
Abstract
As they age, many seniors leave their homes to live in a seniors’ residence. Since those residences are both living environments and places where death happens from time to time, seniors who live there will be confronted to the loss of other residents. How is grief experienced by seniors in this setting? Research on this topic has been close to nonexistent. As part of a qualitative research project, we met 26 individuals older than the age of 65 years who had experienced the loss of another resident. Following our interviews, we conducted a thematic analysis of the data. Our results show that communication practices surrounding end of live and death vary from one seniors’ residence to the next. We highlight the strengths and limitations of these practices as well as their impacts on bereaved seniors. We discuss the ways in which our participants felt their grief was considered by others, look at the meanings of silence and communication and reflect on potential intervention strategies.
Keywords
Introduction
Transitions mark aging trajectories in more or less drastic ways. One of the changes seniors experience as they age is the transition to a new living environment. Many seniors leave their homes to move into what is commonly referred to as a seniors’ residence.
1
In Quebec, the Canadian province where this study took place, a seniors’ residence is defined as the whole or parts of a residential building occupied or destined to be occupied for the most part by individuals aged 65 and over and where the building operator offers, in addition to the rental of rooms or apartments, varied services included in at least two of the following categories, as regulated by law: meals, personal assistance, nursing, safety, domestic help and leisure activities. (Éditeur Officiel du Québec, 2018, p. 130)
Many efforts are made in these dwellings to help residents develop a sense of belonging and trust. Although these are living environments where many positive experiences occur, they are also places where death happens among the residents. For many seniors, this residence will be their last home, the last address of their trajectory (Alftberg et al., 2018; Komaromy, 2000). Consequently, older residents are often confronted with the loss of others. Death is a regular part of life in this setting. But what is known about the lived experiences of seniors who face this reality? A literature review shows that, despite the frequency of these losses, very few research projects have looked at the lived experiences of these seniors. A better understanding of this experience is key to supporting seniors in residence.
With this in mind, we led a qualitative research project in which we sought encounters with those who could tell us about this reality: seniors living in residence who have lost a fellow resident through death. In this article, we focus on the communication surrounding death and bereavement in seniors’ residences. Specifically, we consider the impacts that discourse and silence, which surround death and grief in seniors’ residences, have on their bereavement and reflect on intervention strategies.
Cultural Context: Aging, Death, and Grief
Denial and Fascination: What Place is Reserved for Death and the Bereaved?
To best understand how grief is experienced by seniors in residence, one must consider the broader context in which it occurs. In Canada, as in many Western societies, sociologists, anthropologists, and other scholars have, for many decades, noted that death is often kept under a veil of silence (Byock, 2002; Des Aulniers, 2009). They also note that, more recently, there is a certain fascination toward death, and more precisely, toward violent and spectacular deaths (Byock, 2002; Des Aulniers, 2009). Since these types of deaths are largely publicized, we could be tempted to believe that the denial of death has receded. However, when we observe the situation more closely, we find that underneath this fascination of “spectacular” deaths persists a certain denial of “ordinary” deaths (Byock, 2002; Des Aulniers, 2009). This denial of “ordinary” deaths is sometimes displaced toward the bereaved, who are invited to quickly “move on” and keep their experiences under a veil of silence. This led Jacquemin (2005) to state that, nowadays, we face a prohibition of grief. Given this background, we wondered how bereavement is addressed in seniors’ residences. Specifically, we wanted to know what attempts are made to facilitate communication in this context and which hurdles complicate it.
An Aging Process Often Refused or Idealized
If grief is prohibited, what becomes of aging? Better understanding how aging is perceived in the society where our participants live can help further illuminate their experience. In Canada and other Western countries, we observe many ageist behaviors and discourses (Charpentier et al., 2010; Lagacé, 2010; Nelson, 2005). Many people harbor a negative view of aging; they fight it and even adopt discriminatory behaviors toward seniors (Lagacé, 2010; Nelson, 2005). To explain the causes of ageism, terror management theory proposes that seniors can be perceived as a reminder of human finiteness (Martens et al., 2005). Depending on what we see when we look at them, older individuals would have the potential to trigger or revive existential anguish. Boudjemadi et al. (2015) propose that our reactions to seniors vary based on the type of aging we associate with them, such that we would react more negatively to seniors who evoke images of decay as opposed to those we associate with “idealized” aging. We then ask ourselves whether this also reflects the experience of older adults who grieve others in seniors’ residences. With death a more frequently confronted reality as we age, could senior residents be more likely to experience the type of negative reactions reported by researchers who study terror management theory? If that were the case, could it explain the tendency to ignore their experiences?
“Successful aging” models were developed in reaction to negative views of aging (Havighurst, 1963; Lamb et al., 2017; Rowe & Kahn, 1997). These models value a very positive vision of aging, defined as being in good health and remaining active and engaged in one’s community. Despite associated benefits, this optimistic vision of aging has the side effect of presenting aging only in positive terms. To overvalue the positive aspects of aging has the perverse effect of dismissing and, in some cases, even devaluing all that relates to a senior’s suffering, losses, and grief, even if these experiences are also an intrinsic part of what it means to grow older (Grenier, 2012; Lamb et al., 2017). We therefore wonder how these more positive visions of death and aging impact a senior resident’s ability and willingness to communicate their grief and how that grief is embraced by those around them.
Despite these sometimes polarized views, the experience of aging is more likely located between these two conceptions. The literature shows that seniors are often happy and that their experiences are not reduced to losses and hardship, while recognizing that these can be part of the overall picture (Baars, 2012). Lifespan perspectives highlight how aging is a process colored by transitions, which require adaptation and adjustment (Grenier, 2012; Hallberg, 2004). Theories of the life course, notably the concept of trajectory, present life as a process which generally includes several transitions and changes (Grenier, 2012). These perspectives suggest a more complete view of aging. One that is part of a much broader temporality: that of the entire human life. They also adopt a much more nuanced vision of aging, recognizing that this process encompasses suffering and joy, as well as reflecting on death and end of life (Baars, 2012; Hallberg, 2004). They propose that, by recognizing losses but focusing on transitions, the positive potential present in these experiences becomes apparent, perhaps even opportunities for growth, instead of just adverse impacts (Grenier, 2012; Hallberg, 2004). Our project allies itself with these more nuanced approaches to aging.
The definition of who qualifies as a “senior” has evolved over time and varies from one cultural context to the other. Chronological markers are often used to define aging. In Canada, 65 years is the age most often associated with the start of old age since individuals gain access to varied services and resources at that time. Yet with life expectancy surpassing 80 years old in several countries, gerontological studies now point out that aging experiences differ based on a person’s age group beyond the 65 years of age. The concepts of “third age” and “fourth age” 2 were developed to distinguish two groups of older adults who most often face very distinct realities (Grenier, 2012). While people in the “third age” category are generally healthy and often experience fewer losses, realities of the “fourth age” are different and often characterized by losses and illness (Grenier, 2012). Bereavement is thus recognized as most often experienced by the older group.
The Experience of Grief in Seniors Living in Residence
What is known about the grieving experience of seniors in residence? A review of the literature shows that very little research has investigated this reality. In fact, few studies have looked into seniors’ residences. Instead, most are concerned with the realities of long-term care and nursing homes, living environments which provide more extensive health services than what is offered in seniors’ residences. For example, some studies look into the grief experienced in nursing homes, whether by nurses and other professionals (Anderson & Ewen, 2011; Boerner et al., 2015; Chen et al., 2018; van Riesenbeck et al., 2015) or by loved ones and family members of the residents who pass away (Givens et al., 2011). We found one study (Choi et al., 2008) which considered the grief of residents in a nursing home and proposed a relationship between the suffering of some depressed residents and the frequent losses and reminders of death in their living environments. There is little information available, however, about how a resident’s death is experienced by other residents in the particular context of a seniors’ residence.
The few articles we did find on the topic of life in seniors’ residences highlight various aspects of this experience. It is recognized that many individuals live happily in seniors’ residences, but it can also be a trajectory colored in different ways by losses, transitions, and sometimes by deaths. The very decision to move into housing for seniors is often motivated by the accumulation of transformations and losses (Conlon & Aldredge, 2013; Oswald et al., 2007; Strohschein et al., 2011). In fact, seniors often move to residences precisely because they experience physical or cognitive losses, or because they are bereaved of a spouse and life at home is no longer possible or safe (Conlon & Aldredge, 2013; Wiersma, 2012). Therefore, when they decide to make this move, individuals are often already facing varied losses and are sometimes grieving (Conlon & Aldredge, 2013; Le Doujet, 2005). A seniors’ residence can then be perceived as a haven where one can seek refuge when losses and transformations accumulate. These changes often continue to accumulate during the transition which marks the move into a seniors’ residence. In fact, seniors will then confront leaving their home, which also, at times, implies leaving behind a neighborhood, a social network, and so on. The experience and accumulation of these different losses frequently revive memories of past setbacks and associated grief (Chróinín et al., 2011; Moon et al., 2011). A case study looking at one senior who moved into a seniors’ residence after losing his wife pointed out that support for the bereaved can be lacking in these living environments (Conlon & Aldredge, 2013).
While the move into a seniors’ residence can be the result or precursor of varied losses, it can also be experienced, in some instances, as an improvement. It can, for example, increase one’s sense of security, create opportunities to participate in varied activities (be more social) and decrease the weight of certain tasks. Whether it is experienced positively, with difficulty, or somewhere in between, living in a seniors’ residence can trigger existential reflections about the losses to come and, more broadly, about death. In fact, for many, seniors’ residences are looked on as a last home, the last place they will live prior to their death (Komaromy, 2000; Wiersma, 2012). For seniors, life in residence is, therefore, often associated with reflections about death, the end of their life, and their own finiteness. These reflections happen in a context where transformations are numerous and constant, where the seniors and those they live with are continuously aging, and thoughts on death and vulnerability are more salient.
A study from Komaromy (2000) suggests that seniors who face grief via the death of others in seniors’ residences can see thoughts about their own finiteness revived. This study, which looked at body disposal practices on the death of a resident, pointed out that the death of individuals in seniors’ residences, while relatively frequent, is often considered taboo, kept quiet and hidden (specifically when it comes to transportation of the body), in order to “protect” residents. Yet this attitude can have the adverse effect of indirectly communicating to residents that death is a topic that should not be discussed in those living environments (Komaromy, 2000). Although the author does not address it, we wonder, with Jacquemin (2005), if the weight of this silence might be transferred on the bereaved.
Theoretical Framework
Humanistic Psychology
Our project is rooted in humanistic psychology. Among key topics of interest, humanistic psychologists often pay close attention to intersubjectivity, historicity, temporality, authenticity, growth, and the potentialities of human beings (Cooper & Joseph, 2016; Moss, 2015). The goal of humanistic psychology: as seen by Bugental (1967), is “a complete description of what it means to be alive as a human being.” This goal [ . . . ] includes a description of man’s native potentialities- his growth, maturity, and decline, his interaction with physical and social environment, the range and variety of his experience, and his place in the universe. (Misiak & Sexton, 1973, p. 117)
In this sense, when we consider aging, humanistic psychology invites us to look at both the opportunities it brings about and the possible losses it entails. As we consider seniors’ growth, it compels us to consider the impact of their interactions with their social and physical environments (Baars et al., 2013). In a parallel process, qualitative research also takes into account a subject’s broader circumstances. In fact, there are many ties between humanistic psychology and qualitative research. As Levitt (2016) describes, The close ties between the humanistic worldview and qualitative ontology and epistemology have encouraged the development of these approaches. The strong connection between qualitative approaches and humanistic psychotherapies and psychotherapists can be traced to their foundational values, p. 82.
One of these shared foundations is the belief in the necessary intersubjectivity of human interactions. Specifically, it is thought that all meetings between two individuals produce a field in which the subjectivity of one impacts the other, and vice versa (Buirski & Haglund, 2001). In a research setting, thinking intersubjectively means thinking about the ways in which we approach relationships with our participants and what may limit these relationships. It also means reflecting on our presuppositions and their influences on our perceptions. This way of thinking is relevant when we conduct interviews to collect data which will then be coconstructed (Paillé & Mucchielli, 2012). As for our interest in temporality, is it linked to our viewing grief as a process rather than an event, such that it evolves over time and is marked simultaneously by the past, the present, and the future?
Narrative Identity and Humanistic Psychology
In line with this humanistic perspective, this article also relies on the concept of narrative identity. Telling one’s story is a process which allows individuals to better understand themselves, make sense of their experiences, remember, and organize live events and integrate diverse thoughts and emotions (Pennebaker & Seagal, 1999). Various authors have thought through the processes of narration and the self-narrative. Their research and writings show that there are benefits to telling one’s story orally or in writing, in terms of better physical and mental health (increased ability to cope with adversity, opportunity to make sense of one’s experiences, etc.; Pennebaker, 2000; Pennebaker & Seagal, 1999). It is with those benefits in mind that we choose to focus here on what is at stake when it comes to communicating about one’s grief in seniors’ residences. Ricoeur (1988) and McAdams (2008) developed the concept of “narrative identity,” an identity made up of stories coconstructed with others: Ricoeur proposed that narrative or story is the linguistic form that least distorts temporal experience. From the perspective of humanistic psychology, the basic plot of people’s life stories is about their struggles to actualize their inherent potentials. He believed that a dynamic relation holds between life as narratively emplotted and life as lived. (Polkinghorne, 2015, p. 100)
These stories call on temporality; they are woven from both reconstructed stories from the past and an imagined future (McAdams, 2008). They are also closely linked to our relationships to others. However, relationships change over time, sometimes growing and multiplying but at times also becoming more restricted and ending, such as when death occurs.
Death and Dying
Death is an event which leaves an imprint in an individual’s life story. Indeed, Jankélévitch, (1977) reminds us that death “in the second person,” that is, the death of the other, of a loved one or of a person we were close to and which generally brings about grief, will often impact our story. The death of another can lead us to think more broadly and color our thoughts about our own future and finiteness (Yalom, 2008), which Jankélévitch (1977) calls death “in the first person.” Moreover, Feron (1999) says that the death of the other acts as a royal road to access the meaning of death, thereby highlighting its intersubjective dimension.
But what is grief? This experience can be described in different ways and refers to varied types of losses, both human and material 3 (Hooyman & Kramer, 2006). In this article, we talk about grief in reference to the loss of a loved one who dies. In this sense, grief can be described as a major disturbance which can have significant impacts on the well-being of the bereaved (Steffen & Coyle, 2011). Several theoretical models of grief have been formulated over time. While many of the initial models describe grief in terms of rather linear steps, recent ones propose that grief is experienced as a nonlinear, even oscillating, process. Yet other models explore how this process can lead to growth and meaning making (Hooyman & Kramer, 2006; Neimeyer et al., 2014), thereby reminding us that grief is not a solely negative experience. It can also, in fact, be looked at through the lens of meaning as proposed, among others, by Neimeyer et al. (2014). This psychologist’s therapeutic vision for those who are bereaved aims not only to reduce acute symptoms of grief but also to engage in a process which guides the reconstruction of meaning and encourages broader reflections about the meaning of loss, and of life itself (Neimeyer et al., 2014).
While grief can appear to be a universal experience, cultural influences are observed. For example, the communications and rituals that surround death vary from one culture to the next (Hooyman & Kramer, 2006). In occidental traditions, therapy offered to the bereaved is often oriented towards discussion and the expression of emotions. While this seems beneficial to many, all cultures do not value the same forms of communication in bereavement (Hooyman & Kramer, 2006).
Other elements impact bereavement. Notably, some researchers have observed that socio-economic factors can influence the level of distress associated with grief. Some studies, which did not specifically consider the experiences of seniors, show that having a low income decreases one’s likelihood of having access to sufficient sources of support, while increasing chances of facing additional difficulties and experiencing protracted grief (Cacciatore et al., 2016; Ngwu et al., 2018). These studies also highlight that lower levels of education and family income can increase the risks of developing symptoms of an anxious, depressive or posttraumatic nature as well as intensifying bereavement (Cacciatore et al., 2016; Ngwu et al., 2018).
Following a loss, the bereaved’s relationships to others also play a crucial role in the actualization of grief’s meaning making potential. In fact, social support and acknowledging the loss both contribute to a healthy bereavement journey (Azaiza et al., 2011; Hooyman & Kramer, 2006). Conversely, a lack of support and a denial of one’s loss can contribute to grief being more complicated. It can then evolve into pathology and diverse types of suffering, in some cases leading the bereaved to commit suicide (Azaiza et al., 2011; Elwert & Christakis, 2008; Hansson & Stroebe, 2007). Since individuals who live in seniors’ residences are surrounded by many people, we are tempted to believe that they have easier access to support. However, death in a seniors’ residence can be imbued with taboo and a heavy silence which, on the contrary, leaves the bereaved alone with their suffering (Bacqué, 2004).
Methodology
Our main objective was to better understand how individuals living in seniors’ residences experience bereavement following the death of a fellow residents. Our subgoals were to better understand: (1) the nature and recognizable signs of this type of grief, (2) the suffering potentially inherent to it, (3) what provides relief to the bereaved in this context, (4) what complicates this experience, and (5) how communication practices in the residence setting impact bereavement. This research project was financed by the Fonds Québécois de Recherche Société et Culture.
Qualitative Research Method: The Art of the Encounter
This research is qualitative. Qualitative research methods can be described as an “art of the encounter” (Jeffrey, 2005, p. 117). These research methods aim to understand, in-depth, certain phenomena and lived experiences by questioning both the relevant theories on the topic and the people who have lived through the experience of interest. This method of accessing knowledge recognizes a person’s ability to give meaning to their experiences by analyzing or interpreting them in collaboration with the researcher (Levitt, 2016). This view is in line with our humanistic approach and our decision to give voice to seniors, and to cross-reference their testimonies with existing literature on this topic.
Sample
We developed our sample according to the nonprobabilistic method of convenience sampling (Salkind, 2010). Qualitative research approaches emphasize deepening rather than multiplying the collection of life stories (Denzin & Giardina, 2008; Denzin & Lincoln, 2008; Merriam, 2009). The end of recruitment was decided in accordance with the richness and breadth of the narratives collected during our interviews, as well as the diversity of testimonies and issues that were brought up by participants. To be included in the study, participants had to be 65 years or older, live in a seniors’ residence, have experienced the passing of a person living in the same residence within the past 5 years, speak English or French, and be able to provide informed consent.
We met with 26 seniors (25 women and 1 man) who matched our inclusion criteria (see the appendix). The participants lived in 12 seniors’ residences in Montreal (in the province of Quebec in Canada) and were 65 to 95 years old, with an average age of 79 years old. They had lived in the same residence setting between 3 and 55 years. 4 The majority (24) were originally from Canada, while two were from other countries (1 Mexico, 1 Venezuela). The majority (20) identified as Christian (18 Catholic, 1 Lutheran, 1 Pentecostal), while others identified as Jewish (1) and Agnostic (1). Three participants believed in God but did not identify with a specific religion and one participant did not answer the question on religious belief. Their level of education varied from having completed elementary school to postdoctoral studies. Their income levels varied, with participants reporting incomes between CA$10,000 and CA$20,000 to incomes over CA$90,000. The average income level was between CA$30,000 and CA$40,000. 5 Fifteen participants had children. Nine were widowed, 5 were divorced, 2 were married, and 10 participants were single.
Data Collection: Semistructured Interviews and Sociodemographic Questionnaire
Research Assistants conducted semistructured interviews lasting between 1 and 2 hours, depending on the participant. At the start of each meeting, the Research Assistant presented a summary of the project and verified whether the person was willing to take part in it. When in agreement, participants were asked to read and then sign a consent form 6 .
Interviews were conducted using a grid composed of open-ended questions which touched on the key themes of the project (what factors contributed to the grieving process, the particularities of going through this experience in this setting, the role played by residence personnel, etc.). In order to avoid skewing our results toward the sharing of negative experiences, we made sure to question participants both on what made grief easier to go through and what made it more difficult. At the end of the interview, participants also filled out a short sociodemographic questionnaire with close-ended questions.
Thematic Analysis of the Data
We performed a thematic analysis of the data (Paillé & Mucchielli, 2012). This type of analysis accurately reflects the data by focusing on description rather than interpretation (Paillé & Mucchielli, 2012). This analysis was carried out in steps. Initially, the research team (two Research Assistants and the main researcher) immersed themselves in the data from the first five interviews (Tracy, 2013). Each person analyzed these five interviews independently and wrote a first draft of themes representing the main ideas contained in each interview. A meeting was then held where team members created, based on these individual lists, a preliminary list of themes and rubrics which was used to design the first version of the project’s thematic map.
Next, the team randomly selected five more interviews which were coded separately by each team member, this time using the thematic map as a guide. We then met to compare the results of this intercoder reliability process. For every occasion where coding results differed among team members, a discussion ensued until a consensus was reached. This process allowed us to agree on the final version of the project’s thematic map and to validate how we were using it. This map was then used by the Research Assistants to code the remaining interviews. Once all interviews were coded, we refined our map by grouping themes (the context in which death took place, the way death was announced, reactions to loss, etc.) into rubrics, which we then analyzed one at a time.
To ensure our analysis was valid and rigorous, we respected principles set out by Paillé and Mucchielli (2012); including rootedness, exhaustivity, completion, accuracy, communicability, and conservation. All members of the team took part in all steps of the analysis, which further enriched the validity of the process through crystalization (Merriam, 2009).
In this article, we present the part of our thematic analysis which focuses on what our participants shared about the communication practices surrounding death and bereavement in seniors’ residences and their impacts on grieving.
Results
The testimonies reveal that communication issues are central to the experience of death and grief in seniors’ residences. We investigate these issues and their impacts on seniors’ grief by analyzing: (1) the impacts of communication practices on the bereaved during end of life and death, and (2) the strengths and limitations of communications with the bereaved.
The Impacts of Communication Practices on the Bereaved During End of Life and Death
Advantages of Information Sharing When a Person Is Nearing End of Life or at the Time of Death
Information sharing practices colored the experience of the bereaved seniors at the time of death and its announcement. We noted that these practices vary from one residence to the other. In some places, the death of a resident is announced through multiple methods of communication such as a newsletter or a notice board. However, information sharing practices were very different in the context of a Catholic religious congregation. In this setting, announcements were numerous, diversified, and began as soon as the person was at the end of their life. Jeanne testified to this reality: I find that extraordinary, here. At some point, a list is posted in the dining hall: “Sisters are needed to watch over so-and-so.” I went, in fact, to spend time with the Sister who died recently. I held her hand and from time to time I talked to her because I know she trusted me. (Jeanne, 75 years old)
This way of dealing with death seems to facilitate the experience of loss for other residents, as they can accompany the dying and assimilate more gradually the news of their end of life.
When Silence Surrounds a Resident’s Death: The Bereaved’s Questions
In contrast, in other locations, the announcement of the death takes place many weeks and even sometimes months after the fact. Consequently, during this time some occupants do not know what happened to their friend or neighbor and a long time can elapse before they find out they are dead. This can generate suffering, questions, or lack of understanding.
In some residences, the silence which surrounds the death of a resident is opaque and questions remain unanswered. In this context, residents do not know that someone is at the end of their life or that they have passed. As a result, when individuals no longer show up for activities or meals, their fellow residents ask themselves: Did they die? Are they hospitalized? What happened to them? Another man, my next-door neighbour [ . . . ] I don’t know if he is dead. [ . . . ] They brought him by ambulance and didn’t bring him back. The man didn’t come back. (Maria, 65 years old)
When the relationship to the person who left, and whose condition is uncertain, was not close, participants do not necessarily feel distressed, but questions still remain unanswered. In other cases, especially when the relationship was closer, this silence and the ensuing mystery proves hard to deal with: I spoke to the Director . . . I asked why she didn’t say something . . . I told her that we find it hard. . . . It was someone who lived with us and we can’t know . . . If we were members of the family, they would tell us. . . . She said that was exactly the issue, that they hadn’t been able to reach the family, so they didn’t want to get in trouble . . . (Carmen, 78 years old)
The following quote from Robert shows that silence can be part of the institutional norms in seniors’ residences, or is perceived as such: The policy here is that they don’t tell us . . . [ . . . ] I think they should tell us when somebody goes to the hospital but no, they don’t . . . If a person goes to the hospital and dies there, they don’t tell us . . . [ . . . ] It bugs me because I would like at least to know that they are in the hospital . . . to support them if I’m able . . . send them a card or a flower at least [ . . . ] (Robert, 89 years old)
Even if many interpret the administration’s silence as caring (to avoid making them sad or anxious, e.g.,), some are upset by it. Not knowing makes it impossible to support the person when they are at the end of their life, to say goodbye, or even to simply be able to manifest their affection through a simple gesture.
Discomfort Toward Death in Some Residences: What Message Is Communicated to the Bereaved?
There seems to be a lot of discomfort toward death in some settings, as we can see from Alice’s testimony: The Director talked to us a few months ago [when someone had died] . . . Asked us as much as possible not to talk about it . . . [ . . . ] To try . . . life continues . . . right? She never talked about it again . . . (Alice, 95 years old)
In this case, silence is imposed from the outside. This injunction perpetuates a discomfort which further weighs down the silence that already often surrounds the period following death. We also note that this silence or discomfort is influenced by the cause of death. Thus, when a resident, for example, commits suicide, the silence and discomfort seem even more powerful.
One participant, while labelling as taboo the discomfort, which surrounds death in seniors’ residences, notes that the silence can also be assumed by the other residents: Taboo, I think it’s a taboo . . . People don’t talk about it . . . [ . . . ] I don’t know if it’s because they are all afraid of dying . . . I don’t know, but in any case, it is a subject surrounded by a taboo [ . . . ] People act as if you need to be insensitive . . . Listen, we can’t be impassive with regards to this . . . (Josée, 67 years old)
We see from Josée’s testimony that silence does not sit well with everyone.
Strengths and Limitations of Communications With the Bereaved
Origins and Impacts of the Silence Surrounding the Bereaved
Does the silence we sometimes observe around the end of life and the announcement of the passing transfer to the bereaved? Participants revealed that communication is a complex aspect of bereavement in seniors’ residences and that silence sometimes encompasses their experience. For some, this silence is chosen and holds protective value: [ . . . ] I isolated myself, for almost one month. I had to go through it in my own way. So, I did not go out through the main entrance, rather I exited on foot through the garage [ . . . ] I did not want to see anyone. They all would have asked me, out of kindness, how it happened, how he died, what he died from. I didn’t want to go through this. So, I went through my grief alone. (Renée, 87 years old)
Like Renée, some participants choose, at some point during their grieving process, to avoid conversations about their deceased loved one: “I didn’t really like to hear people talking about it . . . When I’m really sad about someone’s death . . . I prefer others don’t talk to me about it . . . ” (Carmen, 78 years old). Silence can, therefore, be appreciated by those who prefer the process to be more intimate.
However, some participants explained their desire to open up to others and the benefits that accrue from those discussions when they are possible. That’s the case for Irene, who lives in a complex housing a religious congregation: Listening to each other helps a lot and praying together. Then there are the testimonies others give, sometimes at the dining table. They give testimonies that affect us, about the person who left. Whoever we are, we are moved in moments like that. (Irene, 81 years old)
Communicating About Grief: Limitations of Brief and Fact-Based Conversations
Communication is not always possible and when it is, it is often brief and short-lived: Usually in the whole group it goes a bit unnoticed . . . It doesn’t take long to fade away . . . Two, three days, then we no longer hear about it. . . . There is the announcement on the board . . . [ . . . ] their apartment is rented . . . and that’s it, there is a renewal . . . Life continues . . . (Alice, 95 years old)
In this case, even if communication channels open temporarily, we note that silence rapidly masks the experience of grief. Many participants reported that discussions about grief were short, few and far between, and often only descriptive or factual in nature: They don’t talk about it much. They’ll announce it . . . but that’s it . . . [ . . . ] One person who plays sandbags with me said, “Mrs. L. passed away.” I said, “Yes, I heard.” Then she said, “I’ll go to the funeral.” . . . That was it . . . (Irene, 81 years old)
Descriptive discourses are often based on fact-sharing rather than talking about how grief is experienced. They leave little or no place for emotions, as noted by Andrée: We talked about her at the dining table. But we talked about what she had done during her life. This thing, that thing, that was the whole conversation [ . . . ]. It’s really rare that we would talk about how we feel about it, that’s not customary. (Andrée, 75 years old)
For those who wish to share their more intimate experience of the loss, the space allowed for that type of discourse is often restricted, even nonexistent. Many participants mentioned their desire to see a better balance between the communication and silence which surround death and grief: I try to be serene about it [the loss], because it’s easy to be influenced by it, to focus on it as if it was the only thing going on. But there are other things, current events. . . . When it becomes all-encompassing, I try to talk about other things. (Jeanne, 75 years old)
Silence is, therefore, not always a source of suffering, especially when there is a certain balance between communication and silence. Many residents would like to talk about their grief but do not want this topic to dominate all of their conversations.
Talking About the Death of the Other and Reflecting on Your Own Finiteness: When the Death of Other Residents Resonates With Your Own
For bereaved residents, the death of others sometimes evokes reflections about their own end of life and finiteness. Some try to avoid discussions about their grief, and that of others, to refrain from thinking about their own death: “You know, we’re aware that we’re on our last stretch, but as much as possible, we prefer not to think about it, because it would ruin our current life” (Rita, 83 years old). Others make a direct connection between the death of those around them and their own end of life: When I saw the paper on the wall, informing us that she was dead. . . . The picture and all [ . . . ] It hurt me, it hurt me a lot . . . I can’t tell you why [ . . . ] It explains the coexistence, because there is coexistence. So, I tell myself, I’m next! (Maria, 65 years old)
One participant inferred that she, too, could die in the same way her neighbor died: “What did I learn from it? That I could maybe die alone” (Germaine, 94 years old).
The fact that little space is granted to communication on the topic of death and grief can have the perverse effect of spreading the idea that the relationships among residents are not important or acknowledged: “I said, don’t you realize that this woman was well liked by people?” (Lucie, 70 years old). This reality can also involuntarily give the impression that the deceased was not important and is easily replaced, which causes some people to reflect on their own importance and what will happen when they pass away: “They will talk about it a bit, you know [ . . . ] but . . . it will be forgotten. You don’t make your mark . . . ( . . . ) You know, you leave, you are replaced.” (Paulette, 79 years old). Conversely, we see that deeper and more open communications could carry the implicit message that the deceased was indeed important, which could also be interpreted as a sign of solidarity and the acknowledgment that all residents are important and valued.
Discussion
[ . . . ] what image best represents the loss you experienced?
It’s like a [ . . . ] block which detaches itself from the building and you have to [. . .] strengthen ties, rebuild, so the entire building doesn’t collapse. [ . . . ]. We have to stand together, help each other. (Andrée, 75 years old)
The solidarity evoked in this excerpt reinforces the importance of social support during periods of bereavement. The metaphor of a building being reconstructed with materials composed of relationships with others is particularly meaningful. Even if this support can manifest itself in ways other than speech (through gestures, presence, etc.), communication is often the preferred way to process grief. Many humanistic psychologists remind us that dialogue allows us to tell our stories and integrate the loss into our evolving narrative (Neimeyer et al., 2014; Polkinghorne, 2015). This idea is, in fact, a fundamental part of many grief therapies. As Feron (1999) explains, The death of another needs to be told: the other, which is being erased by death, still speaks and confides in me. That is why death needs to be told, not only as a necessity to remember someone who is disappearing, but also as an imperative to name a relationship becoming undone. (p. 127)
Our research shows that the space granted for dialogue about death and grief is not the same from one residence to the next. At times, grief and end of life are integrated into daily life and exchanges, as we noted through some testimonies collected in a complex housing a religious congregation. However, silence, either partial or complete, often hangs over the reality of grief and death in those environments, an observation which converges with Conlon and Aldredge’s (2013) case study and with Komaromy’s (2000) finding that silence can surround death in seniors’ residences. This silence is appreciated by some but causes suffering to others.
From a humanistic perspective, and when we consider the concept of narrative identity mentioned earlier, we wonder: how can we tell our story when the love and friendships in our living environment are not recognized? When we do not even know what happened to our loved one? How can we integrate this event into our narrative and what impacts does this have on our own identity and vision of our own death?
Our participants confirm that the death of the other, death in the “second person,” often revives thoughts about their own death, what Jankélévitch (1977) would call death “in the first person.” Sometimes, even if the relationships between residents and the deceased were not close, their death brings about a type of proximity. As Feron (1999) explains, Every man who dies, given that he is dying, already becomes close to me. It is this proximity which explains the emotion we can feel when someone we don’t know passes away. (p. 115)
How do these deaths in the “second person” influence the vision of death in the “first person?” For some of the seniors we met, the silence surrounding the death of others evoked doubts about their own value as a person living in residence and the value of their relationships to others. It also generated worries about what would happen to them at the time of their own deaths. This type of suffering could very likely be lessened if a space for dialogue or recognition were available to those who wish to talk about their experiences of bereavement. The example offered by participants from the religious congregation illustrates such a space, where communication about death is promoted and expected. However, as we pointed out, the range of topics accepted by that group appeared rather narrow. As such, even if conversations seemed open about some dimensions of the experience, such as the need to notice the loss, announce the passing, and pay tribute to the deceased, it remained closed to other dimensions such as the emotions experienced, and the personal and existential meanings which the death of a friend or colleague can evoke.
Even if they are at times rather upset with the silence of administrative staff, many residents understand this silence is meant to protect them from feelings such as anxiety or depression. In some ways, it is not very surprising that people would be uncomfortable addressing death in the context of seniors’ residences, where the focus is often on promoting safety, well-being, and happiness. This coincides, in part, with Komaromy’s (2000) and Conlon and Aldredge’s (2013) findings. Does the protection offered by this setting refer, in people’s imagination or in more concrete ways, to the desire to postpone or even completely avoid death? Silence can suit some people. However, adopting it outright and not leaving space for communication when it is needed seems to cause suffering to others.
No matter how old we are, talking about death is, admittedly, anxiety-provoking (Heidegger, 1986; Yalom, 2008). Many scholars remind us that death is one of the great “existentials,” which can be veiled in our day-to-day life to avoid anguish (Heidegger, 1986). However, when the veil becomes more opaque and stifling, it can obstruct a more authentic reflection about death and thereby bring about suffering. Several studies show that seniors are more inclined to think about death and that this is not necessarily a source of anxiety for them. In fact, as Baars (2012) points out: In transforming the awareness that our lives are finite into an inspiring perspective for aging [ . . . ] every moment gets a special depth and every life a quality of uniqueness because our times are finite. (p. 236)
Thus, reflections on death and dying can be serene and even contribute to a senior’s developmental trajectory (Baars, 2012; Baars et al., 2013; Hallberg, 2004). Of course, ultimately, no one can shelter themselves from death and its reality looms larger in old age. Since no one can avoid death and its inevitable approach, should not we open a creative space for discourse for those who do want to think about it or try to find meaning in their end of life, and even in their death?
Limitations and Next Steps
Although this study has contributed to understanding the experience of bereaved seniors, it has some limitations with regard to sampling. Since only one man took part in the study, women make up the vast majority of our participants. Our difficulties in recruiting men reflect, in part, the fact that men are few and far between in Quebec’s seniors’ residences (Ministère de la famille, 2018). A comparative study featuring equal numbers of men and women would be of interest, as it would take into account the influence of gender on the experience of grief in the context of seniors’ residences. It is also possible that men’s needs when it comes to communication could be different, so this would be a worthwhile question to explore. In addition, our sample is primarily composed of individuals born in Canada and identifying as Christian. Knowing that cultural and religious characteristics influence manifestations of grief as well as the communications which surround it (Hooyman & Kramer, 2006), it would be quite relevant to investigate how these factors impact communication between seniors from diverse cultural and religious backgrounds who live in the same seniors’ residence.
Although studies have shown that low incomes can adversely impact grief, our participants did not identify their relatively low income levels as a source of the difficulties they faced during their bereavement. It would, however, be interesting to explore the impact of diverse economic situations on the experience of grief in seniors’ residences.
Practical Implications
The testimonies highlight how specific communication practices can facilitate the grieving process when a death occurs in seniors’ residences. Holding discussions with residents about grief and end of life could help resolve a number of potential issues. Best practices can be implemented to facilitate such discussions, including offering adequate training to staff in this regard (Alftberg et al., 2018). Another avenue to consider is for staff to consult residents and obtain their consent to allow for more seamless information sharing in the event that their health should deteriorate and they near the end of life. Other interventions that may facilitate the grieving process include: ensuring that residents have access to any information that is shared, designating a location where those who are grieving can honor the dead, and designing strategies to provide collective support for those who are interested (cafes, discussions, newsletters, etc.). Our participants’ testimonies point to how crucial it is for residents to be able to communicate freely when death occurs. A most promising avenue would be to create spaces where communication can take place freely while at the same time respecting the residents’ choice to speak, and their pick of the best time to do so. Although not the subject of our article, it is worth noting that several studies show that nursing home staff can also experience grief when residents die (Anderson & Ewen, 2011; Boerner et al., 2015; Chen et al., 2018). As such, interventions could be implemented to support at once both staff and residents (e.g., sharing groups). In the second phase of this research project, we will investigate the practices in place in seniors’ residences to determine which are best aligned with the needs of residents, staff, and the specific realities of various living environments.
Conclusion
In this article, we shared the testimonies of individuals living in seniors’ residences who experienced the loss of a fellow resident. This allowed us to gain insight into this experience from an insider’s perspective. It would be interesting to collect testimonies from varied individuals who work in this setting to better understand their experiences surrounding the death of a resident and the motivations underlying their practices. Intersecting these two perspectives would allow for a rich and likely more complete portrait of this reality.
When death happens in seniors’ residences, the experience varies not only between individuals but also from one location to the next. Death is sometimes kept quiet or, to the contrary, it is named and even integrated into daily life. The intentions underlying the silence in some institutions appear laudable. However, this silence can hold various meanings and have different impacts on bereaved seniors. As Josée, a 67-year-old participant pointed out, it sometimes leads to a lack of support which can cause suffering: “Some are OK with it. As for myself, I find it hard, and I would have needed help.” Knowing this, it seems important to tune in to this need and to help people speak more freely about death and grief so that each resident feels that their presence and relationships to others are valued, from the beginning to the end of their trajectory.
Footnotes
Appendix
Participants Demographics.
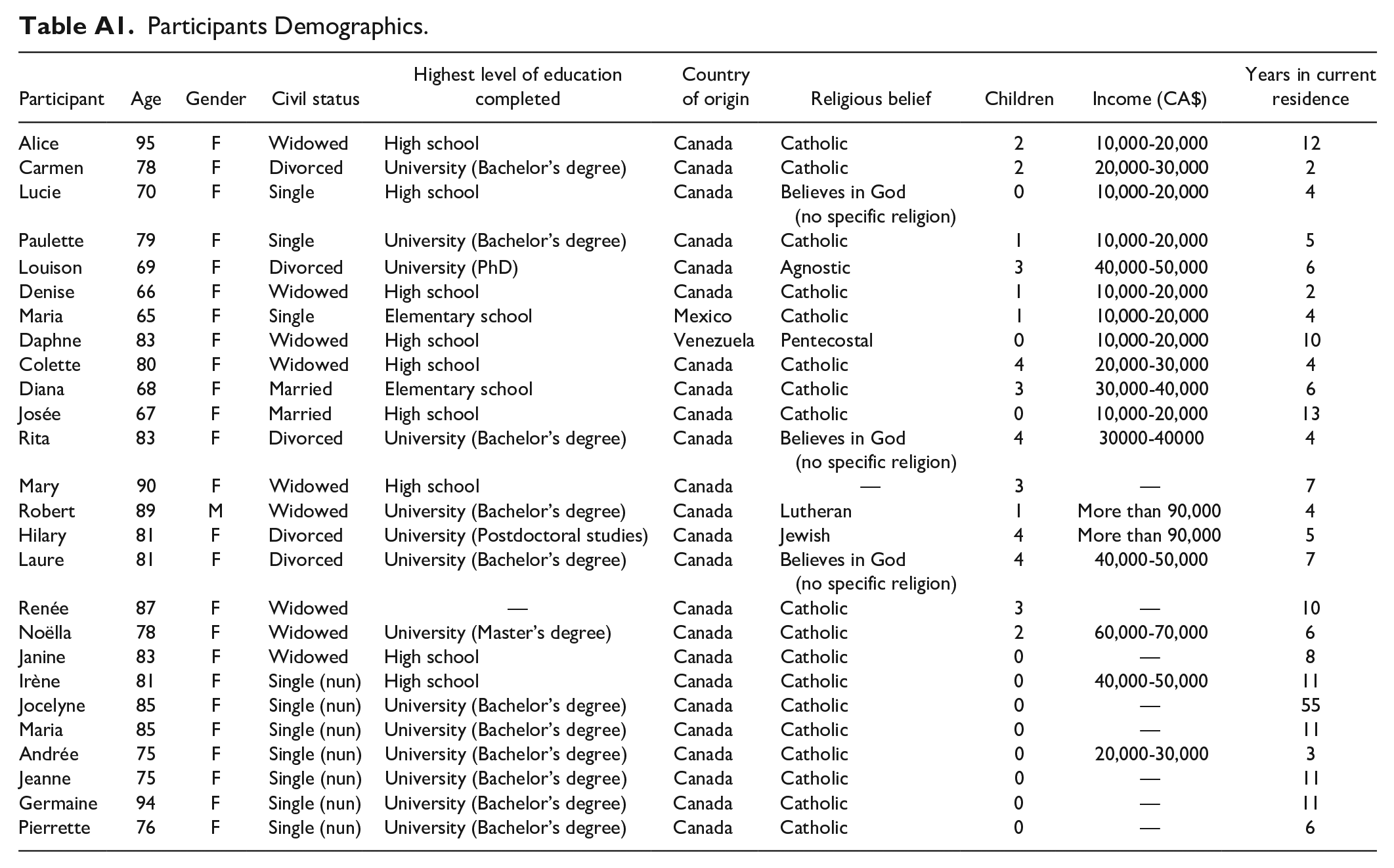
| Participant | Age | Gender | Civil status | Highest level of education completed | Country of origin | Religious belief | Children | Income (CA$) | Years in current residence |
|---|---|---|---|---|---|---|---|---|---|
| Alice | 95 | F | Widowed | High school | Canada | Catholic | 2 | 10,000-20,000 | 12 |
| Carmen | 78 | F | Divorced | University (Bachelor’s degree) | Canada | Catholic | 2 | 20,000-30,000 | 2 |
| Lucie | 70 | F | Single | High school | Canada | Believes in God (no specific religion) | 0 | 10,000-20,000 | 4 |
| Paulette | 79 | F | Single | University (Bachelor’s degree) | Canada | Catholic | 1 | 10,000-20,000 | 5 |
| Louison | 69 | F | Divorced | University (PhD) | Canada | Agnostic | 3 | 40,000-50,000 | 6 |
| Denise | 66 | F | Widowed | High school | Canada | Catholic | 1 | 10,000-20,000 | 2 |
| Maria | 65 | F | Single | Elementary school | Mexico | Catholic | 1 | 10,000-20,000 | 4 |
| Daphne | 83 | F | Widowed | High school | Venezuela | Pentecostal | 0 | 10,000-20,000 | 10 |
| Colette | 80 | F | Widowed | High school | Canada | Catholic | 4 | 20,000-30,000 | 4 |
| Diana | 68 | F | Married | Elementary school | Canada | Catholic | 3 | 30,000-40,000 | 6 |
| Josée | 67 | F | Married | High school | Canada | Catholic | 0 | 10,000-20,000 | 13 |
| Rita | 83 | F | Divorced | University (Bachelor’s degree) | Canada | Believes in God (no specific religion) | 4 | 30000-40000 | 4 |
| Mary | 90 | F | Widowed | High school | Canada | — | 3 | — | 7 |
| Robert | 89 | M | Widowed | University (Bachelor’s degree) | Canada | Lutheran | 1 | More than 90,000 | 4 |
| Hilary | 81 | F | Divorced | University (Postdoctoral studies) | Canada | Jewish | 4 | More than 90,000 | 5 |
| Laure | 81 | F | Divorced | University (Bachelor’s degree) | Canada | Believes in God (no specific religion) | 4 | 40,000-50,000 | 7 |
| Renée | 87 | F | Widowed | — | Canada | Catholic | 3 | — | 10 |
| Noëlla | 78 | F | Widowed | University (Master’s degree) | Canada | Catholic | 2 | 60,000-70,000 | 6 |
| Janine | 83 | F | Widowed | High school | Canada | Catholic | 0 | — | 8 |
| Irène | 81 | F | Single (nun) | High school | Canada | Catholic | 0 | 40,000-50,000 | 11 |
| Jocelyne | 85 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | — | 55 |
| Maria | 85 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | — | 11 |
| Andrée | 75 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | 20,000-30,000 | 3 |
| Jeanne | 75 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | — | 11 |
| Germaine | 94 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | — | 11 |
| Pierrette | 76 | F | Single (nun) | University (Bachelor’s degree) | Canada | Catholic | 0 | — | 6 |
Acknowledgements
We would like to thank the Fonds Québécois de Recherche Société Culture for their financial support through research Grant 2015-NP-181601, which made the completion of this study possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the FQRSC (Fonds de Recherche Société et Culture Québec).