
Abstract
Few studies examine how high-achieving Black women navigate chronic reproductive health morbidities. Black women are disproportionately more likely to experience uterine fibroids, with earlier onset and more severe symptoms. This study leverages a national mixed-methods data set of Black women academics to examine how they describe symptomatic fibroids impacting their careers and lives. We find that participants (1) actively coped by engaging in superwoman schema, (2) postponed treatment due to the demands of their tenure-track position, and (3) normalized pain. Our findings suggest a potentially high prevalence of uterine fibroids among Black women faculty, that symptomatic fibroids were an impediment to some women’s careers, and that women with symptomatic fibroids often identified expectations of their careers as an impediment to seeking timely treatment. We provide insights for how highly educated, successful Black women cope and navigate career stress coupled with challenges resulting from chronic reproductive health morbidities.
Approximately 3% of doctoral degrees are earned by Black women (NCES 2017), and the percentage of Black women in tenure line faculty positions in higher education are similar (3.6%; NCES 2016). However, Black women who achieve entry into the highest ranks of educational attainment may not be conferred the analogous protective health benefits of their status (Colen et al. 2018; Colen, Pinchak, and Barnett 2021). Amid structural racism and the increased likelihood of working in predominantly White spaces where discrimination may be more acute (Van Dyke et al. 2020), highly educated, high-achieving Black people are put at greater risk for poorer health than their White counterparts (Colen et al. 2018; Hudson et al. 2016; Walsemann, Goosby, and Farr 2016). Even at the highest levels of achievement, Black women bear burdens of historical injustice and contemporary attacks on their scholarship and character (Johnson 2024) as a consequence of their positions at the nexus of multiple forms of racism and sexism (Purdie-Vaughns and Eibach 2008; Zambrana 2018). For Black women, ongoing stressors, embodying multiple marginalized identities, and the active coping in which they must engage all increase their risk for poorer health, including reproductive health morbidities (Allen et al. 2019; Erving et al. 2024; Goosby and Heidbrink 2013).
Faculty from historically underrepresented racial groups report experiencing lower work satisfaction and unwelcoming work climates that often result from institutionalized barriers that restrict their potential (Zambrana 2018). Specifically, Black women scholars report experiences of discrimination and isolation in their positions, where they often must excel while also engaging in invisible labor, such as mentoring students of color and being “diversity” representatives in their departments (Kelly and Winkle-Wagner 2017; Settles et al. 2022; Zambrana 2018). There is a dearth of knowledge, however, regarding navigating chronic health conditions—specifically, whether and how their reproductive health morbidities are linked to their stressful, demanding careers. As such, they are a key population to provide insights into the relationships between racism, sexism, and health conditions among a highly educated group.
Uterine fibroids, also known as leiomyomas, are benign uterine tumors that are highly prevalent, with upward of 70% of U.S. women across racial and ethnic groups having fibroids before they reach menopause (Hellwege et al. 2017). Black women are disproportionately more likely to have fibroids, be diagnosed with fibroids earlier, and have larger and more numerous tumors than White women (Hellwege et al. 2017; Stewart et al. 2013). Aside from a handful of examples (Orellana et al. 2022), few studies assess the consequnces of fibroids for women’s work life. Accordingly, we sought to examine how high-achieving Black women, an understudied group, experience diagnosed symptomatic fibroids in relation to their high-pressure work on the academic tenure track.
Leveraging a unique national sample of tenure-track Black women faculty in the social sciences, we explored how these scholars described their experiences with uterine fibroids using semistructured in-depth interviews and surveys. Specifically, we address (1) how participants describe living with symptomatic fibroids and (2) how they navigate and cope with their condition in the context of their tenure-track faculty experiences. Our findings provide key insights regarding how highly educated, successful Black women manage living with this chronic condition and connect their career stress to symptomatic fibroids experiences.
Background
Uterine Fibroids among Black Women
Approximately 70% of women will experience uterine fibroids by age 50, although estimates may be conservative due to undiagnosed asymptomatic women (Hellwege et al. 2017; Marsh et al. 2018). Fibroid symptoms can be painful and disruptive and include abnormal or excessive menstrual bleeding, pelvic pressure, bowel dysfunction, urinary frequency and urgency, low back pain, constipation, and painful intercourse (dyspareunia; De La Cruz and Buchanan 2017). Left untreated, fibroids can lead to increased risk of cesearean delivery, breech pregnancy, preterm deliveries, postpartum hemorrhage for women who do become pregnant, and infertility (Carranza-Mamane et al. 2015). Treatment for fibroids can range from noninvasive interventions (e.g., hormonal contraceptives, nonsteroidal anti-inflammatory medications) to invasive surgical interventions (Hirokawa et al. 2020; Lethaby, Vollenhoven, and Sowter 2002; Savard and Brown 2022; Sayed et al. 2011). Surgical treatments include myoectomy, where fibroids are removed and the uterus remains intact, or hysterectomy, where the uterus is removed, providing a definitive cure but leaving women infertile (Chen et al. 2020; Manyonda et al. 2020; Wallace et al. 2020).
Up to 80% of Black women will experience fibroids, and they are disproportionately more likely to suffer earlier, more often, and with greater symptom severity compared to women of other racial groups (Eltoukhi et al. 2014; Hellwege et al. 2017; Stewart et al. 2013; VanNoy et al. 2021). They are also at greater risk of having aggressive invasive treatment procedures, including myomectomies and hysterectomies (Marsh et al. 2018). Little evidence supports differential genetic predisposition to risk of fibroids development in Black women. Instead, evidence points toward interactions between behavioral and social correlates and epigenetic alterations (i.e., gene expression) elevating fibroid onset risk and severity (Charifson et al. 2022; Katon, Plowden, and Marsh 2023).
Other correlates to fibroids include high body mass index, vitamin D deficiency, exercise, nutrition, smoking, contraceptive use, and high cholesterol (Al-Hendy, Myers, and Stewart 2017). However, evidence linking fibroids to behaviors, such as nutrition, alcohol use, caffeine, and tobacco use, among Black women is inconclusive (Wise et al. 2004, 2013, 2014). Markedly less research has examined possible social and structural factors linked to uterine fibroid risk, particularly among Black women. Qualitative research about Black women with uterine fibroids indicates detrimental financial costs and psychosocial burdens associated with symptoms, including emotional distress and feelings of helplessness (Dykstra et al. 2023; Ghant et al. 2015; Orellana et al. 2022; Sengoba et al. 2017). Black women also report inequitable medical experiences, including difficulty obtaining timely diagnosis and treatment, negative treatment experiences with medical practitioners, and less satisfaction with recovery from treatments (Sengoba et al. 2017; VanNoy et al. 2021). The disruptions of uterine fibroids can also increase the likelihood of missing work and reduced work productivity (Lerner et al. 2008; Marsh et al. 2018; Stewart et al. 2013). However, there are limited insights regarding the ways in which highly successful Black women experience, cope with, and navigate symptomatic fibroids.
Superwoman Schema and Black Women’s Health: A Conceptual Model
Existing literature on the experiences of faculty of color in higher education suggests that higher education institutions often create significant stress that can have deleterious health implications (Zambrana 2018). Although analyses of underrepresented faculty members’ job stress and health outcomes exists (Zambrana 2018), research on Black women is limited. Black women report more difficult pathways to tenure and less mentoring and support and also encounter racism and sexism in their roles (Cobb-Roberts et al. 2017; Kelly and Winkle-Wagner 2017; Zambrana 2018). We use the superwoman schema (SWS) framework as our conceptual model for understanding how Black women faculty actively navigate and cope in the presence of racialized and gendered stressors.
Black women faculty experience marginalization, cultural taxation, and stereotyped perceptions of the “angry black woman” (Davis and Brown 2017) while also being expected to be a superwoman who is strong at all costs (Beauboeuf-Lafontant 2009). In this context, Black women seek to potentially excel as a form of active coping despite the potential health costs. A growing literature demonstrates that Black women, even at higher socioeconomic levels, remain at greater risk for poor health indicators, such as high allostatic load (i.e., wear and tear on the body; Richardson, Goodwin, and Hummer 2021), and outcomes, including preterm births (Fishman et al. 2021) and cardiovascular disease risk (Walsemann et al. 2016). Consequently, in-depth and intersectional analyses of unique simultaneous racial-ethnic, class-based, and gendered experiences of specific reproductive morbidities are needed (VanNoy et al. 2021). We extend the concept of SWS to understand how high-achieving Black women navigate the pressure of the academic tenure track in the presence of symptomatic fibroids, including experiences with fibroids diagnoses, treatments, and daily encounters with symptom management.
Created by Woods-Giscombé (2010), the SWS provides a culturally relevant empirical assessment of the mechanistic pathways linking stress and health, specifically among Black women. Woods-Giscombé (2010) found that Black women, particularly those who were highly educated, reported excessive work habits, having to postpone their medical care, and feelings of fatigue that they knew were consequential for their health. Although the SWS is a form of active coping, it can be physically and emotionally costly (Beauboeuf-Lafontant 2009; Woods-Giscombé 2010). Alhough high endorsement of SWS on some dimensions in the presence of stressors, such as discrimination, may be protective (Allen et al. 2019), high endorsement was also associated with depression, anxiety, and binge eating (Beauboeuf-Lafontant 2009; Liao, Wei, and Yin 2020; Nelson et al. 2024). Furthermore, high endorsement of certain dimensions was associated with poor sleep (McLaurin-Jones et al. 2021), hypertension risk (Perez et al. 2023), and for high-income women, poorer self-rated health (Erving et al. 2024). In this study, we applied the conceptual connection between health, psychological stressors, and SWS in our research design and analysis by employing the scale in our survey and to guide our qualitative questions and analysis (Woods-Giscombé 2018; Woods-Giscombé et al. 2016).
Data and Methods
Data and Participants
Data were from a national mixed-methods study of tenure-track Black women faculty in the social sciences and included three surveys and two rounds of in-depth interviews between 2020 and 2021. The study aim was to examine whether and how racial and gendered stress within institutions of higher education were linked to Black women academics’ health outcomes. After obtaining institutional review board approval (Study No. 2020-0708), participants were recruited via social media and social science organization listservs. Participants were faculty who identified as female and Black and were employed in tenure line positions at degree-granting institutions in the social sciences. Eligible participants completed three online surveys that included health measures (Survey 1; N = 160); active coping as measured by SWS Scale, job support, and racial stress (Survey 2; N = 105); and social support and health behaviors (Survey 3; N = 102). Surveys were administered approximately one to two months apart to reduce participant burden. Overall attrition between Survey 1 and Survey 3 was 36.3%. Table 1 reports select demographic characteristics of the current analytic sample, restricted to participants who completed Surveys 1 and 2.
Demographic Characteristics of Fibroids versus Non-fibroids Survey Participants.
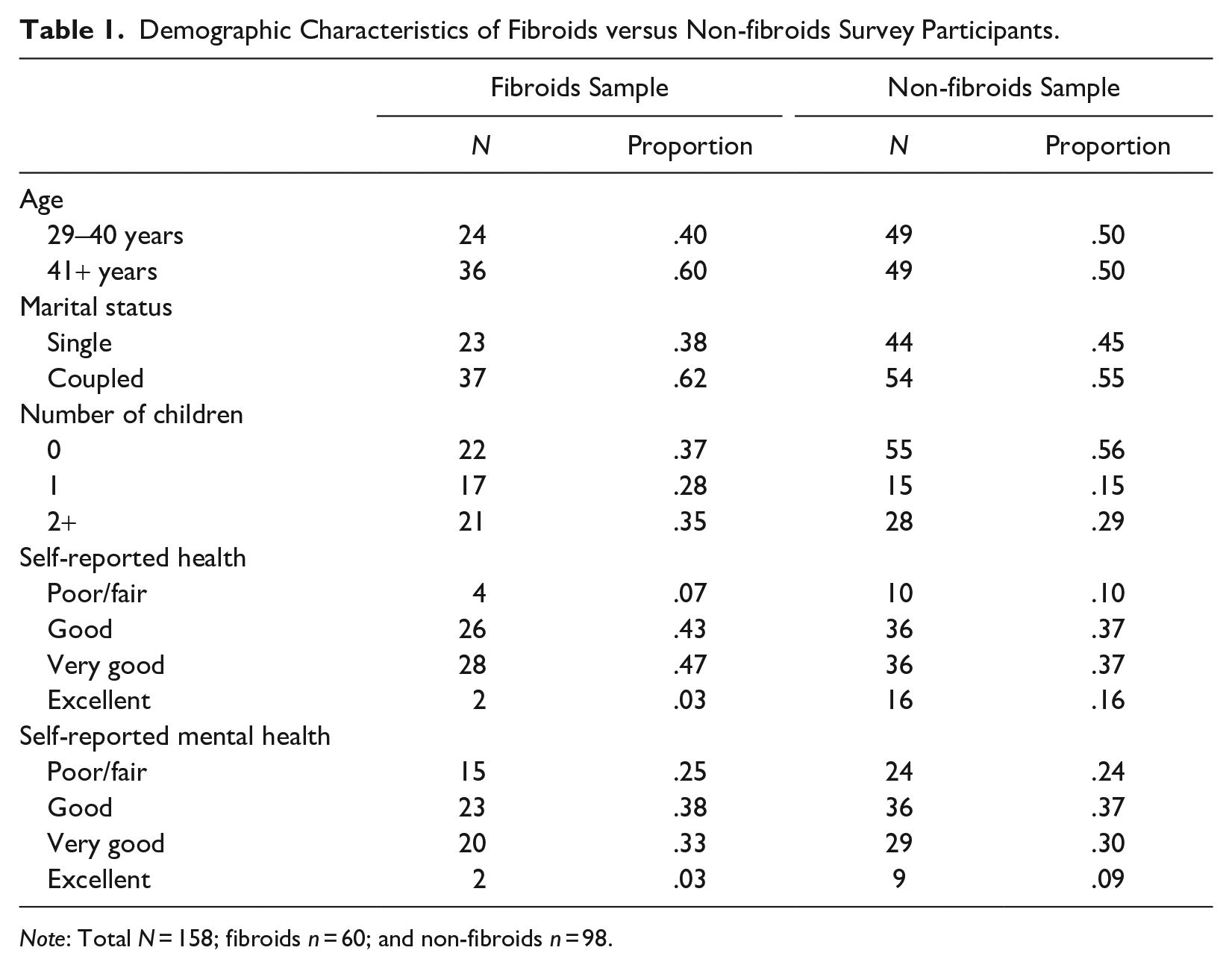
Note: Total N = 158; fibroids n = 60; and non-fibroids n = 98.
Upon completing Survey 1, participants were invited to participate in two rounds of in-depth interviews via Zoom. Sixty-three faculty completed Round 1 interviews, and 48 participants completed Round 2 interviews, for a total of 111 interviews. Participants were provided copies of their transcripts in a data validation process of member checking (Carspecken 1996). The current study focused on responses collected in the first interview, in which participants were asked about the chronic health conditions they listed in their survey, how they were diagnosed, and whether those conditions related to their jobs and stress as faculty members. All participants selected a pseudonym and were de-identified in data reporting.
Methods and Analytic Strategies
The study employed a parallel convergent mixed-methods design in which survey data and in-depth interviews were collected concurrently, with findings from quantitative and qualitative analyses mutually informing each other (Creswell and Zhang 2009). In the current study, descriptive results are reported from the survey with a focus on variables that emerged thematically in the in-depth interviews.
Key Survey Measures
Fibroids diagnosis
Participants were asked to identify conditions that they have ever been diagnosed with, including uterine fibroids, in Survey 1. Specifically, participants were asked if they “have ever been diagnosed with uterine fibroids?” Those who endorsed the conditions were coded as 1 for having fibroids and 0 if they did not.
SWS
SWS, conceptualized as a form of active coping, was measured using data from Woods-Giscombé’s (2010) scale to understand whether Black women academics perceived a need to act as superwomen in their faculty careers. The SWS is composed of 35 items, separated into five subscales: (1) obligation to present an image of strength, (2) obligation to suppress emotions, (3) resistance to being vulnerable, (4) intense motivation to succeed despite limited resources, and (5) obligation to help others (Woods-Giscombé 2010). Our preliminary analysis of the qualitative interviews led us to focus on the image of strength and intense motivation to succeed despite limited resources subscales for the descriptive survey analysis, based on the thematic findings of the qualitative data. For this study, the limited resources were operationalized as the available time and energy required to seek or receive treatment for their condition. Time use disparities is an often neglected factor shaping racial health inequities in which Black women may have less time available to engage in health-protective behaviors such as seeking medical treatment or exercise (Colen et al. 2024). The inability to engage in such behaviors also diminishes energetic resources with deleterious implications for ongoing health and productivity.
Demographic variables reported here (Table 1) included participant’s age, marital status, number of children, self-reported health, and self-reported mental health. Additional analyses are available on request.
Interviews
All qualitative data were initially coded in Dedoose coding software using a codebook that allowed for categories to emerge. Once all the data were analyzed, we ran a query for all data that had been coded as uterine fibroids and/or SWS. With these data, a second analysis was conducted in which we coded data in small sections, allowing themes to emerge. We continued the second round of coding until data were saturated (repeated) under the themes. We engaged in negative case analysis (Carspecken 1996) in which we sought out data that conflicted with the findings reported in the following to analyze them and consider why they conflicted. Descriptive results were compared to the qualitative coding for correspondence and dialogue between the two types of data (McChesney and Aldridge 2019). There were some participants who endorsed having fibroids in the survey that did not discuss symptoms. We do not know whether those who chose not to discuss symptoms were without symptoms or if they were symptomatic and opted not to share the details during interviews.
Weekly research team meetings were conducted to discuss analysis, a peer-reviewing validation technique (Carspecken 1996). A common trustworthiness practice in qualitative research is to contemplate the positionality of researchers in gaining/maintaining participant trust. We discussed the positionality of the team of graduate students and faculty at weekly meetings relative to trust building with participants and related to the interpretation of data. The research team was comprised of Black women, a White woman, and a multiracial woman. Participants were informed of the identities of the researchers (e.g., student/faculty, race, gender) before the interview.
Results
Descriptive Survey Statistics
Table 1 reports select characteristics of the fibroids- versus nonfibroids-endorsing participants in the full survey sample, and Table 2 reports the same characteristics of the interview subsample who endorsed having fibroids in the survey. In the full sample, those endorsing fibroids (40% of the sample) ranged between 29 and 40 years old, and the remainder were above 41. Most participants reported having partners (≈62%), and 63% had children. Overall, both samples reported good to excellent self-rated health (93% fibroids; 88% nonfibroids); however, approximately 25% of both samples reported poor self-rated mental health. In Table 2, the patterns of descriptive characteristics were similar in the interview subsample that endorsed having fibroids.
Demographic Characteristics of the Interview Sample.
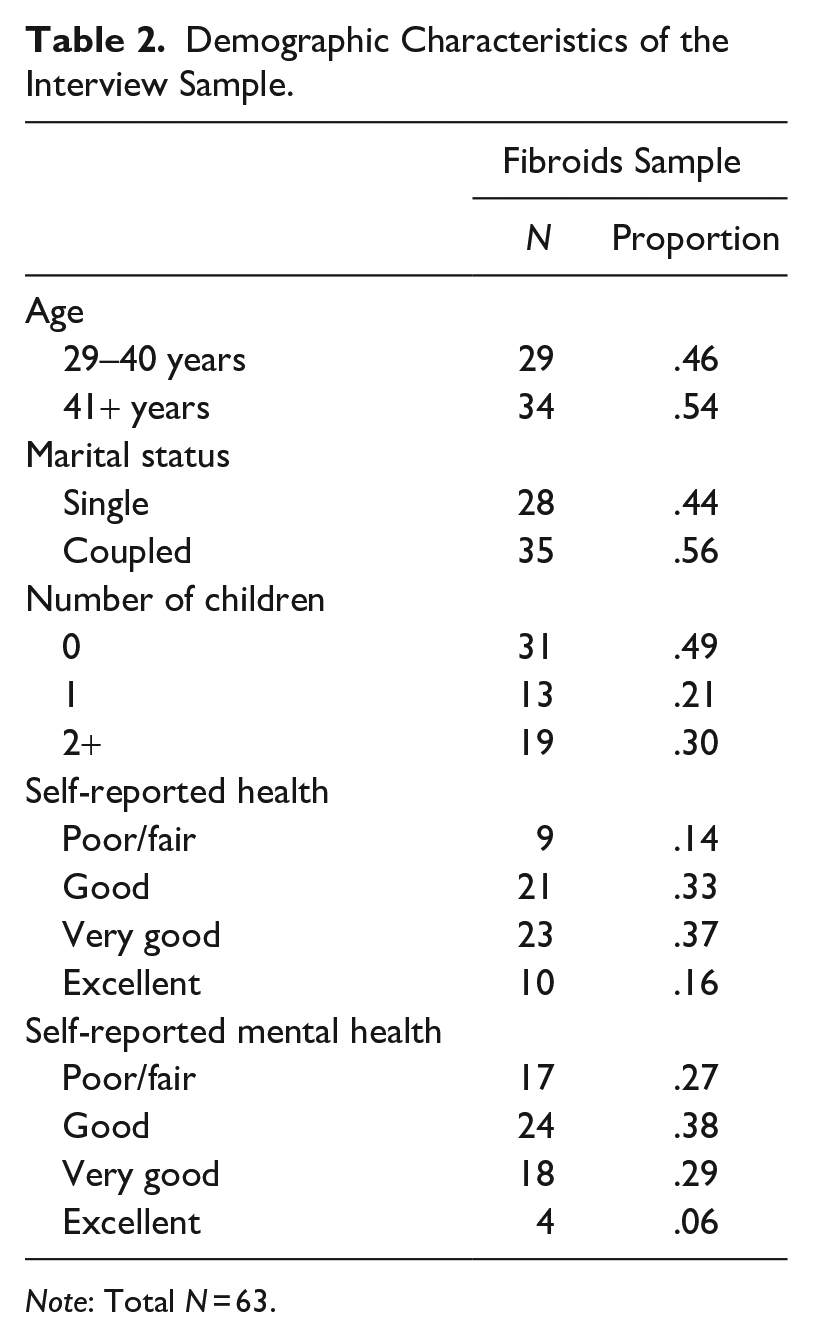
Note: Total N = 63.
Figure 1 reports the descriptive patterns of women who completed the SWS survey questions, broken down into fibroids versus no-fibroids categories, where 40.8% endorsed a fibroids diagnosis. Approximately 67% of participants completed the SWS scale in Survey 2 (N = 103). Of the 42 respondents with fibroids who completed Survey 2, the majority (37 out of 42, or 88.1%) indicated the need to demonstrate strength (moderate or higher) on the SWS Scale. Similarly, most women who did not have a fibroids diagnosis also endorsed moderate or high levels of the obligation to exhibit strength (51 out of 61, or 83.6%). The results are similar when examining the motivation to succeed subscale—of the 42 respondents with fibroids, 39 (92.9%) scored within the moderate or high categories on the motivation to succeed despite limited resources. For the nonfibroids sample, 52 out of 61 (83.9%) respondents scored within the moderate or high categories for the motivation to succeed subscale.
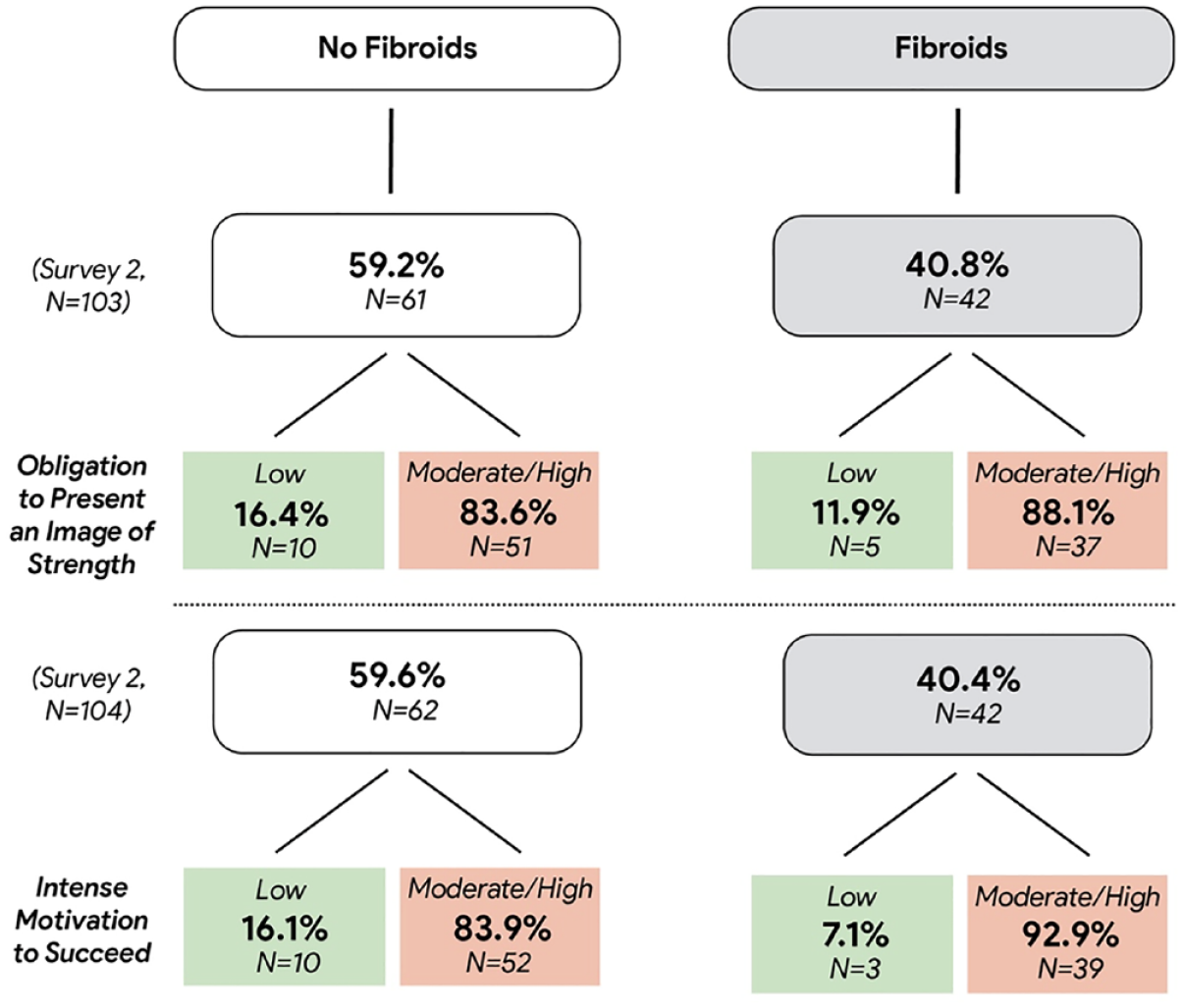
Fibroids and Superwoman Schema Descriptive Statistics.
Significance tests found no statistically significant group differences between the fibroids and nonfibroids samples for endorsement of SWS. Coupled with a smaller overall sample size, this lack of variation is likely the result of high endorsement of SWS across respondents in the study rather than within-group differences by fibroids diagnosis. For women with fibroids, we turned to in-depth interviews to examine their experiences with symptomatic fibroids embedded in the context of the tenure track.
Qualitative Findings
Of the 60 women who endorsed fibroids, 28 of them elected to participate in interviews (≈47.7% of the fibroids sample). Two claims emerged from qualitative data analysis: (1) Faculty job stress related to and possibly exacerbated chronic reproductive health conditions such as uterine fibroids, and (2) pain and suffering were a normalized part of Black women’s faculty experiences, and productivity had to continue regardless of the pain. The following qualitative findings are a sampling of participants who represent typical (more than three participants) cases within the qualitative data.
Faculty Job Stress Exacerbates Reproductive Conditions
Barbara, a fully promoted professor at a private research university in the South, was diagnosed with fibroids on the tenure clock and reflected on her experience compared to other Black women: I think these jobs are stressful. With Black women, I saw a quote, the way we process, even if we are doing what we’re supposed to do, we still default to that we’re not doing enough. We feel like it’s a failure. I think our socialization says you constantly are supposed to do [more]. So, you don’t know when to stop, or you don’t know how to amount to 40, 40, 20 [laughs].
Barbara contemplated the normalized overworking that was expected in the academy more generally—but then underscored ways that Black women specifically perceived a need to do more. In endorsing the superwoman dimension intense motivation to succeed (Allen et al. 2019), she noted the workload, which requires time and energy, often exceeded the typical research institution faculty load of 40% research, 40% teaching, and 20% service. She characterized the job as stressful and overworking as a response to this pressure.
Tonja, an assistant professor at a flagship university in the mid-South, described being diagnosed with uterine fibroids during her doctoral program: Many Black women have reproductive health issues and fibroids in particular. At first, my OBGYN said that she saw something, but I wasn’t having symptoms. She was like, “Well, if you’re not having symptoms, don’t worry about it.” But the level of stress that you undergo when you’re in a doctoral program and all of that can exacerbate stuff. Over time, I did start to have symptoms, which were just really long, heavy periods. I had to take iron supplements, and I did acupuncture. I tried to do all of the nonsurgical things first, and some of them helped for a little while. But nothing helped forever. That’s when I ended up getting the first of three surgeries total. The first surgery was noninvasive, and I was in and out in a day and back on my feet by the end of the day. That one didn’t help. And the second part of that didn’t help. And so that’s when I had to go have the more serious surgery.
After underlining the notable number of Black women who must endure uterine fibroids, Tonja made a direct connection between the stress of the academy, which began during her doctoral program, and the growth of her own uterine fibroids. Fibroids can lead to serious iron deficiencies, so iron supplements are a typical early treatment. In Tonja’s case, she still needed multiple surgeries and sustained years of pain while she simultaneously worked toward tenure.
Isabel, an assistant professor at a state university in the South, started by pointing out her stress levels and being overworked before identifying her numerous health conditions—acid reflux, gastroesophageal reflux disease, and fibroids—all of which she encountered after entering her role as a faculty member: I’ve been so overworked. Maybe it’s all related, I think this is one of the reasons why I want to leave too. I think it’s the unhealthiness of the job. I just need to find a different scenario because I need to be a healthier person. I also have fibroids. Who doesn’t have them? [laughs] But I feel like it’s linked. Just because of the timing. I feel the stress of this job has been really hard. So that was part of wanting to move on as well. Like a new working environment. One that’s a little healthier.
Isabel related her health conditions, including fibroids, to some of the stress she encountered in her position in academia and cited her health as a main reason to search for new roles. Although faculty roles might be normatively difficult for all faculty, with uterine fibroids, it is likely that Isabel’s time and energy were limited resources as she dealt with chronic pain and bleeding. The way she described fibroids, almost as an afterthought while also suggesting that most people have them, was normalizing—as if it is so common for Black women to have fibroids that it was almost not worth mentioning them in relation to her other comorbidities.
Summer, an associate professor at a state university in the Southwest, noted that she did not have to manage chronic health conditions before becoming an academic, saying that her health conditions activated earlier because of stress: The one unknown condition that I did contend with that neither our parents had, including my mom, was I have fibroids. But fibroids are very common for Black women. It causes a lot of pain. So again, I don’t know, it’s hard to say the stress from the academy caused this or not, I would think there’s some probable overlap with the fibroids.
The question still hung in the air for Summer as to whether the stress of being an academic exacerbated her fibroid diagnosis, but it was one condition that was not in her familial health history.
Chronic conditions started for Emily, an assistant professor at a flagship state university in the Northeast, during her doctoral program. She recalled her multiple conditions, such as endometriosis, chronic fatigue, and multiple sclerosis, noting: I also had uterine fibroids. I’ve had two surgeries. I think with the last surgery, there was so much ovarian tissue and stuff removed that it pushed me into an early menopause. I don’t really have like a cycle anymore. I don’t have the same kind of painful monthly cycles, so it kind of did get better. But it got worse in the sense that I shouldn’t have started menopause at 38. I think it switched from one bad thing to something that was equally bad, but not as painful. Or painful in a different way. Because then I had to deal with infertility issues. Those are just the kind of things that I’ve just had to learn to deal with. Some periods are better than others, but sometimes it will be frustrating. But I think over the course of the years, things have gotten better in terms of me having to accept it.
Emily had multiple chronic conditions that compounded together to cause significant pain, infertility, and multiple surgeries during her tenure-track position. Her normalization of her experience concurred with the persistent theme of accepting pain and suffering as part of the Black woman faculty experience, as elaborated on in the next theme.
Normalized Reproductive Pain and Suffering in Faculty Roles
Mildred, an associate professor at a public historically Black university in the South, reflected on ways that Black women were often silenced in conversations about their reproductive health in her generation. She offered advice during her interview with a Black graduate research assistant, pointing out how long she waited to have her fibroid surgery: With Black women, why is it that we all have fibroids? As a Black woman who’s been through both, both of those things, we just go through the pain, we just work through. We work. We work through the pain. My gynecologist, he’s a Black man. He’s like, “Any other woman would have been stretched out on the floor with what you got going on, but no. You got shit to do. We should’ve taken care of this a long time ago. But no, you got shit to do.” I’m like, “Dude, I do have shit to do.”
Mildred did finally get her fibroid surgery after a decade of putting it off while she climbed the ranks as a faculty member. She considered, “Once we got the surgery done, it was like, why did I wait 10 years to do this?” Mildred had already answered her question—she had delayed her fibroid surgery so that she could continue to work in her faculty position, a sign of endorsing the superwoman coping concept of determination to succeed amid the limited resource of time (e.g., needing to put time toward work instead of surgery) and energy (e.g., not feeling as if energy could be put toward recovering from surgery).
Sasha, an assistant professor at a midsized public university in the Northeast, remembered her long journey toward finally getting her fibroid pain diagnosed and treated: All of a sudden, I started having really heavy periods. They found out I have fibroids. So now they’re talking about doing a hysterectomy. I put it off last year. We talked about this a year ago. [My surgeon] was like, “You were here a year ago and we talked about doing the surgery and then we didn’t see you again.” And I’m like, “Yeah, I didn’t have time.” I didn’t have time to have a hysterectomy.
Knowing that a hysterectomy is a lengthy recovery, after she entered a tenure-track position as a new faculty member, Sasha inquired how long she would need to step away from work: You’re going to need at least six weeks to recover. And I said, “Girl, boo, I think it’s a same day surgery. [laughs] I’ll be back next week.” She was like, “No.” So I started asking people who’ve had a hysterectomy. They’re like, “No, you’re going to need like six weeks to heal.” I thought, well, I don’t have six weeks. So, I just did not do it. Now I have it scheduled; I’m going to do it. But I put it off for a long time.
The lack of time for a hysterectomy and the lack of energy to put toward recovering from surgery were normalized for Sasha, as if she had internalized putting all her time and energy toward her work instead of her own care. She also admitted to returning to work six days after the vaginal birth of her daughter and two weeks after the C-section birth of her son, signifying a coping mechanism of needing to exhibit strength and a determination to succeed despite limited resources even if success came at the expense of her health.
Sasha finally opted to get the hysterectomy that she needed to remedy the pain and low iron caused by her fibroids. She contemplated what helped her make the decision: I need this hysterectomy. I need to take care of me. I’ve been putting it off too long, especially because I didn’t want to be off work. Now I’m thinking we’re at home anyway. And we’re teaching online. So I could probably still take a couple weeks off and then resume my classes back up like online. I’ll be okay. I won’t be driving or anything.
Although Sasha had been repeatedly advised to take six weeks to recover from her hysterectomy, even at the time of our interview, she anticipated returning to work online after only two weeks. In part, her decision to only allow one-third of the recommended time to recover was connected to her prior history of normalizing pain and lack of recovery time after the births of her two children. Her willingness to finally get a hysterectomy was also assisted by the context of the COVID-19 pandemic, where she associated the flexibility of working from home with being able to recover even though such efforts still fall outside of the terms of routine recoveries.
When asked about chronic health conditions that she endured, Pearl, an associate professor at a flagship research university in the Midwest, identified, “Hysterectomy and insomnia. Those are the two.” She then described her process of treating her fibroids: I was diagnosed with fibroids when I was 23. It was just the kind of, let’s wait and see, wait and see. Usually when you hear about Black women having fibroids, you think, oh, like, they just get really huge. Mine weren’t huge. I just had a bunch of small ones. I just had many of them. So they just said, “We’ll watch, we’ll watch, we’ll watch.”
The wait for treatment on her fibroids did not last as the fibroids continued to grow: It got to a point that I had very painful periods. Extremely painful. That also felt like torture. When you’re in graduate school, you can manage, I could get out of going to stuff. But when you’re having a career and you have to teach, you have to get up and teach in front of 300 students, I can’t say “I can’t teach because I have cramps.” It was getting really bad. I felt like I couldn’t do my job. So, I went to my doctor and I was like, “I need intervention on this.” We started with different kinds of hormonal therapy. I didn’t want to take birth control because of the family history of breast cancer. But I said I need to do something, I can’t do my job. I’m not going to get tenure [laughs] with this.
Pearl continued, describing attempts to manage the pain: I started different kinds of hormonal therapies, and they weren’t working. I was just getting sick. And my doctor eventually, after a year, she’s like, I think you need to see a surgeon. [The surgeon] looked at my ultrasound [and said], “We need to talk about surgical intervention. You’re not even a candidate for myomectomy because you have so many. It’s like, a blueberry muffin. It’s really hard to remove blueberries from [the uterus]. They’re just baked in there. Some of them are attached. We have to talk about hysterectomy.” In 2019, I went on medical leave, and I had a hysterectomy. I had my uterus, cervix, and fallopian tubes removed, and I was 35 years old. I didn’t ask for a leave for that. I just went on medical leave.
When asked if anyone at her institution knew what she was navigating with her fibroids and surgery, she responded: I told my mentor. I have two mentors. One is a man [laughs]. I was not going to him. Another is an older White woman who [is] very institutionally connected and knowledgeable, and I like her very much. So, I went to her. And to be honest, I was planning to try to schedule that surgery for the day after my last day of teaching so I could use the Christmas break, which was three weeks, to recover and be back. She [my mentor] said, “Absolutely not!” She’s like, “You need to do this surgery now. You’re going on medical leave. If anyone gives you any problems, I’ll deal with them.”
Pearl’s mentor strongly encouraged her to seek treatment for her fibroids immediately rather than waiting for the holidays, saying that she would take on any repercussions—confidence that perhaps came from being more institutionally prominent alongside the privileges of Whiteness. When she was asked how she was feeling postsurgery, Pearl exclaimed: Great. I’m so glad I did it. It was the right decision for me. I think I had gotten to the point where I had decided I didn’t want to have children. But I also didn’t want the option taken away from me either. It was really hard. I think I took two months to decide. I worried about future regret. But you know, when I look back, that’s not living. My period controlled my life. I couldn’t plan things around it. I couldn’t plan research trips around it. I couldn’t go to dinner. I wasn’t living, and I was in a lot of pain. It was the right decision. I don’t have any bad side effects. I feel great. I feel fine. In fact, a lot of my friends are jealous [laughs]. I feel good.
Pearl recognized how before seeking necessary treatment for her fibroids, her regular life had been hampered by pain. She reflected on the path toward caring for her health and summarized, “I’m getting there. I’m getting there.” Although Pearl questioned how normal it seemed for Black women to have fibroids and live in pain, she had still struggled considerably to make time for the surgery she needed. But she confessed, “That was really hard to manage, the demands of my career with the pain, the bleeding, the management. That was really hard. So that’s not an issue anymore.” When Pearl was having years of symptomatic fibroids, such as bleeding and pain, her time and energy would have been very limited, and yet she perceived the pressure to always choose to put her time and energy toward her career at the expense of her health, in this case, recovering from necessary fibroid surgery. This was a clear indication of determination to success despite her limited resources.
During a conversation about what it was like to be faculty, Terri-Ann, an assistant professor in a state system university in the West, discussed her diagnosis of fibroids and endometriosis similarly, almost as if it was just a difficult but normative part of the work life of Black women faculty: [I have] fibroids and endometriosis and things of that sort. I’ve been diagnosed for several years now. I’m grateful that I had my last surgery in February. And then the pandemic hit in March. So that worked out really well. Because the amount of pain and sort of debilitation that occurs, just with my fibroids and endometriosis, and like the cycle and all of that. It really takes a lot out of me. To have to have that in addition to the pandemic, like just would have been chaotic for me. It worked out really well that like, I had surgery in February. And that helped significantly with pain and just sort of like, symptoms. I’m not sure how I would have dealt with it if I had to deal with all of that.
While Terri-Ann described the time and energy that it took to deal with her reproductive health conditions, particularly debilitating pain, the way that she mentioned the diagnosis in conversation highlighted how it was a seemingly routine part of faculty life for Black women. Additionally, without the pandemic, Terri-Ann would have had to navigate in-person teaching and meetings almost immediately after surgery. It was only because of the pandemic that she was able to recover fully at home.
Alisha, an associate professor in the Northeast, began dealing with chronic reproductive health conditions during her graduate program with a diagnosis for endometriosis. The medication to treat endometriosis (Seasonique) made her fibroids grow bigger. She recalled: I had this OBGYN, he was this old White man, he was like, “Well, you got endometriosis, you have got to have a hysterectomy.” And I was like, “No, sir. I’m in my mid-20s. Not gonna do that.” He said, “Well, that’s the only way to fix it.” I don’t care what MDs say. I’m an epidemiologist. I know way better than they do. MDs don’t do what epidemiologists tell them to do. I decided I wasn’t having the hysterectomy. I was going to take Seasonique because the only thing, the only time I feel in pain from endometriosis is when I menstruate.
When we asked Alisha how she learned about her fibroids, she continued to voice frustration at doctors who would not listen to her. At the time of the interview, Alisha had recently started recovering from fibroid surgery to try to deal with the fibroid pain. Her newly found doctor had a very different approach from her initial White doctor who wanted her to have a hysterectomy. By the time Alisha found a doctor who would properly diagnose her fibroids, the pain and bleeding had become intolerable, and Alisha was ready to get the hysterectomy. However, the new doctor’s second opinion after diagnosing the fibroids was fibroid surgery, a decision Alisha accepted: “I had to have the fibroids removed two months ago. But since I had those fibroids removed, I’ve had the lightest menstrual cycles. I haven’t had to take any medication. It’s great.” We asked Alisha if she told her colleagues on campus about her myomectomy surgery. She responded: Oh, I told everybody. If you hear somebody complaining about these symptoms, you need to be able to tell them this is what it is. I have pictures on my phone. I’m like, “Look at the fibroids they took out of me!” I had my surgeon take pictures because I wanted to see what they looked like in the uterus. Then she lined them up on one of the surgical towels, and she took a picture of them lined up on the surgical towels. And then took a picture of them on the weight, like on the scale. I wanted to see it all. I kept showing people. And I looked like I was five months pregnant. They’re just these random fibroids sitting in my uterus. My doctor said there was more fibroid than there was uterus. I just thought everybody should see what that looks like [laughs].
As a scholar who studied medicine herself, Alisha found it very important to tell other Black women about her fibroids experience to protect others from waiting as long as she did to get a diagnosis and surgery. Alisha may have been pushing back on the idea that one must be determined to succeed at the expense of health and well-being.
After surgery, Alisha did continue to have chronic reproductive pain from her endometriosis, but it was perhaps more manageable. She described how she continued to survive the pain of those symptoms while navigating her scholarly career: It hasn’t necessarily impacted my productivity. Sometimes, if I can’t sit up straight because it hurts, I just, I can back out a little. I call it my napping couch, my office couch. I just lay back, and I can work right there. I don’t have to sit straight up to work, especially without my computer equipment.
Even after diagnoses and surgery for fibroids, Alisha normalized her pain and suffering because the pressures to continue producing scholarship outweighed her personal consequences—meaning she found a way to persevere, but that way of surviving meant a determination to succeed despite very limited time/energy resources.
Discussion
As shown through the survey results, a nontrivial number of Black women faculty in this study reported a fibroids diagnosis (N = 60 out of 160; 38%). Although the diagnosis of fibroids is all too common for Black women according to prior research (Eltoukhi et al. 2014; Hellwege et al. 2017; Stewart et al. 2013), there is little scholarship examining how symptomatic fibroids influence Black women’s daily lives and careers. The prior research that connects health outcomes and the work stress of faculty of color (Zambrana 2018) does not focus on Black women or on fibroids specifically. Our qualitative findings with Black women academics, who represent a group of highly educated and successful Black women, provide new insights illustrating how Black women connect career stress to their fibroids diagnosis and how they cope with the pain and disruption of their condition.
Across women who endorsed fibroids and those who did not in the survey component, there was moderate to high endorsement of SWS dimensions of motivation to present an image of strength and motivation to succeed despite limited resources. Limited resources were operationalized as time and energy, which we posit are some of the most important and limited resources for these women, and here, the participants had to balance decisions about their health alongside the pressures and expectations of being on the tenure track. Colen et al. (2024) argue that racial inequities in time use is a critical fundamental factor that shapes inequitable health between Black and White Americans. Specifically, they note that due to structural racism, Black Americans have less “health opportunity time” to engage in health-protective behaviors, such as seeking out medical care for health conditions and obtaining quality treatment (Colen et al. 2024). In this study, some participants noted in interviews that pressure and job demands led to forgoing treatment for serious health-related concerns, thus impacting their energy levels and overall well-being.
The descriptive survey data suggested that the majority of Black women academics with fibroids endorsed moderate and/or high levels of feeling an intense determination to succeed (92.9%) and an obligation to exhibit strength (88.1%). Our study results showed that engaging in high endorsement of SWS is costly for Black women’s health and illustrated how such costs can be manifested. Recent scholarship by Erving et al. (2024) found that higher income Black women who strongly endorsed SWS reported worse health than their lower income counterparts. These results provide more evidence that high status attainment may not confer health-protective opportunities for Black women given their occupation of two marginalized identities, Black and female, but, instead, diminishing returns for high achievement (Erving et al. 2024). Specifically, in the presence of inequitable treatment, they remain at disproportionate risk for morbidities, including reproductive health outcomes (Colen et al. 2018; Rosenthal and Lobel 2011).
The culture of academia is highly demanding, with gendered distinctions in work demands placed on women within and outside of the job, including navigating the intensive demands of academic production while also engaging in household and caregiving demands with implications for fertility timing (Pirtle 2018; Wolfinger, Mason, and Goulden 2009). Although such decisions are common burdens for female faculty members, who frequently must negotiate the timing of fertility-related decisions such as pregnancy with the demands of academia (Ward and Wolf-Wendel 2004), Black women faculty with symptomatic, diagnosed uterine fibroids must additionally contend with the timing of these decisions with the awareness that delaying interventions may result in infertility in the most severe cases. Because Black women are disproportionately more likely to suffer from symptomatic fibroids and at earlier ages and are obligated to take on more caregiving work for immediate and extended family members (Erving, Patterson, and Boone 2021), they may bear more stress and burden than is typical on the tenure track when coupled with the unrecognized labor that they may also engage in at work, such as mentoring and service obligations (Melaku and Beeman 2023).
In our qualitative interviews, some participants made connections between their diagnoses of fibroids and the stress of being a tenure-track faculty member without being primed to do so. Moreover, work stress was also cited as a reason for participants having little time or energy to manage their fibroid conditions in ways that would minimize pain and suffering. Those who had a symptomatic fibroid diagnosis described navigating the ongoing discomfort in ways that indicated a normalization of pain and suffering, with little time to seek care for the condition. Specifically, multiple women put off hysterectomies or other surgeries that may have helped to resolve their fibroids sooner due to work stress and demands.
Although the demands of the job were described by many Black women for delaying treatment and care, the specter of medical racism may also have been a contributing factor. Black women are disproportionately more likely to be given a hysterectomy as treatment for uterine fibroids, which leads to infertility (VanNoy et al. 2021). Although there is limited research on Black women’s experiences in the gynecological setting, a recent qualitative study guided by Black feminist theory illustrated that young adult Black women receiving gynecological care reported experiences of being ignored and having their intelligence insulted when having interactions with some White doctors, whereas those with racial concordance reported better experiences (Wade et al. 2023). The authors noted the importance of empowering Black women to engage in agency with their sexual health, a situation that also emerged in our study. One study participant stated that due to the aggressive treatment recommended by her White male doctor while in her mid-30s, she opted to delay care and ultimately received a second opinion that led to treatment that did not lead to infertility. Although her decision was temporally costly, leading to more symptom-related burdens, her willingness to opt out of care that she believed was not necessary or appropriate in her situation ultimately led to more appropriate, successful treatment later.
This study is not without limitations. Given the focus on in-depth analysis of Black women academics in the social sciences disciplines, we were not able to speak to generalizability (from the surveys) or transferability (from the interviews) to other disciplinary types (e.g., science, technology, engineering) or to other high-status occupations (e.g., medical doctors, lawyers). We captured experiences from survey/interviews at one moment in time and were not able to assess how Black women faculty members’ fibroid symptoms or relationships to being a superwoman might shift over time. A longitudinal examination would provide more insight. Although our emphasis here was on within-group differences among Black women, it could be useful to understand fibroid symptoms and careers across different racial-ethnic groups. Finally, in the interviews, although participants were asked about their general health, the discussion of fibroids was unsolicited. More research specifically focused on fibroids and other reproductive health-related morbidities that impact women in high-stress occupations is warranted.
With an explicit focus on a reproductive health condition disproportionately impacting Black women (i.e., uterine fibroids) in a population that is understudied, this study illustrates how women who occupy two marginalized statuses (Black, female) navigate a potentially life-disrupting health experience. SWS provides a conceptual foundation for understanding Black women’s active coping with gendered and racialized stress and the health costs that can be involved in such engagement. Despite the deeply scarring experiences of racism and sexism, Black women are still expected to perform with unflagging strength, which exacerbates morbidity burdens both psychologically and physically (Erving et al. 2021). In our study, participants embodied pain that may invoke a subtly different type of coping—when linked to concepts such as strength and determination to succeed, this might expand how mind–body connections in daily life are considered.
Future studies should examine psychological coping strategies, how they are employed, and the possible connections between coping and physical manifestations of health conditions. Longitudinal panel surveys, ethnographic fieldwork, and the inclusion of biological markers could be useful methodologies to understand these physical and embodied connections. The way in which Black women academics feel the need to consistently express strength and a desire to succeed could be weathering their bodies—and as their bodies experience wear and tear, the need to engage in high-stress coping could be further activated (Geronimus et al. 2006; Walsemann et al. 2016). Additional studies exploring how structural and environmental factors within institutions like college campuses either ease or exacerbate the need to engage in high-stress coping like the SWS process are needed, along with identifying factors that may mitigate such consequences. This study contributes to the growing body of literature elevating the need to illuminate the burdens that Black women bear even in the presence of “success,” the health costs associated with such achievement, and how existing occupational structures may exacerbate contemporaneous inequities Black women face across multiple dimensions of their lives.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Spencer Foundation Small Grant (#202000223), by grant P30AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging, by grant, P2CHD042849, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and support from the Wisconsin Alumni Research Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.