
Abstract
The mechanisms generating skin-tone-based health inequities among ethnic Black Americans remain poorly understood. To address this gap, our study advances a novel biopsychosocial model of embodied colorism-related distress. We test this model with survey and biomarker data from a community sample of working-age Black adults from Nashville, Tennessee (2011–2014; N = 627). Relying on self-rated, interviewer-rated, and discordant skin tone measures, our analyses reveal that Black adults who perceive themselves as dark-skinned tend to have a lower sense of mattering and shorter telomeres, a biomarker of accelerated cellular degradation and aging, relative to their peers who perceive their skin to be lighter. These patterns hold across various social contexts and regardless of interviewer-rated skin tone, indicating that subjective skin tone may be a particularly robust gauge of colorism-related stress processes. Our study reveals critical and previously unexplored biopsychosocial mechanisms linking colorism to health inequity.
A small but growing line of research identifies “colorism” as an important factor that structures health risks and protective resources among ethnic Black Americans. 1 Reflecting skin-color-based social hierarchies, colorism systematically bestows social and economic advantages to those with more Eurocentric phenotypes—including lighter skin, hair, and eye colors—while denigrating and excluding those with darker, more Afrocentric features (Hunter 2007). Indeed, numerous studies find that Black Americans with lighter skin tones generally report more favorable treatment from individuals and institutions, improved social and economic outcomes, and better health and longevity than their darker-toned peers (see Dixon and Telles 2017).
Although extant research on colorism and health stratification among Black Americans has generally found that Black people with darker skin exhibit worse health than their lighter-toned peers (DeAngelis, Hargrove, and Hummer 2022; Hargrove 2018; Louie 2020; Monk 2015), there remain two key gaps in our understanding of this pattern. First, the mechanisms linking colorism to individual health outcomes remain underexplored. Prior work has examined factors such as socioeconomic status (SES) and discrimination as potential mediators. We, however, know little about the biopsychosocial pathways through which colorism “gets under the skin” to generate inequities in health and longevity. Black Americans may embody colorism-related slights as chronic social stressors with negative health implications, akin to other racism-related stressors (Goosby, Cheadle, and Mitchell 2018). Yet this idea remains underexplored in the colorism and health literature.
A second gap concerns the measurement of colorism in health studies. Evidence suggests that different types of skin tone measures may capture distinct processes that link colorism to health (Dixon and Telles 2017). However, few U.S.-based studies of skin tone and health inequity have thoroughly explored this idea (for an exception, see Monk 2015). Knowing whether different skin tone measures capture distinct social and health stratification processes can improve our understanding of how colorism-related health inequities emerge among Black Americans.
Our study extends previous research by addressing two open questions regarding colorism-related health inequities. First, how does colorism affect the health of Black Americans? Second, do different skin tone measures capture unique colorism-related health stratification processes? To address these questions, we draw from research on social neuroscience and the stress process to conceptualize distinct mechanisms linking colorism to individual health. We then empirically test the associations between multiple skin tone measures and two theoretically relevant outcomes—sense of mattering and leukocyte telomere length—to gain insight into granular biopsychosocial pathways through which exposure to colorism becomes embodied, with the potential to increase subsequent disease risk.
Analyzing survey and biomarker data from Black participants of the Nashville Stress and Health Study (NSAHS), we reveal novel patterns indicative of embodied colorism-related stress. Consistent with an emerging social neuroscience perspective of the health consequences of anti-Black stigma (DeAngelis et al. 2022; Goosby et al. 2018), our findings suggest that colorism-related stress is embodied via physiological processes from social rejection (i.e., negative reflected appraisals). Compared to their lighter peers, Black respondents who perceive themselves as darker than other Black Americans typically report feeling as if they matter less to other people and tend to exhibit shorter leukocyte telomere length, a biomarker of accelerated cellular degradation linked to aging, chronic stress, and inflammation. These patterns hold across various social contexts and regardless of interviewer ratings of skin tone. We discuss the broader implications of our findings for researchers concerned with persistent health inequities among Black Americans.
Background
Skin Tone Stratification among Black Americans
Colorism is a stratification system that differentially allocates social privileges, power, and material resources to individuals based on their physical appearance (Hunter 2007; Monk 2021b). Accordingly, those with more Eurocentric features—including lighter skin, hair, and eye colors—tend to experience systematic advantages relative to peers with more Afrocentric features. Although colorism is distinct from racism, the two systems codeveloped in the United States during the period of race-based chattel slavery and have mutually reinforced each other ever since. For example, both enslaved and emancipated Black Americans with lighter skin were historically afforded more social privileges and opportunities for mobility than their peers with darker skin, given their presumed similarities to Europeans (Reece 2019). Extended over centuries, the systemic preferential treatment of Black Americans with lighter skin has generated skin tone hierarchies within Black communities (Keith and Herring 1991; Monk 2014).
Indeed, colorism continues to structure exposure to health risks and access to health-protective resources today. Black Americans with lighter complexions generally receive multiple benefits relative to their darker-skinned peers, due, in part, to the favorable social meanings ascribed to lighter Eurocentric features and the social consequences of these ascriptions. These benefits include better marriage prospects (Keith and Herring 1991; Reece 2019), higher educational attainment (Keith and Herring 1991; Monk 2014), higher rates of upward mobility (Hunter 2007; Reece 2019), more prestigious occupations (Monk 2014), greater incomes and wealth accumulation (Adames 2023; Goldsmith, Hamilton, and Darity 2006; Monk 2014), better treatment in legal and criminal justice proceedings (Eberhardt et al. 2006; Monk 2019), and greater political influence (Strmic-Pawl, Gonlin, and Garner 2021). Lighter-skinned Black Americans also generally report less racial discrimination than their darker-skinned peers, especially in high-status and predominantly White spaces (DeAngelis et al. 2022; Keith et al. 2017; Klonoff and Landrine 2000; Monk 2015).
Prior work also documents colorism-related health inequities among Black Americans. Studies find that darker-skinned Black Americans tend to experience worse physical and mental health than their lighter-skinned counterparts for many outcomes, including cardiometabolic disorder, psychological distress, depressive symptoms, suicidality, and self-rated physical and mental health (Armstead et al. 2014; Cobb et al. 2016; DeAngelis et al. 2022; Hargrove 2018, 2019, 2023; Klag et al. 1991; Louie 2020; Monk 2015, 2021a; Wassink, Perreira, and Harris 2017). Moreover, skin tone disparities in SES, discrimination, and other psychosocial stressors help to account for some—but not all—of these observed health inequities (DeAngelis et al. 2022; Hargrove 2019).
Thus, lighter-skinned Black Americans have benefited from systemic preferential treatment for centuries, resulting in skin tone stratification across myriad social, material, and health indicators within Black communities. Although some studies suggest that disparities in SES and stressors help to explain colorism-related health inequities, darker-skinned Black Americans often exhibit worse health than their lighter-skinned peers after accounting for these mechanisms. Such findings indicate a need to examine other potential pathways linking colorism to health inequities.
Colorism and Health: A Biopsychosocial Framework
We advance the perspective that the systemic preferential treatment of light-skinned persons—and denigration of dark-skinned persons—can generate unique chronic stressors that become embodied, ultimately contributing to health inequity among Black Americans. Black Americans’ lived experiences with complexion-based discrimination and their broader observations of—and experiences with—complexion-based structural and material inequality in the media and in their social world reinforce messages that “Whiteness” is socially preferred over “Blackness” (Chandler 2017). Over the life course, such observations may contribute to socialization processes whereby many Black Americans gradually learn to attribute negative qualities to their skin color and themselves (Monk 2015; Spencer-Rodgers, Tong, and Liao 2012). We suspect that this socialization process can harm health in two key ways.
First, social preferences for White aesthetics may undermine the psychosocial functioning of Black Americans, particularly those with dark skin, through processes of negative reflected appraisals (Monk 2015). According to the reflected appraisal principle, people generally develop their sense of self-worth over their life course by assimilating into their self-concepts the cues they receive through repeated social interactions with others (Felson 1985; Rosenberg and McCullough 1981). Applied to our study, this principle suggests that darker-skinned Black Americans will receive repeated signals that they are devalued in society, which could damage their self-concept in certain contexts. For example, Thompson and Keith (2001) found that darker-skinned Black adults tended to report lower self-esteem and self-efficacy than their lighter-skinned peers, with some variations by gender and SES. Moreover, Louie (2020) found that dark-skinned Black adolescents reported poor mental health due to a low sense of mastery. Although feelings of mastery and efficacy are not direct measures of reflected appraisals, these studies support the general argument that colorism is a risk factor for diminished self-concept among Black Americans.
Second, colorism-related stress may also affect biological processes (DeAngelis et al. 2022; Goosby et al. 2018). Owing to the legacies of human social evolution, cues of rejection from a desired social group or broader society can profoundly affect the brain and wider organ systems (Axelrod and Hamilton 1981; MacDonald and Leary 2005). One relevant mechanism in this context is “social pain” (Goosby et al. 2018). Social pain comprises the physiological pain and inflammatory responses that often follow social rejection or isolation (Eisenberger 2015; Eisenberger et al. 2017). Applied to our study, darker-skinned Black Americans may experience higher risk of chronic inflammation via colorism-related social pain. Consistent with this hypothesis, studies document elevated health risk factors commonly associated with chronic inflammation among dark-skinned Black Americans, including increased cardiometabolic risk and rapid weight gain (Cobb et al. 2016; Hargrove 2018, 2019; Moore, Williams, and Baird 2021; Uzogara 2019; Wassink et al. 2017). Moreover, a national study found that dark-skinned Black adults reported more discrimination, lower subjective status, and increased inflammation as they attained higher SES over the life course, particularly when compared to their White and lighter-skinned Black peers (DeAngelis et al. 2022).
Our study builds on these previous findings in two ways. First, our study is the first to directly test associations between multiple skin tone measures and reflected appraisals. Although prior scholarship theorized that repeated exposure to colorist slights can diminish self-concept among Black Americans through a process of negative reflected appraisals (Monk 2015), this relationship has not been directly tested. We test this hypothesis by examining the association between skin color and the sense of mattering, a central pillar of self-concept and an indicator of perceived social integration. “Sense of mattering” refers to the degree to which one feels acknowledged, accepted, and cared for by others (Rosenberg and McCullough 1981; Schieman and Taylor 2001). Low sense of mattering has been linked with several poor mental health outcomes, including increased depressive symptoms (Taylor and Turner 2001). Here, we conceptualize a low sense of mattering as a psychosocial indicator of internalized (negative) reflected appraisals linked to chronic exposure to colorism discrimination.
Second, we use a measure of leukocyte telomere length (LTL) to gauge patterns of accelerated cellular degradation associated with chronic inflammation (Adwan Shekhidem et al. 2019; Vaiserman and Krasnienkov 2020). Telomeres are protective protein-based end caps on chromosomes that help to preserve chromosomal stability during cell division (mitosis). Telomeres naturally shorten in length by shedding DNA base pairs during each round of mitosis. Once chromosomes lose a critical mass of telomeric DNA, cells become destabilized to the point of genomic instability in premalignant cells or cellular senescence and death in other types of cells. When enough cells lose their ability to divide and replicate, whole tissues, organs, and organ systems can malfunction. Importantly, studies demonstrate that exposure to chronic stressors—including those stemming from structural inequality or discrimination—can accelerate telomere shortening via oxidative stress and systemic inflammation (Chae et al. 2020; Lee, Kim, and Neblett 2017). Shorter telomere length is therefore a robust predictor of morbidity and mortality (Blackburn and Epel 2017; Brown et al. 2018; Lee et al. 2019; Wang et al. 2018).
For our study, telomere length serves as a parsimonious indicator of chronic colorism-related stress and inflammation embodied throughout the life course. For example, a study found that Black men who expressed more implicit racial bias—an indicator of internalized racism—exhibited shorter telomeres than their peers with less bias, especially if they also reported more perceived discrimination (Chae et al. 2014). These findings have led some scholars to speculate that shorter LTL among Black Americans could be the result of lifelong chronic stress and inflammation linked to internalized anti-Black racism (Hall 2014).
Multiple Measures of Skin Tone
Most prior scholarship on colorism and health among Black Americans has operationalized colorism-related stress using a single skin tone measure (for exceptions, see Monk 2021b; Uzogara et al. 2014; Uzogara and Jackson 2016). Within this body of work, skin tone is typically assessed in two ways, often independently of one another. The majority of studies have used an interviewer-rated measure, which captures a participant’s “observed” complexion (Roth 2016). Observed measures are thought to gauge the health consequences of prior interactions with other people or institutions who may treat participants unequally based on their complexions. Studies employing interviewer-rated skin tone have documented associations between darker skin, increased discrimination, and ultimately, worse health (Armstead et al. 2014; Cobb et al. 2016; DeAngelis et al. 2022; Monk 2015; Uzogara 2019; Wassink et al. 2017).
A second group of studies has used self-rated skin tone measures (Louie 2020; Monk 2015). Self-rated skin tone is thought to reflect a participant’s relative sense of self-worth and position in broader stratification hierarchies, which stem from the internalization of anti-Black stigma and other experiences related to skin color over the life course (Monk 2015). Indeed, compared to observed skin tone measures, evidence suggests that self-perceived skin tone is a more robust predictor of adverse health outcomes tied to social positioning and experiences with discrimination and inequality (Fuentes et al. 2021). Studies using self-rated skin tone have also found associations between darker perceived skin tone and worse mental and physical health (Louie 2020; Monk 2015).
Prior work provides critical insights into the health correlates of interviewer- and self-rated skin tones. However, two key measurement issues remain unaddressed. First, few studies have examined both measures at once. One exception is Monk (2015), who found that when both measures were considered, only self-rated skin tone predicted mental health and hypertension, suggesting self-rated skin tone may be more sensitive to colorism-related stress.
Second, we were unable to find a study that has considered discrepancies between skin tone measures. Put simply, how a person sees themself may not always align with how others see them, and this misalignment itself may be stressful (Campbell and Troyer 2007). Skin tone discordance, in particular, may gauge stress processes related to differences in how one identifies and expects to be treated, on the one hand, and how one is actually treated, on the other. For example, given understandings of anti-dark stigma, someone who perceives themself as darker than how others view them may experience chronic stress from regularly anticipating hostile interactions with other people and institutions (Monk 2015). Alternatively, some prior work suggests that this same person may enjoy less stress and more health benefits from being perceived by others as a member of a privileged racialized group (Jones et al. 2008) — in this case, being perceived as lighter than they would rate themselves. Moreover, discriminatory experiences may be particularly distressing for individuals who perceive themselves as lighter than how others view them given the mismatch between expectations (e.g., of preferential treatment and/or limited discriminatory experiences) and actual experiences (e.g., of discrimination). In short, outcomes may vary not only by self- and interviewer-rated skin tone but also by the degree of discordance between the two.
Data and methods
Data
Data came from self-identified Black respondents (N = 627) of Vanderbilt University’s Nashville Stress and Health Study (NSAHS), a probability survey of working-age, non-Hispanic Black and White women and men who lived in Davidson County, Tennessee, between 2011 and 2014. Data were collected using multistage, stratified cluster sampling techniques with census block groups as the primary sampling unit. Fifty-nine percent of contacted persons participated in the study. Trained, race-concordant interviewers conducted computer-assisted interviews in the respondent’s home or on Vanderbilt’s campus. Interviews lasted approximately three hours. On the morning following the interview, clinicians visited participants’ homes to collect a fasting 12-hour urine sample and blood panel prior to breakfast. Fewer than 2% of respondents refused to provide biomarker data.
For more details on NSAHS data collection and validation, see Turner, Brown, and Hale (2017).
Measures
Sense of mattering
We measured reflected appraisals with a five-item index for sense of mattering (Rosenberg and McCullough 1981). Respondents answered the following questions: (1) “How much do you feel others would miss you if you went away?”; (2) “How important do you feel you are to other people?”; (3) “How much do you feel other people pay attention to you?”; (4) “How interested are people generally in what you say?”; and (5) “How much do other people depend on you?” Original response options were on a 4-point Likert scale ranging from “a lot” (=4) to “not at all” (=1). To aid interpretation, we rescaled items into ordinal percentile ranks ranging from 0 (“not at all”) to 100 (“a lot”). Higher scores indicated a stronger sense of mattering (α = .75).
Leukocyte telomere length
We measured cellular degradation related to chronic inflammation with LTL. Average LTL was measured as the ratio of telomeric DNA (T) to a single-copy sequence (T/S ratio) via the monochrome multiplex quantitative polymerase chain reaction method, with albumin as the single-copy reference sequence (Cawthon 2009). LTL scores reflected the average of two separate measures that obtained R2 values of .94 across independent samples. LTL scores were continuous and normally distributed and reflected relative scores among the NSAHS sample rather than absolute counts of DNA base pairs. Higher scores indicated longer telomeres or less cellular aging (see Hill et al. 2016).
Skin tone
We assessed three measures of skin tone. Respondents were asked, “Compared to most Black people, what shade is your skin color?” Response options included very dark, dark, medium, light, and very light. Interviewers were asked to rate respondents’ complexions as either very dark, dark, somewhat dark, medium, somewhat light, light, or very light. We combined “dark/somewhat dark” and “light/somewhat light” for consistency with the self-rated skin tone measure. Both measures were coded such that higher values reflect darker skin shades. We subtracted the self-rated skin tone measure from the interviewer-rated skin tone measure to construct a third measure, which captures discordance between self- and interviewer-rated skin tones. This resulted in five categories of concordant and discordant skin tone ratings: (1) concordant light (reference), (2) concordant medium, (3) concordant dark, (4) discordant light (i.e., lighter self-rating), and (5) discordant dark (i.e., darker self-rating).
Covariates
Prior research suggests that darker-skinned Black Americans are less likely to be married and tend to have fewer socioeconomic resources than their lighter-skinned peers, presumably due to colorism discrimination (Reece 2019). Given that marital status and SES also tend to be associated with health, our models controlled for employment status (1 = full-time, 0 = part-time/un-employed), marital status (1 = married, 0 = single), educational attainment (in years), and household income (ordinal: 0 = none, 15 = $135,000 or more). Our models also included covariates for age (in years) and sex (1 = female, 0 = male).
Analytic Strategies
Our main analyses proceeded in three steps. First, we assessed basic descriptive statistics of study variables stratified by our two self-rated and interviewer-rated skin tone measures (Table 1). We estimated bivariate associations between skin tone groups and sense of mattering/LTL and examined whether these associations followed a linear (monotonic) pattern across groups. We also assessed whether values for covariates differed systematically across skin tone categories. We identified statistically significant between-group differences using chi-square and t tests.
Descriptive Statistics of Study Variables, Nashville Stress and Health Study (2011–2014) Black Subsample (N = 627).
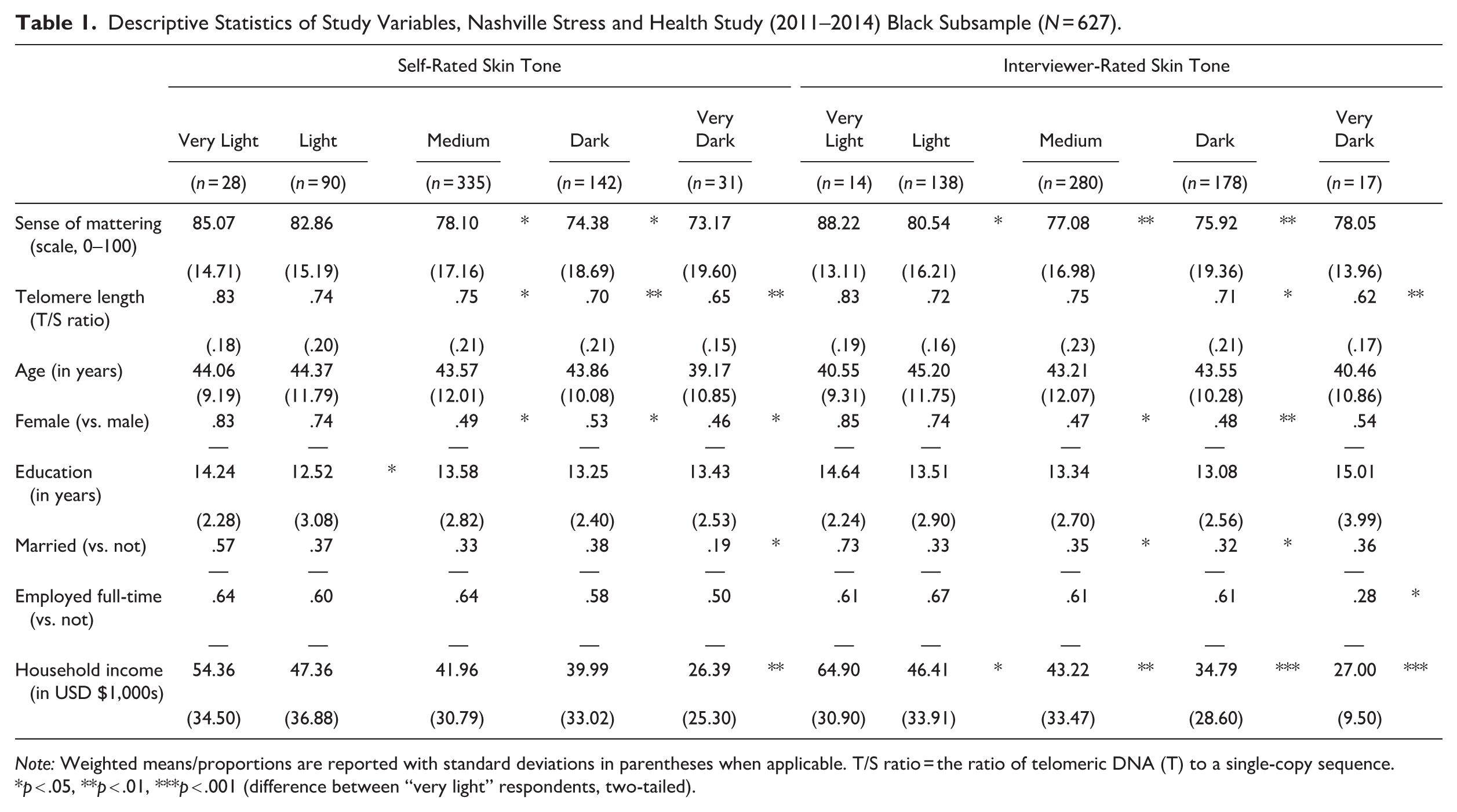
Note: Weighted means/proportions are reported with standard deviations in parentheses when applicable. T/S ratio = the ratio of telomeric DNA (T) to a single-copy sequence.
p < .05, **p < .01, ***p < .001 (difference between “very light” respondents, two-tailed).
Second, we tested a series of nested linear regression models of mattering and LTL (Tables 2 and 3, respectively). For both outcomes, Models 1 and 2 tested bivariate linear associations between the outcome and self- and interviewer-rated skin tone, respectively. Model 3 tested self- and interviewer-rated skin tone simultaneously. Model 4 finally added covariates.
Robust Linear Regression Estimates of the Sense of Mattering, Nashville Stress and Health Study (2011–2014) Black Subsample (N = 627).
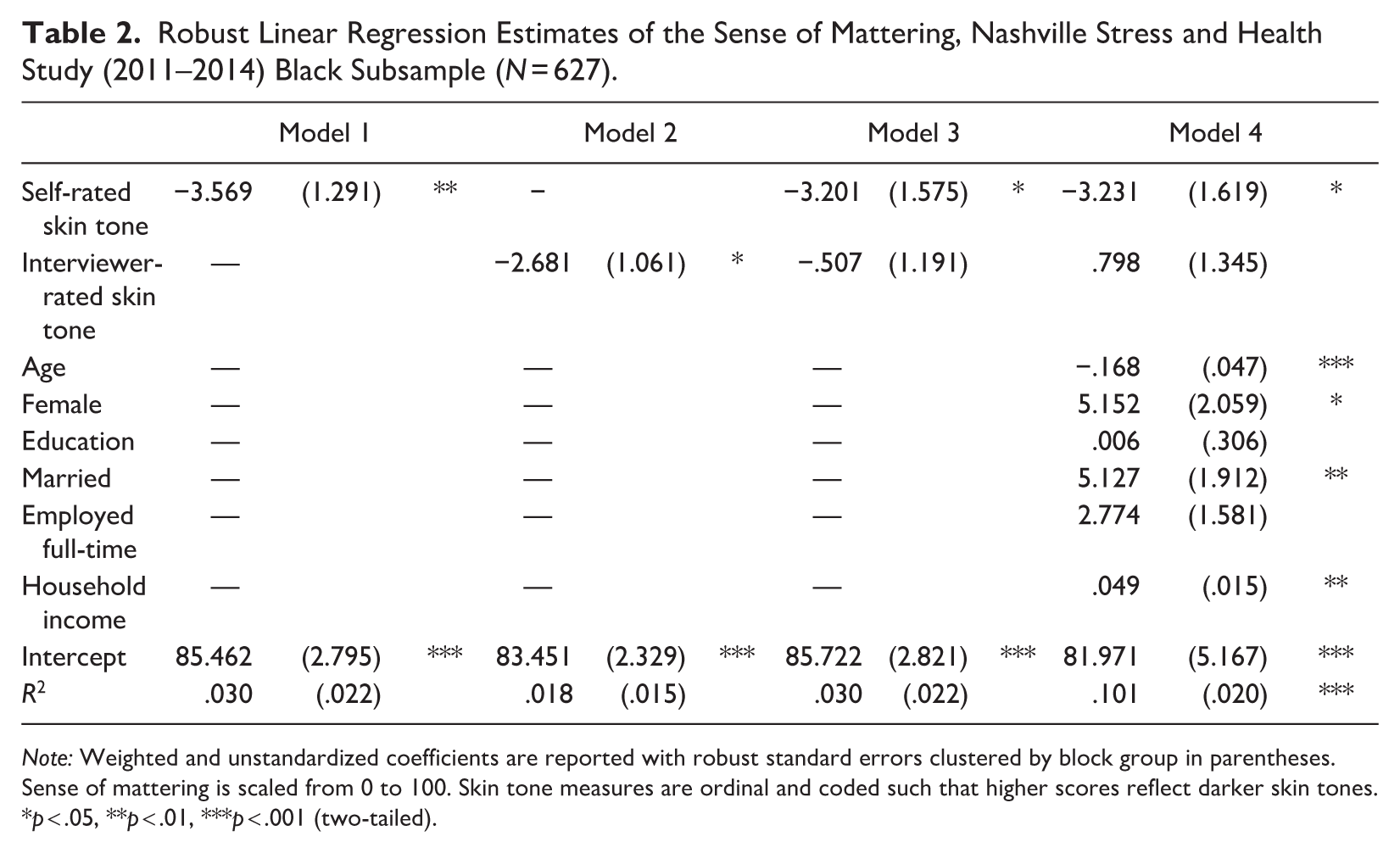
Note: Weighted and unstandardized coefficients are reported with robust standard errors clustered by block group in parentheses. Sense of mattering is scaled from 0 to 100. Skin tone measures are ordinal and coded such that higher scores reflect darker skin tones.
p < .05, **p < .01, ***p < .001 (two-tailed).
Robust Linear Regression Estimates of Leukocyte Telomere Length: Nashville Stress and Health Study (2011–2014) Black Subsample (N = 627).
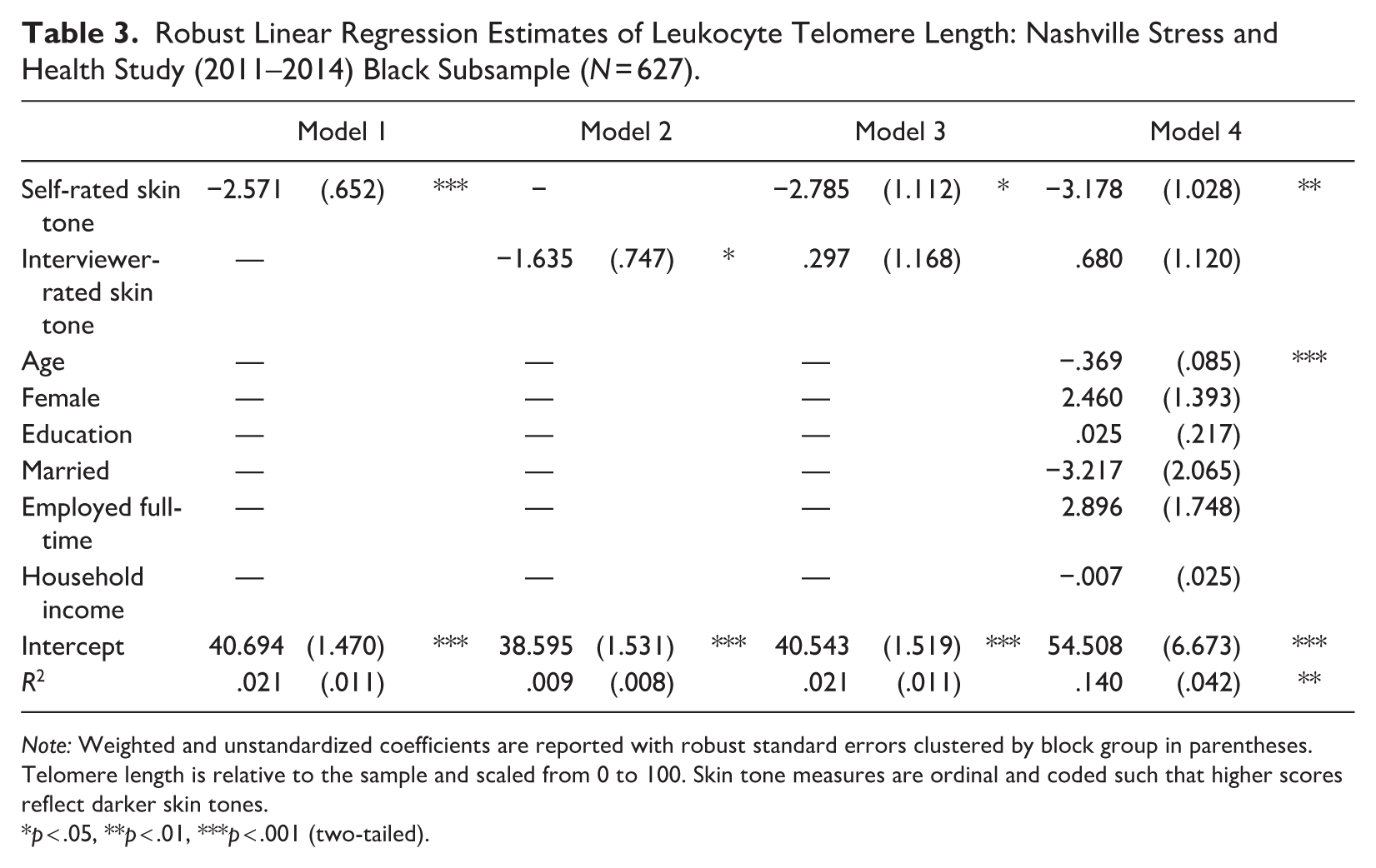
Note: Weighted and unstandardized coefficients are reported with robust standard errors clustered by block group in parentheses. Telomere length is relative to the sample and scaled from 0 to 100. Skin tone measures are ordinal and coded such that higher scores reflect darker skin tones.
p < .05, **p < .01, ***p < .001 (two-tailed).
Third, we tested associations between our measure of discordant skin tone rating and mattering/LTL (Table 4). Model 1 compared respondents who perceived their skin shade to be lighter or darker than the interviewer (i.e., discordant light/dark) with their peers who rated their skin tone the same shade as the interviewer (i.e., concordant). Model 2 disaggregated the concordant group into concordant light, concordant medium, and concordant dark, with concordant light serving as the reference group.
Testing Associations with Measures of Discordant Skin Tone Ratings, Nashville Stress and Health Study (2011–2014) Black Subsample (N = 627).
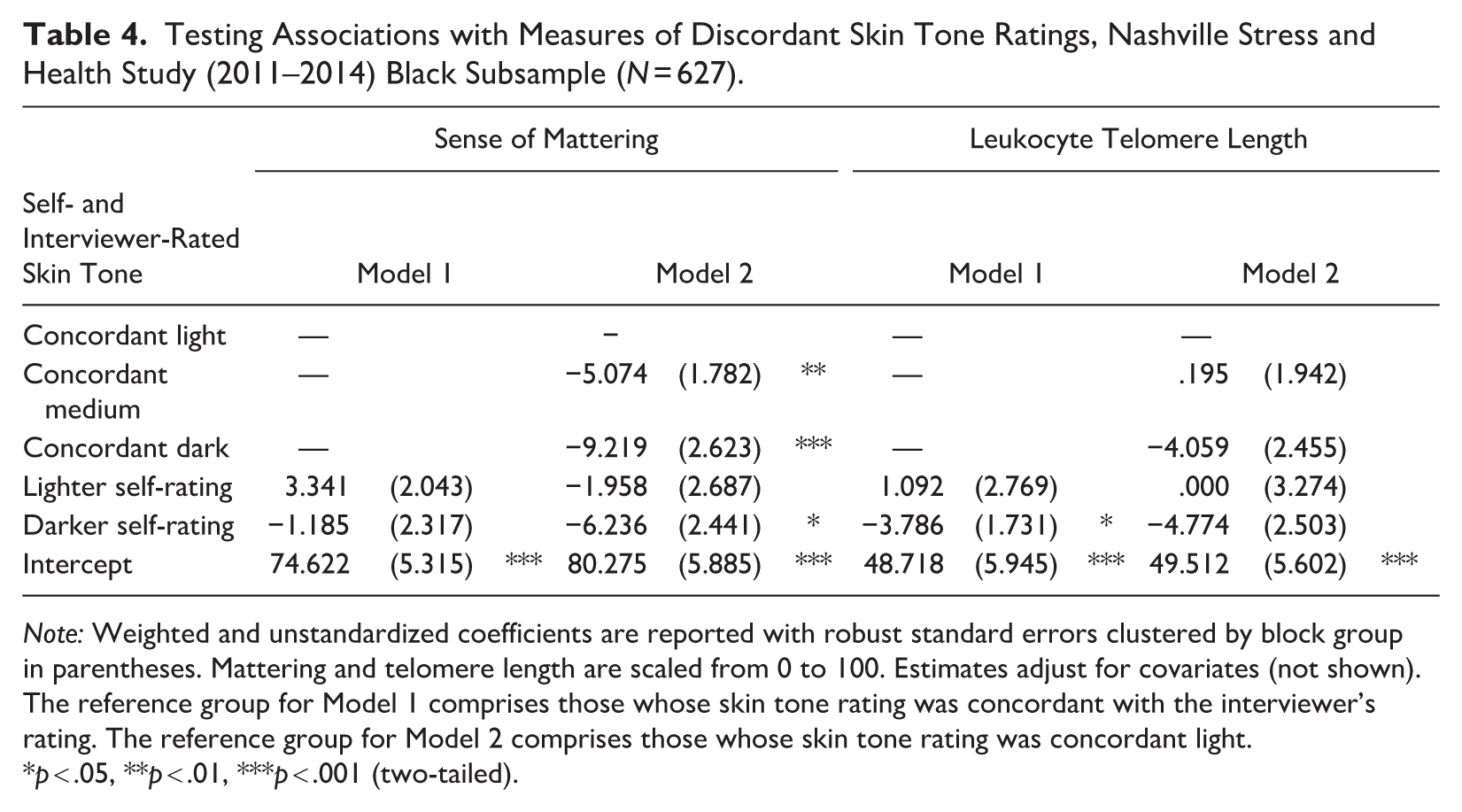
Note: Weighted and unstandardized coefficients are reported with robust standard errors clustered by block group in parentheses. Mattering and telomere length are scaled from 0 to 100. Estimates adjust for covariates (not shown). The reference group for Model 1 comprises those whose skin tone rating was concordant with the interviewer’s rating. The reference group for Model 2 comprises those whose skin tone rating was concordant light.
p < .05, **p < .01, ***p < .001 (two-tailed).
To account for complex survey design, all estimates included poststratification weighting and robust standard errors clustered by block group to permit generalizability to Davidson County’s population of working-age Black women and men. Estimates were derived and missing observations replaced using full information maximum likelihood procedures (Enders and Bandalos 2001). Our findings were substantively identical when missing observations were handled with listwise deletion.
Finally, relying on key tenets of the sociology of stress (Pearlin 1989), we tested a series of interactions to determine whether other contextual factors (e.g., discrimination, familial support) moderate associations between our skin tone measures and mattering/LTL. We briefly report on this sensitivity analysis in the discussion below and describe the measurement of each moderator alongside the tabulated results in the supplement (see Appendix A, Table A1, and Table A2 in the online version of the journal).
Results
Table 1 reports weighted descriptive statistics of our study variables stratified by self- and interviewer-rated skin tone groups. Average scores on both sense of mattering and LTL measures tend to diminish linearly from lighter to darker skin tones, indicating lower sense of mattering and shorter LTLs among darker-skinned Black respondents. This pattern holds for both self- and interviewer-rated skin tones. Moreover, compared to their lighter peers, those who perceive their skin to be very dark are generally younger in age and male, have lower educational attainment, are not married and not employed full-time, and report the lowest household incomes. With some exceptions, similar disparities are also found among interviewer-rated skin tone groups.
Table 2 reports robust linear regression estimates of sense of mattering. Models 1 and 2 indicate that self-rated skin tone and interviewer-rated skin tone are both independently and negatively associated with sense of mattering such that darker skin tones are associated with a lower sense of mattering. However, only self-rated skin tone is associated with mattering after accounting for interviewer-rated skin tone and covariates. Recall that mattering is scaled from 0 to 100 and that skin tone is coded such that higher values reflect darker shades. Thus, in Model 4, an ordinal increase in self-rated darker skin tone predicts an average 3.23% decrease in mattering, conditional on interviewer-rated skin tone and covariates (b = −3.231, p < .05).
To put the magnitude of this association into context, Figure 1 shows that self-rated darker skin tone is more strongly associated with diminished mattering than another common predictor of low mattering: older chronological age. Moreover, the gap in average mattering scores across self-rated skin tone categories is approximately two-thirds the gap between respondents who are single versus married and male versus female. This gap in mattering is also comparable to respondents who are $66,000 apart in annual household income.
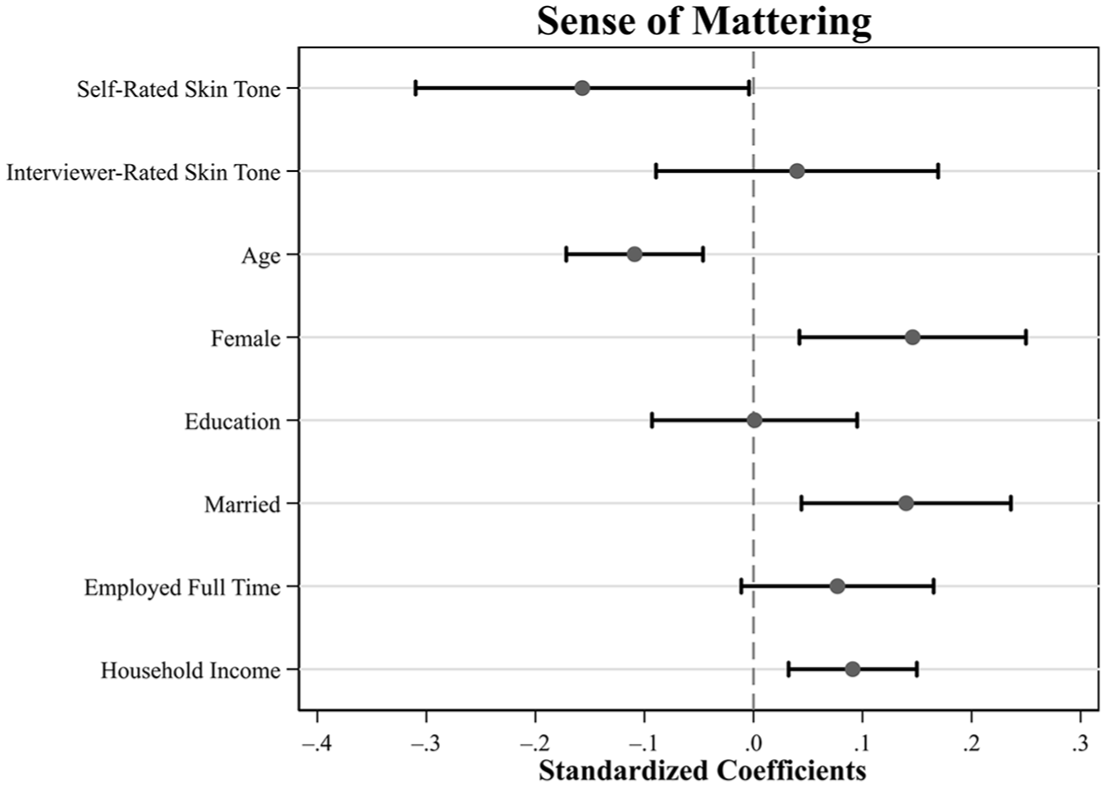
Standardized Linear Coefficients Representing the Associations between Sense of Mattering, Multiple Measures of Skin Tone, and Covariates, Nashville Stress and Health Study, Black Subsample (N = 627).
Table 3 reports robust linear regression estimates of LTL. Similar to sense of mattering, results show that although self-rated and interviewer-rated skin tone ratings are independently and negatively associated with LTL (Models 1 and 2, respectively), only self-rated skin tone is associated with LTL after accounting for interviewer-rated skin tone and covariates. For the sake of comparison, LTL has been rescaled to range from 0 (shortest in the sample) to 100 (longest in the sample). In Model 4, an ordinal increase in self-rated darker skin tone predicts an average 3.18% decrease in LTL, conditional on interviewer-rated skin tone and covariates (b = −3.178, p < .01). The average gap in LTL across self-rated skin tone categories is roughly equivalent to eight additional years of chronological age (age: b = −.369; see also Figure 2).
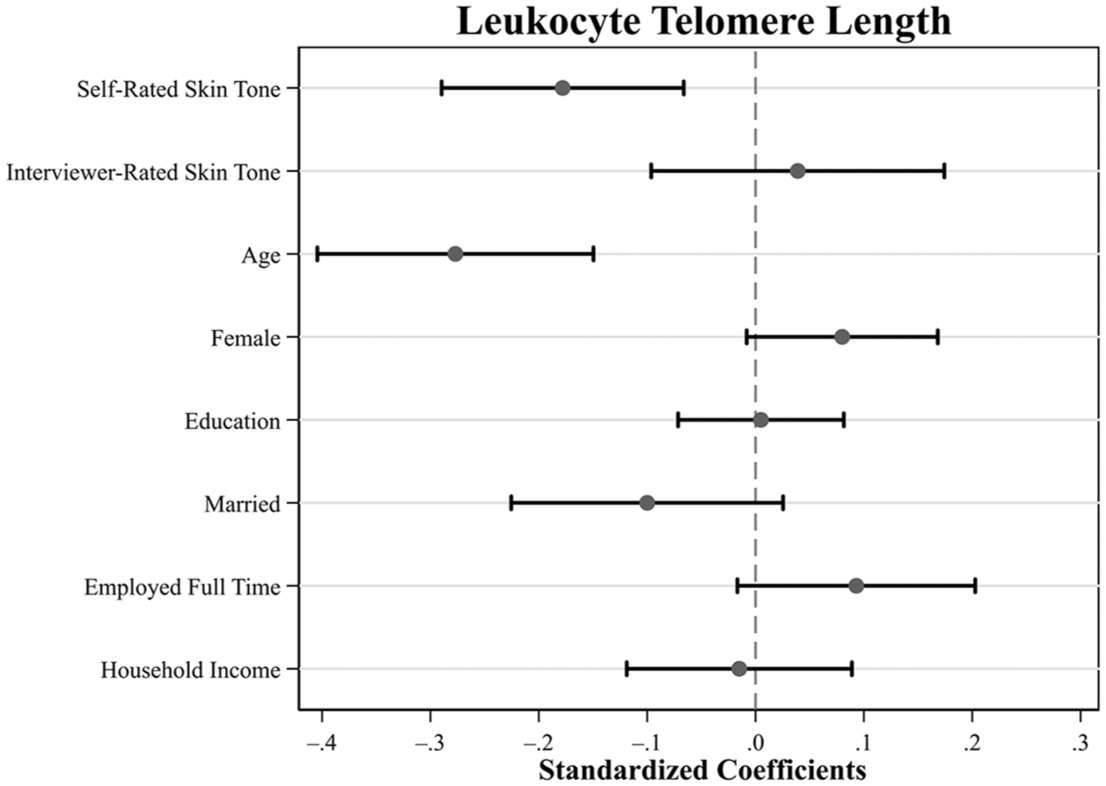
Standardized Linear Coefficients Representing the Associations between Telomere Length, Multiple Measures of Skin Tone, and Covariates, Nashville Stress and Health Study, Black Subsample (N = 627).
Table 4 reports results from our analyses using measures of discordant skin tone ratings. Results indicate that respondents who perceive their skin shade to be darker than the interviewer’s rating also generally exhibit diminished mattering and shorter LTLs. In the case of mattering, those with medium and dark concordant skin tones and those with discordant dark skin tones reported lower levels of mattering relative to their concordant light counterparts. For LTL, a significant gap emerges between discordant dark and all concordant groups.
Discussion
Health inequities predicated on skin tone are well documented among Black Americans. When compared to their lighter-skinned peers, darker-skinned Black Americans typically report worse health across several outcomes, including cardiometabolic disorder, psychological distress, suicidality, and depressive symptoms (Armstead et al. 2014; Cobb et al. 2016; DeAngelis et al. 2022; Monk 2015; Uzogara 2019; Wassink et al. 2017). However, two critical gaps in the literature on colorism and health inequity among Black Americans remain.
First, studies have found associations between exposure to colorism and various indicators of neuroendocrine and cardiovascular stress (Cobb et al. 2016; DeAngelis et al. 2022). However, the underlying biopsychosocial mechanisms through which exposure to colorism becomes embodied over time are largely unknown. Second, it remains unclear whether different types of skin tone measures are interchangeable or if they each capture distinct colorism-related stress processes. Studies conducted outside of the United States mostly suggest that self-rated skin tone is more sensitive to colorism-related stress processes than interviewer-rated skin tone measures (Fuentes et al. 2021). Yet this phenomenon remains relatively underexplored in U.S. populations. Addressing these questions is critical for improving our understanding of colorism as a pervasive health risk for Black Americans. These questions also have important methodological implications for future health inequity research.
Our study extends prior research on colorism and health inequity among Black Americans in three ways. First, this is among the first studies to document an association between skin tone and accelerated cellular degradation within the immune system. Specifically, we found that those with darker self-rated skin tones typically exhibited shorter leukocyte telomere length than their lighter-skinned counterparts. These patterns persisted regardless of the respondent’s age, sex, SES, and interviewer-rated skin tone. Research on colorism and physical health among Black Americans has mostly documented associations between skin tone and cardiovascular indicators, including cardiometabolic disorder, hypertension, and body mass index (Armstead et al. 2014; Cobb et al. 2016; DeAngelis et al. 2022; Hargrove 2018, 2019; Klag et al. 1991; Monk 2015, 2021a; Wassink et al. 2017). Our findings extend this line of work by demonstrating that accelerated cellular degradation from chronic inflammation and immune system damage is another biologically plausible mechanism linking colorism-related stressors to health inequities among Black Americans.
Second, this study is the first to directly document negative reflected appraisals as a parallel psychosocial mechanism of colorism-related stress. Monk (2015) hypothesized that Black Americans continuously assimilate cues about the value of their skin tone through repeated social interactions across the life course (i.e., internalized reflected appraisals). Yet data limitations of Monk’s (2015) study prevented a direct test of this hypothesis. Our study builds on Monk’s (2015) work by testing the association between skin tone and a direct measure of reflected appraisals: sense of mattering (Rosenberg and McCullough 1981). In support of Monk’s (2015) hypothesis, we found that Black Americans with darker self-rated skin tones also tended to report a lower sense of mattering than their lighter-skinned counterparts. Again, these patterns persisted regardless of the respondent’s sociodemographic characteristics or interviewer-rated skin tone. This suggests that darker-skinned Black Americans may gradually learn to perceive themselves as less valuable or worthy than their lighter-skinned peers, specifically through recurring interactions with others and the broader White supremacist U.S. society. Given that reflected appraisals are considered psychosocial precursors to mental health (Taylor and Turner 2001), this finding augments prior research that found similar associations between skin tone and measures of mental health (Hargrove 2023; Louie 2020; Monk 2015, 2021a).
Collectively, our findings indicate that colorism may become embodied through dual psychosocial and biological stress processes, particularly for Black Americans who perceive themselves as dark-skinned. Our analyses comparing outcomes between respondents whose skin tone ratings were discordant from Black interviewers’ ratings further underscored this point. We found that Black respondents who rated their skin tone as darker than their race-concordant interviewers also tended to report a lower sense of mattering and shorter LTL relative to their peers whose self-rated skin tones were either concordant with or lighter than the interviewer’s rating. Black adults who perceive themselves to be darker than how Black peers view them may be hypervigilant about anti-dark societal stigma, anticipating more frequent racist interactions and/or interpreting interactions with others more negatively. Over time, chronic anticipatory stress from hypervigilance could erode dark-skinned Black Americans’ health (Hicken et al. 2013, 2014). This idea warrants additional investigation in future research.
Altogether, our findings support Goosby et al.’s (2018) framework of racism as a chronic stressor that becomes embodied through biopsychosocial processes of chronic social pain. Our study also advances this framework by extending its implications to include chronic stress and social pain from colorism (see also DeAngelis et al. 2022). Thus, although colorism is a stratification system distinct from racism, there may be similarities in the biopsychosocial mechanisms through which colorism- and racism-related stressors become embodied. This idea also warrants further research.
Our study’s third contribution relates to the measurement of colorism-related stress. We found that self-rated skin tone was the most robust predictor of mattering and LTL. Although interviewer-rated skin tone was associated with both outcomes in bivariate models, associations vanished after accounting for self-rated skin tone. This finding is consistent with Monk’s (2015) study and research from Latin American contexts that suggests that self-rated skin tone measures may be especially sensitive to health processes associated with colorism-related discrimination (Fuentes et al. 2021). Our sensitivity analyses further highlight the robustness of the association between self-rated skin tone and mattering/telomere-length (for more detail, see the Supplement in the online version of the article). Informed by stress theory’s notion that the health consequences of social stressors often vary depending on other coping resources and contexts (Pearlin 1989), we tested interactions between self-rated skin tone and eight theoretically relevant contextual moderators. We found that self-rated skin tone remained significantly correlated with lower mattering and shorter telomeres even after accounting for interactions with family support, the centrality of racial-ethnic identity, neighborhood racial composition, general daily and lifetime discrimination, and discrimination attributed to skin color. Altogether, respondents with darker self-rated skin tones reported worse outcomes regardless of their broader social contexts, possession of psychosocial resources, or prior experiences of colorism discrimination.
A major implication of these findings is that different skin tone measures likely capture distinct colorism-related stress processes. According to our results, self-rated dark skin tone appears more sensitive to stress stemming from individuals’ internalized understandings of the social stigmas attached to their complexion. Given that our study was focused on internal stress processes related to diminished self-concept and inflammation (i.e., social pain), self-rated skin tone appeared to be a more relevant measure than interviewer-rated skin tone. This result highlights the importance of deliberately selecting and interpreting skin tone measures in health research because different measures are not necessarily interchangeable (Roth 2016).
More broadly, these findings also underscore the importance for health equity researchers to carefully consider Black Americans’ self-perceptions and lived experiences with colorism. Self-rated skin tone measures have been critiqued as being too subjective and therefore inferior to more direct or “objective” measures (Dixon and Telles 2017). However, we argue that the subjectivity of self-rated skin tone (or other colorism) measures can be a strength, depending on a study’s aims, because different measures likely capture distinct aspects of colorism-related stress and health processes. This interpretation reflects similar arguments about the multidimensionality of race and racism (Roth 2016). We therefore encourage future studies in this area to include multiple measures of skin tone in their analyses when feasible or consider alternative ways of capturing colorism to better gauge the various manifestations of colorism-related stress (see Dixon and Telles 2017; Monk 2015).
Study Limitations
This study has several limitations. First, due to the cross-sectional nature of the NSAHS data, we cannot make strong causal claims about the associations between perceived skin tone and mattering or LTL. Although it appears highly unlikely that LTL influenced respondents’ perceptions of their own skin tone, a respondent’s (or interviewer’s) self-concept could have affected their perceptions of their skin tone for other reasons perhaps unrelated to colorism. However, we observed consistent findings for both LTL and mattering, which suggests that a single underlying stress process is generating both patterns (e.g., chronic social pain).
Second, our findings are only generalizable to working-age, U.S.-born Black adults who lived in Davidson County, Tennessee, between 2011 and 2014. Future research should examine whether the patterns documented here extend to younger and older Black people and those who live in other geographic contexts.
Third, when the NSAHS data were collected in 2011, telomere length was a cutting-edge measure of accelerated cellular degradation associated with biological aging. In the last decade, several new measures of epigenetic aging have been developed (Wang et al. 2022). As such, future studies should replicate these analyses using more contemporary biomarkers of epigenetic aging.
Fourth, it is likely that skin tone measures do not comprehensively capture the many plausible stress pathways through which colorism affects health. Additional measures are needed to operationalize the multiple facets of colorism, including those that assess phenotypic features beyond skin tone, the social meanings ascribed to complexion, and the consequences of those meanings. This represents an important avenue for future research.
Finally, our sample size precluded us from stratifying our analyses by gender. However, some evidence suggests that skin tone disparities are stronger or only observed among Black women (Hargrove 2018, 2019; Perreira, Wassink, and Harris 2019; Perry, Stevens-Watkins, and Oser 2013; Uzogara 2019). Future studies should interrogate whether there are gender differences in the patterns detected here.
Conclusion
Our study extends the existing literature on racialized health inequities by illuminating novel biopsychosocial stress processes among Black Americans stemming from legacies of colorism. Moreover, our study demonstrates that different skin tone measures gauge distinct colorism-related stress processes beyond more common survey measures, such as perceived discrimination. These findings have critical implications for scholars interested in racialized health inequities in the United States, broadly construed, and the granular stress processes generating health inequities among Black Americans, specifically. Our findings indicate that anti-dark ideologies, particularly anti-Black stigma, continues to operate as an insidious chronic stressor that can undermine the self-concepts and health of Black Americans.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251364373 – Supplemental material for Colorism and Health Inequities among Black Americans: A Biopsychosocial Perspective
Supplemental material, sj-docx-1-hsb-10.1177_00221465251364373 for Colorism and Health Inequities among Black Americans: A Biopsychosocial Perspective by Alexis C. Dennis, Reed DeAngelis, Taylor W. Hargrove and Jay A. Pearson in Journal of Health and Social Behavior
Footnotes
Acknowledgements
Telomere data were processed by the Friedman lab at Vanderbilt University. Early iterations of this research were presented at the annual meetings of the Interdisciplinary Association for Population Health Science (2022) and the Population Association of America (2024).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research uses secondary data from the Nashville Stress and Health Study, a project led by the late R. Jay Turner and funded by the National Institute on Aging (R01AG034067). Reed DeAngelis received support from the Duke Aging Center Postdoctoral Research Training Grant (NIA T32-AG000029), and the Population Research Infrastructure (P2C-HD050924) and Biosocial Training (T32-HD091058) programs awarded to the Carolina Population Center at the University of North Carolina at Chapel Hill by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. This content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Appendix A is available in the online version of the article.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.