
Abstract
The John Henryism hypothesis (JHH) suggests high John Henryism may adversely affect the health of individuals with low socioeconomic status (SES). Although prevalent among Black Americans, its impact on Black women’s mental health across ethnic subgroups remains understudied. Using National Survey of American Life data (2001–2003), a factor analysis and negative binomial regression examined John Henryism patterns and psychological distress among 1,209 African American and 371 Caribbean Black women. Distinct factor structures indicated the need for group-specific versions of John Henryism variables to capture its role within each population. The analysis found no direct link between John Henryism and distress for either group. However, after accounting for sociodemographic factors and stressors, high John Henryism was associated with lower distress among Caribbean Black women. Evidence supporting the JHH was found only among Caribbean Black women, where John Henryism was protective for those with low and moderate SES but unrelated to distress for high-SES individuals.
The recently released Frontline PBS documentary, “Two American Families: 1991 to 2024,” explores the enduring pursuit of the “American Dream,” the belief that hard work and perseverance lead to upward mobility and success (Fredericks et al. 2024; Mortimer, Mont’Alvao, and Aronson 2020; Walker 2014). The film follows two Milwaukee families—the Stanleys, who are Black, and the Neumanns, who are White—and documents their struggles with economic instability over three decades (Fredericks et al. 2024). By the end, we return to Jackie Stanley, the Black family’s matriarch, now 70 years old and living with multiple chronic health conditions. Despite her exhaustion, Jackie continues working full-time as a realtor, supplementing her husband’s pension and sustaining the family’s finances. Reflecting on her relentless efforts, she tearfully admits, “I’m tired, and I don’t know how to rest.”
Jackie Stanley’s experience reflects the challenges many Black Americans face in striving for economic security, often at great personal cost (Mortimer et al. 2020; Walker 2014). Despite these difficulties, 52% of Black Americans still believe in the possibility of achieving the American Dream (Borelli 2024). Yet systemic racism and economic barriers persist, impeding progress and contributing to significant psychological distress (Hudson, Collins-Anderson, and Hutson 2023; Sellers and Neighbors 2008; Williams 1998). Mrs. Stanley’s story further illustrates the unique obstacles faced by Black women, who continue to make critical contributions to the economy and their communities while remaining economically undervalued, underpaid, and overburdened (DuMonthier, Childers, and Milli 2020). These disparities coupled with systemic oppression and chronic stress, gendered racism, and financial strain lead to disproportionate mental health burdens (Allen et al. 2019; Collins 2000, Essed 1991; Erving, Patterson, and Boone 2021; Robinson, Erving, and Thomas Tobin 2023; Thomas, Witherspoon, and Speight 2008; Woods-Giscombé et al. 2016).
Although all Black women contend with structural barriers—including racism, gender discrimination, and economic marginalization—their experiences navigating these challenges are shaped by historical, cultural, and social contexts (Saleem, Lambert, and Rose 2022; Sanders and Mahalingam 2012). The U.S. Black population has grown significantly since the 1960s, with Caribbean Black immigrants constituting a large portion of this growth (Erving and Smith 2022; Lorick-Wilmot 2014; Thomas 2012). Despite this demographic shift, research on second-generation Caribbean Black women remains limited, particularly in terms of how they navigate stress and coping strategies (Lorick-Wilmot 2010, 2014; Portes and Zhou 1993; Waters 1999).
Black Feminist Thought (Collins 2000) provides a useful lens for understanding how shared experiences of structural oppression manifest in distinct ways within Black women’s diverse communities. A “Black women’s collective standpoint” acknowledges that although all Black women face systemic barriers, their strategies for resilience may be shaped by intersecting social, historical, and cultural influences. For second-generation Caribbean Black women, this includes navigating an “in-between” identity—racialized as Black in the United States while maintaining ethnic ties to their family’s country of origin (Ida and Christie-Mizell 2012). Given that coping mechanisms are often informed by lived experiences and intergenerational socialization (Meyer, Schwartz, and Frost 2008; Pearlin et al. 1981; Thoits 2010), this study examines how these distinct contexts shape coping strategies like John Henryism among Black women.
Among the many coping strategies employed by Black women, John Henryism reflects a deeply ingrained ethos of perseverance and self-reliance, shaped by both historical oppression and responses to economic and social constraints. Rooted in historical efforts to achieve economic progress despite racial discrimination, John Henryism is a high-effort coping style and culturally relevant form of resilience characterized by (1) mental and physical stamina, (2) commitment to hard work, and (3) an unwavering determination to succeed (James, Hartnett, and Kalsbeek 1983). Originally conceptualized to bring attention to Black Americans’ responses to structural racism post-Civil War, John Henryism remains an important framework for understanding how Black individuals persist in a society that often limits their opportunities (James 1994, 2019; James, Forde, and Glover 2024). Because coping strategies are often socialized across generations, John Henryism continues to shape how Black women navigate racism, capitalism, and systemic inequities today (Hall 2018; Meyer et al. 2008; Pearlin et al. 1981). Although John Henryism can promote resilience, engaging in high-effort coping for prolonged periods—particularly without adequate resources—may ultimately contribute to negative health outcomes (James 1994, 2019). Moreover, the John Henryism hypothesis (JHH) (James 1994; James et al. 1983) provides a critical framework for understanding how John Henryism interacts with socioeconomic mobility. The JHH posits that although high-effort coping may be psychologically protective for individuals with sufficient resources, it can be detrimental for those with low socioeconomic status (SES) because sustained effort without structural support may lead to health risks, including psychological distress (James 1994; James et al. 1983).
Black women navigate persistent economic and social disparities, making it essential to examine how John Henryism influences psychological distress across SES levels. Additionally, distinct social and cultural contexts may shape how African American and Caribbean Black women experience John Henryism and its mental health implications. Although both groups face structural barriers, differences in historical background, family migration experiences, and socialization may lead to distinct approaches to high-effort coping (Saleem et al. 2022; Sanders and Mahalingam 2012). For instance, some Black immigrant families emphasize perseverance and meritocracy as key to success in the United States (Waters 1999), potentially shaping how second-generation Caribbean Black women engage with John Henryism. By contrast, African American families, whose lineage is rooted in generations of systemic racism and economic exclusion in the United States, may socialize their children to recognize both the necessity of hard work and the enduring realities of racial and economic inequality (James 1994, 2019; James et al. 2024). These distinct orientations toward hard work and upward mobility may influence whether John Henryism serves as a protective coping mechanism or a source of distress.
This study examines how John Henryism shapes psychological distress across SES among Black women, assessing distinct patterns among African American and Caribbean Black women. By investigating these dynamics, we assess the applicability of the JHH across Black women’s diverse experiences, deepening our understanding of coping strategies and mental health in the context of the persistent pursuit of socioeconomic mobility.
Background
Psychological Distress among Black Women
Prior research demonstrates that the compounded effects of racism and sexism experienced by Black women not only produce multiple chronic stressors that permeate various aspects of their lives but may also facilitate distinct forms of coping (Erving et al. 2022; Robinson 2022a, 2022b; Robinson and Thomas Tobin 2021). Together, the unique stress and coping experiences of Black women may contribute to their heightened levels of psychological distress (Allen et al. 2019; Woods-Giscombé 2010; Woods-Giscombé et al. 2016). The social stress paradigm (Pearlin 1989; Turner 2013), a prominent theoretical framework in the sociology of mental health, posits that coping is an integral component of the stress process. This paradigm suggests that an individual’s access to a variety of coping resources can significantly influence how stress ultimately impacts their health (Turner, Taylor, and Van Gundy 2004). Importantly, an individual’s social position determines not only the types of coping strategies available to them but also the effectiveness of these strategies for maintaining health (Meyer et al. 2008; Pearlin et al. 1981).
A growing body of literature has examined gender-specific coping mechanisms among Black women, such as the Superwoman schema or the “Strong Black Woman” role (Allen et al. 2019; Woods-Giscombé 2010; Woods-Giscombé et al. 2016). However, fewer studies have examined John Henryism as a form of culturally relevant coping among Black women despite its strong theoretical links to resilience, structural stress, and health (Greer 2007; James et al. 1983). For Black women, who navigate the compounded effects of racial and gender-based oppression, their coping mechanisms are particularly shaped by both structural barriers and intergenerational socialization (Saleem et al. 2022; Sanders and Mahalingam 2012). Examining these coping mechanisms is essential for understanding how Black women manage psychological distress across the life course, particularly because John Henryism may function differently for Black women compared to Black men due to gendered expectations of strength, self-sacrifice, and perseverance.
John Henryism as a High-Effort Coping Strategy for Black Women
John Henryism is a high-effort coping strategy characterized by persistent mental and physical stamina, commitment to hard work, and an unwavering determination to succeed despite structural barriers (James et al. 1983). Although originally conceptualized in relation to Black men’s experiences, recent research suggests that John Henryism is highly relevant for Black women given their unique exposure to both racism-related and gendered stressors (Robinson 2022a, 2022b; Robinson and Thomas Tobin 2021). Inspired by both the legend of John Henry and the real-life struggles of Black laborers, John Henryism was developed as a construct to explain how prolonged high-effort coping in response to structural barriers may contribute to adverse health outcomes among Black Americans (James 1994, 2019; James et al. 2024).
Yet a lesser known figure—Polly Ann, John Henry’s wife—may provide an even more salient narrative for understanding Black women’s engagement with John Henryism. Polly Ann, who took up steel driving after John Henry’s death, is portrayed as embodying both the burden and necessity of high-effort coping. Her words—“This little hammer killed John Henry. Won’t kill me, won’t kill me” (Our Native Daughters 2019)—reflect Black women’s intergenerational resilience but also their acute awareness of the costs associated with overexertion (Robinson 2022a, 2022b). Similar to Jackie Stanley in “Two American Families,” Black women often internalize a sense of responsibility to keep pushing forward despite exhaustion, financial precarity, and systemic obstacles (Robinson et al. 2023). Although it may appear as miraculous and awe-inspiring to the general public, what it takes to confront and overcome these feats is anything but effortless. Black women typically learn early on to embody strength, self-sufficiency, creativity, and courage (hooks 1993). This type of socialization has been intergenerationally transferred from both family and society at large without cease. Nevertheless, there is a severe price Black women pay for this, not just in terms of financial resources but also for mental and physical health and well-being. This gendered dimension of John Henryism, where survival and success require continual self-sacrifice, has not been sufficiently explored in health research.
John Henryism and Health
Research on John Henryism among Black women remains limited. Although numerous studies link John Henryism to physical health issues, such as hypertension and cardiovascular disease (Bennett et al. 2004; Dressler, Bindon, and Neggers 1998; James 1994, 2019; James et al. 1983; Subramanyam et al. 2013), fewer have explored its effects on mental health, particularly among Black women. Existing studies yield mixed results—some suggest that John Henryism buffers against distress (Bennett et al. 2004; Bronder et al. 2014; Kiecolt, Hughes, and Keith 2009; Robinson and Thomas Tobin 2021), and others indicate it may increase psychological strain, particularly when structural support is lacking (Hudson et al. 2016). Recent work by Perez et al. (2023) found a direct positive association between John Henryism and psychological distress among African American women, contributing to the growing literature on high-effort coping and mental health. However, their study did not explicitly test the JHH for distress given that their analysis of interactions between John Henryism and SES appeared to focus on hypertension. As such, few studies have specifically examined John Henryism’s impact on Black women’s health, particularly their mental health, with even fewer considering distinctions between African American and Caribbean Black women (Robinson 2022a, 2022b). These ethnic differences in coping strategies may have important implications for health outcomes yet remain underexplored in existing research.
The John Henryism hypothesis (JHH) suggests that high-effort coping is most effective for individuals with sufficient socioeconomic resources, whereas it may harm those with fewer resources (James 1994, 2019). Yet little is known about how the JHH applies to mental health, particularly for Black women. Studies testing this hypothesis in relation to SES and health outcomes have produced inconsistent findings (Dressler et al. 1998; Felix et al. 2019; Subramanyam et al. 2013), with some research even suggesting that lower John Henryism may increase hypertension risk in low-SES Black women. Expanding this research to include psychological distress is essential for clarifying whether John Henryism functions as a protective or maladaptive coping strategy in different socioeconomic contexts, particularly in light of potential ethnic group distinctions in how African American and Caribbean Black women engage with and experience John Henryism.
Ethnic Variations in John Henryism among Black Americans
Although John Henryism is often conceptualized as a universal coping mechanism among Black Americans, emerging research suggests that its function and impact may vary across ethnic subgroups (Robinson 2022a, 2022b). African American and Caribbean Black women may experience and employ John Henryism in unique ways due to distinct historical, cultural, and social contexts (Ida and Christie-Mizell 2012; Waters 1999). African American women’s engagement with John Henryism may be deeply embedded in intergenerational narratives of racial resilience and economic survival, whereas for Caribbean Black women, high-effort coping may be influenced by migration-based ideals of perseverance, meritocracy, and social mobility.
Despite these potential distinctions, few studies have explored how John Henryism may function distinctly for African American and Caribbean Black women, particularly in relation to mental health. A recent study by Robinson (2022a) highlights that John Henryism’s effects on self-rated health are similar between these groups, underscoring the need to examine whether these patterns also exist for psychological distress. Moreover, research on John Henryism rarely considers the ways that socialization, family expectations, and broader structural factors may contribute to variations in how high-effort coping is used across ethnic subgroups of Black women. Expanding this body of work is essential for refining the applicability of John Henryism to diverse Black populations and understanding how cultural differences shape coping strategies.
The Present Study
This study applies the social stress paradigm (Pearlin et al. 1981; Turner 2013) alongside the JHH (James 1994, 2019; James et al. 2024) and interdisciplinary perspectives on Black women’s coping and resilience (Collins 2000; Woods-Giscombé 2010) to examine how John Henryism functions as a coping resource for Black women facing structural disadvantage. The JHH posits that although high-effort coping may be psychologically protective for those with adequate resources, it can be detrimental for those with low SES because sustained effort to overcome systemic barriers can lead to health costs (James 1994, 2019). Although recent studies have considered John Henryism’s relationship with psychological distress, prior research has not explicitly tested the JHH in this context (e.g., Perez et al. 2023). However, its applicability to Black women’s mental health remains underexplored, particularly in relation to ethnic subgroups and SES levels. Most research on John Henryism has focused on physical health outcomes, with limited and mixed findings on its relationship to psychological distress among Black women. Even less is known about how John Henryism may function as a distinct coping strategy among African American and Caribbean Black women.
Building on this foundation, the present study examines how John Henryism and SES interact to shape psychological distress among African American and Caribbean Black women, addressing these gaps in the literature. We pursue three aims: (1) explore John Henryism patterns among African American and Caribbean Black women, (2) assess the direct association between John Henryism and psychological distress among African American and Caribbean Black women, and (3) test the JHH by evaluating SES as a moderator of the John Henryism–distress relationship.
Our conceptual model (Figure 1) builds on the social stress paradigm by explicitly incorporating stress exposure—including chronic stress, discrimination, and goal-striving stress—as key pathways through which socioeconomic disadvantage and systemic barriers shape psychological distress (Pearlin et al. 1981; Thoits 2010; Turner 2013). Although John Henryism may serve as a coping resource that mitigates distress, its benefits may be conditional on SES and the broader cultural contexts in which Black women are socialized (Erving and Thomas 2018; Robinson and Thomas Tobin 2021).
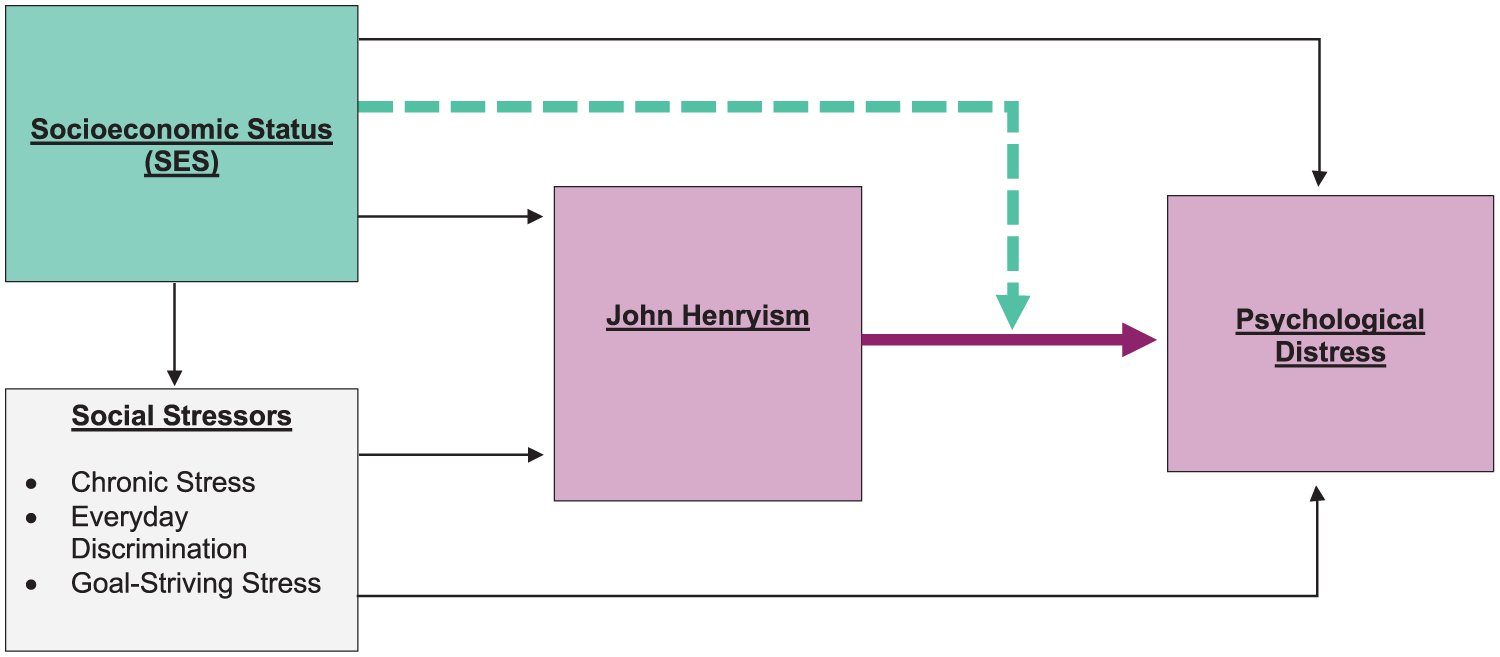
Conceptual Model of the Associations between John Henryism, Socioeconomic Status, and Psychological Distress among African American and Caribbean Black Women.
Given ethnic differences in stress experiences, socialization, and structural barriers, we stratify analyses by ethnicity to explore whether these relationships operate in distinct ways for African American and Caribbean Black women. This approach refines the applicability of the JHH for mental health and deepens understanding of culturally relevant coping among Black women. Understanding these dynamics could inform culturally relevant interventions to reduce health inequities because both SES and coping mechanisms like John Henryism are amenable to change.
Data and methods
Data for this study were drawn from the National Survey of American Life (NSAL), which took place between 2001 and 2003 (Jackson et al. 2010). Similar to the overarching purpose of the NSAL (see Heeringa et al. 2004; Jackson et al. 2004), the current study further explored diversity within the Black population, focusing on gender differences in John Henryism and psychological distress. The survey population included African American, Caribbean Black, and non-Hispanic White noninstitutionalized adults ages 18 years and older who reside in households in the contiguous United States. In the NSAL, African Americans are persons who self-identify as Black but do not report Caribbean ancestry. Caribbean Black indivduals are persons who self-identify as Black and answered affirmatively to any of the following inclusion criteria: (1) of West Indian or Caribbean descent, (2) born within a Caribbean-area country, or (3) had parents or grandparents who were born in a Caribbean-area country. Individuals living on military bases and non-English speakers were excluded from the study. To increase comfort level, respondents were matched with interviewers of the same racial background. Interviews lasted an average of 2 hours 20 minutes.
The overall response rate for the initial survey was 71.5%. A total of 6,082 face-to-face interviews were completed, consisting of 1,621 Caribbean Black individuals and 3,570 African Americans. For the present study, data from the reinterview survey were analyzed given that it contained key study variables such as John Henryism. The reinterview survey had a 56.5% overall response rate (n = 3,438), with rates of 68.0% for White respondents (n = 606), 59.9% for African Americans (n = 2,137), and 42.9% for Caribbean Black respondents (n = 695; Jackson et al. 2010). Given this study’s focus on Black women, White individuals and men of all races were excluded (n = 1,670). Respondents missing data on key variables were also excluded (n = 188). The final analytic sample includes 1,580 Black women (1,209 African American, 371 Caribbean Black). Sensitivity analyses showed excluded cases were similar to the analytic sample on key characteristics (Robinson 2022a, 2022b).
Measures
Psychological distress was assessed in the NSAL with a seven-item (α = .85) scale (Kessler et al. 2003). They asked respondents, “In the past 30 days, about how often did you feel . . . ?,” with items indicating emotional states such as “nervous,” “hopeless,” and “worthless.” The responses ranged from 1 = all to 5 = none. We reverse-coded and summed all items such that higher scores indicated higher levels of psychological distress. Given that there was an overdispersion of zero scores for the distribution of this variable across the sample, we kept psychological distress as a count variable in the analysis (Robinson 2022b).
John Henryism was assessed in the NSAL using the validated John Henryism Active Coping Scale (JHAC-12). This 12-item validated scale (α = .82) was developed by Dr. Sherman James (Jackson et al. 2004; James et al. 1983), and respondents were asked to indicate how true each item or statement was for them. A sample item is “I’ve always felt that I could make of my life pretty much what I wanted.” (James et al. 1983). Response choices ranged from 1 = completely true to 5 = completely false. We reverse-coded and summed item responses for the scale such that higher scores indicated higher levels of John Henryism. Among African American women, the John Henryism scale included a Cronbach’s alpha of .82. A separate analysis showed that two items (Items 1 and 7) of the John Henryism scale did not capture the construct of John Henryism among Caribbean Black women. Thus, we created a John Henryism variable for this group that did not include those two items (α = .80) that was used for analysis limited to Caribbean Black women (Robinson 2022a, 2022b). To account for potential threshold effects (Kiecolt et al. 2009; Robinson and Thomas Tobin 2021) and the skewed distribution of this variable, we categorized John Henryism scores based on the 25th and 75th percentiles, resulting in the following coding: (1) low John Henryism (reference category), (2) moderate John Henryism, and (3) high John Henryism (Robinson 2022b).
Socioeconomic status (SES) was assessed in the NSAL through multiple indicators, including household income and educational attainment. Household income was measured continuously, with participants providing their household income in a dollar amount: African American women, M = $31,936.74, SD = $32,058.28, range = $0 to $200,000; Caribbean Black women, M = $33,584.43, SD = $65,286.49, range = $0 to $200,000 (Erving 2011; Jackson et al. 2004). Educational attainment was also measured continuously with participants indicating the highest number of years of education they had received: African American women, M = 12.69, SD = 2.72, range = 4 to 17; Caribbean Black women, M = 13.57, SD = 6.18, range = 4 to 17. While most values were numeric, the smallest and largest response options were categorized as “4 or less” and “17 or more” (Robinson 2022a, 2022b). We created an SES score for each of the participants. To do so, we first standardized values for household income and educational attainment. Next, we summed the scores for these two dimensions for each participant. This process created an SES index that represents the number of standard deviations higher or lower each participant’s SES level was relative to the sample’s mean SES (Erving and Thomas 2018; Robinson 2022a, 2022b). Higher scores indicated a higher level of SES. By weighing household income and educational attainment equally, this approach allowed for a more complete evaluation of SES (Brown 2014). Moreover, this method of measuring SES may depict an individual’s placement in a socially stratified society more effectively, which is based on their simultaneous positions in various social locations (Erving and Thomas 2018; Robinson 2022b).
Three indicators of stress exposure were used in the present study. Chronic stress was assessed in the NSAL with a 10-item checklist with an initial prompt of, “Over the past month or so, have you . . . ,” with items including “had health problems?” and “had family or marriage problems?” Response options were “yes” or “no.” For each participant, we summed items that were answered with “yes” such that higher scores indicated increased exposure to chronic stress (Robinson 2022b).
Everyday discrimination was assessed using the Everyday Discrimination Scale, which was developed by Williams et al. (1997). This scale includes 10 items (α = .88) that capture experiences of perceived discrimination. The overall prompt was for participants to indicate how frequently they had experienced each of the 10 items in their daily lives over the past calendar year. A sample item is, “People behave as if they think you are not honest” (Williams et al. 1997). Participants were asked to provide responses on a Likert scale of 1 = never to 6 = almost daily (Williams et al. 1997). We summed item responses for each participant such that higher scores indicated a higher frequency of experiencing discriminatory events (Robinson 2022b).
Goal-striving stress was assessed in the NSAL study through four items that measured the discrepancy between an individual’s aspirations for a goal and their achievement of said goal, weighted by the chances of achieving the goal, and the level of disappointment that they would experience if the goal was not achieved (Sellers et al. 2012). The following (from Sellers et al. 2012) is the equation for computing goal striving stress: (Aspirations − Achievement) × (Chances × Importance). Based on this equation, a continuous measure was created where higher scores indicated higher levels of goal-striving stress (Sellers et al. 2012). We assigned participants who indicated that they had no aspirations a goal-striving stress score of zero. Goal-striving stress remained a continuous variable in analysis for both African American and Caribbean Black women (Robinson 2022b).
Age was assessed continuously in the NSAL via asking participants to provide their age in years at the time of the study (Jackson et al. 2004; Robinson 2022b).
Analytic Strategy
Statistical analyses
Given prior research on ethnic differences in stress, coping, and health (Erving and Smith 2022; Williams et al. 2007), we stratified all analyses to clarify how John Henryism and SES interact in distinct ways to shape psychological distress among African American and Caribbean Black women, avoiding potentially obscured patterns in combined analyses (Whitfield et al. 2008). First, we estimated descriptive statistics (e.g., weighted means, percentages) among each group. Second, to explore John Henryism patterns, we conducted a factor analysis of the JHAC-12 to assess whether the construct operated equivalently across African American and Caribbean Black women. Specifically, we examined whether the 12 items reflected a cohesive construct within each group or if differences in factor structure suggested variation in how John Henryism is expressed. Ensuring measurement equivalence was critical for accurately interpreting group-specific patterns and avoiding biases in subsequent analyses. Distinct factor structures (Figure 2) indicated the need to use group-specific versions of the John Henryism variable in subsequent analyses to appropriately capture its role within each population (Robinson 2022b). Next, because psychological distress was a count variable with an overdispersion of zeroes, we used negative binomial regression to estimate incidence rate ratios and 95% confidence intervals (CIs) for (1) the direct association between John Henryism and psychological distress (Model 1); (2) the association between John Henryism and psychological distress, accounting for sociodemographic characteristics and stressors (Model 2); and (3) evaluating the JHH for psychological distress by testing an interaction between John Henryism and SES (Model 3).
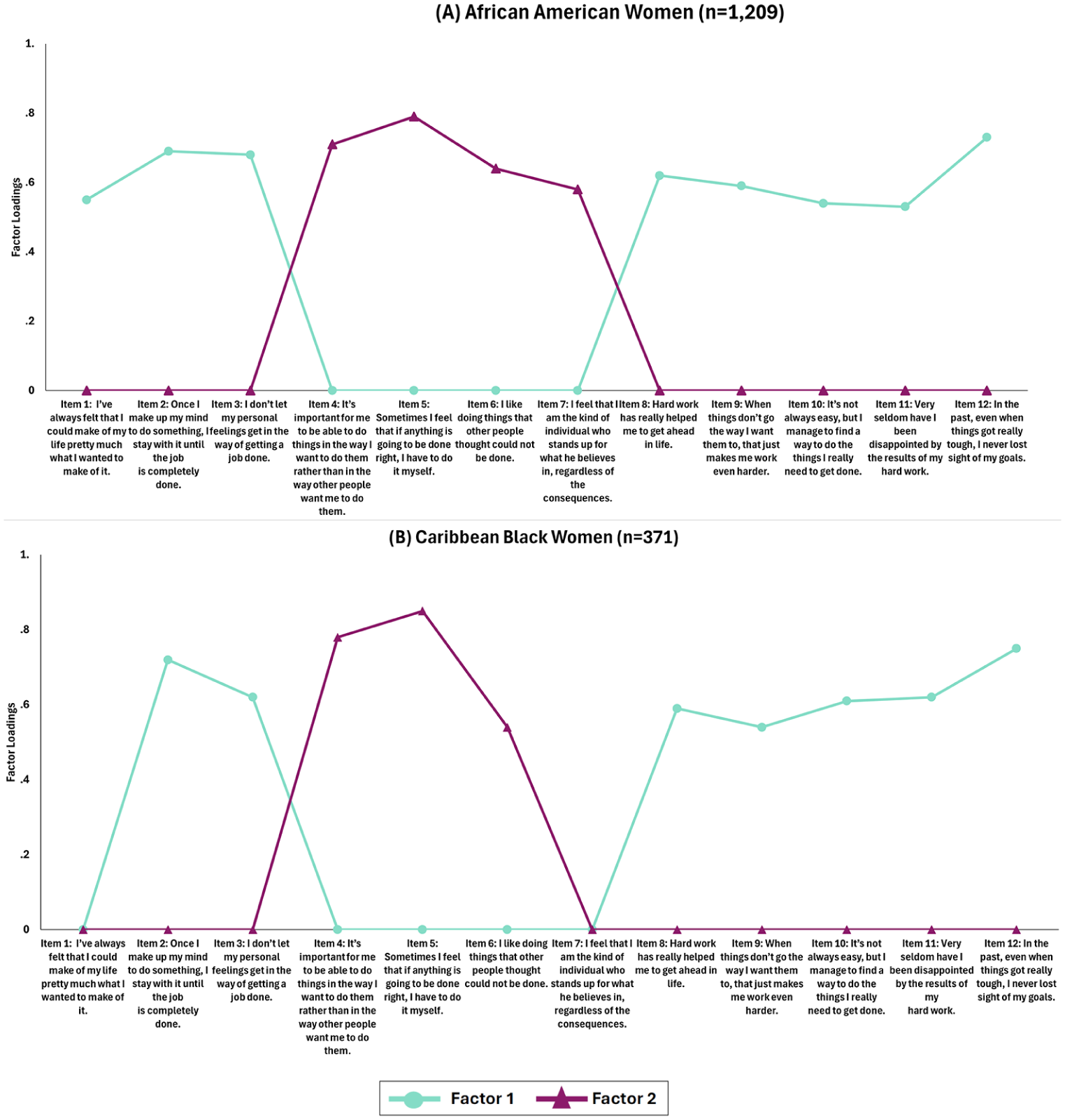
Factor Loadings of John Henryism Active Coping 12-Item (JHAC-12) Scale among African American and Caribbean Black Women, National Survey of American Life (2001-2003), N = 1,580.
Analyses were conducted using Stata 18.0 and with survey weights to account for the NSAL’s complex sampling design.
Results
John Henryism Patterns
African American women
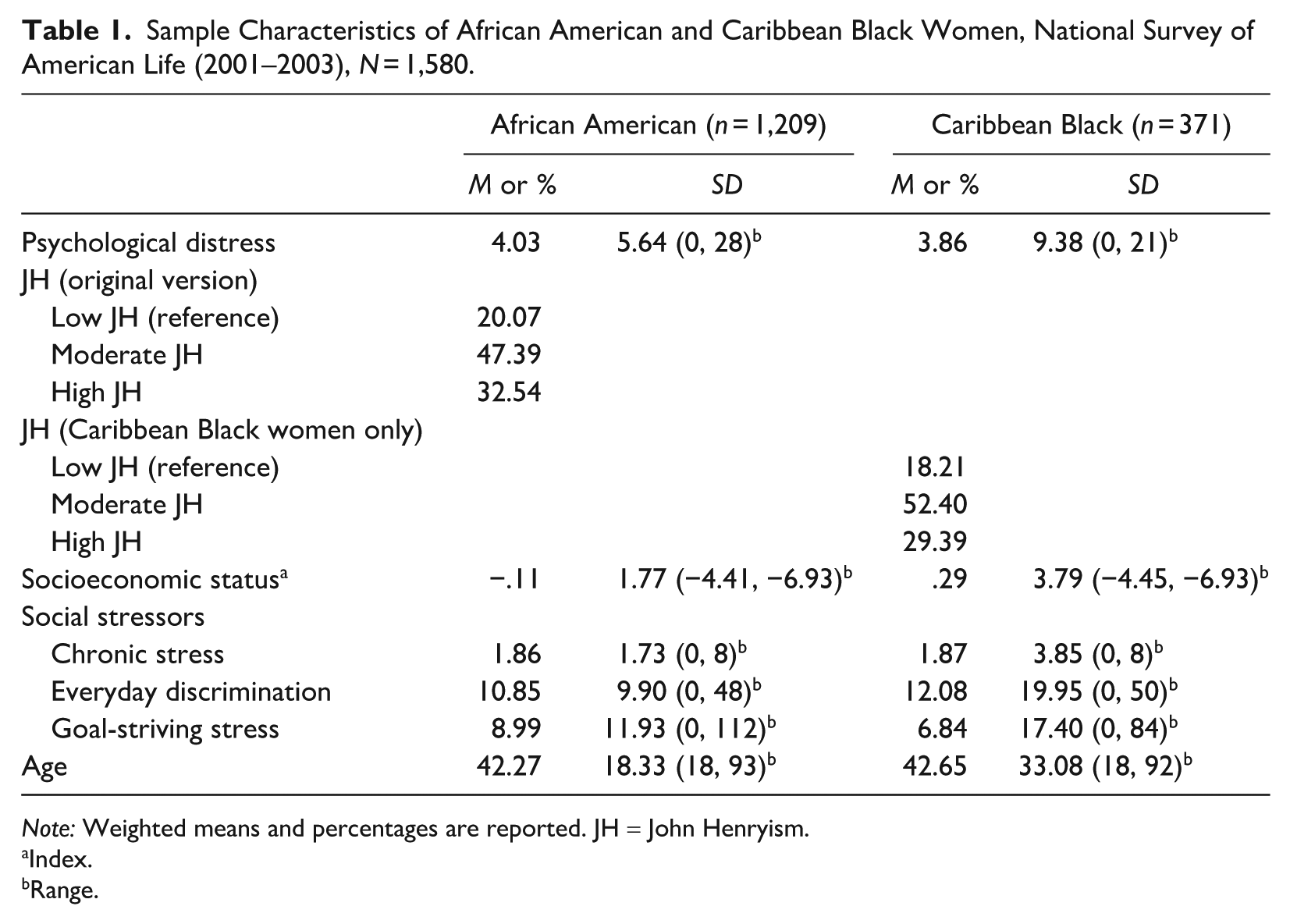
Table 1 shows the distribution of sample characteristics for African American women. The average psychological distress score for African American women in the sample was about 4 (M = 4.03, SD = 5.64, range = 0–28), which is fairly low. Our confirmatory factor analysis indicated that all 12 items of the John Henryism scale met the standard factor loading threshold of .50, confirming that the full measure reliably captured John Henryism among African American women (see Figure 2a). As a result, we retained the full 12-item measure for analyses in this group to maintain conceptual consistency with prior research. Most African American women (47.39%) reported moderate John Henryism, approximately 20% reported low John Henryism, and close to 33% reported high John Henryism. The average SES score was −.11 (M = −.11, SD = 1.77, range = −4.41 to 6.93), which indicates that most African American women reported having a lower SES.
Sample Characteristics of African American and Caribbean Black Women, National Survey of American Life (2001–2003), N = 1,580.
Note: Weighted means and percentages are reported. JH = John Henryism.
Index.
Range.
Caribbean Black women
Table 1 shows the distribution of sample characteristics for Caribbean Black women. The average psychological distress score for Caribbean Black women in the sample was 3.86 (M = 3.86, SD = 9.38, range = 0–21), which is fairly low. Among Caribbean Black women, two items of the John Henryism scale failed to meet the factor loading threshold of .50, suggesting that these specific items did not align as strongly with the underlying construct for this group (see Figure 2b). To ensure measurement validity while preserving the theoretical integrity of the scale, we excluded these two items in analyses for this group. Most Caribbean Black women (52%) reported engaging in moderate John Henryism, about 18% reported low John Henryism, and approximately 30% reported high John Henryism. The average SES score for Caribbean Black women was .29 (M = 0.29, SD = 3.79, range = −4.45 to 6.93), which demonstrates that most Caribbean Black women reported higher SES.
John Henryism and Psychological Distress
African American women
There was no direct association between John Henryism and psychological distress. After we accounted for sociodemographic characteristics and stressors (Table 2), John Henryism remained unassociated with psychological distress among this group.
Negative Binomial Regression Examining the Association between John Henryism and Psychological Distress among Black Women, National Survey of American Life (2001–2003), N = 1,580.
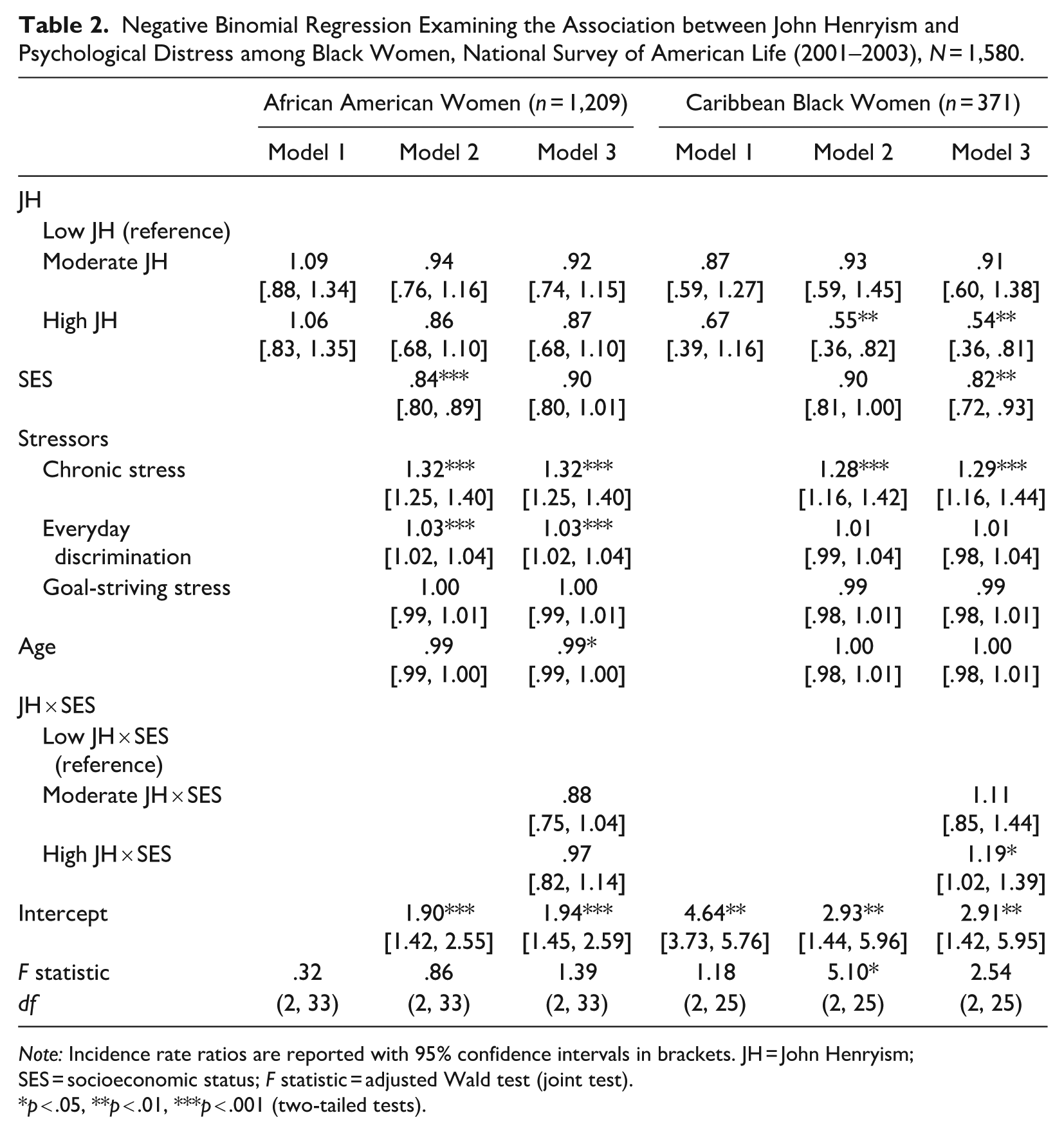
Note: Incidence rate ratios are reported with 95% confidence intervals in brackets. JH = John Henryism; SES = socioeconomic status; F statistic = adjusted Wald test (joint test).
p < .05, **p < .01, ***p < .001 (two-tailed tests).
Caribbean Black women
We did not find a direct association between John Henryism and psychological distress among Caribbean Black women. However, after accounting for sociodemographic characteristics and stressors (Table 2), we found that John Henryism overall shaped psychological distress, F(2, 25) = 5.10, p < .05. More specifically, compared to Caribbean Black women engaged in low John Henryism, those who engaged in high John Henryism reported a rate of psychological distress .55 times lower, all else equal (incidence rate ratio [IRR] = .55, 95% CI = [.36, .82]; p < .01).
The JHH and Psychological Distress
African American women
The interaction between John Henryism and SES was not statistically significant among African American women, indicating no evidence for the JHH among this group.
Caribbean Black women
The impact of John Henryism varied by SES among Caribbean Black women (IRR = 1.19, 95% CI = [1.42, 5.95]; p < .05; see Table 2, Figure 3). For low and moderate SES groups, higher levels of John Henryism were associated with decreased distress, with this effect being strongest in the low SES group. However, this protective effect of John Henryism diminished as SES increased, becoming nonsignificant among high-SES Caribbean Black women. Across all levels of John Henryism, lower SES was generally associated with higher distress, but this gap narrowed as John Henryism increased, leading to almost equal levels of distress across SES groups for those with high John Henryism. Interestingly, among high-SES Caribbean Black women, low John Henryism was associated with the lowest distress levels, contrasting with the pattern seen in lower SES groups. These findings suggest that although John Henryism may serve as a protective factor against distress, particularly for lower SES Caribbean Black women, its benefits may be less pronounced for those of higher SES, who may have other resources to buffer against psychological distress.
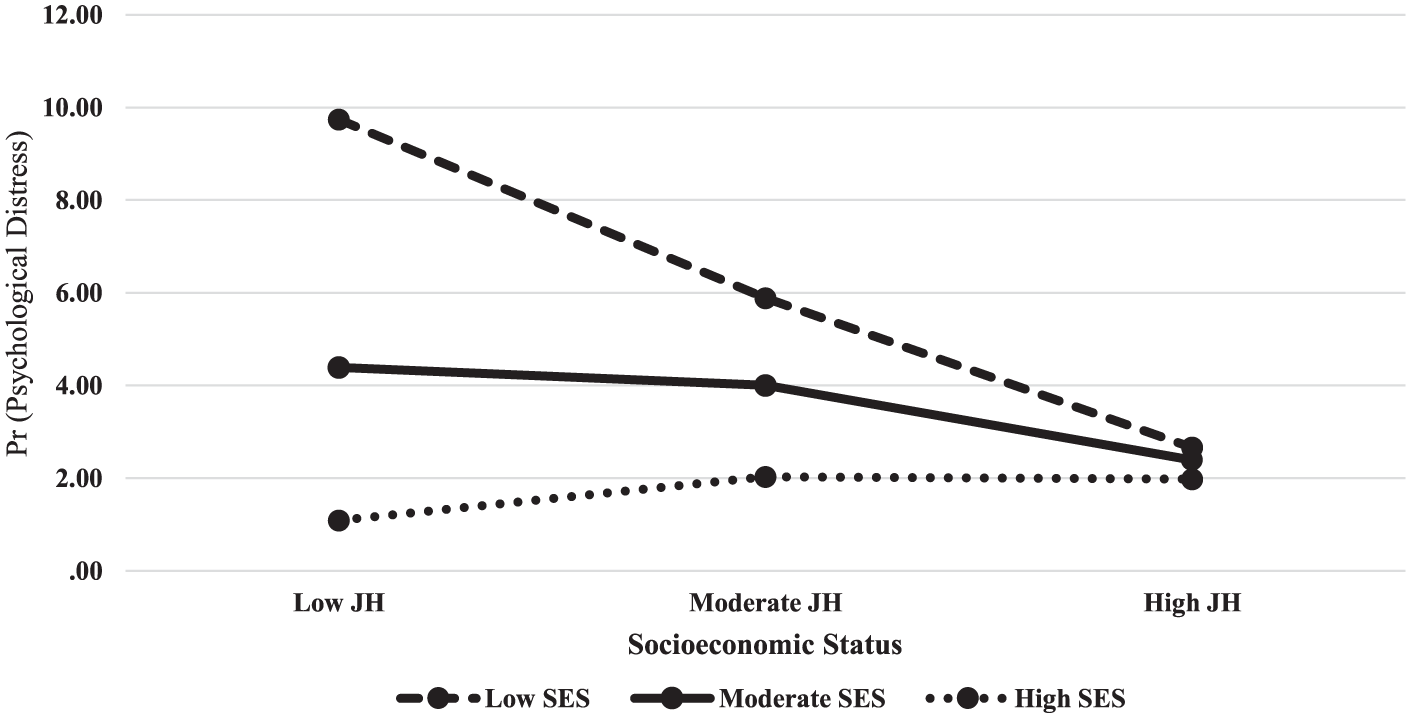
John Henryism Moderates the Association between SES and Psychological Distress among Caribbean Black Women (NSAL 2001–2003), n = 371.
Discussion
The pursuit of the American Dream remains a significant aspiration for Black Americans, with over half of the population still believing in its possibility (Borelli 2024) despite facing persistent systemic oppression and discrimination. This struggle for upward mobility, compounded by various social stressors, contributes to poor mental health outcomes, particularly among Black women (Hudson et al. 2023; Robinson et al. 2023; Sellers and Neighbors 2008; Williams 1998). Many Black Americans have historically engaged in “John Henryism,” a high-effort coping style emphasizing mental and physical stamina, hard work, and a determination to succeed (James et al. 1983). Recent studies suggest John Henryism’s significance for mental health among Black women, but it remains unclear whether these effects depend on SES (as per the JHH) or vary by ethnicity. The JHH posits that low-SES Black women may face greater mental health risks due to limited resources exacerbating John Henryism’s impact (James 2019; Robinson and Thomas Tobin 2021).
The present study aimed to clarify how John Henryism and SES interact to shape psychological distress among Black women, testing the JHH across ethnic groups. The goal was to provide a nuanced understanding of coping strategies and mental health among diverse subgroups of Black women pursuing upward mobility in the United States. Study findings reveal distinct patterns in the relationship between John Henryism, SES, and psychological distress for African American and Caribbean Black women. Although John Henryism did not significantly impact distress among African American women, it played a protective role for Caribbean Black women, particularly those of lower SES. These results highlight the importance of considering ethnic differences when examining coping strategies and mental health outcomes among Black women, suggesting that the effectiveness of John Henryism as a coping mechanism may vary based on cultural and socioeconomic factors. In the following, we consider the implications of these findings for strengthening our understanding of Black women’s mental health.
This study was motivated by a recognition that Black women have historically faced significant challenges, often “making a way out of no way” through strength, self-reliance, and innovation taught from a young age (hooks 1993; Robinson 2022b). This socialization, although seemingly admirable, comes at a cost to their mental health and well-being (Robinson 2022b). Black women experience high rates of psychological distress due to various social stressors, including chronic stress, gendered racism, and systemic oppression, regardless of SES (Collins 2000; Essed 1991; Robinson et al. 2023). However, research suggests that coping styles can potentially mitigate the adverse impact of stress on mental health (Pearlin et al. 1981; Thoits 2010; Turner 2013). Even though we did not find a direct association between John Henryism and psychological distress among African American or Caribbean Black women in the present study, we saw different trends after accounting for sociodemographic characteristics and stressors.
More specifically, among Caribbean Black women only, after these characteristics were considered, we found an association between John Henryism and psychological distress. Compared to Caribbean Black women engaged in low John Henryism, those who endorsed high John Henryism reported lower rates of psychological distress. This finding was somewhat unexpected given that prior work has demonstrated that John Henryism alone led to lower rates of psychological distress (Kiecolt et al. 2009). However, these findings were not disaggregated by race, ethnicity, or gender. Another possible explanation for this unexpected finding is that most of the African American women in the sample reported low levels of psychological distress, which means that they may not have needed to engage in John Henryism to offset feelings of distress. Additionally, much of the previous work that has examined the role of John Henryism in shaping distress has not disaggregated by gender. Therefore, although John Henryism appears to be beneficial for psychological distress among African Americans in sum, this may in fact differ for subgroups, such as women.
Our findings revealed distinct trends for Caribbean Black women regarding the John Henryism hypothesis (JHH). For low- and moderate-SES Caribbean Black women, higher levels of John Henryism were associated with decreased distress, with this effect being strongest among low-SES Caribbean Black women. However, this protective effect diminished as SES increased, becoming nonsignificant among high-SES Caribbean Black women. This is somewhat inconsistent with the JHH, which suggests that low-SES individuals who engage in high levels of John Henryism will experience poor health outcomes. In the present study, we found the opposite for psychological distress. Although Caribbean Black women with the combination of low John Henryism and low SES reported the highest levels of distress, those with low John Henryism and high SES reported the lowest levels. Therefore, the inverse association between SES and distress appears to be more pronounced for Caribbean Black women who scored low on John Henryism than for those who scored high. On the one hand, John Henryism is a form of high-effort coping that provides individuals with the mental fortitude to persevere as they are navigating external challenges and forces (Bennett et al. 2004; Robinson and Thomas Tobin 2021). Therefore, when an individual lacks sufficient financial resources and cannot access the mental capacity needed to push forward, feelings of distress may intensify. This distress stems from their perceived inability to resist circumstances and the profound sensation of being trapped in their situation.
Many second-generation Caribbean Black immigrants experience persistent “in-betweenness,” presenting significant societal challenges. Although they can achieve economic success and access opportunities their first-generation immigrant parents desired, these achievements are juxtaposed with evolving racial and economic systems designed to limit their success (Lorick-Wilmot 2014). For second-generation Caribbean Black women, this discrepancy is further complicated by pressure to adhere to gender-specific roles, particularly as wives, daughters, and mothers, which their first-generation immigrant parents and family typically use to define womanhood (Lorick-Wilmot 2014). This tension between opportunity and systemic barriers coupled with gendered expectations creates a complex landscape for navigating identity and success. When women from these backgrounds are not able to achieve the American Dream and promises of upward mobility, it can be even more debilitating. On the other hand, when individuals have achieved the American Dream and upward mobility, there is less of a need to engage in high levels of high-effort coping because there are likely fewer stressors to contend with, and they likely have access to other resources that can help offset ongoing challenges.
Transnationalism may also offer crucial insight into the experiences of Caribbean Black women and their engagement in John Henryism. Defined as the processes by which immigrants maintain connections between their origin and destination (Schiller, Basch, and Blanc-Szanton 1992), transnationalism often involves sending remittances to family in their country of origin (Henke 2001). Notably, women tend to remit more money and more frequently than men despite earning less (Azam et al. 2020; Rodgers et al. 2020). Even second-generation immigrants maintain these ties (Waters 1999), with significant remittances flowing from the United States to Jamaica ($1.8 million) and Haiti ($1.5 million) in 2017 (Pew Research Center 2019). This transnational context intersects with the historical legacy of colonialism and labor exploitation articulated by Claudia Jones’s concept of “super-exploitation” (Boyce Davies 2007). Jones (1949) highlighted how Black women’s labor was presumed guaranteed and how they were often confined to underpaid service work (Boyce Davies 2007). Colonial policies reinforced this exploitation by limiting employment options and perpetuating workplace patriarchy (Boyce Davies 2013). The 1960s immigration wave to the United States was driven by Caribbean women seeking upward mobility and independence (Boyce Davies 2013). These women faced the complex task of securing employment, settling families, and providing care (Lorick-Wilmot 2010). This historical and transnational context may explain the study’s findings. Although Caribbean Black women may achieve higher SES, their transnational obligations could lead to financial strain and psychological distress. High levels of John Henryism as a coping mechanism might exacerbate this distress, especially if external conditions remain unchanged (Robinson 2022a, 2022b).
Additionally, Caribbean Black individuals, particularly women, are often socialized to prioritize upward mobility as a means to improve social standing (Lorick-Wilmot 2014; Waters 1999). This socialization manifests in a strong goal orientation toward formal education and financial stability. Second-generation Caribbean Black women during this period were particularly focused on educational pursuits and career advancement, driven by the desire to provide for their children and families (Boyce Davies 2013). This worldview, shaped by historical experiences of colonialism, labor exploitation, and immigration, likely influenced how these women navigated systems for survival. Importantly, this perspective was likely transmitted intergenerationally, with Caribbean Black women socializing their second-generation children to preserve this approach to life and success. This intergenerational transmission of coping strategies and worldviews provides context for interpreting the study’s findings, specifically (1) the observed association between John Henryism and psychological distress among Caribbean Black women and (2) the role of SES in shaping this association. These results highlight the enduring impact of colonial legacies on mental health and coping mechanisms. The high-effort coping style characterized by John Henryism may be a direct result of this socialized emphasis on upward mobility and resilience in the face of systemic challenges. The interaction with SES further underscores the complicated interplay between historical experiences, current socioeconomic conditions, and mental health outcomes. Collectively, this understanding emphasizes the importance of considering historical, cultural, and socioeconomic factors when examining coping mechanisms and mental health outcomes among diverse groups of Black women in the United States (Robinson 2022a, 2022b).
Several limitations should be considered in interpretation of these findings. Causality cannot be established because the data for the present analyses were cross-sectional. Additionally, despite being the most broad-based examination of mental health and mental health disorders among people with African ancestry, the data set used to conduct analysis is more than 20 years old (NSAL 2001–2003). Thus, it is possible that the health trends and characteristics of participants in the data set may not align with those of the present day (Robinson 2022a, 2022b). In a related manner, given that the focus of this study examined factors that are very much tied to social, cultural, and political landscapes, these contexts may have shifted in notable ways since the collection of the NSAL, which may impact findings. Accordingly, prospective research examining the links between John Henryism and psychological distress, with emphasis on the JHH, would be greatly enhanced by using longitudinal and more contemporary data. Furthermore, the key outcome variable for this study was psychological distress, a precursor for more severe mental health outcomes (Robinson 2022a, 2022b). Thus, future work on the JHH and mental health among Black women may be strengthened by clarifying how the JHH extends to psychiatric disorders, such as major depression.
Although not without limitations, the present study has provided valuable insights for the study of John Henryism and mental health among Black women. To our knowledge, this study is among the first to explicitly examine the JHH for psychological distress, building on prior research (Perez et al. 2023) by incorporating a nationally representative sample and assessing distinct patterns across African American and Caribbean Black women. This work is especially novel in its consideration of the JHH among ethnic subgroups of Black women. Collectively, these results show that although the direct association between John Henryism was similar for African American and Caribbean Black women, the specific mechanisms for how John Henryism shaped distress among each group was distinct. Findings also reveal that for low- and moderate-SES Caribbean Black women, higher John Henryism levels were associated with decreased distress, with the strongest effect among low-SES women. This protective effect diminished as SES increased, becoming nonsignificant for high-SES Caribbean Black women. These results contrast with the JHH, which suggests that low-SES individuals engaging in high John Henryism will experience poor health outcomes (James et al. 1983).
Contrary to JHH predictions, Caribbean Black women with low John Henryism and low SES reported the highest distress levels, and those with low John Henryism and high SES reported the lowest. Taken together, this study contributes to literature by underscoring that the mechanisms for the JHH may differ for mental and physical health and across ethnic subgroups of populations. Thus, subsequent research would be enhanced by further assessing the JHH among other ethnic subgroups of Black women and understanding additional mechanisms that may be shaping these trends. These findings have important implications for both mental health practice and policy. Given that high-effort coping was particularly beneficial for Caribbean Black women with lower SES, interventions aimed at bolstering resilience should consider culturally relevant strategies that align with the coping frameworks most effective within specific communities. Additionally, mental health practitioners should recognize that a one-size-fits-all approach to coping may not be effective; instead, interventions should incorporate diverse stress-management strategies that reflect the lived experiences of African American and Caribbean Black women. On a policy level, efforts to improve socioeconomic resources—such as increasing access to economic mobility programs, expanding culturally competent mental health services, and addressing structural inequities—are essential to reducing distress and supporting the well-being of Black women across diverse backgrounds.
Overall, our study indicates that there are nuances for how John Henryism as a coping strategy works uniquely for different groups of Black women in shaping their mental health and well-being. Additional scholarship focused on this topic is needed so that we can further clarify the impact of John Henryism on mental health among Black women and use this evidence to inform culturally relevant interventions to reduce health inequities so that Black women are able to “reclaim their ability to live heart-whole” (hooks 1993:49) and thrive.
Footnotes
Acknowledgements
The National Survey of American Life was primarily funded by the National Institute of Mental Health, with a grant (U01-MH57716) to Dr. James S. Jackson. Additional support was provided by the Office of Behavioral and Social Science Research at the National Institutes of Health and the University of Michigan. The authors would like to express gratitude to Dr. Hiram Beltrán-Sánchez, Dr. Cheryl Woods Giscombé, Dr. Christy Erving, Dr. Chandra Ford, Dr. Vilma Ortiz, Dr. Anne R. Pebley, and Dr. Aliza R. Luft for their thoughtful feedback on earlier versions of this article. The authors would also like to express gratitude to Dr. Sherman A. James and Dr. Michael Anderson. The authors would like to dedicate this article in memory of Mrs. Jackie Stanley who passed away shortly after its acceptance. An earlier version of this article was presented at the 2024 Society for Social Work and Research Annual Conference.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M. N. Robinson received funding from the School of Social Work at University of North Carolina, Chapel Hill (UNC-Chapel Hill); the Carolina Postdoctoral Program for Faculty Diversity at UNC-Chapel Hill; National Institutes of Health (NIH)/National Institute on Minority Health and Health Disparities Grant R01MD015388; and the Eugene V. Cota Robles Fellowship at University of California, Los Angeles (UCLA). The authors would like to express gratitude to the Michigan Integrative Well-Being and Inequality (MIWI) Training Program (R25MH136652-06). The authors are also grateful to the California Center for Population Research (CCPR) at UCLA for general support. CCPR receives population research infrastructure funding (P2CHD041022) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. C. S. Thomas Tobin received support from UCLA, Resource Centers for Minority Aging Research Center for Health Improvement of Minority Elderly under NIH/National Institute on Aging Grant P30-AG021684 and from the UCLA Clinical and Translational Science Institute under NIH/National Center for Advancing Translational Sciences Grant No. UL1TR001881. This study was also supported by a grant from the National Institutes of Health, P30 AG015281, and the Michigan Center for Urban African American Aging Research. This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Institutional review board statement
All human and animal studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The National Survey of American Life data collection efforts were approved by the Institutional Review Board at University of Michigan (No. B03-00004038-R1).
Data availability statement
Restrictions apply to the availability of these data. Data were obtained from the Inter-university Consortium for Political and Social Research at the University of Michigan.