
Abstract
Black Americans experience the death of a parent much earlier in the life course than White Americans on average. However, studies have not considered whether the cardiovascular health consequences of early parental death vary by race. Using data from the National Longitudinal Study of Adolescent to Adult Health, we explore associations between early parental death and cardiovascular disease (CVD) risk in early to mid-adulthood (N = 4,193). We find that the death of a parent during childhood or adolescence (ages 0–17) or the transition to adulthood (ages 18–27) is associated with increased CVD risk for Black Americans, whereas parental death following the transition to adulthood (ages 28+) undermines cardiovascular health for both Black Americans and White Americans. These findings illustrate how a stress and life course perspective can help inform strategies aimed at addressing both the unequal burden of bereavement and high cardiovascular risk faced by Black Americans.
Approximately one in every four U.S. deaths is attributable to cardiovascular disease (CVD; Murphy et al. 2020), a risk much greater for Black Americans than White Americans (Javed et al. 2022; Jolly et al. 2010). Research has increasingly focused on stress as a major risk factor for CVD, with particular attention to how stressors throughout the early life course contribute to CVD risk in adulthood (Doom et al. 2017). However, prior studies have not examined whether and how parental death, one of the most stressful and life-altering early life adversities (Luecken and Roubinov 2012), may influence CVD risk in early to mid-adulthood across racial groups.
Stressful events in early life can trigger turning points that disrupt life trajectories and increase stress levels in ways that undermine health across the life course (Pearlin 2010). The death of a parent is a life-changing stressor that is markedly more prevalent among Black Americans than White Americans (Umberson et al. 2017). Indeed, research shows that Black Americans lose family members more often and earlier in the life course than other populations, creating an unequal burden of grief that may contribute to racial inequities in health (Umberson 2017). Although prior studies show that Black Americans are more likely to experience early parental death than White Americans (i.e., increased exposure; Umberson et al. 2017), few explore whether the negative health effects of such losses differ by race (i.e., increased vulnerability). Black Americans are exposed to a myriad of stressors due to systemic racism (Hummer 2023; Williams, Lawrence, and Davis 2019), and the stress stemming from early parental death experiences could compound this already high stress burden, resulting in greater CVD risk.
Prior studies exploring linkages between early life adversities and CVD risk often rely on composite measures of stress that include but do not focus on the death of a parent (Doom et al. 2017). Most studies also focus exclusively on parental deaths occurring in childhood or adolescence (Chen et al. 2020; Li et al. 2014) and do not consider how parental deaths throughout the early life course may undermine cardiovascular health by early to mid-adulthood. This is especially significant considering that the transition to adulthood has lengthened in recent decades (Fry 2023; Settersten and Ray 2010), with children often relying on their parents well into their 20s (Fingerman and Birditt 2011). Moreover, prior studies have not explored how these processes may differ for Black Americans and White Americans, a stark omission considering both the increased risk of early parental death (Umberson et al. 2017) and heightened vulnerability to cardiovascular disease (Javed et al. 2022; Jolly et al. 2010) faced by Black Americans.
To address these gaps, we use nationally representative data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) and the stress process and life course perspectives to examine whether and how exposure to parental death throughout the early life course (from childhood through early adulthood) is associated with CVD risk in early to mid-adulthood in potentially different ways for Black Americans and White Americans. Stressful experiences often generate additional stressors and reactions to stress that can undermine health (Pearlin 2010). Thus, we also explore whether social, psychological, and behavioral factors mediate associations between race, early parental death, and CVD risk. Identifying race differences in early life factors that contribute to CVD risk in early to mid-adulthood is important because although CVD mortality has decreased overall in recent decades, these trends appear to have stalled for working-age adults (National Academies of Sciences, Engineering, and Medicine 2021). Moreover, racial disparities in CVD mortality have widened in recent years (Singh et al. 2015). Thus, explorations into specific early life course stressors that may differentially increase CVD risk in early to mid-adulthood are vital for understanding racial inequities in cardiovascular health.
Background
Stress and CVD Risk over the Life Course
We use the stress process and life course perspectives (Pearlin 2010) to frame our understanding of whether and how the death of a parent from childhood through early adulthood influences CVD risk and in potentially different ways for Black Americans and White Americans. The stress process and life course perspectives suggest that socially patterned exposure to traumatic events and acute and chronic stressors takes a cumulative toll on health over the life course (Elder, Johnson, and Crosnoe 2003; Pearlin 2010). These perspectives also point to the importance of “linked lives” for influencing health across the life course, suggesting that one’s life is embedded in a large network of family and social relationships. The loss of those relationships (e.g., the death of a parent) can trigger important turning points that disrupt individual life course trajectories and increase stress levels with profound and wide-ranging consequences for health (Carr 2018).
Research has examined various types of early life adversities, such as interpersonal violence and parental disability, as predictors of CVD risk later in life (Doom et al. 2017), although much of this research relies on composite measures of stressors that include but do not focus on the death of a parent. One study does find that bereaved children have higher cortisol output in response to acute stress compared to nonbereaved youth (Dietz et al. 2013). Other studies find that parental death in childhood is associated with increased risk of heart disease (Chen et al. 2020) and CVD-related mortality risk in early adulthood (Li et al. 2014) and later life (Smith et al. 2014). However, these studies largely focus on parental deaths in childhood and adolescence only and are based on predominantly White populations in Europe (Chen et al. 2020; Li et al. 2014) or specific regions of the United States (Dietz et al. 2013; Smith et al. 2014). Taken together, prior research suggests that by disrupting a myriad of physiological systems, exposure to the death of a parent can significantly undermine cardiovascular health.
Race as a Social System Shaping the Life Course Context of Early Parental Death and CVD Risk
Pervasive and enduring structures of racism within the United States have produced long-standing racial disparities in health and mortality by limiting access to knowledge, power, freedom, and other health-enhancing resources (Hummer 2023; Phelan and Link 2015; Williams et al. 2019). Consequently, Black Americans experience the death of a parent more often and earlier in life than White Americans (Umberson et al. 2017). Indeed, by age 10, Black children are over 3 times more likely to lose a mother and over 2 times more likely to lose a father compared to White children (Umberson et al. 2017). This disadvantage continues into early adulthood, with Black young adults being almost twice as likely to lose a mother and approximately 37% more likely to lose a father by age 30 compared to White young adults (Umberson et al. 2017). Although prior studies have identified race inequities in exposure to early parental death, they have not considered whether such exposure differentially influences CVD risk in early to mid-adulthood across racial groups.
There are multiple reasons to expect that the negative cardiovascular health effects of early parental death may be stronger for Black Americans compared to White Americans. First, family bereavement experiences in the United States occur within the context of a racialized society that undermines Black Americans’ physical and psychological functioning more than White Americans’ (Williams et al. 2019). Black Americans already face an increased risk of exposure to stressors such as race-based discrimination, harassment, and violence, all of which undermine health (Hummer 2023). Considering cardiovascular health, research has shown that exposure to chronic interpersonal racism is associated with elevated sympathetic nervous system and HPA axis activation (Goosby, Cheadle, and Mitchell 2018). Persistent upregulation of these systems contributes to wear and tear on the cardiovascular system over time and can lead to cardiometabolic conditions (Kiecolt-Glaser et al. 2020). Thus, the added stress from bereavement experiences could compound other race-based stressors to differentially undermine the cardiovascular health of Black Americans compared to White Americans.
Black Americans also generally have less access to important resources that could help protect against the negative health consequences of familial bereavement (Thoits 2010; Umberson and Donnelly 2023). For example, Black Americans have less access to health care, including preventive care that could help detect the early signs of cardiovascular disease (Hall et al. 2015). Even when such services are available, the quality of medical care provided to Black Americans is lower than that of White Americans, and this inequity has been linked to increased mortality risk for Black Americans (Phelan and Link 2015). Thus, less access to and worse quality of health care could increase the likelihood of poor cardiovascular health resulting from early parental death for Black Americans.
Conversely, Black Americans are more likely to maintain relationships with extended family members than White Americans (Taylor et al. 2013), thus increasing the level and quality of support available following the death of a parent. Black Americans also rely on religion to cope with stress more so than White Americans (Taylor, Chatters, and Jackson 2007), and religiosity may be protective for health (Ellison and Hummer 2010). This may be especially true for cardiovascular health because prior research suggests that religiosity may reduce inflammation, particularly for Black Americans (Ferraro and Kim 2014). However, it is important to note that Black Americans generally have fewer social connections they could use to access important health-enhancing resources (e.g., social support, health-related knowledge; Thoits 2010; Umberson and Donnelly 2023), a mechanism that is further compounded by racial inequity in exposure to family member death. Taken together, inequities in stress exposure and diminished access to coping resources may generate cumulative disadvantage over the life course for Black Americans, resulting in increased CVD risk from early parental death relative to White Americans. Thus, we test the following hypothesis:
Hypothesis 1: (a) Experiencing the death of a parent throughout the early life course will be associated with increased CVD risk in early to mid-adulthood and (b) more so for Black Americans than White Americans.
Timing of Parental Death
The stress process and life course perspectives emphasize that the impact of stressful events largely depends on timing over the life course (Elder et al. 2003). Indeed, substantial evidence shows that stressors encountered earlier in life can be more damaging than those in later life because they can lead to lifelong patterns of emotional and physiological arousal that disrupt health across the life course (Pearlin 2010). The death of a parent is a major acute stressor that can have long-term effects on health (Luecken and Roubinov 2012), especially when experienced earlier in the life course than expected (Smith et al. 2014; Stroebe, Schut, and Stroebe 2007). Although most people can expect to lose a parent during mid-to-late adulthood, losses in childhood through early adulthood are generally less common (Scherer 2019). Thus, it is important to consider whether parent death and CVD risk linkages differ based on death timing and particularly whether it occurred before, during, or following the transition to adulthood.
The transition to adulthood, generally marked by leaving the parental home, forming intimate relationships, and having children, has lengthened significantly in recent decades (Fry 2023; Settersten and Ray 2010), with children often relying on their parents well past childhood and adolescence (Fingerman and Birditt 2011). Recent U.S. estimates indicate that the median ages at first marriage (U.S. Census Bureau 2018) and first birth (Eickmeyer et al. 2017) are now in the late 20s. Such demographic trends underscore the need to consider the potential health-damaging effect of parental death beyond those occurring in childhood or adolescence, including during and following the transition to adulthood. Thus, we test the following hypothesis:
Hypothesis 2: Parental deaths occurring earlier in the life course (i.e., in childhood/adolescence or during the transition to adulthood) will have a stronger effect on CVD risk in early to mid-adulthood than parental deaths occurring later (i.e., following the transition to adulthood).
Importantly, the timing and nature of life course transitions often differ by race. For instance, Black Americans leave their parents’ homes at older ages (Goldscheider, Hofferth, and Curtin 2014) and are more likely to return to the parental home than White Americans (South and Lei 2015). Black men also have the highest median age at first marriage (32 years), followed by Black women (30.4 years), White men (29.4 years), and White women (27.9 years; Payne 2019). Conversely, Black Americans enter parenthood at younger ages than White Americans on average (Martin et al. 2015; Stykes 2011). Thus, if Black Americans transition out of the parental home later, marry later, and enter parenthood earlier, the death of a parent during this period may be especially disruptive, resulting in the loss of an important source of support. This is particularly significant given Black children also face other unique early life adversities due to systemic racism (Tilstra et al. 2022), which could exacerbate the negative health consequences of early parental death.
The Role of Social, Psychological, and Behavioral Factors
Stressful events, such as bereavement, often create additional stressors through the process of stress proliferation (Pearlin 2010). Thus, in addition to the direct effects of stress stemming from grief, the death of a parent could undermine health by activating long-term social, psychological, and behavioral risk factors that contribute to CVD risk. For example, parental death, especially early in life, may activate social risks by reducing household income, which can negatively impact health (Kahn and Pearlin 2006). The death of a parent could also decrease the size of a young person’s social network and increase their social isolation (Umberson and Donnelly 2023). This is important because prior studies find that social isolation is associated with elevated systolic blood pressure (Hawkley et al. 2006) and delayed blood pressure recovery from stress (Steptoe and Marmot 2006), both of which are CVD risk factors.
Parental death may activate psychological risks linked to cardiovascular health by causing emotional distress and disrupting perceptions of personal control (McGuire, Ahearn, and Doering 2015). A parent’s death may also elevate health risk behaviors due to the elevated stress of bereavement and the loss of a parent who could serve as a health-promoting figure (Frech 2012). Health risk behaviors associated with cardiovascular conditions include tobacco use, which increases plaque in blood vessels (U.S. Department of Health and Human Services 2014); alcohol use, which is linked to coronary disease, heart failure, hypertension, and cardiomyopathy (Piano 2017); and sedentary behavior and physical inactivity, which are strongly linked to CVDs (Lavie et al. 2019).
Few studies have considered social, psychological, and behavioral pathways between parental death and cardiovascular health. Using a measure of childhood adversity that includes but does not focus on parental death, Doom et al. (2017) find that adversity is associated with increased adult CVD risk through pathways including financial stress, educational attainment, and health behaviors. Chen et al. (2020) find that the parental death and heart disease risk association is partially attributed to smoking, risky alcohol use, and low educational attainment. Smith et al. (2014) find weak mediating effects of marital and socioeconomic status (SES) for linkages between parental death and heart disease. Yet these prior studies rely on samples of predominantly White populations and do not consider possible differences in how the death of a parent shapes CVD risk for Black Americans.
There are notable ways in which the social, psychological, and behavioral pathways that contribute to CVD risk following parental death may differ for Black Americans and White Americans. For example, there is evidence that Black Americans do not receive the same health-promoting returns from higher SES as White Americans (Boen 2016), including cardiovascular health (Bell et al. 2018). Black Americans also face unique racialized stressors that could complicate the pathways from bereavement to health (Tilstra et al. 2022; Williams et al. 2019). As such, we expect that the social, psychological, and behavioral pathways examined in this study will more fully explain the association between the death of a parent and CVD risk for White Americans than for Black Americans. Thus, we test the following hypothesis:
Hypothesis 3: (a) Social, psychological, and behavioral risk factors will mediate the association between the death of a parent throughout the early life course and CVD risk in early to mid-adulthood and (b) more so for White Americans than for Black Americans.
Data and Methods
To examine linkages between race, early parental death, and CVD risk in early to mid-adulthood, we used restricted data from Add Health, a nationally representative school-based study of U.S. adolescents enrolled in Grades 7 to 12 during the 1994 to 1995 academic year (Harris et al. 2019). Systematic sampling methods and implicit stratification were used to select participants based on region of the country, urbanicity, school size, school type (public vs. private), and race-ethnicity. Following initial data collection, later waves of data were collected in 1996 (Wave II), 2001 to 2002 (Wave III), 2008 to 2009 (Wave IV), and 2016 to 2018 (Wave V). The present study uses data from participant survey interviews at Wave I and Wave V and biomarker data collected at Wave V. Our sample is restricted to non-Hispanic Black and non-Hispanic White respondents identified by an Add Health-constructed measure (Udry, Li, and Hendrickson-Smith 2003) who were not pregnant at the time of the Wave V biomarker data collection and had valid sampling weights (N = 4,193). By Wave V, our sample had transitioned to adulthood, with respondents between 33 and 43 years old (M = 37.3 years).
Measures
CVD risk score (CVD risk)
CVD risk was based on four established risk factors for CVD measured at Wave V: (1) waist circumference, (2) blood pressure, (3) hemoglobin A1c (HbA1c), and (4) C-reactive protein (CRP; Walsemann, Goosby, and Farr 2016). Waist circumference is strongly associated with CVDs and mortality and is a well-used clinical indicator for CVD risk (Siren, Eriksson, and Vanhanen 2012). High blood pressure (i.e., hypertension) is associated with elevated hypertensive heart disease, stroke, heart attack, and heart failure risks (Izzo, Sica, and Black 2007). HbA1c, a time-integrated marker of glycemic control, predicts CVD risk in people with and without diabetes, with high HbA1c levels strongly associated with increased coronary heart disease incidence (Goto et al. 2015). Finally, CRP is often used as a marker for systemic inflammation and has emerged as an important predictor of CVD (Ridker 2003).
We classified each indicator based on established clinical cut-points for CVD risk such that 0 = low risk, 1 = moderate risk, and 2 = high risk (Walsemann et al. 2016). Waist circumference was classified into three categories: 0 = <94 cm for men and < 80 cm for women, 1 = 94 to 101 cm for men and 80 to 87 cm for women, and 2 = ≥ 102 cm for men and ≥88 cm for women. Blood pressure was classified using measured systolic blood pressure (SBP) and diastolic blood pressure (DBP) where 0 = normotensive (< 120 SBP and < 80 DBP), 1 = prehypertensive (120–139 SBP or 80–89 DBP), and 2 = hypertensive (≥ 140 SBP or ≥ 90 DBP). Measured HbA1c was used to classify respondents as 0 = nondiabetic (< 5.7%), 1 = prediabetic (5.7%–6.4%), and 2 = diabetic (≥ 6.5%). CRP was categorized as 0 = <1.0 mg/L, 1 = 1.0 to 3.0 mg/L, and 2 = > 3.0 mg/L. The four indicators were summed to create a measure of CVD risk ranging from 0 to 8 and subsequently categorized into a final measure reflecting low (0–2), moderate (3–5), and high (6–8) CVD risk. Analyses using different configurations of the CVD risk measure including a continuous measure (range = 0–8) and two binary measures (1 = high CVD risk; 1 = moderate/high risk) yielded similar results.
Death of a parent
At Wave V, respondents were asked whether their biological mother and biological father were still alive. Add Health also asks respondents to identify the woman and man they feel raised them, with options including a biological parent, adoptive parent, stepparent, and grandparent, among others. If respondents identify their mother or father figure as someone other than their biological parent, they are then asked whether such parent figure is still alive. We used this information to create a dichotomous indicator of parental death inclusive of biological and parent-like figures.
Age at parent death
We used an additional parental death indicator that integrated the respondent age at the time of parent death and was coded as follows: 0 = no parent death, 1 = parent death at ages 0 to 17 (childhood/adolescence), 2 = parent death at ages 18 to 27 (during the transition to adulthood), and 3 = parent death at ages 28+ (following the transition to adulthood). Additional analyses (available on request) using alternative parental death age cutoffs (e.g., ages 0–16, 17–26, 27+; ages 0–18, 19–28, 29+) yielded similar findings. In cases where multiple parent deaths occurred, the age at first parent death was used.
Social risk factors
Social risk factors included household income and social connectivity at Wave V. Respondent self-reported household income at Wave V was adjusted for household size and log-transformed. Social connectivity was an adapted measure that incorporated dichotomized indicators for marital status (1 = married/cohabitating), number of close friends (1 = 6 or more close friends), church attendance (1 = attends 12+ times/year), and volunteering behavior (1 = volunteered in the past year). The four indicators were summed to create a final measure ranging from 0 to 4, with higher values indicating increased social connectivity (Yang et al. 2016).
Psychological risk factors
Psychological risk factors included psychological distress and personal control at Wave V. Psychological distress was measured using five items from the Center for Epidemiological Studies Depression (CES-D) scale (Radloff 1977). Respondents were asked how often during the past seven days they felt (1) depressed, (2) sad, (3) happy, (4) like they could not shake off the blues, and (5) that life was not worth living. Item 3 was reverse-coded, and responses were summed with higher values indicating increased distress (range = 0–15). We used the shortened, four-item version of the Perceived Stress Scale (Cohen, Kamarck, and Mermelstein 1983) to measure personal control. Respondents were asked how often during the past 30 days they felt (1) that they were unable to control important things in their life, (2) confident in their ability to handle problems, (3) that things were going their way, and (4) that difficulties were piling so high that they could not overcome them. All items were summed, with Items 1 and 4 reverse-coded, so that higher values indicated higher levels of personal control.
Behavioral risk factors
Behavioral risk factors included physical inactivity, heavy drinking, and tobacco use at Wave V. For physical inactivity, respondents were asked how many times they performed various activities in the past seven days. Activities were categorized into six groups ranging from light to vigorous exercises, including biking, dancing, yard work, playing sports, and weightlifting. Responses to the six items were summed, and respondents were classified as physically inactive if they reported less than three activities in the past seven days. Respondents were also asked about their alcohol use. Respondents reported how many days in the past 12 months they drank four or more drinks in a row for women and five or more drinks for men. Respondents were categorized as heavy drinkers if they reported doing so more than once a month (World Health Organization 2019). Finally, respondents were considered tobacco users if they reported use of cigarettes, cigars, chewing tobacco, or electronic cigarettes in the past month.
Covariates
Multivariate analyses accounted for gender (1 = woman), age (in years), and other family member deaths (sibling, child, or spouse; 1 = yes) at Wave V. Active infectious and inflammatory diseases can bias estimates of CRP (Whitsel et al. 2024). As such, we controlled for recent infection in the past four weeks at Wave V, including gum disease/tooth loss, active infection, injury, acute illness, surgery, and active seasonal allergies (1 = yes). We also controlled for prescribed anti-hypertension, anti-diabetic, and anti-inflammatory medication use in the past four weeks (1 = yes) at Wave V. Our analyses further accounted for childhood self-rated health (1 = fair/poor health) and childhood family SES measured at Wave I. Childhood family SES is a standardized measure constructed by Add Health that incorporates parent-reported educational attainment, parental occupation, household income, and household receipt of public assistance (Belsky et al. 2018).
Analytic Strategy
We employed ordinal logistic regression to explore the relationship between the death of a parent and CVD risk. Specifically, we used parental death (1) at all ages throughout the early life course and (2) during specific life course stages (childhood/adolescence: ages 0–17; during the transition to adulthood: ages 18– 27; and following the transition to adulthood: ages 28+) to predict CVD risk in early to mid-adulthood. Analyses were conducted using Stata 16 (StataCorp 2019). Missing data for all variables were imputed using the mi impute command with chained equations specification (M = 30). Analyses were weighted using sampling weights provided by Add Health (Chen and Harris 2020). We applied the Stata svyset command to account for the unequal probability of sample selection, clustering of individuals within schools, and stratification by region of residence. Because factors influencing both parental death exposure and CVD risk likely differ by race, analyses were performed separately for non-Hispanic Black respondents and non-Hispanic White respondents. The Stata mysuest command was used to test whether estimates of the effect of parental death on CVD risk differed by parent death timing and/or race. Mysuest is a postestimation command that tests the equality of coefficients by first estimating the difference in coefficients within and/or between models and then testing that the estimates do not significantly differ (Cañette and Marchenko 2018).
To examine whether and how social, psychological, and behavioral risk factors mediate associations between parental death and CVD risk, we added groups of risk factors separately before combining all risk factors in a fully adjusted model. We further conducted formal mediation analyses using the Karlson-Holm-Breen (KHB) method (Karlson and Holm 2011). The KHB method is a formal mediation test suitable for logit models that decomposes the total effect of parental death into direct and indirect effects of multiple mediators (Kohler, Karlson, and Holm 2011).
Results
Descriptive Statistics
Weighted descriptive data in Table 1 show that Black respondents are significantly more likely to experience early parental death than White respondents (p < .001). By Wave V, over 50% of Black respondents report experiencing the death of a parent compared to approximately 29% of White respondents. Black respondents also reported a significantly higher percentage of parent deaths at all early life course stages, including childhood/adolescence (ages 0–17; p < .001), during the transition to adulthood (ages 18–27; p < .001), and following the transition to adulthood (ages 28+; p < .001). Considering CVD risk, Black respondents are significantly less likely to be in the low-risk category (p < .001) and more likely to be in the high-risk category (p < .001) compared to White respondents.
Weighted Descriptive Statistics by Race (N = 4,193).
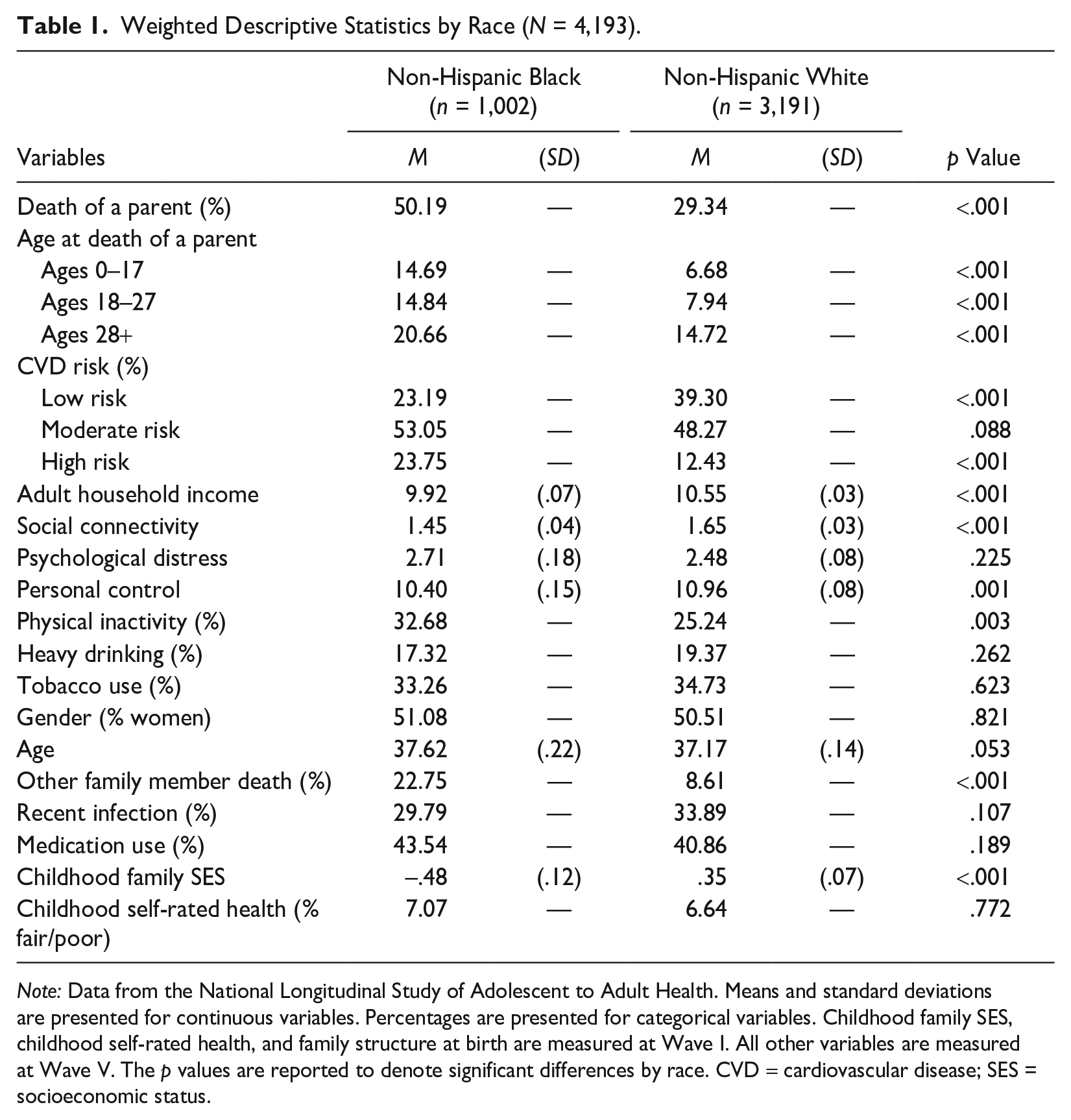
Note: Data from the National Longitudinal Study of Adolescent to Adult Health. Means and standard deviations are presented for continuous variables. Percentages are presented for categorical variables. Childhood family SES, childhood self-rated health, and family structure at birth are measured at Wave I. All other variables are measured at Wave V. The p values are reported to denote significant differences by race. CVD = cardiovascular disease; SES = socioeconomic status.
For social, psychological, and behavioral risk factors, Black respondents report significantly lower adult household income (p < .001), social connectivity (p < .001), and personal control (p < .01) than White respondents. Black respondents are also more likely to be physically inactive (p < .01) than White respondents. Psychological distress and the likelihood of being heavy drinkers or tobacco users do not significantly differ by race. Considering covariates, Black respondents are more likely to report experiencing the death of a nonparent family member (p < .001) and report lower childhood family SES (p < .001) compared to White respondents. Gender, age, recent infection, medication use, and childhood self-rated health do not significantly differ by race.
Death of a Parent and CVD Risk (Test of Hypothesis 1)
Model 1 of Table 2 tests whether the death of a parent throughout the early life course (regardless of parent death timing) is associated with CVD risk in early to mid-adulthood. Results are presented separately for Black respondents (Panel A) and White respondents (Panel B). Results from Panel A, Model 1 indicate that net of covariates, Black respondents who experienced the death of a parent throughout the early life course have 1.85 times higher odds of being in a higher CVD risk category than Black respondents who did not experience the death of a parent (p < .001). For White respondents (Panel B), results from Model 1 indicate that the death of a parent is not significantly associated with the odds of being in a higher CVD risk category (odds ratio [OR] = 1.19; p = .063). Results from postestimation tests of equality confirm a significant race difference, indicating that the association between the death of a parent throughout the early life course and CVD risk is stronger for Black respondents compared to White respondents (p < .05). Overall, these results partially support Hypothesis 1: The death of a parent throughout the early life course is associated with increased CVD risk in early to mid-adulthood but for Black respondents only.
Adjusted Odds Ratios from Ordinal Logistic Regression Models Testing the Death of a Parent on Cardiovascular Disease Risk by Race (N = 4,193).
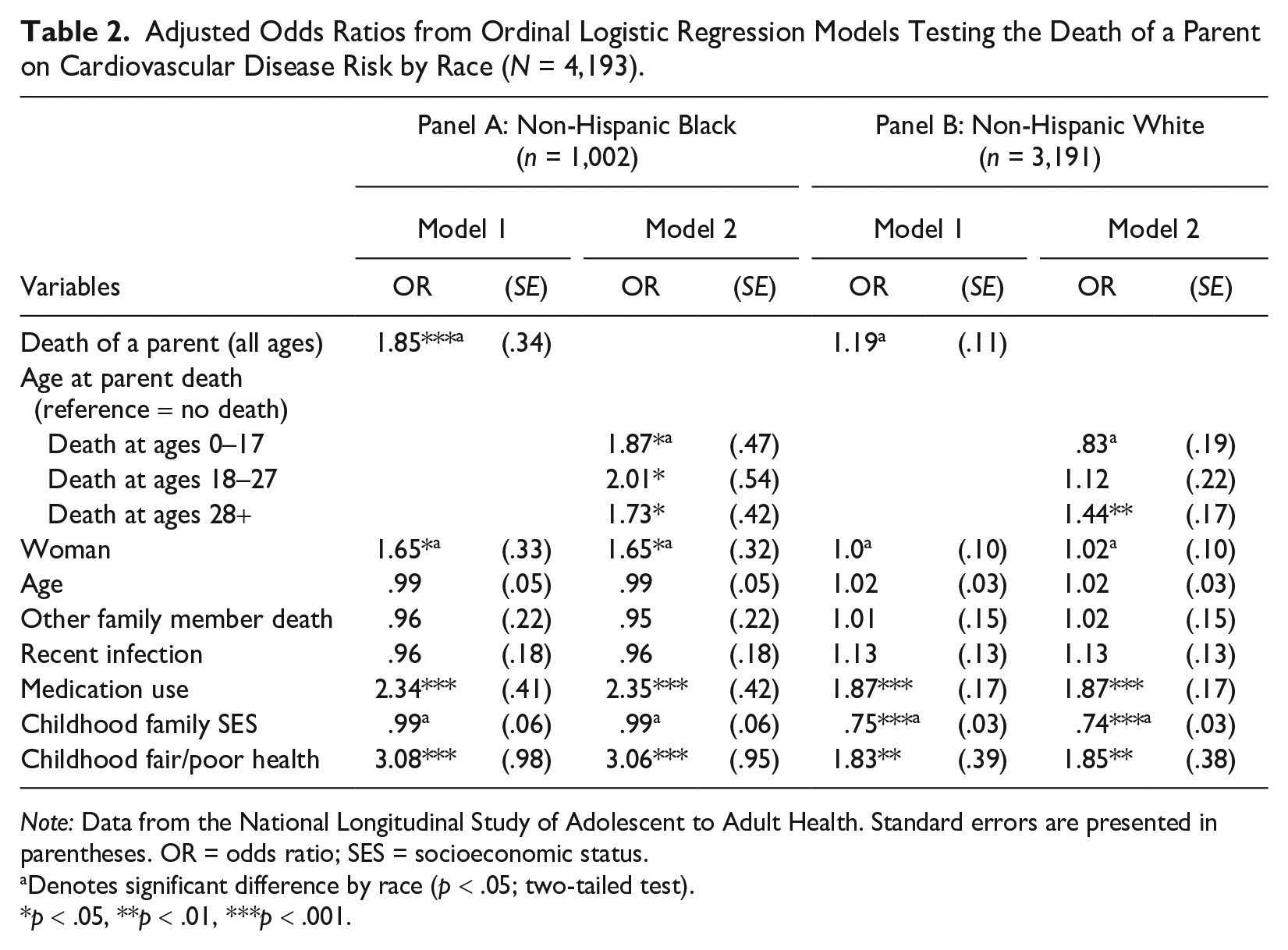
Note: Data from the National Longitudinal Study of Adolescent to Adult Health. Standard errors are presented in parentheses. OR = odds ratio; SES = socioeconomic status.
Denotes significant difference by race (p < .05; two-tailed test).
p < .05, **p < .01, ***p < .001.
Parent Death Timing and CVD Risk (Test of Hypothesis 2)
Next, we test whether the association between early parental death and CVD risk in early to mid-adulthood differs by parent death timing. Specifically, we test whether parental death exposure in childhood/adolescence (ages 0–17) or during the transition to adulthood (ages 18–27) has a stronger effect on CVD risk than exposure following the transition to adulthood (ages 28+). Results from Model 2 of Table 2 indicate that for Black respondents (Panel A), the association between the death of a parent and CVD risk is significant regardless of the life course stage the death occurred in. That is, Black respondents exposed to the death of a parent at ages 0 to 17 (OR = 1.87, p < .05), ages 18 to 27 (OR = 2.01, p < .05), and ages 28+ (OR = 1.73, p < .05) are at increased odds of being in a higher risk CVD risk category compared to Black respondents not exposed to the death of a parent. Results from analyses testing the equality of estimates indicate that the associations are similar across parental death age groups.
Results for White respondents follow a different pattern (Table 2, Panel B). Although Model 1 suggests no significant association between parental death and CVD risk, Model 2 indicates a significant association if the death occurs following the transition to adulthood (ages 28+). That is, the odds of being in a higher CVD risk category are 1.44 times higher among White respondents who experience the death of a parent at ages 28+ compared to White respondents who do not experience the death of a parent (p < .01). Associations for the death of a parent at ages 0 to 17 (OR = 0.83; p = .414) or ages 18 to 27 (OR = 1.12; p = .566) with CVD risk are not statistically significant. Postestimation tests of equality indicate that the association between the death of a parent at ages 28+ and CVD risk is stronger compared to the association for death of a parent at ages 0 to 17 (p < .05) but not ages 18 to 27 (p = .278). Considering between-race differences, the association for the death of a parent at ages 0 to 17 is significantly stronger for Black respondents compared to White respondents (p < .05), providing additional support for Hypothesis 1b. The associations of CVD risk with the death of a parent at ages 18 to 27 and ages 28+ do not significantly differ by race.
Overall, results fail to support Hypothesis 2 for either Black respondents or White respondents: For Black respondents, experiencing the death of a parent throughout the early life course is associated with increased CVD risk in early to mid-adulthood similarly regardless of whether the death occurs in childhood/adolescence, during the transition to adulthood, or following the transition to adulthood, and experiencing the death of a parent is associated with increased CVD risk for White respondents but only if the death occurs following the transition to adulthood.
The Role of Social, Psychological, and Behavioral Risk Factors (Test of Hypothesis 3)
We also explore whether and how social, psychological, and behavioral risk factors mediate associations between early parental death and CVD risk in early to mid-adulthood (Table 3). Model 1 adds social risk factors (household income, social connectivity), Model 2 adds psychological risk factors (psychological distress, personal control), and Model 3 adds behavioral risk factors (physical inactivity, heavy drinking, tobacco use). Model 4 includes all risk factors. Results from Table 3 indicate that for both Black respondents (Panel A) and White respondents (Panel B), household income (Model 1) and physical inactivity (Model 3) are significantly associated with CVD risk. Social connectivity (Model 1) is also significantly associated with CVD risk but only among White respondents. For both Black respondents and White respondents, associations between the death of a parent during each life course stage and CVD risk are not attenuated after accounting for social, psychological, and behavioral risk factors. Results from formal mediation testing using the KHB method (Table 4) confirm that there are no significant indirect effects between the death of a parent and CVD risk through the examined social, psychological, and behavioral risk factors. Overall, these results fail to support Hypothesis 3: The associations between early parental death and CVD risk in early to mid-adulthood are not explained by social, psychological, and behavioral risk factors for either Black respondents or White respondents.
Adjusted Odds Ratios from Ordinal Logistic Regression Models Testing the Death of a Parent on Cardiovascular Disease Risk with Social, Psychological, and Behavioral Risk Factors by Race (N = 4,193).
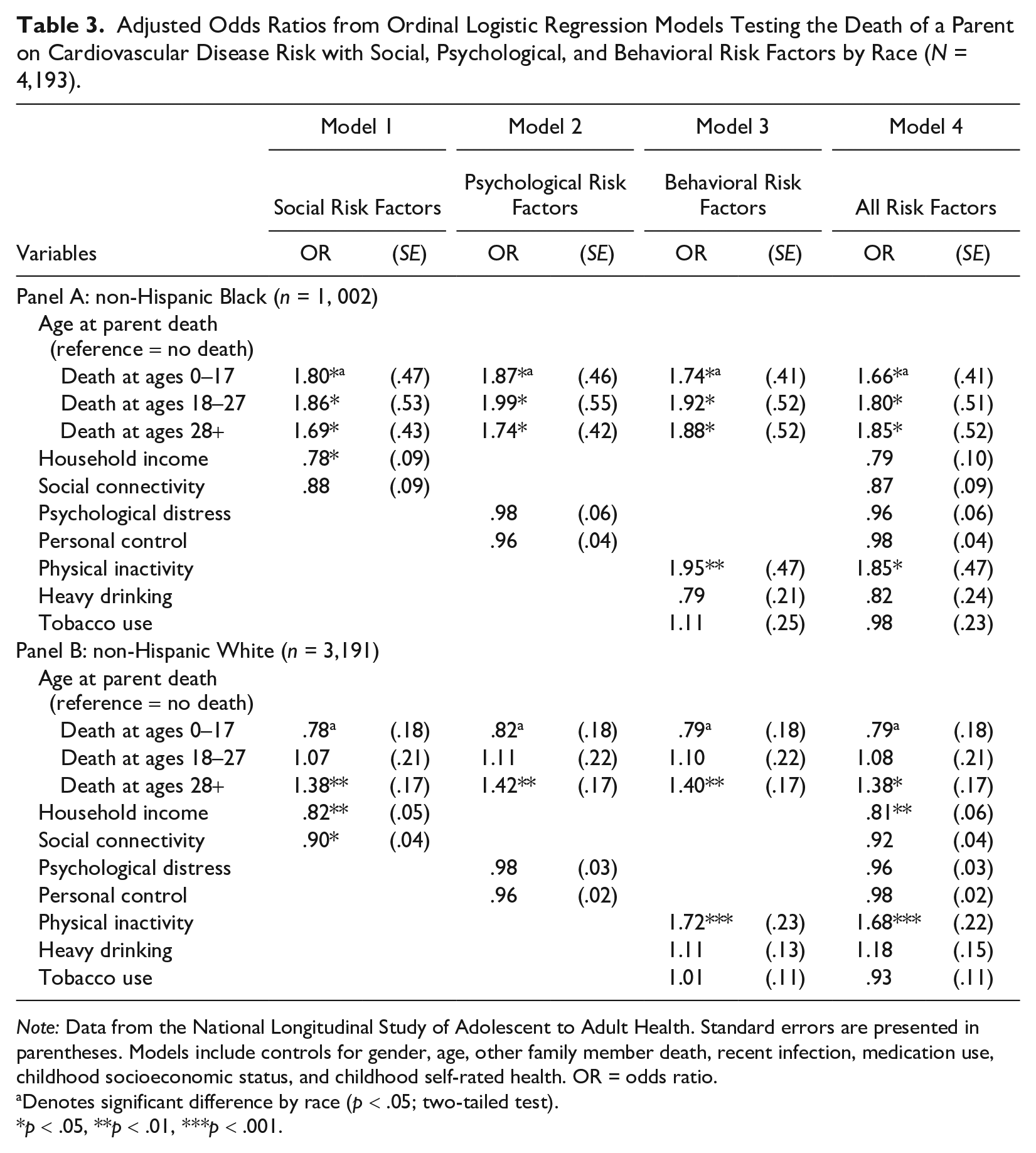
Note: Data from the National Longitudinal Study of Adolescent to Adult Health. Standard errors are presented in parentheses. Models include controls for gender, age, other family member death, recent infection, medication use, childhood socioeconomic status, and childhood self-rated health. OR = odds ratio.
Denotes significant difference by race (p < .05; two-tailed test).
p < .05, **p < .01, ***p < .001.
Adjusted Odds Ratios from KHB Mediation Analysis Results by Social, Psychological, and Behavioral Cardiovascular Disease Risk Factors.
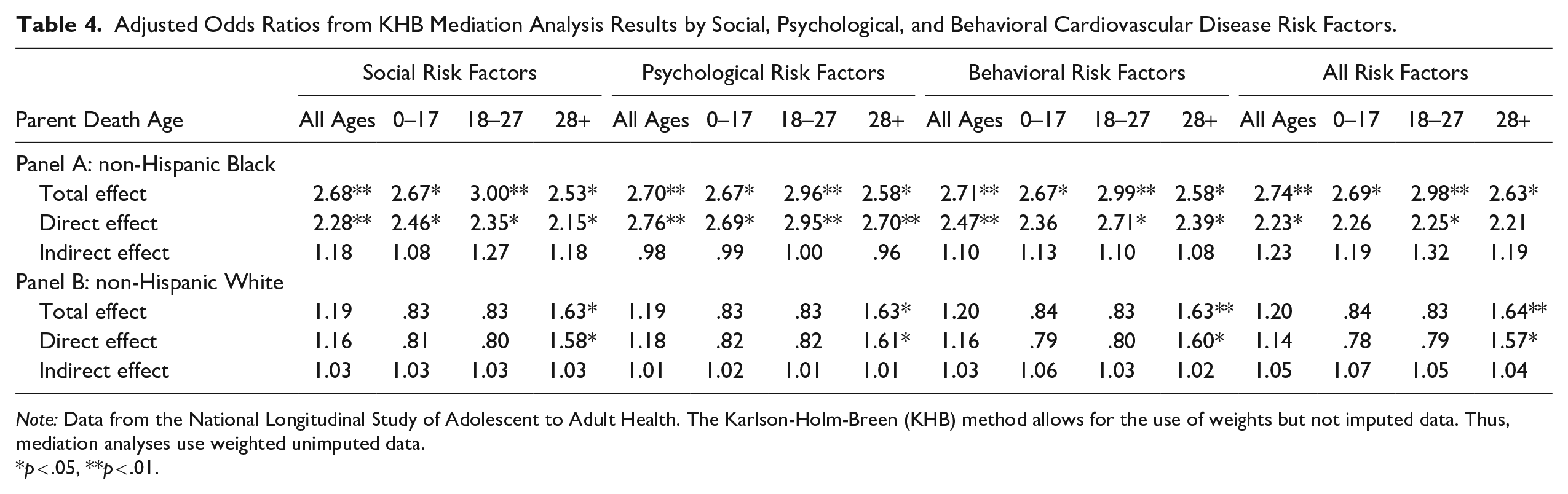
Note: Data from the National Longitudinal Study of Adolescent to Adult Health. The Karlson-Holm-Breen (KHB) method allows for the use of weights but not imputed data. Thus, mediation analyses use weighted unimputed data.
p < .05, **p < .01.
Sensitivity Analyses
To capture parental death experiences from childhood through early adulthood, primary analyses used measures of early parental death, CVD risk, and social, psychological, and behavioral risk factors from the same time point (Wave V). As a robustness check, we performed additional analyses using indicators of parental death and social, psychological, and behavioral risk factors measured at Wave IV to predict CVD risk at Wave V (results available on request). Respondents who reported the death of a parent between Wave IV and Wave V were excluded from analyses to ensure the correct temporal ordering between the mediators and the outcome (n = 580). Because the age of respondents at Wave IV ranged from 24 to 32 years old, we could only capture parental death experiences up to age 24 for the full sample. Thus, the measure of early parental death was altered such that 0 = no parent death, 1 = parent death at ages 0 to 17 (childhood/adolescence), and 2 = parent death at ages 18 to 24 (during the transition to adulthood). Respondents who reported the death of a parent at ages 25 or older were excluded from analyses (n = 246).
Overall, results were comparable to those from primary analyses. Parental death in childhood/adolescence or during the transition to adulthood was significantly associated with CVD risk for Black respondents only (p < .05). Postestimation tests of equality indicate similar associations regardless of the life course stage of death occurrence. Social, psychological, and behavioral risk factors did not mediate these associations. These results suggest a robust association between early parental death and CVD risk in early to mid-adulthood for Black respondents.
Discussion
The present study examines whether and how the death of a parent throughout the early life course (i.e., in childhood, adolescence, or during or following the transition to adulthood) is associated with CVD risk in early to mid-adulthood and is the first to consider how these processes differ for Black Americans and White Americans. Although extant research clearly shows that the death of a parent is a significant early life course stressor with consequences for cardiovascular health (Chen et al. 2020; Dietz et al. 2013; Li et al. 2014; Smith et al. 2014), prior studies often rely on composite measures of early life adversities that include but do not explicitly focus on parental bereavement (Doom et al. 2017). Moreover, prior research typically focuses on parental deaths in childhood or adolescence only and is based almost entirely on White populations (Chen et al. 2020; Dietz et al. 2013; Li et al. 2014; Smith et al. 2014). Notably, Black Americans are much more likely than White Americans to experience the death of a parent, especially in the early life course (Umberson et al. 2017). However, little is known about whether the negative health consequences of early parental death also differ by race. We highlight three major findings that emerge from this study.
First, we find that the death of a parent in childhood or adolescence (ages 0–17) or during the transition to adulthood (ages 18–27) is associated with increased CVD risk in early to mid-adulthood for Black Americans but not for White Americans. Black Americans already face an increased risk of exposure to early parental death (Umberson et al. 2017), and our findings suggest that such exposure may be uniquely linked to their cardiovascular health, particularly when the loss occurs before adulthood. This aligns with prior theoretical work suggesting that socially patterned exposure to stressful experiences (e.g., by race, gender, etc.), especially those occurring early in life, takes a cumulative toll on health across the life course (Elder et al. 2003; Pearlin 2010). As one of the most stressful and life-altering experiences a child can face (Luecken and Roubinov 2012), the death of a parent may trigger a cascade of disadvantage that undermines long-term cardiovascular health. Because Black Americans are also disproportionately exposed to race-based stressors because of systemic racism (Hummer 2023; Williams et al. 2019), this disadvantage may be further compounded.
Conversely, systemic racism benefits White Americans by increasing access to important resources (e.g., health insurance, wealth) that could protect against the negative health consequences of early parental death while limiting access for Black Americans (Williams et al. 2019). Consequently, White Americans may be better equipped to recover from the death of a parent in the early life course. This may help explain the lack of association between the death of a parent in childhood, adolescence, or during the transition to adulthood and CVD risk for White Americans. Even when resources are available, research consistently shows that Black Americans do not experience the same returns to health as White Americans from advantages such as higher SES (Bell et al. 2018; Boen 2016). Thus, although socioeconomic and other resources may protect White Americans from the negative effects of early parental death, limited access to and diminishing returns from such resources may result in enduring cardiovascular health consequences for Black Americans.
Second, we find that experiencing the death of a parent following the transition to adulthood (ages 28+) is associated with increased CVD risk in early to mid-adulthood for both Black Americans and White Americans. Prior theoretical work emphasizes the importance of “linked lives” for understanding trajectories of health across the life course (Carr 2018; Elder et al. 2003). Parents’ and children’s lives are inextricably linked throughout life, and our findings suggest that the death of a parent can serve as a major turning point that adversely affects long-term cardiovascular health even if the death occurs after children have transitioned to adulthood. Our finding that experiencing parental death beyond childhood and even into early adulthood can have long-term implications for cardiovascular health may also reflect that the transition to adulthood in the United States has lengthened significantly in recent decades (Fry 2023; Settersten and Ray 2010). Children now often rely on their parents well into adulthood (Fingerman and Birditt 2011), and thus, experiencing the death of a parent following the transition to adulthood could result in the loss of an important source of social and financial support that could, in turn, undermine cardiovascular health.
Finally, we considered whether accounting for social, psychological, and behavioral risk factors linked to bereavement and cardiovascular health mediated linkages between early parental death and CVD risk in early to mid-adulthood. We find that these linkages endure net of adult household income, social connectivity, psychological distress, personal control, physical inactivity, heavy drinking, and tobacco use. Although these risk factors are often found to be important pathways through which bereavement experiences undermine health, there are other factors to consider. For example, parental deaths often alter educational trajectories (Patterson, Verdery, and Daw 2020) and disrupt family dynamics such as caregiving responsibilities and the quality of relationships with surviving family members (Droser 2020). Data capturing such dynamics and the stress resulting from them may help account for the association between parental death and CVD risk. Prior research also emphasizes the importance of psychosocial resources for buffering the negative health consequences of stressful experiences (Thoits 2010). Whereas the present study focuses on the mediating effects of social, psychological, and behavioral risk factors, future research should consider the potential mediating role of psychosocial resources for understanding linkages between early parental death and CVD risk.
Importantly, structural racism underlies experiences of grief and its effects on health (Umberson 2017; Williams et al. 2019). Thus, the conclusions drawn from the present study should be viewed through a critical lens with the understanding that the measurement of the pathways linking bereavement experiences to health cannot fully capture how structural racism actively undermines the minds and bodies of Black Americans. Future research should assess intervening mechanisms beyond the risk factors examined in the present study to understand how parental death throughout the early life course contributes to long-term disadvantage in cardiovascular health, especially when considering race differences in such processes.
We note several limitations of the present study. First, we cannot account for important parent characteristics that might influence an individual’s CVD risk, including the cause of death and parental health conditions prior to death. Losing a parent to CVD likely influences an individual’s future CVD risk. However, research has shown that the death of a parent undermines health even when a parent dies from unnatural causes (Li et al. 2014). We also include the deaths of parent-like figures in our analyses, including nonbiological relatives such as adoptive or stepparents, providing further evidence that forces beyond inherited disease risk shape the long-term consequences of parental bereavement. It is important to note that although the present study explores the association between the death of a parent and CVD risk in early to mid-adulthood, we are unable to estimate the impact of parental death on the development of CVDs or how these associations may change throughout mid-to-later life. Future research should consider how parental death influences multiple components of cardiovascular health, such as CVD incidence or acute coronary events, across the entire life course. Finally, although this study is the first to establish race differences in the association between early parental death and CVD risk in early to mid-adulthood, it does not assess whether such differences contribute to existing racial disparities in cardiovascular health or CVD-related morbidity and mortality.
Racial inequities in CVD risk are stark and persistent (Javed et al. 2022; Singh et al. 2015). The present study underscores the importance of considering how early life course exposure to the death of a parent differentially influences cardiovascular health for Black Americans and White Americans, which could, in turn, contribute to existing racial inequities. Using nationally representative longitudinal data, we find that experiencing the death of a parent in childhood, adolescence, or during the transition to adulthood is associated with increased CVD risk in early to mid-adulthood for Black Americans. Furthermore, exposure to the death of a parent following the transition to adulthood undermines cardiovascular health for both Black Americans and White Americans. Prior research suggests that disadvantage in exposure to family member deaths may contribute to racial health inequities (Umberson 2017; Umberson et al. 2017). The present study documents this disadvantage by providing the first evidence that the death of a parent throughout the early life course is uniquely linked to the cardiovascular health of Black Americans in early to mid-adulthood. Considering Black Americans’ heightened exposure to the death of family members and increased vulnerability to CVD, this study highlights the importance of screenings and policies that address bereavement as a major public health concern for Black Americans.
Footnotes
Acknowledgements
Add Health was designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Grant R01 AG054624, awarded to Dr. Debra Umberson by the National Institute on Aging; Grant P30 AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging; Grant P2C HD042849, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; Grant T32 HD007081, Training Program in Population Studies, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; and Grant P2C HD050924, awarded to the Carolina Population Center at the University of North Carolina at Chapel Hill by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. This research uses data from Add Health, funded by Grant P01 HD31921 (Kathleen Mullan Harris) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Add Health is currently directed by Robert A. Hummer and funded by the National Institute on Aging cooperative agreements U01 AG071448 (Hummer) and U01 AG071450 (Hummer and Aiello) at the University of North Carolina at Chapel Hill.