
Abstract
Relational depth (RD)—moments of profound connection and engagement between two people—is a humanistic–existential construct, showing preliminary association with psychological growth in psychotherapy. This research investigates the impact of RD, alongside relationship satisfaction and emotional intimacy, on subjective well-being in close relationships in the community. Psychometric properties of latent variables were assessed in a stratified online sample of 497 participants in the United Kingdom (47.1% male, 52.1% female, 1% other; mean age 45.7 [SD = 15.9]; 86.5% white, 7.8% Asian, 3.2% Black, 1.4% mixed and 1% other), followed by lagged regressions, and moderation analyses to assess the role of RD on Personal Well-being Score (PWS). Data were collected at two further time points at 3-month intervals on a stratified subset of participants (n = 297 and n = 267). RD emerged as a significant predictor of subjective well-being in close relationships in the community and was moderated by emotional intimacy and relationship satisfaction. This study provides the first robust evidence of the relevance and impact of the humanistic–existential construct of RD on well-being beyond a psychotherapy context. This points to the value of practices that can facilitate RD experiences in the community.
Keywords
Improving well-being is an important social aim in modern societies (e.g., Health and Wellbeing Strategy, 2020; Schulte et al., 2015; World Health Organization [WHO], 2020). One basis for the well-being of communities is the quality of people’s interpersonal relationships (e.g., Diener & Tay, 2017; Wang et al., 2018). We know, for instance, that the happiest individuals spend less time alone and are more satisfied with their relationships (e.g., Diener et al., 2018; Diener & Tay, 2017). In a psychotherapy context, the therapeutic relationship constitutes a key factor in the reduction of symptoms and improved mental health outcomes (Norcross & Wampold, 2019). Relational Depth (RD) is a quality of the therapeutic relationship emerging from the humanistic–existential literature and may be particularly relevant to the well-being of individuals beyond a psychotherapy context. That is for three reasons: (a) RD is increasingly associated with various aspects of psychological growth in psychotherapy (e.g., Kim et al., 2020; Di Malta et al., 2023); (b) RD experiences can be facilitated through specific practices and training, which have potential to be disseminated beyond a psychotherapy context (e.g., Ray et al., 2019; Wilcox & Almasifard, 2023); and (c) RD experiences are theorized to occur beyond a psychotherapy context (Mearns & Cooper, 2005, 2018).
The concept of RD emerged from the humanistic and person-centered psychotherapy field (Cornelius-White et al., 2018; Mearns & Cooper, 2018; Rogers, 1957)—informed by existential, relational, multicultural, and feminist insights (Buber, 1958; Jordan et al., 1991; Schmid, 2006). The writings of the influential existential philosopher Buber have been particularly foundational to the conceptualization of RD, detailing an ontology that puts relationality, rather than individuality, at its core (Buber, 1958; Cooper et al., 2012; Friedman, 1996). RD has been defined as a “state of profound contact and engagement between people” (Mearns & Cooper, 2018, p. xvii); and, in Rogerian (1957) terminology, has been characterized as empathy, congruence, and unconditional positive regard, experienced bi-directionally and at high levels. Although not termed as such, RD can be considered a core focus across humanistic and existential psychotherapeutic practices: in the “co-presence” of Bugental (1978) or Geller (2013); in Hycner’s (1991) dialogical gestalt therapy; or in the “being for” and “being with” of existential psychotherapy (Spinelli, 1994). Among psychotherapy relationship constructs, RD shares commonalities with the “bond” aspect of the working alliance, entailing a warm and personal connection between therapist and client (Bordin, 1979). It also aligns with the “real relationship,” involving co-genuineness and a mutual, two-way relationship (Gelso, 2004). However, the term “RD” places specific emphasis on the depth of interactive and inter-relational engagement between therapist and client (Mearns & Cooper, 2018). In addition, while phenomena like the working alliance are “gradient,” varying in intensity throughout the therapy relationship; RD is conceptualized, for research purposes, as a “threshold” phenomenon (Cooper, 2005; Knox & Cooper, 2010). That is, it is either present or not present during specific periods of therapy. RD, therefore, uniquely describes moments in therapy characterized by exceptionally intense contact and engagement.
Both qualitative and quantitative data suggest that moments of RD are associated with psychological growth (e.g., Kim et al., 2020; Knox, 2011; McMillan & McLeod, 2006; Wiggins et al., 2012). For instance, clients have spoken about an increased sense of safety at moments of RD, which has allowed them to bring more vulnerability to the relationship (Knox, 2008). Clients reported experiencing something that had “shifted” and that “their eyes had been opened” (Knox, 2011, p 143). Clients also described feeling more connected to themselves, experiencing a greater clarity of thought and self-understanding, as well as improved relationships with family and friends, but also feeling “more alive,” “happier,” and “at ease” (Knox, 2011, p. 147). Many clients saw the experience as a catalyst for change, with an enduring increased connection to the self, others, and the world. In addition, survey research has pointed to associations with reduced psychological distress and increased relationship satisfaction (Di Malta et al., 2023; Leung, 2008). One recent study suggested associations between RD—as measured with the Relational Depth Inventory (Wiggins et al., 2012)—with increased unconditional self-regard and authenticity in 55 psychotherapy clients in a clinical setting (Kim et al., 2020). The frequency of RD moments in psychotherapy clients—as measured by the Relational Depth Frequency Scale (Di Malta, Evans et al., 2020)—was also associated with increased satisfaction with psychotherapy and psychotherapist (Di Malta et al., 2023). Another study found associations of RD with reduced burnout in psychotherapists (Zarzycka et al., 2022).
RD is an experience that may be facilitated with relevant practices and training in psychotherapy (e.g., Ray et al., 2021), or in order for individuals to improve the quality of their relationships and support their own well-being (e.g., Cooper & Knox, 2018). For instance, research suggests that RD may be enhanced by mindfulness training (Baker, 2016). Other research has specifically turned to developing training to support relational depth experiences in humanistic-informed therapies (Ray et al., 2021; Tangen & Cashwell, 2016). These highlighted the importance of students’ own counseling, and the fostering of strong supervisory and mentoring relationships (Tangen & Cashwell, 2016) and taking part in experiential activities (Ray et al., 2021). Wilcox and Almasifard (2023) conducted a meta-synthesis of 27 studies on the experiences of RD to identify the conditions where RD was more likely to be facilitated. They found six themes: (1) establishing a dialogue with one’s inner world, (2) working with attachment, (3) responding sensitively to beliefs and values, (4) deepening each other’s understanding, (5) addressing ruptures, and (6) the client’s role in meeting at RD.
As discussed, Mearns and Cooper (2005, 2018) described RD primarily in relation to psychotherapeutic practice. However, like Buber (1958), they considered it an experience relevant to all walks of life. The authors referred to the following definition: “a state of profound contact and engagement between two people in which each person is fully real with the other, and able to understand and value the other’s experiences at a high level” (Mearns & Cooper, 2005, p. xii). The experience of RD has since been identified in a range of health contexts, and with different client groups. For instance, in the context of sex addiction treatment, RD was found to facilitate addressing issues of shame and attachment insecurities (Woehler et al., 2018; Woehler & Ray, 2022). Cancer patients also experienced moments of RD in their therapy (Anderson et al., 2023). However, to date there is no research that directly explores the experiences of RD in close relationships in the community, that is, in non-therapeutic settings.
RD—as a humanistically and existentially informed way of being—may be relevant and useful to improving subjective well-being outside of a psychotherapy context among individuals in communities. However, no research has directly addressed whether RD does have an impact on subjective well-being in close relationships in a non-psychotherapeutic, community setting.
The Present Study
The aim of this study was to examine whether RD experiences can be identified outside of a psychotherapeutic context and whether they lead to improved subjective well-being in close relationships in the community. The Relational Depth Frequency Scale (RDFS, Di Malta, Evans et al., 2020) was adapted in this study to assess RD for three new contexts: (a) with one close other in the community (a friend, a partner, a family member, etc.), (b) across all relationships in the community, and (c) across all relationships online only.
The emotional intimacy scale (EIS; Sinclair & Dowdy, 2005) and the relationship satisfaction scale (RAS-G; Hendrick, 1988) were used to assess levels of “closeness” in the relationship identified by participants. Emotional intimacy is defined as “a perception of closeness to another that allows sharing of personal feelings, accompanied by an expectation of understanding, affirmation, and demonstrations of caring” (Sinclair & Dowdy, 2005, p. 194). There is some evidence that emotional intimacy may also play a role in the subjective well-being for individuals in the community (Sinclair & Dowdy, 2005).
The main research questions were:
(RQ1) Can individuals experience RD outside of a psychotherapy context?
(RQ2) Does the experience of RD with one single other individual lead to improved subjective well-being?
We also took an exploratory approach to answer the following research questions:
(RQ3) Does the experience of RD across all relationships lead to improved subjective well-being?
(RQ4) Does the experience of RD across relationships online lead to improved subjective well-being?
(RQ5) Do levels of closeness (emotional intimacy and/or relationship satisfaction) moderate the impact of RD on subjective well-being?
(RQ6) Do emotional intimacy or relationship satisfaction lead to improved subjective well-being?
Method
The project was approved by the Open University ethics committee in 2019 under the reference HREC/3603.
Design
This longitudinal study design included three data collection waves and consisted of three parts. In part 1 (wave 1), we examine the reliability and validity of the RDFS, by assessing its internal consistency and factor structure (RQ1). In part 2 (waves 1, 2, and 3), we assess the impact of RD, alongside emotional intimacy and relationship satisfaction, on personal well-being (RQ2, RQ3, RQ4, and RQ6). Part 3 (waves 1, 2, and 3) consists of moderation analyses to examine how closeness in a chosen relationship, as assessed by emotional intimacy and relationship satisfaction, influences the impact of RD on personal well-being (RQ5).
Sampling
The initial sample size was selected to ensure stability when assessing scale structures. Thus, we selected an initial sample size of at least 500. For the following waves, we aimed for (and achieved) a sample size between 200 and 300 based on the recommendations in Kline (2016). The inclusion criteria for participants were 18 years old and over and a resident in the United Kingdom. Using pwrSEM (Y. A. Wang & Rhemtulla, 2021) this gives average power estimates of 1.00 for the item loadings on the latent variables at wave 1 and 0.82 for the regression coefficients for the full Structural Equation Model (SEM) at wave 3.
The sample was collected via Prolific.co, an online platform for sourcing study participants. Recruitment for the first wave was conducted with the aim of achieving a sample representative of the U.K. population across the categories of sex, age, and ethnicity in accordance with U.K. Census Data (Office for National Statistics [ONS], 2011). Given the relatively small numbers involved in certain category combinations and the unpredictability of attrition rates inherent to longitudinal study designs, recruitment for the following waves prioritized the retention of non-white participants in an attempt to maintain the representativeness of the sample across all waves of the study. Any unfilled spaces allocated for non-white participants were opened up to white participants after one week.
Participants
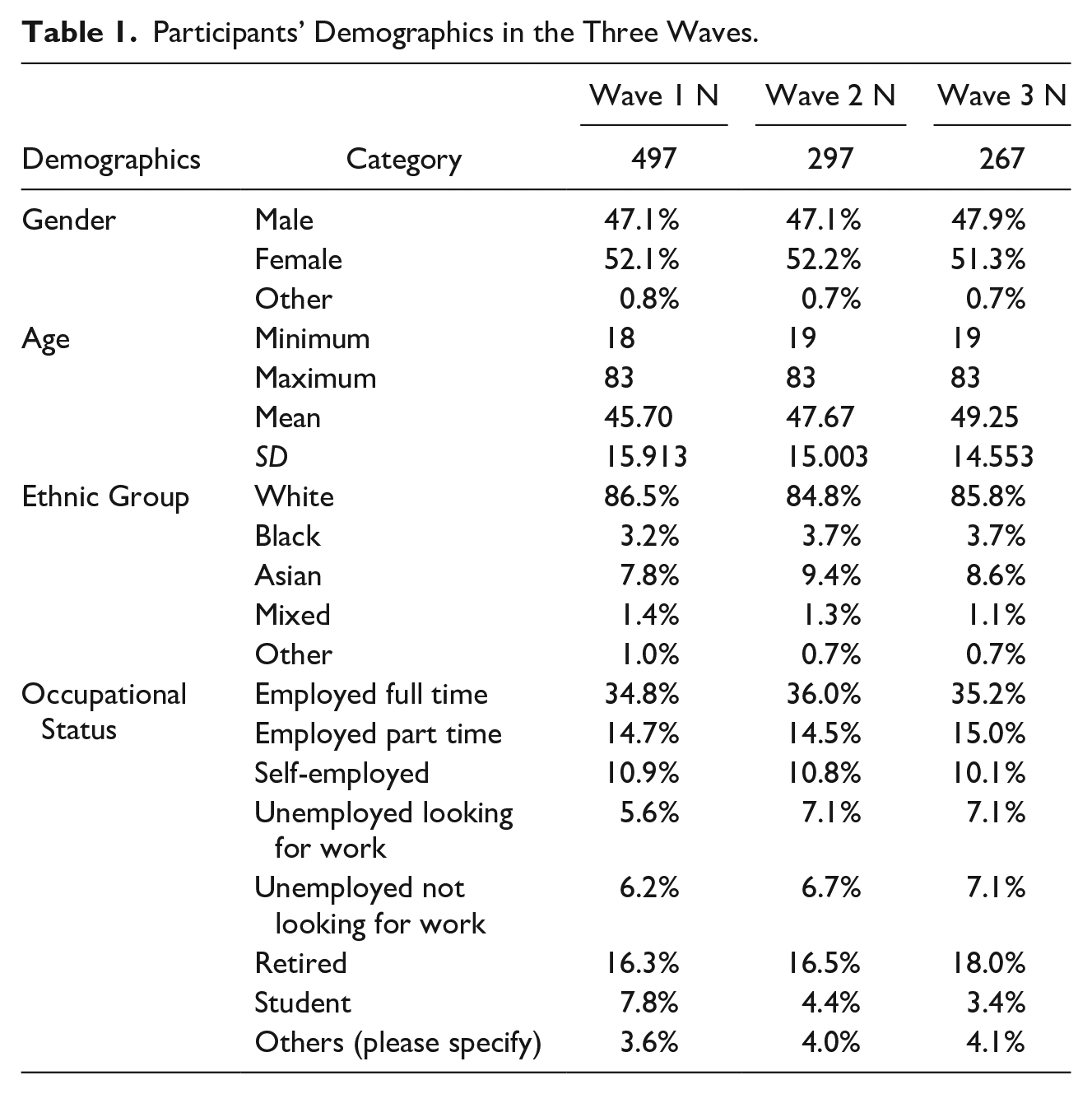
In the first wave of data collection, a total of 523 participants accessed and completed the survey. Subsets of approximately 300 participants were then invited to take part in the following two waves of data collection. In 19 of 523 (3.6%) cases, respondents provided wrong answers to the validity check question, 1/309 (0.3%) respondents provided wrong answers in the second wave, and 5/281 (1.8%) in the third wave. All such cases were excluded from all analyses. This left 504 participants in the first wave, 308 in the second wave, and 276 in the third wave. Of these, seven more were excluded in the first wave due to missing data, resulting in 497 participants in first wave analyses. There were 11 participants who were excluded from the analysis in the second wave due to missing data, resulting in 297 participants. Finally, nine participants were excluded from the last wave due to missing data, resulting in 267 participants. Participant demographics for each wave are presented in Table 1.
Participants’ Demographics in the Three Waves.
Online Survey
The online survey was the same in the three waves of data collection. The survey contained an attention check question asking participants about the subject of the questions they had just answered to increase the validity of responses. Participants selected a significant relationship—“the referent.” When selecting a relationship in the community, most participants nominated their (romantic/marital) partner as their referent (n = 265, 52.7%), though nominated referents also included a friend (n = 93, 18.5%), a parent (n = 55, 10.9%), a child (n = 50, 9.9%), another family member (e.g., siblings, cousins, grandparents; n = 32, 6.4%), or someone else (n = 8, 1.6%). These proportions of participant referents remained broadly consistent (i.e., within 2.5% variability) over the course of the study.
The survey then contained the following questionnaires:
RDFS, Comprising RDFS-s, RDFS-g, and RDFS-g (Online; (Di Malta, Evans et al., 2020, six items each, Cronbach’s α =.93)
The RDFS, a six-item measure, was developed based on humanistic–existential understandings of relationality, and validated to measure deep connection between psychotherapists and clients. It was developed with cognitive pre-testing methods (Di Malta, Cooper et al., 2020), has excellent internal reliability in samples of psychotherapists and clients (Cronbach’s α = .85 and .93, respectively), a single-factor structure, acceptable fit statistics in confirmatory factor analyses (CFA) and Rasch analysis, and is convergent with three measures of the quality of the therapeutic relationship (Zarzycka et al., 2022; Di Malta, Evans et al., 2020). It is divergent with a measure of social desirability and has concurrent validity with a measure of psychotherapy satisfaction (Di Malta et al., 2023). RDFS items focus on the mutuality of connectedness and its intensity in the present moment, as per the construct theory, for example, “We were deeply connected to one another” or “We were immersed in the present moment.” The frequency scale ranges from 1 (not at all) to 5 (most or all of the time). Higher scores indicate a greater frequency of RD.
The measure was adapted for use in this study to assess RD frequency in close relationships in the community. To this effect, the opening stems and instructions were amended. The RDFS-s assessed relational depth in a chosen significant relationship (“the referent”) in the community. The modified stem was: “In my interactions with < the referent > there were moments where. . .” The RDFS-g and RDFS-g (online) assessed the frequency of relational depth with all people in the community (face-to-face or online) and all people online only with the modified stem: “When considering my recent interactions with people [or “in telecommunication”], there were moments where . . .” Items and response options were kept as per the original scale’s.
Emotional Intimacy Scale (EIS; Sinclair & Dowdy, 2005; five items, Cronbach’s α = .87)
The EIS is a self-report measure of emotional intimacy. It begins with the instruction: “Consider how well the following statements describe your current experience with <the referent>. Think in terms of the quality of your relationship with <the referent> in answering these items.” The EIS is focused on perceptions of the other person’s acceptance and care, for example, “this person cares deeply for me” or “This person completely accepts me as I am” and response options range from 1 (strongly disagree) to 6 (strongly agree). Participants were instructed to rate the same referent as the one chosen for the RDFS-s.
Internal consistency and test–retest reliability (after 6 weeks) were .88 and .85, respectively (Sinclair & Dowdy, 2005). The EIS has been found to be convergent with measures of social support, self-efficacy, life satisfaction, and positive affect. In support of criterion-related validity, the EIS predicted outcomes from an intervention program (Sinclair & Dowdy, 2005). Higher scores indicate a stronger sense of emotional intimacy with referents.
Relationship Assessment Scale (RAS-G; Hendrick, 1988, seven items, α = .86)
The RAS-G is a brief, generic self-report measure of relationship satisfaction. Respondents answer seven-item questions (e.g., “How well does your <referent> meet your needs?”) on a 5-point Likert-type scale. Following the rekeying of reverse-scored items, ratings are summed to produce a total relationship satisfaction score. Previous research (Hendrick, 1988) supports the validity of the RAS-G with instrument scores correlating in expected directions with scores on independent measures of love attitudes, intimate self-disclosure, dyadic adjustment, and relationship commitment. Renshaw et al. (2011) report high internal consistency (Cronbach’s α was .89 for parents, .87 for friends, .90 for romantic partners, and .86 for other relatives). Test–retest reliability over 3 weeks was excellent (r = .87 for parents, r = 74 for romantic partners, r = .78 for friends, and r = .89 for other types of relatives). RAS-G showed good criterion validity as it negatively predicted depressive symptoms, r = −.31 (Renshaw et al., 2011).
Personal Well-being Score (PWS; Benson et al., 2019, four items, α = .90)
The PWS is a short generic unidimensional self-report measure of subjective well-being or happiness based on the U.K. Office of National Statistics’s four (ONS4) subjective well-being questions developed for routine use in health care quality improvement evaluation. Items are rated on a 4-point scale from strongly agree to disagree and include an item on overall satisfaction “I am satisfied with my life,” eudemonic well-being “What I do in my life is worthwhile,” current positive experience “I was happy yesterday,” and current negative experience “I was NOT anxious yesterday.” PWS has excellent internal consistency (Cronbach’s α = .90), and good convergent validity, as shown by positive correlations with health confidence (r = .60), health status (r = .58), patient experience (r = .30), and age group (r = .24) (Benson et al., 2019).
Procedure
Participants who responded to the study advertised on Prolific.co were redirected to the Qualtrics survey platform, where they first provided informed consent. Participants were then asked demographic questions and details of their relationship with a close specific person (their referent) in the community, followed by the RDFS-s, EIS, RAS-G, RDFS-g, RDFS-g (online), PWS, and a validity check item (in that order). The same referent (close relationship) was used for the completion of the RDFS-s, EIS, and RAS-G. Subsequent study waves followed the same procedure, with participants reminded of their (previously identified) referent prior to rating the scales. Data collection was conducted over a period of 6 months, with a 3-month interval between each study wave. Participants were paid the equivalent of U.K. minimum wage each time they completed a study wave, along with a bonus payment of up to £1 which was available for successfully completing all waves in the study.
Analyses
Part 1: Reliability and Validity of the RDFS in a Non-psychotherapeutic Context (RQ1)
To assess the validity of the RDFS in community relationships, we examined the robustness of the latent variable structure to be used in the modeling. This consisted of running Cronbach’s α analyses to measure scale reliability and then an exploratory factor analysis (EFA) to ensure that the latent variables are unidimensional. Internal consistency estimates of > .70 were sought (e.g., Bagozzi & Yi, 2012). These analyses were run in the initial wave of data collection (n = 497) using SPSS v.27. In addition, an EFA was conducted across all statements to check that the five individual latent variables were indeed separate constructs.
Following the EFA, CFAs were run on each of the latent variables. CFA was performed to assess goodness of fit and measurement invariance for a single-factor model of the RDFS-s, RDFS-g, and RDFS-g (online). As recommended by Hoyle and Panter (1995) several fit indices were used including the Root Mean Square Error of Approximation (RMSEA), the Comparative Fit Index (CFI), and the Tucker–Lewis Index (TLI). Values greater than 0.95 for the CFI and TLI were considered to reflect good model fit. A RMSEA value of .06 or less is considered to indicate a good fit, although values up to .08 are considered acceptable (Hu & Bentler, 1999). All CFA analyses were run in MPlus 8.6 (Muthén & Muthén, 1998–2017).
The latent variables were also tested for longitudinal invariance. This analysis checked that the underlying structure of the latent variable did not change between waves. The analysis looked at two measures of invariance: metric invariance (the most important measure that checks that the loadings of each item in the latent variable do not change across waves); and scalar invariances, which assesses whether the intercepts of the items (i.e., the expected value of the item if the latent variable mean is zero) changes across waves. The latter test is routinely recommended when testing longitudinal invariance (e.g., Kline, 2016). However, if there has been a situational change among the participants of a study between waves (e.g., there has been a significant change in the relationship between the respondent and their referent), then there should be a corresponding change in the intercept, and so one would not necessarily expect scalar invariance.
Invariance was tested using “nested model tests” (e.g., Newsom, 2015). In this case, three separate SEM analyses were run for each latent variable. The first analysis created three latent variables for each measure, one for each wave with no constraints. The second similarly created three latent variables for each measure but constrained the factor loadings for each item to be equal across all three waves (metric invariance), and the third was the same as the second but constrained both the factor loadings and the intercepts (scalar invariance) for each item to be equal across all three waves.
Because the second model is nested within the first and the third model is nested within both the first and the second models, the differences in the χ2 values between models can be tested for significance. If the differences are not statistically significant, then invariance can be assumed.
Part 2: Lagged Regression Analyses (RQ2, RQ3, RQ4, and RQ6)
Following establishing the robustness of the underlying dimensions, the next wave of analysis was a cross-lagged regression structural equation model to measure the relationship between connectedness at time t and well-being at time (t + 1), controlling for well-being at time t (Newsom, 2015). Two hundred sixty respondents completed all three waves of the study. Because this figure comfortably exceeded the target sample size discussed earlier, it was decided not to artificially increase the overall numbers in the model by imputing data for respondents who had not completed one or more of the waves. The variables used in the regression were the dependent well-being variable PWS and the independent connectedness variables RDFS-s, EIS, RAS, RDFS-g, and RDFS-g (online). All analyses were run using MPlus 8.6 (Muthén & Muthén, 1998–2017).
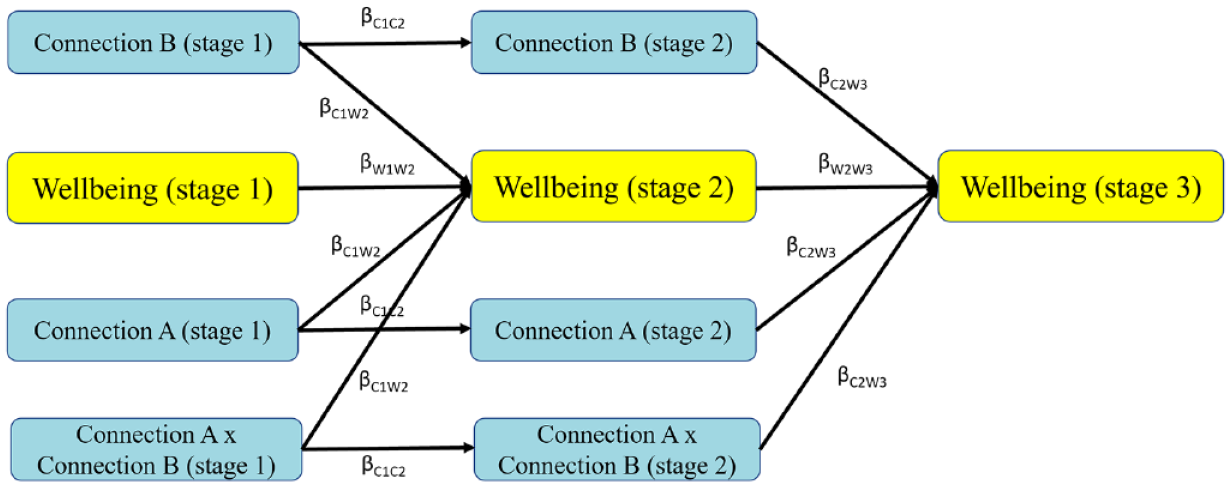
Cross-lagged regressions were run across the three waves with PWS as the dependent variable. Each of the five measures of connectedness was included as the independent variable separately. Figure 1 shows the planned analysis that examines the relationship between connectedness at time t and well-being at time (t + 1), controlling for well-being at time t. Because the analysis was designed to measure the extent to which well-being was predicted by connectedness, the model does not include any relationship between well-being at t = 1 and connectedness at t = 2.

Lagged Regression Model.
Part 3: Moderation Analyses (RQ5)
Following the regression findings, we then conducted an analysis to assess whether or not either or both of the closeness variables (EIS and RAS) moderated the impact of relational depth (RDFS-s) on well-being. This analysis looked at the interaction between the independent variables to see, for example, whether closeness (e.g., EIS) moderated the degree to which the frequency of connectedness (RDFS-s) predicts well-being (Baron & Kenny, 1986). The moderation analysis was achieved by initially creating an interaction term by multiplying the independent variable with the moderator and then running a lagged regression of well-being predicted by relational depth (RDFS-s) plus the moderator (one of the quality connectedness variables (EIS or RAS)) and the product of the moderator and the independent variable (e.g., RDFS-s * EIS or RDFS-s * RAS) (Cohen et al., 2014). This planned analysis is shown in Figure 2.
Lagged Moderation Model.
Results
Part 1: Reliability and Validity of the RDFS in a Non-psychotherapeutic Context (RQ1)
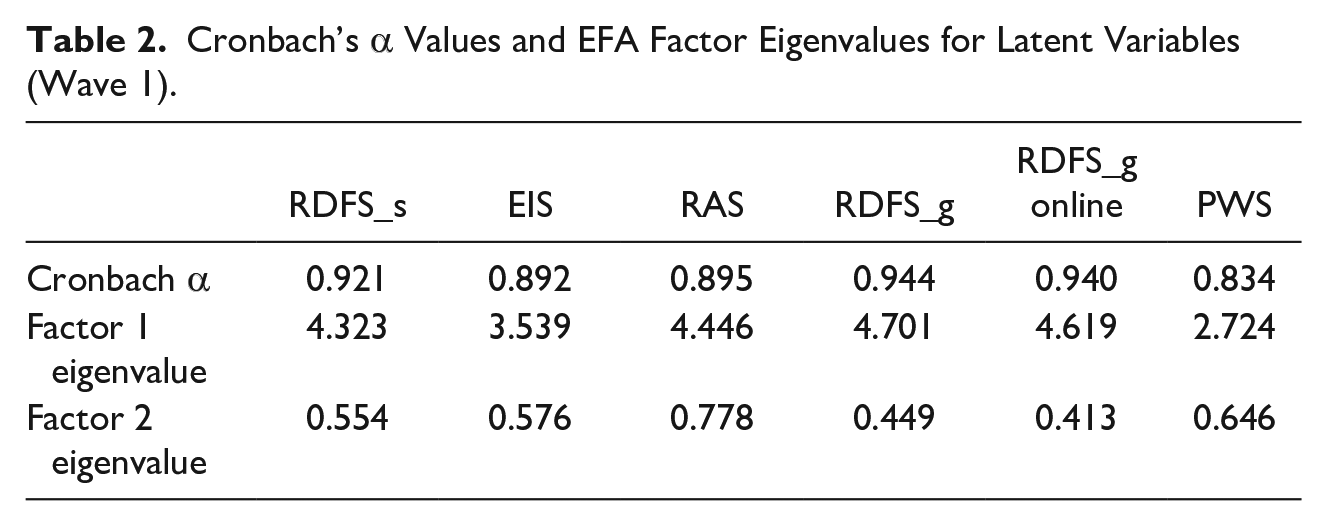
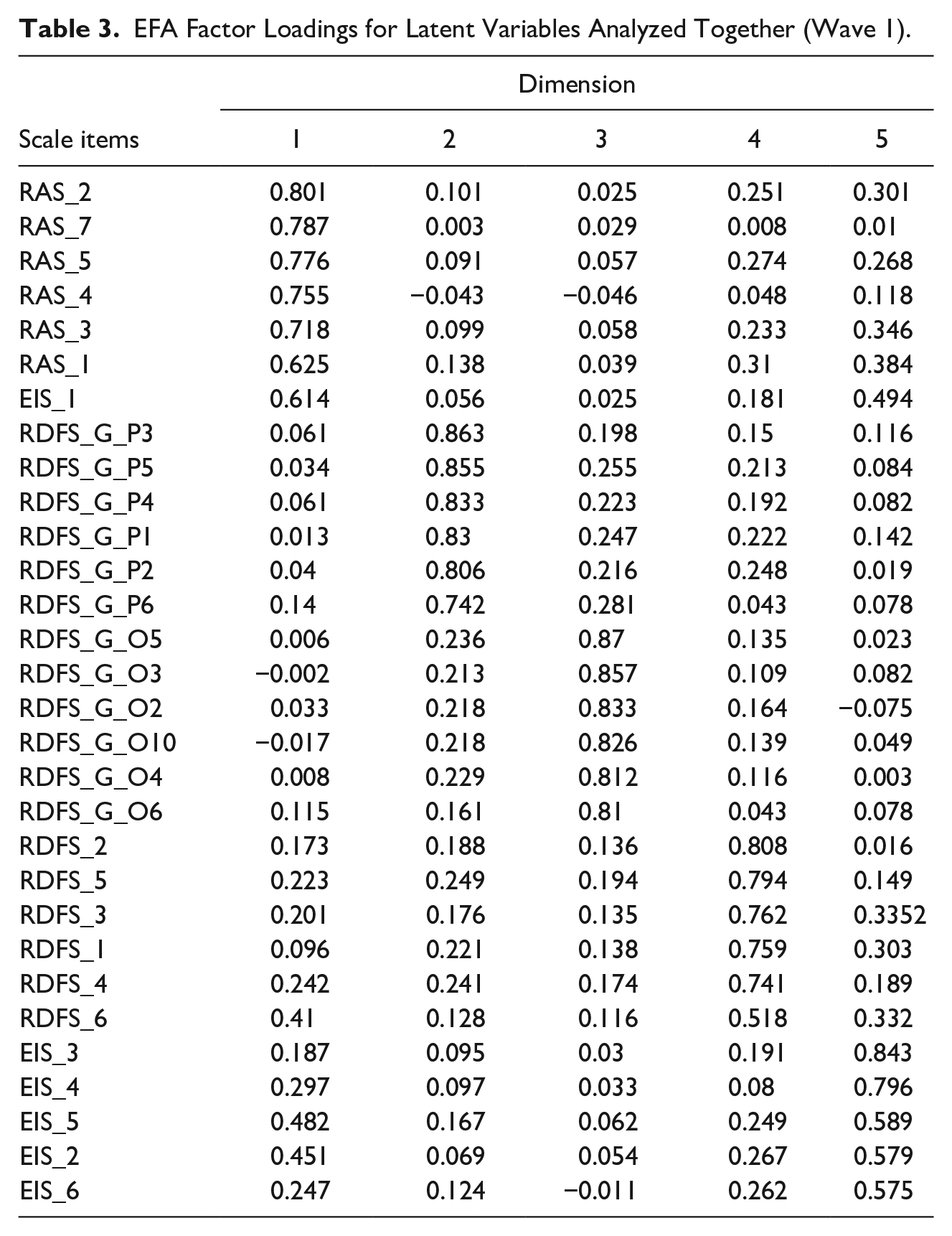
Table 2 presents the latent variables’ factor structures and internal consistency. All latent variables had satisfactory Cronbach’s α scores and were unidimensional, as no variable has an eigenvalue of 1 or more on the second factor. This indicates strong psychometric properties of all the latent variables. Following this, a factor analysis (EFA) was conducted across all 30 statements for the five latent variables. This produced five significant eigenvalues with the loadings shown in Table 3. Apart from a small overlap between one EIS statement in the RAS variable and one RAS statement in the EIS variable (both with the lowest loadings), the data indicate that there exists sufficient discrimination validity between the constructs.
Cronbach’s α Values and EFA Factor Eigenvalues for Latent Variables (Wave 1).
EFA Factor Loadings for Latent Variables Analyzed Together (Wave 1).
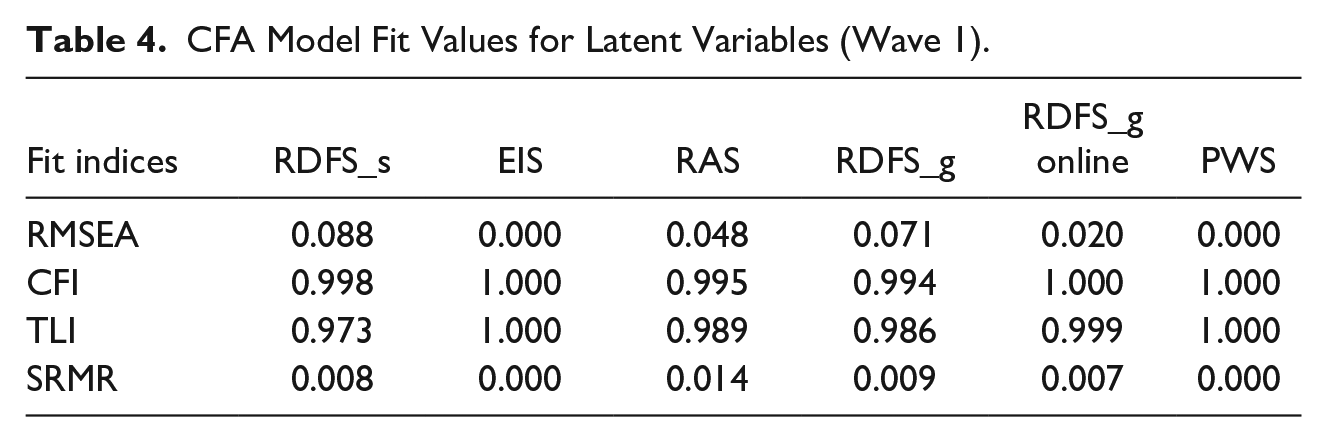
Following the EFAs, the CFA latent variables were created in MPlus using a Maximum Likelihood approach. The model fit statistics for each latent variable are shown in Table 4. Overall, the model fit figures were good. While a couple of the RMSEA figures (RDFS-s and RDFS-g) are slightly high, the other model fit indicators (CFI, TLI, and SRMR) are excellent for all variables (Hu & Bentler, 1999).
CFA Model Fit Values for Latent Variables (Wave 1).
Longitudinal invariance analyses are shown in Table 5. For all latent variables, there are no significant differences between the unconstrained model and the models when the loadings are constrained. Thus, all latent variables are metrically longitudinally invariant. The same is true for scalar invariance apart from the RDFS-s measure, which does show a difference. This difference occurs because the scores for the measure are lower in wave 2 than in either wave 1 or wave 3 (see Table 5). An analysis of variance test on the raw data showed that the size of these differences was not statistically significant, F(2,258) – 1.220, p = .296, and the ω2 effect size is 0.01 (a small effect; Field, 2009). Thus, overall longitudinal invariance can be assumed for the subsequent analyses.
Data Statistics (Waves 1 to 3).
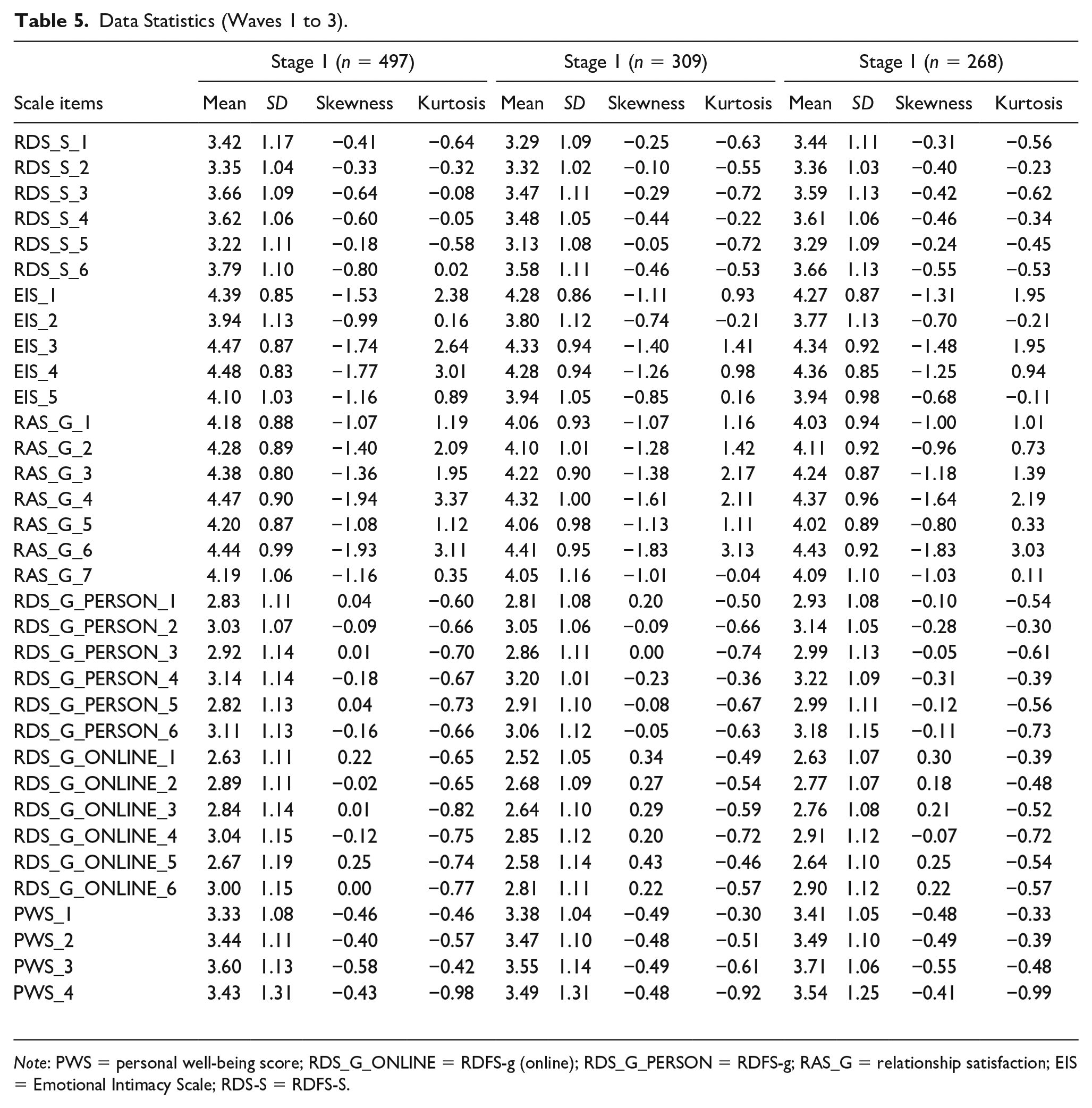
Note: PWS = personal well-being score; RDS_G_ONLINE = RDFS-g (online); RDS_G_PERSON = RDFS-g; RAS_G = relationship satisfaction; EIS = Emotional Intimacy Scale; RDS-S = RDFS-S.
Part 2: Lagged Regression Analyses (RQ2, RQ3, RQ4, and RQ6)
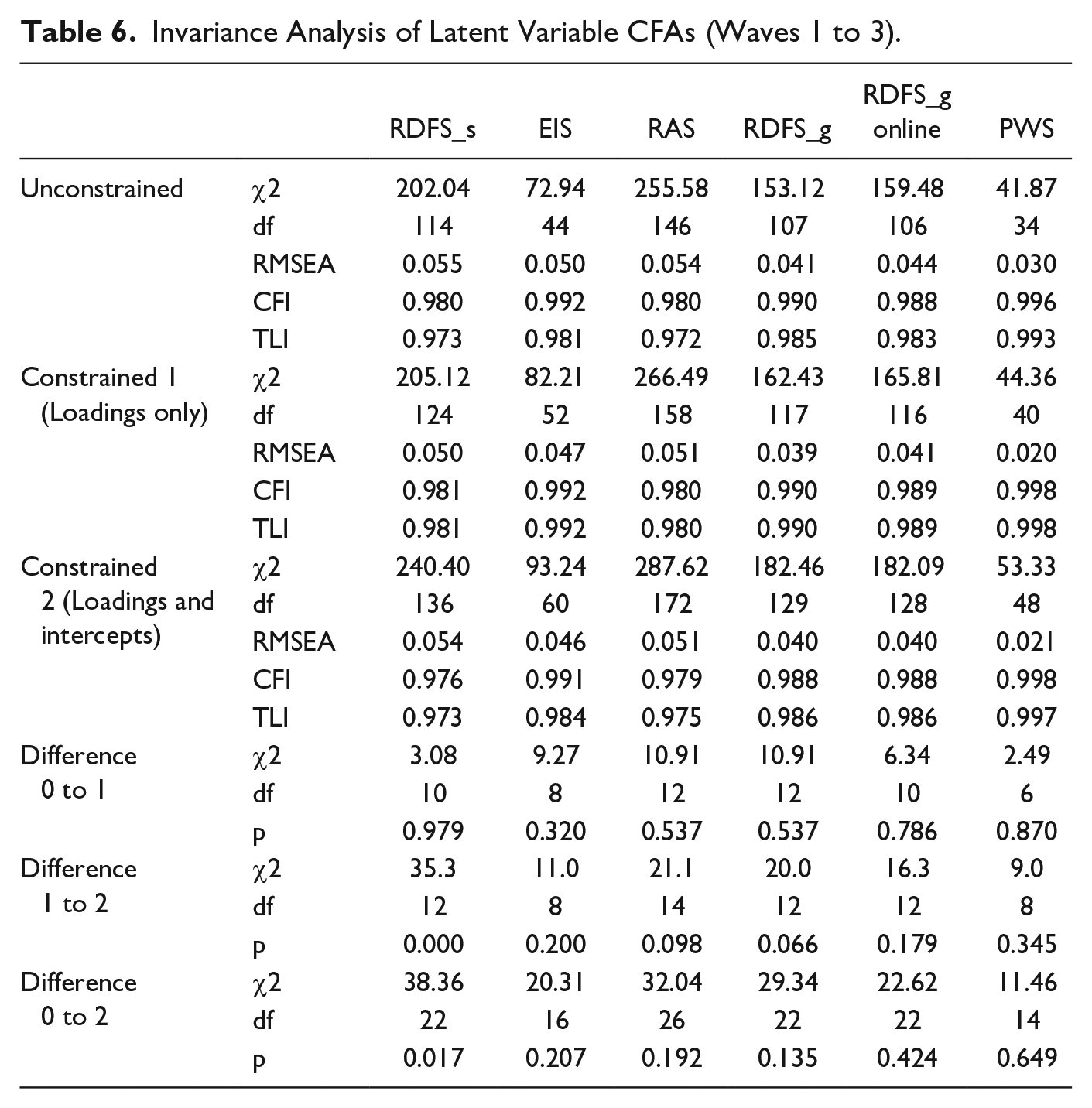
Assumptions of invariance are reported in Table 6. In addition to strong overall model fit figures, the difference between the constrained and the unconstrained CFAs is not statistically significant for any of the variables. This provides evidence of factor invariances for all the latent variables used in the modeling.
Invariance Analysis of Latent Variable CFAs (Waves 1 to 3).
Skewness and kurtosis data for all three waves are shown in Table 5. The skewness and kurtosis figures for all items are satisfactory (−2 < skewness < +2, −7 < kurtosis < +7) (e.g., Byrne, 2010; Hair et al., 2010), so normality can be assumed for creating the latent variables.
Lagged regressions are shown in Table 7. For ease of understanding, the table does not include the autoregressive figures (e.g., PWS at wave 2 on PWS at wave 1). As would be expected, all the autoregressive coefficients were significant with p < .001.
Lagged Regressions of PWS Predicted by Individual Measures of Connectedness.
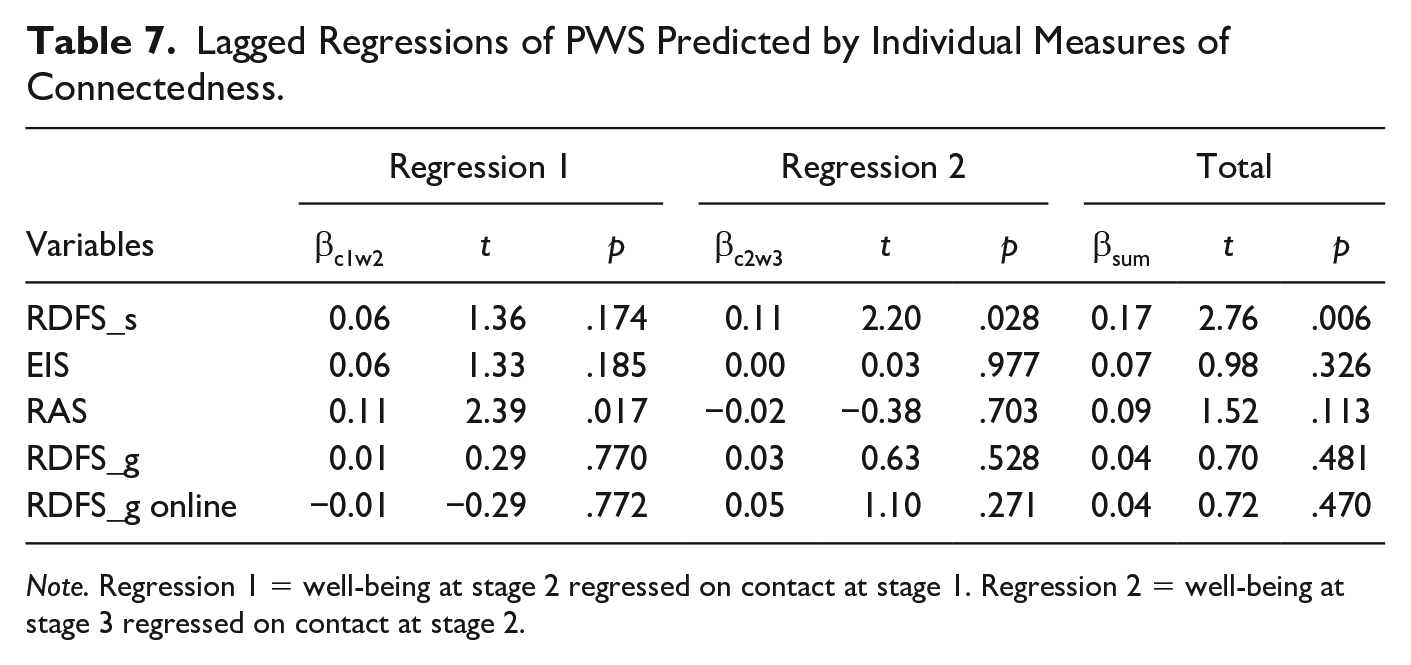
Note. Regression 1 = well-being at stage 2 regressed on contact at stage 1. Regression 2 = well-being at stage 3 regressed on contact at stage 2.
When looking at each of the relationship variables, combining the first regression (well-being at wave 2 predicted by connectedness at wave 1) and the second regression (well-being at wave 3 predicted by connectedness at wave 2), we found that RD in a significant relationship (RDFS-s) is a significant predictor of well-being (t = 2.76, p = .006). In the first regression only (well-being at wave 2 predicted by connectedness at wave 1), relationship satisfaction (RAS-g) is a predictor of well-being (t = 2.39, p = .017). Neither of the two new general relational depth measures created for this study (RDFS-g and RDFS-g (online)) were significant predictors of well-being.
Part 3: Moderation Analyses (RQ5)
The final analysis looked at whether or not either or both of the relationship closeness measures (EIS and RAS-G) moderated the impact of RDFS on PWS.
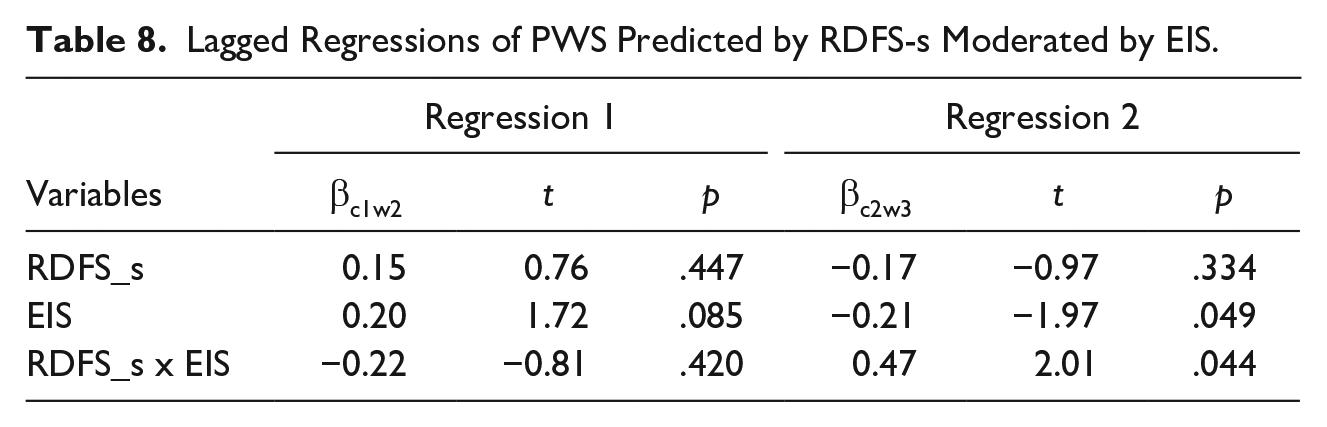
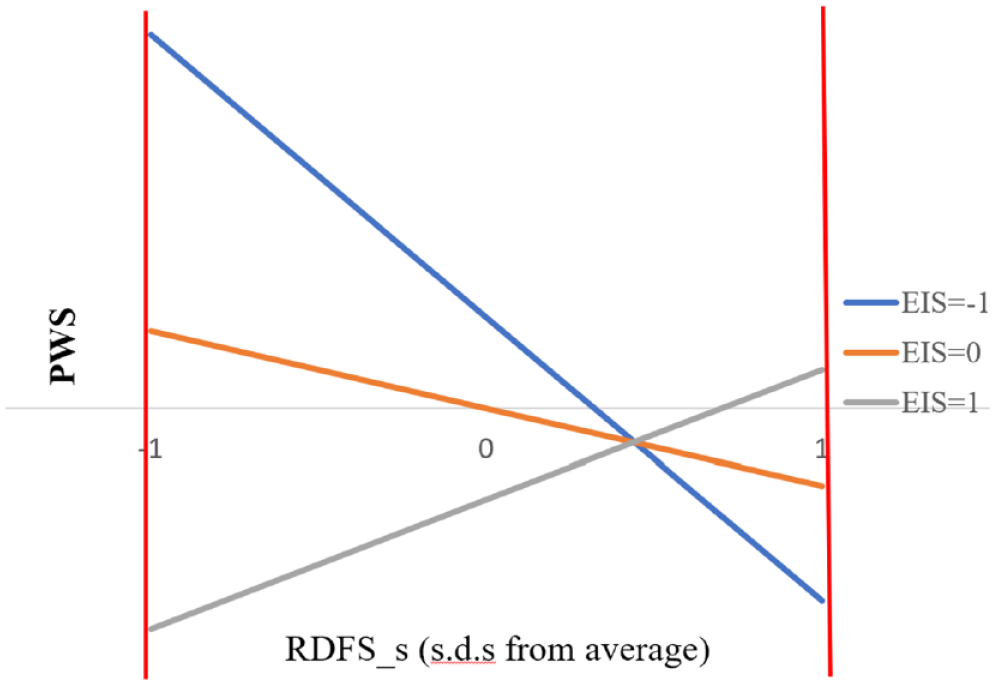
The first moderation analysis looked at well-being regressed on RDFS-s moderated by EIS. The results are shown in Table 8. As before, the table omits the autoregressive coefficients, all of which are significant at p < .001. The second of the two regression elements (well-being at wave 3 predicted by RDFS-s at wave 2 moderated by EIS at wave 2) shows a significant moderating effect. That is, the beta value for the moderating element (RDFS-s × EIS) is statistically significant (t = 2.01, p = .044). This result is shown graphically in Figure 3. This figure shows the relationship between RDFS-s and PWS for three values of EIS, when the closeness is low (EIS = −1 SD from its mean), when it is average (EIS = its mean), and when it is high (EIS = +1 SD from its mean). The blue line shows the relationship between RDFS-s and PWS when EIS is low, and the gray line shows the relationship between RDFS-s and PWS when EIS is high. It can be seen that when there is a low relationship closeness, then increasing the frequency of connectedness results in lower levels of well-being. Conversely, when relationship closeness is high, increasing the frequency of connectedness results in higher levels of well-being.
Lagged Regressions of PWS Predicted by RDFS-s Moderated by EIS.
PWS (wave 3) regressed on RDFS-s (wave 2) moderated by EIS (wave 2).
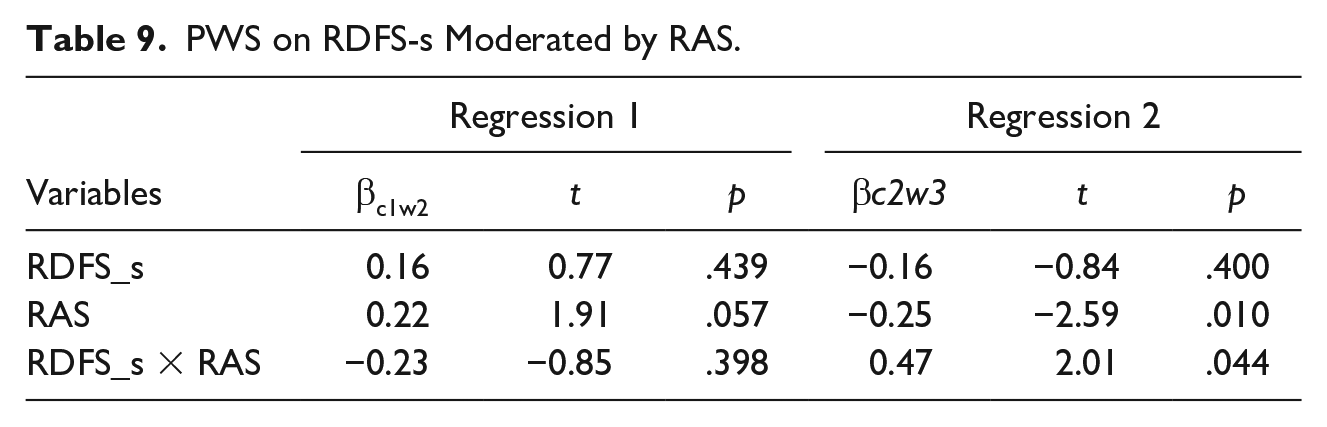
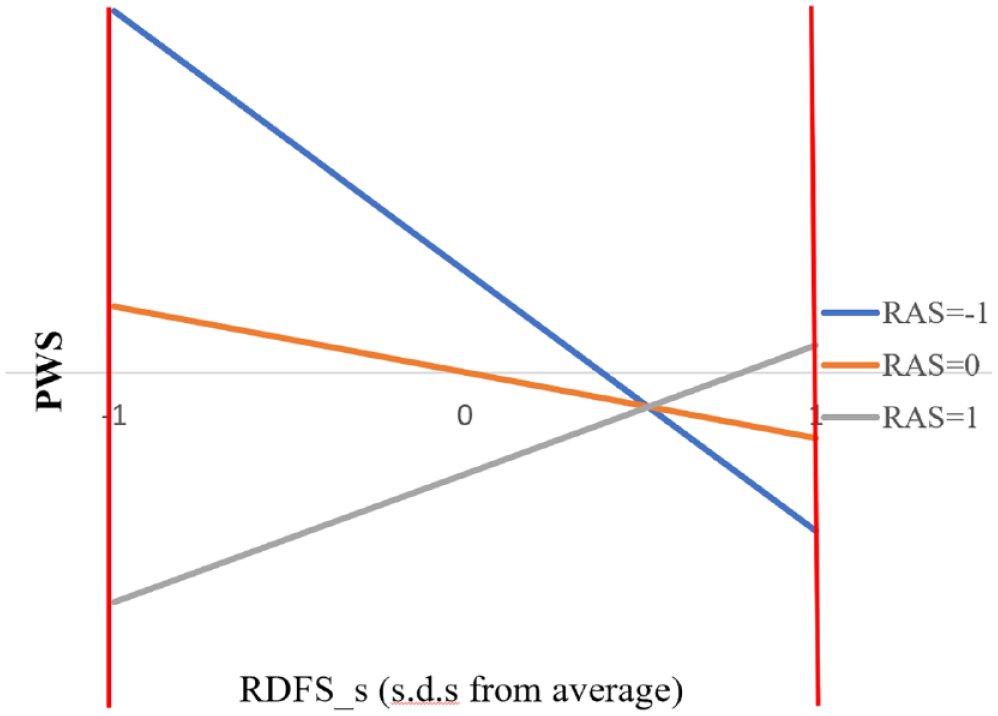
The same analysis was run looking at well-being (PWS) regressed on relational depth (RDFS-s) and moderated by relationship satisfaction (RAS). The results of this are shown in Table 9. The pattern of coefficients is the same as with EIS. The moderating value in regression 1 is non-significant, so it is only the second regression where the moderation effect is seen. Once again, this can be illustrated graphically (see Figure 4).
PWS on RDFS-s Moderated by RAS.
PWS (Wave 3) Regressed on RDFS-s (Wave 2) Moderated by RAS (Wave 2).
Discussion
The results provide further support for the hypothesis that RD can be experienced outside of a psychotherapy context and is a significant predictor of subjective well-being when assessed in relation to a selected close person in the community. There is no evidence to suggest that RD as experienced across all a person’s friends and contacts or with their contacts online, positively impacts well-being. In addition, although emotional intimacy does not directly impact on well-being, and relationship satisfaction does so only inconsistently across the three waves, both variables moderated the impact of RD on subjective well-being.
Findings from the present study suggest that the frequency of RD is a key construct that contributes to subjective well-being when experienced with a close other. This is consistent with preliminary findings from psychotherapy research that RD contributes to psychological growth (e.g., Kim et al., 2020; Knox, 2011; Wiggins et al., 2012), as well as evidence from the wider field on the association between social relationships and mental and physical well-being (e.g., Holt-Lunstad et al., 2010). Our data show, however, the specific importance of RD to day-to-day living. This is an important finding for the humanistic and existential field because of the centrality of relationality to our ontologies, theories of development, and conceptualizations of effective psychotherapy (Buber, 1958; Bugental, 1978; Hycner, 1991; Spinelli, 2015; Yalom, 2001). In much contemporary humanistic and existential thinking and practice, human beingness exists as a relatedness to others (as well as to our worlds). Our findings show that moments of deep relatedness with a significant other are, indeed, core to people’s psychological experiences of being in the world.
When individuals were asked about their experience of RD in relation to all people they knew, RD was not associated with more well-being. Similarly, RD did not impact on well-being when experienced with all people online. Overall, this finding supports psychology literature and suggests that it is RD with one close individual that is most significant for subjective well-being (be that a partner, close friend, or other significant person in the community), rather than the total sum of relationships (e.g., Tay & Diener, 2011). It is also aligned with Mearns and Cooper’s (2005, 2018) theoretical developments of RD in psychotherapy. However, while these findings support prior research suggesting that RD can be experienced in groups (Wyatt, 2012), in the context of symbolizing all relationships in one’s community, RD had no impact on subjective well-being.
We found that the closer the relationship—as assessed by higher levels of emotional intimacy and relationship satisfaction—the more RD impacts on well-being. Conversely, when there is less closeness in the relationship, higher levels of RD impact negatively on well-being. This would suggest that for RD to be effective in improving well-being, it is essential that it happens as part of a truly close and positive relationship characterized by high emotional intimacy and relationship satisfaction. These findings support the existing understanding of RD as an experience that is grounded in a person-centered, humanistic relationship characterized by empathy, genuineness, and warmth (Mearns & Cooper, 2005; Rogers, 1957). It is possible that without this grounding in a positive close relationship, RD is more likely to be experienced as risky (e.g., Knox, 2011). Thus, this study supports the assertion that the benefits of frequent RD come as part of an intimate and satisfying close relationship (e.g., Cornelius-White et al., 2018).
Limitations
Our findings are limited in several ways. First, while the findings clarify the temporal order of relational depth and well-being, they cannot wholly establish a cause-and-effect relationship as there may be other variables not included that significantly impact RD experiences. Second, while the study included emotional intimacy and relationship satisfaction as moderating variables, there may have been other covariates that contributed to associations between RD and well-being. Third, the multi-item scales used in this study were all selected for their brevity to limit participant fatigue; while this is a strength of the study, it balances with the limitations that such short scales may detect less variability within participants over time. It is thus possible that our results may not represent the full impact of these variables. Fourth, the self-report measures prompted participant recall over the past 2 weeks. Future studies need to examine associations between these variables and different recall periods. Finally, the study was based on a stratified U.K. sample and therefore findings can only be generalized to the U.K. population and need replicating in other countries to extend the findings.
Implications for Future Research, Practice, and Community Mental Health
This study provides initial support for the value of community mental health interventions that aim to strengthen RD experiences in close relationships. For instance, practices that facilitate RD could be taught to improve existing community mental health interventions in existing services (e.g., Iwano et al., 2022; Talk4Health, 2020). Our findings that emotional intimacy and relationship satisfaction are moderators of the impact of moments of deep connection also suggest the value of “ongoing” community group set-ups that continue to build and maintain close relationships. Findings from this study also suggest that one-on-one connection and pairing of individuals within a group setting may need to be prioritized over group-based activities. Further research should develop and evaluate new guidelines on RD training for use in communities. Relationality is a core element of humanistic and existential approaches, and our findings indicate the importance of this experience to emotional well-being beyond the psychotherapy context.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Open University Strategic Research Investment Fund.
Consent
Written informed consent for publication of their details was obtained from the study participant.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, GDM, upon reasonable request.