
Abstract
Introduction
The United States has made marked improvements in addressing the opioid overdose crisis, with recent data from the Centers for Disease Control and Prevention (CDC) suggesting the fewest number of overdose fatalities in any 12-month period since 2020 (CDC, 2025). Despite this progress, the human toll of the decades-long crisis looms large. More than 645,000 people in the United States have died of an opioid-involved overdose since the opioid epidemic began, a death toll that has been exacerbated by worsening mental health across the country (Congressional Budget Office, 2022). Nearly two-thirds of individuals with an opioid use disorder also meet the criteria for a psychiatric comorbidity (Evans et al., 2020; Hser et al., 2015; Jones & McCance-Katz, 2019; Substance Abuse and Mental Health Services Administration, 2023b).
The mix of private and public payors contributes to a fragmented national health care landscape. Each payer has its own coverage policies, provider networks, health information technology and quality requirements, and level of accountability to behavioral health parity laws (Erickson et al., 2020; Ettner et al., 2016; Kessel et al., 2015; McConnell et al., 2020). As a result, many Americans lack health coverage and those that do must navigate a system ill-suited for managing chronic and comorbid conditions (Enthoven, 2009). Integrated approaches to care, characterized by a high degree of communication between healthcare providers and the simultaneous treatment of both mental health and substance use concerns, are an important tool in addressing the ongoing opioid epidemic (Minkoff & Covell, 2022; SAMHSA, 2020). However, in reality, individuals often access care in settings poorly equipped to manage their co-occurring diagnoses, and as a result, many receive suboptimal care (Kilbourne et al., 2010; King et al., 2014; Mauro et al., 2016; McGovern et al., 2012; Snell-Rood et al., 2021).
Substance Use Recovery Housing
Recovery residences, sometimes referred to as “sober living homes” or “recovery homes” (Mericle et al., 2022), provide safe, communal housing for individuals in recovery from substance use (Mericle et al., 2015). The U.S. recovery residence landscape is diverse, with homes ranging from democratically run homes (Level I), houses managed by staff (Level II), staffed homes that include recovery-oriented services (Level III), and houses with clinical services (Level IV; National Alliance for Recovery Residences, 2016). Unlike treatment settings, such as inpatient medical or community detoxification services, recovery residences focus on social aspects of recovery. Across all four levels of recovery housing, the model is rooted in the idea that peers with similar lived experiences can build mutually supportive, recovery-sustaining relationships when living together (Jason et al., 2022; Polcin et al., 2014). Research on the impacts of recovery housing is growing. A recent systematic review highlighted that living in recovery housing was associated with improved substance use outcomes, better rates of employment, and higher income (Vilsaint et al., 2025). A cost-effectiveness analysis of a Level I housing organization suggests that while recovery housing is cost-effective, resulting in more than $17,000 of net benefit per resident when accounting for reduced criminal-legal system interactions and improved substance use outcomes (Lo Sasso et al., 2012).
Mental Health in Recovery Housing
There are few recovery housing resources specific to individuals with co-occurring mental health needs (Pannella Winn & Paquette, 2016). Recovery housing organizations may consider an individual’s mental health needs in determining if the home is adequately resources to meet the prospective resident’s needs (SAMHSA, 2023a). However, the prevalence of mental health diagnoses among those with substance use disorders is high. Unsurprisingly, this high comorbidity is reflected within recovery residences. Estimates suggest that as many as 79.8% of residents living in recovery housing meet the criteria for at least on mental health condition, and nearly one-third are taking at least one mental health medication (Krentzman et al., 2022; Majer et al., 2002; Polcin et al. 2012, 2014). The burden of mental health conditions in a recovery residence can create challenges within the home and for an individual’s overall recovery, with more severe mental health symptoms associated with worse retention in recovery residences, increased rule-breaking in the home, and a higher risk of returning to substance use (Polcin et al., 2012, 2014). Despite these challenges, recent studies suggest that people with co-occurring mental health needs, in many cases, can still be successful in and benefit from recovery residences (Polcin et al., 2012; Polcin & Korcha, 2017). A recent qualitative study on residents’ mental health revealed that the social support from other residents and house staff and safe living environment of the recovery home allowed individuals to integrate mental health recovery into their recovery from substance use (Stewart et al., 2024).
Medications for Opioid Use Disorder (MOUD) and Mental Health
Medications for opioid use disorder (MOUD) are the standard of care for managing opioid use disorder in the U.S. and include three medications approved by the Food and Drug Administration: methadone, buprenorphine, and extended-release injectable naltrexone (SAMHSA, 2021). Taking MOUD helps reduce opioid cravings and is associated with decreased opioid use and increased abstinence (National Academies of Science, Engineering, and Medicine, 2019). Many individuals who receive MOUD also have psychiatric comorbidities and are taking psychotropic medications (Morin et al., 2020; Peles et al., 2007; Samples et al., 2018). For example, 71.4–87% of individuals receiving MOUD reported at least one co-occurring psychiatric diagnosis, and nearly half were taking at least one psychiatric medication (Morin et al., 2020; Peles et al., 2007; Samples et al., 2018).
The interplay between MOUD and mental health can be complex. Co-occurring mental health conditions may impede MOUD initiation and lead to worse treatment outcomes (Bastien et al., 2024; Ghabrash et al., 2020; Litz & Leslie, 2017; Xu et al., 2023). Some people taking MOUD might experience side-effects that exacerbate their mental health challenges, such as anxiety or insomnia, and others must navigate medication interactions precipitated by concomitant psychotropic medication use (Elkader et al., 2009; Kampman & Jarvis, 2015; Lamont et al., 2020; Maremmani et al., 2019; Pedrelli et al., 2011; Zoorob et al., 2018). Most side-effects and contraindications are mild and well-managed in integrated health care models (Hurley et al., 2021). However, clinical case reports suggest that some people experience serious adverse psychiatric events, particularly when tapering or changing their medications (Agnoli et al., 2021; Goldstein & Jimenez, 2022; Lee et al., 2009; Lin et al., 2022).
The risks associated with MOUD use by individuals with co-occurring mental health needs are exacerbated by the complex, fragmented healthcare landscape of the United States. Patients may visit providers that are that are not linked through common health-information portals that would enable clinicians to share information about a patient’s different conditions and medications (Avula, 2020). As a result, side effects and contraindications that put patients’ health and safety at risk can be missed (Calcaterra et al., 2024). As a result, best practice is for individuals with co-occurring mental health concerns to receive ongoing psychosocial support during opioid pharmacotherapy (Kampman & Jarvis, 2015).
MOUD in Substance Use Recovery Housing
Traditionally, substance use treatment and recovery support service settings have stigmatized MOUD (Kepple et al., 2019), and recovery housing is no exception. Many recovery residences have historically not admitted clients taking MOUD (Jason et al., 2022; Wood et al., 2022). However, there has been an uptick in recent attention to the issue of MOUD-related stigma within recovery housing. In 2022, the Civil Rights Division of the US Department of Justice released guidance reiterating that individuals taking MOUD are protected from discrimination by the Americans with Disabilities Act (U.S. Department of United States Department of Justice, 2022), making it clear that practices like categorically denying people on MOUD from recovery housing are illegal. Two of the largest recovery housing networks, Oxford Houses and NARR, have released guidance documents designed to reduce discrimination towards prospective and current residents who are taking MOUD (Jason et al., 2025; NARR, 2019). The attempts to create a culture shift appear to be effective. Hernandez et al. (2025) pointed to the fact that 63.4% of recovery housing operators surveyed in Arizona reported that residents in their homes had access to MOUD. Similarly, Jason et al. (2025) found that approximately half of current residents and alumni living in Oxford Houses, a national network of Level I homes, felt positively or very positively about MOUD. Many recovery residence operators and staff desire support in adapting their residences to serve those taking medications (Miles et al., 2021). Currently, however, there is little guidance for residence operators, perhaps due to a lack of research on best practices for providing services to people using MOUD and living in recovery residences (NARR, 2018). Recent findings indicate that homes that cater to people taking MOUD help residents manage the medication-related stigma they face elsewhere in the larger recovery community (Gallardo, Wilkerson, et al., 2024). A recent qualitative study on recovery housing organizations serving clients taking MOUD also suggests that staff can help connect residents to MOUD providers and provide social and instrumental support (e.g., transportation) to help residents mitigate barriers to MOUD adherence (Gallardo, Zoschke, et al., 2024).
Given the prevalence of co-occurring mental health needs among those with a history of problematic opioid use, and considering the increasing number of recovery residences working to serve clients taking MOUD, it is likely that those running recovery residences will experience a greater number of clients with co-occurring mental health needs who are also taking MOUD. However, the dearth of literature on medication use within recovery residences means that the interaction between MOUD and mental health within these settings is poorly understood, leaving recovery residence operators with little guidance upon which to draw as they develop policies and procedures. Using qualitative data from a large sample of staff and residents living or working in recovery housing, we explore the complex interplay between MOUD and mental health within this unique setting. In particular, we drew on these interviews to understand mental health experiences of residents living in recovery homes serving clients taking MOUD and the operational considerations staff take as a result.
Methods
Parent Study
Here, we report on a subset of data from a larger, ongoing evaluation of substance use recovery housing for individuals taking MOUD, titled Housing for MAR Expanded Opioid Services (Project HOMES; Wilkerson et al., 2024). This project is currently evaluating 15 different National Association of Recovery Residence (NARR) accredited Level II and Level III recovery residences across five Texas cities that are providing services to residents taking MOUD. Unlike Level IV homes, residences in Project HOMES do not have clinical staff and are managed by live-in peer staff, called house managers. In the qualitative portion of the study, we employ ethnographic research techniques to better understand the experience of living in a city-specific recovery home, including through in-depth interviews and participant observations. In this analysis, we present findings from in-depth interviews with residents and recovery housing stakeholders.
Sampling and Recruitment
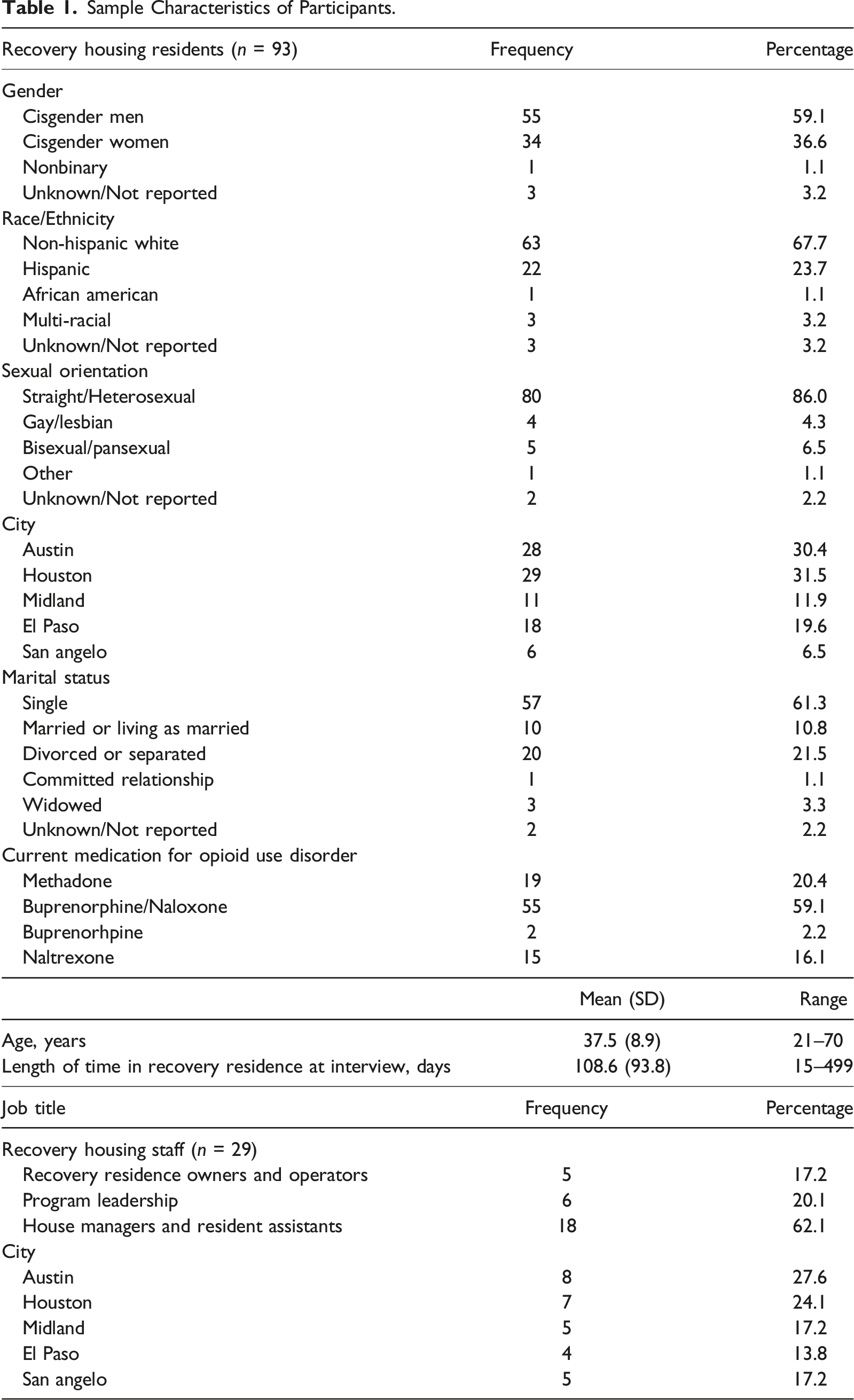
Based on the maximum variation framework for sampling in qualitative research and considering the multi-sited, longitudinal nature of the project, we aimed to recruit a large sample of interviewees (Daniel 2019; Malterud et al. 2016; Malterud et al. 2021). From July 2021 to April 2023, we conducted in-depth interviews with recovery housing residents (n = 93) and stakeholders (n = 29) across 14 residences affiliated with Project HOMES. One recovery home became affiliated with the project in 2024 and was not included in the present analysis. Residents were eligible to participate in the qualitative portion of study if they were age 18 or older, currently or previously lived in a project-affiliated recovery home and could complete the in-depth interview in either English or Spanish. Stakeholders were eligible to participate in an interview if they currently worked with an organization affiliated with Project HOMES, including live-in staff at the recovery home (i.e., house managers and resident assistants) and leadership within the recovery residences’ parent organizations. Each year, research staff made several site visits to each recovery residence. Prior to these visits, residents and stakeholders were given information about the qualitative portion of the study and invited to schedule an interview. Prior to the interview, research staff thoroughly explained the interview, including the topics covered by the interview guide and the measures taken to protect participants’ anonymity. Participation in the interview was entirely voluntary, and deciding not to participate had no impact on the participants’ ability to participate in other aspects of Project HOMES. All participants provided verbal consent prior to the start of the interview. Residents were compensated with a $25 gift card following the interview. Project stakeholders did not receive financial compensation for participation.
Data Collection
Interviews were conducted with the help of separate semi-structured interview guides for resident and stakeholder interviews. Resident interviews focused primarily on their experiences living in recovery housing, their recovery journeys, and their use of MOUD. Stakeholders answered questions regarding the logistics of recovery housing serving clients taking MOUD. As data were collected, we periodically updated the interview guides to further explore emerging concepts or develop new lines of inquiry (Glaser & Strauss, 1999; Seidman, 2013). Over the course of data collection, the salience of mental health as an integral part of the residents’ recovery journeys became quite apparent, and in September 2022, we added focused questions regarding mental health to the interview guides to further explore the topic.
In most cases, we conducted interviews in-person, though virtual interviews were available to accommodate pandemic-related safety precautions or to provide flexibility for participants’ schedules. All interviews were conducted in English, except in one case where a Spanish-speaking resident participated in an interview with the help of a bilingual member of Project HOMES staff. We recorded and transcribed interviews verbatim before uploading them into ATLAS. ti (Version 23) for analysis.
Analysis
Coding
Guided by the parent study’s research questions and literature regarding substance use and recovery, two study team members developed a provisional deductive codebook to apply to the data (Saldaña, 2021). The qualitative team then identified three transcripts against which to test these codes. Each team member individually applied the codebook, adding inductive codes as necessitated by the data, to the first transcript before meeting as a team to compare code applications. Inconsistencies across team members resulted in deliberation until consensus was reached, modifying the codebook to reflect these changes (Roberts et al., 2019; Sandelowski & Barroso, 2007). Following deliberations on the first transcript, the team then applied the modified codebook and agreed-upon coding conventions to the second test transcript, and the process was repeated until agreement was reached on the coding process across all three selected transcripts. With rigorous coding processes in place, each transcript was then coded by a single member of the qualitative research team. During weekly peer debriefings, team members presented their coding, reviewing segments of data together to ensure consistency in the coding process (Nowell et al., 2017).
Thematic analysis
To investigate the relationship between MOUD and mental health, the first author used co-occurrence tools within ATLAS. ti to identify transcripts where codes related to mental health (e.g., “mental health”, “access to services”) occurred within the same segment of text as or in close proximity to codes related to MOUD (e.g., “medication policies”). These data extracts were used to construct preliminary themes in the data through thematic analysis. The first author then compared these preliminary themes to the entire data set. Each transcript was read closely, resulting in an analytic memo that explored how each interview supported or contradicted the preliminary set of themes. This iterative process led to multiple thematic revisions, striking, collapsing, or broadening themes to ensure they were consistent with and well-represented within the data (Braun & Clarke, 2006). To enhance the rigor of the analysis and credibility of the findings, these revised themes were then presented to the rest of the qualitative team and project investigators to ensure the themes accurately reflected experiences conveyed in the interviews and staff experiences working within the recovery residences (Morse, 2015).
Member checking
In April of 2024, the first author used a member checking process to garner input from four of the five groups of recovery residence managers and program directors participating in Project HOMES on the two final themes (Birt et al., 2016). In each instance, groups of recovery residence staff and organizational leadership were presented with the theme, a short analytical summary, and several supporting quotes (Carlson, 2010). The first author then asked probing questions to validate and extend the analytical interpretation of the data, keeping field notes in the process. These sessions added additional depth to the analysis and further validated that our analytic interpretation was consistent with the lived experiences within the recovery homes.
Results
Sample Characteristics
Sample Characteristics of Participants.
Thematic Analysis
Residents and staff discussed the unique mental health implications of recovery housing serving clients taking MOUD. Participants in Project HOMES reported both individual-level impacts and organizational-level impacts. For residents in the recovery homes, taking MOUD as part of their recovery journey came with the potential for medication interactions and side effects that impacted their mental health. At the organizational level, the development of policies designed to facilitate the safe use of MOUD in the homes also allowed recovery housing staff to better serve clients who were taking mental health medications.
Medication Interactions and Mental Health Side Effects
Residents and staff spoke to several unique considerations of MOUD-friendly recovery housing, including the need to be vigilant about medication interactions and the ways in which MOUD could create or exacerbate mental health symptoms. Many of the residents in the homes disclosed taking both MOUD and medications for their mental health. Because residents often received their mental health and substance use treatment services from different medical care teams, they reported having to be vigilant to communicate about all their current medications with each provider they see. During the member checking process, one group of house managers explained how poorly integrated systems of care, particularly for those taking methadone, sometimes led to miscommunication between providers. This is illustrated when one resident described an interaction at the methadone clinic after being prescribed quetiapine, an atypical antipsychotic, by a psychiatrist: One of the doctors told me, he was like, “You’re not supposed to take those [methadone and quetiapine] together. That can kill you.” And I was like, “What?” I write down every medication I’m on every time I go to the doctor. But things like that can get overseen, I guess. (Female, 36 years old, living in home approx. one month).
Luckily for this resident, the contraindicated medications were identified by a healthcare professional soon after they were prescribed, giving providers the opportunity to better monitor for signs of adverse events. But this was not the case for all residents. One resident recalled a harrowing experience that they and their house manager attributed to the combined sedative effects of methadone and an antipsychotic: When the doctor changed my [antipsychotic] meds, I had a blackout…I don’t even remember what happened. All I know is, [the house manager] was waking me up at 1:30 in the afternoon on my bed. And I think that was from that [antipsychotic] mixed with my methadone…So, my doctor told me just to take it [the antipsychotic] at night, not to take it during the day. (Gender Unreported, 41 years old, living in home approx. two months).
In addition to medication interactions, periods where a resident switched or tapered their MOUD could also make residents vulnerable to mental health challenges. One participant described her experience adjusting to a lower dosage when attempting to taper off methadone, saying: I was so close [to being off methadone], and I ended up having an episode. Like a manic episode or something like that. And I went to the mental hospital…and then my doctor agreed with me that I needed to come back up on it [methadone] and stabilize and everything. (Female, 36 years old, living in home approx. six months).
Similarly, a staff member recounted an experience when a resident had switched from Suboxone, a partial opioid agonist, to methadone, a full opioid agonist: She [the resident] had a terrible, terrible time adjusting to it [methadone]...As a matter of fact, she ended up going to the mental health hospital for three days to stabilize…The point is that she had a terrible encounter with it [methadone] to the point that she had a mental breakdown (Recovery Residence Program Coordinator).
In many cases, staff felt the fractured, siloed U.S. healthcare system was to blame for much of the residents’ challenges with medications. Most of the time, resident’s clinical encounters with their providers were brief, leaving little time for residents to communicate new health information or ask relevant questions. In addition, staff felt that many prescribers were not well-versed in caring for patients on MOUD, recovery residence staff felt that their residents were left to manage contraindications and negative side effects without much clinical support. As a result, house staff and other residents often ended up being the first to recognize and respond to these challenges. These instances led the recovery housing staff and residents to put safeguards in place when modifications were being made to residents’ medication.
In some homes, residents experiencing mental health symptoms associated with medication interactions, medication changes, or tapering were exempt from certain chores. In other cases, house managers scheduled additional check-ins to support the resident. In at least two project-affiliated residences, house staff procured release of information forms so that they could talk directly to a resident’s clinicians about medication concerns. Some residents developed their own informal processes. For example, one participant explained that she made sure that the staff and her fellow housemates were “made aware” of any plans to change her medications so that they could intervene quickly if the resident “started acting funny or anything like that” (Female, 38 years, living in home approx. One year).
While these mental health-related challenges could be difficult, for most residents, the mental health side effects of MOUD dissipated over time. As they stabilized on their medications, some residents reported that their MOUD use actually began to help alleviate the mental health symptoms they had experienced throughout their life. A former resident reported that, “after a couple of days, you actually get used to it.” She went on to say that her medication eventually started to give her “energy, instead of feeling down and, you know, depressed and all that” (Female, 41 years, move-in date not reported). Another resident echoed that experience saying, “It’s been a process of adjusting to the right dose. But immediately, I had some relief. I could feel my mood in my head was changing. The craving wasn’t there. The debilitating depression wasn’t there” (Female, 53 years, living in home approx. Three months).
The process of finding and adjusting to the right medications takes time for many people, and managing both substance use and mental health needs can make that process even more challenging. However, the environment provided by these Level II and III recovery homes provided residents with additional support outside of the clinical setting. Their recovery home environment, including social support and monitoring by staff and peers, helped residents manage mental health challenges posed by medication use without destabilizing their sobriety.
Policies Developed for MOUD Help Facilitate Psychiatric Medication Use in the Homes
Each site participating in Project HOMES has robust medication policies in place to support the safe use of MOUD in the recovery home. These policies included mechanisms like medication counts, medication logs, and rules about how medication was stored or accessed. As an unintended consequence, these policies also allowed them to support residents taking medication to manage their mental health. This was in contrast to many recovery residences where there was a general ban on medication use. As one staff member puts it: [O]ur policy is you will take your medicine, I will take my medicine, and we will all have a better day. [Laughter]...I know that there are houses [recovery residences] that don't allow any medication, including mental health medication, and just take everyone off their meds when they go in there. And I can't imagine how you maintain a functioning household when you have a bunch of people with unmanaged mental health (Recovery Residence Program Director).
One staff member noted that their organizations handle mental health medications “pretty much the same way” as they do the MOUD. They go on to say: “We have a medication closet where we now keep all kinds of medications. We go by the log. You know, every resident has to log his name, and the medications taken, and the doses” (Recovery Residence Program Coordinator). Staff felt that residents adhering to their psychiatric medication was an important part of the residents’ recovery and the overall health of the home. They appreciated that the medication policies allowed them to support residents in remembering to take their medication and to take it appropriately. As one staff member explained, “if someone’s bipolar or has a schizophrenia diagnosis, we need to make sure that they are taking their meds” (Recovery Community Organization Leadership). They then detail how the medication policies, especially the medication storage and documentation policies, help staff monitor that: “We know where the medication’s at. We know the times they’re supposed to be taking it.” Another staff member demonstrated how these policies helped support an individual who was struggling to take their mental health medication. She recalls telling the resident “I will hold onto your mental health meds. You will get those at the same time that we dispense [MOUD]. That way, I can try to monitor it to try to help you” (House Manager). Residents echoed these ideas and appreciated that they had structures in place to remind them to take their medications. One resident stated, “I take psych meds, and...I’ve always been on medication, I’ve just never taken it. So, I think the fact that we have med times, it’s a really good reminder every day to take it, you know” (Female, 47 years, living in home approx. Two months).
These policies were especially important in that they allowed recovery residences to serve clients who might need medications that have abuse potential, like benzodiazepines or stimulants. During member checking, recovery residence staff acknowledged that some residents may need to take a controlled substance to better address their mental health. While they preferred residents to look for alternatives to these types of medications, they felt better knowing they had clear policies to help them mitigate diversion and abuse. One home decided to use the medication safes that were intended to store MOUD to also store other controlled substances. As a result, one resident noted that she was now able to take Adderall: “I don’t have a problem with Adderall. I would take that, and it helped my depression. It helped me with a lot of things. I’ve never misused it.” Now that she can “keep it locked up” in a lockbox, she feels confident that other residents and the house staff can trust her to take her medication appropriately and without damaging her recovery (Female, 55 years old, living in residence approx. Three months). The medication policies also allow house staff to intervene if they suspect that someone is using their mental health medication inappropriately. As one staff member notes, “Our policies and procedures, we only count their MAT [another word for MOUD]. But we can count their mental health medications, things like that, if it becomes a problem (Recovery Residence Program Director).” When presenting these findings to recovery residence staff, one recovery residence operator explained that this phenomenon called for a “more holistic understanding of what we mean by ‘medication assisted recovery’” (Recovery Residence Operator) in that they had begun to think about the ways that all types of medication, not just MOUD, could facilitate residents’ health and personal growth. Creating policies and procedures to safely integrate MOUD into the recovery residence setting had inadvertently increased the homes’ capacity to better serve residents who needed mental health medications.
Discussion
Our findings suggest that the integration of MOUD into recovery housing has implications for both the residents, house staff, and the recovery housing organization. Some residents experienced adverse side effects or medication interactions that impacted their mood, or in extreme cases, their physical and psychological safety. Our findings add to previous research indicating that fragmented and siloed systems of care increase the risk that residents’ medication use, side-effects, and adverse events are missed by their healthcare teams (Calcaterra et al., 2024). Recent policy changes in the United States, like the loosening of federal requirements for prescribing buprenorphine, have attempted to increase the integration of substance use treatment in behavioral health and primary care settings (Stein et al., 2023). However, policy change designed to increase access to methadone, particularly outside opioid treatment programs, has been slow-moving (Singer, 2023). Given the prevalence of co-occurring mental health and opioid use challenges, integrated care by knowledgeable providers is imperative to ensure that all an individual’s health needs are adequately and safely addressed. In the absence of these changes, substance use recovery housing appears well-suited to help residents navigate these often-complex systems of care.
The staff and peers in the homes support residents who are managing side effects and adverse events. Residents in Project HOMES have been medically underserved in their years of active substance use and may not be aware of the need to ensure their clinicians are aware of all their medications. Unlike clinical addiction treatment facilities, recovery housing organizations often do not have clinicians on site. As a result, residents most often see healthcare professionals outside of the home. Recovery housing organizations may consider providing additional coaching for residents on how to communicate across their clinical care teams about their health history, medication use, and any side effects they may be experiencing. Within Project HOMES, recovery residence staff and operators have developed internal strategies to support residents actively experiencing some of these challenges. For example, one home developed a formal policy that a resident could request leniency with required chores while adjusting to medication changes. At other times, staff could provide additional peer support. However, the strategies used by project-affiliated organizations were often developed through trial and error. As more homes transition to serving clients taking MOUD, recovery housing organizations should plan for some residents to experience medication-related interactions and side-effects and ensure appropriate supports are in place when such events occur.
The results presented here also highlight the positive unintended effects of adapting recovery housing policies for the integration of MOUD. The development and implementation of medication policies designed to support safe MOUD use helped both residents and staff feel more comfortable with the use of psychiatric medication in the home. Like MOUD, many psychiatric medications have, at times, been stigmatized in mutual-help settings (Vogel et al., 1998). Some individuals may benefit from using medication to manage underlying mental health concerns, including medications with abuse potential. Previous research from MOUD-friendly recovery housing suggests that these environments can serve as a buffer against MOUD-related stigma and support residents in their medication-assisted recovery (Gallardo, Wilkerson, et al., 2024). The themes presented here extend these findings to psychiatric medication and show how supervised medication times, medication storage, and medication-specific support can help residents incorporate mental health medications into their overall recovery journey. However, the integration of MOUD and other medications into recovery housing is new, and many recovery housing organizations may not know how to effectively serve individuals taking medication.
As more recovery residences consider how to serve clients taking medication, states may consider using a portion of opioid settlement funds to provide technical assistance to recovery housing organizations hoping to become medication-inclusive and to the development of best practice resources to ease this transition. The National Alliance for Recovery Residences (NARR) has released a set of standards against which recovery residences may be certified. Through this process, recovery residences are required to have policies and procedures that address residents’ medication use. Given the prevalence of medication use among people with mental health needs within recovery residences, states interested in increasing the availability of recovery housing competent in serving individuals with co-occurring psychiatric disorders could also incentivize voluntary certification against the NARR standards. Not only does the certification process require operators to develop and show evidence of medication policies, but the state NARR affiliates, which oversee the certification process, are well-positioned to provide ongoing technical assistance and support in the implementation of said policies.
Limitations
The large sample size and triangulation of data across both recovery housing residents and staff speaks to both the depth and breadth of this qualitative analysis. However, the findings should be interpreted with attention to several limitations. Project HOMES is specific to Texas. Given that cultural and political factors can shape an individual’s access to health care and recovery services, it is possible that our findings may not transfer to other geographic settings (Lincoln & Guba, 1985). In addition, this project only includes staffed recovery residences classified as Level II or Level III according to the NARR standards. Several of the key findings in this analysis point to the role of house staff and organizational policies in supporting residents. As such, these results may not generalize well to Level I homes, which are democratically run by residents and not staffed and, or Level IV homes, which offer clinical services. Additional research is needed to understand how medication can be integrated across the spectrum of recovery housing structures. Finally, the participants in the qualitative portion of the data set are predominantly White, straight, and cisgender. Minoritized communities are underrepresented in this data and in the recovery residence literature more broadly. Additional research is needed to better understand the experience of these communities in recovery housing.
Conclusion
Our findings suggest that managing co-occurring mental health and substance use within the recovery housing environment is a complex challenge. As more residents taking MOUD enter recovery housing, the number of medication interactions and medication side effects with mental health implications may increase. However, the transition to MOUD-inclusive recovery housing also allows recovery housing organizations to develop policies and procedures that have the additional benefit of better addressing residents’ need for medications that help manage their mental health. Attention to co-occurring mental health needs and concomitant psychotropic medication use will be vital for the long-term success of MOUD-inclusive recovery housing.
Footnotes
Acknowledgements
The authors thank all Project HOMES community partners and participants for supporting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project HOMES is supported by Texas Targeted Opioid Response, a public health initiative operated by the Texas Health and Human Services Commission through federal funding from the Substance Abuse and Mental Health Services Administration grant award 1H79TI083288.
Disclaimer
Therefore, the views expressed do not necessarily reflect the official policies of the Department of Health and Human Services or Texas Health and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. or Texas Government. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and decision to submit the manuscript for publication.