
Abstract
Alcohol, cannabis, cocaine, heroin and benzodiazepines account for 95% of treatment cases in Ireland. This study examines first episode treatment data from the European Treatment Demand Protocol to examine access to services based on primary problem substance. The (N = 37,550) main presenting substances were alcohol (48.2%) and cannabis (21.4%). Alcohol had the highest proportion of women seeking treatment (37.6%) while cocaine had the lowest (19.0%). Alcohol cases were the oldest (40.7 years) while cannabis cases the youngest (22.9 years). Irish Travellers had higher rates of presentation for heroin and benzodiazepines use. Alcohol had the longest duration between first use and accessing treatment (24.2 years), while cannabis had the shortest (7.9 years); these differences were statistically different compared to all other substances. Alcohol cases were more often referred by medical sources and cannabis from criminal justice and community/social services. These findings emphasise that there were considerable periods between first use and first treatment and there are different demographic presentations between different substances.
Keywords
Introduction
Substance use represents a significant health issue in many countries with considerable resources being allocated to both prevention and treatment. While substance use itself can cause significant physical, psychological and social harm to an individual it remains one of the key modifiable risk factors for a variety of disorders. Since 2024, 346,203 substance use treatment episodes were recorded in Ireland, with 43.1% first ever treatment episodes (Health Research Board, 2026). Of all the treatment cases, alcohol (44.9%), heroin (23.1%), cannabis (12.2%) and cocaine (10.5%) are the most common substances. These four substances and benzodiazepines account for over 90% of all treatment cases with benzodiazepines accounting for a further 4.6% of cases (Health Research Board, 2026).
Addressing substance use consists of various interventions. Prevention and harm reduction interventions aim to prevent substance use before it starts or reduce the harm experienced by those who are using a substance and hopefully preventing the development of a substance use disorder (SUD) (James et al., 2014). The substance an individual is using can have significant implications for their treatment and the demands on services. Medical interventions are particularly relevant for those using opioids, benzodiazepines and alcohol where treatment of withdrawal and stabilisation is often required. Meanwhile there are no approved pharmacological treatments for cocaine use disorders (Buchholz & Saxon, 2019) and a similar picture arises for cannabis. Although some medications have evidence of effectiveness for treating cannabis withdrawal, psychosocial treatments are the primary approach for cannabis use disorder (Bahji et al., 2021; Brezing & Levin, 2018).
Like most countries, Ireland has its own idiosyncratic approach to providing substance use treatment. Traditionally substance use was seen as another mental health difficulty and treatment was the preserve of the mental health system (Government of Ireland, 1984). However, the emergence of a heroin epidemic, primarily in the Irish capital Dublin in the 1980s, a more traditional medical approach was sought and addiction treatment moved from mental health to public health services (Barry, 2002). Furthermore, substance use treatment was guided by various national policies which sought to coordinate treatment between statutory services and a growing number of local and national non-statutory agencies. Consequently, treatment provision is now somewhat hodgepodge with most treatment provided in local community services through a network of statutory and voluntary agencies funded primarily from the public purse. The national policy endorses a harm reduction, recovery oriented approach (Department of Health (DoH), 2017) and psychosocial and pharmacological interventions are available along with inpatient services. However services providing abstinence and 12-step approaches are also available. As services are publicly funded the individual does not pay for treatment in most cases however some private treatment options are also available, typically funded through health insurance. Further information on the development of Ireland’s national drug policies is available elsewhere (Comiskey, 2020).
Considering the complicated array of substances and treatments, it is important to examine the pattern of those attending services to target both prevention and treatment interventions appropriately. This study aims to describe the characteristics of those presenting for substance use treatment in the Republic of Ireland, based on their primary substance of use and to describe the pattern of substance use.
Objectives
To identify demographic patterns in those presenting for different substances.
To explore delays to accessing treatment for people using different substances.
Methodology
Study Design and Data Sources
Considering the exploratory focus of the research objectives, this study can be classified as an exploratory descriptive study with a cross-sectional design. The data for the study involves secondary analysis of routine surveillance addiction treatment data previously gathered by the Health Research Board (HRB). A European Union (EU) protocol has been developed which requires member countries to gather specific information to measure the substance use treatment demand in their jurisdiction (European Monitoring Centre for Drugs and Drug Addiction, 2012). In Ireland, this data is gathered by the HRB on behalf of the Government using a database called the National Drug Treatment Demand Reporting System (NDTRS) where data on episodes (or cases) of substance use treatment is recorded, mainly from publicly funded services. The study focused on cases reported as never having received treatment for alcohol of drug use previously, from 2016–2022 inclusive.
The initial dataset for the period included 49,548 first treatment episodes with a primary substance identified. Of these cases, 95.4% (n = 47,278) are accounted for by five main substances: alcohol, benzodiazepines, cannabis, cocaine and heroin. The final dataset included only clients who were recoded as having never previously been treated for both drugs or alcohol leaving a final sample of 37,550.
Data Analysis
Data was obtained from the HRB in an SPSS file and so all analysis was completed in SPSS v27. The dataset was then cleaned which is a process that involves identifying “inaccurate, incomplete or unreasonable data” and then removing or correcting errors in the data to improve the data analysis (Chapman, 2005). Primarily this involved running frequencies for categorical variables and descriptive statistics for continuous variables to ensure the reported values make sense (Pallant, 2016).
Exploratory data analysis was initially undertaken to help understand the variables available as well as their distribution, the quality of the data and patterns within the data as this informed the selection of appropriate statistical tests (Albers, 2017). Following exploration of the data the appropriate tests were chosen to examine differences across the five drug types. For continuous variables ANOVAs were preformed while chi-squared tests were chosen for categorical variables (Bettany-Saltikov & Whittaker, 2014).
Ethics
This study is a component of a larger PhD study examining the barriers and enablers of young people accessing treatment for substance use. The data was obtained from the HRB for this purpose following ethical approval being granted by the Ethics Committee of the Faculty of Health Sciences, Trinity College Dublin (Ref: 231003).
Results
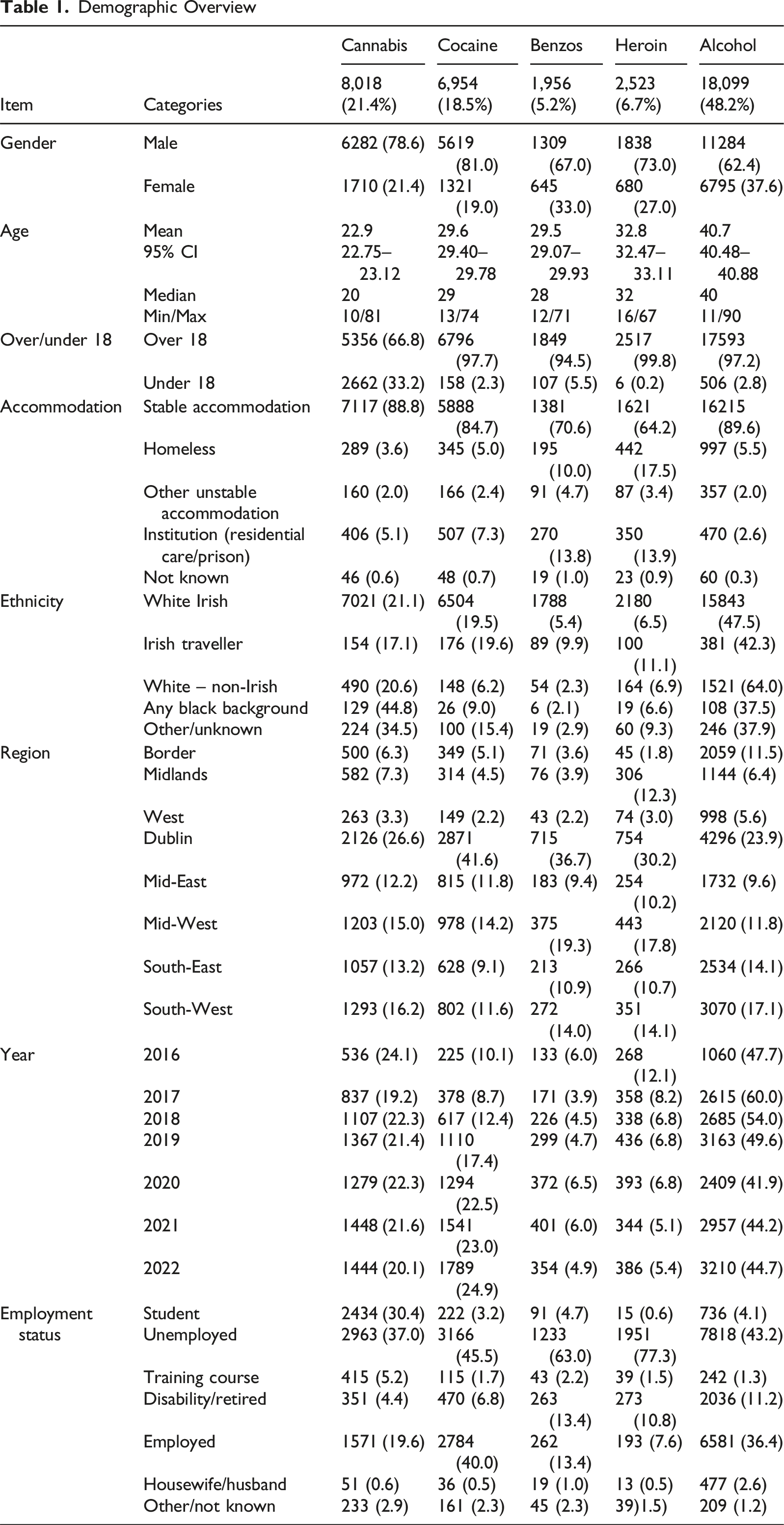
The dataset for this study includes all those who are recorded as never having accessed treatment for drugs or alcohol previously to ensure that each treatment case refers to a unique individual. Cases were limited to those presenting from 2016 to 2022 and have one of the five main drugs listed as their main substance of abuse. Of these cases (N = 37,550) the primary problem substance listed were alcohol (n = 18,099, 48.2%), cannabis (n = 8,018, 21.4%), cocaine (n = 6,954, 18.5%), heroin (n = 2,523, 6.7%) and benzodiazepines (n = 1,956, 5.2%).
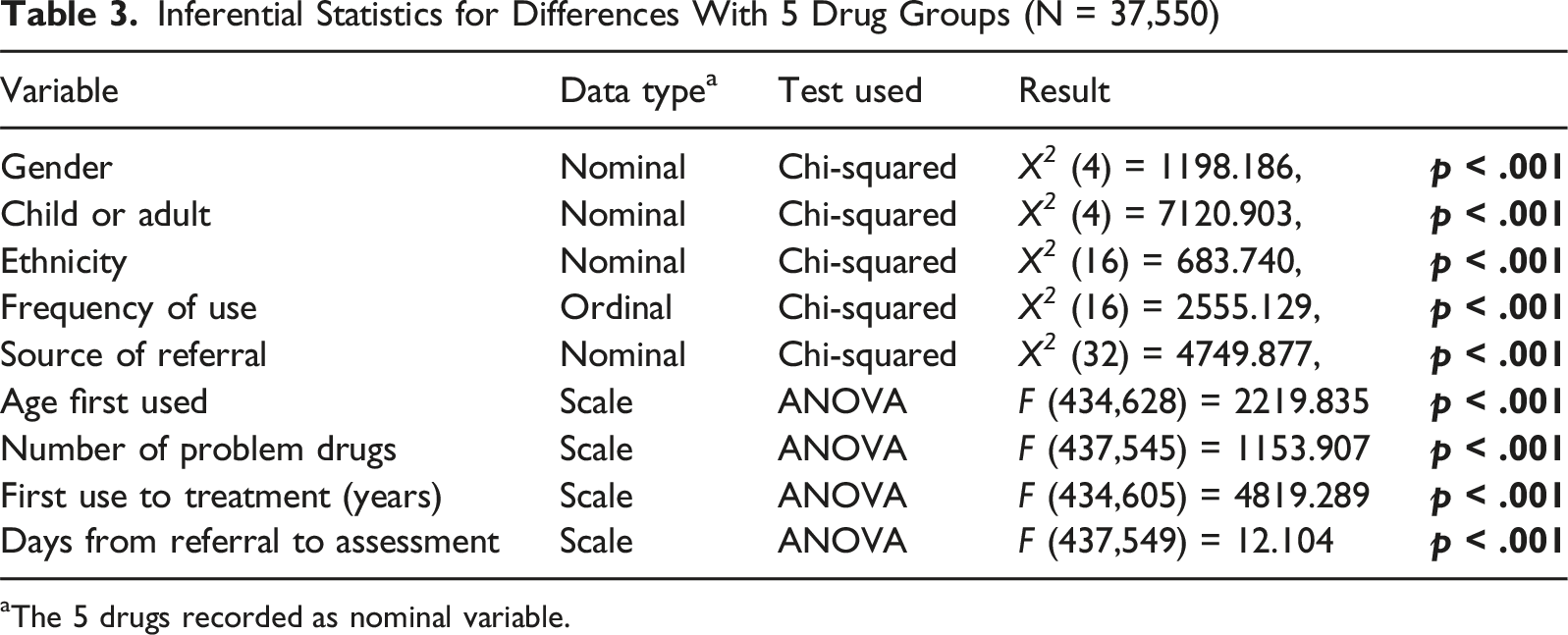
Demographics
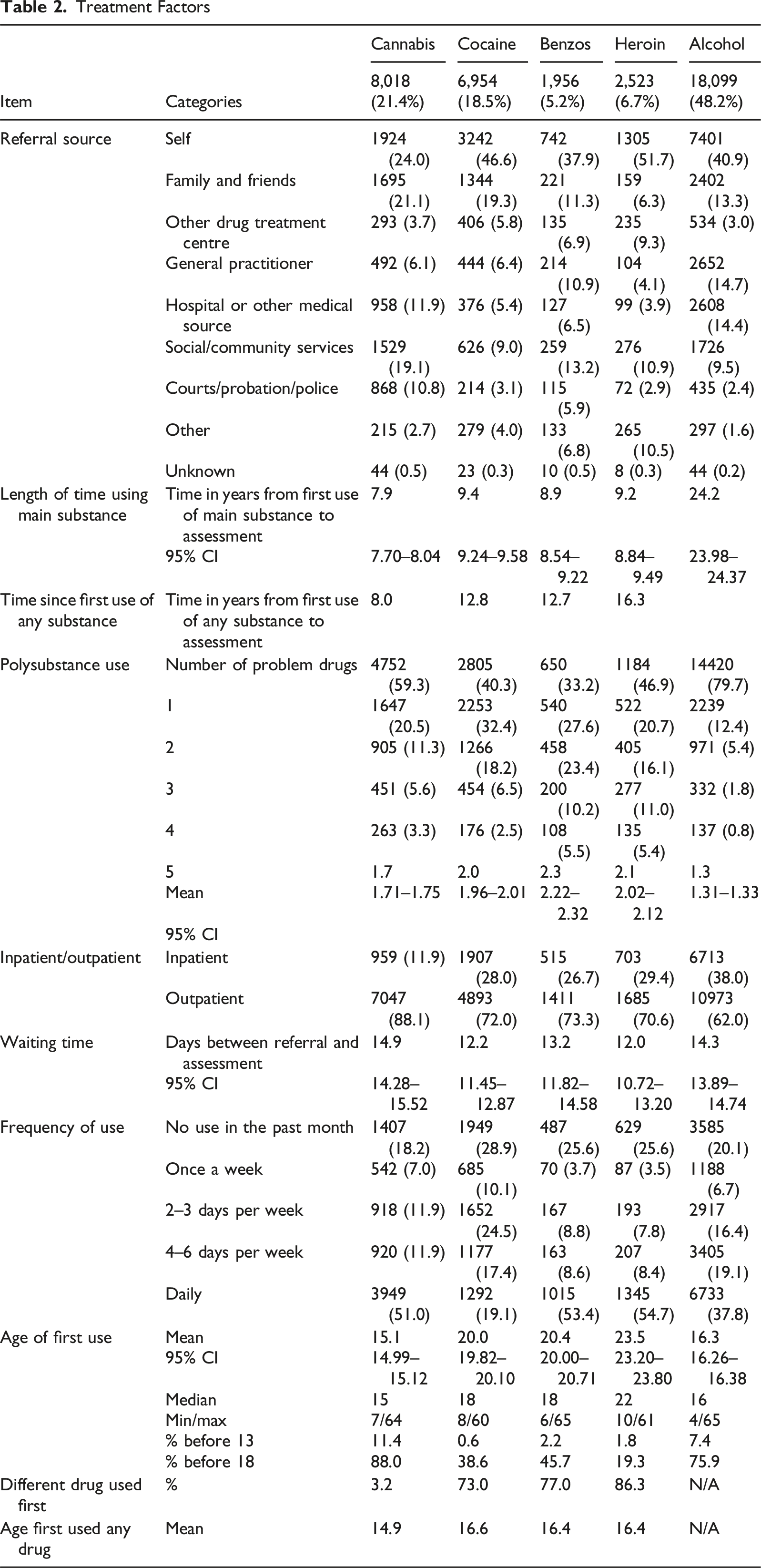
The mean age of cases’ first attendance to treatment is 33.7 years with females (36.8 years) noticeably older than males (32.5 years). While women account for 29.7% of cases overall, they account for a significantly smaller portion of those using cocaine (19.0%) and cannabis (21.4%) and a larger proportion of alcohol cases (37.6%). These differences were statistically significant, X 2 (4, n = 37,483) = 1198.186, p < .001. The cohort using heroin is the only group where the mean age for males is older than females (33.3 v 31.3 years). Cannabis users are the youngest cohort seeking treatment and alcohol the oldest cohort. Of those seeking treatment for cannabis, 33.2% are aged under 18, with benzodiazepines (5.5%) the group with the next largest proportion of under 18s, and again these results were statistically significant, X 2 (4, N = 37,550) = 7120.903, p < .001. Age of first use of the substance was significantly lower for cannabis (15.1 years) and alcohol (16.3 years), which was again statistically significant as determined by one-way ANOVA (F (4,n = 34,628) = 2219.835, p < .001). Almost nine out of ten (88.0%) of the cannabis cohort commencing use before age 18, and 11.4% before age 13. Those who presented for treatment for heroin use were the least likely to commence use before 18 with only 19.3% doing so. However, 77.1% of those presenting for treatment of heroin had commenced use of a different substance, excluding alcohol, before turning 18 years old. Only 3.2% of those seeking treatment of cannabis reported using a different substance (excluding alcohol and tobacco) before using cannabis. By contrast those seeking treatment for cocaine (73.0%), benzodiazepines (77.0%) and heroin (86.3%) were must more likely to report using a different substance first. When years from first use of any substance to assessment is examined, we see that cannabis cases are using substances eight years prior to assessment while those using cocaine (12.8), benzodiazepines (12.8) and heroin (16.3) are using substances over considerably longer. This is primarily because in over three-quarters of cases cannabis is the first substance people use.
Demographic Overview
Treatment Factors
Treatment Factors
Inferential Statistics for Differences With 5 Drug Groups (N = 37,550)
aThe 5 drugs recorded as nominal variable.
Some differences were also noted within the five drug groups that are worth highlighting in relation to how quickly people access treatment. While females tended take longer to access treatment than males (18.5 versus 15.1 years), they tended to attend quicker than males for cocaine (F (1,6358) = 13.009, p < .001) and heroin (F (1,2313) = 42.232, p < .001). Regardless of the substance individuals were presenting with, ethnic minorities such as those from Black, other and Irish Traveller background tended to present similar. Likewise, across the five drug groups, those with one problem substance tended to take longer to attend and each additional problem substance shortened the time to treatment.
Crosstab of Relationship Between Drug Groups (n = 37,550)

aBenzodiazepines Most common secondary substance in bold.
Discussion
This study sought to examine the difference in demographics and route to treatment of people entering substance use treatment in the Republic of Ireland for the first time. Several of the findings warrant further discussion. The data available does not indicate how long people may have been experiencing problems related to their substance use prior to seeking treatment, only how long they have been using the substance. However, the finding that those seeking help for illicit drug and alcohol use are using the substance for over eight and twenty-four years respectively before accessing treatment for the first time warrants further research. Previous research found that 70% of cannabis dependence cases develop within three years of first use and 50% of alcohol dependence within four years (Behrendt et al., 2009). Other research suggests that by age twenty-three, 80% of cannabis dependence cases have occurred while approximately 50% of cocaine and alcohol dependence cases have occurred by twenty-three (Wagner, 2002). The short wait for treatment, typically under two weeks, suggests that there is little delay accessing treatment quickly once it is sought. The gap between first use and accessing treatment aligns with an Australian study which found that those with a SUD had a median of 8 years from problem onset to treatment and that alcohol was associated with a longer delay (Birrell et al., 2025). Findings from other studies also indicate that those with SUD have lower rates of treatment access compared to anxiety or depressive disorders (Birrell et al., 2025; Wang et al., 2007). Meanwhile a US study found that while 13% of those with drug dependence access treatment within a year, only 5% of alcohol dependent individuals do so (Blanco et al., 2015). A similar study in the Netherlands reported that lifetime treatment for individuals with a SUD was only 16.7% compared to 81.8% and 60.9% for mood and anxiety disorders respectively (Ten Have et al., 2013). Ten Have et al. (2013) also reported that only 10.5% of SUDs presented within a year of onset. A large international study across 15 countries found that the six European countries had 12% to 18% of those with a SUD accessing treatment in the first year of onset. But these rates were superior to all other countries including the USA, Japan and New Zealand (Wang et al., 2007). Research indicates that those who commence illicit substance use at a younger age, particularly as children, are more likely to have longer (Dennis et al., 2005) and more severe substance use problems (Tillson et al., 2019). Irish research focusing on people who use cannabis indicates that for each year onset of cannabis use is delayed corresponds to an 11% decrease (OR = 0.89; 95% CI: 0.82, 0.98) odds in having a cannabis use disorder (Millar et al., 2021). Taken together, these findings suggest that work is needed to ensure that those who develop SUDs access treatment quicker than they currently are. Recent Irish research has shown that cocaine use increases sharply between ages 17 and 20 and is associated with alcohol use at a young age with those drinking by age 14 having a 19 times increased odds of using cocaine at age 20 (Brennan et al., 2025).
US data suggests that while 19.1% of the population above 12 years old required SU treatment in 2023, only 4.5%, or less than one in four who required it, actually received treatment in the past year (SAMHSA, 2024). This is possibly explained by the concurrent finding that of those who had a SUD and did not receive treatment, 96.6% of under 18s, and 94.7% of adults did not perceive that they needed treatment (SAMHSA, 2024). These individuals are unlikely to access treatment without being directed towards it and perhaps explains the finding that referrals for medical sources were most common for alcohol, the substance with the longest gap to treatment. Conversely, cannabis with the shortest gap to treatment was most likely to have criminal justice or social or community service referrals. Further examination is needed to examine referral pathways to SUD treatment, with some research indicating complicated procedures and lack of knowledge around procedures and patient eligibility are challenges (Blevins et al., 2018).
The difference between genders and substance use are well documented with men generally reporting more use of substances as well as more SUDs (McHugh et al., 2018). US studies suggest that men are 94%, 39% and 10% more likely to have a cannabis, cocaine and heroin use disorder in the past year respectively (Ellis et al., 2024). Irish research also found that males were about five times as likely to have a cannabis use disorder as women (NACDA, 2018). Our results indicate that women tend to present with use of sedative substances such as benzodiazepines and alcohol. While females are more likely to receive treatment if they have an anxiety or depressive disorder, they appear less likely to receive treatment if they have a SUD (Birrell et al., 2025).
Ethnicity also appears to play a role in substance use with those from Irish Traveller backgrounds having the largest proportion of both benzodiazepine and heroin use and the presentation of these substances appears to be increasing among the Traveller community (Carew et al., 2013). The most recent national survey of substance use reported that those from the Traveller community were more likely to be excluded as they often do not reside in private households (Mongan et al., 2022) and the need for more targeted research on this marginalised community has long been flagged (Van Hout, 2010). The finding that those from Black and other backgrounds have the highest proportion of cannabis presentations is perhaps unsurprising given a similar emerging trend in the US (Montgomery et al., 2022; SAMHSA, 2023). Further study on the substance use patterns of ethnic minorities is warranted considering the rapidly changing demographics within the Irish population where the proportion of the population born outside of Ireland increased by 25.5% between 2016 and 2022 (Central Statistics Office, 2023).
Limitations
Several limitations of this study ought to be noted. While the large sample is a strength the use of secondary data means that there are limitations to the data available for analysis. As noted previously, while all these individuals were assessed and accessed treatment for substance use, there is no way of determining how long the SU problems existed prior to presenting to treatment. It is worth noting that the cases here included only first ever treatment episodes which may affect generalisability. However, a strength of the research is the use of data which was collected using clear protocols and guidelines. Finally, while these are first substance use treatment episodes, some individuals may have accessed self-help groups such as AA or counselling previously where substance use was addressed but not disclosed. The treatment demand protocol does not explicitly state whether self help groups ought to be considered prior treatment but in the authors’ experience they are not recorded as previous treatment.
The NDTRS coverage is high with 71.1% of eligible services participating (Lynch et al., 2025). However there is considerable variance in the level of participation with some service types having close to 100% participation while only 43.7% of eligible GPs participated in 2024 (Lynch et al., 2025). As a result, all eligible treatments may not be recorded leading to some errors in the data. Also, the NDTRS only currently collects data on opioid agonist treatment from general practitioners (GPs). This means that individuals whose first treatment episode for other substances was with a GP would not be included. GPs may have provided treatment such as detoxification for alcohol would not have been recorded and would have an impact on the figures. However, for many, GPs would have referred onwards to a specialist service rather than providing specific addiction treatment and we can see they were most likely to refer people for alcohol and benzodiazepines.
Conclusion
The findings of this study indicate that while many people access treatment for substance use in Ireland there is considerable time between when they first start to use a substance and subsequently accessing treatment. If the harms of substance use are to be reduced, health messaging and earlier intervention needs to be prioritised. While services tended to respond quickly once people sought treatment, this study cannot account for why most were using substances for many years before seeking treatment. However, the literature suggests that in most cases even those with significant substance use problems do not perceive themselves as requiring treatment. Reducing this gap to treatment as well as increasing the proportion of those with SUDs accessing treatment ought to be key targets. Qualitative research in the future would help to elucidate the reasons for people not accessing treatment. The findings included here indicate that different substances tend to be used by different groups and alcohol is associated with a long time between first use and accessing specialised treatment.
Women present much more frequently for treatment of sedative substances, particularly alcohol and benzodiazepines, and less frequently for cannabis and cocaine. Treatment providers need to adapt their services to meet the needs of the changing gender and ethnic minority presentations. Doing so will allow for more targeted and responsive services that can address barriers to treatment access.
Data Collection Instrument
Further information regarding the National Drug Treatment Reporting System, including copies of the data collection tool are publicly available from the Health Research Board in Ireland. See https://www.hrb.ie/data-collections-evidence/alcohol-and-drug-treatment/about-addiction-treatment-data/.
Footnotes
Acknowledgements
The Health Research Board Ireland provided the dataset for this study. The authors would like to thank Dr. Suzi Lyons and the NDTRS team at the Health Research Board, and all the services who provide treatment data to the Health Research Board.
Ethical Considerations
The data was obtained from the HRB for this purpose following ethical approval being granted by the Ethics Committee of the Faculty of Health Sciences, Trinity College Dublin (Ref: 231003).
Consent to Participate
Data used was secondary analysis of anonymised treatment data collected in line with an EU wide protocol. The data is collected in anonymised format so neither the Health Research or the authors were able to gather consent. This was noted and approved by the approving ethics committee.
Author Contributions
Philip D. James, Dr. Michael Nash, Dr. Sonam Prakashini Banka-Cullen, Professor Catherine Comiskey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Philip D. James completed this study as part of their PhD which is funded by a scholarship from the School of Nursing & Midwifery, Trinity College Dublin; 2020-2030. No other funding was received.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Identifying Information
Name of the ethics committee removed from the article to aid anonymous review.