
Abstract
This study addressed the possibility of integrating learning theory into humanistic counseling. We consider that such an approach may enable client self-counseling either between sessions or after therapy has finished. Carl Rogers was a keen advocate of person-centered learning facilitation in the classroom and his principles of learning provide a natural start-point for a humanistic therapy based on learning theory. A variety of other learning processes also lend themselves to a learning based therapy such as establishing client learning goals based on self-efficacy, enabling the client to understand their own learning processes and blocks to learning, encouraging the client to access their own learning resources, and then enabling long-term learning. A case study was therefore designed to test some of these processes in a therapeutic setting. A White, British, middle-aged female was recruited for the case study. During the course of six sessions, the content of which was analyzed using thematic analysis, a selection of learning processes were applied to the humanistic therapeutic process. In summary, it was established that facilitated learning processes could provide a practically acceptable basis for humanistic counseling, and these processes are offered here as the foundation to a model of “therapeutic learning.”
Keywords
This case study addressed the question of whether a range of learning processes could be integrated into humanistic therapy to develop a learning based therapy. We focused particularly on Rogers’s principles of learning, adding other learning theories consistent with a humanistic perspective into an integrative therapeutic process. Designed as a trial for some basic learning concepts, we hope that this case study may provide the foundations to a “therapeutic learning” methodology to be developed through further studies. We hope that in turn, this method may enable client self-counselling both between sessions and post therapy.
Providing the framework for this potential learning-based approach, humanistic philosophy has at its core, a search for the meaning of what it is to be vitally and holistically human. It concerns itself with existential themes such as “meaning, morality, freedom, limitation, values, creativity, and spirituality” (Schneider & Längle, 2014, p. 370). It focuses on the unique lived experience for each individual and emphasizes the capacity for freedom and choice in the process of development and growth. On this basis, humanistic therapies address the personal domain; the interpersonal domain; and clients’ reflections on their relationship with self, with others, and with the wider context of their psychosocial world (Whitton, 2003). Humanistic therapy includes approaches such as person-centered therapy (Rogers, 2003), Gestalt therapy (Perls, 1992), and emotion-focused therapy (Elliott & Greenberg, 2017). Common themes run through these therapies (Cain, 2016) such as; working at relational depth, collaboration and cooperation between counsellor and client, the definition of client goals and methods to achieve goals, and the creation of a mutually affirming therapeutic relationship.
The most relevant principles of learning for humanistic therapy are those of Carl Rogers, since his theories of learning are built on his humanistic theories of person-centered therapy. They include the following:
Human beings have a natural potentiality for learning
Much significant learning is acquired through doing
Self-initiated learning which involves the whole person of the learner-feelings as well as intellect-is the most lasting and pervasive
The most socially useful learning in the modern world is the learning of the process of learning (Rogers & Freiberg, 1969).
Through these principles, the natural potential for human growth is engaged experientially and facilitated in the context of the core conditions of empathy, congruence and unconditional positive regard. Conversely, in applying Rogers’s learning theories to therapy, it is worth noting that some of them require more than the core conditions on the part of the therapist. Therefore, the learning approach for this study modifies and expands on Rogers’s (2003) fundamental principles of person-centered therapy by including methods more consistent with broader humanistic therapies such as the goal definition of existential therapy (Van Deurzen & Arnold-Baker, 2018) or personal mastery from psychosynthesis therapy (Whitmore, 2013). Furthermore, a more integrative perspective is offered by the inclusion of techniques such as motivational interviewing (Miller & Rollnick, 2013) and self-therapy from cognitive behavioral therapy (Kazantzis & Stuckey, 2018).
In addition to Rogers’s learning theories, an extensive range of further learning theories were also reviewed in order to establish those with a natural fit within a humanistic therapy: behavioral learning theory for example can be useful in a counseling context in that simple behavioral reinforcers can be applied either in the form of direct feedback, or more subtly as behavioral modeling. Even Dijksterhuis and van Knippenberg’s (1998) notion of “priming” could be implemented. The idea that behaviors can become automatically linked to goals would support the need to define the client’s aims for therapy. As Austin and Vancouver (1996) suggest, goals enable clients to compare where they are now with where they want to be, which in turn affect processes such as motivation, planning, action, and affective responding. If these goals are absolutely clear, then behaviors, in theory, could also be “shaped” with a view to achieving them (Skinner, 1974).
Cognitive learning theory provides an equally useful perspective from which to define learning processes and outcomes, particularly as it aims to define the developing sense of self. Experiential learning (Bruner, 1961) encompasses this cognitive domain. Theories of experiential learning suggest that it is the knowledge, skills, attitudes, values, and senses that can be distilled and consolidated from a client’s experience and which can be transferred to other similar situations. Derived from this perspective is the experiential learning theory of Kolb and Kolb (2009) from which emerged a cycle of learning based on concrete experience, reflective observation, abstract conceptualization, and active experimentation. In the longer term, a “learning self-identity” can be the aim.
In the domain that encompasses both behavioral and cognitive learning theory, there is the concept of client expectancy that a goal will be achieved, which in itself fuels outcomes, as automatic processes or habits are formed. Constantino et al. (2011) found in their metaanalysis, for example, that outcome expectancies were positively related to the outcomes of therapy in most of the 24 studies they reviewed. Duncan’s (2015) research into common factors also suggests that “Models achieve their effects in large part, if not completely, through the activation of placebo, hope, and expectancy” (p. 466).
Cognitive/affective learning processes can also be enabled. The complex interplay between feelings, cognitions and actions is often unconscious, and therefore opportunities to explain the interrelationships can be sought. For example, Carey et al. (2007) suggest that therapeutic change is best approached by facilitating the client’s progress toward an impasse from which they then find solutions for themselves. Thus, Gestalt conceptual “wholes” are addressed by drawing together disparate parts resulting in insight. Facilitating a connection with affect, potentially denied to awareness, is part of this process.
Consistent with Rogers’s views, self-efficacy is considered by Bandura (1982) to be a particularly important element of self-directed learning and is demonstrated in a client’s belief that they can produce desired effects by their actions. The various influences on self-belief, such as past successes and failures, emotional states, and vicarious experiences can be addressed through therapy. Unconditional positive regard can also support this process, as can modelling self-belief and giving positive feedback (Bandura, 1977).
The goal of long-term learning is achieved on the basis of successful learning transfer. This may be facilitated first, by the use of metacognitive strategies, which would enable learning to be transferred to a similar situation, to similar issues, or in fact to any new situation in which the client may see learning potential. Finally, a permanent change in cognitions and behavior would emerge. Also relevant are the transfer of learning processes, enabled for example, by metacognitive questioning (Flavell, 1979). Furthermore, metacognitive strategies, such as learning planning could be enabled, and a level of engagement activated to encourage learning to continue.
Many learning theories have the potential to be applied in the context of humanistic therapy; however, those theories chosen for this study were intended to be consistent with Rogers’s principles of learning facilitation such as “The facilitator helps to elicit and clarify the purposes of the individual . . . ” and “He regards himself as a flexible resource to be used . . . ” (Rogers & Freiberg, 1969, pp. 164-166). In line with Rogers’s views on learning, a clear distinction was drawn between the role of a learning facilitator—someone who enables the process of development in another, and that of an expert teacher who imparts knowledge.
The aim for the study was to trial some key learning processes which sat well within a humanistic therapy framework, focusing particularly on Rogers’s principles of learning, in the case of one client. We wanted to establish those which the therapist found the most useful to implement during the course of the therapy and to gain the reaction of the client once the therapy had finished as to how useful she had found them to be.
We considered that a case study would be the most appropriate approach to answering the question of which learning theories would be most applicable to integrative/humanistic therapy: Context-independent theory is not obtainable according to Flyvbjerg (2006), so it is the context-dependent knowledge which can be produced through the study of an individual case that “ . . . is important for the development of a nuanced view of reality” (p. 223). Furthermore, Easton (2010) notes that the main benefit to using case studies is the potential to understand an issue comprehensively, in-depth and in a rich, real-world context. Processes in addition to outcomes and their underlying associations can be teased out in a real setting, giving access to contextual cues and therefore greater meaning. So, a decision was made to study the real depth, nature and complexity of learning processes and their associated tacit skills in therapy, by describing, exploring and then attempting to explain them.
By necessity in this case study, the research not only brought a preordained framework to the situation, but manipulated the case process in order to observe the effects of that manipulation on the individual observed. To that extent, it could be regarded as a quasi-experimental case study (Neuman, 2014). Etic issues, in this case those that relate to the learning process, were brought to the study (Abma & Stake, 2014), and observations made largely from the point of view of the observer. In addition, an emic perspective, or that derived from the client’s view point, was integrated into the analysis. Therefore, the case is further conceptualized as contained within a bounded system, here bounded by the theoretical framework and the aims and experience of both client and therapist (Abma & Stake, 2014), and constrained within a specific context. So, the more modern interpretive, constructionist perspective of case study research is less appropriate here than that of Yin (1981) which is described as the production of: “(a) an accurate rendition of the facts of the case, (b) some consideration of alternative explanations of these facts, and (c) a conclusion based on the single explanation that appears most congruent with the facts” (p. 61).
Farquhar (2012) notes the limits of utilizing pure approaches to reasoning, acknowledging that a combination of approaches is often appropriate. This case study used a combination of retroductive and abductive reasoning, based on a critical realist perspective: As elements of theory and researcher assumptions were brought to the research, hypotheses were drawn from inferences made about causal mechanisms identified through the analysis. Furthermore, data emerging in addition to that being tested was amalgamated and tentative theories generated. This case study represents ideally, the first of many cases which, “via recursive cycling among the case data, emerging theory and later extant literature” (Eisenhardt & Graebner, 2007, p. 25) would be necessary to develop any robust learning methodology with any potential for generalization.
A purposive strategy was used in selecting the sample for this case study since, as Patton (1999) suggests, the purpose was to understand and illuminate an important case rather than to generalize from a sample to a population. Patton (1999) also suggests that a “highly successful” case can yield more specific results than a “typical” case, and it was this perspective that the researchers concluded may give it relevance (p. 1198). If a client could be found who would be more likely to engage in learning mechanisms and be more able to articulate their own understanding of them, this may represent an “extreme” or “most likely” case. And furthermore, as Flyvbjerg (2006) suggests, “Atypical or extreme cases often reveal more information because they activate more actors and more basic mechanisms in the situation studied” (p. 229). The researcher’s decision to choose the specific client was therefore based on the premise that a client who was trained in therapy and life coaching and was acutely aware of and interested in her own analytical processes from an academic perspective, would potentially yield more data than a “typical” counseling client. It is suggested therefore, that the case may be defined as paradigmatic, or an exemplar of the domain of therapeutic learning, with metaphorical or prototypical value (Flyvbjerg, 2006). Ethical approval for the study was obtained from the Sheffield Hallam University, Ethics Committee.
Method
Participant
The individual invited to participate in the case study had undertaken Person-centered therapy with the first author 3 years previously and was confirmed not to be in any state of mental health crisis, but engaged in a process of sustained personal development. The individual is White, British, was in her 40s and lives in the north of England with a particular ability to be both internally involved in and externally observing her own personal processes at the same time, coupled with a good understanding of experiential learning. The client was recruited simply through an e-mail and a telephone conversation to explain the aims of the study. She was very keen to participate since she regarded herself as being at a cross-roads in her life and was in need of some support.
The first researcher took on the role of therapist on the basis of having higher level qualifications and experience in both Person-centered therapy and training/learning and development.
Procedure
The plan for the therapy was for the therapist/researcher to integrate a small selection of learning processes and theories into a humanistic therapeutic process. We focused on the learning theories that we considered would most likely produce some benefit for the client, although it was expected that other learning processes may emerge through the course of the therapy. The initial processes were intended to be:
A philosophical approach of self-directed learning, that is, not “teaching” but “facilitated learning”
Goal setting using a questionnaire based on the idea of the fully functioning individual (Renger & Macaskill, 2021)
A focus on the analysis and recap of learning processes
The explanation of learning models in order to support client progress
Use of guided enquiry, or directive questioning
Evaluation of progress: that of client insight or learning
Materials
The client briefing materials (sent by e-mail), included an explanation of the objectives of the study and the intended therapeutic learning approach. A face-to-face briefing then covered the therapeutic approach in more detail and the use of a goal-setting questionnaire. The questionnaire listed 71 items describing the “fully-functioning” person (Renger & Macaskill, 2021), which the client took home to review, and was intended to represent a potential “curriculum”; 6 × 1 hour therapy sessions were planned at weekly intervals. Each session was audio-taped, transcribed, and analyzed using Braun and Clarke’s (2006) thematic analysis before the next session, allowing for the structure of subsequent sessions to be planned.
The case study below details only brief highlights from the original narrative for reasons of space, and the case study client is referred to by the pseudonym “Jane.” In the transcripts, “T” are therapist statements, and “C” refers to the client.
Session 1
The first session covered the goals which had emerged from Jane’s consideration of the questionnaire that had been supplied in the prebriefing. This was intended to represent a kind of ‘curriculum’ of potential learning goals. The client had determined what she wanted to achieve through this process and had therefore generated a sense of ownership of her goals:
Would you mind talking me through principally what you decided, and pick out the ones that you think are relevant? (Referring to the 71 items)
. . . so part B, my specific goals. So this is kind of sat on the surface, consistency, self-soothing, balance, health. So they’re all kind of here. So this is kind of what I’m struggling with in the world, so on a day to day basis—responsibility, productivity, um, health, balance, creating that balance.
The engagement of goal-directed behavior was then facilitated on the basis of these learning goals by encouraging the client to describe what she considered would be a successful outcome:
Well how would you look, if you were looking in on yourself and describing yourself, what kind of person would you be?
A sense of self-efficacy is foundational to self-directed learning, so Jane’s existing strengths, which had the potential to help her move forward, were also identified through the following question:
What is it that you want to bring with you from the past into this future?
This session also looked at the blocks to progress the client was experiencing:
So for me I feel a little bit “I’m not quite ready to do this within my business ‘cos I can’t quite do it for myself” . . . So, that is the main thing, and that’s my block.
Following further discussion, and in summary, it seemed that trying to meet others’ expectations was becoming exhausting, and more importantly, affecting the client’s belief in herself. This was ultimately what she wanted to address through therapy.
On reaching the end of the first session, and indeed at the end of every session, the client was encouraged to recap the main learning points and commit to implementing some ideas before the next. So, for example, at the end of this session, Jane commented:
On reflection from this session is, what I’d like to move forward is, to pull down the information . . . I think I need to practice it. . . . So, it will create a consistency and a balance and a productivity . . . so it’s learning to stay in the middle when I’m in a very stressful situation.
Session 2
Focusing on learning mechanisms, each subsequent session started with a recap of what the client had implemented between sessions, what had been learned from it, what needed addressing as a result, and what impact there was on long-term goals, if any. It seemed that revisiting the pretherapy questionnaire had been helpful in consolidating these issues:
I’ve reflected on the session and my homework . . . but what’s come up is the security. Um, so in here (the questionnaire), this is fabulous, so it’s a really good way of referring back.
Another important area to discuss with the client in the context of learning was her motivation to achieve her goal of a secure and authentic working life that allowed her to truly be herself:
What is motivating you to change to be something that’s different . . . ?
. . .when I really tap into it, it’s almost like I’m dying every day the more I don’t do this. Wow. And I can feel myself kind of depleting and I’m thinking “oh, my goodness, I’m not living”
The final segment of this session was intended to establish for the client that she was in a self-directed learning process and that progress would be managed by her. This perspective was demonstrated in the following questions: “What do you want to do to achieve all that?” and “What can we usefully do together, to help you with your long-term goal?” Her use of the therapist as a resource was also addressed and then confirmed in a later session when she asked for some support in communicating more effectively:
What you’re saying is, can you have some tools to enable that to happen?
Session 3
This session began by facilitating an understanding of the client’s own learning processes to enable her to plan her own learning away from therapy. After some discussion, it was clarified that she was an experiential learner:
So in terms of how we’re going to plan this learning experience (yeah), this learning process (yeah), for you, it is that it’s going to be, it sounds like it’s going to be a fully experiential process . . .
Yes, definitely. So, if I’m writing an essay, I will speak it, I will dance it, I will paint it, and then that helps . . .
Finally, this session clarified and summarized learning objectives, preferred ways of learning, and resources the client would require to enable progress. Jane was happy with this overview, but at this stage, was unsure of the detail of her “learning plan.”
So, do we need to have that detail laid out?
I think we do . . . It’s the next level, for me, my understanding, my logical head, the next level down of ‘OK well practically how do you then implement that in the world.
Session 4
Since the learning process in the context of this therapeutic approach is facilitated, in common with some humanistic approaches it is directive to a degree. For example, the client’s goals, motivation and sense of self-efficacy had been established through a specific process of questioning. Session 4, for example, began with a directive question:
OK. So, between when I saw you last time and now, what would you say has been the movement if any?
I don’t know why I’m surprised by this, but the more I’m engaging in this process . . . things like this (clicks fingers) are happening and they’re falling from the sky.
It was interesting to note that in recapping the learning between sessions, Jane’s insight, that “The learning opportunity is—every aspect of me is there and present” indicated that she realized that every aspect of her could be subject to new learning.
Other directive questions/statements in this session included “Is that a new experience for you generally?” which clarified a learning point; then “So as you step back out of the process and do a bit of a helicopter view on it . . . ” enabled process observation; and finally “I want to see if there’s a way, if you learned how to do that, so that you can do it again” began to look at learning transfer.
Session 5
Much of the therapy focused on enabling the client to understand her own learning processes. During one conversation she identified her holistic approach to learning:
So for me, in a learning process, that learning process you just talked about, that is very much the intellectual side. For me there’s another level, which is the emotional. So if you think that they kind of all blend in, there’s an emotional side that impacts the physical and the spiritual.
Between Sessions 4 and 5, a big decision to move forward with her life seemed to have been made by Jane. Reflecting on her learning points from sorting through old memory boxes, Jane had realized that she had been relying on others for her security for years and denying her own strength. Here, she seemed to have initiated her own learning at the “concrete experience” point in Kolb and Kolb’s (2009) learning cycle and defined it as holistic and experiential. This “total experiencing” seemed to have been the catalyst for the learning process. At this point, Kolb’s learning cycle was explained for reference in order that Jane could refer back to it in the future.
Also evident in this session was the enabling of process observation. This was important on an ongoing basis in order that the client was able to understand and reenact processes which were relevant for her: For example, the therapist asked: “Do you know what it was that um, made that happen? . . . if you need to access that state again, what brings that kind of emotion on?”
Session 6
The facilitation of metacognition and the application of potential theories were two specific learning techniques used throughout the sessions, demonstrated in questions such as: “Can you explain any more what was going on in your mind at that time, what you were thinking or what had happened?” Then a “thinking–feeling–acting” perspective (Mueller et al., 1994), a Rational Emotive Behavior Therapy perspective (Ellis, 2013) and Games People Play (Berne, 2011) were each explained in order that the client could assess the models for their fit with her thinking going forward. Some principles of assertiveness and interpersonal skills such as understanding her partner’s perspective through questioning were also discussed to provide a framework for metacognition. For example, Rational Emotive Behavior Therapy was referenced in the following question: “You said um, you take full responsibility for it (yes). What’s behind that statement?” Assertiveness theory was behind the following question: “Are you saying that if you managed to stay firm in what you needed and wanted (yeah), and articulated and explained that effectively (yes), you might get a bit further (yes)?” And the theory of self-efficacy prompted this question: “So do you think you’ve got a right to feel the way you do, or do you think ‘Underneath actually, that person’s right?’ Whatever their criticism is, they’re (hmm) probably right?”
Finally, ensuring that learning is embedded and will transfer is one of the most significant elements of learning theory, so this was addressed regularly. For example:
OK, so, what’s the learning to take forward?
The learning to take forward is (pause) what I’ve brought to you. . . . Oh gosh, that’s really interesting. What I’ve brought to you is fundamentally security and in this session I have clearly identified (pause), it’s because I’ve not felt secure in my Child place.
Closing Session
A final session was planned to allow Jane time to reflect fully on her learning from the sessions with a view to embedding key points in her long-term memory. Furthermore, it would give her the opportunity to initiate a new learning plan which would continue her development after the therapy had finished and would ensure that the client would be self-sufficient in her therapeutic progress:
I feel like I’m right in that central heart, hub of what that is, like that gold little nugget. And it feels like there’s another part that needs to say, that we need to work on, or part of the therapeutic process of “How are we now going to put that in place?” So a very action based “This is now.” So when you asked that question “What are you going to do for the next 6 months, a year or my time frame?” For me, um, I’ve been doing some research about where to go and I’ve very clearly identified what’s happened and why I feel this way and where I need to go with this, and what’s very, very clear, support to put in place and why.
Feedback Session
In a final feedback session, Jane was asked to rate the success of the process for her on an increasing scale of 1 to 10, to which she replied “8.” She was then asked to step out of the therapeutic mode and consider how the process had compared to other therapies she had knowledge of. She commented that “ . . . it feels very different. So for me, there’s dialogue, conversation of every learning part of me . . . and then “What are we going to do about it? Let’s move it forward.”
We talked in detail about the idea of engaging in an identified learning process and using that as a tool for self-counseling over time. Jane was clear that it helped her focus in on her issues, to decide on a practical way forward and plan on a process to make real changes in the longer term. Jane was asked whether the whole idea of having goals was helpful and she identified that, given her propensity to self-analyse, they were very helpful in “changing her state.” Furthermore, she considered the length of time spent drilling down to establish the root of her issues was well spent since it enabled her to uncover the detail of her fundamental issue. Next, she was asked about the questionnaire and how helpful it was to the therapeutic process. Jane commented “ . . . by the end I was like “Oh, it’s my best friend,” explaining that it became a working document which she referred to every day. She went on to explain that the questionnaire had helped her focus a fundamental need into practical areas to work on.
Finally, Jane was asked whether she considered that her experience may represent a methodology which was worth pursuing as an approach in its own right. She responded “Yes, yes, most definitely, most definitely.” And when asked how she would describe it to a potential client, she said: I would describe it as a talking therapy, with a most definite forward motion of an outcome. And when you have the outcome, you have the skills to say “I’m going to move this forward” and then you can implement that, so then the problem isn’t a problem again. It might bob up again, but you have the tools to go “Oh, OK, I’m going to go and do this.”
Data Analysis
Each therapy session was transcribed and analyzed on completion using Braun and Clarke’s (2006) thematic analysis, from a critical realist perspective; analyzing the text from the point of view of the empirical, the actual, and then the perceived underlying mechanisms: First, a total of just under 50,000 words were broken down into 619 segments of related text and then, an assessment of what the client might be saying produced for each segment. Summary statements were emailed to the client after each session to be checked for accuracy. Once the text had been validated by the client, a view was taken on what the client was actually saying. And next, an assessment of the drivers or mechanisms supporting the comments was made. With a view to ensuring accuracy, the categories of the “real” and “underlying mechanisms” were reanalyzed and refined at the end of all of the sessions in the light of greater knowledge of the client. The text was finally collated into 70 segments of discussion topics defined by specific learning processes which were largely initiated by the therapist/researcher during therapy. The second author undertook validity checks matching topics to learning processes and where there were differences of opinion, a third counsellor provided input until consensus was reached via discussion.
Results
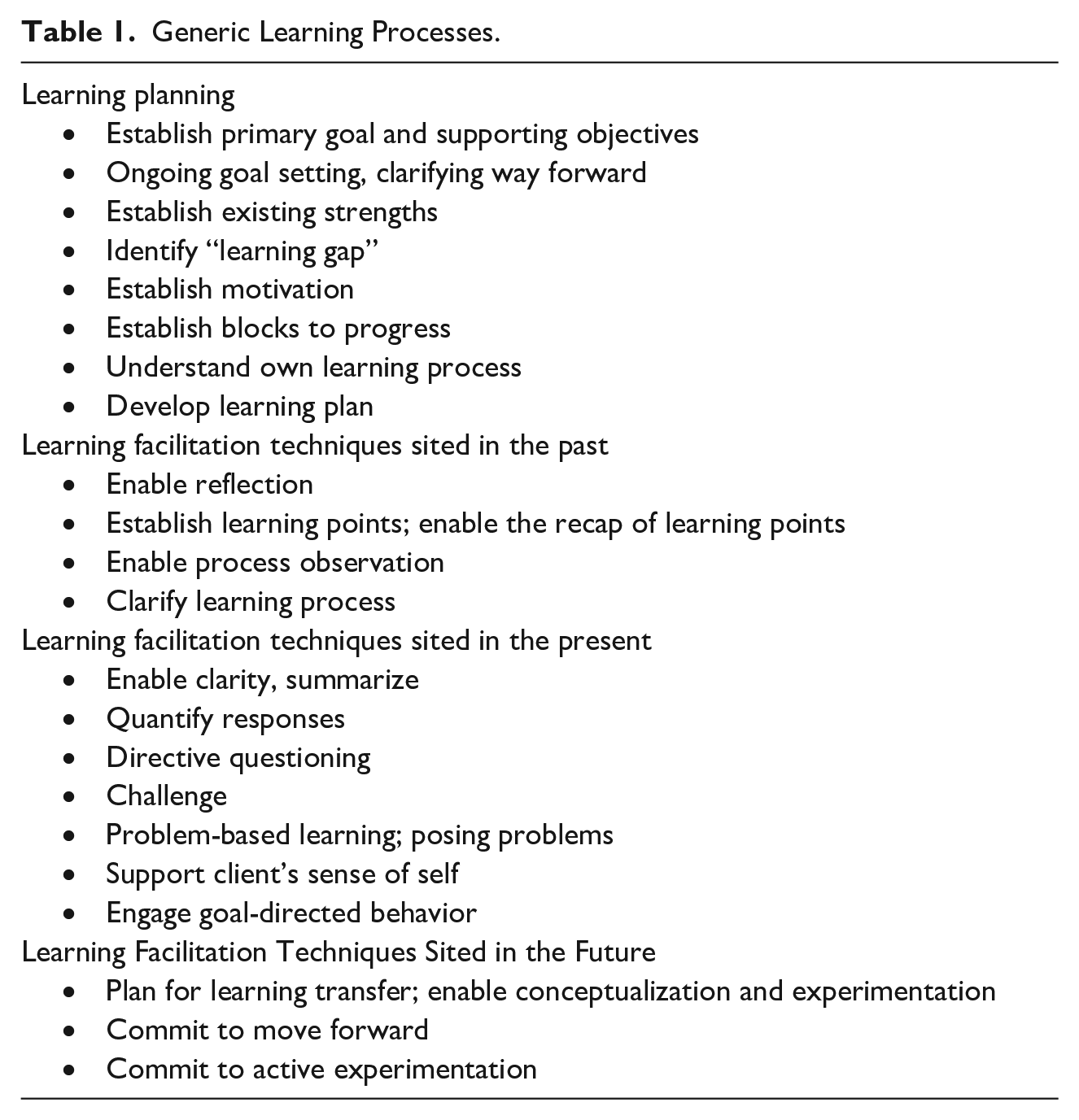
The aim of the case study was to integrate a small number of learning processes into a humanistic therapeutic context, and to identify any further learning mechanisms which emerged through the engagement. Through analysis of the therapy transcripts, 27 generic learning processes were identified, such as “establishing existing strengths,” and “engaging goal-directed behavior,” and a further eight specific theories emerged that were pertinent for this particular client. Interestingly, although there had been an explicit intention to include certain learning methodologies within the therapeutic encounter from the start, it was in the experience of the therapeutic encounter that they emerged with any kind of clarity and sense of order. The generic learning processes that emerged as themes are summarized in Table 1.
Generic Learning Processes.
Discussion
This case study was designed with a specific intent—to test the integration of learning principles into humanistic therapy. It was hoped that in six sessions, the client would have explored her issues and set some goals for change. It was also intended that the client would have developed some ability to manage her own learning and therapeutic development in relation to those and other identified goals in the future. These therapeutic aims for the case study client seemed to have been achieved. Furthermore, it was hoped that ongoing client development would be facilitated by the client’s own understanding of how she learned, a sense of self efficacy, and a need to continue learning.
From a methodological perspective, three key learning principles were implemented and emerged from the course of the case study to be central to the whole process. First, Rogers’s learning principles meant that it was a facilitated learning experience, not a taught one. Therefore, an overriding principle of directive “guided enquiry,” based on the views of Dewey (1997) was intended to enable the client to gain therapeutic insights and to understand and transfer her learning processes to her own self-counseling. Second, the therapeutic relationship was intended to be one of coenquirers and colearners. The client brought knowledge of their own needs and processes, the facilitator brought knowledge of learning processes: The exchange of that information created learning for both. Finally, it was intended that the client would become a long-term “self-learner” in relation to therapeutic issues. Once the learning processes were understood, they could be implemented as a matter of course indefinitely. The client would become an autonomous learner (Betts, 1985; Knowles, 1978) and enabled to develop a “learning self-identity” (Kolb & Kolb, 2009). In summary, the client becomes Rogers’s idea of a “lifelong learner” (Kirschenbaum & Henderson, 1997).
Fundamental to each of these key learning principles were the dialogical processes that guided them. These were not only informed to a degree by the Person-centered approach but also by dialogical elements from a wider range of methodologies. Dialogue in a person-centered context is a process of confirmation of the “otherness” of the client (Buber et al., 1997), or of mutual revelation and authentic receipt (Schmid, 2001). This relational approach provides the foundation to successful learning (Rogers & Freiberg, 1969). However, guided enquiry for example, draws on the Socratic dialogue more commonly used in cognitive behavior therapy (Kazantzis & Stuckey, 2018) and supports goal-focused work particularly. Dialogue that develops the colearner relationship requires that instead of editing and interpreting the client’s narrative using the therapist’s logic and expertise, “the therapist’s curiosity invites the client’s curiosity, and thus the seemingly one-sided inquiry becomes a mutual or shared inquiry” (Anderson, 2005, p. 500). Furthermore, therapeutic dialogue which becomes internalized is also important in facilitating long-term learning. As Marble et al. (2019) suggest, the dialogue between client and therapist continues post therapy as clients seek to reexperience their therapeutic encounter as they face new situations.
Core Factors That Defined This Case Study
Although this case study was planned to test a small number of potential learning theories for development into a more complex model, a core foundation of therapeutic learning principles did emerge:
Limitations
There is a perception that case studies tend to confirm ideas preformulated by the researcher, and in this case, a broad framework of tacit assumptions and beliefs about the possibilities of facilitating learning in a therapeutic setting were brought by the researchers. A range of learning theories were also identified before the research started—to act as a framework. Thus researcher bias was designed into the process. While the client in the case study had issues she wished to work on, this was not accompanied by significant emotional distress. It may be that applying these techniques with clients who are suffering from mental illness and are emotionally unstable will be more challenging but would be worth further research. And clearly, a sample of one client is a significant limitation to the study. The fact that the researcher had previously conducted therapy with the client could also be regarded as problematic since the client was keen to maintain a good relationship and be of help to the researcher. Her positive bias may well therefore, have skewed the results.
Conclusion
The outcome of this case study is a tentative set of learning principles which can be integrated into a humanistic therapeutic context, but would require further testing to be considered robust. It should also be noted that the principles tested here represent a tiny proportion of possible learning processes available for use in therapy. The main learning components emerged as a philosophy of long-term learning, with a “self-learner” identity, coupled with a facilitated learning experience, in a climate of co-enquiry. Processes such as goal setting, establishing a learning need, defining the client’s learning preferences and establishing their motivation provided the backdrop. Using specific learning facilitation techniques with predominantly directive questioning, focusing on learning outcomes, process analysis and metaframeworks made up the bulk of the activity. Finally, a plan for ongoing learning and evaluation, and assessment of effectiveness concluded the process. A complete learning methodology, although inclusive of these elements, would be much broader in scope, so this study aimed merely to provide a start point for further research. Initially, further case studies would help to test a broader range of learning processes for their suitability to a humanistic therapeutic context: For example, problem-based learning, giving feedback, using behavior modelling techniques, the use of mental maps, social learning theory and reinforcing or shaping behaviors. Then the core model, with the flexibility to include a range of these learning processes, could be tested on a much wider sample of clients. Training for therapists in the approach, backed up by a therapist manual would need to be available at this stage.
Implications
A humanistic therapeutic approach based systematically on learning facilitation is unavailable to counselors and clients at present. This study considers the theoretical foundations for such an approach and tests the implementation of initial principles. There is the possibility, therefore, that self-directed learning principles may result in greater efficiencies, effectiveness or long-term retention of positive outcomes for counselees, but further research would be necessary to validate these possibilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies