
Abstract
This research adopts an analytical spatial perspective to explain ethno-national health inequality between Palestinians and Jews in Israel. The work identifies the forces that instigated and maintained the spatial segregation of Palestinians and elaborates the role of segregation in generating health gaps between Palestinians and Jews. The analysis suggests a novel conceptualization of two types of segregation: (a) exclusion from the center and confinement to the periphery and (b) segregation within the geographic periphery. Using administrative data on COVID-19 incidence, hospitalization, and death and various health indicators for localities, I devise a decomposition method that evaluates the relative contribution of each type of segregation to the total health gap. The findings indicate that the segregation of Palestinians from the center and their confinement to peripheral regions are crucial determinants of their poor health outcomes and that the segregation of the Palestinian community within the geographic periphery also contributes to poorer health.
Keywords
The spread and progression of coronavirus in Israel revealed an unexpected pattern of health inequality. For approximately the first six months of the pandemic, the incidence, morbidity, and mortality rates of COVID-19 were significantly lower among the Palestinian community, an ethno-national minority in Israel, than among the dominant Jewish population (Birenbaum-Carmeli and Chassida 2020). Given that communities and social groups with lower socioeconomic status (SES) have been disproportionately affected by COVID-19 in Israel and elsewhere, the Palestinian community’s unexplained initial resistance to the virus is puzzling because by all accounts, Palestinians have lower SES, less political power, and worse health outcomes than Jews. I argue that the extreme spatial segregation of the Palestinian community drove this unanticipated pattern of health inequality. The severe spatial, residential, and social segregation of Palestinians in Israel from the Jewish majority delayed the spread of the virus into their communities, which induced a false sense of immunity to COVID-19 among the Palestinian community.
This observed advantage of the Palestinian community was only temporary—eventually, Palestinians experienced higher rates of COVID-19 than Jews, an expected outcome given their poorer health outcomes and lower SES. I argue that both patterns—the observed health advantage of the Palestinian community in the early stages of the pandemic and the community’s later health disadvantage—resulted from the same condition: extreme spatial segregation.
The Palestinian community’s experience with the coronavirus outbreak highlights the significance of spatial segregation for explanations of ethno-national and racial health inequalities. To test whether these effects were specific to the COVID-19 outbreak, the analysis also explores the impact of segregation on health in the period immediately preceding the pandemic. Together, these analyses constitute a comprehensive examination of the enduring role of spatial segregation in generating ethno-national and racial health gaps. In addition, the project both emphasizes the role of a structural “upstream” causal factor (spatial segregation) in the development of ethnic and racial health inequalities and reveals how state policies helped create this structural condition. I begin by providing a brief review of the history of spatial segregation in Israel and outlining segregation’s consequences for the health and social positions of Palestinians.
Background
Spatial Segregation of Jews and Palestinians in Israel
In Israel, the Palestinian minority (about 20% of the population) and the Jewish majority (about 80%) are highly spatially and socially segregated. Since the establishment of the state of Israel in 1948, most Palestinians, about 90%, live in fully segregated localities where all residents are Palestinian (Central Bureau of Statistics [CBS] 2023c). Indeed, nearly all cities and towns in Israel are either Jewish or Palestinian—of the approximately 200 urban localities in the country, only 8 are administratively defined as “mixed localities” that include both Jews and Palestinians. These so-called mixed localities include a Palestinian minority living primarily in segregated neighborhoods alongside a Jewish majority. The spatial segregation of Jews and Palestinians is exacerbated by a difference in native languages—the former speak Hebrew, and the latter speak Arabic—that has led to near complete segregation in the school system. The separation in the school system reinforces residential segregation—Palestinian families with children are hesitant to move to Jewish cities or towns because these localities do not offer this basic service for native Arabic speakers. In addition, the two groups are relatively highly segregated in the labor market, partly due to factors such as peripherality and social segregation (Schnell and Shdema 2016; Yonay and Kraus 2018) and the uneven distribution of the workforce across local labor markets, which leads to high levels of workplace segregation (Garmash 2023). At the same time, the labor market and, in particular, workplaces are the most common sites of interactions between Palestinians and Jews (Darr 2023).
The ideology of separation and segregation emerged during the prestate period of the Zionist movement in late nineteenth century. The movement’s primary goal was to create a national homeland for Jews in Palestine “while ensuring separation, disengagement, and differentiation from the Palestinian population, which historically had always been the majority in the country” (Bäuml 2017:103). This goal was achieved in 1948 with the establishment of the state of Israel via a war and large population transfers. The exile of about 80% of the Palestinians who lived in the areas that fell under Israel’s control and the absorption of large waves of Jewish immigrants changed the population balance and created a new Jewish majority (Bäuml 2017; Boger 2008; Tzfadia 2008).
Israel confined the Palestinians who remained in the area (the subject of this study) and became citizens of the new state to a set of small, segregated spaces or ghettos (Boger 2008). This process of ghettoization not only ensured the separation of Jews and Palestinians but also allowed the Israeli government to enforce different regimes in Palestinian and Jewish spaces. In the two decades after the establishment of Israel, from 1948 to 1966, Palestinian spaces fell under the rule of the Israeli military, which enforced severe restrictions on the population’s movement and effectively controlled Palestinians’ intermittent presence in mainstream Israeli/Jewish spaces (Bäuml 2017; Sa’di 1995).
The segregation of Palestinians aligned with Israel’s main spatial policy of Judaization dispersal (Tzfadia 2008), or the dispersal of Jewish immigrants across frontier and internal frontier regions to ensure Jewish dominance and control of the land. During the 1950s, this policy targeted Jewish immigrants arriving mostly from Arab and Islamic countries in Asia and North Africa (known as Mizrahi Jews). A centralized real estate regime forced Mizrahi Jewish immigrants to settle in frontier and internal frontier regions, specifically, the Galilee and Negev regions or the Northern and Southern Districts, respectively. The implementation of this policy helped create a geographic, social, and economic periphery (and class structure) in Israel that follows ethno-national and ethnic boundaries. Most first-generation Mizrahi Jewish immigrants and most Palestinians became part of this newly produced periphery (although the two groups lived in separate localities), and Jewish immigrants from European countries who had moved to the area earlier lived predominantly in the central region of the country (Tzfadia 2006, 2008; Tzfadia and Yacobi 2011).
In 1966, the cessation of the military regime ended the legal measures limiting the free movement of Palestinians; however, the change did not end segregation. Israel implemented other measures and practices that continued the policy of Judaization dispersal and ensured the endurance of segregation. In the mid-1970s, motivated by reduced travel time between the periphery and the center due to new networks of roads and increasing rates of car ownership, upper-middle-class Jews began moving to the peripheral regions of the Galilee and the Negev, which were then inhabited by a Palestinian majority. The state facilitated this development through a joint national project called “Judaizing the Galilee” and “Judaizing the Negev.” To intensify Jewish control of this space (and the Palestinian population), the Israeli government established new Jewish settlements between Palestinian villages and towns—largely on land confiscated from Palestinian villages—to interrupt the territorial continuity of the Palestinian population (Plonski 2018; Yiftachel 2006). Although this policy brought Jews and Palestinians closer geographically, it created Jewish settlements that are separate from the existing Palestinian settlements by design. In addition, many of the new settlements are “communal settlements,” with entry overseen by admission committees that ensure Jewish exclusivity. In sum, overt practices of segregation, such as military rule, were replaced by obscured practices of segregation (Shafir 2018). Indeed, the selection process in combination with relatively high housing prices ensured that the new settlements were home exclusively to Jewish middle- and upper-middle-class families and thus intensified the separation between Jews and Palestinians and between class-based groups within Jewish society (Tzfadia 2008).
Residential segregation in Israel, which originated with the Zionist ideology of the separation of Jews and Palestinians and was instigated by state policies and practices, is deep and enduring. Cohen and Gordon (2018) argued that residential segregation is the most salient feature that organizes space in Israel. Segregation helps Israel’s bio-spatial project ascribe and inscribe Jewishness to and in space and constructs space as a racialized category. Thus, this residential pattern enforces the experience of space as either Jewish or Palestinian and solidifies a complete isomorphism between space and ethno-nationality: Space is ethno-nationality, and ethno-nationality is space.
Socioeconomic and Health Consequences of Spatial Segregation
Spatial segregation enables the implementation of not only separate systems of governance for Palestinians and Jews but also disparate development policies, with a clear preference for Jewish spaces over Palestinian ones in state investment in infrastructure, social services, and allocations of municipal budgets (Cohen and Gordon 2018; Khalidi and Shihadeh 2017; Wesley 2013). State budgets and resources are usually allocated to new Jewish settlements, such as the community settlements in the Galilee and the Negev, to make them attractive to middle-class Jewish households, especially with regard to lands and services (Cohen 2015; Cohen and Gordon 2018; Tzfadia 2008). In addition, most Palestinian towns have been excluded from the industrial parks the state has developed in the periphery to stimulate local economic growth (Khalidi and Shihadeh 2017; Schnell, Benenson, and Sofer 1999; Wesley 2013).
The inequality of development policies across racialized space added another dimension to the ethnonationality-space isomorphism: SES. One manifestation of this link is gaps between Palestinian and Jewish localities on measures of SES and peripherality. Based on measures developed by the CBS, which classify each locality into 1 of 10 clusters (these measures are described in detail in the methods sections), Palestinian localities are overrepresented in clusters with the lowest SES: In 2019, 80% of these localities, which are home to 87% of the total population in all Palestinian localities, are in the lowest SES clusters (1–4), and none are in the three highest clusters (8–10; CBS 2022).
In addition, as shown by research on social stratification in Israel, spatial segregation has an adverse impact on the social mobility of Palestinians. The distance of Palestinian localities from Israel’s geographic center, which is also the economic and financial center of the country, limits the access of the Palestinian labor force to many high-tech industries. Thus, spatial segregation severely constrains Palestinians’ industrial and occupational opportunities (Kraus and Yonay 2000; Shdema, Abu-Rayya, and Schnell 2019; Yonay and Kraus 2001), generating inequality and segregation between Palestinians and Jews in the labor market. Moreover, the data indicate that these inequalities are largest in areas with active conflict over space and land, such as in the Southern District and East Jerusalem (Cohen 2015; Yonay and Kraus 2018).
Many studies consider residential segregation a structural condition that adversely impacts the health of ethnic-racial minorities and contributes to ethnic and racial health gaps, for example, the gaps between Black and White populations in the United States (e.g., Anderson, Lopez, and Simburger 2021; Sewell 2016; Williams and Collins 2001). Despite the extreme spatial segregation of Palestinians and Jews and clear health gaps between the two groups—in 2017 to 2021, life expectancy at birth was 79.5 years for Palestinians and 83.3 years for Jews (CBS 2023c)—and data repeatedly showing the negative impact of segregation on Palestinians’ socioeconomic outcomes, research on health inequality in Israel has rarely assigned a significant role to spatial segregation.
The few exceptions to this pattern indicate that the spatial segregation of Palestinians limits their ability to access health services. Semyonov-Tal (2021) reported that length of stay in emergency departments, a measure of access to advanced health care, is considerably shorter for Palestinians than for Jews (and shorter for residents of the periphery than residents of the urban center) and concluded that these ethno-national disparities are fully attributable to patterns of spatial segregation.
Findings reported by Daoud et al. (2012) support a similar conclusion, specifically, that spatial inequality hinders access to health care. Their study investigated experiences and perceptions of infant care among mothers from the Bedouin community in the Negev region (Southern District) who cited factors related to the region’s spatial conflict—land disputes, lack of community recognition, living in temporary “illegal” dwellings under threat of demolition, and forced displacement—as obstacles to accessing adequate infant care. Arguably, this severe spatial inequality leads to poor health among children in the Bedouin community—for example, in 2012, in the Negev region, the infant mortality rate among Palestinians was 12.0 deaths per 1,000 live births compared to 3.5 deaths per 1,000 births among Jews and 6.6 per 1,000 births among all Palestinians (CBS 2013).
Yacobi and Milner’s (2022) study of the Bedouin community in the Negev region is of special interest here; they analyzed the space-health nexus by emphasizing the political context of settler colonialism. They argued that the settler colonial production of space, which entails territorial control, biopolitics aimed at the indigenous Bedouin community, and the dispossession of this community, means that health inequality (and other types of inequality) is profoundly spatially produced. For the Bedouin community, the settler colonial production of space manifests as a lack of infrastructure, intensive exposure to environmental hazards, and the lack of accessible health services, which, in turn, produce poor health outcomes.
An analysis of gaps in life expectancy at birth between Palestinians and Jews conducted by Saabneh (2022) revealed a clear spatial-ethnonational hierarchy: Jews living in predominantly Jewish regions or in the center of the nation have the longest life expectancy in Israel (87.5 years). Furthermore, in the peripheral regions shared by Jews and Palestinians, Jews have a longer life expectancy (79.9 years) than segregated Palestinians (78.7 years). Thus, “the disadvantage for Palestinians is twofold; they are confined to a space with low life expectancy (relative to the Jewish space) and, within this space, they are segregated into localities with lower life expectancy than the neighboring Jewish ones” (Saabneh 2022).
Building on Saabneh’s (2022) findings, this study distinguishes between two types of spatial inequality endured by Palestinians. The first type is exclusion from the regions that constitute the economic and industrial centers of Israel and confinement to peripheral, less developed areas. This type of spatial inequality was largely achieved with the establishment of the state of Israel in 1948, when Palestinians who lived in center regions were expelled and most became refugees in neighboring countries, making center regions predominantly Jewish spaces. The second type of spatial inequality occurs within the peripheral and less developed regions, where almost all Palestinians reside. State-led settlement and development efforts in these regions established and supported new Jewish settlements geographically close to but separate from existing Palestinian ones, thereby producing peripheral regions that are shared by Palestinians and Jews, but with Palestinians segregated into less developed localities with a lower SES than the neighboring Jewish communities.
Previous research on the consequences of spatial segregation for the socioeconomic and health outcomes of Palestinians has not clearly articulated the distinction between these two types of segregation, (a) exclusion from the center and confinement to the periphery and (b) segregation within the geographic and social periphery. In this article, I use this distinction as an analytical tool that sheds light on the mechanisms through which spatial segregation impacts health (and socioeconomic) outcomes. In addition, I conduct a novel decomposition of the total ethno-national health gap into two components, each representing the contributions of one of these types of spatial inequality to the total gap.
Data and Methods
The analysis proceeded in five steps: (1) a comparison of rates of COVID-19 infections, hospitalizations, and deaths in Jewish and Palestinian spaces in the early phase of the pandemic; (2) an examination of the relation between a locality’s SES and rates of incidence and hospitalization at three points during the pandemic; (3) an assessment of prepandemic trends in the association between localities’ socioeconomic and mortality levels; (4) a decomposition of the identified gaps in various health indicators in the prepandemic period according to two types of spatial inequality; and (5) an estimation of center–periphery health gaps regardless of a locality’s ethno-national composition.
Palestinian space was defined as the aggregate of all Palestinian localities. Jewish space was defined as the aggregate of all Jewish localities and mixed cities (with a mixed population but a Jewish majority and a Palestinian minority), excluding the Palestinian community within these cities. To distinguish Palestinian neighborhoods from the dominant Jewish spaces in mixed cities, I used data at the level of statistical areas 1 (SAs), an administrative geographic unit that is part of a locality and consists of approximately 3,000 to 5,000 residents, and used the ethno-national composition of each SA’s population in 2020. I classified areas in which more than 70% of residents were Palestinian as Palestinian SAs and those in which more than 70% of residents were Jewish as Jewish SAs. A small number of SAs that include relatively even proportions of Palestinians and Jews were excluded from the analysis.
I also identified SAs where the majority of residents are Ultra-Orthodox Jews, who are considered a distinct group within Jewish society. Because of their strict adherence to Jewish law and traditions and high level of religiosity, Ultra-Orthodox Jews prefer to live separately from secular Jews, and thus they constitute another residentially segregated group. I used the results of the national elections to the Israeli parliament, which are published at the level of SAs, to identify Ultra-Orthodox neighborhoods. Specifically, I classified areas where 70% or more of the votes in the 2015 national elections were for Ultra-Orthodox parties as Ultra-Orthodox SAs. Previous studies of patterns of COVID-19 morbidity and mortality in Israel consistently show that Ultra-Orthodox Jews were affected by, responded to, and coped with the pandemic differently than the rest of the Jewish population (e.g., Bank of Israel 2021; Birenbaum-Carmeli and Chassida 2020, 2021; Muhsen et al. 2021; Waitzberg et al. 2020; Weinreb 2021). My examination of morbidity and mortality trends among Ultra-Orthodox Jews aligns with these observations (e.g., Appendix A, Figure 4, in the online version of the article), especially with regard to infection rates. Because of their distinct experience with the pandemic, Ultra-Orthodox Jews were excluded from the main analysis of gaps between Palestinians and Jews in various COVID-19 outcomes. Running the same comparisons without excluding Ultra-Orthodox Jews produces only slight differences from the main results, primarily because Ultra-Orthodox Jews comprise only about 11% of Jews (presented in Appendix A in the online version of the article).
Although these classifications based on ethno-nationality, space, and religiosity among Jews create four distinct groups, the current analysis compares only two of them: the non-Ultra-Orthodox Jewish majority (about 89% of all Jews) and Palestinians living in separate Palestinian localities (about 91% of all Palestinians). Ultra-Orthodox Jews (about 11% of all Jews) and Palestinians living in separate neighborhoods in the mixed cities (about 9% of all Palestinians) are excluded from the analysis.
Data on COVID-19 were obtained from the Ministry of Health (MoH). 2 The data consisted of administrative registration records of daily counts of verified cases of infection, hospitalization, and mortality from COVID-19 over the first 19 months of the pandemic, from March 11, 2020, through September 30, 2021. Because the spatial units that define each space-population group were localities and SAs, I used daily counts for localities and for SAs where necessary. Rates were calculated using the daily counts of these events at the level of the locality or SA (numerator) and estimates of the 2020 population of the localities and SAs (denominator). The use of administrative data and three COVID-19-related outcomes ensured that the estimated patterns were not biased because of reporting problems (as would likely be the case if only incidence rates were used).
The analysis used the measures of SES and peripherality of each locality developed by the Israel CBS: the peripherality index of localities in Israel 2020 (CBS 2023b) and the socioeconomic index of localities 2019 (CBS 2022). The peripherality measure reflected two elements: the locality’s geographic proximity to the boundary of the Tel Aviv District (defined as the most central district) and the proximity to each of the other localities, where these distances were weighted by the size of the locality. The SES index represented multiple socioeconomic outcomes in the locality, including (among others) education, employment, income, standard of living, and demographic composition (for detailed descriptions of these indices, see Appendix B in the online version of the article). Using factor analysis techniques and these index values (that are continuous standardized indicators), each locality was classified as belonging to 1 of 10 socioeconomic clusters (where cluster 1 included localities with the lowest SES and cluster 10 included localities with the highest SES) and 1 of 10 peripherality clusters (where cluster 1 included the most peripheral localities and cluster 10 included the least peripheral ones).
I argued earlier that Palestinians endure two types of spatial inequality. First, they are confined to peripheral, less developed regions and exclusion from the more developed, predominantly Jewish center. Second, within these peripheral regions, they endure segregation into separate localities, which because of their ethno-national composition, enjoy relatively less economic development and investments and therefore become areas with relatively lower SES. In the fourth and fifth steps of analyses, I examined the patterning of various health indicators in the prepandemic period according to these two types of spatial inequality.
The total ethno-national gap in various health indicators was decomposed into the two types of spatial inequality. The portion of the ethno-national health gap due to the first type of spatial inequality was estimated as the difference in health outcomes between Palestinian localities (almost all of which are peripheral) and the Jewish center (almost all localities in the center are Jewish). The portion of the ethno-national health gap due to the second type of spatial inequality was indicated by the difference in health outcomes between peripheral Palestinian and peripheral Jewish localities. According to this decomposition, the total gap was represented as a weighted average of these two types of gaps, where the weights were the proportions of the Jewish population in the center (.57) and in the periphery (.43). That is, the total gap was a sum of two gaps: (1) the absolute gap due to the exclusion of Palestinians from the center weighted by the proportion of the Jewish population in the center and (2) the absolute gap due to segregation within the periphery weighted by the proportion of the Jewish population in the periphery (see Appendix C in the online version of the article).
The health indicators used in this step of the analysis, which were calculated at the locality level and were available for urban localities with 10,000 or more residents, included standardized death rates (per 10,000 persons) in 2016–2020, hospitalization rates (per 1,000 persons) in 2017–2019, and rates of diabetes (per 1,000 persons) in 2017–2019. I excluded the city of Jerusalem because it has a large Palestinian population (close to 40% of all residents) whose members have a different civic status than other Palestinians in Israel (they live in East Jerusalem, the part of the city that Israel annexed to its territory after the 1976 war, and they were granted permanent residency but not citizenship at that time; thus, they exercise limited political power and are excluded from local politics, which seriously hampers the provision of municipal services, including health and educational services, to group members). Three mixed localities with small Palestinian populations (less than 15% of residents) were classified as Jewish spaces. Two mixed localities with Palestinian populations ranging from 15% to 30% were excluded from the analysis (including them as Jewish spaces did not change the results).
Results
COVID-19 Patterns
In the first step of the analysis, I compared trends in COVID-19 incidence, hospitalizations, and death rates in Jewish and Palestinian spaces during the first 18 months of the pandemic. Figure 1 compares trends in cumulative COVID-19 infection, hospitalization, and death rates in Palestinian and Jewish spaces during the first 12 months of the pandemic. The findings reveal two distinct periods. In the early period, between March and September of 2020, rates among the Palestinian communities were lower than rates among Jewish communities. In the later period, between September 2020 and March 2021, the gaps are reversed—rates among Palestinian localities exceed those among Jewish ones.
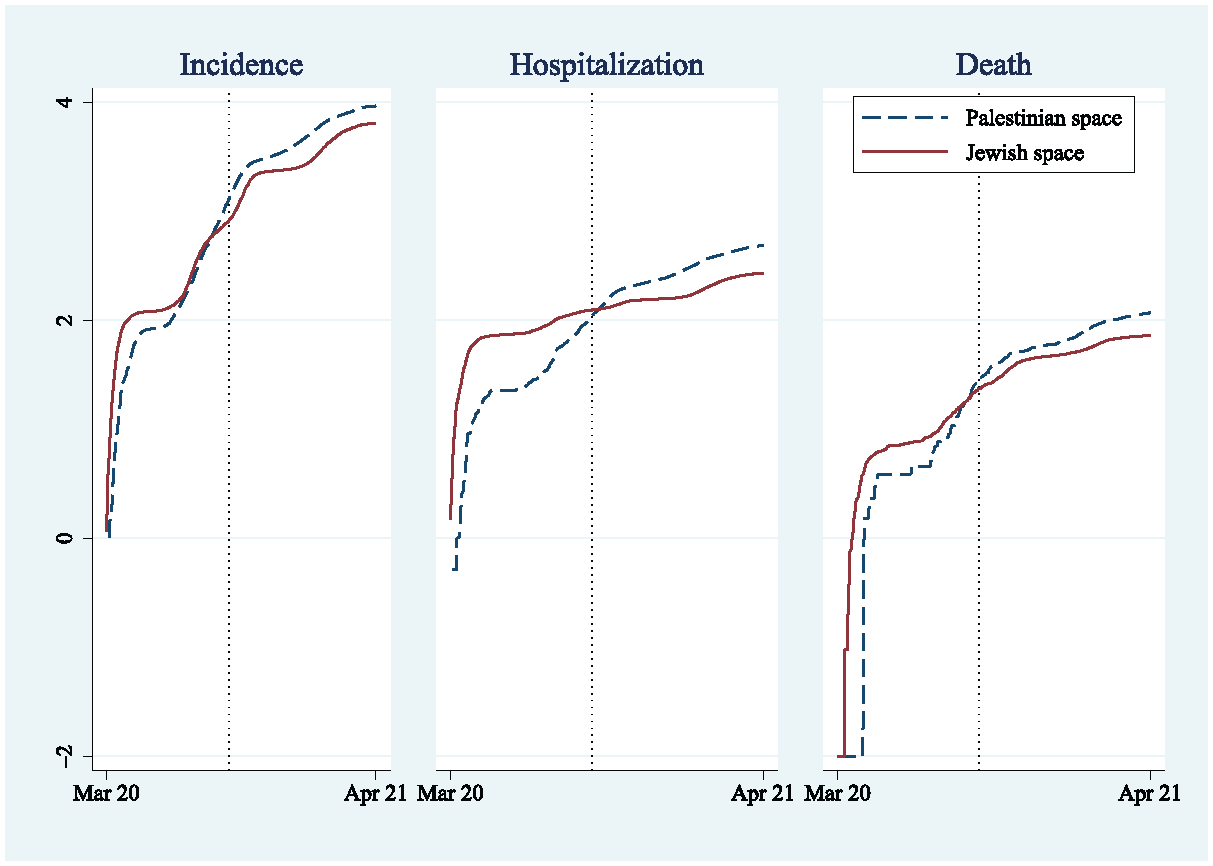
Incidence, Hospitalization, and Death Rates per 100,000 Persons from COVID-19 (Log Scale) between March 2020 and March 2021.
In the second step of the analysis, I examined the association between a locality’s SES and rates of incidence and hospitalization at three time points: June 2020 (in the first period), September 2020 (about the time the gaps reverse), and March 2021 (in the second period). Figure 2 plots each locality’s SES and the pertinent COVID-19 rates, shown in different colors for Jewish and Palestinian localities (death rates are not presented because of the small number of cases, especially in small localities).
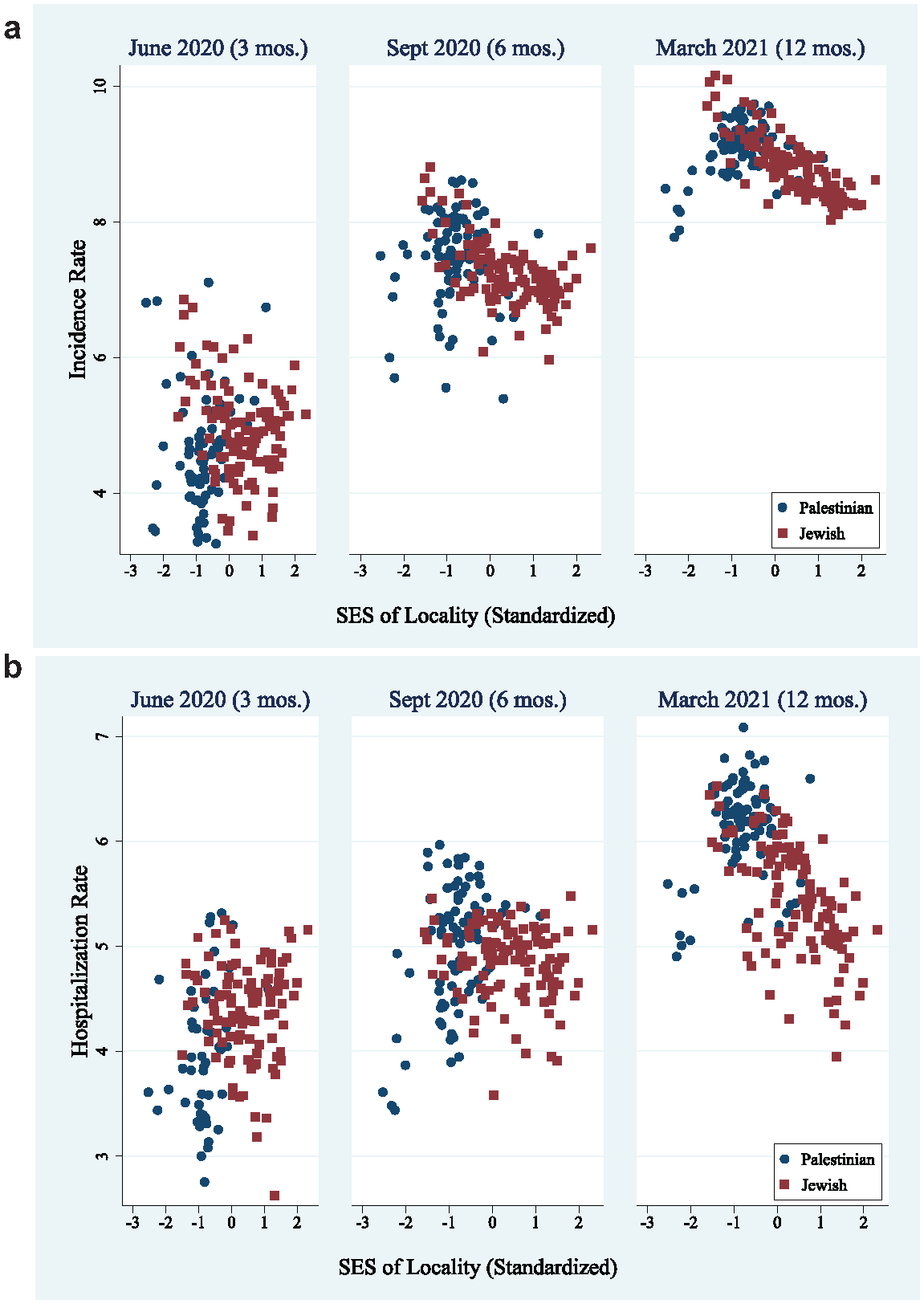
(a) Incidence Rates per 100,000 Persons, Log Scale, in Different Times since the Start of COVID-19 Epidemic by Socioeconomic Status (SES) and Racial Composition of Locality.
During the first period, there is no clear pattern of association between localities’ SES and rates of incidence and hospitalization (see Figures 2a and 2b). However, a clear negative association emerges in the later period—the higher the SES, the lower the incidence and hospitalization rates. A comparison of Palestinian and Jewish localities shows that this negative pattern develops earlier and is stronger among Jewish localities than among Palestinian ones. These results suggest that the observations from Palestinian localities obscure the appearance of a robust association between SES and these health measures in the early period of the pandemic. Although Palestinian localities are concentrated in the lower socioeconomic clusters, they experienced lower rates of incidence and hospitalization during this period. Later, when rates rose in these localities, the expected socioeconomic–health association emerged.
Pre-pandemic Trends: Associations between Localities’ Socioeconomic and Mortality Levels
In the third step of the analysis, I further tested the argument that the spatial segregation of Palestinian communities delayed the arrival of the virus in these communities and for half a year, generated a novel pattern—a reversal of the usual ethno-national health gap and a distortion of the robust association between SES and health outcomes. Specifically, I examined the association between localities’ socioeconomic and mortality levels in the period shortly before the COVID-19 pandemic, thus providing another reference point against which I can evaluate the novelty of the early period of the pandemic. The results show a clear negative association between SES and health outcomes in the prepandemic period. In 2017, localities with higher SES, mainly Jewish ones, had lower levels of all-cause mortality (see Figure 3), whereas Palestinian localities, which are concentrated at lower SES, had higher levels of all-cause mortality. This pattern is similar to the one that emerged in the later period of the pandemic and differs from the observations early in the pandemic.
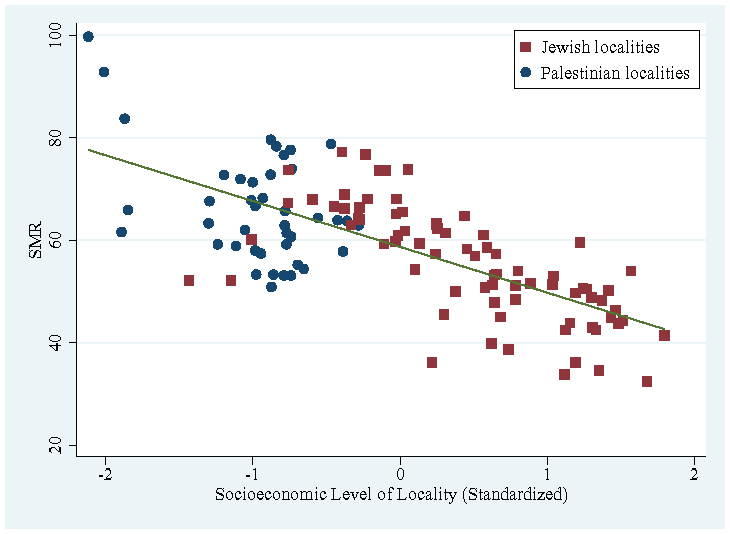
Standardized Mortality Rate (SMR) by Socioeconomic Level of Locality, 2017.
The lack of an association between localities’ SES and their COVID-19 outcomes in the early period of the pandemic combined with the existence of this association both before the pandemic and in the later stages of the pandemic and the evidence that observations from Palestinian localities are responsible for this “breakdown” of the association prompt me to conclude that the novel early pandemic pattern is not solely attributable to common causes of ethno-national health gaps (e.g., inequality in access to health care and socioeconomic measures). My argument that spatial segregation played a “protective” role in the early period of the pandemic and thus created a novel context in which the impact of these common causes of health gaps was temporarily deterred aligns with basic observations about the COVID-19 virus, specifically, that it spreads over time, across space, and via social networks; that it came from outside Israel; and that within Israel, it first appeared in Jewish spaces and only later appeared (at significant rates) in Palestinian spaces. The simple answer to one of the main questions motivating this investigation—Why did it take more than six months for the virus to appear at higher rates in Palestinian spaces than in Jewish spaces, as would be expected given higher morbidity and mortality among Palestinians?—is that these are segregated spaces, both spatially and socially. 3
Decomposition of Pre-pandemic Gaps in Health Indicators
To test the relative contribution of the two types of spatial inequality to health gaps, I conducted a series of comparisons of the three health indicators across spaces. First, I compared all Jewish localities to all Palestinian localities, with localities weighted by the size of their populations, to calculate an estimate of the nationwide Palestinian–Jewish gap. The results reveal clear ethno-national health gaps in all three health indicators (see Table 1, row H). The annual all-cause mortality rate (per 10,000 persons) in Palestinian localities is 662 deaths compared to a rate of 551 deaths in Jewish localities, a gap of 111 deaths per 10,000 persons. 4 In addition, Palestinian localities have higher rates of hospitalization (a gap of 41 cases per 1,000 persons) and diabetes (a gap of 36 cases per 1,000 persons).
Regional, Racial, and Regional-Racial Gaps in Various Health Indicators, the Peripherality Index, and Socioeconomic Status.

Source: Data are from the Central Bureau of Statistics.
Note: Peripherality level is measured by the peripherality index (see Appendix A in the online version of the article). Socioeconomic status is measured on a 1 to 10 scale, where 1 is lowest level and 10 is the highest. The reported figures of the peripherality index and socioeconomic status represent mean values for each group.
Next, I decomposed the total ethno-national gap into the two types of spatial inequality: segregation from the center and segregation within the periphery. The results of the decomposition are summarized in Table 1. Results for the mortality gap show that the unweighted absolute gap due to the first type of spatial inequality (141 per 10,000 persons) is higher than the unweighted absolute gap due to the second type (71 deaths per 10,000 persons). When weighted, the total gap of 111 deaths per 10,000 persons is decomposed into 80 deaths per 10,000 persons contributed by first type of spatial inequality and 31 deaths per 10,000 persons contributed by the second type of spatial inequality. In percentages, exclusion from the center accounts for 72% of the total mortality gap, and segregation within the periphery accounts for 28% of the total mortality gap.
The results for gaps in rates of hospitalization and diabetes show similar relative contributions of each type of spatial inequality to the total respective health gap. The relative contributions of the first and second types of inequality to the total ethno-national gap in hospitalization are 71% and 29%, respectively. The figures for the total ethno-national gap in the prevalence of diabetes are 63% and 37%, respectively. In sum, the decompositions of the ethno-national gap in various health indicators suggest that both types of spatial inequality contribute to the health gap between Palestinians and Jews, but the contribution of the first type (exclusion from the center) is more prominent than the contribution of the second type (segregation within the periphery).
I also applied the decomposition method to ethno-national gaps in SES and peripherality indicators to shed light on the mechanism through which spatial segregation impacts health. The results show that the contribution of exclusion from the central regions accounts for about 72% of the total gap in localities’ SES. The contribution of the same type of spatial inequality to the total gap in peripherality is, of course, higher, at 84%. Notably, however, 16% of the peripherality gap between Palestinians and Jewish localities is the result of segregation within the peripheral regions, meaning that Palestinian localities experience a deeper peripherality than Jewish localities in these regions.
Center–Periphery Gaps
The estimates in Table 1 (rows A–G) enable an estimation of other relevant health gaps. For example, by comparing localities in the central and peripheral districts, I can derive an estimate of center–periphery health gaps in Israel regardless of the ethno-national composition of localities. The results indicate substantial gaps between the geographic center and periphery in Israel. Regardless of their ethno-national composition, localities in the periphery have lower SES (and, of course, are more peripheral) and higher rates of mortality, hospitalization, and diabetes (see Table 1). For example, the annual all-cause mortality rate (per 10,000 persons) in the center region is 529 deaths compared to 609 deaths in the periphery, a gap of 80 deaths per 10,000 persons.
These center–periphery health gaps persist when the comparison is limited to Jewish localities; however, they are smaller than the general center–periphery gaps (87%, 82%, and 55% of the general death, hospitalization, and diabetes gaps, respectively). This pattern indicates that the general center–periphery health gaps are only partially due to ethno-national health gaps. In general, the results point to significant center–periphery health gaps. In addition, the results suggest that Palestinians and Jews are not equally exposed to this type of inequality; almost all Palestinians but less than half of Jews are subject to the harmful effects of peripherality.
COVID-19 Gaps
Finally, I applied the decomposition method to gaps in COVID-19 infection and hospitalization rates. Using the same data as in the earlier analysis of COVID-19 gaps over time, I decompose gaps measured at the end of the observation period, when the harmful, long-standing impact of segregation had taken effect, and Palestinians had higher rates than Jews. The results show that the first and second types of inequality contributed equally (both 50%) to the total ethno-national gap in infection. The figures for the total ethno-national gap in the rates of hospitalization from COVID-19 are 44% and 56%, respectively, indicating that exclusion from the center makes a larger contribution to gaps in COVID-19 outcomes (less than half of the total gap) than to gaps in health indicators measured before the pandemic (about two-thirds of the total gap). Because COVID-19 outcomes are cumulative rates that summarize the experience of each ethno-national group from the start of the pandemic until the latest observation and because in the early stage of the pandemic, being far from the center temporarily played a “protective” role for Palestinians, this type of segregation contributed less to the total gap than to gaps in health measures before the pandemic.
Discussion
Although the observation of unexpectedly low rates of COVID-19 mortality and morbidity among Palestinian communities in Israel early in the pandemic, despite their long-standing lower SES and poorer health outcomes, was the initial motivation for this study, a more profound impetus is the development of an analytical framework that explains this unforeseen outcome and ethno-national and racial health gaps in general. The study presents a framework, which has been largely overlooked in prior studies of health gaps between Palestinians and Jews in Israel, that emphasizes the consequences of spatial inequality and segregation for health inequality. The results show that the Palestinian population is highly spatially, residentially, and socially segregated from the Jewish population, and this fundamental condition impedes economic development in Palestinian spaces and propels them into a state of peripherality. In addition, the results highlight the negative impact of these spatial inequalities on Palestinians’ health outcomes. MoH reports have acknowledged regional health inequalities in mortality, morbidity, and provision of health care services (Israel Ministry of Health 2021, 2022) and have noted multiple health gaps between Palestinians and Jews; however, these reports discussed the two types of inequality separately. This examination extends the extant literature by revealing the strong, intricate connections between space and ethno-nationality in Israel and thus between spatial and ethno-national (and racial) health inequalities.
Sewell (2016) argued that the segregation of the Black community in the United States does not cause racial inequality; rather, the forces that instigate segregation are the “true causes” of racial inequality. Borrowing Sewell’s (2016) approach, this study sought to identify the ways political, societal, and economic forces and conditions intersect in contributing to observed health inequalities between a dominant majority and a subordinate minority in a given society. Specifically, the analysis pointed to state policies and practices that aim to control space and population, including policies of settlement and economic development, as the major forces that instigated segregation. In this framework, urban and economic development plans serve as tools for controlling and racializing space, and policies of population transfer, displacement, and distribution and policies of (de-)development work in concert with processes that create separate, racialized, and unequal spaces. Thus, health inequality is conceptualized as an outcome not of segregation per se, but of the forces and powers that instigate spatial segregation and inequality.
The analysis of COVID-19 patterns is a unique opportunity to test arguments about the impact of segregation on health. The unexpected initial pattern of lower COVID-19 morbidity and mortality rates among Palestinians challenges explanations that focus only on the Palestinian minority’s relatively low SES (e.g., lower levels of income, education, and employment) and prepandemic poorer health outcomes (e.g., higher rates of morbidity and lower life expectancy) because these conditions would have predicted COVID-19 outcomes opposite from those observed. Only a consideration of the extreme spatial, social, and residential segregation of Palestinian communities illuminates the unique time-space dynamic of the spread the coronavirus. The spatial-temporal progression of the pandemic—beginning in Jewish spaces and later moving toward Palestinian ones—highlights the dual role of residential segregation: It first played a “protective” factor by delaying the arrival of the virus for a few months, during which time, the manifestation of common health determinants, such as socioeconomic factors, was impeded. Eventually, with the increase in infection rates, the impact of Palestinian communities’ lower SES and poorer prepandemic health condition on COVID-19 outcomes emerged, demonstrating the long-term, harmful impact of segregation.
Although unexpected patterns of COVID-19 outcomes motivated this investigation and revealed how residential segregation and the policies instigating this segregation help explain these unexpected events, a key contribution of the project comes from analyzing health inequalities between Palestinian and Jewish spaces in the period before the start of the pandemic. This analysis sheds light on two distinct types of spatial segregation. My focus on the distinction between being segregated from the center and being segregated within the periphery is novel—the few studies that have referred to segregation’s harmful impact on social and health outcomes in Israel (e.g., Saabneh 2022) have overlooked this twofold nature of segregation. The results reveal that exclusion from the center (a dimension of segregation originally proposed in this research) and being segregated within the geographic periphery make distinct contributions to the poor health and low SES of Palestinian spaces—both factors are significant, but they differ in magnitude. Specifically, being segregated from the center accounts for more than two-thirds of the examined health gaps. Importantly, the impact of being segregated within the periphery is meaningful even though it is smaller in magnitude.
Some may argue that segregation from the center should be understood not as a separate dimension of spatial segregation but rather as an aspect of geographic peripherality, which characterizes both Palestinians and Jews. Yet both types of spatial inequality (or dimensions of segregation) were motivated by same ideology of separation (Jewish nationalism), were created by the same forces (state institutions and agents), and materialized via the same policies and practices of space production (population transfers, new settlement, and the economic development of space). Thus, segregation does not entail simply Palestinians and Jews living in largely separate localities (or in the few cases of mixed localities, in separate neighborhoods), which in itself is a very profound and fundamental social fact. Rather, segregation entails the combination of two types of spatial inequality—being pushed away from the center (i.e., segregated from the center’s Jewish population and social networks, labor market, health care, and other services) and being segregated from Jewish settlements within the Jewish periphery. This two-pronged segregation of Palestinians and the forces and powers that instigated this segregation are fundamental determinants of health (Sewell 2016; Williams and Collins 2001).
Recent studies of health inequality that point to the settler colonial nature of Israel’s political regime have sought to move beyond the framework of social determinants of health (SDoH) or “causes of causes,” arguing that settler colonialism is a fundamental determinant that precedes any other determinant of health (Asi et al. 2022; Qato 2020; Tanous et al. 2023; Wispelwey et al. 2023). Yacobi and Milner (2022) argued that the SDoH framework, although suitable to the examination of health inequality in liberal democracies where inequality is primarily manifested in the unequal distribution of resources such as education and income, is less suitable to discussions of health inequality in the Israeli case of settler colonialism, which requires the examination of inequality in other factors, such as conflict over land and space and control of resources and territory (especially in the case the Bedouin community in the south). They concluded that because “[h]ealth determinants are spatial, the colonial project of appropriating, controlling and ordering space is crucial to understanding the institutional foundations that produce health disparities” (Yacobi and Milner 2022:585). This analysis bolsters this argument by providing new evidence of a bold spatial inequality that characterizes all Palestinian localities. In addition, the analysis shows that this spatial inequality impacts and thus precedes SDoH (e.g., socioeconomic outcomes) and elucidates the association between this inequality and ethno-national health gaps. Furthermore, the analysis aligns with these studies in that it points to the same culprits as sources of ethno-national health inequality, that is, state institutions and agents.
The decomposition of segregation also helps identify and evaluate the mechanisms linking spatial segregation and health outcomes. Williams and Collins (2001) considered the residential segregation of racial-ethnic minorities (with emphasis on the Black community in the United States) a “fundamental cause” of health—meaning it is related to poor health outcomes via multiple mechanisms and for multiple disease outcomes—that has strong ties to socioeconomic achievements and overall life chances. Many other researchers have agreed with this assessment (e.g., Anderson and Ray-Warren 2022; Karbeah and Hacker 2023), and they described multiple mechanisms through which segregation is related to poor health outcomes, arguing that segregation limits access to high-quality education and labor markets, constrains access to a variety of key community resources such as health care and public services, and increases exposure to environmental dangers and crime. The current results align with these findings, showing that the spatial segregation of Palestinian localities, especially the exclusion of Palestinians from the center, contributes to their relatively lower SES (compared to Jewish localities). Furthermore, the results suggest that Palestinians’ limited access to the dominant labor market found in the center region (e.g., Kraus and Yonay 2000; Yonay and Kraus 2018) and the relatively low economic development of Palestinians’ peripheral localities are significant mechanisms that link segregation and poor health among this population.
Another mechanism that drives health gaps is differential access to health care and health services (Anderson et al. 2021; Anderson and Ray-Warren 2022; Williams and Collins 2001). Consistent with previous reports, the current findings reveal geographic differences in health services in Israel such that the population in the center enjoys greater access and more advanced services than residents of the periphery (Israel Ministry of Health 2021, 2022). The findings also show that Palestinians are much more exposed to peripherality than Jews and thus are more likely to experience limited access to health services. Just as importantly, this analysis highlights the historical context that produced and maintained the peripherality of Palestinian communities. Ignoring this context naturalizes ethno-nationality, in the sense of encouraging the incorrect perception that Palestinians are naturally peripheral, and wrongly promotes the idea that center–periphery gaps in health (and other outcomes) in Israel are merely geographic and are ethno-nationality neutral.
In sum, this research makes several theoretical and methodological contributions. First, the project presents an analytical spatial perspective for explaining ethnic and racial health inequality that has been largely overlooked in studies of health gaps between Palestinians and Jews in Israel. Second, the work entails a comprehensive examination of spatial policies and practices, identifies the forces that instigated and maintained the spatial segregation of Palestinians, and elaborates the role of segregation in generating health gaps between Palestinians and Jews. In addition, this research suggests a novel operationalization of the impact of segregation on health outcomes by proposing a model of two types of spatial inequality and devising a decomposition method to evaluate the relative contribution of each type of segregation to the total health gap. The findings indicate that the segregation of Palestinians from the center and their confinement to peripheral regions are crucial determinants of their poor health outcomes and that the segregation of the Palestinian community within the geographic periphery also contributes to lower levels of health.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465241283455 – Supplemental material for Spatial and Ethno-national Health Inequalities: Health and Mortality Gaps between Palestinians and Jews in Israel
Supplemental material, sj-docx-1-hsb-10.1177_00221465241283455 for Spatial and Ethno-national Health Inequalities: Health and Mortality Gaps between Palestinians and Jews in Israel by Ameed Saabneh in Journal of Health and Social Behavior
Footnotes
Acknowledgements
Earlier versions of this study were presented at the Summer Institute in Computational Social Science 2022 at the University of Haifa (SICSS-Haifa), the Population Association of America 2023 Annual Meeting, and the European Population Conference 2024.
Supplemental Material
Appendices A through C are available in the online version of the article.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.