
Abstract
Introduction
Image and Performance Enhancing Drugs
Image and performance enhancing drugs (IPEDs) are a category of human enhancement drugs typically used to develop physical appearance and performance. They include anabolic androgenic steroids (AAS) – a specific category of some of the most used and researched IPEDs, thermogenic compounds (e.g., clenbuterol), human growth hormone (hGH), and a range of other substances (e.g., Melanotan II) (Dunn & Piatkowski, 2021; van de Ven et al., 2019). Typically, the use of IPEDs extends over a period of weeks or even months (referred to as a ‘cycle’), with one common approach being ‘blast and cruise’, in which an individual engages in a continuous cycle of use which alternates between periods of high doses (i.e., the ‘blast’ phase) and low doses (i.e., the ‘cruise’ phase) of IPEDs (Chandler & McVeigh, 2014; Sagoe et al., 2015). People who use IPEDs often combine and ‘stack’ various substances (also known as polypharmacy), and follow complex regimes and protocols which are designed to enhance the efficacy of the drugs they use whilst also mitigating health harms (e.g., the use of ancillary agents; Kanayama & Pope, 2012). In a further bid to enhance their health following the cessation of IPEDs, some consumers engage in post-cycle therapy (PCT), consuming a combination of drugs and engaging in a range of behaviours in an attempt to restore natural hormonal functioning, reverse or mitigate side effects, and/or avoid side effects associated with the discontinuation of IPEDs (Griffiths et al., 2017). However, balancing dual goals (health management and physique enhancement) poses a challenge for some individuals who use IPEDs, who may lack experience and knowledge in navigating the complexities associated with this type of drug use.
IPEDs are associated with various acute and chronic harms. These include, but are not limited to, adverse cardiovascular, haematological, hepatic, renal, endocrine, reproductive, and musculoskeletal effects (e.g., Kanayama & Pope, 2012; Pomara et al., 2015). More specifically, IPEDs have been linked to increased oxidative stress response (e.g., Arazi et al., 2017), hypertension and dyslipidemia (e.g., Achar et al., 2010), cardiomyopathy, cardiac arrhythmia, and myocardial infarction (e.g., Fadah et al., 2023; Perry et al., 2020), and reduced fertility parameters (e.g., Mulawkar et al., 2023). Furthermore, the use of AAS has been associated with increased neurotoxicity (Gomides et al., 2019), as well as psychological issues including increased aggression (e.g., Piatkowski et al., 2024) and risk-taking behaviour (e.g., Nelson et al., 2022), as well as mood destabilisation (e.g., Piaciento et al., 2015).
Due to the array of health implications that might arise from the use of IPEDs, various approaches have been developed to tackle such concerns. Two distinct approaches exist when AAS are considered: the first of which centres around prohibition. Largely intertwined with legal frameworks and based upon paternalistic values, this approach to AAS is based upon laws and policies put in place to ultimately discourage, deter, and prevent use. For example, whilst the United Kingdom and Australia incorporate harm reduction principles within their policy approaches, both countries enforce legislation surrounding manufacture, distribution, and supply of AAS, and in the case of Australia specifically, personal use of AAS is illegal without prescription (see Piatkowski et al., 2023). Though the aim of these approaches may not be to eradicate AAS-using behaviours entirely, such legislative enforcements and the threat of punishment surrounding the use of AAS makes them increasingly difficult to access, and considerably less desirable (Hawk et al., 2017; Mulrooney et al., 2019). Alongside legal frameworks, anti-doping policy prohibits the use of many IPEDs, including AAS, in sporting competitions at both elite and recreational levels around the globe (Cox et al., 2022; WADA, 2024). This stance is largely governed by the World Anti-Doping Agency (WADA), who reinforce an approach which seeks to prevent, deter, and sanction people who are caught using various IPEDs (please check WADA’s Prohibited List for a full outline of prohibited substances and methods). Collectively, these distinct approaches reinforce moral disapproval related to this specific type of drug use and underpin a narrative of deviancy.
The second approach to AAS is rooted in autonomy and facilitating choice, viewing IPED use through a harm reductionist lens. Harm reduction refers to interventions which aim to reduce the negative consequences of drugs, as opposed to reducing or eliminating the drug use itself (Hawk et al., 2017). Within Western countries (e.g., the UK), harm reduction strategies such as needle and syringe programmes (NSP), which typically provide clean needles and syringes and allow for the disposal of used equipment, have been developed to address health risks such as the transmission of blood-borne viruses amongst people who inject drugs (Chandler & McVeigh, 2014; McVeigh et al., 2015, 2022). Although research has evidenced considerable uptake and beneficial effects of NSP amongst illicit drug consumers (e.g., Fernandes et al., 2017; Tookes et al., 2024), barriers such as perceived stigma limit the uptake and subsequent success of these services amongst people who inject AAS specifically (see Cox et al., 2024). Moreover, while NSP exist, Kimergård and McVeigh (2014) argue that these services vary in terms of the service delivery that they provide, something that is considered a current limitation. In conjunction, the provision of harm reduction services for AAS consumers has somewhat fallen behind those offered to people who inject other types of drugs (e.g., heroin), with some services limited exclusively to the provision of sterile injecting equipment (Bates et al., 2021; McVeigh & Bates, 2022). This is problematic for the IPED community, in particular, for AAS consumers who exclusively use oral tablets rather and injectable preparations, who will miss out on opportunities to engage with healthcare providers, as they will not engage with NSP (Cox, Piatkowski, & Dunn, 2025). Hence, researchers have emphasised the need to broaden the scope of culturally appropriate approaches to support people who use IPEDs (e.g., Bates et al., 2019, 2021; Cox et al., 2024).
Image and Performance Enhancing Drug Coaching
In the absence of governmental support for IPED consumers, and in response to the arising need to protect people from harm when engaging with this type of drug use, multiple do-it-yourself (DIY) interventions have arisen within the IPED community (Henning & Andreasson, 2022). Such developments have emerged to fill gaps within the privatized landscape of harm reduction (see Turnock et al., 2023), with IPED coaches seen as one notable branch. IPED coaches, termed elsewhere in the literature as ‘steroid mentors’ (van de Ven & Mulrooney, 2017) and ‘anabolics coaches’ (Gibbs et al., 2022a), are individuals who support paying clients who use IPEDs, providing them with information and advice surrounding drugs and drug protocols. In line with their overarching goals, improving the client’s physique or performance, and minimising adverse health effects associated with these drugs, IPED coaches offer IPED-related guidance either as one component of a broader physique coaching relationship, or as a stand-alone service (Gibbs et al., 2022a; Piatkowski et al., 2024, 2025). Although the practice of IPED coaching is a long-standing and normalised service within the bodybuilding community (Gibbs et al., 2022a), research specifically exploring the roles and practices of IPED coaches has only gained increasing attention within recent years (e.g., Cox et al., 2025; Gibbs et al., 2022a; Piatkowski et al., 2024, 2025).
For example, within Gibbs et al.'s (2022a) study, ethnographic observations and semi-structured interviews were conducted to explore the contemporary anabolics coaching industry. Within that study, the support levels of anabolics coaches were found to vary from one-off advice, to prescribing of IPED cycles. However, some participants operating within the anabolics coaching space were eager to detach themselves from the label of ‘anabolics coaches’, emphasising that IPED advice cannot be disentangled from the wider context of physique enhancement practices (e.g., diet and training). In this sense, participants perceived the role of an anabolics coach as an ‘overseer’, monitoring client’s IPED use and proposing adjustments in accordance with client progress and goals.
This notion that services offered by IPED coaches are both varied and adaptable was underscored within Piatkowksi et al.’s (2024b) recent study, which implemented semi-structured interviews to understand how IPED coaches perceived their roles, specifically in terms of facilitating harm reduction. Findings somewhat mirrored those of Gibbs et al. (2022a), whereby IPED coaches dismissed the title of solely ‘IPED coaches’, instead deeming themselves as ‘comprehensive coaches’, with IPED services comprising just one facet of their offering. In accordance with their roles, IPED coaches were invested in a continuous pursuit of knowledge acquisition via engagement with academic literature and a process of seeking and sharing information within the community. Coupled with their own lived experiences, this quest for learning offered IPED coaches a level of credibility and trust amongst their clientele (Piatkowski, Cox, et al., 2024). With respect to this, coaches recognised the power dynamics at play within coaching relationships and thus, steered clients towards informed choices and decisions regarding IPEDs. Acting as gatekeepers to use, IPED coaches attempted to balance ethical practice with client empowerment and autonomy through a process of collaborative discussion and decision-making (Piatkowski, Cox, & Collins, 2024). In this way, IPED coaches valued client care as a critical component of the IPED coaching relationship, not only emphasising harm reduction (i.e., minimising harms associated with IPED use), but also health enhancement (i.e., assessing variables outside of IPED use to maximise wellbeing, such as diet, weight, and sleep) (Piatkowski, Cox, & Collins, 2024). Parallels are also noted by Paoli and Cox (2024) who examined the services offered by ‘Performance and Image Enhancing Drug (PIED) influencers,’ that is individuals who have built notable online followings on social media platforms (e.g., Instagram, YouTube and TikTok etc.,) through ethnographic observations. Although not focusing specifically on IPED coaches, PIED influencers offered IPED coaching as part of several other services (e.g., supplement and diet advice, bloodwork testing and analysis, the provision of discount codes and the supply of IPEDs), which underscores the notion that IPED coaching is sometimes blended within and across various other services. Moving beyond one-to-one coaching, knowledge exchange approaches adopted by IPED coaches’ have also been found to extend to the delivery of both face-to-face and online workshops, courses, seminars, and lectures (Cox et al., 2025), further emphasising the demand for IPED-related information and advice.
Taken together, the above-mentioned studies have provided valuable insights into the roles (e.g., overseer, mentor), practices (e.g., consulting, advice giving), and values (e.g., knowledge, care) of IPED coaches. Although these qualitative studies have identified commonalities amongst IPED coaches, this body of research is still in its infancy, and there is an absence of quantitative research studies within this specific area. As a result, to date, our knowledge of IPED coaches has been primarily based upon small sample studies (e.g., n = 10; Piatkowski, Cox, et al., 2024), which do not provide the scope of data required to comprehensively profile and understand the role of an IPED coach. For instance, there remain gaps in knowledge specifically with regards to our understanding of precisely what and who IPED coaches are. Given that IPED coaches place emphasis on their own lived experiences, it is of particular importance to build a better and more comprehensive picture of their personal IPED use, as this underpins their coaching practices in turn. Furthermore, existing research exploring IPED coaching has primarily done so within restricted Western regions of the world (e.g., UK and Australia), which means that possible variations and cultural trends surrounding IPED coaching have been overlooked.
Underpinning Theory
To address these gaps within the literature, the current study adopted a cross-sectional survey design to explore how coaches develop their IPED coaching practices and insights. The study was underpinned by the framework of ethnopharmacology (see Monaghan, 2002), which focuses on understanding the use and knowledge of drugs within specific cultural and social contexts. Ethnopharmacology emphasises how communities, through lived-living experience and cultural practices, develop their own systems of understanding substances, often outside of mainstream medical or scientific systems (see Piatkowski, Cox, et al., 2024; Piatkowski, Cox, et al., 2025), which the IPED community typically reject. The practice of coaching, particularly in the realm of IPEDs, is shaped by experiential knowledge gained through personal use and engagement with a community of like-minded individuals. This knowledge is garnered and learnt through doing, where ‘chemical capital’ (Piatkowski, Cox, et al., 2024) is curated and built to inform specific approaches to drug use. Coaches often act as repositories of this informal, yet highly valuable, knowledge, passed down through interactions, shared experiences, and peer networks. Therefore, in the context of IPED coaches, ethnopharmacology provides a lens to examine how these individuals accumulate, refine, and disseminate their knowledge of IPEDs in the wider IPED community, shaping drug norms and behaviours. By applying an ethnopharmacological perspective, this study places a central focus on the lived-living experiences of IPED coaches, emphasizing how their personal experimentation with IPEDs informs their coaching services and techniques. This framework helps contextualize how knowledge of IPEDs is cultivated, maintained, and shared in spaces that are often outside and beyond the reach of traditional, formal education or healthcare systems.
Methods
Study Design
The current study employed a cross-sectional survey design to gather data on demographics, usage patterns, and coaching practices related to IPEDs. Characteristically, cross-sectional designs gather data from a single time point, and allow researchers to record information relating to the properties and attributes of a specific population (e.g., IPED coaches; Cummings, 2018). Hence, a cross-sectional survey design was deemed the most appropriate approach to explore the types of substances consumed, as well as the types of services provided amongst IPED coaches.
Participants
The survey was distributed to IPED coaches, targeting a diverse international audience. Participants were recruited through online forums, social media platforms (e.g., YouTube), and community organizations associated with fitness, bodybuilding, and performance enhancement. The latter part of recruitment was facilitated by Vigorous Steve (VS), an PIED influencer, who has built a sizable online following on social media platforms (e.g., YouTube, Instagram). Drawing upon his well-known status and social power within IPED communities, VS shared survey links within specific online communication (e.g., YouTube video descriptions) to draw and attract interest and underscore the importance of IPED coaches’ participation within the study. The sample consisted of 41 IPED coaches with a mean age of 29.3 years (range: 20–58 years, SD = 7.58). The majority identified as male (97.6%), with one participant preferring not to disclose their gender. Participants resided in diverse locations, with the largest proportion from the United States (29.3%), followed by Germany (12.2%), Australia (9.8%), and the United Kingdom (9.8%). Smaller proportions were reported from Canada, India, South Africa, and other countries, reflecting the international reach of IPED coaching and the need for a broader understanding of its dynamics across different cultural contexts.
The mean age of drug onset was 22.8 years (range: 17–43 years). The most common initiation ages were 18 years (28.6%) and 22–23 years (10.7% each). Regarding IPED use patterns, 56.3% of participants engaged in blast and cruise (never coming off IPEDs), while 34.4% reported blast and cruise cycles with intermittent breaks. Only a small proportion (6.3%) followed a cycle and post-cycle therapy (PCT) approach, while 3.1% used a traditional cycle method.
Data Collection
Ethical approval was granted by the research ethics committee at Swansea University prior to commencement of this study. All participants were informed about the purpose of the study and provided e-consent before completing the survey. This included the provision of information sheets which outlined the study details and its aims, providing prospective participants with an extensive overview to ensure informed consent could be attained. All identifiable data was removed to protect participant anonymity. Data were collected using a structured, online questionnaire developed to assess various aspects of IPED use and coaching. The online platform utilized was Qualtrics XM. In consideration of the social stigma that is perceived amongst individuals using IPED (e.g., Cox et al., 2024; McVeigh & Bates, 2022), the online delivery of the survey allowed for anonymous responses to encourage candid participation and reduce social desirability responding (Nayak & Narayan, 2019). Indeed, participants were able to complete the surveys in the comfort their own homes, or in a location where they felt most at ease.
The questionnaire consisted of three sections. In section one, participants provided information on their age, gender, and country of residence, as well as their drug usage history, usage methods, routes of administration (i.e., oral or injectable), and drug choices in the past 12 months (including injectable and oral steroids, IPEDs, and ancillary medications). In section two, participants provided information on their client base, including their number of clients, typical client demographics and goals, service delivery methods, and sources of IPED-related information. Finally, in section three, participants reported on their online marketing strategies, as well as their social media following.
Data Analysis
Descriptive statistics were employed to analyze the demographic characteristics, drug usage patterns, and coaching practices of the participants. Valid responses were summarized, while missing data were documented to provide transparency regarding response rates for individual questions.
Results
Substance Use Practices
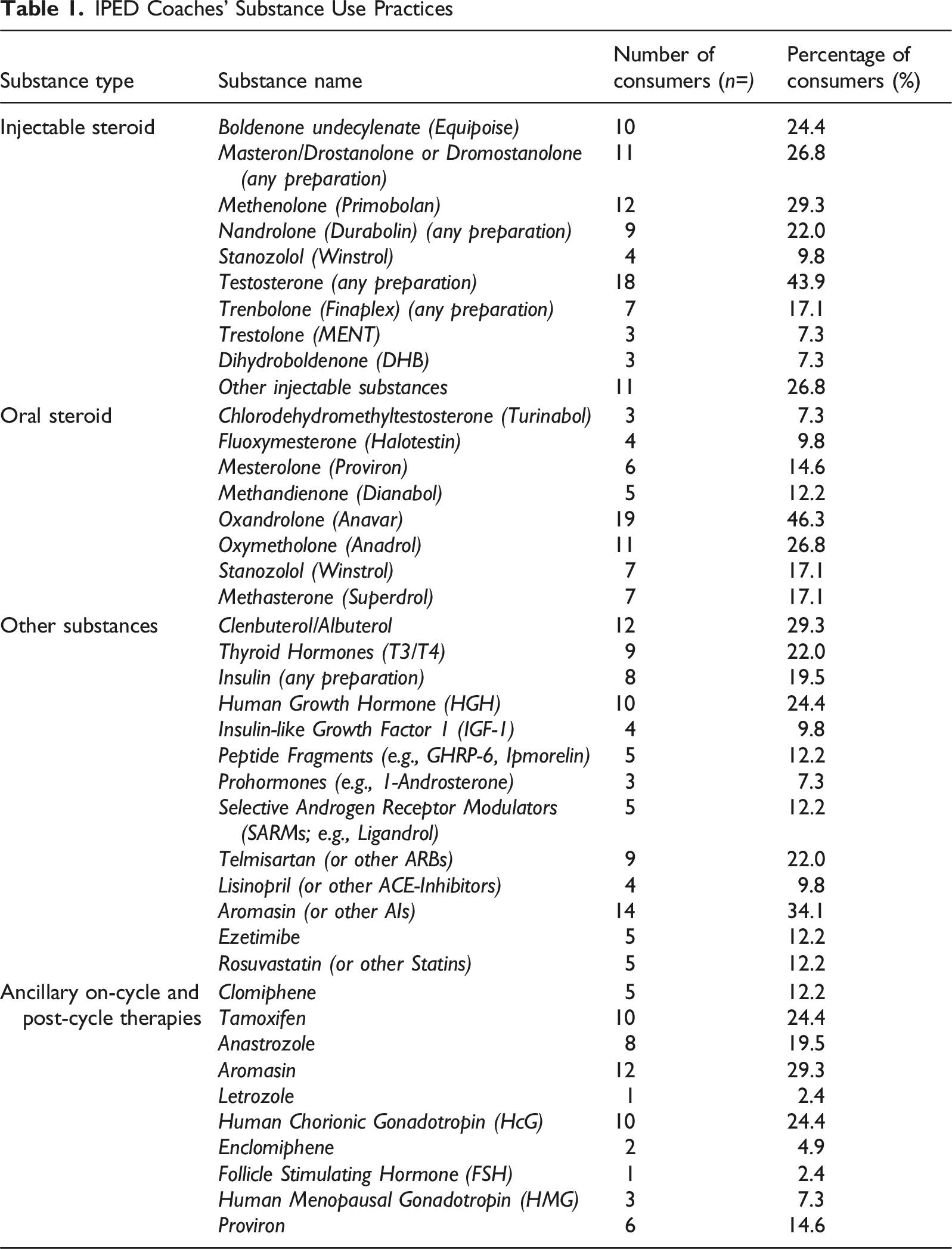
IPED Coaches’ Substance Use Practices
IPED-Related Harms and Service Provision
In the second part of survey, of the 26 participants who provided valid responses regarding IPED-related harms, 24 participants (92.3%) considered the possible short-term health implications of their IPED use, while 2 (7.7%) did not. Likewise, 24 participants (92.3%) considered the possible long-term health implications of their IPED use, while 2 (7.7%) did not. In relation to IPED coaches’ lived experiences, 18 participants (69.2%) reported not using medically prescribed TRT, while 8 (30.8%) indicated they were using medically prescribed TRT. Eight participants (30.8%) reported experiencing IPED-related harms, including acne, blood pressure issues, mental health effects, and other side effects. Finally, 24 participants (92.3%) reported not having had surgery due to IPED use, while 2 (7.7%) had undergone surgery for gynecomastia.
Out of 24 valid responses regarding the services provided by the IPED coaches, 12 participants (50%) reported serving between 0 and 10 clients, 3 participants (12.5%) served between 11 and 20 clients, and 3 participants (12.5%) served between 21 and 30 clients. A small percentage (1 participant, 4.2%) served between 41 and 50 clients, and 2 participants (8.3%) reported serving between 51 and 60 clients. One participant (4.2%) reported serving over 70 clients. The majority of IPED coaches reported serving male clients (15 participants, 62.5%), with fewer serving female (2 participants, 8.3%) or mixed-gender clients (7 participants, 29.2%). Out of 23 valid responses, 13 participants (56.5%) reported providing services nationally, 1 participant (4.3%) internationally, and 9 participants (39.1%) provided both national and international services. Regarding modality of coaching delivery, 16 participants (66.7%) provided both online and offline services, 7 participants (29.2%) provided services online, and 1 participant (4.2%) provided services offline.
In relation to the types of advice and guidance offered, out of 24 valid responses, 13 participants (54.2%) reported offering bloodwork advice or analysis, while 2 participants (8.3%) did not. Additionally, 9 participants (37.5%) provided specific advice related to bloodwork. Fourteen participants (58.3%) offered advice on post-cycle therapy (PCT), while 1 participant (4.2%) did not. Like bloodwork advice, 9 participants (37.5%) provided more detailed PCT advice.
Regarding supply of IPEDs, out of 24 valid responses, 13 participants (54.2%) did not supply IPEDs to clients. A smaller percentage (3 participants, 12.5%) reported supplying IPEDs, while 8 participants (33.3%) stated that they supplied IPEDs sometimes. Eleven participants (45.8%) suggested ‘trusted IPED suppliers’ to their clients, 3 participants (12.5%) did not, and 10 participants (41.7%) suggested them sometimes.
Finally, IPED coaches referred to a range of information sources from which they acquired their IPED-related information. Specifically, out of 24 valid responses, 8 participants (33.3%) mainly used online sources such as forums, YouTube, and Instagram, 9 participants (37.5%) relied on scientific articles, 1 participant (4.2%) used gyms to acquire information, and 6 participants (25%) cited other sources.
Online Presence
In the third section of the survey, the number of valid responses decreased again. In relation to the platforms used to market their services, 22 participants provided valid responses. Most participants (16 participants, 72.7%) used Instagram to market their services. Smaller percentages used other platforms (4 participants, 18.2%) or YouTube (2 participants, 9.1%). Among 10 valid responses, the average social media following was 1,803.2 followers, with a median of 1,225 and a standard deviation of 1,825.24. The minimum following reported was 240, and the maximum was 5,200.
Discussion
The current study sought to develop an initial profile of IPED coaches, to enhance understanding relating to how IPED coaches operate and provide support for the IPED community. Using a cross-sectional survey design, this study is the world’s first to provide quantitative data relating to the practices of IPED coaches, offering insight relating to their drug consumption patterns, and the scope of their IPED coaching services. The findings of this study build upon those of previous qualitative studies indicating the multifaceted role that IPED coaches play with regards to providing instruction to IPED consumers, and working alongside them to improve appearance and performance whilst minimising adverse effects (Gibbs et al., 2022a; Piatkowski et al., 2024). Specifically, the current findings provide an initial illustration of the exact scope of IPED coaches’ services, including (1) the size of their client base, (2) the modalities through which they offer coaching services, (3) the geographical reach of their client base, and (4) the gender split of their clientele.
Relating to the scope of IPED coaching services, it is understood that IPED coaches operate primarily within the semi-professional, professional, and high-end athlete market, working alongside athletes in sports such as bodybuilding, powerlifting, and strongman competitions (Gibbs et al., 2022a). In addition, many IPED coaches offer their services either partly or exclusively online (Gibbs et al., 2022a), as was also reported by coaches within the current study. Moving beyond this broad understanding, the current study was the first to gauge the size of IPED coaches’ client bases, indicating a range between zero, and over 70 clients. Coaches within the current study also reported working with clients on both a national and international scale. These findings are significant and should be viewed as a positive, as they allude to the widespread accessibility of IPED coaching services, as well as the potential for further growth and reach of such services. In the face of perceived stigma and lack of trust in healthcare professionals (e.g., Cox et al., 2024), there is an increasing need to broaden the scope of harm reduction services available to IPED consumers. IPED coaching offers one pragmatic and highly accessible alternative to engagement with healthcare professionals, serving to bridge the gap between IPED consumers’ needs, health monitoring, and health enhancement (Piatkowski, Cox, & Collins, 2024). However, while IPED coaching plays a considerable role in harm reduction, the male-dominant gender composition of coaches and their clients should be acknowledged as a distinct trend worthy of further discussion. This point is particularly salient considering the suggested increasing use of IPEDs amongst women, and the specific use patterns and harms related to this population (Sverkersson et al., 2024).
Further relating to the clientele of IPED coaches, it should be noted that the lack of female clientele reported within this study does not necessarily mean that females seek IPED coaching less frequently than males. While IPED use is less prevalent within female populations compared to their male counterparts (e.g., Kimergård & McVeigh, 2014), research indicates there is growing use amongst this population (Piatkowski, Whiteside, et al., 2024). Indeed, a preference for same-sex coaching relationships may offer an explanation as to why the majority of clientele within this study were male. For instance, within Gibbs et al.'s (2022a) study, one IPED coach reported limiting his client base to males only, due to his limited knowledge of female anatomy, IPED use, and long-term negative side effects. It is therefore plausible that this was also true of the male IPED coaches within the current study, hence the lack of female clientele they worked with, reflecting their commitment to responsible and ethical practice (e.g., Piatkowski, Cox, & Collins, 2024). Similar parallels can be drawn from the work of Sverkersson et al. (2024), who note that women seek IPED information online, however, males sometimes muddy the waters, and provide inaccurate and non-adapted information to females. This is problematic from a public health perspective, as misinformation has the potential to shape community norms, beliefs, and behaviours. Such evidence holds weight in the current investigation concerning IPED coaches, with some coaches underprepared and ill-equipped to support female clients, but perhaps taking them on nevertheless, in order to earn capital.
Moving beyond the demographics of their client base, IPED coaches’ commitment to responsible and ethical practice was further exemplified within the sources they used to educate themselves and further their knowledge of IPED use. As found within Piatkowski et al.’s (2024b) research, coaches reported relying on scientific research articles and other online sources for their IPED information, providing support for previous anecdotal claims that well-intentioned coaches will actively seek knowledge on best practice relating to IPED (Piatkowski & Dunn, 2022). As noted elsewhere in the literature, expertise that is built through exchanges of ethnopharmacological knowledge enables the transition from IPED consumer to IPED manufacturer (Monaghan, 2002; Piatkowski, Cox, et al., 2025). Applying this understanding to the context of IPED coaches specifically, it can be understood that through utilising sources such as scientific articles, coaches develop their ethnopharmacological knowledge (Monaghan, 2002), which in turn, sets IPED coaches apart from their non-coaching peers, making them a well sought-after and profitable commodity (Gibbs et al., 2022a). Elsewhere, this collective approach to knowledge building within the IPED community has been referred to as ‘broscience’ (see Underwood, 2025), but such an approach has not been investigated for its potential to reduce harm. Importantly, however, IPED coaches might also draw upon online information sources which might contain dubious sources of information. For example, Cox and Paoli (2023) investigated ‘PIED influencers,’ and recognized that whilst these individuals provided a range of important information informed in-part by science, some individuals provided sometimes risky information which might influence and increase health harms. Further, trust asymmetries, whereby clients place greater trust in IPED coaches over healthcare professionals, have the potential to increase harm by shifting power dynamics and concentrating influence in non-clinical settings. While these qualities foster connection and support, they empower coaches to guide client health decisions on issues that may exceed their expertise (Piatkowski, Cox, & Collins, 2024). The problematic nature of this is evident when such information is adapted and packaged up by IPED coaches, who harness the potential to shape the behaviours of a subsection of the IPED-consuming community.
Turning attention towards the profitability of IPED coaching, although the body of literature surrounding IPED coaches underscores their credibility, IPED coaching is inextricably linked to financial gain for those offering such services (e.g., Gibbs et al., 2022a; Piatkowski et al., 2024). Profit-driven motives have the potential to significantly shape the behaviour of IPED coaches, as financial incentives may influence not only their business practices but also the kind and quality of information they share with clients. For example, Piatkowski, Cox, and Collins (2024) note that coaches act as ‘gatekeepers’ of knowledge, controlling access and dissemination in a manner that serves both harm reduction and business interests. Researchers have indicated the ways in which IPED coaches attempt to capitalise on the profitability of their vocation, marketing themselves and their services by leveraging their own physical appearances, that is their ‘body capital’ (Piatkowski, Cox, et al., 2024), building trusting relationships with clients (Piatkowski, Cox, & Collins, 2024), and advertising their services on social media platforms (Gibbs et al., 2022a). Similar strategies were also reported within the current study, in which IPED coaches used platforms such as Instagram and YouTube to market their coaching services. With social media having previously been identified to facilitate the promotion of IPEDs, including AAS (Cox et al., 2023; Cox & Piatkowski, 2026), this is not surprising. Importantly, this focus on financial gain often overlaps with another key aspect of IPED coaching: involvement in the supply of IPEDs.
Substantial crossovers exist between IPED coaching and supply (Gibbs et al., 2022a) offering another avenue for IPED coaches’ financial gain. Such crossovers were exemplified within the current study, whereby a small proportion (i.e., 12.5%) of IPED coaches reported supplying IPED to their clients, with a greater number (i.e., 45.8%) confirming that they recommended trusted suppliers to their clients. Although some IPED coaches do so in line with their harm reduction motives, to ensure clients are accessing trusted and reputable IPED sources, the fact that IPED coaches undoubtedly have a vested interest in themselves as a service provider, and potentially a vested interest in the IPED sources they supply or recommend, poses a significant conflict of interest (e.g., Gibbs et al., 2022a; Piatkowski et al., 2024). When individuals within the community adopt the dual role of IPED coach and IPED supplier, profit-driven motives have the potential to undermine harm reduction and care-based motives, which in turn has implications in terms of jeopardising the health of the IPED consumer/client base (Piatkowski, Cox, & Collins, 2024). In order to truly understand the potential harm clients may be exposed to when the boundaries between IPED coaching and supply become blurred, future research should explore the extent to which IPED coaches hold a vested interest in the IPEDs they recommend or supply. For example, by considering Gibbs’ (2023) supplier typologies and expanding upon them to apply to the IPED coaching community specifically.
Finally, in relation to the types of IPED consumed by IPED coaches, the current study found that coaches personally utilised a range of injectable (primarily Testosterone) and oral (primarily Anavar) steroids, in addition to other drugs such as thermogenic compounds (primarily Clenbuterol), and ancillary compounds (primarily Aromasin). These findings bear importance, given the role of IPED coaches’ lived experiences in relation to their coaching practices (Gibbs et al., 2022a; Piatkowski et al., 2024) and the range of specific harms associated with each route of administration (Cox, Piatkowski, & Dunn, 2025). Extant research has demonstrated that the coaching practices of IPED coaches are not only based upon their engagement with various reputable sources of knowledge, but are also influenced by their own experimentation and lived experiences with drugs (Piatkowski, Cox, & Collins, 2024; Piatkowski, Cox, et al., 2025). The use of personal experience as a tool to guide IPED-related advice-giving also extends beyond the community of IPED coaches, to IPED influencers online (Cox & Paoli, 2023).
Taking this into consideration, it is plausible that the drugs of choice selected by the coaches within this study may reflect the drugs being recommended and/or supplied to clients, which in turn has implications in terms of potential harms that clients are exposed to. In essence, where IPED coaches possess high levels of ethnopharmacological knowledge derived through personal experience, there may be a protective downstream effect for their clientele, whereby coaches’ lived experiences serve as valuable lessons, teaching them about the physical and psychological consequences associated with various drugs, in turn enabling them to guide others more effectively (Monaghan, 2002; Piatkowski, Cox, et al., 2024). On the other hand, where coaches lack ethnopharmacological knowledge or lived experience of IPED use, this may pose significant risk for clients to whom they recommend or prescribe potentially deleterious IPED protocols. Indeed, the liability of such advice is dubious from an ethical, legal, and a public health perspective, with some coaches receiving criticism for their role within their clients’ deaths (Abelson et al., 2022).
Limitations
Whilst the current study offers novel insights into IPED coaches’ drug choices and the scope of their IPED coaching services, several limitations persist. Firstly, participant retention issues were evident within the current study, with significant attrition witnessed over the course of the survey. Valid response rates varied between questions, resulting in incomplete data for several questions and subsequently, a smaller dataset than anticipated. Additionally, the study acknowledges the potential impact of section-to-section attrition within the survey, whereby participant dropout may lead to incomplete response patterns and reduced statistical power, thereby limiting the generalisability and interpretive robustness of the findings. Data was also of a self-report nature, meaning amongst those valid responses provided, social desirability responding may have been present (Brenner, 2020). This is a particularly salient consideration considering the sensitive nature of the topics explored within the survey, and the hard-to-reach nature of the IPED community. Although, the anonymous and online format of the survey served to counteract this as much as possible. Much like previous studies (e.g., Piatkowksi et al., 2024a), the generalisability of these findings is further limited by the uneven gender distribution present within the sample. It is plausible that women’s experiences of IPED use, as well as the coaching services they provide, differ in meaningful ways from those of men; however, the predominantly male composition of the present sample precludes any robust comparative analysis or gender-specific conclusions.
Future Research
Researchers should attempt to recruit a larger sample of IPED coaches, comprised equally of males and females, and building upon Cox et al. (2025) recent study, should include more participants from the Global South to ensure representativeness to the wider IPED coaching population (Cummings, 2018). In addition, to allow more interpretive conclusions to be drawn regarding the different types of IPED coaches that exist, future researchers should continue to explore the varying experiences and practices of IPED coaches, including their personal IPED consuming history (e.g., lived experience of harms), their journey to becoming an IPED coach (e.g., their process of knowledge acquisition), as well as the exact nature of the IPED services they offer. Gaining a greater understanding of these areas may help to determine at which point IPED consumers/non-coaches make the switch to become an IPED coach, and provide a more nuanced understanding of the different backgrounds, practices, and behaviours of IPED coaches. In turn, this may assist with the generation of a complete typology of the different types of IPED coaches that exist (Gibbs et al., 2022b), as seen already in relation to both IPED consumers (e.g., Christiansen et al., 2017; Zahnow et al., 2018), and IPED suppliers (Gibbs, 2023). Developing a typology of IPED coaches, specifically, has important practical implications in terms of raising awareness of the reputable and unreputable coaches that may exist within the community, such as those who may act with good intention, and those who may be profit- and/or supply-driven (Gibbs et al., 2022a, 2022b; Harvey & van Teijlingen, 2022).
Conclusion
In conclusion, the current study was the world’s first to utilise a cross-sectional survey design to examine the ways in which IPED coaches provide support for the IPED community. Drawing upon the concept of ethnopharmacology, this study builds upon extant knowledge relating to IPED coaches by exploring IPED coaches’ lived experiences of IPED use, and the ways in which they acquire and disseminate their IPED knowledge through their coaching services. In addition, this study is the first to demonstrate the scope of services offered by IPED coaches, including the size (i.e., 0-70+ clients) and reach (i.e., national and international) of their client base, and the types of services offered (i.e., bloodwork analysis, drug supply). These findings lay the foundations for further research into the nature and practice of IPED coaching, to develop a comprehensive typology of the different types of IPED coaches that may exist. Of particular importance is building a clearer picture of female IPED coaches, who currently remain a vastly under-represented population. From a public health perspective, the development of a typology could inform harm reduction interventions, identify best practice, and ensure living-lived experience is embedded within future approaches seeking to provide support, care, and guidance to IPED communities.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.