
Abstract
For decades, sociological research has examined the role of stigma in contributing to health disparities, yet such research seldom grapples with the interplay between individuals and structures. There is a particular paucity of research on abortion that concurrently examines individual experiences with stigma and structural barriers. In this article, we use telehealth abortion as a case, which now accounts for one in five abortions in the United States. We conducted 30 interviews and approach the data using a structural stigma framework in tandem with conceptualizations of felt, internalized, and enacted stigma. Findings advance a sociological theory of structural abortion stigma: a combination of structural barriers, internalized beliefs, and interpersonal shame. Telehealth reduces structural barriers to abortion and mitigates internal and interpersonal experiences of stigma. The latter is achieved by the ability to avoid the traditional abortion clinic, which many interviewees view as the site where stigma is produced and experienced.
For the regular [American Medical Association] AMA physicians, the limitation of abortion became one way of asserting their own professional domination over other medical practitioners. In their crusading, these physicians had translated the social goals of cultural and professional dominance into moral and medical language. They lobbied long and hard to convince legislators of the danger and immorality of abortion. (Conrad and Schneider 1980:12)
Abortion in the United States is a highly common medical experience, and yet it has been subject to a unique stigmatization process. This stigma has translated to decades of anti-abortion legislation, which came to a tipping point in 2022 after the Dobbs v. Jackson Women’s Health Organization Supreme Court decision overturned Roe v. Wade. Abortion has largely been overlooked by sociologists as a site of theoretical exploration despite representing a growing structural problem with major implications for social inequality and health disparities. Specifically, only seven articles on abortion have been published in top sociological journals since the year 2000 (Kimport and Kreitzer 2023). And yet, analyzing abortion care provides a critical case for exploring key questions within sociology regarding stigma as well as medicalization, cultural norms, gender and sexuality, social movements, and structural inequality.
In fact, in a now canon text in sociology, Conrad and Schneider (1980) utilize the case of abortion to develop a theory on medicalization and deviance—two central themes in sociology. As their work argues, abortion became moralized in the mid-nineteenth century United States to professionalize medicine and assert dominance over alternative healers and midwives. This history clashes with a common assumption in the cultural imaginary that “[a]bortion was always defined as deviant and illegal in America prior to the Supreme Court’s landmark decision in 1973” (Conrad and Schneider 1980:11) The assumption that abortion has always been (and thus will always be) defined as deviant has allowed for abortion care to be marginalized by two key social institutions: medicine and the law. Abortion care in the United States has long been siloed to a limited number of freestanding clinics that are frequented by protestors, which further denotes abortion as separate from “ordinary” gynecological and reproductive health care. Abortion is incredibly common; 25% of pregnancies end in abortion (Jones 2024). However, abortion training is largely left out of medical school curriculums: Half of medical schools offer no formal training on abortion or only a single lecture (Burns and Shaw 2020). The lack of training in tandem with the stigma and violence against abortion providers for doing “dirty work” have led to decreased numbers of providers over time (Joffe 2010). Legislation is also regularly passed to limit access to abortion via politically motivated abortion bans, the closing of physical clinics, and the exclusion of abortion from insurance plans and Medicare (Cohen and Joffe 2020). Taken together, individual beliefs about abortion being immoral or worthy of stigma become codified structurally such that abortion is continually medically inaccessible and under legislative attack.
However, most sociological work on abortion focuses on the individual level, including examinations of the ideological underpinnings of abortion stigma (Kumar, Hessini, and Mitchell 2009; Luker 1984) and analyses of abortion patients’ internalized feelings of shame (Becker 2019; Cockrill and Nack 2013), fear of being stigmatized (Hanschmidt et al. 2016), and secrecy behaviors (Cowan 2017). This work is largely separate from work on the structural barriers to abortion, which primarily come from the field of public health and focus on barriers to care (Biggs et al. 2020; Upadhyay, Cartwright, and Grossman 2022; Upadhyay, McCook et al. 2021). In this article, we advance a sociological theory on “structural abortion stigma,” which refers to the ways in which the stigmatization of abortion operates on the macro (state- and nation-wide legislation) level and in turn manifests in the meso (medical institutions, interpersonal interactions) and micro (individual) levels. In the process, this article provides a sociological framework for how cultural norms and stigma around abortion coalesce to create structural inequity to abortion access. As we argue, the social conditions, organizations, systems, and policy around abortion produce the individual-level phenomena that scholarship on abortion stigma tend to focus on. Moreover, by focusing on telehealth abortion as a case, we demonstrate how telehealth—a practice that is becoming an increasingly established norm in health care—can mitigate the effects of stigma across other cases.
Background
Barriers to Abortion Care
Barriers to abortion care are manifold because its provision is often constrained by ideological political decisions rather than driven by scientific evidence. Patients in need of abortion care must often travel for care—whether to the other side of the city or across state lines—because its provision is excluded from the formal health care system (Kimport and Rasidjan 2023). Therefore, access hinges on a patient’s socioeconomic status given limitations in many states on private insurance coverage for abortion and the Hyde Amendment, which bars abortion coverage for patients in many states on Medicare and Medicaid (Dennis, Blanchard, and Cordova 2011). Beyond paying for the abortion itself, other costs arise in the form of travel, time off work, the cost of childcare and dependent care, and the cost of lodging, particularly for those living in states with waiting periods, which require 24 to 72 hours in between an initial clinic visit and the abortion itself (Upadhyay, Cartwright, and Grossman 2022). Gestational limits are also a substantial barrier, particularly for those experiencing pregnancy complications at later gestations, and few clinicians provide abortions at later gestations (Foster, Dobkin, and Upadhyay 2013). Moreover, abortion medications are under intense legal scrutiny, including the recent Supreme Court case U.S. Food and Drug Administration v. Alliance for Hippocratic Medicine (2024), which experts had anticipated would severely limit access to mifepristone, the first of two medications typically used in a medication abortion. Lastly, after the Dobbs decision that overturned Roe v. Wade, abortion bans in various states have led to the criminalization of abortion for patients, providers, or both. This criminalization carries over to self-managed abortion. The criminalization of abortion, in part, distinguishes structural stigma of abortion from structural barriers. Using structural stigma as a lens elucidates the ways that these various barriers to care are a codification of stigma, which ultimately further perpetuate abortion stigma. Although sweeping legislation and increased public education are key for reducing barriers and stigma at the individual level, this article will indicate the ways that telehealth abortion mitigates and disrupts various manifestations of structural abortion stigma.
Telehealth Abortion as a Case
We develop a theoretical framework of structural abortion stigma by using telehealth abortion—in which the entire medication abortion process occurs remotely—as a case. Key cultural, technological, and legislative changes in the past three years have led to increased salience of telehealth abortion. First, the onset of the COVID-19 pandemic necessitated and normalized innovations in remote health care, allowing fully remote telehealth models to expand. Next, at the height of the pandemic, the U.S. Food and Drug Administration permanently lifted restrictions on in-person dispensing of mifepristone (Belluck 2021). These changes permitted the formation of virtual clinics—abortion clinics without an affiliated brick-and-mortar facility—whereas previously, only some brick-and-mortar clinics offered telehealth. Additionally, despite previous regulations, new data collected during this time showed that telehealth medication abortion provision is equally safe and effective as in-clinic medication abortion, including telehealth abortion without an ultrasound or other form of in-person test (Anger et al. 2021; Upadhyay, Koenig et al. 2024; Upadhyay, Koenig, and Meckstroth 2021; Upadhyay, Raymond et al. 2022).
Moreover, the reversal of Roe v. Wade in 2022 resulted in many states outright banning abortion, leading to the closing of clinics in those states and longer wait periods in protected-access states, leading to an increased demand for abortion care beyond brick-and-mortar clinics (Society of Family Planning 2023). With these various sociocultural and legislative changes in motion, growing proportions of patients are expected to rely on telehealth abortion in the coming years (Aiken and Upadhyay 2022). From April 2022 to December 2022, for instance, there was a 137% increase in the number of virtual clinic abortions (Society of Family Planning 2023). Presently, one in five abortions are provided via telehealth (Society of Family Planning 2024). Furthermore, in past work, we found that telehealth allowed patients before the Dobbs decision to avert a median of 10 miles and 25 minutes of round-trip driving and 1 hour 25 minutes of round-trip public transit time (Koenig et al. 2023). After Dobbs, entire regions of the country are now abortion deserts (Cartwright et al. 2018), and travel time to the nearest abortion facility is significantly greater, with Black, Indigenous, and other people of color experiencing the greatest increases in travel time to abortion facilities (Rader et al. 2022).
Sociological scholarship has failed to grapple with the increasing salience of telehealth. Medical and public health literature has long discussed the capacity for telehealth to produce better health outcomes for patients, gather better data, and reduce health expenditures (Edwards et al. 2014; Toole 2013; WHO Global Observatory for eHealth 2011). However, sociological work tends to critique the meaning of telehealth and other digital health technologies, focusing on how telehealth changes the provision of health care and extends the medical gaze and surveillance into patient homes (Lupton 2013, 2014; Lupton and Maslen 2017). We conceive of telehealth at a unique intersection of medicalization and demedicalization (Halfmann 2012; Torres 2014; Zola 1972) given that it involves interacting with a licensed medical provider while simultaneously circumventing the physical clinic. Abortion via telehealth challenges central assumptions about how abortion needs to be provided—in a clinic, after ultrasounds and other tests, often after a waiting period—and provides a hybrid experience of medicalized and demedicalized care: the privacy and comfort of demedicalized at-home care with the supervision and direction of medicalized care.
In this article, we fill a critical gap in sociology scholarship through our focus on the use of telehealth for a stigmatized health practice. We argue that telehealth is a way to mitigate stigma. We find that obtaining abortion care by telehealth aids patients in managing the various cultural, societal, and policy-based manifestations of abortion stigma by circumnavigating the need to enter a clinic—a space that can heighten feelings of stigma for some—and by reducing the barriers to care that we argue are the product of stigma. Telehealth largely eliminates disruptions to one’s schedule and associated cost and allows patients to feel more in control and experience a greater degree of privacy. As such, by examining the benefits of telehealth abortion, we advance a sociological framework for structural abortion stigma—the ways that structural barriers coalesce with abortion stigma to produce structural inequality and a structural stigmatization of abortion.
Stigma
The stigmatization of health behaviors is a complex social process that can lead to poor health outcomes and lower quality of health care provision (Hatzenbuehler, Phelan, and Link 2013; Link and Phelan 2001; Norris et al. 2011). Although stigma has been applied to various realms of medicine, including mental illness and sexually transmitted disease, abortion stigma continues to be undertheorized (Hanschmidt et al. 2016). This lacuna in the literature leaves questions regarding the effects of abortion stigma and how individuals navigate and manage abortion stigma. In particular, there is a paucity in examinations of the structural manifestations of abortion stigma, which Kumar et al. (2009) introduced. Instead, there is substantial focus on stigma on the individual level, with little theoretical connections made between barriers to access and the codification of stigma on a structural level and between the individual and institutions.
In a special issue on structural stigma, Hatzenbuehler and Link (2014:2) defined structural stigma as “societal-level conditions, cultural norms, and institutional policies that constrain the opportunities, resources, and well-being of the stigmatized.” In this article, we apply this theoretical framework to the realm of abortion—a highly stigmatized health care treatment—to advance social scientific literature on stigma. Abortion fits squarely within the study of structural stigma because cultural norms and policies not only constrain the well-being of and resources for abortion patients but also “[create] environments that have increased threat, punishment” (Richman and Lattanner 2014:95) for patients and providers alike. Although abortion is relatively simple to provide and demonstrably safe, the societal and cultural conditions have transformed access to abortion into what Cohen and Joffe (2020) refer to as “an obstacle course.”
Moreover, we apply Hatzenbuehler and Link’s (2014) conceptualization of structural stigma in tandem with Herek, Gillis, and Cogan’s (2009) three levels of stigma: enacted, felt, and internalized levels of stigma. Enacted stigma refers to “overt behavioral expressions” (Herek et al. 2015:21), which in the case of abortion stigma can include the targeted violence and harassment ubiquitous across physical abortion clinics. Felt stigma refers to an individual’s “expectations about the probability” (Herek et al. 2015:20) of being the target of the overt expressions of enacted stigma. This level of stigma has a particular bearing on people’s behaviors because it causes individuals to engage in coping strategies to avoid or reduce the risk of discrimination. In the case of abortion, this can manifest as keeping an abortion secret or seeking to avoid a physical clinic through self-managed abortion or telehealth. The final level of stigma in Herek et al.’s (2009) framework is internalized stigma, which occurs when an individual accepts the beliefs underpinning stigma as part of their own value system. In the case of abortion, internalized stigma could manifest as shame or guilt.
Although the prevailing trend in abortion stigma literature fails to account for the way that structures and individuals interact, there are notable exceptions. In the first, Kimport and Rasidjan (2023) describe the emotional burden on individuals when forced to travel for an abortion to surpass local restrictions. In the context of Ireland, Broussard (2020) expounds on the way that structural abortion stigma manifests in peoples’ embodied experiences with abortion, with the barriers to care manifesting as internalized stigma. Moreover, Coleman-Minahan et al. (2021) argued that “multilevel” abortion stigma is reinforced by the judicial bypass process, required in Texas of young people seeking abortion without parental consent. Abortion stigma also inhibits the quality of care received by patients, as found in a scoping review conducted by Sorhaindo and Lavelanet (2022), and can lead people to unsafe abortion methods to maintain keeping the procedure a secrecy (Cárdenas et al. 2018). Lastly, various researchers have examined how abortion stigma can lead to subpar and judgmental care from providers in various non-U.S. contexts, including Peru, Nepal, Senegal, and South Africa (Favier et al. 2018; Palomino et al. 2011; Puri et al. 2012; Suh 2018). In this present article, we build on this nascent work by using telehealth abortion as a case to advance a theory on structural abortion stigma while elucidating the way telehealth mitigates structural stigma for individual patients.
Data and Methods
We conducted 30 in-depth interviews with individuals who had a telehealth medication abortion between May 31, 2021, and January 17, 2022. Participants were purposively sampled from the California Home Abortion by Telehealth Study, a longitudinal evaluation of the safety, effectiveness, and acceptability of telehealth abortion care provided by three U.S. virtual clinics: Abortion on Demand, Choix, and Hey Jane (Koenig et al. 2023, 2024; Upadhyay, Koenig et al. 2024). These services offer fully remote, synchronous and/or asynchronous medication abortion care. Although the eligibility criteria differed slightly among the three providers, patients were generally eligible for medication abortion care if they lived in an approved state and their pregnancy duration was less than 70 days (assessed by date of last menstrual period or by ultrasound). 1 The services ranged in price from $199 to $289. Once their eligibility was approved by a licensed medical provider, patients received abortion medications via a mail-order pharmacy. Patients also received follow-up messages via secure text message or phone after receiving the medications. At the time of this study, Abortion on Demand, Choix, and Hey Jane served a combined 20 states and Washington, D.C., across the continental United States, primarily in the West and Northeast but with 2 states in the Midwest and 5 in the South.
Sample
We recruited 30 individuals (Table 1) who had a telehealth medication abortion with one of the three participating virtual clinics to participate in semistructured interviews. In a previous stage of the study, we conducted three longitudinal surveys with 1,600 individuals: a baseline survey at abortion intake, a second survey approximately one week after intake, and a final survey four weeks after intake. Individuals were eligible to participate in an interview if they had completed the series of longitudinal surveys and agreed to be contacted again in the future regarding an interview, resulting in a subsample of 1,260 individuals. We then used a purposive sampling method to account for a diverse interview sample in terms of race and ethnicity and age and to include those who required additional medical care after taking the abortion medications.
Sample Characteristics (N = 30).
Interview participants ranged in age from 16 to 39, with an average age of 27, and 5 participants were adolescents (19 years or younger). In terms of race and ethnicity, 9 identified as non-Latinx White, 6 as Asian, 5 as non-Latinx Black, 5 as Latinx, and 5 as multiracial. Three participants reported requiring additional medical care after taking abortion medications. Participants were recruited from 11 states (CA, CO, GA, IL, MA, MN, NY, NJ, PA, RI, VA), representing all four regions in the country—West, Northeast, Midwest, and South. In terms of abortion history, 18 participants reported 0 prior abortions on the intake survey, and 12 reported 1 or more prior abortions.
Procedures
Interviews were conducted remotely via Zoom by the first, second, and third authors between July and September 2022. The in-depth interviews followed a semistructured interview guide of 20 questions. The questions addressed the factors that contributed to participants’ decisions to choose telehealth medication abortion and their overall experience of telehealth abortion. Sample questions included: “How did you first hear about telehealth abortion?” “What appealed to you about this service?” “Did you consider or call a brick-and-mortar clinic first?” “Can you tell me about your experience taking the abortion medications?” and “What kinds of things did you like and not like about the telehealth service?” The interviews lasted between 40 and 90 minutes. Patients provided informed consent for participation in the interview and audio recording. Interviews were audio recorded via Zoom and transcribed verbatim. Participants were compensated with a $50 electronic debit card for their participation. All procedures were reviewed and approved by the University of California, San Francisco’s institutional review board.
Analysis
The data were coded by the first and second authors using a flexible coding approach on Dedoose. Flexible coding is a rigorous method of qualitative data analysis that uses both deductive and inductive approaches to coding and theory development (Deterding and Waters 2018). During the first stage of data analysis, the authors began by developing a codebook that categorized broad topics that were addressed in the interviews (e.g., “reason for abortion,” “reason for telehealth,” “feelings about abortion”). To allow for flexibility, the authors also identified emergent codes from the text and refined existing codes based on ongoing analysis. Once the overarching theme of “structural abortion stigma” was selected, the first and second authors conducted axial coding to identify key subthemes (e.g., “financial barriers,” “fear of the clinic,” “internalized stigma”). Divergences in coding were discussed by the research team to ensure congruence across coding during the entire process of data analysis.
Results
To utilize telehealth abortion as a case for advancing a theory on structural abortion stigma, we present the findings in the following two sections. First, we review the ways that telehealth mitigates structural barriers to abortion care—how telehealth removes travel to potentially distant physical clinics and, in the process, reduces logistical and financial hurdles. These findings build on a growing body of work on the benefits of telehealth and a long-standing literature on structural barriers to abortion care. Next, we present novel findings on how telehealth manages various manifestations of stigma—internalized, felt, and enacted—by circumnavigating the physical clinic and the visibility of being an abortion patient. Taken together, these findings contribute to a theoretical framework for structural abortion stigma.
How Telehealth Mitigates Structural Barriers
For many participants, telehealth medication abortion services increased access to needed health care. Structural barriers to accessing abortion care were mitigated by being able to obtain medication abortion through telehealth, from reduced waiting times and more affordable prices to the eliminated need to travel. Telehealth felt “convenient” and “easy” for participants, often resulting in positive abortion experiences.
Participants emphasized how telehealth reduced barriers to accessing abortion by offering fast and convenient care. Unlike brick-and-mortar clinics, participants felt that telehealth services more quickly accommodated their appointments and shipped medications. For example, Rachel, an 18-year-old White woman living in Illinois, explained the barriers she faced while looking for care at physical clinics: So when I had called Planned Parenthood, I had to have a first appointment, which would’ve been in a month, I think, and then a second appointment after that. And . . . I didn’t want to wait that long. And also it was very expensive to go there. So that was mostly why I didn’t go with that one. And then I called around to other clinics too, like OBs, and they either said that they didn’t deal with that kind of stuff or that they didn’t take my insurance.
Long wait times for appointments at physical clinics were a major barrier to accessing care for participants. Telehealth mitigated this barrier by offering the ability to quickly schedule appointments. Elaine, a 27-year-old multiracial law student in New Jersey, felt that telehealth removed multiple barriers to care, particularly those related to wait times and travel. She explained: Well, I really do think it kind of just boiled down to the difficulty of, not that I couldn’t get somewhere, but finding somewhere that had an appointment available and having an appointment to pick because most of them didn’t have appointments anytime soon. It was weeks away, month away, month and a half, whatever. And then trying to figure out what classes do I have that day? Do I have something else going on? Do I have something I have to do the next day? Well, if I need the car, does my boyfriend have work that day? Things like that. Telehealth was like, I could just take care of it. I didn’t even have to go anywhere . . . it was so much easier.
Many participants also appreciated how telehealth mitigated other logistical barriers to accessing abortion care, such as taking time off work or finding childcare. Sara, a 34-year-old White woman living in Massachusetts, succinctly explained: “Honestly, I liked the fact that I didn’t have to take any time off work. I didn’t have to go anywhere. Didn’t have to worry about all that.” Similarly, Tess, a 39-year-old White woman who lives in Rhode Island with her husband and son, shared how the telehealth model provided a much more convenient way to complete her abortion at home: Having to take an extra day off would have added such a massive hindrance to the whole procedure. Being able to do this on my time, on my schedule, from my home, so I didn’t have to get childcare coverage or take time off from work. So the convenience of it was huge. . . . It was easy. There were no hoops to jump through. It was: Google search, set up an appointment, pay for it, get the stuff done. Not: find the clinic, go make the appointment, have somebody take you to the appointment, find childcare to cover while you’re going to the appointment. So the convenience, the ease of telehealth was good.
Telehealth also removed another critical structural barrier: traveling to a physical clinic. For many participants, the ease of accessing abortion care through telehealth was not simply a convenience; rather, it was a necessity. This was the case even in patients living in legal, protected states. Whether participants lacked reliable transportation or lived in abortion deserts, the telehealth model aided participants in accessing needed care from home. Had Alyssa, a 24-year-old Black woman, not lived in New York—where abortion care is generally more accessible—completing her abortion would have been “impossible.” She explained: It’s something that I could just do right on my phone. So I feel like for a lot of people, especially someone like myself, I didn’t have a car, which I was in New York at the time. But if I was in another state, that probably would’ve made things a lot harder for me or made it impossible for me to go to a clinic. So I feel like that’s a good option for people who maybe don’t have reliable transportation, are able to get to an actual clinic.
Similarly, Michelle, a 36-year-old Black woman living in New Jersey, shared her experience: The area where I live, there are literally no abortion providers whatsoever. And I did not have the actual time to travel to the area where they do have actual abortion providers in person . . . and at the time, I was working. Some weeks, it was seven days a week. And myself, I didn’t physically have the time to get [to the nearest abortion clinic]. But I was, “If I have to take sick time, I’ll do it. And I’m going to have to go far.”
Although Michelle may have been willing and able to travel to a clinic to receive care, the telehealth model removed the burden of travel and made abortion care more accessible.
This accessibility was crucial given that many other participants were simply unable to travel. In particular, participants living in rural areas faced numerous structural barriers to accessing abortion care. Katie, an 18-year-old White woman in rural Minnesota explained: “The closest [abortion clinic] was in [the nearby city], and that’s probably a two-and-a-half-hour drive. I didn’t want to go alone, so it would’ve just been harder to have to figure out me and my mom’s schedule to be able to both go together.” Similarly, Adriana, a 15-year-old Latina living in central California, described the difficulties she faced when trying to access abortion care: “The nearest clinic that was open was two hours away. There used to be [a clinic in my town], but there hasn’t been one in a while.” Further complicating her experience, Adriana also mentioned that she had not told her parents about the pregnancy or abortion. Thus, being too young to drive herself coupled by a lack of transportation or family support, “to find an excuse and a way to go that far [to a clinic] was just too hard.”
Another recurring theme across all interviews was the affordability of telehealth medication abortion. Cost is one of the greatest barriers to abortion care and a key reason why many participants sought out telehealth as opposed to medication abortions at physical clinics. Participants felt surprised by the affordability of telehealth services. Rebeca, a 19-year-old Latina in New York, explained: “I felt like it was affordable because I’ve heard that abortions could be up to $800 . . . but I was like, ‘$250? That’s not bad. I’ll do that. I’ll pay for it.’ To me it felt like a good price. It’s realistic.” Similarly, Angelica, a 38-year-old White woman in California, described her shock at learning the cost of an abortion at her local in-person clinic, leading her to explore telehealth options: Compared to having to go to a clinic and meet someone in person, [telehealth] was a lot cheaper. Because . . . I think it was about $800 or maybe even a little more [at the local clinic]. So that kind of shocked me. I didn’t think it would be so much. I didn’t know. So I can’t remember exactly how much it was with [the telehealth service]—maybe a couple of hundred or something—so, by comparison, it was a lot cheaper. And I didn’t mind paying it because you’re paying for the convenience of it and just being able to be at home.
For Annie, a 28-year-old Asian woman in California, the affordability of telehealth was particularly important because she did not have health insurance at the time of her abortion. She explained: I felt like, compared to [other options] in the area, it was very affordable . . . [and] the closest [abortion] clinic was an hour away from me. And even then, the earliest appointment that I could get was probably two weeks. There was no guarantee that when I got there I wouldn’t have to wait longer as well . . . I feel like time-wise, it was very effective for me. And also, cost-wise, it was as well. It was very expensive at [another health clinic]. I don’t remember the exact price, but having to pay for the consultation and then having to pay for the medication, as well. And at the time, I didn’t have health insurance to be doing something like that.
The affordability of telehealth abortion was critical given that many participants cited financial hardship as a key reason they wanted the abortion. For example, Sara, the 34-year-old White woman living in Massachusetts, succinctly noted: “One of the main reasons we aren’t having another child right now is because we’re broke. So I mean, [telehealth] was a few hundred bucks compared to [a more expensive in-clinic procedure].”
To understand the ways in which telehealth mitigated financial burdens, consider Maya, a 20-year-old multiracial woman in California. When Maya found out she was pregnant, she was already working two jobs to make ends meet. Due to these financial hardships and lack of family support, Maya knew that having a child “would be a huge struggle.” Although she knew abortion was the right decision, she noted the cost of abortion care as a significant barrier. She explained: When I first found out that I was pregnant, I wasn’t in the right financial means to have the child. And I knew even if I did choose to have it, it would be a really hard struggle for me. And so, then when I decided to go through with [the abortion], I was considering going to [an abortion clinic], but then when I went over there for the prices and stuff, I was just kind of iffy about it.
After working “long hours just trying to be able to get the money,” Maya was able to pull together enough funds to pay for the telehealth medication abortion. Without telehealth, Maya would have likely encountered even more delays in care in order to afford a more expensive in-clinic procedure. These participants’ experiences demonstrate how telehealth mitigates structural barriers by reducing logistical and financial burdens, affording them the ability to have the abortions they wanted and needed.
Avoiding the Clinic, Managing Stigma
In addition to structural barriers, many participants discussed the benefit of telehealth as a way of avoiding interpersonal and individual experiences of stigma by avoiding physical abortion clinics, which many participants view as the primary site where abortion stigma is experienced. In these accounts, entering the physical clinic represents facing abortion stigma across various levels—from having to drive to a different city or state or to a remote part of town to encountering anti-abortion protesters outside to physically being in a room as an abortion patient and requesting abortion pills face-to-face. Having a telehealth option circumnavigated these various facets of abortion care. As such, in addition to telehealth as a means of navigating costs, travel, and logistics, avoiding the physical clinic also allows one to manage internalized, felt, and enacted abortion stigma—together comprising structural abortion stigma. This adds insight into the ways that individuals’ feelings of shame about a stigmatized health procedure can be mitigated by removing a primary place where abortion stigma is experienced.
As an example of how telehealth allows for the managing of abortion stigma across these various levels, consider Tess, the 39-year-old White woman who lives in Rhode Island with her husband and son mentioned previously. She was able to schedule and have her abortion while balancing her two-hour daily commute to work and being the primary caregiver to her son. In addition, access to telehealth aided in managing or avoiding internalized, enacted, and felt stigma. For instance, despite identifying as “pro-choice,” she holds shame in choosing an abortion for herself. When probed about what she meant about her abortion evoking “hard feelings,” she said the following through tears: I had to confront a lot of internal biases that I didn’t really even know that I had, where I didn’t deserve an abortion because financially, I could afford another child. I had to confront this internal bias that I had that abortions are for people on hard times . . . and that, as an intelligent person, I feel like I should have known better. I should have made smarter choices, and these are consequences that come up from them. So, that’s hard . . . because this was a life.
While Tess was sifting through these complicated emotions—or internalized abortion stigma—she felt certain that an abortion was the correct choice for her and her family. The telehealth model aided in Tess managing these feelings and reducing additional layers of abortion stigma. She mentioned being comforted by the ability to avoid the physical clinic and potential protestors in making “an uncomfortable situation somewhat less uncomfortable.”
I didn’t want to face the idea of there being protestors . . . you see all the footage of people standing outside and harassing people, and I’m already dealing with a super hard decision. I don’t need people screaming in my face. I was nervous about that. So when I Googled and I found out that you can just do this via web interview, over the phone, I was like, I’m here for it.
Indeed, many participants mentioned anticipating stigma by having to confront protestors and anti-abortion signage outside of the clinic, with the severity of anti-abortion vitriol impossible to predict. Lindsey, a 30-year-old Asian American woman living in Colorado who had a previous in-clinic abortion in Louisiana—where abortion has long been highly restricted—said the following about the benefits of telehealth abortion: Just imagine living in a red state, and people are screaming and yelling at you and showing you these photoshopped pictures of babies being vacuumed out of women’s wombs. That could be terrifying. And not having to experience that and being able to do an abortion in the comfort of your own home and your own space and being private about it and having, I guess, the choice to be private, I think that’s great.
As Lindsey indicates in this excerpt, telehealth allows for a greater degree of privacy and comfort by being able to have the abortion process from one’s home—specifically, “the choice to be private.” In addition, Lindsey’s quote indicates that telehealth mitigates both felt and enacted stigma by avoiding the feeling of anticipating being stigmatized when accessing a physical clinic and avoiding the enacted stigma in the form of protestors.
In addition to the presence of protestors, many participants mentioned that simply entering the physical clinic sparked negative emotions from the physicality of the space itself. For instance, consider Emily, a 24-year-old Asian American woman living in California. Earlier on in our interview, she mentioned that the ability to have the process remotely, and particularly the option to use the secure messaging feature, caused “less guilt” about the abortion. When asked to elaborate, she said the following about avoiding the physical clinic: If you go to a clinic then there’s people that are outside of it with signs saying that it’s bad and I don’t have to deal with that or be confronted with it. It helped me in the process of not having to go to a clinic . . . and just having to be in the clinic is kind of just very depressing just in itself . . . I don’t know. It just feels weird because there’s putting names to faces and they know why I’m there rather than just doing it online. And you have someone that’s there for you if you need help, but you’re not sitting there looking at someone. So there’s kind of less guilt into it.
As this quote indicates, for Emily and others in the study, being physically in the clinic, embodying “the abortion patient,” conjures negative feelings due to multiple factors in addition to having to confront protestors. In such cases, receiving abortion care mediated through a phone or computer screen lessens internalized stigma or other negative feelings associated with an abortion because being seen in person by providers, other patients, and any potential onlookers seems to increase feelings of stigma.
In addition, as participants explained, having a telehealth option allows a greater degree of secrecy regarding the abortion, allowing patients increased control about who to disclose the abortion to. This, in turn, mitigates feelings of stigma. Rebeca, the 19-year-old Latina living in New York, for instance, said she appreciated telehealth because “I wouldn’t want people to know that I’m having an abortion at the time. It’s still something I’m not really proud of, so I would want it to be as secretive as possible.” In this case, secrecy helps manage internalized stigma. The desire for privacy and secrecy is particularly the case for those living in small towns or rural areas. Take, for instance, Katie, the 18-year-old living in Minnesota. In addition to managing having an abortion while being a teenager living with her parents, Katie was also managing the fear of being seen and recognized at a location that provides abortions. As she said: When I go to the clinic, I know a lot of the nurses, the office people, so I just didn’t want them to know what I was doing. And then, potentially, I know they can’t say anything, but I mean you never really know, and I didn’t want to be viewed different, I guess. So, that’s why I wanted to keep it more confidential and not have to worry about someone seeing or hearing or saying something about it.
Indeed, anonymity and being in one’s home were repeatedly mentioned as the benefits of telehealth. As Lindsey recounted: Just being able to do it in the safety of your own home and being absolutely 100% anonymous. They don’t know what you look like. I mean, they know your name and they know your information, but they’re not going to see you out on the street and be like, “Hey, she got an abortion.” You know?
Advances in telehealth therefore disrupt stigma processes by removing the embodied element of receiving stigmatized health care, which could have implications beyond abortion, including other types of sexual and reproductive health or even mental health.
Additionally, although sociological literature on structural barriers and on stigma tend to be separate, many participants alluded to the structural barriers themselves being a source of stigma. This contributes to a sociological theory of structural abortion stigma by demonstrating a cycle in which abortion stigma leads to structural barriers, which then implicitly lead to abortion stigma. In the following excerpt, Michelle describes the connection between the reduction in structural barriers and the reduction in stigma, both of which telehealth provides.
I don’t think that it would be such a devastating process if Abortion on Demand or services like it were easily available and accessible to women. Because it destigmatized it a lot for me. Destigmatized it to the point where I’ve actually recommended it . . . ever since then, I’m, “You should go to this Abortion on Demand site . . . ” Because it was such an easy process. It made it, like I said, like you can go get this done without it being an epic poem of emotion and having to figure out, am I going to be able to walk through the doors of some place? And it was so easy. I don’t even know how many other people know about it. And that’s why I want people to know. It’s a safe place to get something done that could very well be very unsafe if you don’t know that you have this option.
As Michelle describes, it is often the structural barriers of abortion that cause receiving this health care to be “a devastating process” or even “an epic poem of emotion.” The process itself of having to find a physical clinic, plan a trip, and anticipate and/or encounter protestors fuels feelings of shame and sadness given the marginalization of the procedure. In fact, in the following excerpt, Michelle describes feeling surprised by her lack of negative emotions despite initially feeling very guilty about not continuing the pregnancy.
I worried often, for the time during and afterwards, that I wasn’t more emotionally connected to the process. Why am I not crying? Why am I not sad? Why am I not feeling like a bad person? And the answer is, because I didn’t have to feel like a bad person. I didn’t have to seek thousands of miles or millions of dollars’ worth of care in order to get this thing done. And when I got it done, I felt physically safe. I felt physically taken care of. . . . But the fact that I don’t have to deal with the mental consequences thereafter, that is probably where I place most of the value here. Because a lot of women that I have talked to are, “I feel so guilty that I’ve done this years later.” And I sometimes have forgotten that I’ve done it. And I don’t mean to sound callous, but this was not a pregnancy that I was ever going to be able to carry to term healthfully.
As this findings section demonstrated, there is a need for a theory of abortion stigma that combines structural barriers with internal and interpersonal experiences of stigma. The barriers themselves are a result, or codification of, individual-level abortion stigma, and the barriers then lead to feelings of abortion stigma for individuals receiving this care (in addition to providers, although the present study does not speak to this element of abortion stigma).
Discussion
Our findings demonstrate the importance of understanding experiences with a telehealth model for abortion care. More broadly, this article makes important contributions to social scientific literature on stigma and health inequality. We found that a telehealth model aided patients not only in accessing abortion via reduced costs, time, and logistical hurdles but also in the managing of internalized, enacted, and felt stigma. Using telehealth abortion as a case, we connect barriers to care with the individual and interpersonal experiences of stigma to advance the theoretical concept of structural abortion stigma—a combination of structural barriers, internalized beliefs, and interpersonal shame (see Figure 1). The findings may help direct future policy on expanding access to telehealth abortion, especially in the wake of the reversal of Roe v. Wade, which has and will continue to exacerbate long-standing inequities in abortion access.
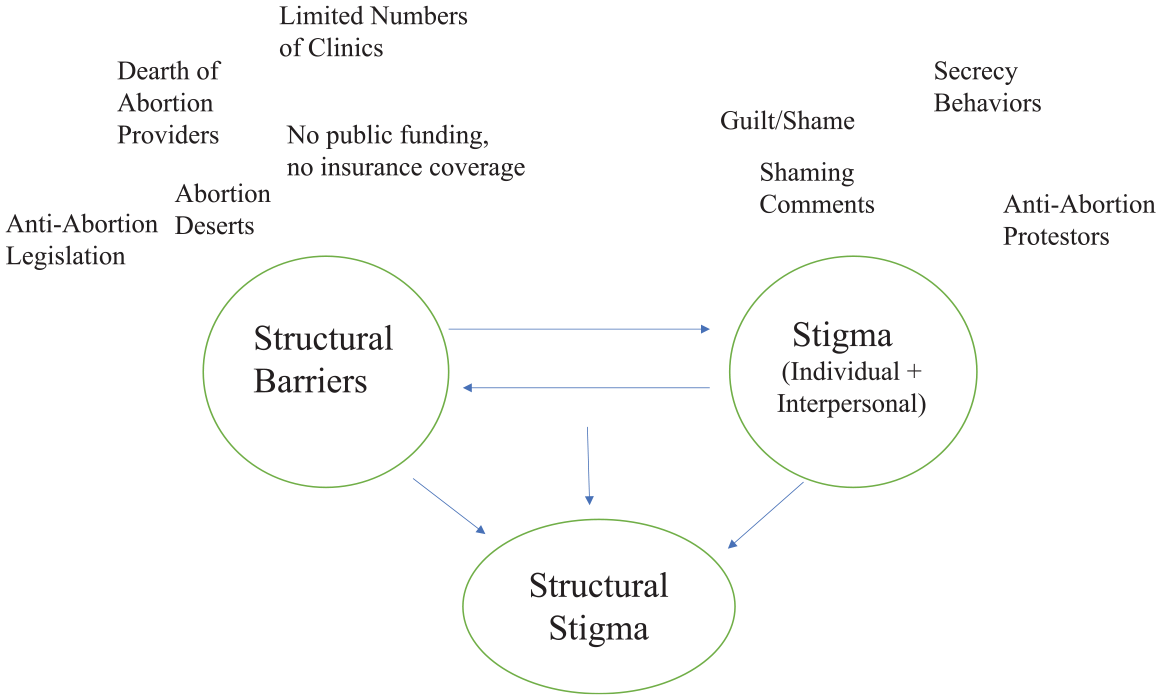
Structural Abortion Theoretical Model.
Interview data point to a telehealth abortion model as a way of reducing structural abortion stigma that we define by modifying Hatzenbuehler’s (2014) structural stigma framework. Structural abortion stigma is the product of cultural norms, societal-level conditions, and policies around abortion that constrain the opportunities, resources, and well-being of abortion patients. Due to geographic variation in abortion acceptance across the country, abortion stigma has been structurally codified via abortion deserts and states without abortion access—also referred to as spatial stigma (Kelaher et al. 2010). Abortion stigma has also been codified via policies that silo abortion care to freestanding abortion clinics where the presence of protestors has been normalized and via policies—including the Hyde Amendment—that render abortion financially unfeasible for many.
These various structural manifestations of stigma, in turn, exacerbate individual-level stigma. Being forced to surpass these various obstacles created by the structural marginalization of abortion care—particularly the need to travel—increases feelings of shame and exclusion and of being deviant or “abnormal” (Kimport and Rasidjan 2023). By continuing to explore the interplay between structures and the individual in the study of stigma, our findings build on a growing, relatively nascent body of work in sociology that can be applied to various stigmatized elements of health and health care—including mental health, sexually transmitted illness, and gender-affirming care for trans populations.
Our study indicates that telehealth abortion aids patients in managing the various cultural, societal, and policy-based manifestations of abortion stigma by circumnavigating the need to enter a physical clinic—where patients may encounter stigmatizing actors inside and outside of the clinic—and by reducing the barriers to care that we argue are the product of stigma. Most of the sample pointed to the ease and convenience of telehealth in seamlessly fitting the abortion in their schedule. This includes accommodating job schedules and child and elderly care, eliminating the need to travel, reducing the cost of the abortion itself, and reducing associated costs, such as lost wages, childcare, travel, and accommodations. This supports prior research on telehealth abortion as both a patient-centered model and a potent tool for reducing barriers to care, including by drastically reducing cost barriers (Endler et al. 2019; Kerestes et al. 2021; Raymond et al. 2019; Upadhyay, Koenig et al. 2024; Upadhyay, Schroeder et al. 2024).
As telehealth becomes increasingly part of U.S. health care models post-COVID-19, it is critical for sociologists to continue to theorize how this model disrupts long-standing social inequities. Moreover, it is long overdue for the field of sociology to seriously grapple with abortion as a site of theoretical exploration, interconnected as it is within the fields of health, gender, stigma, the family, and technology studies and perennially unresolved tensions between structures and agency. This study therefore constitutes a key step in addressing the exclusion of abortion from mainstream sociological theorization while contributing key findings that could aid in paving the way for patient-centered health models both within abortion care and beyond.
Footnotes
Acknowledgements
The authors appreciate contributions to data collection and management and other input on the California Home Abortion by Telehealth Study from Maricela Cervantes, Linda Shin, Kelly Song, and Lisa Peters. We thank Cindy Adam, Mark Adam, Kate Baron, Stephanie Bussmann, Leah Coplon, Lauren Dubey, Lindsay DuBois, Kiki Freedman, Gaby Izarra, Jamie Phifer, and Aisha Wagner for supporting data acquisition. We appreciate overall guidance from Elizabeth Raymond on classifying adverse events.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the BaSe Family Fund, Erik E. and Edith H. Bergstrom Foundation, Isabel Allende Foundation, Jess Jacobs, Kahle/Austin Foundation, Lisa and Douglas Goldman Fund, Preston-Werner Ventures, and a Resource Allocation Program (RAP) Award from the UCSF National Center of Excellence in Women’s Health. Ms. Koenig was funded in part by a training grant from the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award No. T32MD015070 for the duration of the study. The funders had no role in the study design, data collection, and analysis; the writing of the report; or the decision to submit the paper for publication.