
Abstract
While studies have found medication assisted treatment (MAT) to produce beneficial outcomes, few scholars have explored the immediate impact of jail-based MAT on mental well-being. Improved mental well-being arising from MAT participation in jail may increase the likelihood of continued participation in MAT post-release. To understand the impact of jail-based MAT on psychological well-being, pre- and post-test surveys with residents from a county jail in the northeastern U.S. were conducted to measure changes in stress, anxiety, depression, and self-esteem. The study also explored possible differences between jail residents participating in MAT alone and those who combined MAT with other available treatment programs. Results revealed significant differences in anxiety and stress among those participating in MAT. Bivariate and multivariate analyses also indicate that MAT combined with a jail-based drug treatment community, produces better outcomes than MAT alone.
Keywords
Introduction
While medication-assisted treatment (MAT) constitutes the standard of care for opioid dependency, few incarcerated persons have access to MAT during their incarceration (Linden et al., 2018). Opioid use disorder (OUD) is the most common medical issue found among incarcerated populations (Ferguson et al., 2019), leaving offenders at high risk for overdose following release (Brinkley-Rubinstein et al., 2019). Participating in MAT appears to result in significantly lower mortality rates among those with OUD, compared to non-MAT participants, especially within the month following release (Chladek & Chui, 2024; Ma et al., 2019). Additionally, when someone with OUD is incarcerated in a facility without the opportunity for MAT, the severe withdrawal symptoms experienced can create an aversion to MAT participation in the future (Maradiaga et al., 2016).
Creating a positive MAT experience for those incarcerated with OUD may help to increase MAT adherence long after release. Psychological well-being is an important component to both sobriety and MAT adherence, and the association between stress and addiction is well-established, encompassing both the emergence and reinstatement of addictive patterns (Sinha, 2008). To understand the role MAT plays in an incarcerated person’s well-being, pre- and post-test surveys were distributed to MAT participants in a northeast jail to determine the impact of MAT on jail participants after four weeks. MAT’s impact on mental health outcomes were examined along with the differences between those who participated in MAT and those who participated in MAT combined with other therapeutic treatments. Results suggest that combining additional treatments with medication-assisted treatment (MAT) may be more effective than MAT alone. These findings reinforce the critical need for continued MAT support for individuals released from incarceration, especially given evidence of higher treatment adherence rates when MAT is initiated during incarceration.
Literature Review
Opioid use disorder (OUD) affects an estimated 16 million individuals globally, with 3 million cases reported in the United States (U.S.)
MAT – Medication Assisted Treatment
MAT is the standard of care recommended for OUD, particularly in its ability to reduce the morality rate from overdose, by the National Institute on Drug Abuse (NIDA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the American Medical Association (AMA) and the World Health Organization (WHO; Martin et al., 2019; Westreich, 2019). However, despite these recommendations, coupled with the high rate of OUD among incarcerated populations, there is limited MAT programming available inside American carceral institutions, which limits the ability of medical professionals to provide proper medical care (Bovell-Amnon et al., 2024; Linden et al., 2018). Despite increased availability of MAT in jails within the past decade, significant access barriers remain (Chladek & Chui, 2024). MAT is available in approximately 25% of jails and these jails are most likely in urban settings, leaving rural populations vulnerable. Furthermore, there appears to be insufficient support for MAT among rural corrections administrators (Thomas & Coveney, 2023). Without MAT, withdrawal symptoms can be severe and painful (i.e., nausea, vomiting, diarrhea, body aches, etc.), and given the availability of effective treatments, some argue that withholding MAT is not only considered inhumane but violates the Hippocratic oath of “do no harm” (Bruce & Schleifer, 2008).
Benefits of MAT Within Carceral Institutions
When MAT is available for incarcerated persons, the results are quite promising. The risk of fatal overdose is substantially decreased for individuals with OUD after release from incarceration, making this a critical period for intervention and support (Brinkley-Rubenstein et al., 2019). Medications typically used in MAT programs are buprenorphine (a partial opioid agonist which binds to opioid receptors and reduces cravings, as well as withdrawal symptoms), methadone (a synthetic opioid agonist that activates opioid receptors in the brain and decreases withdrawal symptoms), and naltrexone (a competitive mu-opioid receptor antagonist that blocks the uptake of opioids in the receptors; when given in injectable form, it does not have the same potential for misuse or diversion when compared to other MAT drugs). The most commonly used buprenorphine-related drugs are Sublocade (buprenorphine extended-release injection) and Suboxone (a combination of buprenorphine and naloxone, which is a film for sublingual or buccal use). Subutex (buprenorphine taken sublingually) was removed from the market in 2011 due to concerns with misuse. Cost is a factor that must be considered. While Naltrexone can be given once a month in injectable form (Vivitrol), eliminating the issue of drug diversion and reducing the number of staff needed to distribute medication, it is the most expensive MAT medication, costing $14,112 per year, per client, while buprenorphine and methadone’s direct yearly costs are less than half of naltrexone ($5,980 per year and $6,552 per year respectively; NIDA, 2018).
Previous studies provide empirical support for the implementation of MAT in correctional institutions, most commonly decreased drug use, recidivism, and mortality rates. A MAT intervention implemented with the Rhode Island Department of Corrections (DOC) resulted in decreased withdrawal symptoms, decreased use of drugs while incarcerated, and an increased commitment to continue MAT after release (Brinkley-Rubenstein et al., 2019). Most importantly, participants felt that the availability of MAT led to a more positive environment, which was conducive to maintaining their sobriety. In another study of the Rhode Island DOC (Martin et al., 2019), the majority of those in MAT while incarcerated continued in a community-based MAT program upon release. Within the Massachusetts Department of Correction, MAT participants also had lower rates of overdose deaths following release (Bovell-Amnon et al., 2024).
A meta-analysis conducted by Moore et al. (2019) found that methadone given during incarceration increased one’s treatment adherence following release and decreased overall drug use but did not impact recidivism rates. In contrast, other researchers found appreciable effects on recidivism rates with MAT (Evans et al., 2022; Pecoraro & Woody, 2011). Results from Moore et al.’s (2019) meta-analysis suggest that buprenorphine and naltrexone are more effective in decreasing drug use after release when compared to methadone. In another study of residents at Riker’s Island in New York City, no difference was found in drug use or recidivism rates between MAT participants on buprenorphine or methadone; however, those on buprenorphine were more likely to continue their treatment upon release when compared to those on methadone (Magura et al., 2009). Overall, MAT use during incarceration leads to decreased substance use (for opioids, as well as other drugs), decreased recidivism, and increased treatment adherence (Boksán et al., 2023). Despite some contrary findings, empirical data demonstrate positive outcomes.
Barriers to MAT within Carceral Institutions
Barriers to MAT implementation within American correctional facilities are not atypical and include, but are not limited to, funding, space, client resistance, and negative staff perception regarding MAT and OUD (Ferguson et al., 2019). When a correctional institution is planning to implement MAT, there is concern about drug diversion. If not checked properly after drug administration, participants can “cheek” and sell their medications. This issue is addressed in a study of rural jail residents using injectable Vivitrol, an injectable form of naltrexone (Bratina et al., 2020). With injections, diversion is not possible, and daily administration is not necessary (i.e., shots are administered monthly). Although long-acting injectable medications can eliminate the risk of drug diversion and do not require daily administration, staff resistance to MAT can still present a significant challenge. While negative staff views of MAT can be a barrier to its implementation, those views can be overcome with time, training, and education (Thomas & Coveney, 2023). Other studies find that improvements are needed in existing MAT programs including wait time before receipt of the first dose, more accessibility to treatment-related programming to support MAT such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), earlier discharge planning to increase treatment adherence within the community, and education and training of staff to reduce the stigma often associated with MAT (Brinkley-Rubenstein et al., 2019). Such education and training helps staff to view OUD as a medical condition requiring treatment (Pecoraro & Woody, 2011). It is also important to remember that while MAT may be available at a county jail, it is not necessarily available upon transfer to a state or federal prison and discontinuing MAT during incarceration can create severe withdrawal symptoms, leading to future MAT aversion (Maradiaga et al., 2016). Additionally, resistance to MAT can be found among potential clients. Those with OUD believe that using MAT while incarcerated might increase their drug tolerance, leading to more painful withdrawals in the future (Fox et al., 2015).
Stress, Anxiety, Depression & Self-Esteem
When individuals enter the correctional system, they often bring with them a complex history of mental health and substance use challenges. Stress, anxiety, and depression are commonly found in persons who are incarcerated and often co-occur with substance abuse disorder, which is also highly prevalent among incarcerated individuals (Willy-Gravley et al., 2021). Untreated, these mental health conditions can contribute to maladaptive behaviors (Collica-Cox et al., 2024; Thomas & Coveney, 2023) and can have very serious effects on one’s physical health (Trivedi, 2004). Although low self-esteem may play a role in the development of substance use issues, the impact of self-esteem on treatment outcomes remains unclear, with research yielding mixed results (Yang et al., 2019). Moreover, the relationship between self-esteem and crime is complex and not fully understood, with some research findings yielding a correlation between low self-esteem and crime and others indicating the opposite (Oser, 2006).
There is comorbidity between stress, anxiety, depression, suicidal ideations, and PTSD, which can all be manifestations of trauma (Belet et al., 2020). When left untreated, they can also serve as a hindrance to one’s sobriety. Stress, anxiety, and depression are correlated with relapse, as well as delayed treatment response (Andreescu et al., 2007; Kushner et al., 2000; Mulder et al., 2009; Sinha, 2008). There is limited research on the connection between MAT and its direct impact on such psychological stressors. Existing research demonstrates mixed results with some showing that MAT, without alternative treatment, may not be enough to produce a significant impact (Zullig et al., 2018) and others demonstrating the hypothesized direction (Amura et al., 2022). These studies, however, have examined community-based MAT, rather than institutional MAT. Solutions is a 6-week cognitive behavioral therapy based residential drug treatment program at the WCDOC and overseen by staff from St. John’s Riverside Hospital. While the Solutions program has not specifically been the subject of empirical research, prior research indicates that CBT-based drug treatment programs can reduce the odds of relapse (Lopez et al., 2021; Pelisser et al., 2001). Furthermore, CBT combined with pharmacotherapies like MAT have been found to be more effective at reducing relapse than CBT alone (Lopez et al., 2021).
Methodology
This study was conducted with male and female residents housed in the Westchester County Department of Correction (WCDOC), a northeast suburban jail averaging less than 600 residents daily and serves as both a county jail and a federal holding facility. WCDOC, like all New York State jails, is subject to a state mandate to implement MAT programming in its facility. New York State’s medication-assisted treatment (MAT) law, signed by Governor Kathy Hochul, requires NY jails and prisons to provide medication-based treatment for people with substance use disorders (SUDs). The law went into effect on October 7, 2022, and includes appropriate screening for substance disorder, access to MAT medications such as methadone, buprenorphine, & naltrexone, access to qualified medical personnel who can make decisions regarding dosing and treatment, and discharge planning (see Consolidated Laws of New York, 2024, 2025).
Anyone in WCDOC screened and verified as having substance abuse disorder (SUD) can obtain MAT. While MAT participants are offered a drug treatment community and/or other drug-related programming, it is not a requirement to obtain MAT while incarcerated or upon release. All MAT participants are offered discharge planning services to connect them with a community-based MAT provider, regardless of their treatment participation. If those with OUD are on MAT in the community, they can continue their treatment upon admission to the facility. Others who were not on MAT in the community upon their arrest, but screen positively for SUD upon jail admission, will work with medical personnel to choose a preferred MAT medication. New York State (NYS) law requires that all three MAT medications – buprenorphine, methadone, and naltrexone – be offered to every incarcerated person who presents with SUD.
Sample
WCDOC, which partners with a community-based hospital, St. John’s Riverside Hospital, for MAT services, provided the researchers with a list of MAT participants on a monthly basis. After a two-week quarantine period, but within of month of intake, eligible participants were invited to participate in a survey regarding their experiences in the MAT program. Participants were informed that this process was confidential and voluntary, and all participants were required to read and sign the consent form, which has been approved by a university Institutional Review Board (IRB). Within four weeks, the same participants (if still in the facility) would be called down by the researcher to complete a second survey. This survey would seek to measure any changes between the pre- and post-tests within the four weeks a resident participated in the MAT program. Upon completing the second survey, participants received a $5 calling card for their assistance.
The sample consists of 154 demographically diverse MAT participants. The sample is primarily male, as is common for incarcerated samples (see Table 1). Across genders, the sample has a roughly equal distribution of Caucasian, African American, and Latinx participants, with an average age of 39. A majority of the sample had completed no more than a high school diploma or GED and were unemployed at the time of arrest. While most of the men reported being single and never married, only 17% of the women reported similarly.
Measures
Stress, anxiety, and depression were assessed using the DASS-21 Scale, a Likert-type instrument with response options ranging from “does not apply to me at all” (0) to “applies to me most of the time” (3; Lovibond & Lovibond, 1995). The scale consists of seven items per subscale, with scores categorized into five severity levels ranging from ‘normal’ to ‘extremely severe,’ calculated by averaging the responses within each subscale. Measures for each subscale (stress, anxiety, depression) were created by taking the sum of values in each subscale. Pre- and post-test differences for all three subscales were calculated for use in multivariate analysis. The DASS-21 has been deemed to be valid and reliable for measuring these psychological states (Brown et al., 1997; Crawford & Henry, 2003; Osman et al., 2012) and has been applied in various contexts (Caravaca Sánchez et al., 2019; Kavanagh et al., 2010), including among incarcerated men (Grennan & Woodhams, 2007).
Self-esteem was evaluated using Rosenberg’s 10-item Guttman self-esteem scale, which has demonstrated strong reproducibility and scalability (Rosenberg, 1965). Pre- and post-test values and pre- and post-difference measures of self-esteem were created similarly to the DASS-21 measures. The Rosenberg scale is a reliable predictor of varying self-esteem levels (O'Brien, 1985) and has been validated for use in incarcerated populations in previous studies (Folk et al., 2019). Responses are recorded on a Likert-type scale, ranging from “strongly agree” to “strongly disagree.”
Predictors used in multivariate analysis included typical demographic information and self-reported substance use and criminal history. Demographic data collected included age, gender, and race. Other demographic items included education level (less than high school, high school diploma/GED, etc.), religion measured as self-reported religious affiliation with choices for atheism and agnosticism, employment status (none, part-time, full-time), and marital status (single/never married, married, co-habitation, divorced/separated, and widowed).
Data for several non-demographic items were also collected, largely focusing on participants’ histories with substance use and treatment. The post-test measured treatment program participation by asking if they had participated in Solutions, Narcotics or Alcohol Anonymous (NA/AA), or some other program and was dummy coded as 0 or 1 depending on whether or not they participated in a particular program. Participants were also asked to self-report any emergency room (ER) visits for alcohol, drugs, or both during the previous 12 months, with 40% of the sample reporting visiting an ER for those reasons. Self-reported MAT type was measured by asking participants if they were prescribed methadone (40%), buprenorphine (56%), or naltrexone (4%).
Results
Bivariate Models
The first of two sets of two-sample t-tests were used to determine if statistically significant differences existed between pre- and post-test measures for stress, anxiety, depression, and self-esteem (see Table 2). Results indicated no significant differences in pre- and post-test depression or self-esteem measures. However, decreased anxiety (t [7753] = 14.542, p < .001) and stress (t [7001] = 7.643, p < .001) levels were found to be statistically significant.
The second set of two-sample t-tests revealed that observed differences in outcome measures between Solutions participants and non-Solutions participants were statistically significant (see Table 3). Solutions participants experienced decreased levels of depression (t [6465.01] = 5.276, p < .001) and anxiety (t [6503.48] = 2.429, p < .05) compared to non-participants. Contrary to expectations, Solutions participants expressed an increase in stress levels in post-testing compared to the non-Solutions group (t [6900] = −2.067, p < .05). Solutions participants also demonstrated a significant increase in self-esteem compared to those not in Solutions (t [3454.96] = −3.339, p < .01).
Finally, the study examined mental health outcome differences based on prior MAT, comparing those who had participated in MAT during the 12 months prior to arrest with those who had not. Results indicated significant group-based differences for all four mental health outcomes (see Table 4). Compared to those without recent MAT history, those who had participated in MAT in the previous 12 months expressed increased depression (t [2382.02] = −9.794, p < .001), anxiety (t [2637.97] = −5.016, p < .001), and stress (t [2187.92] = −5.905, p < .001). Prior MAT participants also reported lower self-esteem (t [852.617] = −2.936, p < .01). While unanticipated, the changes in mental health outcomes may point towards participants’ experiencing unfavorable emotions caused by returning to jail despite being in treatment.
Examining group-based differences between Solutions participants and non-Solutions participants for prior MAT and no prior MAT (see Tables 5 and 6), significant differences were discovered. Among those without MAT use in the previous 12 months, Solutions participants reported increases in depression (t [1121.85] = −2.634, p < .01), anxiety (t [1660] = −6.18), p < .001), stress (t [1509] = −9.758, p < .001), and self-esteem (t [660.7) = −4.485, p < .001) compared to non-Solutions participants. The observed increases in depression, anxiety, and stress combined with decreased self-esteem again may indicate the impact of being incarcerated on the individual’s mental health. In contrast, among those who had been in a MAT program before arrest, decreases in depression (t [4836.34] = 6.615, p < .001), anxiety (t [5286] = 5.216, p < .001), and stress (t [4639.19] = 3.015, p < .01) were observed possibly highlighting the importance of combining MAT with other treatment programs.
Multivariate Models
Backward stepwise OLS regression models were used to examine possible differences between Solutions participants and non-Solutions participants among inmates engaged in MAT when controlling for demographic measures and treatment histories (see Tables 7–10). While there was no significant change in self-esteem based on Solutions participation, the models revealed significant reductions in depression (b = −1.46, p < .001), anxiety (b = −1.095, p < .001), and stress (b = −.559, p < .01).
MAT medication differences were found to have some impact on mental health outcomes. Compared to those taking methadone, MAT participants taking naltrexone experienced lower levels of anxiety (b = −3.465, p < .001) and higher self-esteem (b = 6.037, p < .001). Similarly, those taking buprenorphine experienced less anxiety (b = −.637, p < .01) compared to those taking methadone. However, buprenorphine users reported higher levels of depression (b = 1.307, p < .001) and stress (b = .964, p < .001) and lower self-esteem (b = −2.153, p < .001) compared to methadone users.
OLS models also revealed that participants’ prior emergency room (ER) visits impacted mental health outcomes. Compared to participants who did not visit an ER for a substance-use related issue in the last year, those who visited an ER for alcohol treatment reported lower levels of depression (b = −1.204, p < .05) and stress (b = −1.561, p < .01). Substance-use related ER visits in the previous year resulted in higher levels of depression (b = .389, p < .05, stress (b = 1.272, p < .001) and self-esteem (b = .887, p < .001). Finally, those who sought ER treatment for both alcohol and drugs, compared to those who had not, reported lower depression (b = −4.829, p < .001) and stress (b = −3.6027, p < .001), but increased anxiety (b = 1.250, p < .001).
As expected, demographic characteristics had some impact on mental health outcomes. Compared to male participants, females experienced less depression (b = −3.105, p < .001), anxiety (b = −1.608, p < .001), and stress (b = −3.048, p < .001) while taking MAT. However, females also reported lower self-esteem compared to the men (b = −.503, p < .05). Compared to Caucasians, African-American participants experienced increased stress (b = 2.368, p < .001) and depression (b = .465, p < .05) along with lower self-esteem (b = −2.612, p < .001). In contrast, Latinx participants demonstrated lower levels of depression (b = −1.655, p < .001), anxiety (b = −1.72, p < .001), stress (b = −1.776, p < .001), and self-esteem (b = −.774, p < .001).
Differences in mental health outcomes based on educational achievement were also noted. Compared to those without a high school diploma or a GED, increased depression levels were reported by those with a high school diploma or GED (b = .650, p < .01), some college but no degree (b = 1.273, p < .001), and a vocational certificate or college degree (b = 2.623, p < .001). Similar results were found when examining anxiety levels for high school graduates (b = 1.189, p < .001), those with some college (b = 2.927, p < .001), and a college or vocational degree (b = 4.387, p < .001). Stress levels were also higher for those with only some college (b = .713, p < .01) or a college degree (b = 4.298, p < .001) compared to those without a high school diploma. While self-esteem was found to be higher among those with high school diplomas compared to those without (b = .659, p < .001), those with some college (b = −1.268, p < .001) or a degree (b = −1.537, p < .001) reported lower self-esteem.
Participants’ outcome measures were also significantly affected by relationship status. Married participants reported lower anxiety (b = −.338, p < .01) compared to those who were single and never married. Interestingly, they also displayed lower self-esteem (b = −.4.9, p < .001) compared to unmarried participants. Results were similar for those who were either divorced, widowed, or separated who reported lower depression (b = −3.399, p < .001), anxiety (b = −1.385, p < .001), stress (b = −2.71, p < .001), and self-esteem (b = −.544, p < .01). Those who were living with an intimate partner reported both higher self-esteem (b = 2.309, p < .001) and lower levels of depression (b = −1.221, p < .001), anxiety (b = −1.986, p < .001), and stress (b = −1.598, p < .001) compared to unmarried participants.
Finally, those who were employed full or part-time reported significant change on outcome measures when compared to unemployed participants. Part-time workers reported lower levels of depression (b = −1.713, p < .001), anxiety (b = −2.065, p < .001), stress (b = −2.407, p < .001), and self-esteem (b = −2.093, p < .001). While full-time employees demonstrated high levels of depression (b = 1.421, p < .001), anxiety (b = 1.25, p < .001), and stress (b = 1.313, p < .001), as well as lowered self-esteem (b = −1.822, p < .001).
Discussion
The findings add to the existing literature by focusing on the immediate impact of MAT within a jail-based population. While bivariate analyses found significant reductions in stress and anxiety over a short four-week treatment period, results for depression and self-esteem were mixed or insignificant. This suggests that MAT, although effective in managing some mental health outcomes within a short timeframe, may require more time to produce meaningful impacts. Bivariate results indicating improvements in stress, anxiety, and depression with those continuing MAT after their arrest, without comparable improvements among those without a recent history of MAT, serve to reinforce this conclusion. Observed increases in mental health outcomes and decreases in self-esteem may be indicative that individuals on MAT in the community experience more harmful effects on mental health and self-concept.
Multivariate examination of the impact of prior MAT participation and Solutions combined with MAT provides a more comprehensive picture. Even when controlling for a recent history of MAT use, Solutions participation is associated with reduced depression, anxiety, and stress as anticipated. MAT’s impact on self-esteem appears to be mediated by the impact of increasing education level, relationship status, and employment status. Interestingly, in contrast to the bivariate results, prior MAT participation effects are mixed and only significant for depression and anxiety. Further, these results may indicate an increased vulnerability to worsening mental health outcomes among individuals being arrested despite being in treatment. Future studies may look to examine how arrests for drug impact mental health outcomes differently than arrests for other reasons. Results of the present study may indicate that incorporating group-based substance treatment in addition to MAT is more likely to create desired benefits to clients during short-term jail stays than MAT alone. More study, however, is needed to verify these conclusions.
Limitations
Several limitations were associated with the current study design. First, research conducted within correctional settings often faces significant methodological challenges, which limit the generalizability and validity of findings (Wimberly & Xue, 2016). This study lacked a true comparison group and randomization of subjects, limiting the ability to draw definitive conclusions about the effectiveness of the intervention. Although there was no randomization of subjects, all MAT participants were given the opportunity to complete the survey. Second, while some research suggests that programming of eight weeks or longer is more effective than shorter programming (Taylor et al., 2020), our analysis of the MAT intervention was limited to four weeks. Even at four weeks, due to the transient nature of the jail setting, several pre-tested participants left the facility prior to post-testing. While eight weeks or longer may prove to be most effective, anything longer than four weeks in the jail setting is unlikely to yield an adequate sample size. Finally, jail intake processes and scheduling resulted in pre-testing that sometimes occurred after participants began the MAT program. However, the period between pre- and post-testing remained largely consistent throughout the study.
Policy Implications & Future Research
For MAT to be most effective, it is crucial to have leadership from government and correctional officials, adequate funding, and strong partnerships with community-based organizations (Ferguson et al., 2019). To implement a successful program, support from correctional administrators and staff, a strong community partnership, detailed policies and procedures, education and training for both staff and participants, and discharge planning are essential (Meyer et al., 2023). While participation in MAT can impact recidivism and overdose rates, those released from carceral institutions often have difficulty accessing MAT in the community, which is an integral component of their rehabilitative and reintegrative success (Chladek & Chui, 2024). Common characteristics of effective community programming for MAT include mobile treatment, text messaging to remind participants of appointments, peer support, and MAT education. More effort is needed to ensure a seamless transition to community-based MAT, and transportation issues must be addressed. Drug exposure and stress-related life events pose challenges for MAT adherence, but interventions that provide access to MAT and MAT education are likely to provide more effective treatment (Fox et al., 2015).
If incarcerated participants feel that the availability of MAT leads to a more positive environment, which is conducive to maintaining their sobriety, it is important for the state to provide funding to support treatment that complements MAT (Brinkley-Rubenstein et al., 2019). MAT, without supplemental treatment, may not be enough to produce a significant impact on psychological factors such as stress, anxiety, and depression, all of which are important to maintaining sobriety (Zullig et al., 2018). While MAT reduces overdose deaths, to reduce relapse, MAT participants would benefit more by participating in a therapeutic community while incarcerated.
NYS legislators may want to consider reforming parts of the state mandated MAT legislation. If federal detainees are transferred to another federal facility and cannot continue their MAT, they may not be suitable candidates. Federal detainees will experience withdrawal symptoms upon transfer. If the research reveals that this can create an aversion to MAT participation in the future, it seems counterproductive to the law's intended objectives (Maradiaga et al., 2016).
Future research may want to focus on studies that examine treatment adherence for longer periods after release, as well as the cost-effectiveness of using MAT in the correctional setting, compared to the costs associated with overdose and rearrest (Kelly & Rosenberg, 2024). This can be particularly challenging in a transient setting like the jail system. The average jail stay is approximately 25 days compared to an average prison stay of 2.6 years (4.7 years for those with a violent crime; Kaeble, 2018; Zeng, 2018). This makes assessment and follow-up quite difficult. Researchers may also want to conduct a more detailed cost-benefit analysis of naltrexone in injectable form. While it is the most expensive MAT medication, it eliminates the possibility of drug diversion and misuse, and only needs to be administered monthly, rather than daily like other MAT medications. Fewer trips to the clinic and fewer investigations for disciplinary infractions from misuse or diversion of MAT medication may help offset some of the direct higher costs associated with injectable naltrexone. Lastly, more funding is needed to track individuals in the community for longer periods to determine if they are continuing their treatment and more research is needed to determine which types of alternative treatment are most effective for MAT participants during and after incarceration.
Footnotes
Consent to Participate
Study methodology and informed consent procedures were approved by the Stephen F. Austin State University Institutional Review Board (IRB-FY2025-38). Informed consent was obtained from all participants in writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Biographies
Appendix
Descriptive Statistics Note. N = 154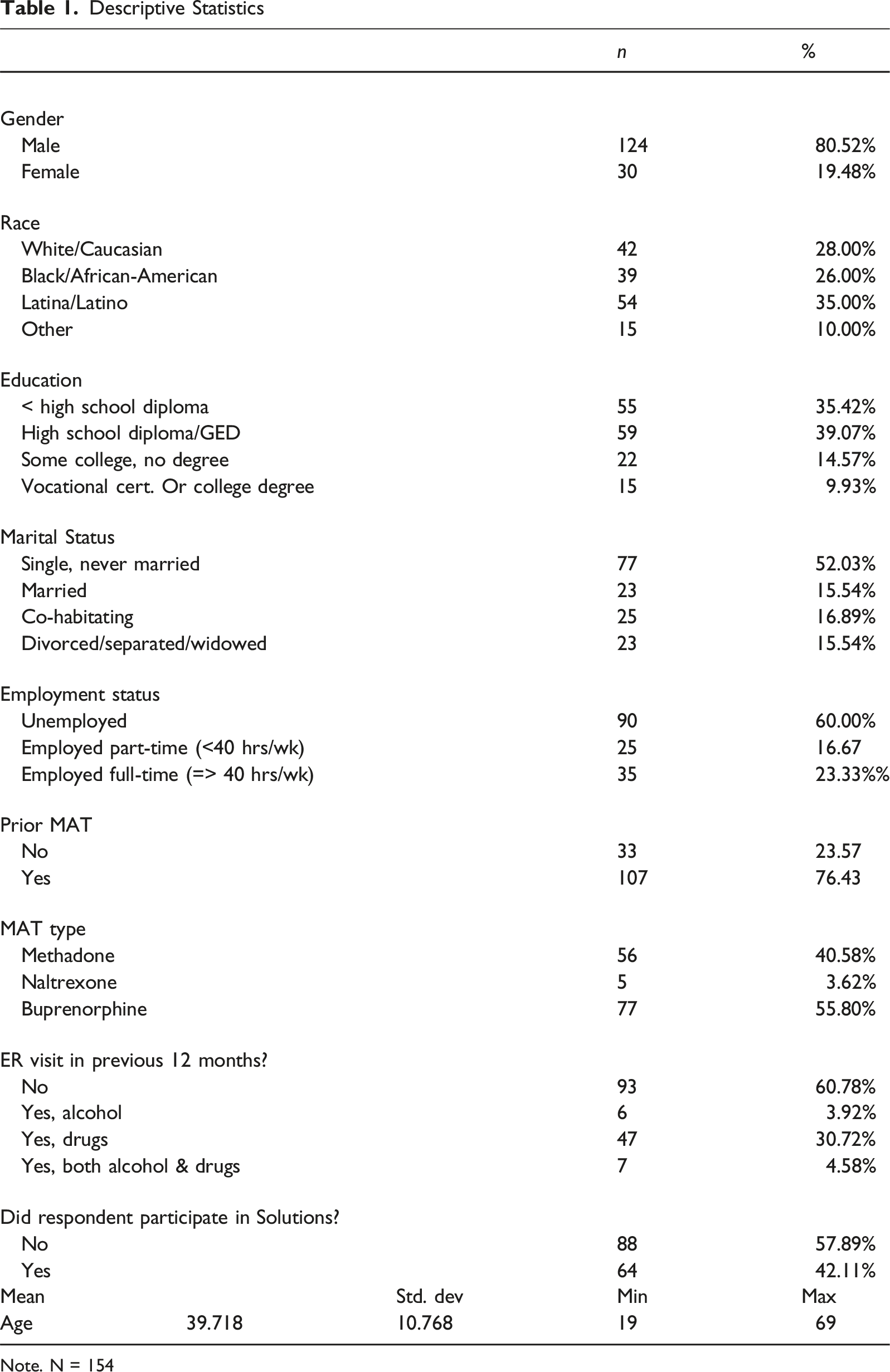
n
%
Gender
Male
124
80.52%
Female
30
19.48%
Race
White/Caucasian
42
28.00%
Black/African-American
39
26.00%
Latina/Latino
54
35.00%
Other
15
10.00%
Education
< high school diploma
55
35.42%
High school diploma/GED
59
39.07%
Some college, no degree
22
14.57%
Vocational cert. Or college degree
15
9.93%
Marital Status
Single, never married
77
52.03%
Married
23
15.54%
Co-habitating
25
16.89%
Divorced/separated/widowed
23
15.54%
Employment status
Unemployed
90
60.00%
Employed part-time (<40 hrs/wk)
25
16.67
Employed full-time (=> 40 hrs/wk)
35
23.33%%
Prior MAT
No
33
23.57
Yes
107
76.43
MAT type
Methadone
56
40.58%
Naltrexone
5
3.62%
Buprenorphine
77
55.80%
ER visit in previous 12 months?
No
93
60.78%
Yes, alcohol
6
3.92%
Yes, drugs
47
30.72%
Yes, both alcohol & drugs
7
4.58%
Did respondent participate in Solutions?
No
88
57.89%
Yes
64
42.11%
Mean
Std. dev
Min
Max
Age
39.718
10.768
19
69
Pre-/post-test Comparison, t-test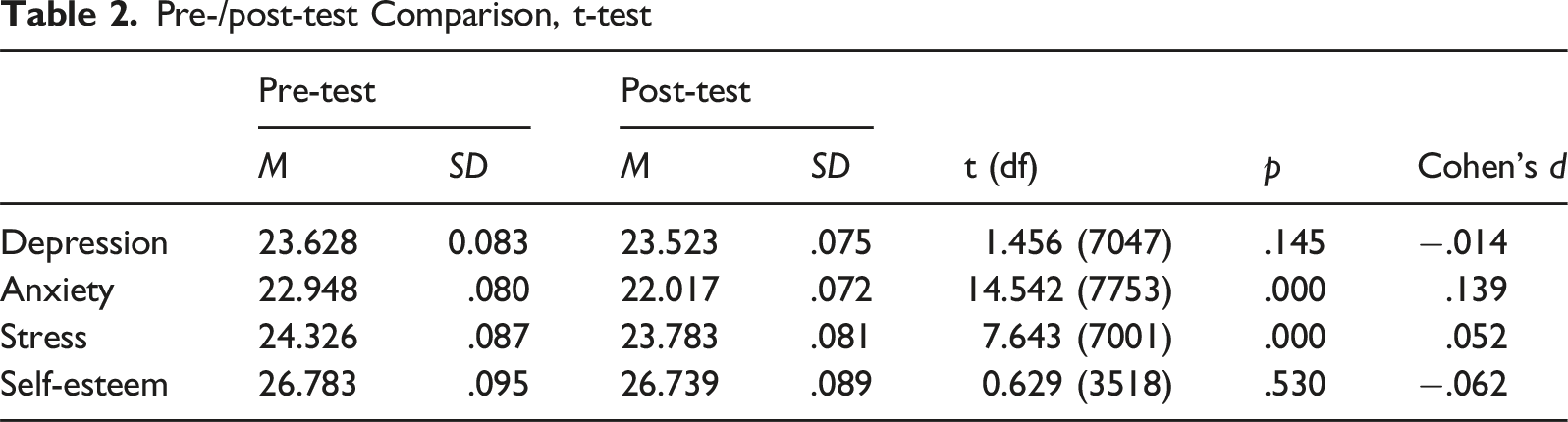
Pre-test
Post-test
t (df)
p
Cohen’s d
M
SD
M
SD
Depression
23.628
0.083
23.523
.075
1.456 (7047)
.145
−.014
Anxiety
22.948
.080
22.017
.072
14.542 (7753)
.000
.139
Stress
24.326
.087
23.783
.081
7.643 (7001)
.000
.052
Self-esteem
26.783
.095
26.739
.089
0.629 (3518)
.530
−.062
Solutions/non-solutions Comparison, t-test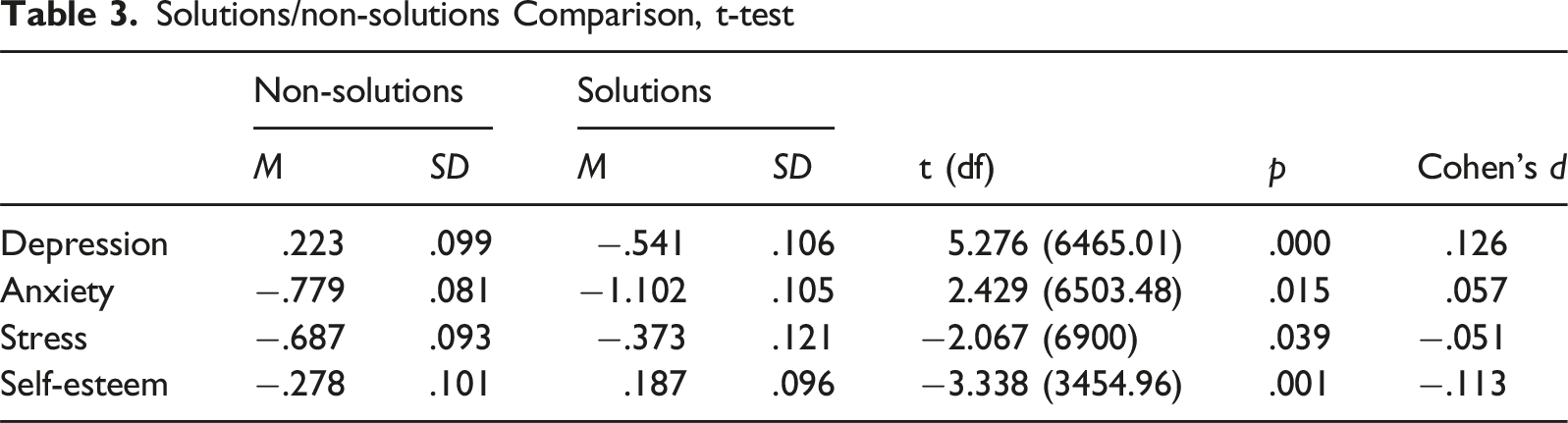
Non-solutions
Solutions
t (df)
p
Cohen’s d
M
SD
M
SD
Depression
.223
.099
−.541
.106
5.276 (6465.01)
.000
.126
Anxiety
−.779
.081
−1.102
.105
2.429 (6503.48)
.015
.057
Stress
−.687
.093
−.373
.121
−2.067 (6900)
.039
−.051
Self-esteem
−.278
.101
.187
.096
−3.338 (3454.96)
.001
−.113
Prior MAT/no-Prior MAT Comparison, t-test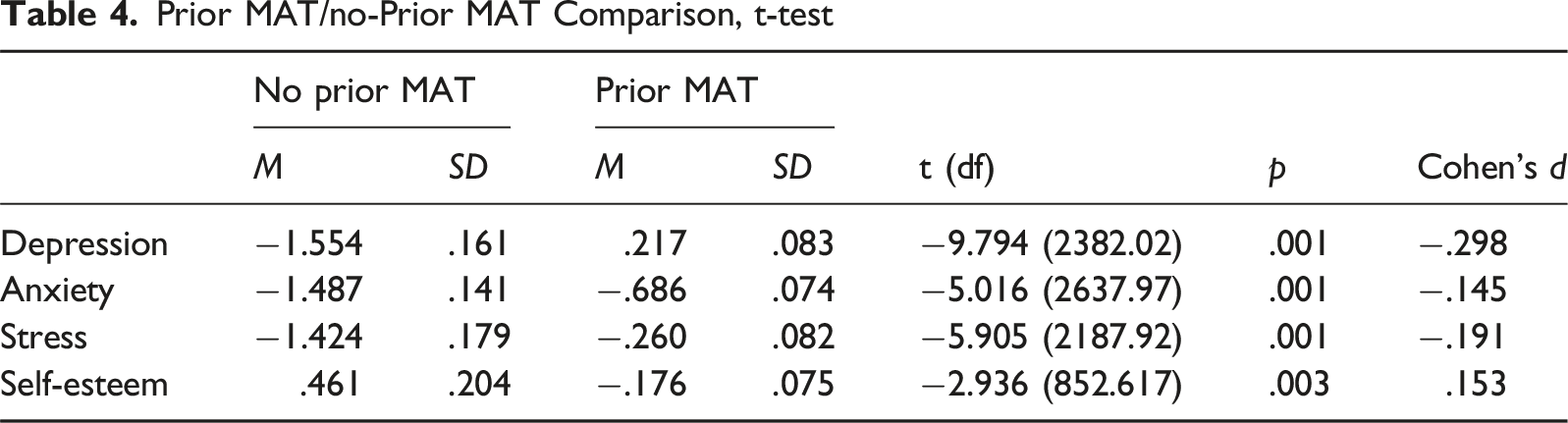
No prior MAT
Prior MAT
t (df)
p
Cohen’s d
M
SD
M
SD
Depression
−1.554
.161
.217
.083
−9.794 (2382.02)
.001
−.298
Anxiety
−1.487
.141
−.686
.074
−5.016 (2637.97)
.001
−.145
Stress
−1.424
.179
−.260
.082
−5.905 (2187.92)
.001
−.191
Self-esteem
.461
.204
−.176
.075
−2.936 (852.617)
.003
.153
Solutions/non-solutions Comparison Without MAT, t-test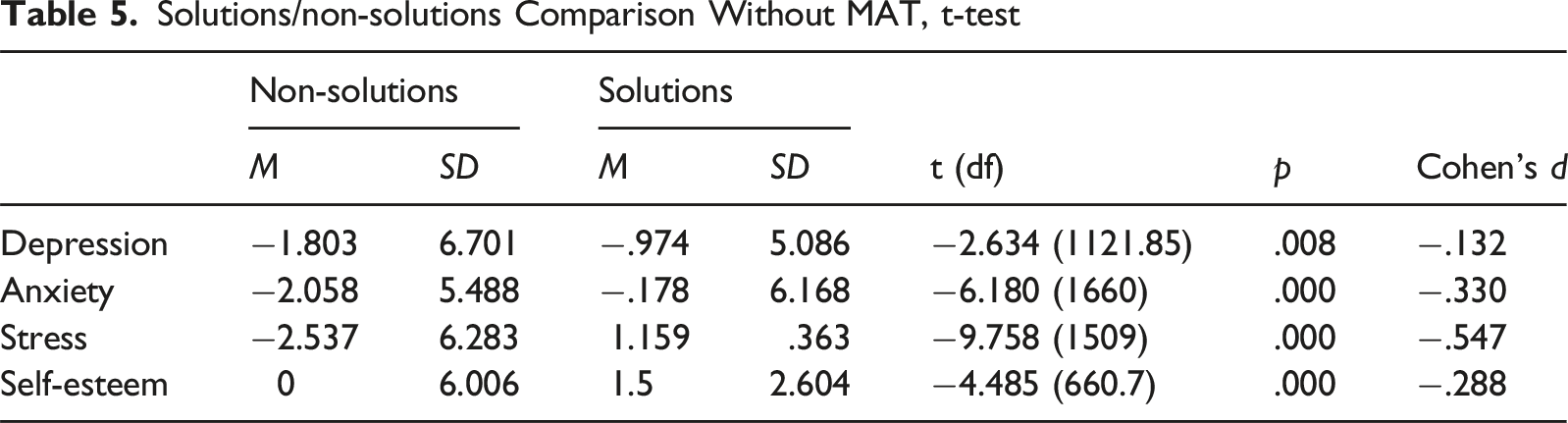
Non-solutions
Solutions
t (df)
p
Cohen’s d
M
SD
M
SD
Depression
−1.803
6.701
−.974
5.086
−2.634 (1121.85)
.008
−.132
Anxiety
−2.058
5.488
−.178
6.168
−6.180 (1660)
.000
−.330
Stress
−2.537
6.283
1.159
.363
−9.758 (1509)
.000
−.547
Self-esteem
0
6.006
1.5
2.604
−4.485 (660.7)
.000
−.288
Solutions/non-solutions Comparison With MAT, t-test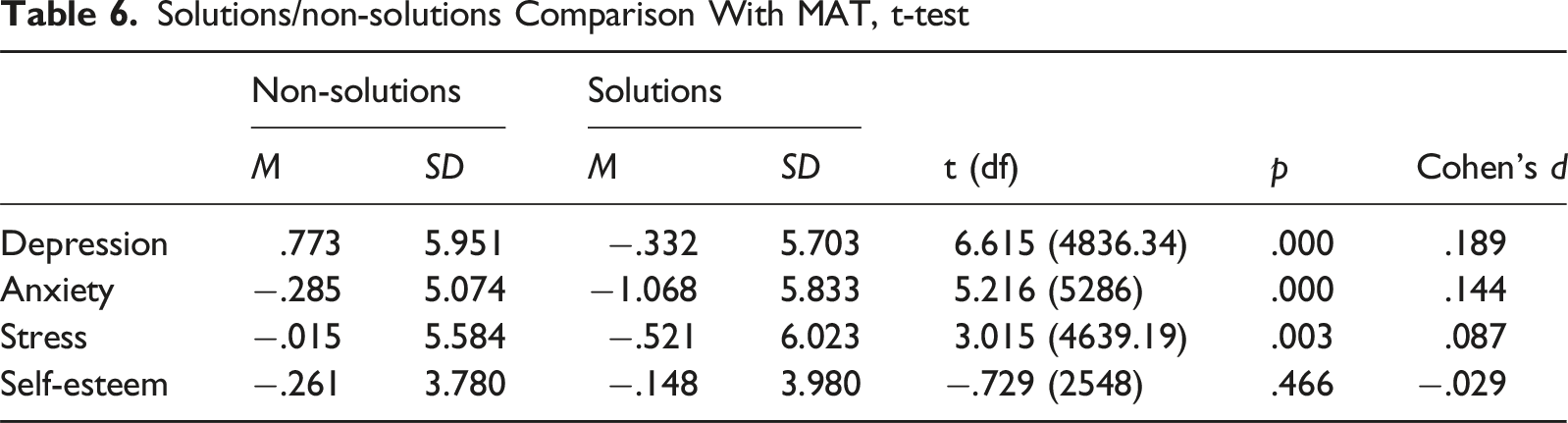
Non-solutions
Solutions
t (df)
p
M
SD
M
SD
Cohen’s d
Depression
.773
5.951
−.332
5.703
6.615 (4836.34)
.000
.189
Anxiety
−.285
5.074
−1.068
5.833
5.216 (5286)
.000
.144
Stress
−.015
5.584
−.521
6.023
3.015 (4639.19)
.003
.087
Self-esteem
−.261
3.780
−.148
3.980
−.729 (2548)
.466
−.029
Regression Results - Depression Note. n = 5275; F(18, 5256) = 77.71, p < .001; Adj R2 = .207.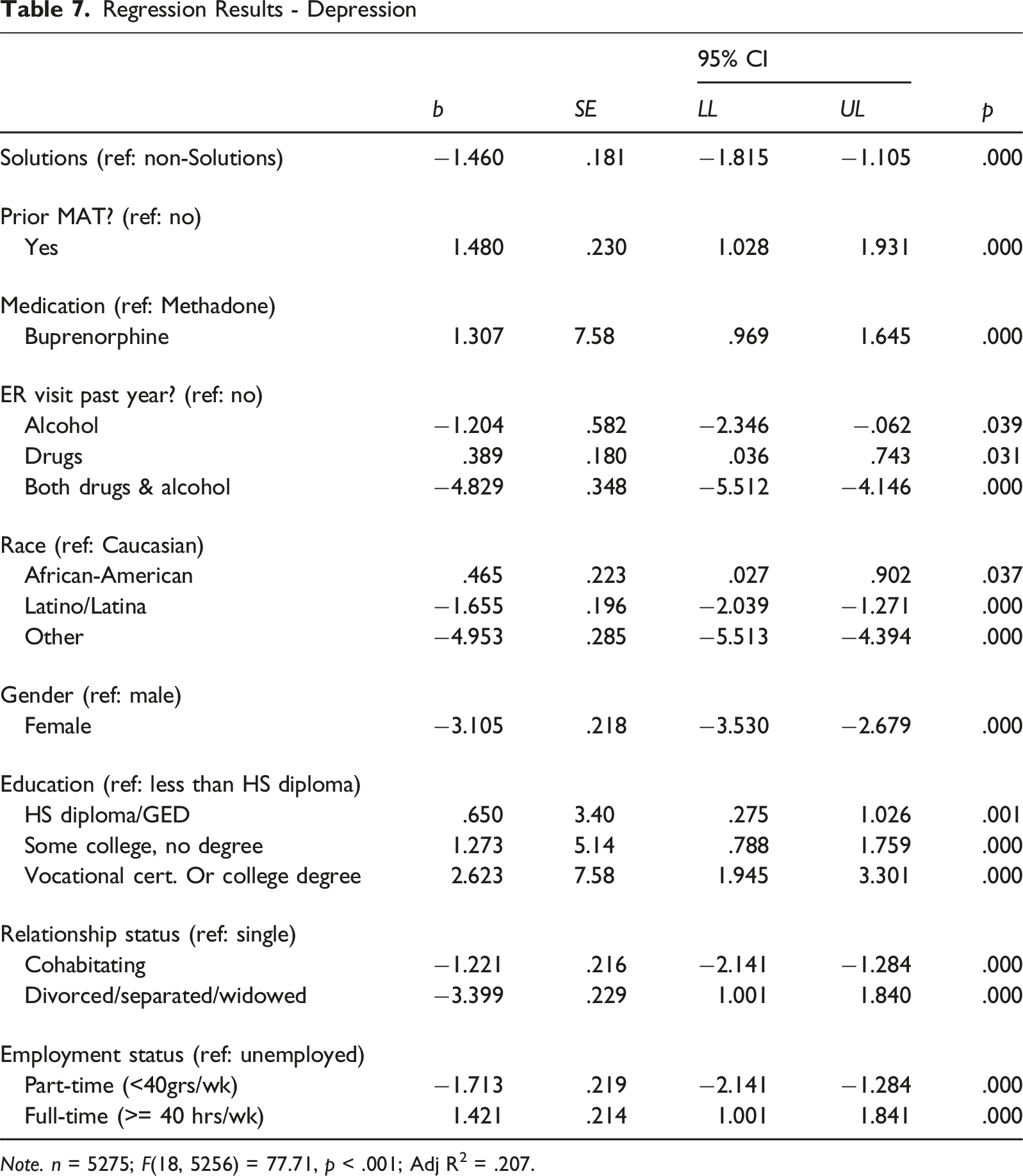
b
SE
95% CI
p
LL
UL
Solutions (ref: non-Solutions)
−1.460
.181
−1.815
−1.105
.000
Prior MAT? (ref: no)
Yes
1.480
.230
1.028
1.931
.000
Medication (ref: Methadone)
Buprenorphine
1.307
7.58
.969
1.645
.000
ER visit past year? (ref: no)
Alcohol
−1.204
.582
−2.346
−.062
.039
Drugs
.389
.180
.036
.743
.031
Both drugs & alcohol
−4.829
.348
−5.512
−4.146
.000
Race (ref: Caucasian)
African-American
.465
.223
.027
.902
.037
Latino/Latina
−1.655
.196
−2.039
−1.271
.000
Other
−4.953
.285
−5.513
−4.394
.000
Gender (ref: male)
Female
−3.105
.218
−3.530
−2.679
.000
Education (ref: less than HS diploma)
HS diploma/GED
.650
3.40
.275
1.026
.001
Some college, no degree
1.273
5.14
.788
1.759
.000
Vocational cert. Or college degree
2.623
7.58
1.945
3.301
.000
Relationship status (ref: single)
Cohabitating
−1.221
.216
−2.141
−1.284
.000
Divorced/separated/widowed
−3.399
.229
1.001
1.840
.000
Employment status (ref: unemployed)
Part-time (<40grs/wk)
−1.713
.219
−2.141
−1.284
.000
Full-time (>= 40 hrs/wk)
1.421
.214
1.001
1.841
.000
Regression Results - Anxiety Note. n = 5790; F(18, 5771) = 76.06, p < .001; Adj R2 = .189.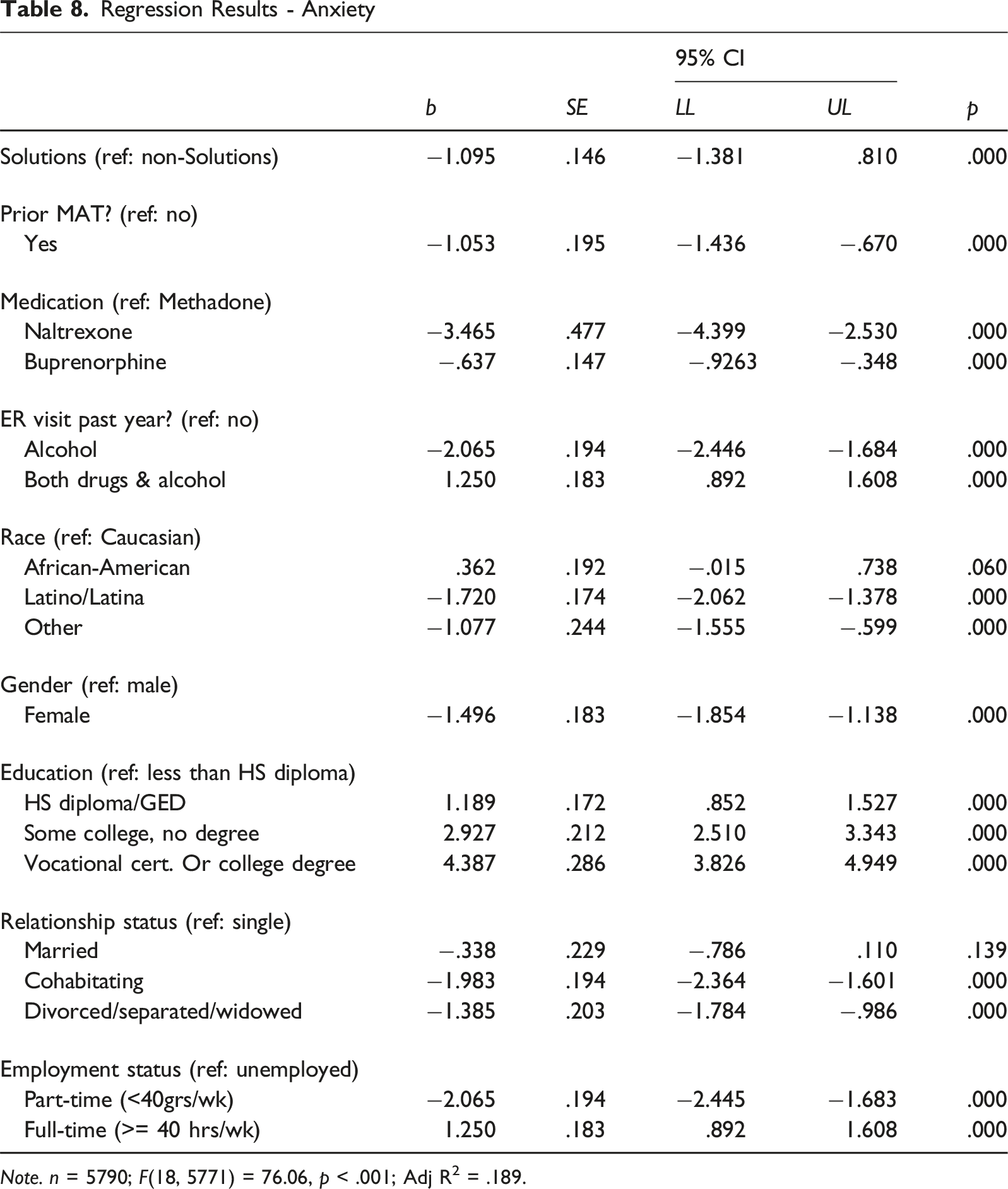
b
SE
95% CI
p
LL
UL
Solutions (ref: non-Solutions)
−1.095
.146
−1.381
.810
.000
Prior MAT? (ref: no)
Yes
−1.053
.195
−1.436
−.670
.000
Medication (ref: Methadone)
Naltrexone
−3.465
.477
−4.399
−2.530
.000
Buprenorphine
−.637
.147
−.9263
−.348
.000
ER visit past year? (ref: no)
Alcohol
−2.065
.194
−2.446
−1.684
.000
Both drugs & alcohol
1.250
.183
.892
1.608
.000
Race (ref: Caucasian)
African-American
.362
.192
−.015
.738
.060
Latino/Latina
−1.720
.174
−2.062
−1.378
.000
Other
−1.077
.244
−1.555
−.599
.000
Gender (ref: male)
Female
−1.496
.183
−1.854
−1.138
.000
Education (ref: less than HS diploma)
HS diploma/GED
1.189
.172
.852
1.527
.000
Some college, no degree
2.927
.212
2.510
3.343
.000
Vocational cert. Or college degree
4.387
.286
3.826
4.949
.000
Relationship status (ref: single)
Married
−.338
.229
−.786
.110
.139
Cohabitating
−1.983
.194
−2.364
−1.601
.000
Divorced/separated/widowed
−1.385
.203
−1.784
−.986
.000
Employment status (ref: unemployed)
Part-time (<40grs/wk)
−2.065
.194
−2.445
−1.683
.000
Full-time (>= 40 hrs/wk)
1.250
.183
.892
1.608
.000
Regression Results - Stress Note. n = 5239; F(16, 5222) = 82.55, p < .001; Adj R2 = .199.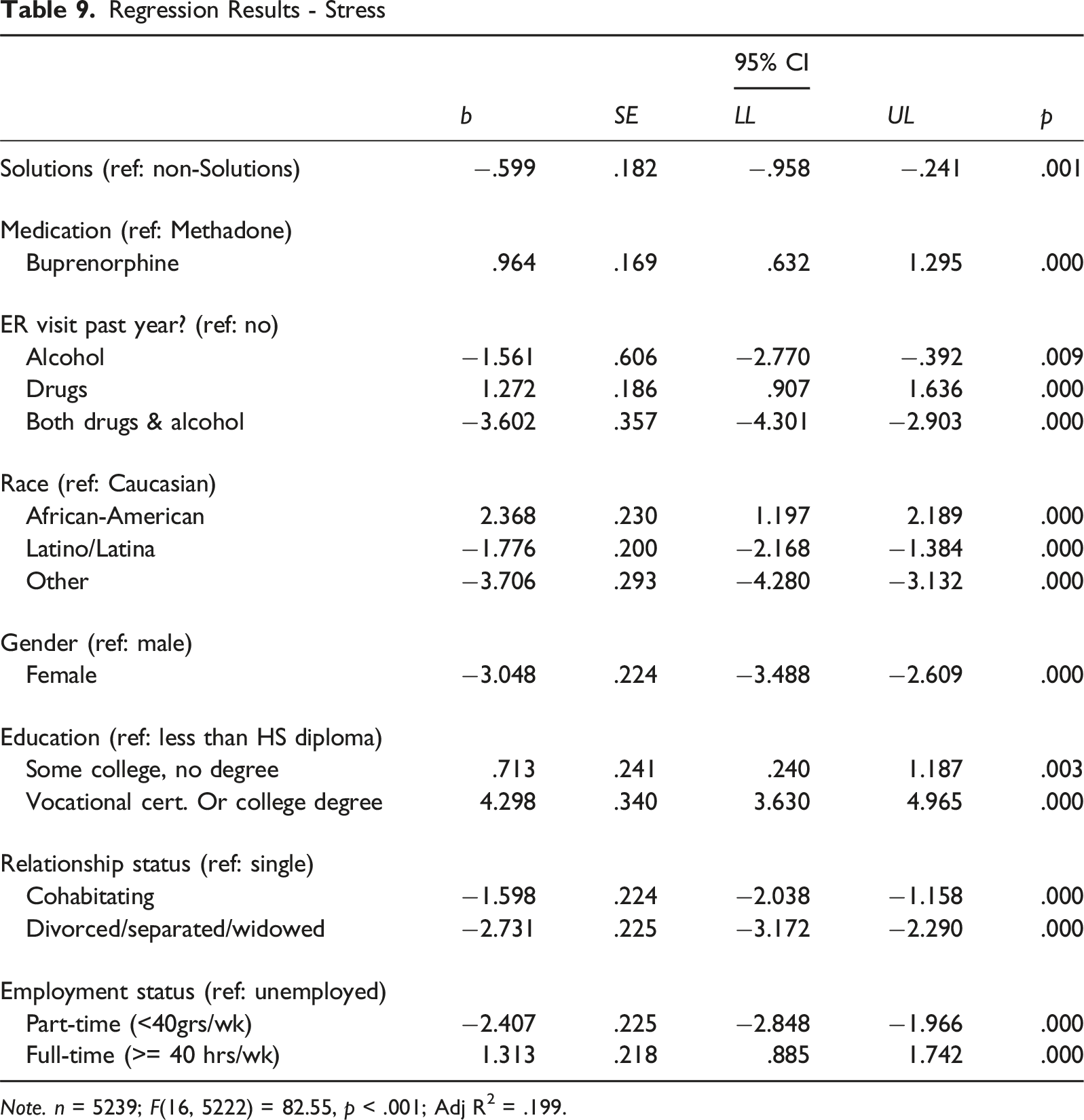
b
SE
95% CI
UL
p
LL
Solutions (ref: non-Solutions)
−.599
.182
−.958
−.241
.001
Medication (ref: Methadone)
Buprenorphine
.964
.169
.632
1.295
.000
ER visit past year? (ref: no)
Alcohol
−1.561
.606
−2.770
−.392
.009
Drugs
1.272
.186
.907
1.636
.000
Both drugs & alcohol
−3.602
.357
−4.301
−2.903
.000
Race (ref: Caucasian)
African-American
2.368
.230
1.197
2.189
.000
Latino/Latina
−1.776
.200
−2.168
−1.384
.000
Other
−3.706
.293
−4.280
−3.132
.000
Gender (ref: male)
Female
−3.048
.224
−3.488
−2.609
.000
Education (ref: less than HS diploma)
Some college, no degree
.713
.241
.240
1.187
.003
Vocational cert. Or college degree
4.298
.340
3.630
4.965
.000
Relationship status (ref: single)
Cohabitating
−1.598
.224
−2.038
−1.158
.000
Divorced/separated/widowed
−2.731
.225
−3.172
−2.290
.000
Employment status (ref: unemployed)
Part-time (<40grs/wk)
−2.407
.225
−2.848
−1.966
.000
Full-time (>= 40 hrs/wk)
1.313
.218
.885
1.742
.000
Regression Results – Self-Esteem Note. n = 2856; F(18,2837) = 67.08, p < .001; Adj R2 = .294.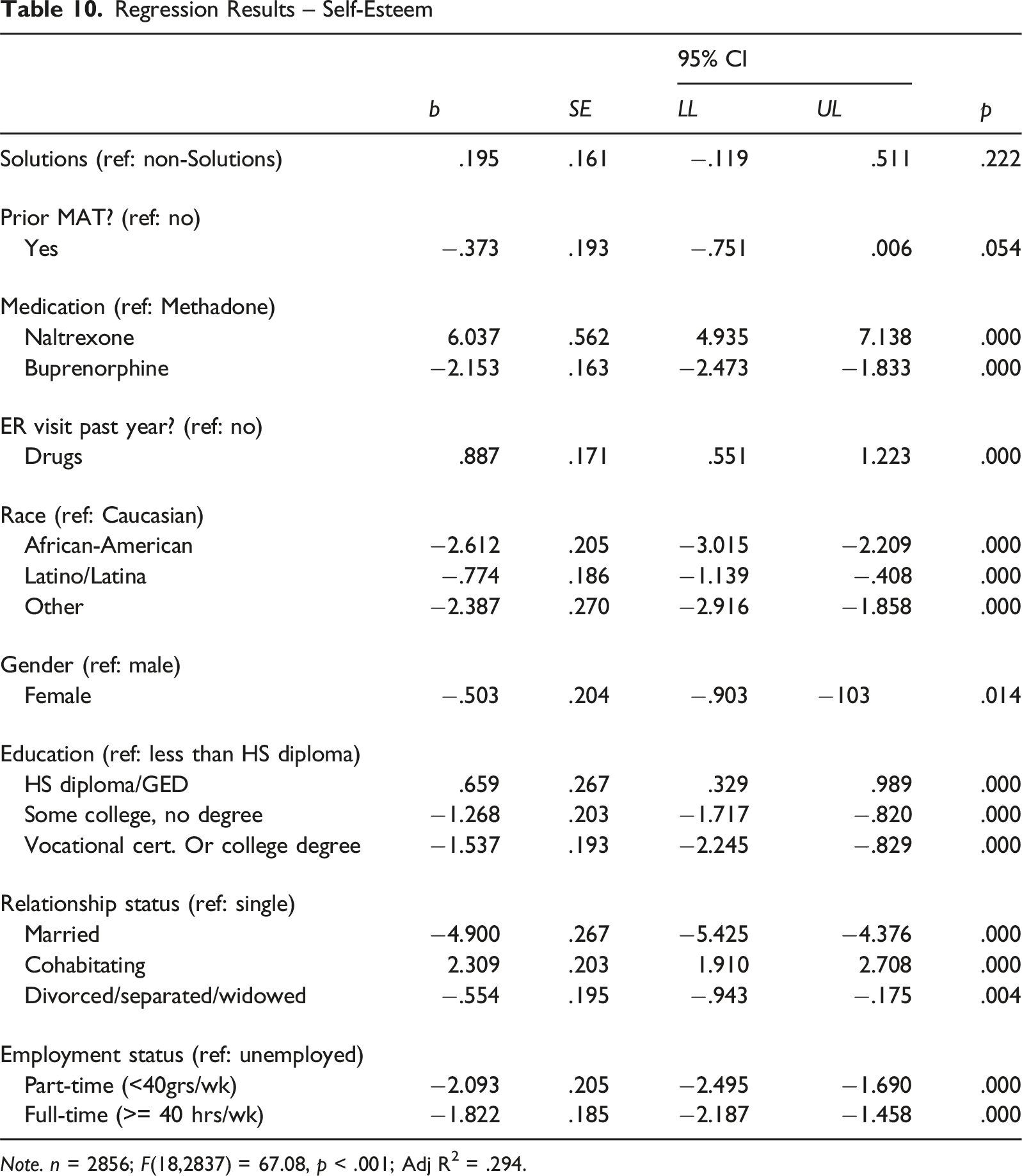
b
SE
95% CI
p
LL
UL
Solutions (ref: non-Solutions)
.195
.161
−.119
.511
.222
Prior MAT? (ref: no)
Yes
−.373
.193
−.751
.006
.054
Medication (ref: Methadone)
Naltrexone
6.037
.562
4.935
7.138
.000
Buprenorphine
−2.153
.163
−2.473
−1.833
.000
ER visit past year? (ref: no)
Drugs
.887
.171
.551
1.223
.000
Race (ref: Caucasian)
African-American
−2.612
.205
−3.015
−2.209
.000
Latino/Latina
−.774
.186
−1.139
−.408
.000
Other
−2.387
.270
−2.916
−1.858
.000
Gender (ref: male)
Female
−.503
.204
−.903
−103
.014
Education (ref: less than HS diploma)
HS diploma/GED
.659
.267
.329
.989
.000
Some college, no degree
−1.268
.203
−1.717
−.820
.000
Vocational cert. Or college degree
−1.537
.193
−2.245
−.829
.000
Relationship status (ref: single)
Married
−4.900
.267
−5.425
−4.376
.000
Cohabitating
2.309
.203
1.910
2.708
.000
Divorced/separated/widowed
−.554
.195
−.943
−.175
.004
Employment status (ref: unemployed)
Part-time (<40grs/wk)
−2.093
.205
−2.495
−1.690
.000
Full-time (>= 40 hrs/wk)
−1.822
.185
−2.187
−1.458
.000