. Five hundred and fourteen full data sets were collected, out of which 63 participants indicated they were below 18 years and hence not allowed to participate in the study while 2 eventually decided to decline participation. Another 246 participants responded with excerpts extracted verbatim from online sources, keyed in only single-word answers to the essay questions, or demonstrated response sets and were thus excluded from the study. This leaves a final sample size of 203. The average time taken to complete the survey was approximately 16 min.
Most of the participants were from the United States (73.4%) while the rest were from India, Brazil, and other countries (e.g., Kenya and England). Their age ranged from 19 to 64 years (M = 35.9 years, standard deviation (SD) = 10.34). The majority of the participants received at least two doses of vaccination (47.8%) and had personal experience with COVID-19 (58.6%; i.e., personally or had relatives who had contracted COVID-19 or quarantined due to COVID-19).
Materials
Short Health Anxiety Inventory
The Short Health Anxiety Inventory (SHAI) consists of 18 items assessing individuals’ symptoms of health anxiety (hypochondriasis) and their attitudes as to how unpleasant it would be if they were to develop a particular illness (Salkovskis et al., 2002). Four statements of varying levels of health anxiety would be presented within each item. For instance, when asked about general worries about health, the statements were “I do not worry about my health”; “I occasionally worry about my health”; “I spend much of my time worrying about my health”; and “I spend most of my time worrying about my health.” Respondents were instructed to choose one of these four options which reflected their level of health anxiety. The items are rated on a Likert-type scale of 0 to 3 with higher ratings indicating higher anxieties. Items 1 to 14 assessed an individual’s level of health anxiety with total scores ranging from 0 to 52. Items 15 to 18 assessed an individual’s attitude toward the negative consequences of developing a severe illness. The total scores ranged from 0 to 12. Salkovskis et al. (2002) reported that the SHAI converged with a two-factor solution through confirmatory factor analysis with a health anxiety factor and a negative consequence factor. The Cronbach αs were .92 for health anxiety and .79 for the attitudes toward negative consequences of developing severe illnesses subscale for this study.
MS Manipulation
Participants were asked to pen down their thoughts and feelings about either (a) their own death (standard MS condition), (b) contracting a severe and highly transmissible flu virus (severe pandemic condition), (c) contracting a mild and low transmissible flu virus (mild pandemic condition), or (d) dental pain (control condition). Those who were assigned to the pandemic conditions were instructed to read the following passage before responding to the two questions: The World Health Organization (WHO) has recently announced the discovery of a new flu virus. Based on the analysis of the epidemiological data over the last three months from countries with cases, WHO and pandemic experts have classified this virus to be highly contagious with severe symptoms (severe pandemic condition) / not contagious with mild symptoms (mild pandemic condition). Frontline observations (i.e., General Practitioners, Hospitals) reported that the hospitalization rate for infected cases is as high as 10% (1,000 in 10,000 people) and fatality rate stands at a high rate of 1% (100 in 10,000 people) (severe pandemic condition) / as low as 0.5% (50 in 10,000 people) and fatality rate stands at a low rate of 0.02% (2 in 10,000 people) (mild pandemic condition) for those who contracted the virus.
They were then asked to respond to the following “Please briefly describe the emotions and possible consequences that the thought of contracting this new flu arouses in you” and “Jot down, as specifically as you can, what you think will happen to you physically get the new flu and once you have physically gotten the new flu.” Previous research on diseases has shown that asking individuals to reflect on their thoughts, feelings, and physical conditions if they were to contract the disease would be sufficient to heighten death thoughts (Arrowood et al., 2017; Bélanger et al., 2013).
Positive and Negative Affect Schedule—Expanded Form (PANAS-X)
Participants were then asked to rate their present feelings and emotions on the PANAS-X (Watson & Clark, 1999). The scale comprises of 30 positive and 30 negative emotions. The PANAS-X has been shown to have two higher-order factors of positive (e.g., cheerful) and negative affect (e.g., sad). Participants rate their emotions on a scale of 1 (very slightly or not at all) to 5 (extremely). Items making up the positive and negative affect scales were summed together. Higher scores suggest higher levels of positive and negative affects. Scores ranged from 10 to 50 for the higher-order factors of positive and negative. The PANAS-X assesses the emotions the participants are feeling after completing the essays on the MS inductions. The Cronbach αs for positive and negative affects in this study are .91 and .95, respectively.
DWFT
The DWFT consists of 25 incomplete word stems which were used to access death-related thoughts. Out of the 25-word stems, six can be completed with a neutral or death-related word. For example, the word stem “DE _ _” can be completed as either “DEAD” (death-related word) or “DEED” (neutral word). Participants complete the task by filling letters in the blanks to create words that first come to their mind. The more death-related words completed, the higher the death-thought accessibility. This measure was selected as it was one of the common tools to assess for death-thought accessibility in TMT studies (Hayes et al., 2010; Naidu et al., 2020).
Procedures
A 4 (IV 1: standard MS vs. severe pandemic vs. mild pandemic vs. dental pain) × 2 (IV 2: delay vs. no-delay) between-subjects design was used with death-thought accessibility as the dependent variable (DV). Participants were informed that they would be participating in a survey ostensibly about personality, health beliefs, and emotions, which would take about 30 min. The survey was hosted on Qualtrics, and the Qualtrics link was placed on the mTurk platform.
Informed consent was taken through participants’ declaration if they consent to take part in the study and if they were 18 years and above. After indicating their consent, participants began the survey by responding to the SHAI, before being randomly assigned to one of the four MS conditions. Participants were then randomized to the delay or no-delay group. For those assigned to the delay group, they rated their emotions on the PANAS-X and completed a filler task related to a short story. They then completed the 25-word stem-dependent measure. Those in the nondelay condition completed the 25-word stem immediately after responding to the MS questions. They then proceeded to complete the PANAS-X. All participants ended the survey by filling in a demographic form.
Based on the manipulation checks conducted after the questionnaires, none of the participants were aware of the true purpose of the study. They were then presented with a list of mental health resources if they felt uncomfortable after having participated in the survey. After completing the survey, participants were given USD$1.50 on the mTurk platform. This procedure was approved by the university’s institutional review board (IRB) (Approval number: H8295).
Study 1 Results
The data were analyzed using Ststical Package for Social Sciences (SPSS) Version 22 with the alpha level set at .05. In accordance with standard MS studies, the effect of MS on negative affect was examined to assess whether the MS effects are due to unique death concerns rather than negative affect. A 4 × 2 between-subjects ANOVA was conducted to assess the effects of MS on negative affect on the PANAS-X. Results showed that MS, F(3,195) = .611, p = .61, and delay, F(1,195) = .075, p =.79, did not have a significant effect on negative affect. There was no significant interaction effect of MS and delay on negative affect, F(3,195) = .86, p = .46.
To test the hypothesis, a 4 × 2 between-subjects analysis of covariance (ANCOVA) was performed to examine the effects of MS and delay on death-thought accessibility while controlling for health anxiety. Results did not find significant effects of MS, F(3,193) = 1.03, p = .38, and delay, F(1,193) = .04, p = .84, on death-thought accessibility when controlling for health anxiety. The interaction effect of MS and delay, after controlling for health anxiety, was also not significant on death-thought accessibility, F(3,193) = .68, p = .57. No significant main effect of nationality was yielded when nationality was included into the analysis. This indicates that familiarity with English based on nationality was not related to the number of death words generated. The means and SDs for the DWFT are shown in Table 1.
Means and Standard Deviations of Words Completed on the DWFT.
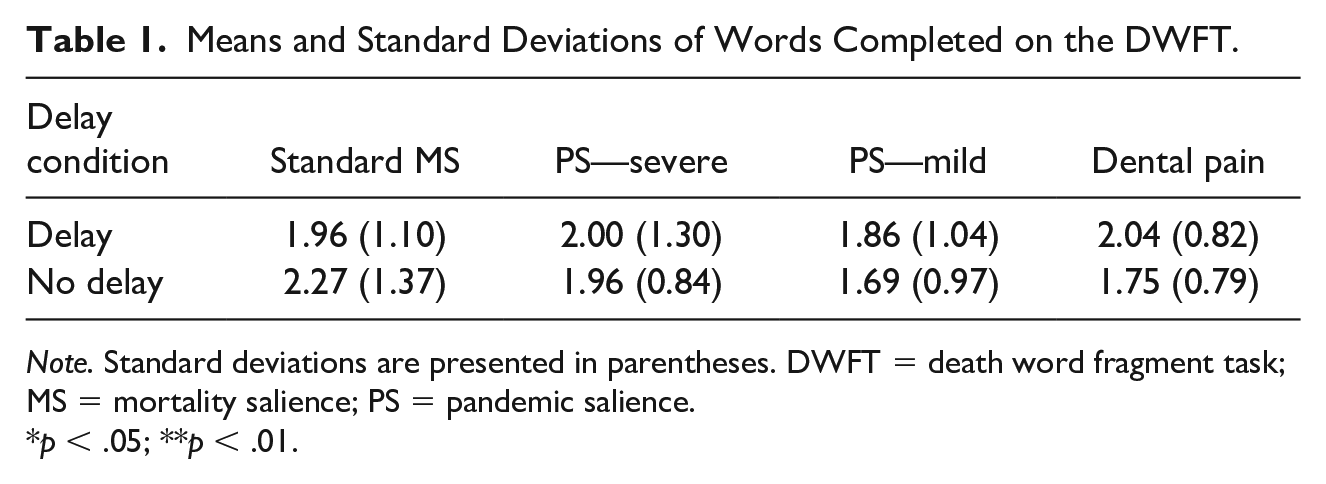
Note. Standard deviations are presented in parentheses. DWFT = death word fragment task; MS = mortality salience; PS = pandemic salience.
p < .05; **p < .01.
Study 1 Discussion
Study 1 set out to investigate the MS effects of varying pandemic conditions on death cognitions and to isolate the effects of MS on death-thought accessibility while controlling for health anxiety. However, there were no significant differences in death-thought accessibility between standard MS, severe or mild pandemic and control conditions, and between delay and no-delay conditions, even when controlling for health anxiety. Hence, our hypothesis was not supported.
These findings were inconsistent with previous studies that have found robust MS and delay effects on death-thought accessibility (Hayes et al., 2010; Steinman & Updegraff, 2015). The nonsignificant results could be accounted for by five reasons. First, the presentation of the health anxiety inventory prior to the test conditions could have primed participants of death thoughts. Although unlike typical Death Anxiety Scales (DASs) which make explicit references to death, the health anxiety inventory did assess individuals’ attitudes toward severe illnesses, which would have implicitly triggered associations with death and consequently death thoughts (Steinman & Updegraff, 2015). When death reminders were indirect, individuals were less likely to engage in active suppression of death thoughts to self-preserve. Instead, death thoughts would hover subtly in their awareness and time delay would not be required before the death thoughts became accessible (Steinman & Updegraff, 2015). Nevertheless, if the health anxiety inventory had acted as a subtle death reminder, the current results would have found significantly higher death-thought accessibility in the no-delay conditions. This was not the case, which suggests that the likelihood of SHAI triggering death-thought accessibility was low.
Another potential explanation for the lack of evidence for death cognitions in critical incident salience condition (i.e., pandemic condition) could be related to the severity of the conditions prepared. If a critical incident condition was mild and did not trigger a life-threatening perception, it might not trigger death cognitions. When examining the effects of COVID-19, Hu et al. (2020) found that it was the perceived threat of COVID-19, rather than the objective fatality and infection information of COVID-19, which was related to MS effects. When reviewing some of the responses in the high-severity pandemic condition, some participants reported that they were not concerned about being infected and believed that practicing infection control measures would protect them from the flu virus. Stated differently, the practice of infection control strategies, which are consistent with proximal defense (i.e., health-oriented behaviors) in the terror management health model (TMHM), could have allayed some of the death anxiety which was triggered by the exposure to the pandemic conditions. In addition, the pandemic conditions employed in this study had been pretested and had shown a significant difference in the perceived threat triggered by the conditions.
A third possibility could be due to the immersion in the year-long COVID-19 pandemic. The COVID-19 pandemic could have heightened death cognitions and psychological distress in individuals more than the 2 to 3 years. As highlighted by Courtney et al. (2020) and Pyszczynski et al. (2021), individuals had responded in accordance with the TMT and TMHM during COVID-19, suggesting heightened death cognitions. Other studies have also shown elevated levels of general and death anxiety during COVID-19 (Bigot et al., 2021; Shakil et al., 2020). Being immersed in the pandemic could have already triggered and maintained the anxiety, obscuring the MS effects being explored in this study.
A previous study exploring the MS effects of critical incident had not been able to find MS effects of terrorism, as the community had just gone through a recent terrorist attack (Lyall & Thorsteinsson, 2007). The authors postulated that the experience of a recent terrorist attack had elevated death cognitions in their sample, thus masking the MS effects of their studies. While terrorist attacks are relatively time limited, other studies examining longer term critical incidents such as wars have also reported similar patterns in their findings (Ginzburg et al., 2010; Llabre & Hadi, 2009). Longitudinal studies have revealed that soldiers’ depressive, anxiety, and post-traumatic stress disorder symptoms stayed elevated more than 20 years of war (Ginzburg et al., 2010). These negative effects continued to have postwar adverse effects on individual health such as poor sleep quality and obesity, suggesting the long-lasting effects of critical incidents (Llabre & Hadi, 2009). Research examining the effects of natural disasters has also shown that survivors continued to experience elevated levels of distress as compared to controls 4 years post disaster (Van Den Berg et al., 2008). These seemed to indicate that even if the critical incidents are over, their effects could have a long-lasting impact post incident, which could have attenuated the MS effects, let alone a prolonged critical incident like the COVID-19 pandemic.
A fourth explanation is the limited sensitivity of the DWFT. The utility of the word stem had been tested and compared with other measures of death-thought accessibility. Although widely used in TMT, a recent study by Naidu et al. (2020) found that the DWFT had not been able to distinguish between MS conditions. Rather, other implicit measures, such as the lexical-decision task, dot-probe task, and ambiguous inkblot pictures, demonstrated higher sensitivity to differentiate the conditions. The DWFT might not have been sufficiently sensitive in this instance and had not captured the death cognitions to distinguish the MS conditions despite its prevalence and success in detecting death-thought accessibility in other TMT studies.
Finally, the nonsignificant results could also indicate a failure to replicate the MS effects. While TMT has shown robust evidence that supports the relationship between MS and death cognitions (Greenberg et al., 1994; Hayes et al., 2010), some studies had not been able to replicate MS effects (Haaf et al., 2020; Lyall & Thorsteinsson, 2007; Sætrevik & Sjåstad, 2022; Ullrich & Cohrs, 2007). In view of these issues, a replication study in the form of Study 2 is required.
Study 2
Data collection for Study 2 was conducted between December 2021 to February 2022, during which COVID-19 continued to ravage the world. By then, the global population had been immersed in COVID-19 for at least 2 years and different governments continued to relax and tighten the COVID-19 infection control measures based on the evolving situation. The study design is the same as Study 1, except for the removal of the mild pandemic condition and a change of DVs to assess death-thought accessibility. The mild pandemic condition was removed as it did not trigger significant perception of threats in our pilot study and there were no significant effects of mild pandemic condition on death-thought accessibility in Study 1. The DWFT was replaced with the DAS, lexical-decision task, and the dot-probe task. These DVs were selected as they had been used to assess death-thought accessibility in TMT studies (Arndt et al., 2007; Vail et al., 2012). Also, as reported by Naidu et al. (2020), the lexical-decision task and dot-probe task were more sensitive measures of death thought accessibility (DTA)as compared to the DWFT. Permission was obtained from Naidu et al. (2020) to use the same stimuli for the lexical-decision task and dot-probe task.
Similar to Study 1, Study 2 hypothesizes that the pandemic condition and the standard MS condition will yield significantly higher levels of death cognitions than the control condition after a time delay, while controlling for health anxiety. Study 2 was preregistered with Open Science Framework (OSF) Registries (Registration DOI: 10.17605/OSF.IO/4SD2J).
Study 2 Method
Participants
For this study, a minimum sample size of 158 was required to achieve a high-powered test (Steinman & Updegraff, 2015; i.e., d = 0.25, α = 0.05, 1–β = 0.8). Responses were collected from mTurk, Prolific, a local telegram community “SgResearchLobang,” and the university’s research participation program. Five hundred and thirty-five full data sets were collected. After removing 372 responses which used verbatium content from online sources, comprised single words (e.g., good), indicated response sets (e.g., all the same scores), and/or those which did not meet Naidu et al.’s (2020) inclusion criteria for the lexical-decision task and dot-probe tasks (i.e., no more than 10 errors, response time <200 and >1500 ms after presentation of stimuli), 163 complete responses were retained for data analysis. Participants were mainly from Europe (39.3%), Africa (26.4%), followed by America (22.1%) and Asia (11.7%). The age ranged from 18 to 63 years (M = 27.75 years, SD = 9.0). The majority of the participants received at least two doses of vaccination (81.0%) at the time of the study and had personal experience with COVID-19 (79.8%).
Materials
The Lexical-Decision Task
The lexical-decision task stimuli were made up of 24 words—eight death-related words as the DWFT (e.g., skull and grave), eight threat-related words (e.g., criticism, and crisis), and eight positive-related words (e.g., kindness and cheer). Each of the words was paired with a neutral word of corresponding word length, word frequency, and arousal. The nonwords were also matched with corresponding length and syllables using the Wuggy pseudo-word generator. Participants would be shown the word stimuli and were instructed to press the spacebar when the stimulus was a word and not to respond if it was a nonword. They completed 15 practice trials which comprised neutral words before attempting the actual 96 trials.
Dot-Probe Task
Twenty-four word pairs were formed with the same stimuli from the lexical-decision task, with one word from each word categories (i.e., death, threat, and positive), and a neutral word matched on word length and frequency. Each trial began with a fixation display at the center of the screen for 500 ms, after which a word pair would be presented simultaneously, one on to the upper-middle and another on the lower-middle of the screen. A probe “*” or “**” then appeared for 500 ms in the location of either the death-, threat-, or positive-related word (congruent presentation), or the neutral word (incongruent presentation). Participants were instructed to press corresponding arrow keys as quickly and accurately as possible to differentiate between two probes when they saw either one or two probes, respectively. Participants completed 192 critical trials, which were presented in a randomized order. An attentional bias (AB) index was computed by subtracting response time for congruent (probe at presentation category location) from incongruent presentations (probe at neutral word location).
DAS
The DAS (Templer, 1970) is made of 15 items. Individuals would respond if the items were “true” or “false” in their experience. An example of the items is “I am very much afraid to die.” The total scores ranged from 0 to 15, with higher scores indicating higher death anxiety. The DAS has been found to have good convergent validity with other scales measuring death anxiety such as the Fear of Death Scale (Templer, 1970). It has been translated to other languages and has demonstrated good reliabilities and validities (Tomás-Sábado & Gómez-Benito, 2002).
Procedures
All instructions and materials were the same as Study 1 except for (a) the removal of the mild pandemic condition and (b) the use of different dependent measures. Participants were randomly assigned to one of the conditions before completing all the three dependent measures. The lexical-decision task and dot-probe task were programmed in accordance with Naidu et al. (2020). Together with the DAS, the lexical-decision task and dot-probe task were presented in a randomized manner on the Millisecond Inquisit Software. Participants were required to enter their participant number or their workers’ ID number at the beginning of the computer tasks and when they were directed back to the final phase of the study (i.e., demographic information) after the computer tasks to ensure that data sets are accurately matched.
Study 2 Results
The data were analyzed using SPSS Version 22 with the alpha level set at .05. Among the final group of participants, the average time taken to complete the survey was 1525.30 s or approximately 25 min.
The Cronbach αs were .90 for health anxiety and .69 for the attitudes toward negative consequences of developing severe illnesses subscale for this study. The Cronbach αs for positive and negative affects in this study are .92 and .90, respectively.
The means and SDs of the DVs are presented in Table 2. There was no significant effect of MS on positive affect, F(2,157) = .09, p = .92, or negative affect, F(2,157) = 1.55, p = .22. Delay also did not have any significant effects on positive affect, F(1,157) = .27, p = .61, or negative affect, F(1,157) = .03, p =.87. The interaction effect of MS and delay was also not significant on both positive and negative affects, p > .05.
Means and Standard Deviation of the Death Anxiety Scale (DAS), the Lexical-Decision Task (LDT), and the Dot-Probe Task (DPT).

Note. Standard deviations are presented in parentheses. DAS = Death Anxiety Scale; DPT = dot-probe task; MS = mortality salience; PS = pandemic salience; LDT = lexical-decision task.
p < .05; **p < .01.
To address the hypothesis, a 3 (IV 1: standard MS vs. severe pandemic vs. dental pain) × 2 (IV 2: delay vs. no-delay) between-subjects ANCOVA was performed to examine the effects of MS and delay on the lexical-decision task while controlling for health anxiety. Results showed that MS has a significant effect on lexical-decision task death and positive words, F(2,155) = 3.17, p = .05 and F(2,155) = 3.37, p = .04. To ascertain whether familiarity with English could have influenced the results, nationality was included into the ANCOVA analysis. There were no main effects of nationality on any of the lexical-decision task DVs.
Post hoc analysis with the Tukey honestly significant difference (HSD) revealed that response time to death words was significantly faster in the pandemic (M = 495.93, SD = 64.52) than dental condition (M = 545.50, SD = 117.85, d = .53). Similar post hoc Tukey HSD analysis found that response to positive words was significantly faster in the pandemic (M = 493.39, SD = 47.84) than dental condition (M = 541.66, SD = 114.05, d = .55). There were no significant differences in response times between death and positive words between standard MS and control condition. The faster response time toward lexical-decision task death words in the pandemic than the control condition provided partial support for our hypothesis. There were no significant differences in response times between death and positive words between standard MS and control conditions.
The MS effect on dot-probe task and DAS was not significant. Dot-probe task results did not reveal differences for AB toward death-related words between conditions. There were no significant main effects of MS on AB toward death-related words, F(2,158) = 1.17, p = .31, positive words, F(2,158) = 2.44, p = .09, and threat words, F(2,155) = .42, p = .66. There was also no main effect of delay or interaction effect of MS and delay on dot-probe task and DAS scores, p > .05. Thus, our hypothesis was partially supported as response time was significantly faster toward lexical-decision task death words in the pandemic than control condition but not for the other DVs, when controlling for health anxiety.
Study 2 Discussion
The purpose of Study 2 was to examine issues raised in Study 1 findings. This study found that the response times were significantly faster toward lexical-decision task death words than threat words following exposure to the severe pandemic as compared to the control condition. However, this inclination toward death words was not observed for dot-probe task. Although not formally recorded, several participants had reported that the dot-probe task was challenging as they could not comprehend the task. This could have impacted the performance and outcomes on the dot-probe task. In addition, the dot-probe task has been criticized to have poor reliability, suggesting its limitation in accessing death cognitions and anxiety (Kappenman et al., 2014; Torrence & Troup, 2018). An increase in death anxiety was also not observed on the DAS. As demonstrated by Naidu et al. (2020), the death cognitions and anxiety might not have been as easily accessible in individuals’ consciousness and thus not reflected through the responses on the DAS, which is an explicit assessment of death anxiety.
The results obtained from the lexical-decision task suggest that death thoughts were more accessible, leading individuals to respond faster to death words when they were reminded of severe pandemics. The effect of MS on death-thought accessibility remained significant when we controlled for health anxiety, supporting the hypothesis that the severe pandemic condition was able to trigger MS effect, and continued to do so when controlling for health anxiety. This finding also increased the confidence that the absence of death-thought accessibility in Study 1 was unlikely to be a consequence of the exposure of SHAI-Short Form but rather a consequence of the use of a less sensitive death-thought accessibility measure. In addition, the world continued to be ravaged by COVID-19 when Study 2 was conducted. This makes the obscuring of death-thought accessibility arising from prolonged exposure to COVID-19 an unlikely explanation for the absence of the death-thought accessibility in Study 1.
Apart from significant differences in response time toward lexical-decision task death words, results also showed that participants responded significantly faster toward positive words. This might appear counterintuitive given that MS typically trigger death-related anxiety. Nevertheless, some studies have suggested that this attunement to positive stimuli could be a coping response in the face of MS (DeWall & Baumeister, 2007; Kelley et al., 2014). When confronted with personal death reminders, participants were likely to regulate the anxiety aroused by seeking positive information such as responding faster to positive word associations or gazing longer at positive images (DeWall & Baumeister, 2007; Kelley et al., 2014). The seeking of positive information was found in both delay and no-delay MS conditions. Through a series of three studies, DeWall and Baumeister (2007) have consistently found an inclination toward positive information immediately and after a time delay following MS presentation, leading the authors to postulate that the regulation of death anxiety by seeking positive information began immediately after death reminders and persevered throughout the time delay. In line with this research, participants in this study have demonstrated this inclination toward lexical-decision task positive words, possibly as an attempt to regulate the anxiety arising from death reminders in the pandemic condition.
The MS effect of pandemic was prevalent in both delay and no-delay conditions. Based on the dual process model of TMT, the MS effects are expected to be more robust following a time delay. This is a result of the rebound effects following the active suppression of death thoughts which were triggered immediately after death reminders. Nevertheless, the effect of delay on death-thought accessibility was not found in this study, suggesting that death-thought accessibility was triggered immediately after exposure to the pandemic condition, and stayed elevated after a time delay.
One possible explanation is the presence of cognitive load when individuals were embarking on the computerized tasks assessing the DVs. As noted by Hayes et al. (2010), suppression of death-thought accessibility would be disrupted when a competing task was introduced, allowing the manifestation of death-thought accessibility. For instance, participants in this study could have been engaging in other competing tasks as it is not uncommon for individuals to multitask when embarking on online surveys and studies (Revilla & Ochoa, 2015). This multitasking could have interfered with the active suppression of death thoughts following exposure to the pandemic condition, allowing the manifestation of elevated death-thought accessibility immediately after MS induction.
A second possibility is the subtlety of MS prime of the pandemic condition. As compared to the standard MS condition, the severity of the pandemic condition was presented using statistics on fatalities and gravity of the symptoms experienced, after which participants were asked to jot down their thoughts and emotions if they “had gotten” the virus rather than “die” from the virus. This presentation of the impact of the pandemic condition on participants could have been perceived as less explicit and confrontational, thereby triggering death thoughts in a subtle manner, making them more accessible immediately (Steinman & Updegraff, 2015).
Finally, there had been evidence that MS effects could weaken following a time delay (Trafimow & Hughes, 2012). Trafimow and Hughes (2012) consistently found that death-thought accessibility was elevated on DWFT or lexical-decision task immediately after the MS induction. The current results follow a similar pattern of significant elevation of death-thought accessibility immediately following pandemic salience. Hence, the interference of thought suppression from multitasking, the subtlety of the MS presentation of the pandemic condition, and the possible absence of a delayed MS effect on death-thought accessibility could account for the current results.
While there was a MS effect of severe pandemic on death-thought accessibility, there was no MS effect observed in the standard MS condition in the two studies, suggesting a failure to replicate the standard MS effect. The failure to replicate results of published psychological research has been a topic of contention, with some suggesting that publication biases have contributed to this issue (Francis, 2012; Maxwell et al., 2015). Indeed, most studies examining critical incidents seldom compared death-thought accessibility between standard MS and critical incident conditions (Leung et al., 2022). Among the limited published literature investigating the MS effects of diseases, Leung et al. (2022) only found one peer-reviewed article which compared the death-thought accessibility between Ebola and control conditions, but this had not included the standard MS condition (Arrowood et al., 2017). Also, studies which reported a nonsignificant effect of standard MS and critical incident seemed to be under-represented, with only one study in Leung et al.’s (2022) review reporting null effects of standard MS and terrorism on death-thought accessibility (Ullrich & Cohrs, 2007). These could indicate a possibility that research which did not detect standard MS effects on death-thought accessibility have not been represented in published literature.
Recent large-scale replication efforts have also challenged the robustness of the MS effects (Haaf et al., 2020; Klein et al., 2019; Sætrevik & Sjåstad, 2022). A large-scale replication effort by Many Labs 4 which replicated MS experimental designs had not found significant MS effects (Klein et al., 2019). This absence of MS effects holds even when the original authors were involved in the replication studies (Klein et al., 2019) and following a Bayesian reanalysis of the Many Labs 4 data (Haaf et al., 2020). More recently, Sætrevik and Sjåstad (2022) attempted to replicate MS effects on traditional and novel measures using sample sizes that are statistically powerful enough to detect the MS effects but to no avail. These failures to replicate seemed to be cumulative evidence implying that MS effects were not as robust as previously published.
General Discussion
This research aimed to examine the MS effect of pandemic salience condition in view of the COVID-19 pandemic. To the best of the authors’ knowledge, it is also the first study which assessed death-thought accessibility of pandemic salience using TMT-endorsed measures (Cox et al., 2019). Using the DWFT, the first study had not found significant MS effects on death-thought accessibility. This was contrary to past studies, which have found MS effects of diseases (e.g., Ebola and cancer) on death-thought accessibility as assessed by the DWFT (Arndt et al., 2007; Arrowood et al., 2017). However, death-thought accessibility was significantly elevated in the pandemic condition than in the control condition when we replaced the DWFT with the lexical-decision task in the second study. In particular, participants responded significantly faster toward death words in the pandemic condition as compared to the control condition. The shorter response time toward death words was consistent with other TMT studies assessing death-thought accessibility with lexical-decision task following exposure to pictures of buildings destroyed by war (Hayes et al., 2008; Vail et al., 2012).
It is interesting to note that unlike past studies (Arrowood et al., 2017; Das et al., 2009; Kastenmüller et al., 2011), MS effects on death-thought accessibility, as assessed by the DWFT, were not significant in Study 1. This led to questions about the sensitivity and psychometric properties of the DWFT, which were explored by Naidu et al. (2020). In their first study, responses on the DWFT did not show significant differences in death words generated between MS and the control condition. However, responses on implicit tasks were able to distinguish between MS and control conditions, in which participants responded significantly faster to death words in the lexical-decision task and reported more death images based on the inkblot stimuli. Similarly, Study 1 did not find significant differences in death words generated on the DWFT between MS and control conditions. Instead, response time toward death words in the lexical-decision task was able to distinguish pandemic and control conditions when we replace DWFT with lexical-decision task, supporting the idea that DWFT may be less sensitive than other implicit measures in assessing death-thought accessibility (Naidu et al., 2020). We also found that following pandemic reminders, individuals showed a faster response time toward positive words, which some studies have interpreted as an immediate coping after MS inductions (DeWall & Baumeister, 2007; Kelley et al., 2014).
Another point to note for this study is the failure to replicate MS effects of standard MS inductions. While the standard MS effects have been found to be robust (Hayes et al., 2010; Steinman & Updegraff, 2015), this study did not find effects of standard MS on both the DWFT and lexical-decision task. Apart from the absence of MS effects of the standard MS induction, the absence of the MS effects on the DWFT could also be attributable to the limited sensitivity of the DWFT (Naidu et al., 2020). Recent studies have tried to replicate the standard MS induction (i.e., asked about thoughts and feelings evoked by death), as well as employed appropriate statistical analysis, but to no avail (Haaf et al., 2020; Klein et al., 2019; Sætrevik, & Sjåstad, 2022). However, we were able to find MS effects of death-associated conditions (i.e., severe pandemic), which were indicative of MS effects consistent with TMT.
Although there have been heated discussions over the absence of MS effects, there has not been conclusive evidence to debunk TMT. Rather, many have proposed refinements to TMT to better explain MS effects. Some researchers like Treger et al. (2023) proposed that perhaps death is not as “terrifying” as we had imagined, and thus blunted the standard effects. On the contrary, Meng et al. (2021) suggested the role of culture in influencing our acceptance and emotions toward death. Cultures which embrace death or believe in an after life tended to report lower anxiety and fear toward death. The acceptance of death or belief that there is a continuation after physical death has been found to buffer the effects of standard MS in TMT studies (Jong, 2020; Wang et al., 2023). In addition, individuals’ experience and interpretation of death could impact their acceptance and feelings toward general death. Some individuals could have developed significant anxiety over death in general if they had witnessed suffering or violent deaths while some could have experienced peaceful deaths (Mosheva et al., 2021; Kristensen et al., 2012). When faced with standard MS stimulus, individuals’ responses will likely be influenced by their cultural and personal experiences. Moreover, standard MS instructs respondents to write freely about their deaths, which is open to individuals’ interpretations and experiences of deaths which could be filled with suffering or tranquil. On the contrary, MS induction with pandemics and critical incidents may present a more uniform type and process of death (e.g., COVID and terrorism), which usually depict suffering and violence, thereby triggering significant death thoughts and anxiety as compared to standard MS.
The mode of data collection could also play a role in impacting the current results. Treger et al. (2023) proposed several challenges inherent to online data collection which could obscure the standard MS effects. One such difficulty is the lack of control researchers have over the time delay between presentation of MS stimuli and response to outcome measures, which could have influenced the strength of MS (Chandler et al., 2015). Another challenge involved mTurk participants’ possible familiarity with TMT stimuli or outcome measures, which then desensitized them to death anxiety. This could be a consequence of repeated exposure of similar experimental conditions to mTurk participants as mTurk has gained much popularity as a data collection platform over the years (Webb & Tangney, 2022). Related to online sampling is the low acceptance rate demonstrated in this study. In fact, concerns over data quality and poor acceptance rates on mTurk had been raised (Cox et al., 2021; Webb & Tangney, 2022). Our study acceptance rates are 45% (Study 1) and 30% (Study 2), which did not deviate significantly from the 38% reported in Cox et al.’s (2021) study on TMT and benefit finding. While the limitations of online data collection are duly acknowledged, it was the only viable option during the pandemic, and it allowed access to a wider population across geographical locations and demographics.
Overall, this study suggests individuals perceived that their lives were more threatened in pandemics. This finding that death anxiety, rather than health anxiety, has a significant impact on death-thought accessibility, points to a complex picture of psychological processes when determining individual reactions in pandemic situations. The presence of death anxiety in pandemics could offer a point of intervention to maintain psychological well-being and to facilitate helpful behaviors and attitudes in communities during crisis situations such as a pandemic. As recommended by Leung et al. (2022), interventions targeting death thoughts and anxiety can be conceptualized and implemented to help individuals regulate death anxiety, restoring psychological homeostasis and encouraging individuals to take adaptive coping actions during pandemics. On a community level, public messaging can frame adaptive health behaviors (e.g., maintain social distancing and wearing of face masks) as a means to lower infection rates and consequently fatalities, thereby reducing death cognitions. Future research can examine the effectiveness of individual and community interventions conceptualized based on the TMT framework. Another area to extend the current research is the replication of this study with more sensitive measures of death anxiety (e.g., implicit measures). It will be especially helpful to examine the MS effects of standard death, pandemics, and/or other critical incidents on death-thought accessibility, as well as individuals’ perception of the different MS inductions, to assess whether there is a relationship between the perceived death experiences in different situations (e.g., death in general and death in critical incidents) and death-thought accessibility. The inclusion of face-to-face data collection, and clarification if participants had participated in similar TMT experiments and surveys, may shed light into the possible impact of modalities on data quality mentioned above. This study has two limitations. First, the samples are mainly made up of individuals from the United States in Study 1 while Europeans formed the majority of participants in Study 2, thus making these results unlikely to be generalizable to other populations. A related second limitation is that data were collected online due to the COVID-19 social-distancing restrictions. This could have biased sampling, as there could be inherent differences between individuals who had a strong online presence as compared to those who do not. Nevertheless, with online data collection being more prevalent, studies examining TMT effects have continued to report robust TMT effects, similarly when data collection was done face-to-face.
In conclusion, this study found a MS effect in the pandemic condition on death cognitions when they were assessed on the lexical-decision task instead of the DWFT. This could be a result of the limited sensitivity of the DWFT. Also, standard MS effect was not present regardless of death-thought accessibility measures employed, leading to a consideration of the failure to replicate. Nevertheless, more research and unbiased publication are needed to re-examine the issue of a failure to replicate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study received ethical approval from the James Cook University’s ethics committee (approval no. H8295).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.