
Abstract
Introduction
Disclosing medicinal cannabis (MC) use to friends, family, healthcare professionals or other networks is a challenging decision influenced by the context and audience. Patients may choose to discuss MC with health professionals to receive a recommendation or seek medical guidance on routes of administration, dosing, and adverse effects (Boehnke et al., 2023; Kurtzman & Greene, 2023). Individuals may discuss their MC use with friends and family to seek emotional support and information, all of which shape their decisions (Sena et al., 2024; Shrestha et al., 2024). Interviews with 23 female MC users in New Zealand (NZ) found that their decisions to seek MC prescriptions were most influenced by the level of support received from their social circles (Withanarachchie et al., 2025).
Social stigma remains a key barrier to disclosing MC use in social and healthcare settings (Dahlke et al., 2024; King et al., 2024). Despite legal acceptance of MC, stigma persists because non-medical cannabis use remains illegal in many jurisdictions including in NZ (Borojevic & Söhner, 2025). Most existing research on MC non-disclosures has focused on disclosure in healthcare settings (Fordyce, 2024; Vidot et al., 2024), identifying stigma, fear of criminality, and patients’ perceptions that their physicians would not prescribe as reasons for non-disclosure (Borojevic & Söhner, 2025; Morris et al., 2024). Physicians’ reluctance to prescribe MC is a known barrier to discussing MC use in clinical practice (Martin et al., 2025; Syed et al., 2025), which may prevent patient disclosures of MC use. Limited clinical trial evidence beyond epilepsy, chronic pain, spasticity, and cancer-related nausea and vomiting (Hoch et al., 2024), highlights the need for medical oversight to ensure safety and risks are monitored. Patients accessing MC from illegal markets also risk exposure to contaminated products of unknown potency and combination of cannabinoid compounds (Raymond et al., 2021; Therapeutic Goods Administration, 2021). While MC patients engage their families for support (Lertaroonchai et al., 2024; Morris et al., 2024), studies show that they avoid situations where they might face judgement from others (Dahlke et al., 2024) and have experienced strained relationships due to their MC use (Borojevic & Söhner. 2025). While cannabis stigma can drive non-disclosure in personal and healthcare settings (Borojevic & Söhner, 2025; Morris et al., 2024; Pomey et al., 2024), little research exists whether vulnerable or minority demographic groups are more likely to conceal their use due to stigma and institutional related barriers.
Research has found that employees may not disclose their MC use due to concerns about employer perceptions, drug testing policies, or fears they be viewed as less competent or reliable (Boehnke et al., 2023). The literature on accommodating MC use in workplaces is emerging as MC schemes become more common, with implications for both employees (Lee et al., 2025) and employers (Winn, 2020), particularly in safety-sensitive jobs or duties that involve operating a motor vehicle or machinery. MC users may experience side effects (Bar-Lev Schleider et al., 2022; Rychert et al., 2020), raising employers’ concerns about potential impairment associated with cannabis use (Hazle et al., 2022). Side effects reported by MC users i.e. sedation, nausea/vomiting, dizziness, and euphoria, may manifest as poor focus, slower reaction times, difficulty driving or operating machinery safely, and an increased risk of falls in workplaces (O’Neil et al., 2023).
Disclosing MC use to government services may be influenced by how governments and welfare agencies support – or fail to support – MC access, as well as the clarity and consistency of policies. While 47 US states have legalised some forms of MC, illegality at the federal level creates uncertainty for patients and providers when conflicting with state regulations (Hong et al., 2024). In a different approach, Germany has integrated MC into their healthcare system, with public health insurance covering MC prescription costs for terminally ill patients, on a case-by-case basis, and provided other treatments are unsuitable (Woźniak, 2023). Many patients rely on government pensions or disability allowances to fund MC products due to chronic medical conditions (Erku et al., 2022; Olson et al., 2023), however little is known about their disclosure decisions in these settings.
New Zealand Context
The New Zealand Medicinal Cannabis Scheme (NZMCS), introduced in 2020, allows patients to access regulated MC products in pharmaceutical-grade and herbal forms. At the time of writing (July 2025), there are 56 medicinal cannabis products consented for sale under the MCS. Products are available with a prescription from registered physicians and purchased from pharmacies or dispensaries owned by cannabis clinics (Withanarachchie et al., 2023). While most MC consumers self-medicate by accessing the illegal market, the proportion of MC prescription holders is increasing fast, reflecting growing engagement with the NZMCS. The New Zealand Drug Trend Survey (NZDTS) recently reported that the proportion of NZ MC prescription holders increased from 2% in 2020 to 37% in 2024, reflecting a growth in the availability of MC products and prescriptions. However, many MC users surveyed (n = 1,742) reported that they felt their doctor would not prescribe (42%) or were too embarrassed to ask (40%) (Rychert et al., 2025). Recent analysis of NZ MC prescription records showed women received 42% of MC prescriptions in the past year (2023/2024) and Māori remain underrepresented in legal prescriptions despite reporting higher rates of MC use (Pledger et al., 2016).
Most MC products are considered unapproved medicines in NZ and are not government-subsidised (Withanarachchie, Rychert, & Wilkins. 2022). In some cases, government agencies cover the costs of MC with a physician’s recommendation and when other subsidised treatments have been ineffective (ACC, 2023; MSD, 2023). Workplace impairment policies are also determined at an individual business level, with health and safety responsibilities shared between employer and employees under the Health and Safety at Work Act 2015 (WorkSafe, 2020). Therefore, workplace MC policies can vary widely and are contingent on the employer’s decisions.
When receiving hospital or general health treatment, MC disclosures are often deemed necessary for safe prescribing and coordinated care for patients, while disclosure within personal networks may be a catalyst for garnering support. MC disclosure in workplaces and to government services may be necessary if a subsequent drug test is required, or it is relevant to accessing entitlements such as disability allowances and jobseeker support or employment protections such as rationale for a positive drug test result. Stigma, fear of judgement and negative employment outcomes persist as barriers, especially among marginalised groups. For MC users accessing illegal markets, disclosure carries the risk of criminalisation and receiving contaminated products with unverified concentration of active ingredients (Raymond et al., 2021). Existing research on MC disclosures has been largely limited to healthcare settings and has not examined levels of disclosure among vulnerable and minority groups. Consequently, this paper seeks to explore (1) the demographic predictors of MC disclosures in (i) healthcare, (ii) personal networks, (iii) employers, and (iv) government social services; and, (2) reasons for MC non-disclosures among different demographic groups, including vulnerable and minority groups.
Methods
Survey Design
The New Zealand Drug Trends Survey (NZDTS) is an anonymous online survey promoted through a paid campaign on MetaTM. It provides an annual snapshot of drug use patterns and drug market trends in NZ (e.g. prices, availability, drug harm). Recruitment focuses on individuals who are 16+ years, residing in New Zealand, and who express interest in activities associated with substance use (e.g., entertainment, nightlife, certain music genres). No financial incentive for participation is offered and completed surveys are audited to remove duplicates or incomplete surveys. Data for this paper was collected from 20 February to 3 July 2024. Of the 12,763 surveys initiated, 10,781 individuals completed the survey. Surveys were audited for quality and completion levels, and no IP addresses were saved or stored. A custom software solution converted IP addresses into non-reversible codes to detect potential duplicate responses. A total of 1,982 responses were excluded, including 18 duplicates, 1,964 responses without invalid ages (no age provided or outside of the 16-100 years range) or surveys that were less than 16% completed. The final sample was 10,781 completed surveys, with the median completion time of 12 minutes.
Measures
Demographics
Participants were asked their age (open text field), gender (female, male or other gender), ethnicity (Māori, NZ European/Pākehā, Pacific Peoples, East Asian, Southeast Asian, South Asian, European, American/Canadian, Australian, Latin American, Middle Eastern, African, or other), highest level of education (University, High school, Polytech/Trade School, Primary/Intermediate, or none), main occupation (Working full-time/part-time, Student, Retired/Parenting/Unpaid work, Sickness, Unemployed), and personal income before tax (No personal income, $30,000 or less, $30,001 to $60,000, $60,001 to $80,000, $80,001 to $100,000, $100,001 or more, or prefer not to say).
Cannabis and Medicinal Cannabis Use
Individuals who used cannabis in the past six months were asked how much of this cannabis was for “medicinal reasons” and could choose from: “none”, “a little”, “some”, “most”, or “all”.
Cannabis Use Frequency (including for Medicinal Purposes)
Individuals who used cannabis (for any reason) in the past six months were asked about their use frequency and could choose from the following options: “once or twice (in the last 6 months)”, “monthly”, “once or twice a week”, and “daily”.
Conditions Indicators
Participants who used MC in the past 6 months were asked to select all conditions they treated with MC (“women’s health”, “pain”, “sleep”, “mental health disorders”, “substance use disorders”, “gastrointestinal conditions”, “neurological conditions”, “cancers”). Participants were asked whether they had a medical diagnosis for each condition(s) and they chose (yes or no).
Drug Testing Indicators
Participants were asked whether they had experienced a drug test, either at work or in any other place and could select either, “no”, “yes - in the past 12 months”, or “yes - in the previous years.”
Prescription Status
Participants who indicated that they used any of their cannabis for medical reasons were asked if they had a MC prescription and could select: “yes - in the last 6 months”, “yes” - previously”, “no - haven’t asked”, or “no - asked but refused by a medical professional.”
Medicinal Cannabis Disclosures and Non-disclosures
Participants who had used any of their cannabis medicinally in the past 6 months were asked if they had disclosed their MC use to a “spouse/partner”, “friends, other family”, “employer”, “health professional (doctor/nurse)”, “government social services (ACC, Work and Income)”, or have not disclosed to anyone. Respondents who did not select all of the disclosure options were asked about their reasons for not sharing with more people and could select multiple responses (i.e., “fear of police/legal concerns”, “worried my employer might find out”, “friends and family will judge me”, “I prefer to keep it private”, “it is considered taboo in my culture/religion”, and “it is less accepted for women to use it”).
Data Analysis
Twelve separate logistic models were constructed to predict disclosure of MC use and reasons for non-disclosure of MC use among the sample of MC users who used “most” or “all” of their cannabis for medicinal purposes. The categories, “spouse/partner” and “friends and/ other family” were collapsed to form “friends and family”. The following binary (yes/no) outcomes were examined for disclosure of MC use to: “anyone”, “health professionals”, “friends and family”, “employers”, and “government social services”. Similarly, for reasons for non-disclosure: “fear of police/legal concerns”, “worried my employer might find out”, “friends and family will judge me”, “I prefer to keep it private”, “it is considered taboo in my culture/religion”, and “it is less accepted for women to use it”. The following covariates were included in the analyses: Gender – Female vs. Males and other genders (reference group), Age group (16-29, 30-59, [60+ years reference), Education level (University degree vs. High school, none (reference)), Occupational status (Working or studying vs. Not in the workforce (reference)), Ethnicity (Māori (indigenous people of NZ) vs. non-Māori (reference)), NZ European/Pākehā vs. non-NZ European/Pākehā (reference)), Pacific (vs. non-Pacific (reference)), Asian vs. non-Asian (reference)), Residential area (Small town, Rural area vs. City (reference),), Annual income (>$60,000 vs. ≤$60,000(reference),), Medical conditions treated with MC (“Women’s health”, “Pain”, “Sleep”, “Mental health disorders”, “Gastrointestinal conditions”, “Neurological conditions”, “Cancer”), Prescription status for cannabis (Yes vs. No (reference)), and Medical diagnosis status (Yes vs. No (reference)), Cannabis use frequency (Daily vs. Once or twice in the last 6 months), Daily vs. monthly), Daily vs. once or twice a week). For the “it is less accepted for women to use it” model, the sample was restricted to female participants, and gender was excluded as a covariate.
Prior to model interpretation, we assessed multicollinearity among predictor variables using Variance Inflation Factors (VIF). VIF was low (less than (2) for all variables in each of the models indicating no concerning multicollinearity among predictors. Data analysis was restricted to participants who responded “all” or “most” to the question: “How much of the cannabis you used in the past six months was for medicinal reasons (to treat a physical or mental health condition or symptom)?” This was done to ensure the findings represented the experiences of those who were primarily using cannabis for health reasons. Each model reported odds ratios with corresponding 95% confidence intervals. All statistical analyses were performed using R software (R Core Team, 2023).
Results
Sample Demographics
Sample Characteristics of Participants Who Used “all” or “Most” of Their Cannabis for Medicinal Reasons
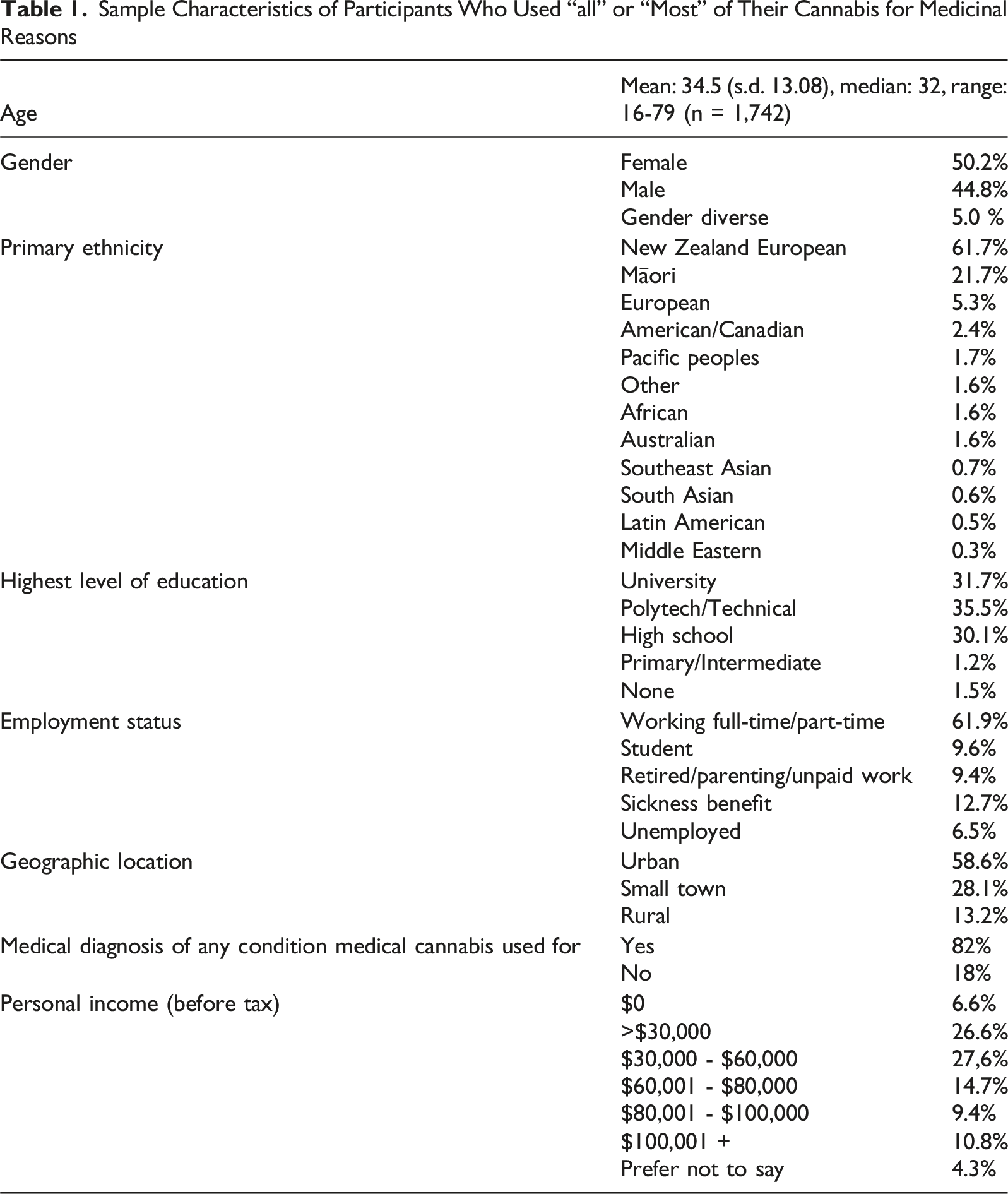
Among New Zealand European MC users (n = 1,385), 1,322 reported disclosing use to anyone: 791 (60% of those who disclosed; 57% of all NZ Europeans) to healthcare providers, 1,314 (99%; 95%) to family and friends, 312 (24%; 23%) to employers, and 164 (12%; 12%) to government or social services. Among Māori (n = 350), 333 disclosed to anyone: 193 (58% of those who disclosed; 55% of all Māori) to healthcare providers, 330 (99%; 94%) to family and friends, 80 (24%; 23%) to employers, and 48 (14%; 14%) to government or social services. Among Asian respondents (n = 38), 32 disclosed to anyone: 19 (59% of those who disclosed; 50% of Asians) to healthcare providers, 31 (97%; 82%) to family and friends, 7 (22%; 18%) to employers, and 4 (13%; 11%) to government or social services. Among Pacific Peoples (n = 52), 48 reported disclosing to anyone: 28 (58% of those who disclosed; 54% of Pacific Peoples) to healthcare providers, 47 (98%; 90%) to family and friends, 15 (31%; 29%) to employers, and 8 (17%; 15%) to government or social services (Table 2).
Overall, most MC consumers disclosed their use to family and friends (>90% in all groups), around half to healthcare professionals (55-57%), and fewer to employers (18-31%) or government and social services (11-17%). These patterns were broadly similar across all the ethnic groups surveyed, despite smaller sample sizes for Asians and Pacific Peoples.
Medical Conditions Treated With MC
MC was mostly used to treat mental health disorders (73.8%), sleep (71.6%), and pain (59.5%) conditions. Approximately a fifth (22.4%) were using MC to treat women’s health issues. Fewer participants used MC for gastrointestinal issues (14.8%), neurological conditions (13.5%), and substance use disorders (10.4%). MC was least used to treat cancer, reported by only 2% of respondents.
MC Disclosures
MC Disclosures to Any Group
MC prescription holders were four times more likely to disclose their MC use to others (OR = 4.13). Similarly, those with a medical diagnosis for a given condition were more likely than those without a diagnosis (OR = 2.16) to disclose their MC use. Finally, university degree holders were more likely than those without a degree to disclose their MC use (OR = 1.78). Conversely, Asians (OR = 0.28), those treating cancers (OR = 0.30), and those who consumed cannabis for only once or twice in the last 6 months (OR = 0.18) were less likely to disclose their use to others compared to daily users.
Disclosures to Health Professionals
University degree holders (OR = 1.32), those subjected to a drug test in the past (OR = 1.30), those treating pain (OR = 1.61), neurological conditions (OR = 1.87), or substance use disorders (OR = 1.43) those with a MC prescription holders (OR = 4.06), or with a medical diagnosis ((OR = 2.24) were all more likely to have disclosed their MC use to a health professional. In contrast, individuals who were working or studying (OR = 0.55), with an income of $60,001+ (OR = 0.69), consumed cannabis once or twice a week (OR = 0.53), monthly (OR = 0.40), and only once or twice in the last 6 months (OR = 0.36) were less likely to have disclosed in healthcare settings compared to daily users.
Disclosures Within Personal Networks
MC prescription holders (OR = 3.04) were three times more likely to disclose their MC use to personal networks, and those with a medical diagnosis were also more likely to disclose to personal networks (OR = 1.72). Asians (OR = 0.28), individuals treating cancers with MC (OR = 0.34), those who consumed cannabis once or twice in the last 6 months (OR = 0.24) were less likely to disclose to personal networks.
Disclosures to Employers
Pacific Peoples (OR = 1.98), MC prescriptions holders (OR = 2.46), and those treating pain conditions (OR = 1.57) were also more likely to disclose in workplace settings. Tertiary-educated individuals (OR = 0.62) and individuals who consumed cannabis once or twice in the last 6 months (OR = 0.40) were less likely to disclose to employers compared to daily users.
Disclosures to Government/ Social Services
MC prescription holders (OR = 2.96) and individuals treating mental health disorders (OR = 1.89) were more likely to disclose to government support services. Respondents working or studying (OR = 0.29), who consumed cannabis once or twice a week (OR = 0.37), and those earning $60,001+ (vs. below this threshold) (OR = 0.55) were less likely to disclose to government services.
Reasons for MC Non-disclosure
Many respondents reported multiple reasons for non-disclosure within the same context. Among participants who did not disclose MC use, 44.61% endorsed more than one reason for non-disclosure. The most common co-occurring reasons were concerns about “Fear of police/legal concerns” and “I prefer to keep it private” (24.13%) followed by “Fear of police/legal concerns” and “Worried my employer might find out” (23.01%) (Table 3).
Fear of Police/Legal Concerns
Women (OR = 1.32), Māori (OR = 1.49), those treating pain conditions (OR = 1.29), mental health disorders (OR = 1.33), gastrointestinal conditions (OR = 1.36), and neurological conditions (OR = 1.79) were more likely not to disclose their MC use due to “fear of police or legal consequences”. MC prescription holders (OR = 0.48), individuals aged 30-59 years old (compared to 60+ years) (OR = 0.57), and those who consumed cannabis monthly (OR = 0.48), or once or twice a week (OR = 0.56) were less concerned about these consequences compared to daily users.
Worried My Employer Might Find Out
Māori (OR = 1.38), those who had been drug tested in the past 12 months (OR = 1.73), and high-income earners (OR = 1.50) were more likely to be concerned that their employer would discover their MC use. Individuals who consumed cannabis once or twice a week (OR = 0.59), monthly (OR = 0.55) or once or twice in the last 6 months (OR = 0.44) were less likely than those who consumed cannabis daily or near daily to worry their employer would find out.
Friends and Family Will Judge Me
Tertiary educated individuals (OR = 1.47), New Zealand European (OR = 1.59), and those treating mental health disorders (OR = 1.66) were more likely not to disclose because they feared judgement from their friends and family. Māori (OR = 0.69) and respondents treating pain conditions (OR = 0.74) were less concerned about judgement from personal networks.
I Prefer to Keep it Private
Women (OR = 0.732), those who had been drug tested in the prior 12 months (OR = 0.76) or in the past (OR = 0.60), MC prescriptions holders (OR = 0.77), and those who consumed cannabis once or twice a week (OR = 0.47) were less likely than daily users not to disclose their MC use because they wanted to keep their MC use private.
Cultural/Religious Taboo
Asians (OR = 2.96) were nearly 3 times more likely not to disclose due to “cultural and religious reasons”. Those treating sleep conditions and those who consumed cannabis once or twice a week (OR = 0.47) or once or twice in the last 6 months (OR = 0.26) were less likely to choose this option as a reason for non-disclosure compared to daily users (OR = 0.56).
Less Accepted for Women to Use it
Of the 735 women who had not disclosed to anyone or not all groups, 148 (20%) cited the reason for non-disclosure was because it was less accepted for women to use MC. Those with a MC prescription (OR = 0.57) and women who consumed cannabis monthly (OR = 0.36) or once or twice in the last 6 months (OR = 0.41) were less likely to report this, while women treating substance use disorders (OR = 2.02) were more likely to choose this reason.
Discussion
We found that MC prescriptions holders and those with medical diagnoses were more likely to disclose their medicinal cannabis use to others. This is likely because their conditions and treatments have been formally legitimised through the healthcare system, contributing to less fear around open dialogue. MC prescription holders may also perceive legal MC routes as safer, quality-controlled, and free from criminal implications (Sinclair et al., 2023; Withanarachchie et al., 2025), making it more socially acceptable to discuss.
Around a fifth of women who had not disclosed their MC to anyone or not to all groups reported their reason was the societal view that MC use was not acceptable for women to use. Though women are a growing demographic for MC use in NZ and overseas (Glazer & CannaWay Clinic, 2022; Gulbransen et al., 2020), fear of judgement may prevent the disclosure of their MC in health settings (Fordyce, 2024; Sinclair et al., 2023). Our previous work has found women MC users perceive less support from their personal networks for MC use (Withanarachchie et al., 2025). Gendered expectations around caregiving, femininity, and motherhood also subject women to heightened scrutiny and social repercussions for MC use (Withanarachchie et al., 2025). Additionally, women may be concerned that their MC disclosures may reflect poorly on their caregiving, thereby compromising their parental rights (Boyd, 2019; Kwak, 2017).
University degrees holders were more likely to disclose their MC use to others, including health professionals. This is consistent with prior research indicating that university students generally support MC legalisation, recognise the therapeutic value of MC, and believe MC should be integrated into medical education (Jacobs et al., 2022; Paiva et al., 2024). However, most of these studies have been with medical students who may be more receptive to MC and have greater health literacy than other students. Employees and students were less likely to disclose to employers, and high-income earners were more likely not to disclose because they were worried their employers would find out, presumedly due to concerns that it would damage their professional reputation and future advancement (Sinclair et al., 2023).
Asian respondents were much less likely to disclose their MC use and more likely to cite cultural or religious beliefs as reasons for non-disclosure. For Chinese respondents, for example, this may reflect broader disapproval of cannabis within Chinese culture (Chung et al., 2022) and fear of government surveillance and repercussions based on historical experience in NZ and mainland China, along with healthcare barriers driven by social stigma and religious beliefs (Ransing et al., 2022). Māori were more likely to cite fear of police and legal consequences as reasons for non-disclosure. Māori (Rapana et al., 2022) and MC patients from racialised backgrounds (Fataara et al., 2023) are disproportionately represented in cannabis-related criminal offences and face systemic barriers in healthcare access (Gibson et al., 2024), which may deter disclosures for fear of repercussions. Lower concern among Māori about facing judgement from their personal networks for MC use may reflect high prevalence of MC use in Māori communities (Pledger et al., 2016). Interviews with Māori cancer patients and their whanau (families) (n = 24) highlighted a shared cultural emphasis on holistic approaches to managing pain, with some using cannabidiol and other MC products to support pain relief and improve sleep (Signal et al., 2023). Prior to the NZMCS, Māori communities also submitted recommendations urging the MC advisory committee to engage with Māori traditional healers and their patients to consider the place of cannabis in Rongoā Māori, their traditional healing system (Ministry of Health, 2019; Taurua, 2018).
Pacific Peoples were more likely to disclose their MC use to their employers. While this is unexpected given reported workplace discrimination faced by Pacific Peoples, (Park, H. M., & Hughes, 2020; Haar, 2023), such experiences may encourage greater openness with employers to prevent misunderstandings or to explain positive workplace drug testing results. In the 2012/2013 New Zealand Health Survey (aged 15+ years), 31% of Pacific adults who reported using cannabis in the past 12 months indicated it was for medicinal purposes (Ministry of Health, 2015). To our knowledge, no other recent studies have focused on Pacific People’s relationships with MC use, and this warrants further research.
Workplace drug testing is an important factor influencing MC disclosures, even for legally prescribed patients. Although evidence from New Zealand is limited, international studies and commentaries suggest that employees may face discriminatory or unfair employment practices and social stigma from MC use and disclosure (Oyaas, 2016; Weisenfeld, 2020; Sinclair et al., 2022; 2023). Disclosures are further complicated by unclear and inconsistent legal frameworks, which provide little guidance for employers on managing MC use in the workplace, particularly in relation to balancing employment protections and occupation safety (Hazle et al., 2022; Lydon, 2022).
In New Zealand, there is no specific employment laws regulating workplace drug testing; rather, the law requires employees to perform their work free from impairment that can compromise health and safety and obliges employers to provide a safe working environment. Therefore, individual businesses are responsible for developing their own impairment policies and conduct drug testing as they see fit (WorkSafe, 2020). Workplaces involving safety sensitive roles such as driving vehicles or operating heavy machinery may implement more frequent or comprehensive impairment testing. Without clear legal thresholds to distinguish impairment from the mere presence of THC, current drug testing methods which rely on urine or saliva may detect THC long after consumption, however, cannot reliably detect functional impairment (Hazle et al., 2022), which is critical in safety-sensitive roles. Unclear regulatory parameters may contribute to ongoing stigma and affect workplace MC behaviours with employees fearing negative employment consequences from MC disclosures.
Respondents treating cancer with MC were less likely to disclose their use to others. While research has outlined why cancer patients choose to use MC (Morris, Loyer, & Blunk, 2024; Nayak, Revette, & Chai, 2023), stigma and fear of judgement has also been found to hinder open discussions by patients in these studies. Similar disclosure patterns are reflected by cancer patients using complementary alternative medicines (CAM). A systematic review of 30 studies (n = 8,721 total participants) found that non-disclosure of CAM to healthcare providers was common due to perceptions that their physicians would be unreceptive or lack the knowledge to support CAM use (Akeeb et al., 2023). Cancer patients also feared judgment, disapproval, or stigma from both healthcare professionals and caregivers, contributing to non-disclosure of CAM use (Ashrafizadeh & Rassouli, 2024).
While no studies have directly examined how prior exposure to drug testing influences MC disclosures in clinical settings, our findings suggest that individuals familiar with drug testing may be more likely to disclose sensitive information in institutional environments. While drug testing is associated with policing fitness to work or drive, some may have encountered it in clinical settings e.g. pain management or opioid monitoring, where cannabis use is detectable and testing is understood as a routine part of care. A recent study of 145 US patients using prescribed long-term opioids for pain found that most considered urine drug testing a routine and necessary part of clinical care (Wyse et al., 2021). MC is frequently prescribed for pain-related (Mills et al., 2024; Tait et al., 2025) and neurological conditions (Cowley et al., 2025; Szejko et al., 2024), and emerging MC clinical trial evidence for these conditions (Hoch et al., 2024), may support more open patient-provider discussions about MC.
The upcoming implementation of roadside drug testing legislation in New Zealand in late 2025 ((Land Transport (Drug Driving) Amendment Bill)) has important implications for medicinal cannabis users, particularly those employed in safety-sensitive occupations such as professional drivers (e.g., truck drivers and couriers), and whether they should disclose their MC use to their employer. Under the Act, if two oral fluid tests return a positive result, the driver is issued an infringement notice and a mandatory 12-h driving prohibition or face criminal charges depending on drug concentration. Drivers may then elect for a blood sample test to confirm drug concentration and level of impairment (Land Transport Act, 1998, 57A (3)). If it is an infringement-level offence, drivers using prescribed medicines (including medicinal cannabis) can submit a medical defence to the Police Infringement Bureau by providing a copy of the prescription and dispensing label and show that they followed the physician or manufacturer’s instructions (New Zealand Police, n.d). This must be done before the infringement is paid or transferred to the Fines Collections Unit and does not apply to criminal charges. If the defence is rejected, the driver may contest it in court. When the legislation was first developed in 2022, MC was less commonly prescribed, and testing measures were implicitly designed to target illegal use. As MC prescriptions have significantly increased (Rychert & Wilkins, 2024), legally prescribed users may face legal and professional consequences such as temporary driving bans, employers’ disciplinary processes, and the burden of proving therapeutic cannabis use in court proceedings.
Those treating mental health conditions were more likely to disclose MC use to government social services in our study. In NZ, individuals seeking health and disability allowances must provide medical certificates (Welfare Expert Advisory Group, 2019), and government support services may require evidence of unsuccessful prior treatments before considering funding cannabis-based products (ACC, 2023; MSD, 2023). A 2019 NZ report found that individuals with mental health conditions represented the largest group of health and disability welfare beneficiaries, with over a third (34%) of adults aged 40+ years receiving Supported Living Payments and nearly half (42%) of “Jobseeker Support” (Health condition or Disability) recipients citing mental health as their primary incapacity (Welfare Expert Advisory Group, 2019). The same report noted that less than a third (22.3%) of disabled people were in employment compared to non-disabled people (70%) and many reported lower levels of income. Formal requirements for medical documentation to access government benefits may explain why our respondents using MC for mental health were more likely to disclose to government support services.
MC users who did not consume cannabis daily/near daily were less likely to disclose to personal networks, health professionals, workplaces, or government services. Occasional users may perceive disclosure as unnecessary, particularly in healthcare settings where discussions around medication use are driven by perceived clinical relevance. Similarly, they may feel less need to disclose in other areas of their lives, as cannabis use may not represent a part of their daily routines. In contrast, daily cannabis users may have greater need for ongoing clinical oversight. Occasional users were also less likely than daily uses to report withholding disclosure due to fears that their employer might find out, potentially reflecting greater fears of negative employment consequences among more frequent users.
Demographic Predictors of Medicinal Cannabis Disclosures in Various Settings
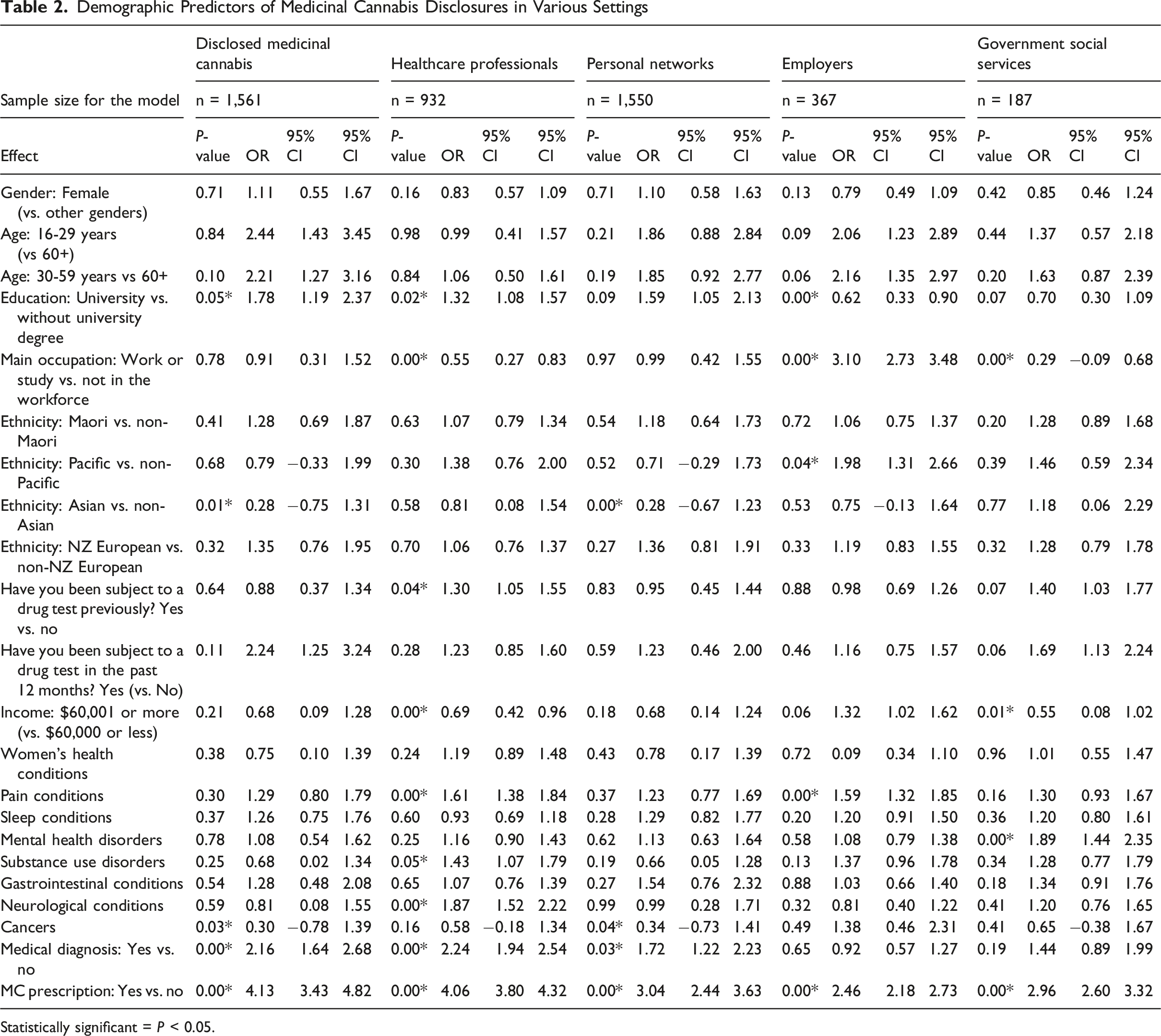
Statistically significant = P < 0.05.
Demographic Predictors of Medicinal Cannabis Non-disclosures
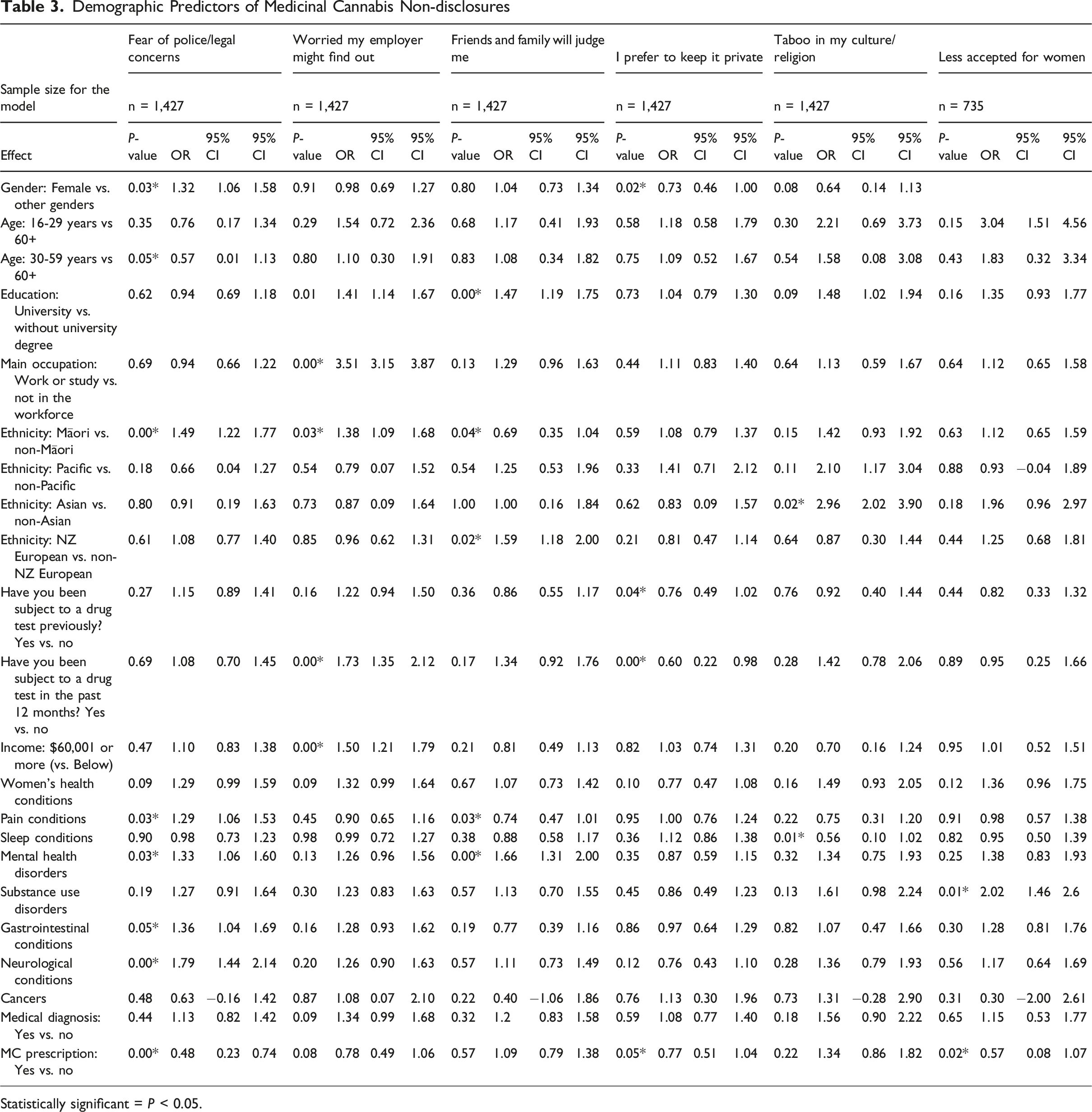
Statistically significant = P < 0.05.
Conclusion
MC prescription holders were more likely to disclose medicinal cannabis use in all settings, indicating that engagement with the NZMCS is facilitating more open dialogue around legal medicinal cannabis use. However, long standing social and cultural stigma and the prior illegal status of cannabis continue to shape prescribed medicinal cannabis disclosure behaviours. Māori expressed fear of legal prosecution, and women reported reluctance to disclose MC due to long standing social stigma that cannabis use was unaccepted for women, highlighting how past social attitudes still influence these groups. Participants treating pain or neurological conditions, where there is more scientific evidence for MC effectiveness (Hoch et al., 2024), were more willing to discuss their medicinal cannabis use. In contrast, patients with cancer, where MC evidence is still emerging, were less likely to disclose, reflecting concerns about judgement from health professionals and deviating from conventional treatments. Patients appeared selective with MC disclosures based on perceived benefits and risks, gender, context and cultural background. University graduates were more likely to disclose to health professionals, likely in pursuit of medical support, but less likely to disclose in workplaces where MC policies may still be developing, and disclosures could affect employment. Similarly, patients using MC for mental health issues were more likely to disclose to government support services, where structured pathways and eligibility assessments may necessitate transparency. To improve engagement with the NZMCS, future research is needed to understand how stigma and cultural perceptions of MC influences disclosures, particularly among Māori, Pacific Peoples, Asians and women, in order to inform support services and facilitate greater access.
Footnotes
Ethical Considerations
This study was approved by the Massey Human Ethics Committee Southern A. (approval no. OM1 23/50).
Consent to Participate
Not applicable. This study used an anonymous online survey, and no identifiable personal data were collected.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was funded by the Health Research Council of New Zealand (contract number: HRC-23-244).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analysed during this study are included in this published article.