
Abstract
Sexual and gender minorities (SGMs) have experienced progressive change over the last 50 years. However, this group still reports worse health and health care experiences. An innovative survey instrument that applies stereotype threat to the health care setting, health care stereotype threat (HCST), offers a new avenue to examine these disparities. We harmonized two national probability data sets of SGMs—Generations and TransPop—capturing 503 gay men, 297 lesbians, 467 bisexuals, and 221 trans people. Using these data, we, first, explored how HCST’s association with self-rated health and psychological distress changed while considering more established constructs: discrimination and stigma. Second, we examined how HCST’s association varied across SGM groups. Results suggest that HCST is a unique predictor net of the associations with discrimination and stigma. Furthermore, results highlight the more consequential associations for trans people on well-being compared to gay men. We discuss implications of these findings for future research and potential interventions.
Keywords
Sexual and gender minorities (SGMs), including those who identify as lesbian, gay, bisexual, and transgender, report lower levels of health and well-being at every stage of life than their heterosexual, cisgender counterparts (Fredriksen-Goldsen and Muraco 2010; Smalley, Warren, and Barefoot 2016). Experts have largely pointed to daily discrimination and stigma as a primary source of these health disparities (Hatzenbuehler, Phelan, and Link 2013). Recent evidence, however, suggests that the way SGMs interface with the health care institution may also have a notable impact on health and well-being disparities (Aronson et al. 2013; Cruz 2014; Dickey et al. 2016; Fingerhut and Abdou 2017; Gessner et al. 2020).
The health care institution regulates who does and does not have access to high-quality care. Negative stereotyping of particular social groups has been shown to be important to health outcomes because it contributes to poorer access (Cruz 2014; Paine 2018) and poorer treatment (McNair, Hegarty, and Taft 2012; Poteat, German, and Kerrigan 2013) and has been linked to poorer health behaviors (Davis, Dewey, and Murphy 2016; Sabin, Riskind, and Nosek 2015). For instance, the presence or anticipation of racist stereotypes in the medical setting is associated with heightened anxiety (Abdou and Fingerhut 2014), increased distrust of medical providers, and increased likelihood of not disclosing important medical information (Thorpe, Iyiewuare, et al. 2022) for Black women.
A recently developed survey instrument (Abdou and Fingerhut 2014), health care stereotype threat (HCST), has been used to examine the role of the health care institution in shaping health disparities. HCST measures fear individuals specifically have about medical providers judging, evaluating, and diagnosing them differently due to negative stereotypes. HCST has been associated with negative psychological and physical health outcomes and health disparities among minority groups, especially groups differentiated based on race-ethnicity and age (Abdou 2017; Abdou et al. 2016; Abdou and Fingerhut 2014; Fingerhut and Abdou 2017). To date, only one study has evaluated the association between HCST and health disparities among SGMs. This study included a combined sample of sexual minorities (i.e., lesbian, gay, and bisexual individuals) and showed that HCST was positively associated with psychological distress and the number of bad physical health days (Fingerhut et al. 2022). Although this project provides an important foundation for understanding the role of the health care institution on health disparities facing SGMs, it is not clear whether the negative consequences of HCST persist even when accounting for everyday discrimination and stigma among SGMs or whether HCST differentially impacts the health of specific SGM groups.
The current project is the first to evaluate the specific impact of stereotype-based discrimination practices within the health care institution (using HCST) on the health and well-being of a national probability sample of multiple SGM groups. Specifically, we used a nationally representative, harmonized data set based on two studies—Generations and TransPop. This data set allows us to evaluate the association between HCST and two well-established measures of overall mental and overall physical health: self-rated health and psychological distress. The findings from this study provide initial evidence that suggests that targeted efforts to eliminate health disparities for SGMs should explicitly consider the role of HCST.
Background
Minority Stress Theory and Health Disparities among SGMs: The Role of Discrimination, Stigma, and Stereotype Threat
On average, SGMs report worse health outcomes compared to cisgender heterosexuals (Ahuja et al. 2015; Buchmueller and Carpenter 2010; Fredriksen-Goldsen and Muraco 2010; Herek and Garnets 2007; Hsieh and Shuster 2021; Meyer 1995, 2003). The primary framework used to explain why SGMs experience worse health than their heterosexual counterparts is minority stress theory. This classic theory was originally conceptualized by Brooks (1981) and suggests that stigma, discrimination, and prejudice experienced by SGM groups in everyday life increases the risk of a variety of health problems due to chronically elevated stress and exclusion from important social institutions and structures (Meyer 1995, 2003). SGMs report heightened rates of both stigma and discrimination throughout the life courses from adolescence into late life (Ahuja et al. 2015; Fredriksen-Goldsen et al. 2013), which is argued to contribute to higher depression and anxiety, increased suicidality, increased likelihood of smoking and binge drinking, and higher rates of substance abuse (Smalley et al. 2016).
Discrimination “is the unjust or prejudicial treatment of a category of people” (Goosby, Cheadle, and Mitchell 2018:320). Discrimination is often enacted through interpersonal means in which any number of status-based bigotry can be the driving factor. As Goosby et al. (2018) detail, discrimination is a form of social exclusion in which sections of our brain process these experiences as social pain. As they explain, the act of being socially excluded—and an individual’s acknowledgment of such acts—increases activity in the sympathetic nervous system as a stress response, which has physiological and psychological consequences. When the hypothalamus-pituitary-adrenal axis, the part of the brain that regulates the neuroendocrine responses to stress, is chronically activated due to everyday external exposures of discrimination, individuals experience increased risk of a range of health problems over time. For instance, chronic discrimination is related to increased cardiometabolic conditions and general cardiovascular wear and tear (Goosby et al. 2018).
Stigma related to SGMs is a belief system that positions LGBTQ identities as “denigrated, discredited, and socially constructed as invalid relative to heterosexuality” (Herek 2009:57). “Felt stigma” is different from “enacted stigma” because it is associated with an individual’s awareness and the negative psychological effects that accrue from their awareness that their identities are being scrutinized or attacked. We conceptualize stigma in our article based on this notion of felt stigma as the fear of enacted stigma (e.g., instances of discrimination; Scambler and Hopkins 1986). Similar to discrimination, stigma as defined in this way is also linked to social isolation and has been shown to disrupt interpersonal relationships (e.g., with medical providers) and engagement with social institutions (e.g., health care). These interpersonal relationship disruptions contribute to actual, perceived, and anticipated stigma (Hatzenbuehler et al. 2013).
Stereotype threat, which can co-occur with everyday discrimination and felt stigma, is also based on the tenets of minority stress theory, focusing specifically on situations when individuals anticipate being judged—based on fear and/or previous experiences—in terms of the characteristics of a group from which they belong (often based on race-ethnicity, age, or gender). Stereotype threat is measured as an internal fear that an individual will confirm negative stereotypes about their social group (Steele and Aronson 1996) without information about their actual personal merit (Inzlicht and Schmader 2012). Stereotype threat can lead to an erosion of one’s sense of identity and belonging and poorer overall functioning (Abdou 2017; Fingerhut and Abdou 2017; Thorpe, Tanner, and Hargons 2022).
Health Care Stereotype Threat
HCST is a novel application of stereotype threat applied specifically to the health care setting. HCST is (1) the fear of confirming negative stereotypes about one’s social group (e.g., one’s sexual orientation) and the fear that one’s social group status negatively influences how medical providers (2) judge, (3) evaluate, and (4) diagnose the patient (Abdou and Fingerhut 2014). HCST is influenced by individual (e.g., social statuses), interpersonal (e.g., patient-doctor relations), and structural (e.g., homophobia and transphobia) factors that are related to potential or actual/perceived experiences with the health care institution, all of which have been shown to be associated with health outcomes (Abdou and Fingerhut 2014; Fingerhut et al. 2022; Hatzenbuehler et al. 2013; Paine 2018). HCST has been shown to increase the likelihood of numerous adverse outcomes regarding well-being and health care experiences, such as increasing anxiety, poorer physical and mental health outcomes, increasing distrust of medical providers, and decreasing adherence to beneficial health behaviors (Abdou et al. 2016; Abdou and Fingerhut 2014). HCST was developed to better understand how this form of stereotype threat creates a barrier to utilization of health care services and contributes to health disparities in minority populations (Abdou and Fingerhut 2014). An example of HCST as a barrier to health care is how its anticipation made Black women more likely to withhold important medical information and their sexual identity and was associated with heightened feelings of being stigmatized (Thorpe, Iyiewuare, et al. 2022; Thorpe, Tanner, and Hargons 2022).
The application of stereotype threat in the context of the health care institution has potential to be especially important to understanding health disparities among SGMs because the success of health care treatments often requires individuals to trust and engage with health care experts. SGMs often need to discuss personal issues, such as sexual behaviors, STI treatment and prevention medications, and gender transition treatments, to receive medical advice, medications, or medical tests. If an individual feels that a health care provider is not listening to them or that they are basing their treatment on negative stereotypes, then they are less likely to seek out health care services (Cruz 2014; Petroll and Mosack 2011) and health care professionals are less likely to provide appropriate treatments (Martos et al. 2019; Paine 2018). Once trust is lost in the health care institution, individuals lose access to critical information they need to maintain their health and diagnosis care, and consequently, their avoidance of health care could lead to acute conditions becoming chronic (Willging et al. 2019) and lead to earlier onset of a variety of health conditions.
To date, there is only a single study that examines the influence HCST on the health of sexual minorities. Specifically, Fingerhut et al. (2022) showed that HCST was associated with worse outcomes for sexual minorities’ health based on psychological distress and overall number of bad physical health days. This research demonstrates that HCST is an important and potentially modifiable source of health disparities based on sexual minority status. However, no research has evaluated the role of HCST on transgender people’s well-being or evaluated differences across SGM groups to determine if consequences are more substantial for specific groups.
The Current Study
The current study builds on previous research by addressing two primary gaps: (a) isolating the specific association of HCST on health and well-being among SGMs, accounting for stigma and discrimination, and (b) evaluating variations by SGM groups in the health consequences of HCST. Furthermore, this is the first study to examine health associations with HCST in a study that includes trans people.
Regarding the first gap, minority stress theory argues that the persisting stress imposed by everyday discrimination and stigma is a key factor contributing to health disparities in SGMs. However, as noted previously, the health care institution has a unique role in influencing health outcomes in SGM groups. HCST is related to multiple aspects of the patient–provider relationship, such as increasing distrust (McNair et al. 2012), and SGMs’ beliefs that medical providers are culturally incompetent, prejudicial, or unable to make competent referrals for the care needed (Cruz 2014; Davis et al. 2016; Poteat et al. 2013; Sabin et al. 2015). Therefore, we hypothesize (a) that discrimination and stigma in everyday life will be independently associated with health and well-being outcomes and (b) that HCST will have a persisting negative association with health even when accounting for discrimination and stigma.
Regarding the second gap, we hypothesize that the consequences of HCST will vary by SGM group. Specifically, we hypothesize that transgender and bisexual individuals will experience greater health consequences in association with HCST than other sexual minority counterparts. This argument is based on the premise that these more vulnerable sexual minority groups have fewer resources and face more barriers to accessing resources, reducing their available resources to address the consequences of HCST. In addition, these vulnerable groups also are more likely to experience a higher everyday stress load, partially related to experiencing more structural forces of discrimination that reduce access to resources.
For instance, recent policies like the infamous “Bathroom Bill,” introduced originally in North Carolina and now appearing in other state agendas, explicitly discriminate against transgender individuals, increasing risks of harassment and violence in a variety of contexts (Liu and Wilkinson 2017). In addition, bisexuals, compared to gay men and lesbians, report significantly higher psychological distress (Bostwick et al. 2010; Ranji and Beamesderfer 2018), and this may be attributed to the fact that bisexuals have a heightened likelihood to hide their bisexuality (Brown 2019), which may explain why they also experience heighted levels of internalized heterosexism and biphobia in everyday life (Bostwick 2012). Furthermore, transgender individuals, because of other forces of discrimination, are less likely to have access to care. An astonishing 3 in 10 SGMs face difficulties accessing care as a result of costs, but cost is a reported barrier by an even higher proportion (more than half) of transgender people than other groups (Center for American Progress 2020). Once health care access is achieved, cisgender gay and lesbians are more likely to have doctors with experience providing treatment and care.
Among trans people who do receive health care, one-third report having to educate their doctors on transgender individuals to receive appropriate care (Center for American Progress 2020). Even if all sexual minorities had similar access to health care, these kinds of policies and social environments may accentuate the extent to which anticipating discrimination in a health care environment leads trans people and bisexuals to be more likely than other sexual minority groups to delay care (Cruz 2014; Poteat et al. 2013; Willging et al. 2019). That is, the burden of receiving the care they need is placed on these more vulnerable sexual minority groups, who are not only hesitant to use available health care services due to concerns about how they will be treated in health care environments but also less confident that their health care providers will have the skills or motivation to provide them with the needed care.
Finally, the consequences of HCST experienced by vulnerable sexual minorities are likely to be further accentuated by other structural barriers to health care, including reduced access to health-related lifestyles and health care environments equipped to support their long-term health and well-being. Trans people’s postponement of care is associated with lower likelihood of having health insurance or a primary place of care (Dickey et al. 2016), which has a variety of health consequences (Willging et al. 2019), including increased reliance on the emergency room for nonurgencies (Dickey et al. 2016). Across gender, trans men are especially likely to postpone medical care (Cruz 2014), and trans women report lower quality diets compared to other sexual minorities, which is correlated with higher psychological distress (Cohen et al. 2002). As a result of these collective factors, we hypothesize that bisexuals and trans people will report more significant consequences of HCST than other sexual minorities.
Relative to their more vulnerable sexual minority counterparts, gay men have experienced significant gains in social status and reduced levels of overall discrimination, which may be why gay men have the highest income and educational attainment across SGM groups. These outcomes have been argued to be a key source of upward mobility in work environments and, consequently, across a range of other social environments (Bauer, Clevenstine, and Macklin 2022; Pew Research Center 2013). Furthermore, in part because of their increased social standing and socioeconomic gains, gay men are more likely to have access to culturally competent health care providers (Brown 2019). For these reasons, in our study, we evaluate differences in the consequences of HCST on health across SGM groups by comparing all groups to gay men, who we anticipate, based on previous research, are likely to experience not only the lowest levels but also the fewest consequences of HCST on their health.
In summary, this study is designed to test two primary hypotheses:
Hypothesis 1: HCST will be independently associated with lower overall self-rated health and higher overall psychological distress even when accounting for the associations of everyday discrimination and stigma among SGMs.
Hypothesis 2: Bisexuals and trans people will be more vulnerable to the consequences of HCST on health and will show more significant declines in self-rated health in association with HCST and more significant increases in psychological distress in association with HCST relative to gay men.
Data And Methods
Data and Sample
To address these research questions and hypotheses, we harmonized two national probability samples (Generations and TransPop data sets) collected in 2017. The Generations study (www.generations-study.com) is the first of its kind to have longitudinal data on three generations of sexual minorities (i.e., gay men, lesbians, and bisexuals). Currently, there are three waves of the quantitative data available. TransPop (http://www.transpop.org/) is the sister study of the Generations study. There is one wave of TransPop, and these data are a national probability sample of transgender people in the United States. To harmonize these data, we used the first wave of Generations and merged it with the TransPop data. Next, we systematically matched variables in each data set to have all participants included on a single version of the variables of interest. We also applied a weight created by the data collectors to leverage these data’s probability sampling on the results.
These data were collected through Gallup, Inc., in two phases. The first used random-digit dialing (RDD) for both landlines and cellphone users. The RDD list was stratified to make the unweighted samples proportionate to the time zone and census region. Gallup created weights to mitigate effects of disproportionalities as a result of nonresponse and selection probabilities. In the second phase, SGMs were identified and invited to participate in the Generations and TransPop studies. These participants completed the survey either by mail or online.
The creators of Generations and TransPop imputed variables from other data sources when possible, which substantially decreased missingness (Krueger et al. 2020). For example, there was missingness on age, race, sex at birth, sexual identity, gender identity, and household income in these data that the researchers were able to pull from the Gallup sampling/screening survey used during phase one. To address our research questions, two samples from these data were required. First, to address Hypothesis 1, we solely utilized the first wave of the Generations data because the questions pertaining to stigma were not asked of trans people. The remaining research questions and hypotheses were explored with both first waves of data from Generations and TransPop. Individuals were excluded from the analyses if they had missing values on any of the variables of interest. The analytic sample for Hypothesis 1 was 1,267. The analytic sample for Hypothesis 2 was 1,488 (for descriptive statistics, see Table 1). The descriptive statistics in Table 1 and those presented in the “Measures” section are based on the analytic sample for Hypothesis 2.
Descriptive Table of Variables by Sexual and Gender Minority Status.
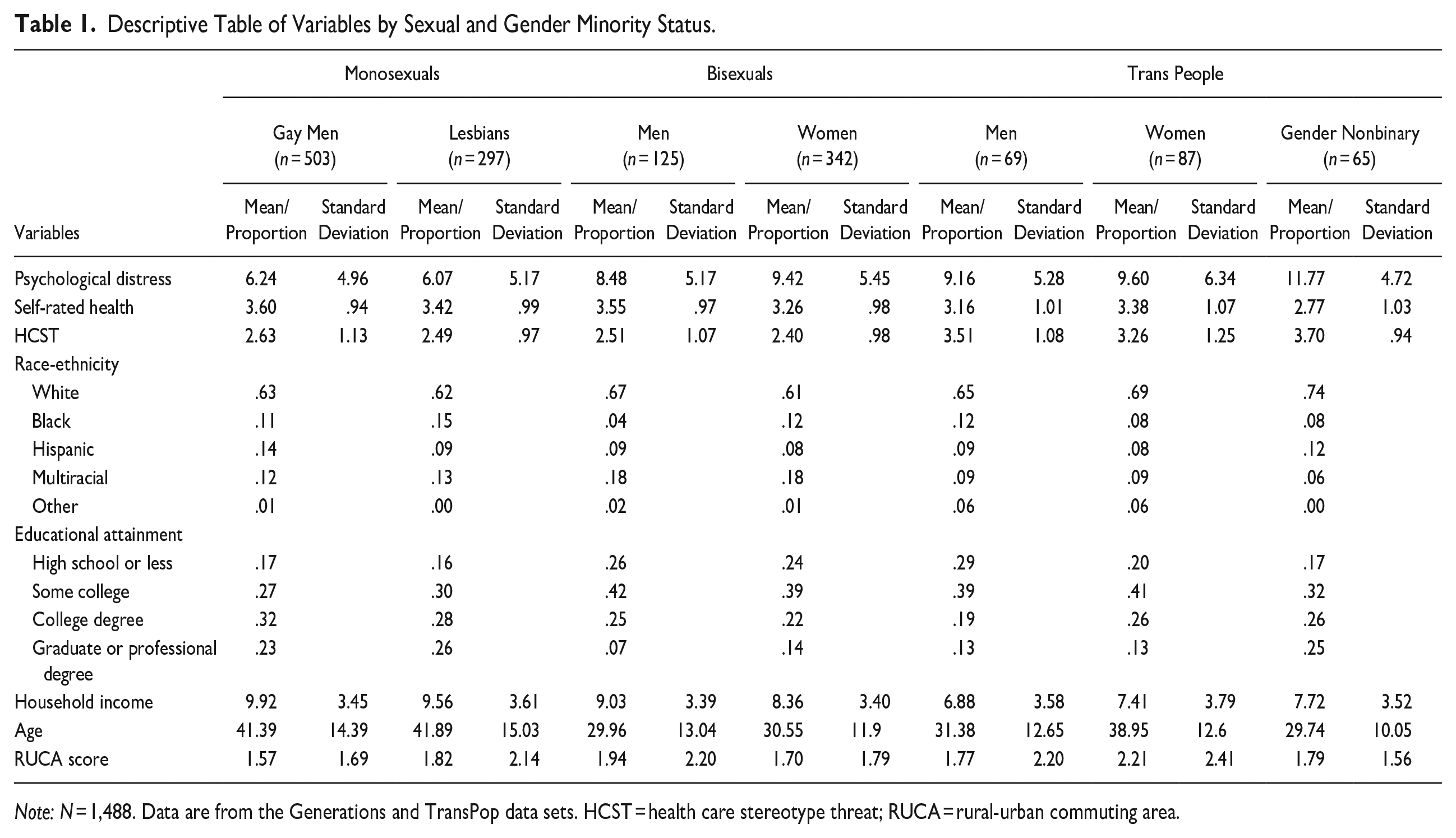
Note: N = 1,488. Data are from the Generations and TransPop data sets. HCST = health care stereotype threat; RUCA = rural-urban commuting area.
Measures
Dependent variables
The two dependent variables were self-rated health and psychological distress. Self-rated health was measured by asking, “Would you say that in general your health is . . . ”: (1) poor, (2) fair, (3) good, (4) very good, (5) excellent (Centers for Disease Control and Prevention 2014). This outcome was coded so that higher numbers indicated better health (mean = 3.41, range = 1–5).
Psychological distress was measured by using the Kessler-6 scale (Fushimi et al. 2012). This scale consisted of six items that are averaged. All items were asked on a frequency base from (1) none of the time to (4) all of the time. Items included asking, “During the last 30 days, about how often did you feel . . . ”: (1) nervous, (2) hopeless, (3) restless, (4) depressed, (5) everything was an effort, (6) worthless. The mean for the sample was 7.70, the range was 0 to 24, and the Cronbach’s α was .89. Higher numbers indicated more distress.
SGM groups
We used a categorical measure of SGM status: 1 = gay men (n = 503), 2 = lesbians (n = 297), 3 = bisexual men (n = 125), 4 = bisexual women (n = 342), 5 = trans men (n = 69), 6 = trans women (n = 87), and 7 = trans gender nonbinary (n = 65). All participants in these data who identified as gender nonbinary were also transgender. Although the TransPop data do include a heterosexual, cisgender comparison group, they were not asked the HCST items and were excluded from the analytic samples. The TransPop data also included a sexual orientation measure. It should be noted that sexual orientation and gender minority status are not mutually exclusive. However, as a result of sample sizes, we were unable to separate transgender people by sexual orientation.
HCST
HCST was the main independent variable, which was measured by four items answered on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree; Abdou and Fingerhut 2014). These items covered fears of confirming negative stereotypes about one’s social group and fear of their SGM status negatively influencing how medical providers judge, evaluate, and diagnose them (for the full instrument, see Appendix C in the online version of the article). An example item is, “When seeking healthcare, I worry about being negatively judged because of my sexual orientation or gender identity.” As a result, it is not clear which status or if both were considered by the participant when answering the HCST items. The scores from these items were averaged into a single measure (mean = 2.66, range = 1–5, Cronbach’s α = .90).
Discrimination
Everyday discrimination was measured by averaging nine statements about discrimination answered on a frequency scale (Williams et al. 1997): (1) never, (2) rarely, (3) sometimes, and (4) often. A selection of these items includes, “In your day-to-day life over the past year, how often did any of the following things happen to you?”: You were treated with less courtesy than others, treated with less respect, received poorer services, people acted as if they were afraid of you. The Cronbach’s α was .91; the mean was 1.90, with a range of 1 to 4.
Stigma
Experiencing stigma was measured by answering three statements on a 5-point Likert scale from (1) strongly disagree to (5) strongly agree (Herek 2009). The statements measured participants’ perceptions of how “most people” and “most employers” felt toward LGB people, such as “Most people where I live think less of a person who is LGB,” “Most employers where I live will hire openly LGB people if they are qualified for the job,” and “Most people where I live would not want someone who is openly LGB to take care of their children” (Herek 2009). The scores were averaged into a single measure (mean = 2.66, range = 1–5, Cronbach’s α = .70).
Control Variables
We included control measures to account for factors associated with both self-rated health and psychological distress. Demographic variables included race-ethnicity (1 = White, 2 = Black, 3 = Hispanic, 4 = multiracial, 5 = other) and age. We also included socioeconomic controls such as educational attainment (1 = high school and less than high school, 2 = some college, 3 = college degree, 4 = graduate or professional degree) and household income as measured by Gallup categories (1 = under $720 to 12 = $240,000 and up). Geographically, we controlled for urbanicity (mean = 1.73, range = 1–10.6). Controls that were excluded for parsimony and their nonsignificant associations on the outcomes and interaction term include partnered status, region, having health insurance, and having a health care place they regularly go to for services. For additional sensitivity analyses, see the appendices in the online version of the article for health care insurance and health care place (Appendix A), tests across race and ethnicity (Appendix B), and a general test of health disparities compared to a cisgender heterosexual sample (Appendix D).
Analytic Strategy
To test Hypothesis 1, we used ordinary least squares (OLS) regression to calculate the direct associations of HCST and the direct associations of everyday discrimination and experiencing stigma both individually and collectively on self-rated health and psychological distress. For these analyses, we used the Generations data because trans people were not asked the stigma questions. Specifically, we standardized all three variables—HCST, discrimination, and stigma—to make direct comparisons and calculate HCST’s association on the standardized outcomes accounting for the effects of everyday discrimination and experiencing stigma (see Table 2 and Figure 1). For the second hypothesis, we used the Generations and TransPop harmonized data set. Here we used OLS regression to explore the direct (see Table 3) and interaction effects (see Figures 2 and 3) of HCST on self-rated health and psychological distress for SGMs.
Standardized Association Results of HCST, Discrimination, and Stigma on Self-Rated Health and Psychological Distress.
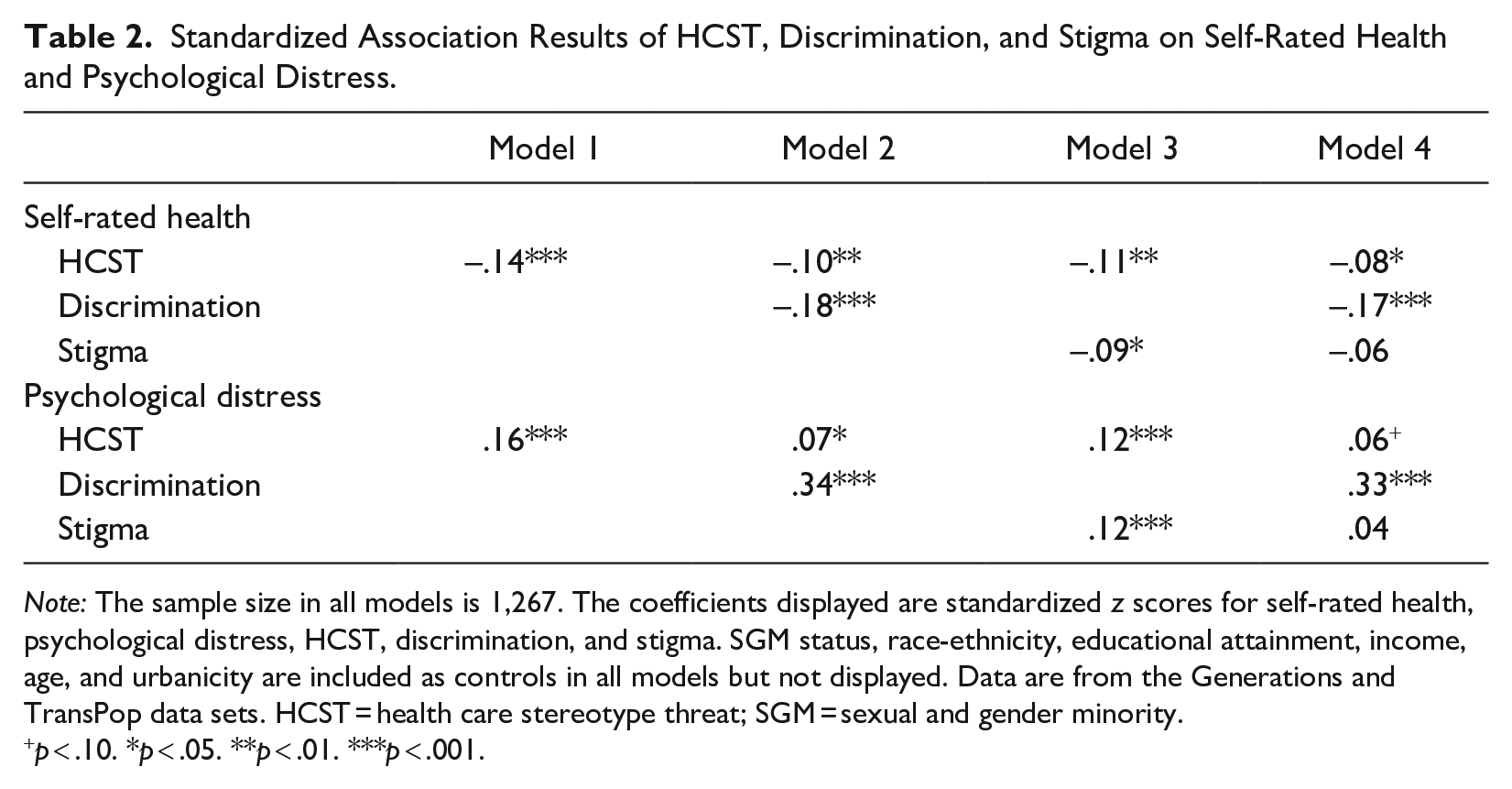
Note: The sample size in all models is 1,267. The coefficients displayed are standardized z scores for self-rated health, psychological distress, HCST, discrimination, and stigma. SGM status, race-ethnicity, educational attainment, income, age, and urbanicity are included as controls in all models but not displayed. Data are from the Generations and TransPop data sets. HCST = health care stereotype threat; SGM = sexual and gender minority.
p < .10. *p < .05. **p < .01. ***p < .001.
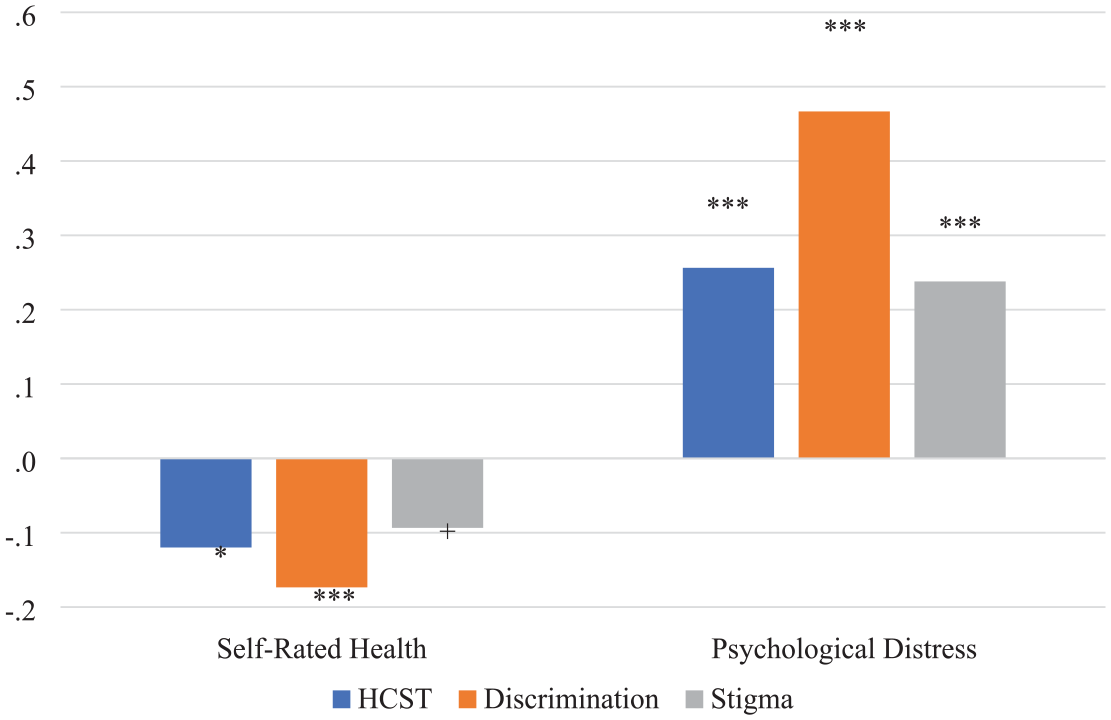
Marginal Analyses of Standardized Associations of HCST, Discrimination, and Stigma on Standardized Outcomes at 1 SD above the Mean.
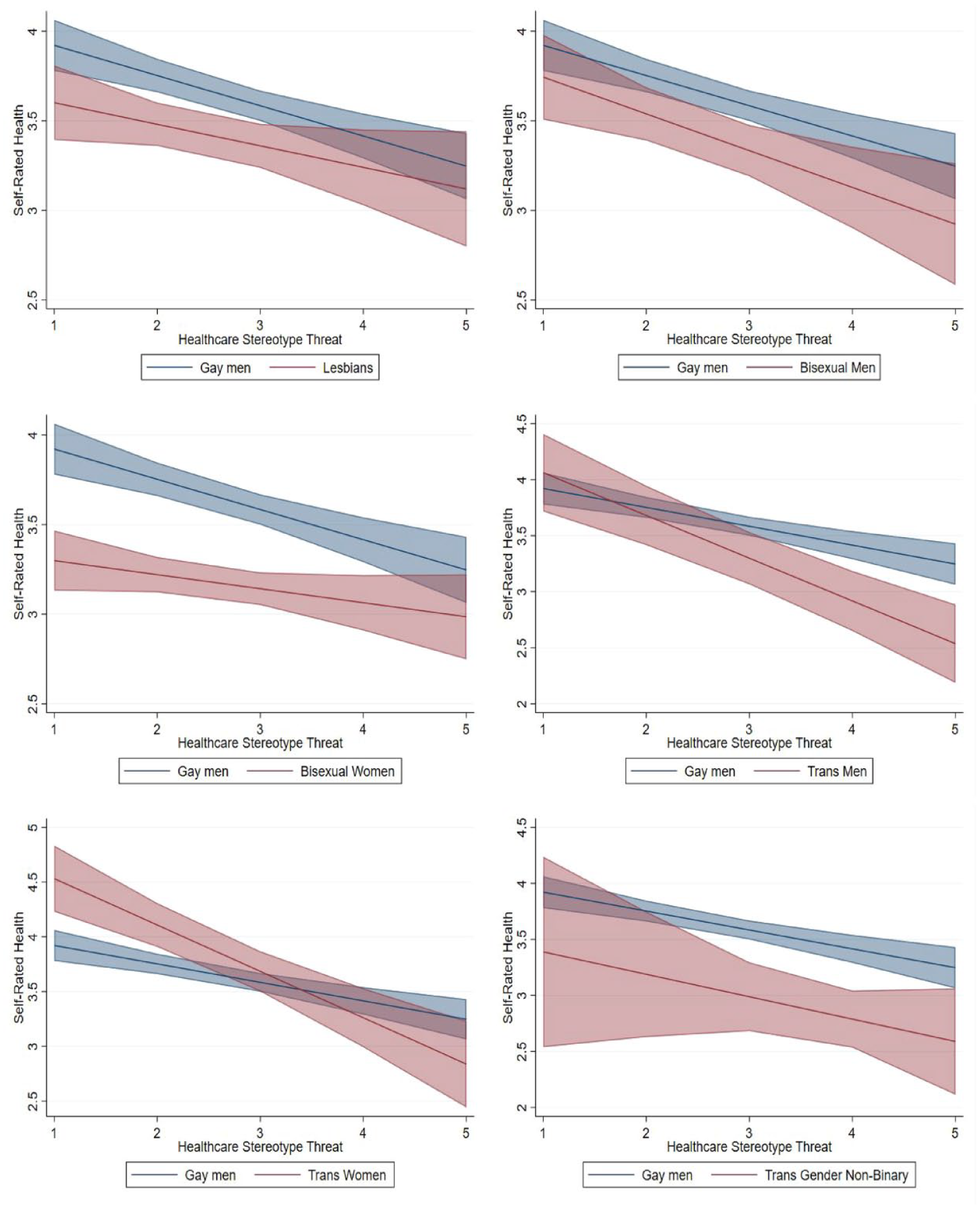
Interaction Effects of HCST on Self-Rated Health for Each Group Compared to Gay Men.
Interaction Effects of HCST on Psychological Distress for Each Group Compared to Gay Men.
Ordinary Least Squares Regression Results for Self-Rated Health and Psychological Distress.
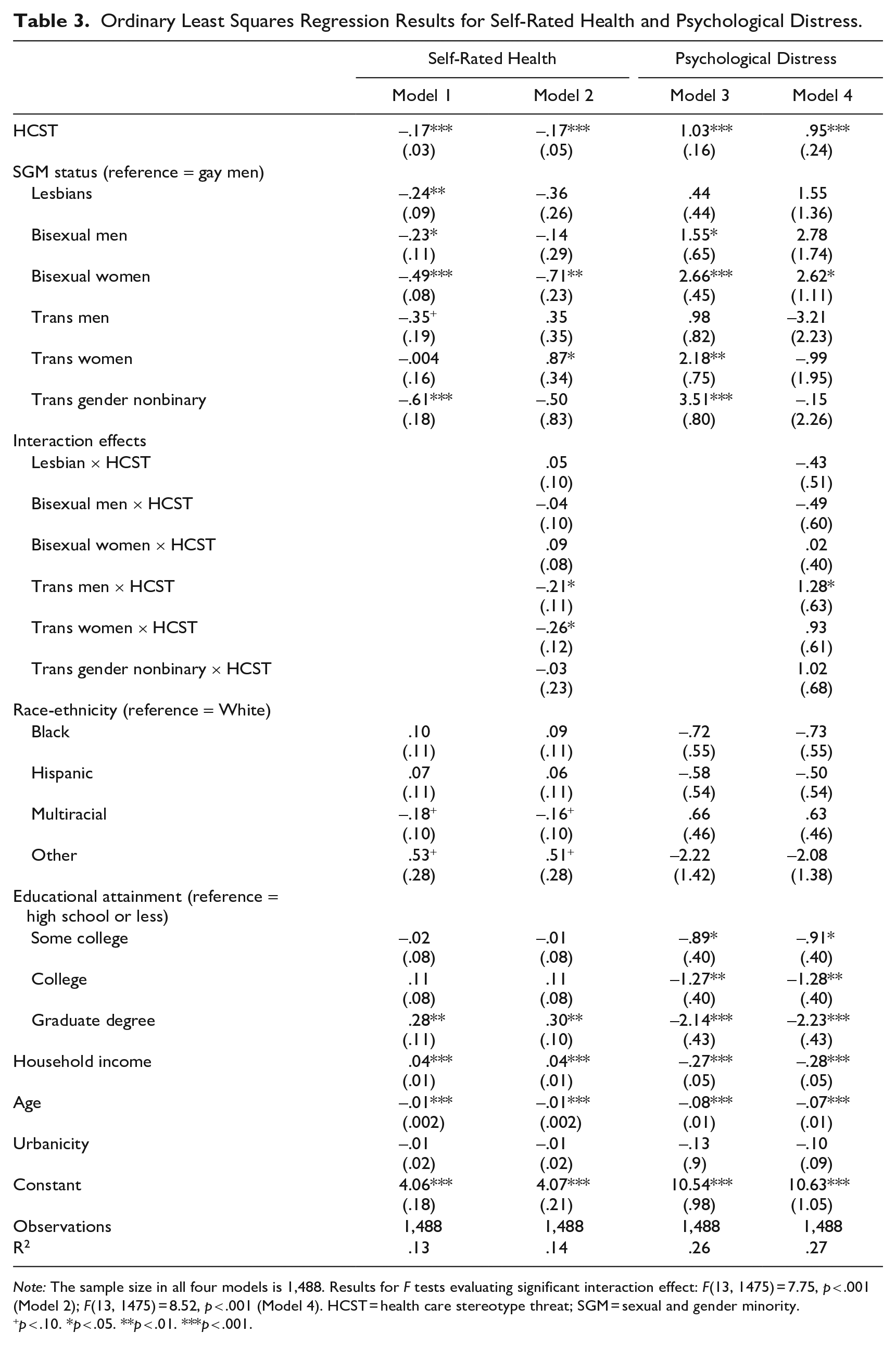
Note: The sample size in all four models is 1,488. Results for F tests evaluating significant interaction effect: F(13, 1475) = 7.75, p < .001 (Model 2); F(13, 1475) = 8.52, p < .001 (Model 4). HCST = health care stereotype threat; SGM = sexual and gender minority.
p < .10. *p < .05. **p < .01. ***p < .001.
To evaluate our results more carefully, we used marginal effects calculations for each health outcome (using Stata’s postestimation command margins), calculating the predicted health outcome value at each level of HCST for each SGM group holding all other factors in the model at the mean. We provide figures showing each SGM group relative to gay men given our hypothesis that this group will be least vulnerable to the consequences of HCST. We included 84% confidence intervals for our figures to show statistical differences between the groups, calculated using the average standard error of the difference between each group at each data point net of all other factors in fully controlled models, with statistical differences confirmed using the margins dydx command in Stata. We used 84% confidence intervals per previous researchers’ findings that an 83% or 84% size for interval is closer to an approximate .05 test of significance because their results showed the 95% confidence interval gave very conservative results closer to a 99% interval (Payton, Greenstone, and Schenker 2003; Schenker and Gentleman 2001). Furthermore, the use of this approach is growing in top-tier sociology journals (see Homan 2019), including this publication (see Homan, Brown, and King 2021).
In addition to the models provided, we conducted sensitivity tests exploring whether the effects of HCST on health outcomes in our SGM sample were explained by race, health insurance, or having a regular place for receiving health care services. We observed no significant moderating associations associated with these factors (see Appendixes A and B in the online version of the article).
Results
HCST, Discrimination, and Stigma
To test our first hypothesis, we test the association between HCST and self-rated health and psychological distress, accounting for stigma and discrimination. Table 2 displays four models where we evaluate the direct association of HCST alone (Model 1), with discrimination (Model 2), with stigma (Model 3), and accounting for all three factors (Model 4) on both outcomes. Table 2 displays standardized effects of the self-rated health, psychological distress, HCST, discrimination, and stigma variables while controlling for SGM status, race-ethnicity, educational attainment, income, age, and urbanicity, although the control variables are not displayed.
Results show that HCST remains statistically significant in association with self-rated health and psychological distress even when accounting for discrimination and reported experiences of stigma. Given that the effects of HCST are attenuated when accounting for stigma and discrimination, self-reported experiences of discrimination and stigma appear to play a role explaining the association between HCST and health (see Table 2). However, because HCST remains statistically significant accounting for these factors, this suggests that HCST is a unique factor that explains potential health disparities among SGMs, supporting our first hypothesis.
Figure 1 explores Table 2, Model 4 more closely by displaying the standardized marginal effects of HCST, discrimination, and stigma at 1 SD above the mean on the outcomes. These results show all three factors hold a large and significant influence on psychological distress, with HCST’s association on par with the association of stigma. For self-rated health, however, discrimination and HCST emerged as significant factors. This supports an argument that HCST seems to matter more for self-rated health than stigma when also considering discrimination (see Figure 1).
HCST, Self-Rated Health, and Psychological Distress
The second hypothesis is that bisexuals and trans people will report worse associations of HCST on their well-being compared to gay men. To explore this, we first conducted OLS regression analyses (see Table 3). Results show that HCST is associated with worse outcomes for both self-rated health and psychological distress. A one-unit increase in HCST is associated with a .17 decrease in self-rated health (p < .001) and a .95 increase in psychological distress (p < .001). These significant associations persisted with the inclusion of an interaction effect between HCST and SGMs.
Intragroup Variations of HCST’s Association
Self-rated health
Second, we used marginal effects to test Hypothesis 2 by examining how HCST associations on the outcomes vary across groups (see Figures 2 and 3). Figure 2 displays the graphed marginal effects of the interaction term (HCST × SGM status) on self-rated health (Table 3, Model 2). Overall and compared to gay men, lesbians (β = −.26, p < .01), bisexual men (β = −.23, p < .05), bisexual women (β = −.48, p < .001), trans men (β = −.38, p < .05), and trans gender nonbinary (β = −.61, p < .001) reported significant slopes where their self-rated health was worse (see Table 3, Model 1). Examining the interaction term shows that the effect of HCST on self-rated health is stronger for trans men (β = −.22, p < .05) and trans women (β = −.24, p < .05) compared to gay men (see Table 2, Model 2 and Figure 2). Although the direct slopes of both bisexual groups are significant compared to gay men, the interaction effect was not statistically significant.
Generally, for bisexual women, results show that they report significantly lower self-rated health than gay men at the lower levels of HCST. However, these groups appear more similar at higher levels of HCST. Importantly, Figure 2 displays stark differences in slopes for trans people compared to gay men. Although trans men do not significantly differ from gay men at lower levels of HCST, their self-rated health is significantly worse at higher levels of HCST. At the highest HCST level, trans men’s self-rated health is .76 points lower (p < .01) than gay men’s health. Figure 2 also shows that the slope is steeper for trans women compared to gay men, with their self-rated health being approximately 1.5 points lower when HCST is high compared to trans women reporting low HCST. A similar pattern emerged for trans gender nonbinary people’s self-rated health; it becomes significantly worse than gay men’s health when HCST is high. These results lend support to Hypothesis 2. Our results show that as HCST increases, trans people’s self-rated health is severely undermined regardless of their gender identity.
Psychological distress
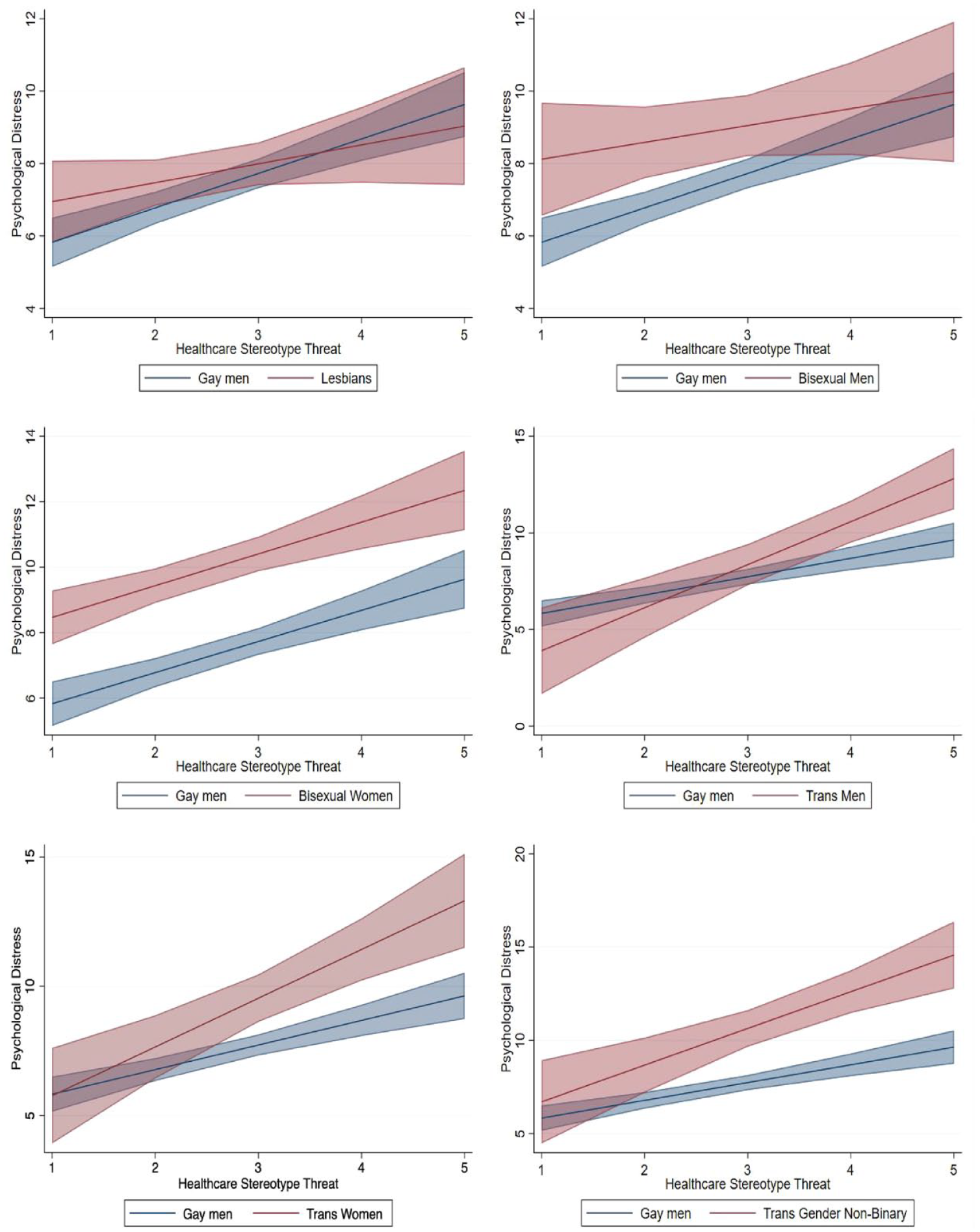
Figure 3 displays the graphed marginal effects of the interaction term for psychological distress (see Table 3, Model 4). This panel also uses 84% confidence intervals (Homan 2019; Payton et al. 2003; Schenker and Gentleman 2001). Overall and compared to gay men, bisexual men (β = 1.54, p < .05), bisexual women (β = 2.53, p < .001), trans women (β = 1.97, p < .01), and trans gender nonbinary people (β = 3.32, p < .001) display significant slopes showing that their psychological distress was worse as HCST increased (see Table 3, Model 3). The interaction term shows that trans men (β = 1.36, p < .05) display a significant slope compared to gay men (see Table 3, Model 4 and Figure 3).
Figure 3 also displays how SGM groups differ from gay men at each level of HCST on psychological distress. Significance between the groups is indicated graphically by nonoverlapping confidence intervals. Significant differences emerged for bisexual women and all three trans people groups compared to gay men. Bisexual women hold significantly higher levels of psychological distress than gay men at all levels of HCST. Trans men’s psychological distress, on the other hand, showed a significant slope compared to gay men’s, which leads to their distress surpassing gay men’s. In the higher levels of HCST, trans men’s distress was 2.0 points higher at Level 4 (p < .05) and 3.2 points higher at Level 5 (p < .01) compared to gay men. This trend emerged for trans women and trans gender nonbinary people as well, with higher levels of HCST associated with more psychological distress to the degree that both groups are significantly different from gay men. Similar to Figure 2, Figure 3 highlights the plight of trans folk and gives insight into Hypothesis 2 on how trans people generally fare worse as a result of HCST compared to gay men. These results partially support Hypothesis 2.
Discussion
Scholars have long studied health disparities and how they vary across social groups. Many common factors are often central to these analyses, such as experiencing discrimination, stigma, and stereotyping—especially for research examining sexual (i.e., gay men, lesbians, and bisexuals) and gender (i.e., trans people) minorities. Recently, psychologists have applied stereotype threat specifically to the health care setting to further investigate SGM health disparities (i.e., HCST; Abdou 2017; Abdou et al. 2016; Abdou and Fingerhut 2014). Although previous researchers have begun detailing the associations HCST has on well-being for sexual minorities (see Fingerhut et al. 2022), much remains unexplored. Thus, this work contributes to this discourse in several ways: (1) by examining how HCST’s association performs while considering the associations of discrimination and stigma, (2) by being the first study to include transgender people in HCST–health analyses, and (3) by paying specific attention to intragroup differences across SGM groups. We approached these goals by using two national probability samples of SGMs—Generations and TransPop—that we harmonized.
The results suggest that HCST holds a significant direct, adverse association with self-rated health and psychological distress net of the associations of experiencing discrimination and stigma. Thus, these results supported the first hypothesis that HCST is a significant factor in explaining persistent health disparities net of these other prominent variables used in previous work. Although HCST has clear overlapping theoretical ground with both discrimination and stigma, these results support the idea that narrowing in on the health care setting specifically has unique and important implications in uncovering and addressing barriers that SGMs face that can sustain and potentially widen health disparity gaps relative to the heterosexual population when left unconsidered.
Overall, HCST was associated with lower self-rated health and higher psychological distress. In support of the second hypothesis, results showed that HCST is associated with worse self-rated health and psychological distress for trans people compared to gay men and that, on average, gay men experience fewer consequences of HCST relative to other SGM groups. Compared to gay men, most often, trans men, trans women, and trans gender nonbinary folks report worse outcomes based on the interaction between HCST and SGM group analyses. The negative influence of this stereotyping on health is consistent with previous work (Abdou and Fingerhut 2014; Fingerhut et al. 2022; Hatzenbuehler et al. 2013). Researchers suggest that both the experience of and the anticipation of experiencing stereotyping function as a barrier to interacting with the health care system, and this, in turn, leads to higher risk of experiencing acute conditions that subsequently may become chronic (Willging et al. 2019). However, this work is the first to include trans people’s outcomes in the analyses and to show how HCST’s association significantly varies across SGMs.
Detailing these variations across SGM groups is how the results support targeted interventions to mitigate these processes. As Figures 2 and 3 display, trans people reported significantly worse outcomes as HCST increased. For example, on psychological distress, all trans groups increased at a rate where their psychological distress levels significantly surpassed gay men’s. For trans men and trans gender nonbinary people, high levels of HCST are more psychologically distressful than for gay men. Although we understand that HCST undermines health from previous work, novel results here highlight disparities within this marginalized subpopulation. One reason for the heightened negative impact of HCST for trans people could be the myriad of other issues this group faces, such as a higher likelihood of not having health insurance or a primary place for health care (Dickey et al. 2016) and heightened levels of poverty (Brown and Grossman 2014), experiencing discrimination (Paine 2018), and socioeconomic disadvantage (Lagos 2018). Another primary source present in these processes is the day-to-day stigma that is either experienced or anticipated to a degree that it is associated with worse health (Hatzenbuehler et al. 2013), which is to argue how HCST can be conceptualized as an upstream (Link and Phelan 1995) factor that influences an array of health outcomes and behaviors, such as poor self-rated, functional limitations, and diagnosed depression, as recent researchers document (see Stacey and Wislar 2023).
These results have important implications for interventions focused on addressing the health disparities SGMs face. The national probability sampling strategy of the data used herein assigns important and unique merit to the results presented. The Generations and TransPop data sets are the first of their kind, which gives us new and reliable insights into the processes that SGMs are facing nationally. Here specifically, we have detailed how the actual, perceived, or anticipated HCST is adversely associated with two highly established health outcomes. Thus, these results have the weight of providing guidance into mitigating HCST in the health care setting in multiple ways, such as through medical student training, modifying health care environments, and improving the standards of practice—all of which have the potential to positively shape health outcomes over time.
As previous researchers have shown, anticipation of discrimination or stereotyping in the health care setting works as a direct barrier to seeking care (Abdou 2017; Cruz 2014; Fingerhut and Abdou 2017; Gessner et al. 2020), and this delaying of care increases the likelihood of conditions worsening (Willging et al. 2019). Thus, the health care setting and the providers who fill those positions are the direct points of intervention to mitigate the process of HCST. Medical provider training needs modification such that SGM variation is treated as part of the natural variation rather than being medicalized as a deviation that cannot lead to proper care (Burgess et al. 2010; Davis et al. 2016). Through these new approaches of SGM patient–doctor interaction, the distrust (Underhill et al. 2015) can be attenuated, as can SGMs’ perceptions of medical providers’ cultural incompetence (Paine 2018).
However, it is also important to not overemphasize cultural incompetence interventions in the place of explicitly taking steps to address and name homophobic and transphobic practices in medical provider training institutions (Parsons 2020). As a review of cultural competence interventions focusing on race by Jongen, McCalman, and Bainbridge (2018) found, none of the interventions explicitly tackled the ideas of how racism and health practitioner biases are cogs in the machine of health disparities. As a result of researchers detailing how providers see giving “successful care” through a heterosexist viewpoint (Davis et al. 2016), medical provider training interventions must explicitly name and discuss the effects of heterosexism, homophobia, and transphobia as direct factors that influence the lives of SGMs inside and outside of the doctor’s office.
There are important limitations to the current study. First, these analyses do not explore how well-being changes over time. It important to consider how HCST’s association could increase or decrease because of numerous contextual factors, such as finding a pro-queer health provider, experiencing a major health concern that requires medical attention, and if and how a person can leverage newly acquired resources to positively influence their health care setting (e.g., gaining health insurance). Future researchers should also consider exploring how HCST interacts with the aging process because those in later life may still interact with the health care setting out of necessity, net of being dissuaded by HCST.
The operationalization of HCST in these data creates a limitation around what status(es) is considered when the participant answers the question. For example, these HCST item stems do not separate sexual orientation or gender identity; thus, it is unknown if and how participants used one or both identities when rating their answers. In future research, we suggest that researchers designing population-based surveys use an HCST instrument that can be provided to both SGMs and non-SGM samples and other important social groups who experience health disparities, such as racial and ethnic minorities, so it is possible to evaluate effect size differences for HCST on health across a range of social categories. For instance, what may be masked in our study is whether SGMs who are also from racial or ethnic minority groups are particularly likely to be exposed to HCST.
Finally, these results do not speak to how HCST occurs within the patient–doctor or patient–setting interaction. Exploring this avenue of questioning may be most fruitful if examined through qualitative methods, which can highlight the process through which SGMs experience and potentially challenge HCST. This line of questioning is also highly relevant to understanding specific points of intervention in regard to changing the practiced patterns of care and how these practices can be revised to further create health care environments that are conducive for better SGM health, health care use, and health care plan adherence.
Despite these limitations, this study offers novel theoretical and empirical findings by examining the influence of HCST on self-rated health and psychological distress for SGMs, net of well-established health factors—everyday discrimination and felt stigma—that supports our claim that HCST is a unique and important health indicator for future researchers to consider. Although previous work shows how stereotyping is generally negatively associated with well-being, this study suggests that within SGMs are important differences in disparity mechanisms that highlight points of mitigation and the heightened adverse associations specifically experienced by trans people. This finding is important because it underscores how critical it is for health disparity research to explore differences across sexual and gender minority groups rather than merely comparing LGB and LGBT populations to cisgender heterosexual samples as though they are monolithic. Our examination of effect sizes across these SGM groups shows that HCST interventions have potential to be an important pathway toward reducing health disparities. However, the design and subsequent success of future HCST interventions should be justly analyzed by considering SGMs compared to one another, not just to cisgender heterosexuals.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465231205549 – Supplemental material for Health Care Stereotype Threat and Sexual and Gender Minority Well-Being
Supplemental material, sj-docx-1-hsb-10.1177_00221465231205549 for Health Care Stereotype Threat and Sexual and Gender Minority Well-Being by R. Kyle Saunders, Dawn Carr and Amy M. Burdette in Journal of Health and Social Behavior
Footnotes
Acknowledgements
The authors thank the Aging Research on Contexts, Health, and Inequalities working group at Florida State University for their feedback and support that significantly improved this article.
Supplemental Material
Appendices A through D are available in the online version of the article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.