
Abstract
Health care research has long overlooked the intersection of multiple social inequalities. This study examines influenza vaccination inequities at the intersection of sexuality, gender, and race-ethnicity. Using data from the 2013 to 2018 National Health Interview Survey (N = 166,908), the study shows that sexual, gender, and racial-ethnic identities jointly shaped flu vaccination. Specifically, White gay men had the highest vaccination rate (56%), while Black bisexual women had the lowest rate (23%). Across Black, Hispanic, and White individuals, sexual minority women had lower vaccination rates than heterosexual women, but sexual minority men had higher or similar vaccination rates than heterosexual men. Economic enabling, noneconomic enabling, and need-based factors together explained a substantial portion of these gaps. However, they cannot explain all the disadvantages faced by Black lesbian, bisexual, and heterosexual women and Black heterosexual men. Findings offer new evidence of hidden health care inequities and inform health policies from an intersectional perspective.
Most studies of health care inequities have focused on a singular dimension of socially constructed inequality, such as race-ethnicity, gender, or sexuality. The extant research suggests that racial-ethnic minorities, men, and sexual minorities tend to underutilize health services because they have inadequate resources, experience prejudice and discrimination, or face cultural barriers to care (Courtenay 2000; Dahlhamer et al. 2016; Hsieh and Shuster 2021; Smedley, Stith, and Nelson 2003; Springer and Mouzon 2011). Although this research has created a foundation for understanding inequities in health care experiences, it has not revealed how multiple social identities and positions intersect to influence individuals’ experiences. In recent years, a nascent body of research has begun to use an intersectional approach to assess health care access and utilization among Black and Hispanic sexual minority people; however, these studies focus primarily on sexual/reproductive health care, such as HIV/STD prevention (Padilla et al. 2019). Few studies have examined inequities in health services beyond the sexual/reproductive health area faced by multiply minoritized populations.
The current study addresses these gaps in knowledge by analyzing influenza (flu) vaccination inequities at the intersection of sexual, gender, and racial-ethnic identities using a nationally representative sample of the U.S. adult population. According to the Centers for Disease Control and Prevention (CDC), flu vaccination is the primary method to reduce the burden of flu illnesses and related medical visits, hospitalization, and deaths. During 2019 to 2020, the most recent flu season before the COVID-19 pandemic, flu vaccination prevented an estimated 7.5 million influenza illnesses, 3.7 million medical visits, 105,000 hospitalizations, and 6,300 deaths (CDC 2021b). In the wake of the COVID-19 pandemic caused by the SARS-CoV-2 virus and emerging viral mutations, identifying hidden vaccination gaps in the population and the mechanisms creating these gaps is imperative for designing future public health measures. Population-level data on flu vaccination, which cover an extended period and diverse social groups, are invaluable for understanding and predicting vaccination inequities more broadly.
Background
Conceptual Framework: Behavioral Model of Health Services Use and Intersectionality
Much of the research on health services utilization has employed the behavioral model of health services use (BMHSU), which theorizes major factors—predisposing, enabling, and need-based factors—that jointly determine health care use (Andersen 2008; Andersen and Newman 2005; Babitsch, Gohl, and von Lengerke 2012; Lederle, Tempes, and Bitzer 2021). Figure 1 presents the conceptual framework of this study adapted from the BMHSU. Predisposing factors include demographic and structural variables that shape downstream enabling and need-based factors that, in turn, drive health care utilization. For example, sexuality, gender, and race-ethnicity are sociodemographic characteristics that expose certain subgroups of individuals to oppression and privilege (heterosexism, sexism/patriarchy, and racism), which can impact their access to resources (enabling factors) and health status (need-based factors) and, in turn, lead to unequal utilization of health care (National Academies of Sciences, Engineering, and Medicine 2020; Phelan and Link 2015).
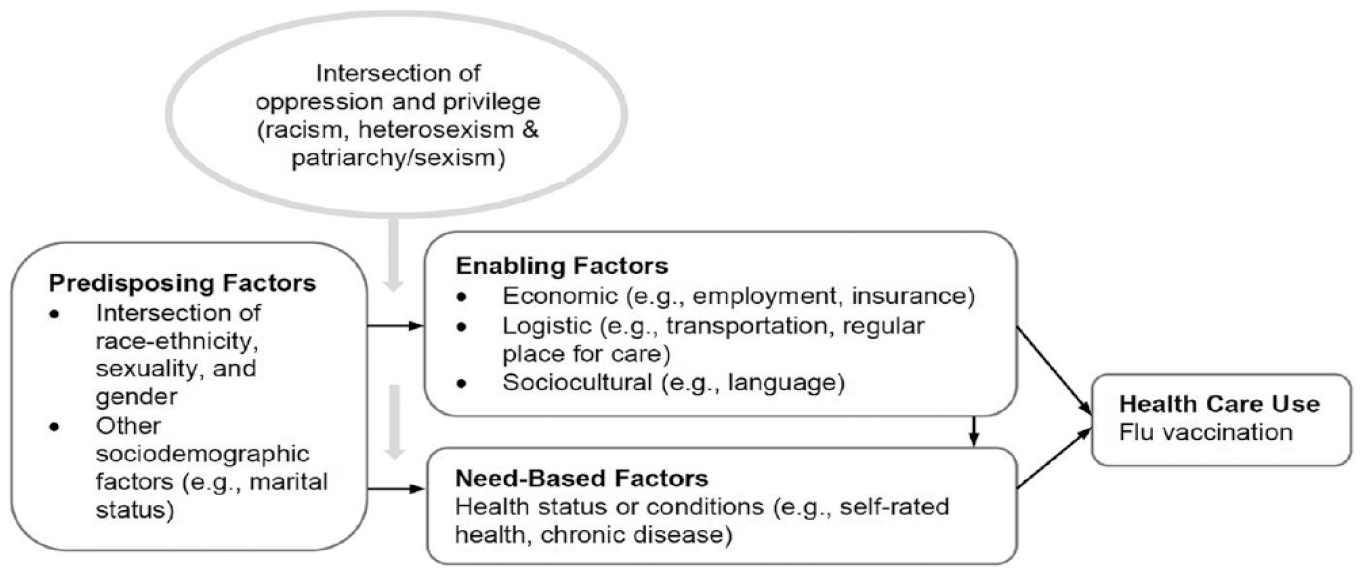
Conceptual Framework of Flu Vaccination based on Behavioral Model of Health Services Use and Intersectionality.
Enabling factors include economic, logistic, and sociocultural resources that make health services more or less accessible to individuals (Gage-Bouchard 2017; Hsieh and Ruther 2017; Quinn, Bowleg, and Dickson-Gomez 2019). Need-based factors include health statuses/conditions that require medical attention or treatment (Andersen and Newman 2005). Because minoritized populations, such as sexual and racial-ethnic minorities, often exhibit higher morbidity than their majority counterparts due to oppression and lack of resources (National Academies of Sciences, Engineering, and Medicine 2020; Williams and Sternthal 2010), their greater needs for health care or higher risk of experiencing severe complications may encourage greater use of certain preventive services (Bleser, Miranda, and Jean-Jacques 2016; CDC 2021a). The BMHSU has been widely used to examine how a variety of sociodemographic/structural dimensions may influence individuals’ utilization of health care resources (Babitsch et al. 2012; Lederle et al. 2021). However, most scholarship based on the BMHSU has not explicitly incorporated an intersectional approach to systematically assess how multiple predisposing factors may intersect to shape health care behaviors until lately (see e.g., Wilkins [2022] on vaccination inequities jointly shaped by sexual and racial-ethnic identities).
Intersectionality, a framework of critical inquiry and praxis addressing power relations and social injustice (Collins and Bilge 2016; Crenshaw 1991), argues that multiple systems of oppression and privilege jointly produce stigma, stress, coping resources, and resilience, thereby influencing individuals’ health behaviors and outcomes (Agénor 2020; Bowleg 2008). Intersectionality emphasizes that discrete systems of power inequality such as racism, patriarchy/sexism, and heterosexism are interconnected and mutually reinforcing, and their impact on individuals are impossible to untangled (Collins and Bilge 2016; Misra, Curington, and Green 2021). Notably, intersectionality is not simply about identities, and its focus on power and structural inequality cannot be downplayed (Bowleg 2021). Despite increasing evidence for the importance of intersectionality, most health and health care studies have focused on a singular dimension of inequity, and therefore researchers have yet to identify both the health care inequities faced by multiply disadvantaged groups and the mechanisms underlying these inequities (Guan et al. 2021; Hsieh and Shuster 2021). Studying health care experiences through an intersectional lens is a critical step toward fully understanding the heterogeneity of the challenges and opportunities facing diverse minority populations. The following section explores how sexuality, gender, and race-ethnicity may independently and jointly influence health care utilization, with a focus on vaccination.
Health Care Utilization and Vaccination by Sexuality, Gender, and Race-Ethnicity
Sexuality
Research on health care experiences of sexual minorities has shown that relative to their heterosexual counterparts, lesbian, gay, and bisexual (LGB 1 ) individuals have poorer access to and utilization of health services, with the exception of certain types of sexual health care (Dahlhamer et al. 2016). Overall, LGB populations are more likely to delay/avoid seeking care, not have a regular provider, and skip needed treatment. However, heterogeneity among LGB groups also exists. Bisexual individuals are more likely to report barriers to care than their gay/lesbian counterparts, and this difference is more pronounced among sexual minority women than sexual minority men (Dahlhamer et al. 2016; Everett and Mollborn 2014). Major barriers to care among LGB individuals include a lack of adequate health care coverage, financial insecurity, and low levels of trust in the health care system due to sexuality-based stigma (Badgett, Choi, and Wilson 2019; Hsieh and Shuster 2021; McNair, Hegarty, and Taft 2012). Furthermore, prejudice and disrespect among providers and a lack of knowledge and sensitivity about sexuality also deter sexual minorities from utilizing health services (Agénor et al. 2015; Everett and Mollborn 2014; Sabin, Riskind, and Nosek 2015).
Most studies of health care utilization among sexual minorities have focused on sexual/reproductive health care, such as HIV/STD testing and prevention, and therefore little is known about flu vaccination coverage among this group (Padilla et al. 2019). The findings on human papillomavirus (HPV) vaccination, a focal area of vaccination research for sexual minorities, indicates that compared to their heterosexual counterparts, bisexual women, bisexual men, and gay men all had higher rates of HPV vaccination, but lesbian women had lower rates (Griffin, Jaiswal, and Stults 2021; Solazzo et al. 2019). However, limited evidence suggests that bisexual individuals have lower flu vaccination rates than their heterosexual and gay/lesbian counterparts (Srivastav et al. 2019), but this vaccination gap may depend on gender or race-ethnicity. For example, bisexual women but not bisexual men had lower vaccination rates than their heterosexual counterparts (Polonijo and Vogelsang 2023), and bisexual individuals of Asian non-Hispanic background but not other racial-ethnic background had higher vaccination rates than their heterosexual counterparts (Wilkins 2022). The mixed findings on HPV and flu vaccination may be the result of differences in the target populations for certain health services (e.g., many programs focus on encouraging sexual minorities to use selected sexual health care) and focal age groups (e.g., HPV vaccination research focuses on adolescents and young adults).
Gender
Like sports and occupations, health behaviors are among the variety of activities used to construct and demonstrate gender (Courtenay 2000). For example, men may conform to dominant and socially expected gender norms through concealing vulnerability and dismissing the need for health care. Although masculinity garners more power and socioeconomic status than femininity, the former is associated with fewer health-promoting beliefs and behaviors, such as attending visits with health care providers and utilizing preventive health services (Courtenay 2000; Springer and Mouzon 2011). Relatedly, studies of gender dynamics in intimate relationships have found that in heterosexual couples, female partners often do more health care work (e.g., making health appointments) for their male partners than vice versa; meanwhile, partners in same-sex relationships tend to share the responsibilities of health facilitation more equally (Reczek et al. 2018; Umberson, Donnelly, and Pollitt 2018).
Although few studies have explored the link between gender and flu vaccination, there is some evidence that men have lower vaccination rates than women in the United States (Applewhite et al. 2020). The National Center for Health Statistics (2017) consistently reported lower flu vaccination coverage among men than among women from 1989 to 2016. Also, men who strongly support practices of conventional masculinity (e.g., concealing emotions) are less likely than men who do not endorse these practices to have received a flu shot in the past 12 months (Springer and Mouzon 2011). Recent findings have also shown that transgender adults have lower vaccination rates than cisgender adults (Polonijo and Vogelsang 2023).
Race-ethnicity
Racial-ethnic inequities in health care resources are well documented. Prior studies have shown that compared to White Americans, American Indian/Alaska Native (AIAN), Asian, Black, Hispanic, and Pacific Islander Americans receive less intense and lower quality health services across a wide range of procedures and disease areas (Malat et al. 2010; Saha, Arbelaez, and Cooper 2003; Smedley et al. 2003; U.S. Commission on Civil Rights 2004, 2018). Lower socioeconomic status and greater economic barriers to care due to institutional racism contribute to some of these inequities (American Psychological Association 2016; Rothstein 2017; U.S. Commission on Civil Rights 2018). Furthermore, provider bias against racial-ethnic minorities and patients’ experiences of racism foster mistrust, poor treatment adherence, and underutilization of medical care (Feagin and Bennefield 2014; Hall et al. 2015; Trivedi and Ayanian 2006). In addition, racial-ethnic minorities who are immigrants or indigenous Americans may experience challenges accessing health care due to cultural barriers such as differences in languages, health views, and healing approaches (Chae and Ayala 2010; Mackay 2022; Yoo, Gee, and Takeuchi 2009).
Studies of racial-ethnic variation in flu vaccination indicate largely consistent patterns: Black, Hispanic, AIAN, and Pacific Islander Americans have lower rates of vaccination than White Americans (Brewer et al. 2021; Grohskopf, Liburd, and Redfield 2020; Singleton, Santibanez, and Wortley 2005). These coverage gaps have persisted despite increasing flu vaccination coverage across racial-ethnic groups over time (Lu et al. 2014). In a recent flu season (2021–2022), non-Hispanic White (53.9%) and Asian people (54.2%) had significantly higher coverage than people self-identified as non-Hispanic Black (42.0%), Hispanic (37.9%), AIAN (40.9%), and Pacific Islander (42.6%; CDC 2022). Notably, cost concerns, not having a regular provider, missed opportunities (having a doctor visit but not receiving a vaccine recommendation from the provider), and mistrust in pharmaceutical companies and government agencies due to the history of medical racism in the United States are significant drivers of lower flu vaccination rates among racial-ethnic minorities (Bleser et al. 2016; Chen et al. 2007; Jamison, Quinn, and Freimuth 2019; Maurer, Harris, and Uscher-Pines 2014; Singleton et al. 2005).
Intersection of sexuality, gender, and race-ethnicity
The literature reviewed shows that sexual minorities, men, and racial-ethnic minorities tend to underutilize health services and thus may have lower rates of flu vaccination. However, the prior evidence does not necessarily imply that these effects are additive, in other words, that sexual minority men of color have the lowest flu vaccination rates in the population. Indeed, intersectionality research has shown that the health effects of multiple disadvantaged positions may interact in unexpected ways, and unique configurations of social positions may be associated with particularly large risks or benefits for health (Bauer et al. 2021; Bowleg 2008).
A nascent group of studies has begun to address inequities in health care experiences via an intersectional lens (Agénor et al. 2015; Hsieh and Mirzoyan 2021; Quinn et al. 2019; Wilkins 2022). However, most of these studies focus on sexual/reproductive health care or examine the intersection of only two inequity dimensions. For example, qualitative research on Black sexual minority people has shown that racism and heterosexism from health care providers intertwine to hinder the use of PrEP and cervical cancer screening (Agénor et al. 2015; Quinn et al. 2019). Quantitative research has found that race-ethnicity complicates the variation in flu vaccination by sexual orientation (Wilkins 2022) and that sexual minority women experience less culturally competent care than both heterosexual women and sexual minority men (Hsieh and Mirzoyan 2021). The current study is one of the first to investigate vaccination inequities at the intersection of sexuality, gender, and race-ethnicity using a nationally representative data set.
Hypotheses
Hypothesis 1: Sexual, gender, and racial-ethnic identities jointly shape vaccination inequities in a pattern that is not predicted by prior research based on a singular dimension of inequality, which suggests that sexual minority men of color would have the lowest flu vaccination rates.
Hypothesis 2: Economic enabling factors (e.g., employment and insurance coverage), noneconomic enabling factors (e.g., language and logistic barriers to care), and need-based factors (e.g., chronic conditions) contribute to vaccination inequities at the intersection of sexual, gender, and racial-ethnic identities. However, the relative importance of these factors may vary across intersections.
Data And Methods
Data and Sample
The analysis used data from the adult sample of the 2013 to 2018 National Health Interview Survey (NHIS), a household survey that covers a broad range of health-related topics (Blewett et al. 2022). The survey sample is representative of the civilian, noninstitutionalized U.S. population age 18 and older. Since 2013, the NHIS has included a sexual identity question in its adult questionnaire, allowing researchers to examine health care and health inequalities by sexual identity.
To ensure sufficient sample sizes, the analysis focused on the intersection of a limited number of identity categories: gay, lesbian, bisexual, and heterosexual for sexuality; woman and man for gender; and non-Hispanic White, non-Hispanic Black, and Hispanic for race-ethnicity. Although some respondents identified as “something else” for sexual identity and some identified as “Asian, Native American, or multiracial” for race, the number of cases in each of these groups was too small for statistical analysis when further stratified by the other two identity types (e.g., n = 25 for bisexual Asian women). Accordingly, these groups were not included in the analysis. Moreover, the analysis did not include other gender identities (e.g., transgender and nonbinary) because the NHIS measures sex/gender in a cisgender binary way. Notably, these data limitations reflect multiple forms of institutional oppression. For example, the small representation of Native Americans in population surveys results from excessive deaths related to colonialism and the continuously underfunded health care systems for Native Americans (U.S. Commission on Civil Rights 2004, 2018).
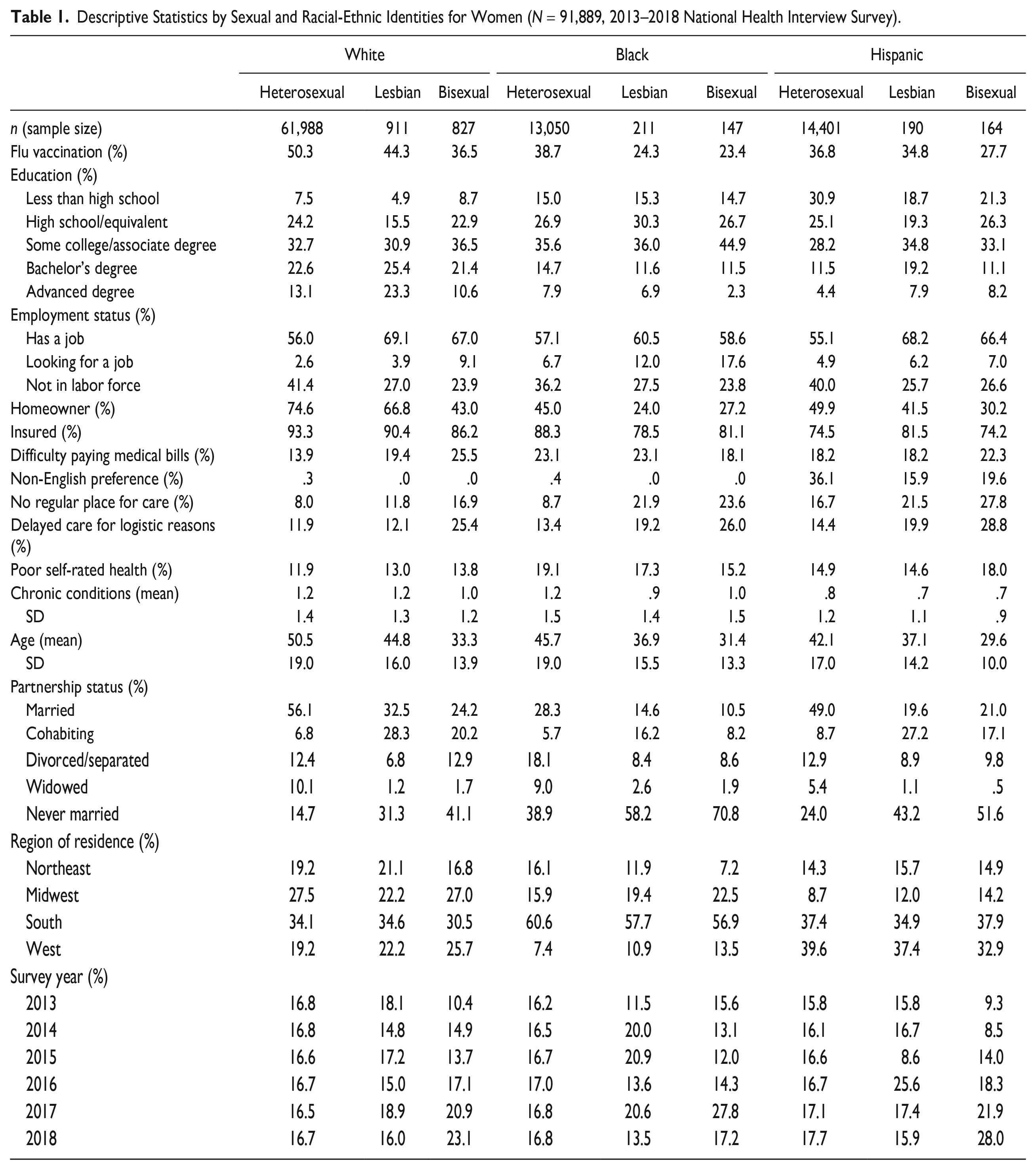
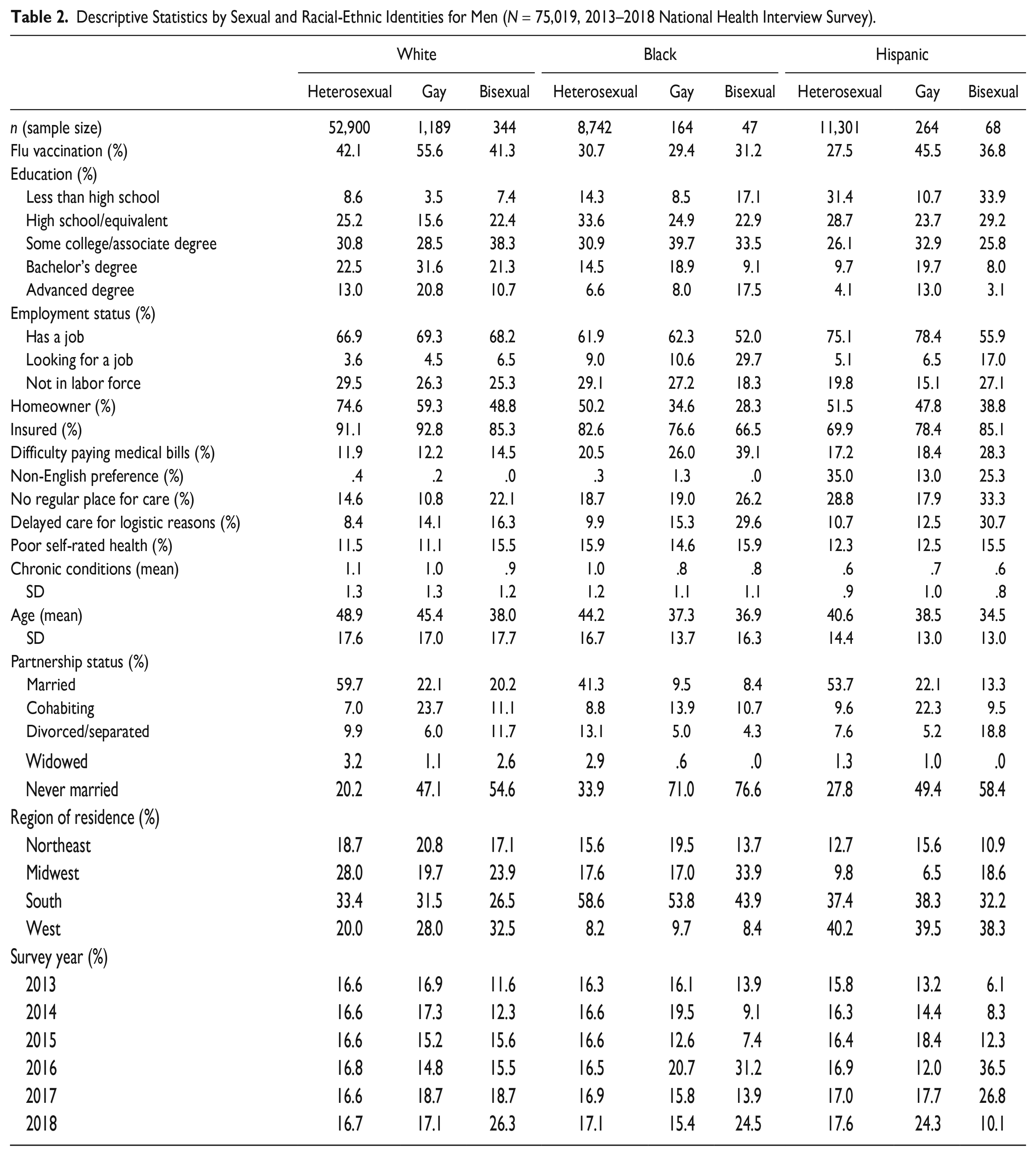
The initial NHIS sample included 190,111 adults; among them, 168,442 people were eligible for inclusion in the analytic sample based on their sexual, gender, and racial-ethnic identities. After removing cases with missing values (<1% of the eligible sample) on one or more covariates, the final analytic sample included 166,908 people. Tables 1 and 2 present the sample sizes for the 18 analytic subgroups.
Descriptive Statistics by Sexual and Racial-Ethnic Identities for Women (N = 91,889, 2013–2018 National Health Interview Survey).
Descriptive Statistics by Sexual and Racial-Ethnic Identities for Men (N = 75,019, 2013–2018 National Health Interview Survey).
Measures
The dependent variable was flu vaccination status, which indicated whether the respondent received an influenza vaccine in the past 12 months (1 = yes, 0 = no). The independent variables included predisposing, enabling, and need-based factors likely associated with flu vaccination. The primary predisposing factors included in the analysis were sexual, racial-ethnic, and gender identities. To facilitate an intersectional analysis, I used a cross-classification approach to create a joint variable based on sexual and racial-ethnic identities that included nine categories: White heterosexual, White gay/lesbian, White bisexual, Black heterosexual, Black gay/lesbian, Black bisexual, Hispanic heterosexual, Hispanic gay/lesbian, and Hispanic bisexual (both White and Black groups are non-Hispanic). A separate variable, gender, approximated by whether the respondent identified as female or male, 2 was used to both stratify the analysis and serve as an interaction variable (see “Analytic Plan”).
The enabling factors comprised both economic and noneconomic variables that might contribute to a respondent’s vaccination status. The economic enabling factors included education, employment status, homeownership, insurance coverage, and difficulty paying medical bills. Education contained five categories: less than high school, high school or equivalent, some college or associate degree, bachelor’s degree, and advanced degree. Employment status indicated whether the respondent was working at a job, looking for a job, or not in the labor force in the past week. Homeowner indicated whether the respondent or a family member owned the house/apartment in which they were living (1 = yes, 0 = no). Insured indicated whether the respondent was covered by a health insurance plan (1 = yes, 0 = no). Difficulty paying medical bills indicated whether the respondent had any problems paying their medical bills in the past 12 months (1 = yes, 0 = no).
The noneconomic enabling factors included language preference, no regular place for care, and delayed care for logistic reasons. Non-English preference indicated that the respondent chose to complete the interview in a language other than English (1 = non-English, 0 = English). No regular place for care indicated that the respondent did not have a usual place to go for medical care (1 = yes, 0 = no). Delayed care for logistic reasons indicated that in the past 12 months, the respondent delayed getting care for any of the following reasons: they could not get an appointment soon enough, the doctor’s office was not open, they could not get through to the office by phone, they lacked transportation, or the wait at the doctor’s office was too long (1 = yes, 0 = no).
The analysis also included two need-based factors: self-rated health (SRH) and chronic conditions. Poor SRH indicated that the respondent rated their general health as poor/fair rather than good/very good/excellent (1 = poor/fair, 0 = otherwise). The chronic conditions variable measured the respondent’s number of diagnosed high-risk conditions that are subject to a strong medical recommendation for the flu vaccination (CDC 2021a); these conditions include asthma, arthritis, chronic bronchitis or emphysema, cancer, diabetes, heart disease, hypertension, and stroke. Finally, sociodemographic variables included age (in years, 18–85), partnership status (married, cohabiting, divorced/separated, widowed, never married), region of residence (Northeast, Midwest/North Central, South, West), and survey year (2013, 2014, 2015, 2016, 2017, 2018).
Analytic Plan
The study used a combination of cross-classification, stratification, and decomposition approaches to conduct intersectional analysis (Guan et al. 2021). Given a large sample size (N > 50,000) and a common outcome (prevalence > 15%), this analytic strategy is expected to achieve high estimation accuracy (Mahendran, Lizotte, and Bauer 2022). Logistic regression models were performed to predict flu vaccination status. Because there were major gender differences in vaccination rates across sexual-racial-ethnic intersections (see the interaction analysis in the Appendix in the online version of the article), a series of regression models were estimated separately for women and men. Model 1 assessed the association between sexual-racial-ethnic identification and flu vaccination, revealing unadjusted vaccination gaps. Models 2 to 5 added sociodemographic, economic enabling, noneconomic enabling, and need-based factors, respectively, into the analysis to determine the extent to which each cluster of factors explains the vaccination gaps. Model 6 included all covariates to estimate fully adjusted variations in vaccination. Seemingly unrelated estimation based on adjusted Wald tests was performed to test whether the changes in coefficient estimates across models reached statistical significance. Finally, the Karlson–Holm–Breen (KHB) method was used to decompose the identified vaccination variation into the portions explained by key factors (Breen, Karlson, and Holm 2013). All analyses were weighted using the svy, subpop function in Stata 17 to account for the sampling design, including oversampling of racial-ethnic minorities and nonresponse.
Results
Descriptive Statistics for Key Variables
Figure 2 presents the percentages of respondents who received a flu vaccine by racial-ethnic, sexual, and gender identities. Vaccination rates varied across all three social dimensions, with White gay men being most likely to be vaccinated (55.6%) and Black bisexual women being least likely (23.4%). There are several notable patterns in the vaccination gaps. First, White individuals had higher vaccination rates than Black and Hispanic individuals with similar sexual and gender identities. The Black–White difference was particularly pronounced. For example, the difference between Black and White lesbian women was 20 percentage points (24.3% vs. 44.3%), and the difference between Black and White heterosexual men was more than 11 percentage points (30.7% vs. 42.1%). Notably, all Black–White differences were statistically significant except the difference for bisexual men. Second, heterosexual women had higher vaccination rates than heterosexual men across all racial groups, but lesbian and bisexual women tended to have lower vaccination rates than gay and bisexual men, suggesting that gender differences in vaccination depend on sexual identity. Lastly, sexual minority women were less likely than heterosexual women to be vaccinated in all racial-ethnic groups, whereas the patterns for men differed across racial-ethnic groups. Among both White and Hispanic men, gay men had significantly higher vaccination rates than heterosexual men. For Black men, however, vaccination rates were similar across sexual identity groups. Taken together, these results suggest that gender, race-ethnicity, and sexuality intersect to shape vaccination behavior in nuanced ways not predicted by prior research.
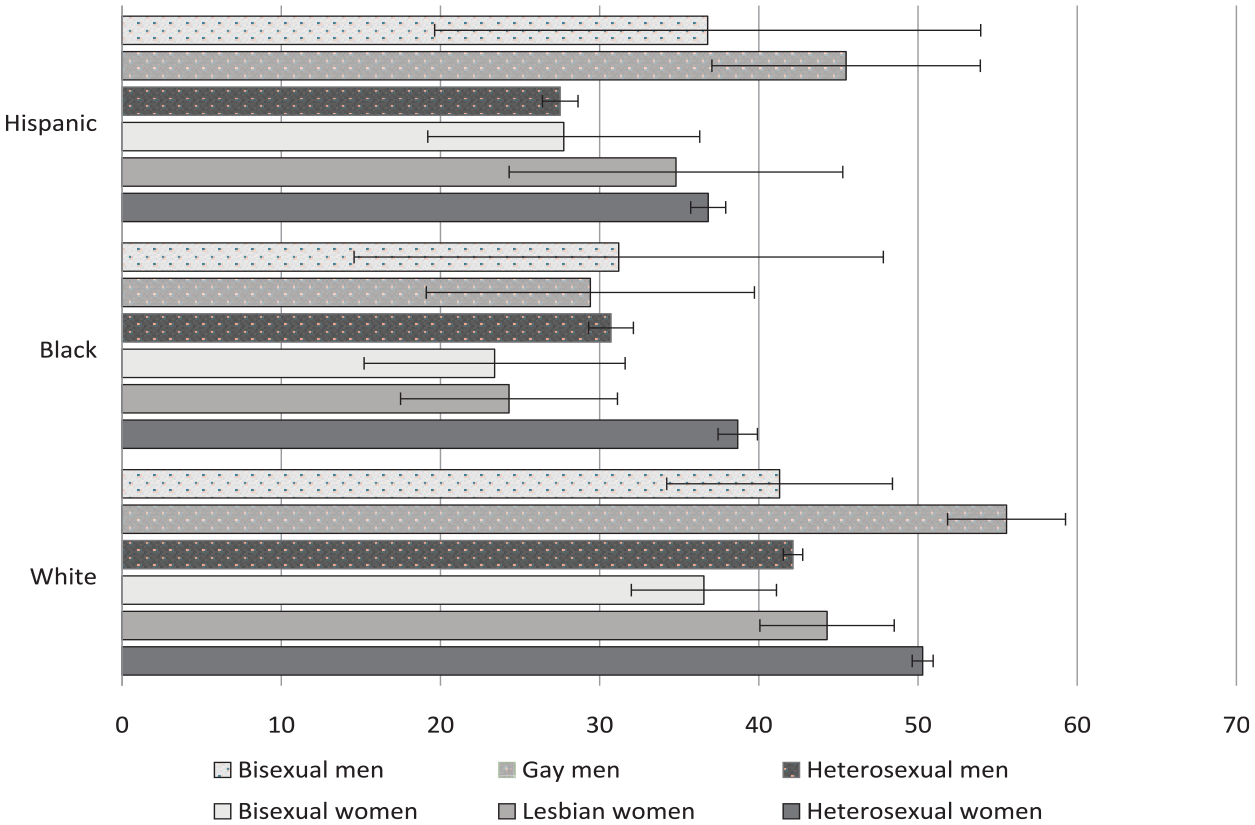
Percent Receiving a Flu Vaccine in the Past 12 Months (% People Vaccinated and 95% Confidence Interval) by Racial-Ethnic, Sexual, and Gender Identities, 2013–2018 National Health Interview Survey.
In addition to showing rates of flu vaccination, Table 1 (for women) and Table 2 (for men) present descriptive statistics for all covariates that might influence vaccination status. Among women, White and Hispanic lesbian women were more likely than their same-race-ethnicity heterosexual counterparts to have a bachelor’s or advanced degree, but no parallel educational advantage was identified among Black lesbian women. Across all racial-ethnic groups, sexual minority women tended to experience more economic disadvantages than heterosexual women, as shown by their higher rates of looking for a job, lower rates of homeownership and insurance coverage, and greater difficulty paying medical bills. Additionally, being Black, Hispanic, or bisexual tended to further exacerbate these economic disadvantages. Regarding noneconomic enabling factors, Hispanic women were more likely than White and Black women to use a language other than English. Meanwhile, having no regular place for care and delaying care for logistic reasons were more prevalent among sexual minority women of color than their heterosexual or White counterparts. Finally, differences in need-based factors (health conditions) were modest across sexual and racial-ethnic identity groups.
For many covariates, patterns in descriptive statistics were similar for men and women. However, a few notable differences emerged. First, although sexual minorities did not have an educational advantage among Black women, they did among Black men—Black gay and bisexual men were more likely than their Black heterosexual counterparts to hold a bachelor’s or advanced degree. Second, regardless of race-ethnicity, gay men were no less likely than heterosexual men to report having a regular place to obtain care. In fact, White and Hispanic gay men were more likely to have a regular place for care than their same-race heterosexual counterparts. By contrast, all lesbian women were less likely than their same-race heterosexual counterparts to have a regular place for care. With these few exceptions, the economic and noneconomic disadvantages associated with bisexual and Black/Hispanic identities were largely similar for men and women.
Findings from Regression and Decomposition Analyses
Table 3 presents results from the logit regression models of flu vaccination for women. Relative to White heterosexual women, all groups of sexual and racial-ethnic minority women had significantly lower odds of receiving a vaccine (Model 1). Black lesbian and bisexual women and Hispanic bisexual women faced particularly large vaccination gaps. Sociodemographic covariates accounted for a sizable portion of the vaccination inequity, as demonstrated by significant changes in the odds ratios (denoted by bold type) for all the minority groups when these factors were included in the analysis (Model 2). When sociodemographic covariates were adjusted, the vaccination disadvantages faced by White lesbian and bisexual women and Hispanic lesbian and bisexual women declined to statistically insignificant levels. Moreover, economic factors also explained a significant share of the vaccination inequities (Model 3). Having a higher level of education, having a job or not currently looking for one, owning a home, being insured, and having less difficulty paying medical bills were all associated with higher odds of vaccination. Together, these factors explained a substantial portion of the disadvantage experienced by racial and sexual minority women except White lesbian women. Furthermore, noneconomic enabling factors such as non-English preference and not having a regular place for care accounted for a somewhat smaller yet still statistically significant proportion of the vaccination gaps (Model 4). Notably, these factors accounted for a larger portion of the vaccination inequity among Hispanic individuals than other racial-ethnic groups.
Logistic Regression Models of Flu Vaccination for Women (Odds Ratios, N = 91,889, 2013–2018 National Health Interview Survey).
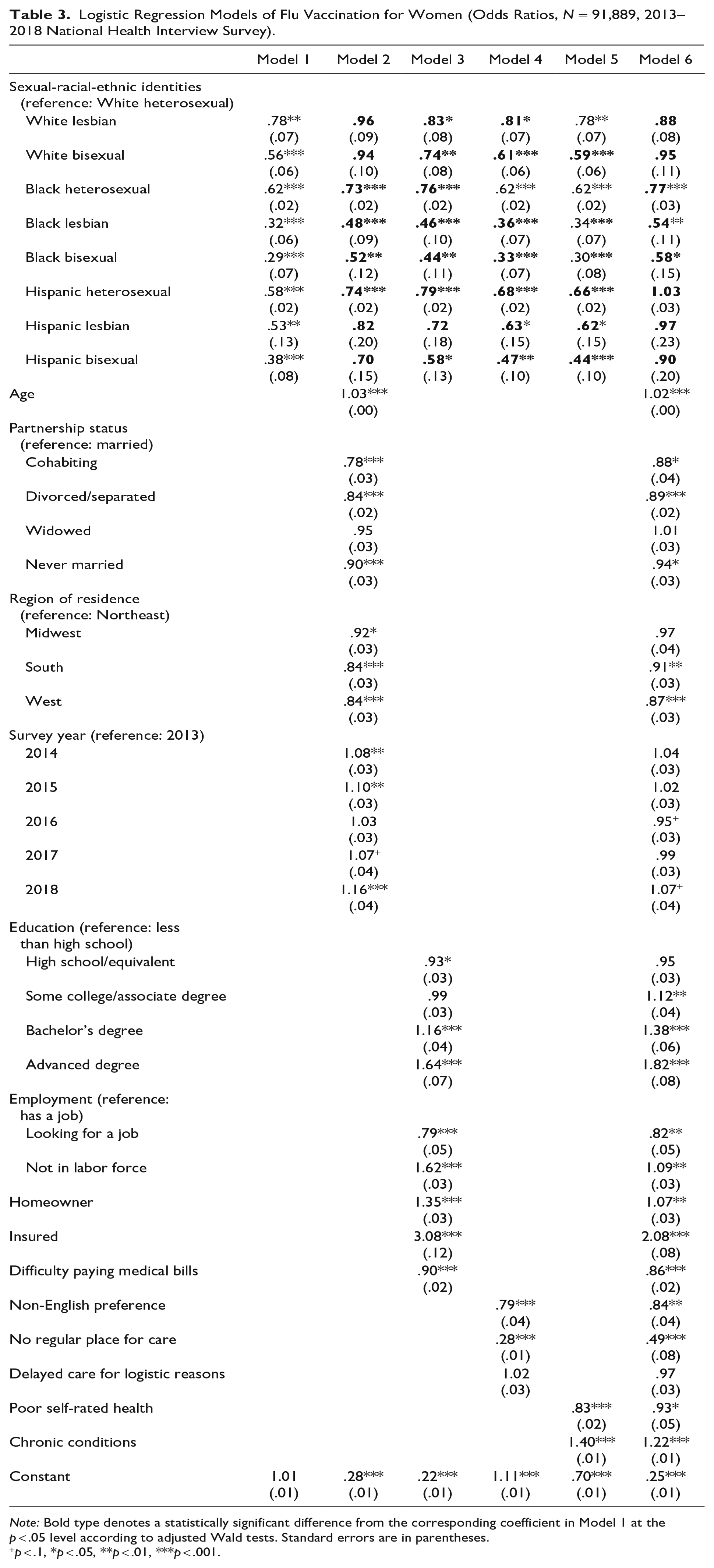
Note: Bold type denotes a statistically significant difference from the corresponding coefficient in Model 1 at the p < .05 level according to adjusted Wald tests. Standard errors are in parentheses.
p < .1, *p < .05, **p < .01, ***p < .001.
Although health conditions (need-based factors) were significantly associated with flu vaccination, they accounted for a limited portion of vaccination inequity across all groups except Hispanic women (Model 5). Interestingly, poorer SRH was related to lower odds of vaccination, whereas number of chronic conditions was related to higher odds of vaccination, possibly because SRH entails mental well-being, and poor mental health may deter health care utilization (Westwood 2016). When all covariates were included in a single model, the vaccination gap largely disappeared for White and Hispanic women regardless of sexual identity (Model 6). However, the disadvantages faced by Black women, especially Black lesbian and bisexual women, remained substantial even when all observed factors were controlled.
To disentangle potential confounding between the economic enabling, noneconomic enabling, need-based, and sociodemographic factors, Table 4 summarizes the KHB decomposition of contributions to vaccination inequity from each type of factor (based on Model 6 in Table 3). Overall, the covariates jointly explained 51.8% to 104.8% of the vaccination gaps between subgroups of minority women and White heterosexual women. For White lesbian and bisexual women, sociodemographic factors made the largest contribution by far; however, economic enabling factors were also responsible for a substantial part of the disadvantage faced by White bisexual women. For Black women, both economic and sociodemographic factors contributed to the vaccination gaps experienced by all sexual identity groups. For Hispanic women, each type of factor explained a nontrivial portion of their disadvantages across all subgroups. Notably, noneconomic enabling and need-based factors were more important for Hispanic women than for Black or White women of the same sexual identity.
Karlson–Holm–Breen Decomposition of Flu Vaccination Inequities for Sexual and Racial-Ethnic Minority Groups by Gender (N = 91,889 for Women and N = 75,019 for Men, 2013–2018 National Health Interview Survey).
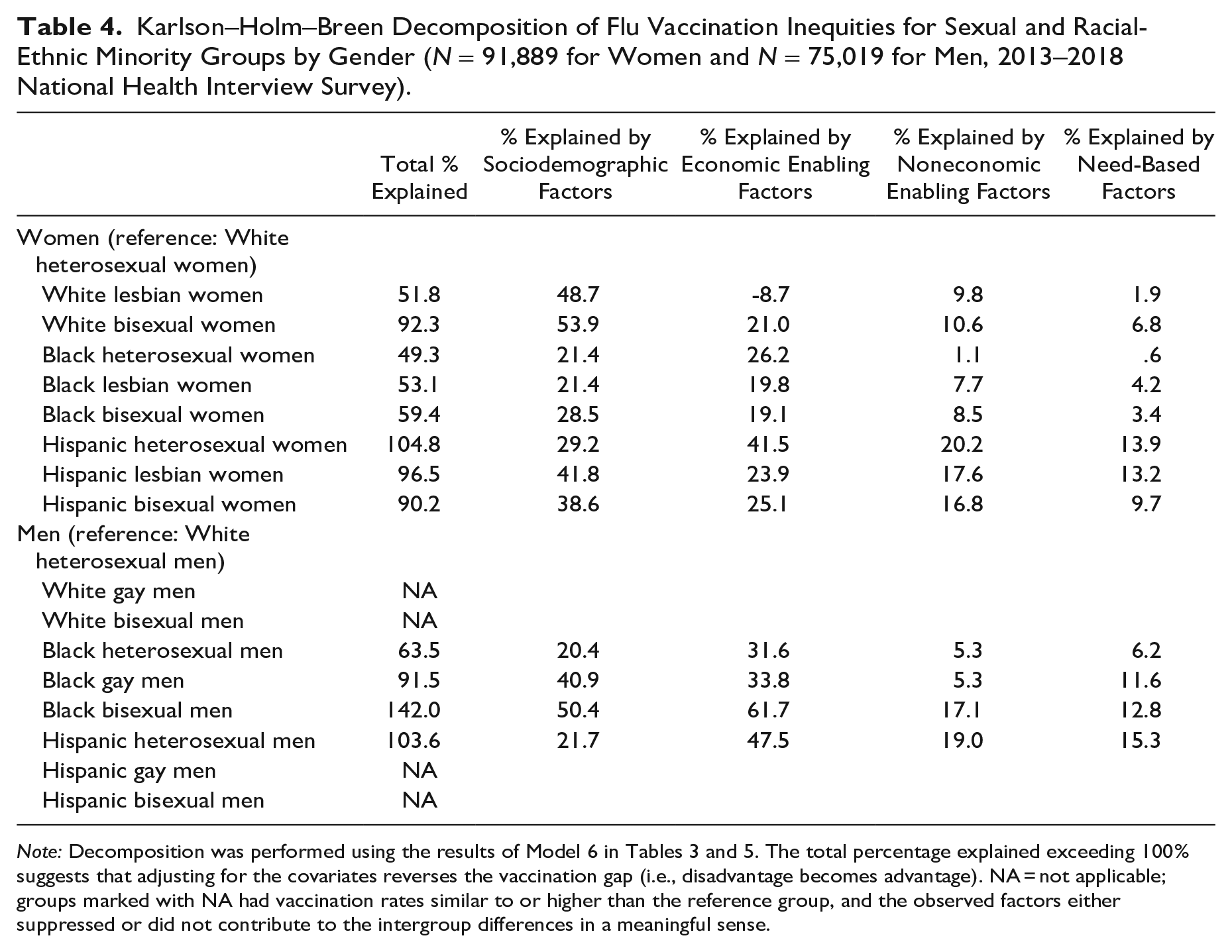
Note: Decomposition was performed using the results of Model 6 in Tables 3 and 5. The total percentage explained exceeding 100% suggests that adjusting for the covariates reverses the vaccination gap (i.e., disadvantage becomes advantage). NA = not applicable; groups marked with NA had vaccination rates similar to or higher than the reference group, and the observed factors either suppressed or did not contribute to the intergroup differences in a meaningful sense.
Unlike women, many groups of racial-ethnic or sexual minority men showed no disadvantage in flu vaccination compared to their White heterosexual counterparts. As Table 5 shows, White gay men had higher odds of vaccination than White heterosexual men, whereas White bisexual men, Hispanic gay men, and Hispanic bisexual men all had odds of vaccination similar to those of White heterosexual men (Model 1). The only three groups with significantly lower odds of vaccination than White heterosexual men were Black heterosexual, Black gay, and Hispanic heterosexual men. Black bisexual men also exhibited lower odds, but their disadvantage did not reach statistical significance, likely due to small sample size. For the four minority groups that experienced vaccination disadvantages relative to White heterosexual men, sociodemographic and economic enabling factors explained most of the disadvantage (Models 2 and 3). When all covariates were included in the model, Black heterosexual men were the only group with a remaining vaccination disadvantage (Model 6). These findings were further confirmed by the results of the KHB decomposition analysis in Table 4.
Logistic Regression Models of Flu Vaccination for Men (Odds Ratios, N = 75,019, 2013–2018 National Health Interview Survey).
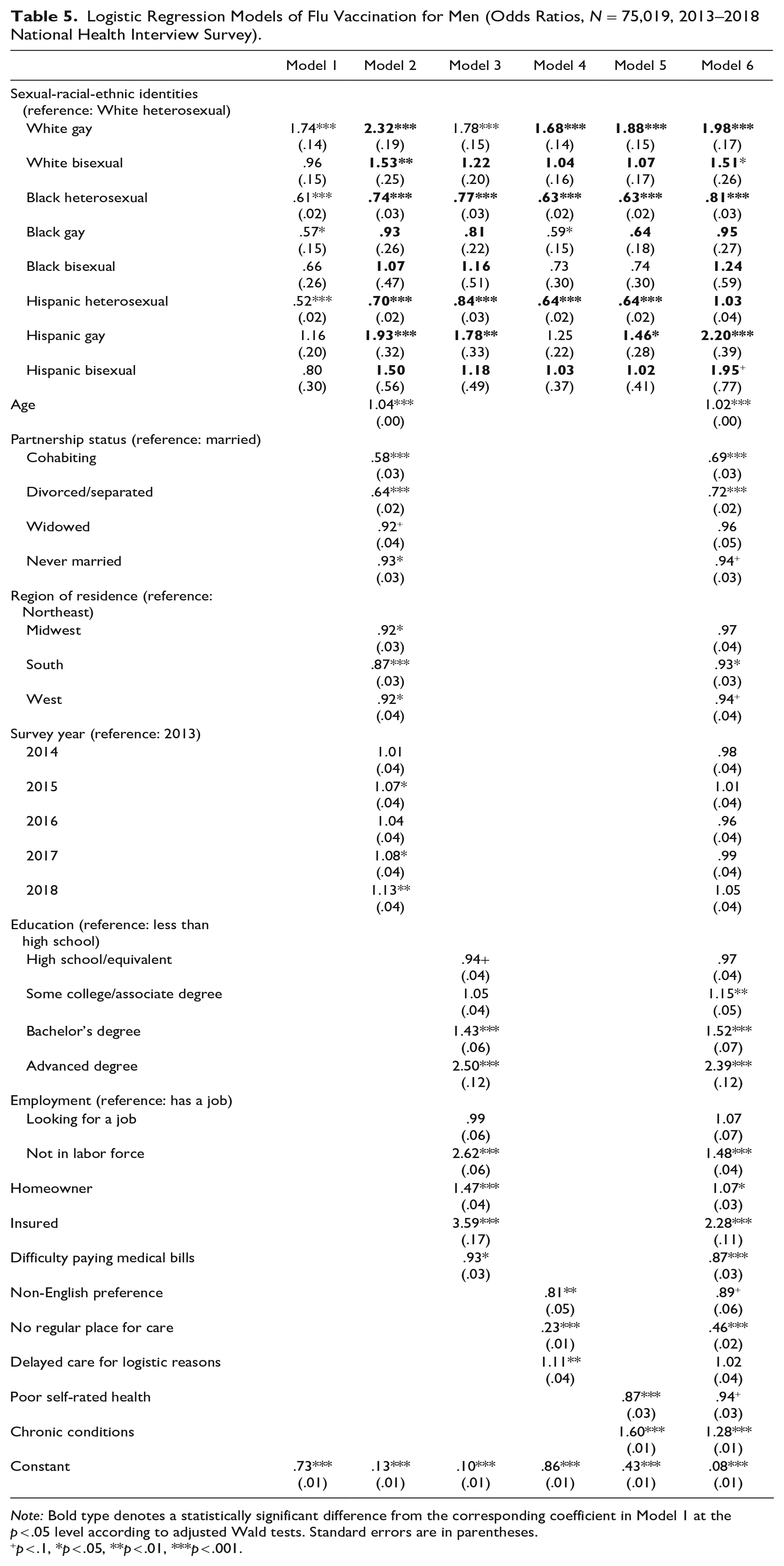
Note: Bold type denotes a statistically significant difference from the corresponding coefficient in Model 1 at the p < .05 level according to adjusted Wald tests. Standard errors are in parentheses.
p < .1, *p < .05, **p < .01, ***p < .001.
Discussion
Population-based studies of health care inequities have long focused on singular dimensions of inequality and have rarely examined how multiple social identities and positions jointly shape health care experiences. Although an emerging group of studies have used an intersectional approach to assess the inequities faced by Black and Hispanic sexual minorities, these studies have primarily examined sexual/reproductive health care while paying little attention to other important health care. Informed by intersectionality and the BMHSU, the current study examines flu vaccination inequities at the intersection of sexual, gender, and racial-ethnic identities. The results show that flu vaccination varied significantly across the intersections of these identities and that the specific intersectional patterns did not necessarily align with prior studies that examined only one of these dimensions. Furthermore, the results indicate that enabling, need-based, and sociodemographic factors all contribute to the inequities in flu vaccination, but the contribution of each of these factors differs according to the respondent’s configuration of identities. Overall, this study advances the understanding of the heterogeneous health care challenges and opportunities faced by diverse minority populations by identifying both hidden vaccination gaps and the mechanisms driving these gaps. Next, I discuss major findings and their implications.
First, the study reveals significant gaps in flu vaccination, with White gay men having the highest vaccination rate and Black bisexual women having the lowest rate. Although earlier studies generally predicted that sexual minorities have less access to and utilization of health services than heterosexual people (Hsieh and Shuster 2021; National Academies of Sciences, Engineering, and Medicine 2020), that men use health care less frequently than women (Courtenay 2000; Springer and Mouzon 2011), and that racial-ethnic minorities have less access to and utilization of adequate care than White people (Smedley et al. 2003; Williams and Sternthal 2010), the current results indicate that these effects are not additive (i.e., sexual minority men of color do not experience the largest vaccination disadvantage). Rather, sexual minority women of color, especially Black bisexual and lesbian women, experience the largest disadvantage. Thus, the current findings support Hypothesis 1 regarding nonadditive notion of intersectionality and reveal that gender modifies the relationship between sexual identity and vaccination across racial-ethnic groups.
Specifically, among Black, Hispanic, and White individuals, sexual minority women had lower vaccination rates than their heterosexual counterparts, but sexual minority men had vaccination rates similar to or higher than their heterosexual counterparts. This gendered pattern may be the result of a combination of factors, including access to culturally sensitive care and the practice of conventional masculinity. Prior research suggests that relative to heterosexual women, sexual minority women perceive less respect in health care encounters and are less satisfied with the care they receive; by contrast, sexual minority men may not experience poorer health services than heterosexual men, and gay men in particular tend to report more positive experiences with patient–provider interactions (Hsieh and Mirzoyan 2021; Smalley, Warren, and Barefoot 2015). This relatively positive experience may be traced back to community building and health information sharing for gay men living with HIV/AIDS, which enhanced awareness of the need to seek culturally sensitive care (Aggleton and Parker 2015; Martos, Wilson, and Meyer 2017). Moreover, previous studies on gender and health have indicated that men who conform to conventional gender norms (e.g., being tough) have fewer health-promoting behaviors, including the use of preventive care (Springer and Mouzon 2011). That heterosexual men are more likely to adopt conventional gender norms than sexual minority men may further explain their lower rates of flu vaccination (Courtenay 2000; Reczek et al. 2018; Umberson et al. 2018). This suggests that oppression/privilege may harm not only subordinate groups but also dominant groups.
Second, in support of Hypothesis 2, the current analysis showed that economic enabling, noneconomic enabling, and need-based factors each explained a significant share of the vaccination gap; in addition, sociodemographic factors played a critical role in the observed inequity. However, the relative importance of these factors varied by the intersection of race-ethnicity, sexuality, and gender. Notably, for Black and Hispanic heterosexual men and women, economic enabling factors outweighed other factors in explaining vaccination disadvantages. For Black gay, lesbian, and bisexual men and women, both economic enabling and sociodemographic factors were important contributors to their disadvantages. For many Hispanic people (including lesbian, bisexual, and heterosexual women and heterosexual men), noneconomic enabling factors such as language preference and need-based factors such as having chronic conditions accounted for the additional gaps in vaccination they faced. By contrast, sociodemographic characteristics were the dominant factors underlying the disadvantages faced by White sexual minority women.
Moreover, vaccination rates among White and Hispanic sexual minority men were higher than or similar to rates among White heterosexual men; none of the focal factors made a significant contribution to either the advantage among White and Hispanic gay men or the lack of advantage/disadvantage among White and Hispanic bisexual men. Overall, some of the current findings align with prior research showing that economic and noneconomic barriers to care underlie the health care inequities experienced by many racial-ethnic or sexual minority groups (e.g., Badgett et al. 2019; Chae and Ayala 2010; Rothstein 2017). However, the intersectional approach used in the current study further reveals that different mechanisms underlie the health care experiences of specific subgroups.
Finally, the results show that when all observed factors were controlled, the only minority groups for which a vaccination disadvantage remained were Black lesbian, bisexual, and heterosexual women and Black heterosexual men. Prior research on flu vaccination found that the reasons for lower vaccine coverage among Black Americans extend beyond economic and logistic barriers. For example, the historical mistrust of medical systems and the government, which is rooted in institutional racism and historical trauma, has contributed to the persistent vaccination inequity faced by Black Americans (Chen et al. 2007; Feagin and Bennefield 2014; Jamison et al. 2019). Moreover, missed opportunities to receive a flu shot during a health visit, likely connected to provider bias against Black patients, may also contribute to vaccination inequity (Hall et al. 2015; Maurer et al. 2014).
For Black sexual minority women, heterosexism and sexism may further complicate health care use, leading to even lower vaccine coverage. As our findings indicate, Black lesbian and bisexual women faced the largest remaining gap in vaccination rates after covariates were adjusted. This supports the core intersectionality tenet that multiple systems of power inequality intersect and reinforce one another to influence life circumstances (Collins and Bilge 2016; Misra et al. 2021). Black sexual minority women’s social position may expose them to a greater level of provider prejudice and medical mistreatment for a combination of racist, sexist, and heterosexist reasons that cause delay or avoidance of health encounters. For example, providers’ presumptions of lower socioeconomic status and heterosexuality based on patients’ racial identification and biological sex and patients’ sense of not belonging in health care spaces due to their gender expression and sexual identity/behavior may all deter the utilization of health services (Agénor et al. 2015; Hsieh and Shuster 2021). Findings from this study suggest that policies that enhance economic equity and reduce costs of health care, more public health outreach to communities of Black sexual minority women, and better training on structural inequality and cultural sensitivity/humility among health professionals may facilitate reducing vaccination inequities. This study confirms that intersectionality as a critical inquiry and praxis tool is necessary for understanding complex power relations and their joint influence on health and for guiding equitable interventions (Bowleg 2021).
This study has several limitations. Due to insufficient sample size or lack of appropriate measures, the analysis focused on a limited number of intersecting identities and did not consider certain groups that experience severe health care inequities, such as Native Americans and gender-diverse populations. To better understand health care and health inequities, future data collection efforts should adopt an intersectional lens by, for example, oversampling not only racial-ethnic minorities but also sexual and gender minorities. Without adequate sampling and questionnaire designs, population-based research will continue to overlook groups whose members inhabit multiple marginalized positions. Moreover, although this study tested a range of proximal, individual-level factors (economic enabling, noneconomic enabling, and need-based factors) linked to vaccination inequities, distal factors that structure/contextualize those proximal factors, such as residential segregation that leads to unequal access to health care facilities by race-ethnicity and socioeconomic status and discrimination in health care and labor market, were not analyzed because NHIS lacks the required measures. The current study provides initial evidence on intersectional inequities in preventive care utilization in the context of the literature on structural barriers to care. When appropriate data are available, future research should consider testing how structural/contextual factors influence health care use (Agénor 2020).
Despite these limitations, the current study contributes to a more nuanced understanding of health care inequities by identifying previously overlooked vaccination gaps and showing that different factors underlie those gaps across diverse populations. Highlighting inequities structured by oppression and privilege, the findings offer new evidence that can inform future public health efforts for equitable vaccination coverage and that should encourage future health care research to incorporate an intersectional perspective.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465231199276 – Supplemental material for Unpacking Intersectional Inequities in Flu Vaccination by Sexuality, Gender, and Race-Ethnicity in the United States
Supplemental material, sj-docx-1-hsb-10.1177_00221465231199276 for Unpacking Intersectional Inequities in Flu Vaccination by Sexuality, Gender, and Race-Ethnicity in the United States by Ning Hsieh in Journal of Health and Social Behavior
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: U.S. Department of Health and Human Services, U.S. Public Health Service, Agency for Healthcare Research and Quality R03 HS029329.
Supplemental Material
The Appendix is available in the online version of the article.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.