
Abstract
The aim of the study was to provide evidence on the oral health of Northern Finnish people with experience of illicit drug use, referenced against the age-matched general population, Northern Finland Birth Cohort 1986 (NFBC1986). In total, 118/1551 subjects, average age 33/34 years, and 66%/40% males participated in the studies for the people with experience of drug use and NFBC1986, respectively. Most of the people who use drugs were single, unemployed, or retired, and had a low level of education, whereas the opposite was true for NFBC1986. A majority of the people with experience of drug use were active smokers whereas 17% in NFBC1986 reported smoking. The people who use drugs had fewer teeth, more caries lesions, more severe consequences of caries and plaque, and more frequently reduced salivary flow, than the general population. The people who use drugs had poorer oral health compared to the age-matched general population.
Keywords
Introduction
Illicit drug refers to a psychoactive substance that is illegal to produce, sell, or use. These drugs are often prohibited under international drug control treaties and include substances like heroin, cocaine, methamphetamine, ecstasy, and cannabis (World Health Organization, 1994; United Nations Office on Drugs and Crime, 2016). A rise in the use of illicit drugs has been seen in Finland as well as elsewhere in the world (Karjalainen et al., 2023; United Nations Office on Drugs and Crime, 2023). According to the Finnish National Institute for Health and Welfare, this trend has been continuing for the past 30 years (Karjalainen et al., 2023). Approximately one in four Finnish adults has tried illicit drugs at some point in their lives, men more frequently than women (37% vs. 21%) (Karjalainen et al., 2023). Drug experiments and use are most common among 25–34-year-olds, but during the period of 2018–2022, experimentation and use also increased in older age groups (35–44 and 45–69 years), exclusively in men (Karjalainen et al., 2023; Rönkä et al., 2020). It has been contended that COVID-19 might have led to a decline in the use of illicit substances. Conversely, others argue that lockdowns actually facilitated greater access to drugs (Adejoh et al., 2024; Bade et al., 2021; Otiashvili et al., 2022).
According to the latest register data, the percentage of problematic user of amphetamines and opioids in Finland is estimated to be 0.9 – 1.3% of the total population aged 15 – 64 years, which translates to 31,100 – 44,300 individuals (Rönkä et al., 2020). In northern Finland, the proportions of amphetamine and opioid users are estimated to be 0.3 – 0.7 and 0.3 – 0.5, respectively (Rönkä et al., 2020). In Oulu region, this would mean about 1000 problematic illicit drug users.
In addition to social and general health hazards, drug use also affects oral health. These effects can occur either directly as adverse effects or indirectly in the form of indifference towards oral hygiene or failure to attend dental appointments (Cossa et al., 2020; Riemer & Holmes, 2014; Teoh et al., 2019). For example, cannabis, amphetamines, and opioids cause dry mouth, which predispose one’s teeth to dental caries, which in turn causes pain and impacts well-being (Baghaie et al., 2017; Scully, 2003). Further, due to tooth ache and pain, illicit drugs can be used as ‘self-medication’ to alleviate symptoms and avoid visits to dentist. In a systemic review and meta-analysis of Baghaie et al. (2017), altogether 28 studies with more than 4000 participants and 28,000 controls were included. Participants with experience of substance use had more decayed teeth, more severe caries and more periodontal disease, but had received less dental care than the general population (Baghaie et al., 2017). Also, erosive tooth wear (ETW) (Cossa et al., 2020; Vainionpää et al., 2019), periodontal diseases (gingivitis and periodontitis) (Quaranta et al., 2022; Yazdanian et al., 2020), temporomandibular disorders (TMD) (Aldosari et al., 2023), and edentulousness have been reported (Sun et al., 2018).
Some studies have been conducted recently among people who use drugs and homeless people in other Nordic countries: a Norwegian survey on the experiences of people who inject heroin in oral health care (Vanberg et al., 2016) and a Danish clinical study on socially vulnerable people (Hede et al., 2019). In addition to the studies mentioned above, a comparative cross-sectional study at the Karolinska Institute in Sweden was conducted on the oral health of people using illicit drugs (n = 95) and in linear regression analyses controlled for age and gender substance type was found to be a statistically significant predictor of number of teeth (p = .03) and DMFT (p = .001) (Rafat et al., 2020). In all these studies, oral health was found to be threatened among this marginal group.
The illegality of drugs and the stigmatization associated with them make research among people who use illicit drugs challenging. They are also a demanding and complex group of patients. As literature on the oral health of Finnish people who use illicit drugs is limited, this study aims to provide information on the topic, using as a reference point the general population of the same age in the Northern Finland Birth Cohort participants born in 1986. In addition, this research aims to produce information which can be used for planning the oral health care of people who use illicit drugs.
Materials and Methods
Subjects
The participants in this cross-sectional field study were customers of substance abuse services in the Oulu region, located in Northern Ostrobothnia, Finland. The study population comprised people 18 years or older with experience of active or former illicit drug use. Also, individuals on pharmaceutical substitution and maintenance therapy, or medically assisted drug rehabilitation were included. To determine the size of the study population, a power calculation was performed with a confidence level of α = 0.05 and at a ratio of 0.1 (10 %). Based on this calculation, the required size of the study population was determined to be 139 participants.
The reference group was comprised of participants of the Northern Finland Birth Cohort 1986 (NFBC1986), whose health and behaviour have been monitored since they were born, most recently in 2019–2020.
The study samples and protocols are described in Figure 1. Examination protocols among a group of people with experience of illicit drug use and the reference group of same age, Northern Finland Birth Cohort 1986 participants (NFBC1986). *https://www.oulu.fi/en/university/faculties-and-units/faculty-medicine/northern-finland-birth-cohorts-and-arctic-biobank/northern-finland-birth-cohorts.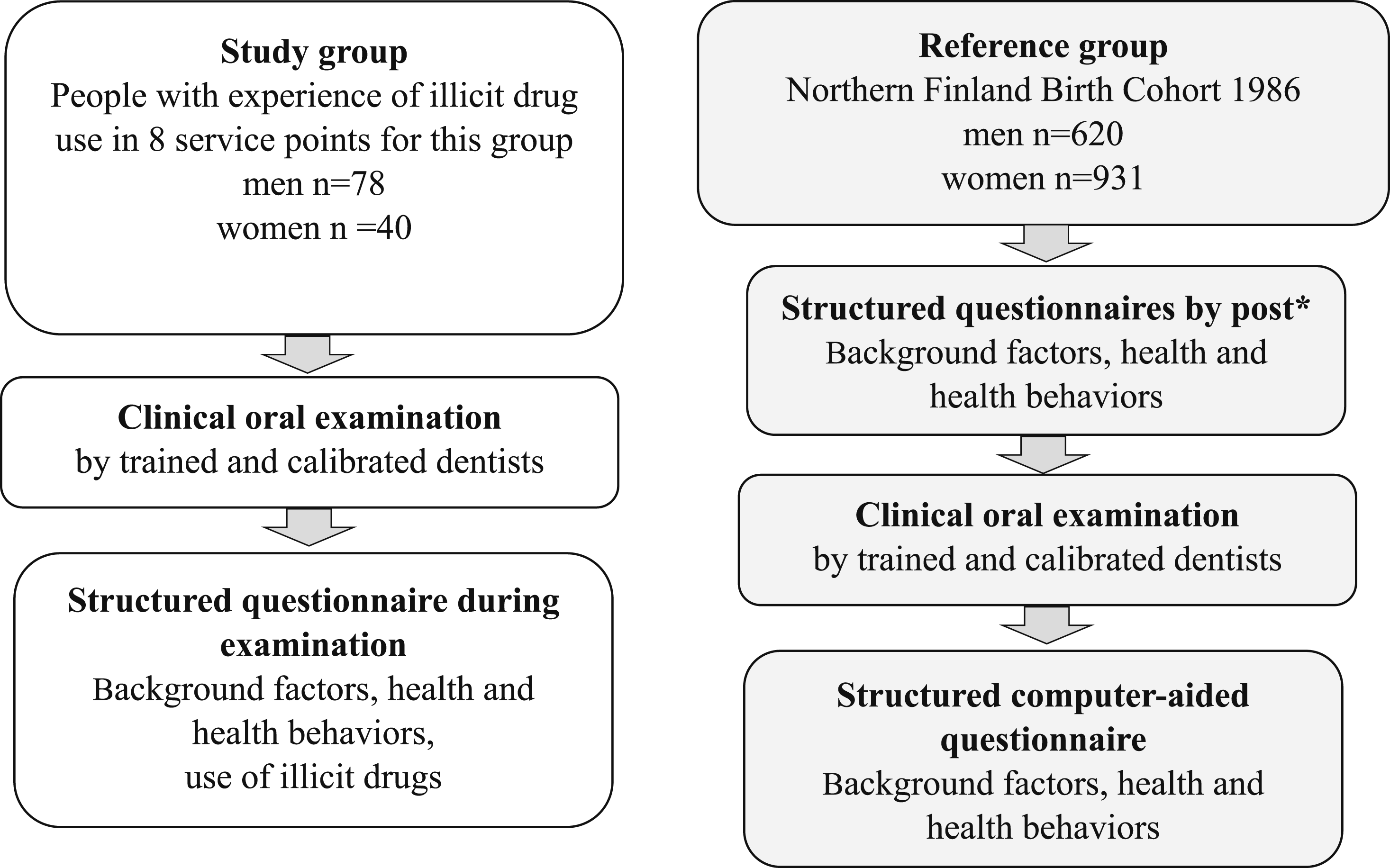
Study Protocol Among People Who Use Illicit Drugs
In total, eight different substance abuse service units were recruited to join the study. Six of them were administered by the Oulu City health and social services: one outpatient clinic (health education/needle exchange clinic), three substitution and maintenance therapy clinics (Oulu northern and southern clinics), one inpatient clinic (substance abuse rehabilitation clinic) and one ‘day activity center’ for the homeless. Two units out of eight were third-sector organizations: one women’s shelter and one guided functional peer support center.
After getting permissions, research group members (VA, AT, RV) contacted all the substance abuse service units or their chief organizations. The research schedule was planned with the staff of the organizations. The staff informed their customers or patients about the study and its protocol. They also recruited the participants and arranged for the facilities to conduct the study. The participants were voluntarily enlisted. Written and oral information about the study was given to the participants beforehand. All the participants gave their written consent and had the option decline participation in the study at any time.
The study protocol consisted of a survey and a clinical oral examination, which took an average of 75 minutes per participant. Three examiners (OK, AT, RV) visited the units and carried out the clinical examinations. During the same visit, information of the background factors, self-reported health, health-related behaviors and use of illicit drugs was collected using a structured questionnaire. To ensure that questions were properly understood, the questionnaire was filled with the help of the examiner. The examiner read the questions and completed the questionnaire according to the answers of the participant. The data was collected between October 2020 and May 2022. The COVID-19 pandemic prolonged the field phase.
Study Protocol in the Northern Finland Birth Cohort 1986 (NFBC1986)
NFBC1986 is a longitudinal study on the health and well-being of the population. The cohort included all the children (n = 9432 live births) whose expected date of birth was between July 1st 1985 - June 30th 1986 in the two northernmost provinces of Finland (Oulu and Lapland). The data have been collected four times after the baseline, the latest about 33 years after the first time (2019–2020) with clinical examinations and a questionnaire. (Northern Finland Birth Cohorts)
In 2019, participants were invited to take part in a clinical oral examination as part of their 33-year follow-up study. Of those invited, 1553 attended the clinical oral examination and provided answers to the questionnaires.
Examiner training, calibration process and validation
The researchers examining the people who use drugs (OK, AT, RV) were trained and calibrated by an experienced specialist (VA at baseline, RV later) before clinical examinations. The calibration on the caries diagnostic criteria was carried out by a Power Point presentation with 20 images of extracted teeth with carious lesions of various depth and activity (ICDAS) (Ismail et al., 2007). A consensus was achieved by the team members for each carious lesion. The ICDAS criteria were available to the researchers in a printed version throughout the study. The training also included principles for periodontal examination, evaluation of erosive tooth wear (ETW) using the Basic Erosive Wear Examination index BEWE (Bartlett et al., 2008), evaluating the PUFA index (Monse et al., 2011) as well as guidelines on how to perform a quick test of salivary flow from the lower lip, as it has been reported to be valid (Ogami et al., 2004) instead of oral Schirmer’s test (Stevens, 2011), using a time window of 60 seconds. After the training and calibration session, the researchers evaluated 15 carious lesions from the Power Point images and inter- and intra-examiner agreement (Cohen’s and Fleiss Kappa) values were calculated (intraexaminer kappa was 0.73 and interexaminer kappa was 0.51).
Two or three researchers were always present at the examinations. The senior researcher (RV), who was familiar with field studies (NFBC1986; Vainionpää et al., 2017) and the calibration process, acted as a golden standard and was present at every examination location except one. In unclear cases, to reach a consensus, the clinical findings were discussed between the team members and the golden standard before recording. Because the study lasted for a long period, training and calibration were repeated on two occasions during the field phase to ensure the quality of the clinical examinations.
Three examiners (OK, AT, RV) took turns carrying out clinical oral examinations among the people who use drugs, while one recorded the findings on a structured sheet used in a previous study (Methuen et al., 2021). Dental units were not available in the study locations. The participants either sat on a chair or laid down on a hospital bed or something similar during the oral examination. Dental loupes, an oral mirror, a World Health Organization periodontal probe, and tweezers were used as instruments. In addition, dental cotton rolls and gauze were available.
In the NFBC1986 study, the clinical examinations were performed by seven dentists using a standardized clinical examination protocol. All the examiners were trained to use the ICDAS criteria. They were also calibrated before the field phase, and the calibration was repeated every three months.
The clinical examinations of the NFBC1986 cohort study were carried out in a modern dental university clinic. The light of the dental unit, a three-in-one syringe, as well as a World Health Organization periodontal probe and an oral mirror were used as instruments, along with dental loupes and tweezers. Dental radiographs were not taken from either of the two groups of participants.
Dental Status
Caries findings, both among the people who use drugs and among the cohort study participants, were recorded using the International Caries Detection and Assessment System (ICDAS) (Ismail et al., 2007). ICDAS scores ≤ 3- were regarded as initial caries and ICDAS scores ≥3+ as decayed carious lesions needing restorative treatment. For the people with experience of drug use, PUFA values were calculated as follows: teeth with clinical signs of any severe consequence of dental caries got a value of 1, whereas teeth without such signs got a value of zero (range 0–28). The consequences were described as consisting of pulpitis (P), ulceration (U), fistula (F) or an abscess (A) (Monse et al., 2011).
Additionally, in both groups, the highest BEWE score (0–3) from each sextant was recorded and the BEWE sum score was calculated (0–18) (Bartlett et al., 2008). The number of decayed root remnants as well as attrition were reported. Salivary flow among the people who use drugs was studied from the small salivary glands of the lower lip (yes/no; yes, if saliva droplets appeared within 60 s) (Tandon et al., 2013) and salivary pH was measured using pH paper. In the NFBC1986, the resting salivary flow was measured for 15 min; the cutoff for reduced resting salivary flow was 0.1 mL/min (Pedersen et al., 2018).
Periodontal Status
For both the people who use drugs and the NFBC1986 participants, the periodontal examination included measurements of teeth with visible dental plaque on the buccal surface. In this study, teeth with gingival bleeding (BOP) (a positive score was recorded if bleeding occurred within 10–15 s after probing) (Weinberg & Hassa, 2012), probing pocket depth with a periodontal probe (≥4 mm and ≥ 6 mm), and tooth mobility (Mob) were measured and reported only among the people who use drugs; BOP and periodontal pockets were measured from six sites of the teeth: distobuccal, buccal, mesiobuccal, disto-oral, oral, and mesio-oral.
Questionnaires
The questionnaire included 34 questions that were modified from previous surveys (Northern Finland Birth Cohorts) and the study among Finnish conscripts (Anttonen et al., 2012).
The following were recorded as background factors: age (years), gender (woman/man), marital status (single/in a relationship), work life (employed/unemployed/retired/student), and educational level (basic = compulsory 9 years education/2 nd degree education = vocational/high school/3 rd degree = university or university of applied sciences). The participants were asked if they have any long-term illness (lasting more than 2 months) that requires medication (yes/no), and open questions about what long-term illness they had and what medication they were taking.
Smoking habits (never or former smoker/active smoker on daily or almost daily basis), use of snus (never or former use/active use), and use of alcohol (no/monthly/weekly or more often) were asked. Habits concerning illicit drug use (no/tried once/tried two to four times/used five or more times/ using regularly), as well as the age (years) when drug use was started and how long the person had been using drugs, were asked (years). The question about the type of the illicit drugs used included a total of sixteen different options of illicit drugs (Appendix Table 1). Participants were also asked to name the main illicit drug(s) they used.
Similarly to the people with experience of drug use, the background questionnaire in the NFBC1986-study also included questions on marital status, work life, educational level, smoking, alcohol consumption, snus use, use of illicit drugs, and questions on medication and chronic diseases. Background and health questions were sent by post before clinical examinations. Data on oral health were collected during the dental clinical examinations using a computer-aided questionnaire (Northern Finland Birth Cohorts) (Figure 1)
Statistical Analyses
In this cross-sectional descriptive study, we present the distribution of participants by background and health, and drug use variables in terms of frequencies and proportions. Clinical variables were presented additionally as means and their standard deviations. A comparison between men and women was done using the Chi-square test or Fisher’s exact test for the study sample and reference population. For comparing means, an independent t test was used. Differences between the genders were considered significant at p-values <0.05.
The variables in both study groups were categorized as follows: marital status (single/in a relationship), work life (employed/unemployed/ retired/ student), educational level (basic/second degree/third degree), smoking and use of snus (never or former use/active smoker), use of alcohol (no/ monthly/weekly or more often). Among the people who use drugs, the main illicit drugs were grouped as follows: cannabis, amphetamine, opioids, and amphetamine & opioids. In the NFBC1986, use of drugs and psychoactive substances were categorized as follows: sedatives (without alcohol), pain medication (without alcohol), alcohol and medication, huffing/sniffing (glue, thinner), cannabis, hard drugs (ecstasy, heroin, amphetamine), and use of drugs intravenously. The BEWE sum score (the sum of the highest score in each sextant) was grouped as follows: 0–2, 3–8, ≥9. The number of decayed teeth (D) was grouped as follows: 0, 1–4, ≥5. Decayed root remnants per patient were presented as yes/no. The number of teeth with dental plaque was categorized as 0–7, 8–15, ≥16. The number of teeth with gingival bleeding (BOP) was grouped as follows: 0–7, 8–18, ≥17. The number of teeth with deepened periodontal pockets was categorized as follows: 0, 1–3, ≥4. The number of teeth with signs of pulpitis, ulcerations, fistula, or abscess (PUFA) was grouped as follows: 0, ≥1. Observations of reduced salivary secretion were recorded (yes/no) and the pH of saliva was expressed as a numeric value.
As the questions for the people who use drugs and participants in the NFBC1986 were similar, they could be categorized similarly except for the questions about drug use. In the NFBC 1986, drug use was categorized as never, used 1–4 times, or used ≥5 times / regularly.
Ethical Approval
The permissions to conduct the research were given by the regional medical research ethics committee of the Wellbeing services county of North Ostrobothnia (September 2020, EETTMK: 85/2020), The City of Oulu (June 2020, §45/2020 and February 2021, §12/2021) and ‘Friends of the Youth’ Registered Association (August 2020). Also, the regional medical research ethics committee of the Wellbeing services county of North Ostrobothnia approved the use of the Northern Finland Birth Cohort 1986 Study (NFBC1986) data on the dental license application (January 2018, EETTMK: 108/2017).
Recorded data were analyzed using SPSS software version 28.0, Inc, Chicago, IL, USA.
Results
The total number of people who use drugs participating in the study was 118, of whom 66% were men, whereas in the NFBC1986, the respective figures were 1551 and 40%. The mean age of the people who use drugs was 33 years (SD 8.0; min. 20 years, max. 65 years). In 2020, when the data collection among the NFBC1986 took place, the participants were about 34 years. One third (n = 39) of the people who use drugs were attending medically assisted drug rehabilitation; 42.5% (n = 17) of the women and 28.2% (n = 22) of the men.
Distribution of the Four Main Illicit Drugs in the Study Sample (n = 117) by Gender (Self-Reported Substance or Substance Combination When Asked ‘Which is the Main Illicit Drug You Use?’).
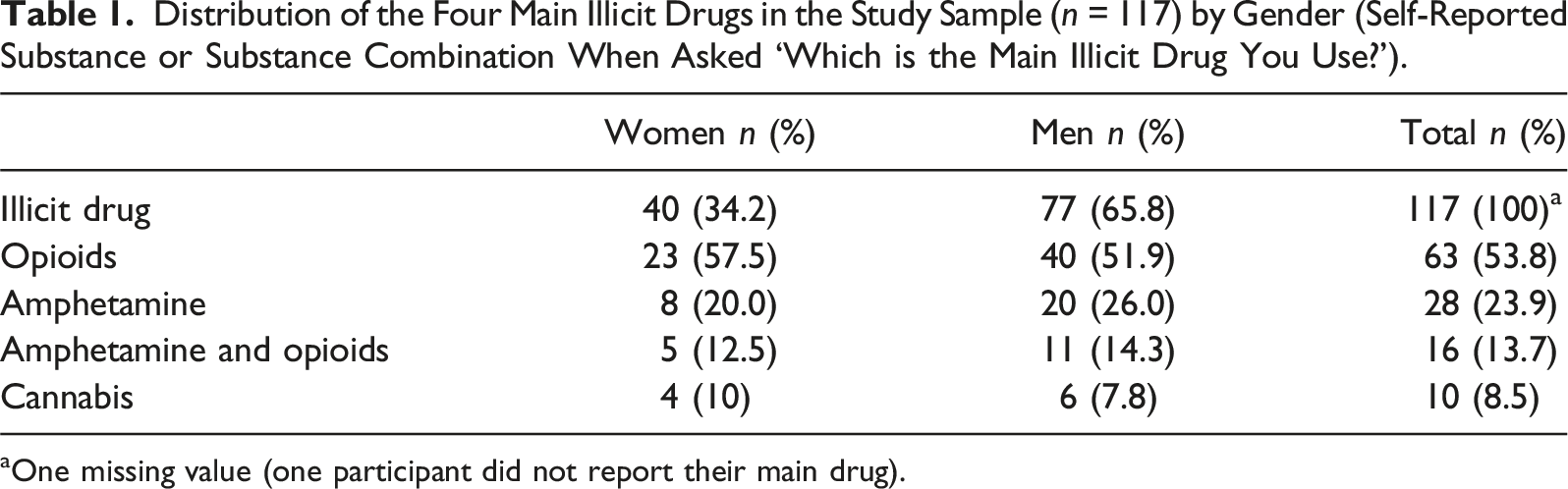
aOne missing value (one participant did not report their main drug).
Use of Illicit Drugs and Psychoactive Substances Among Northern Finland Birth Cohort 1986 (NFBC1986) Participants (n = 1551) by Gender.
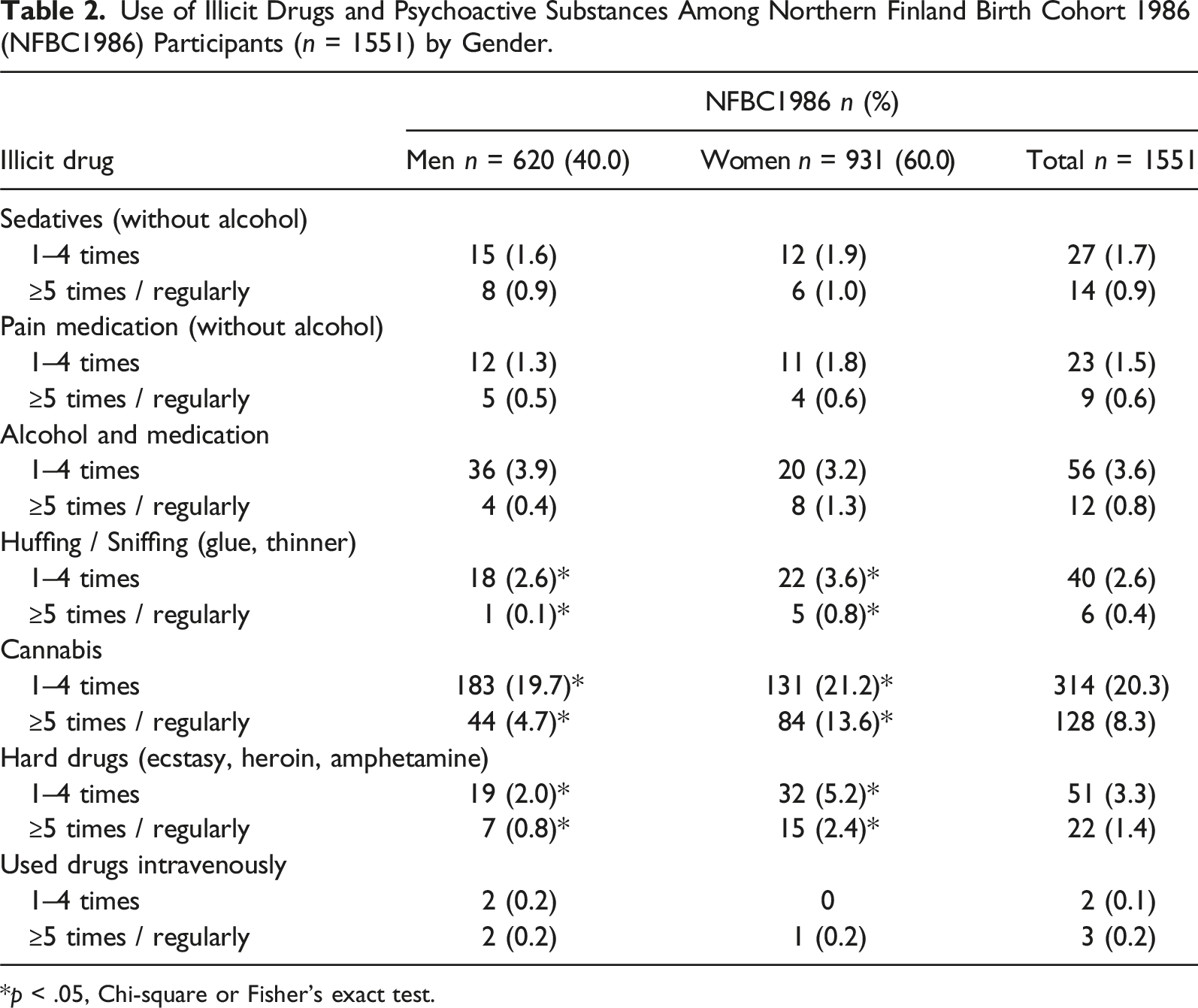
*p < .05, Chi-square or Fisher’s exact test.
Descriptive Statistics by Gender Among People With Experience of Drug use (n = 118) and Northern Finland Birth Cohort 1986 (NFBC1986). The Number of Participants in the NFBC1986 Varied From 1548 to 1553 Depending on the Variable.
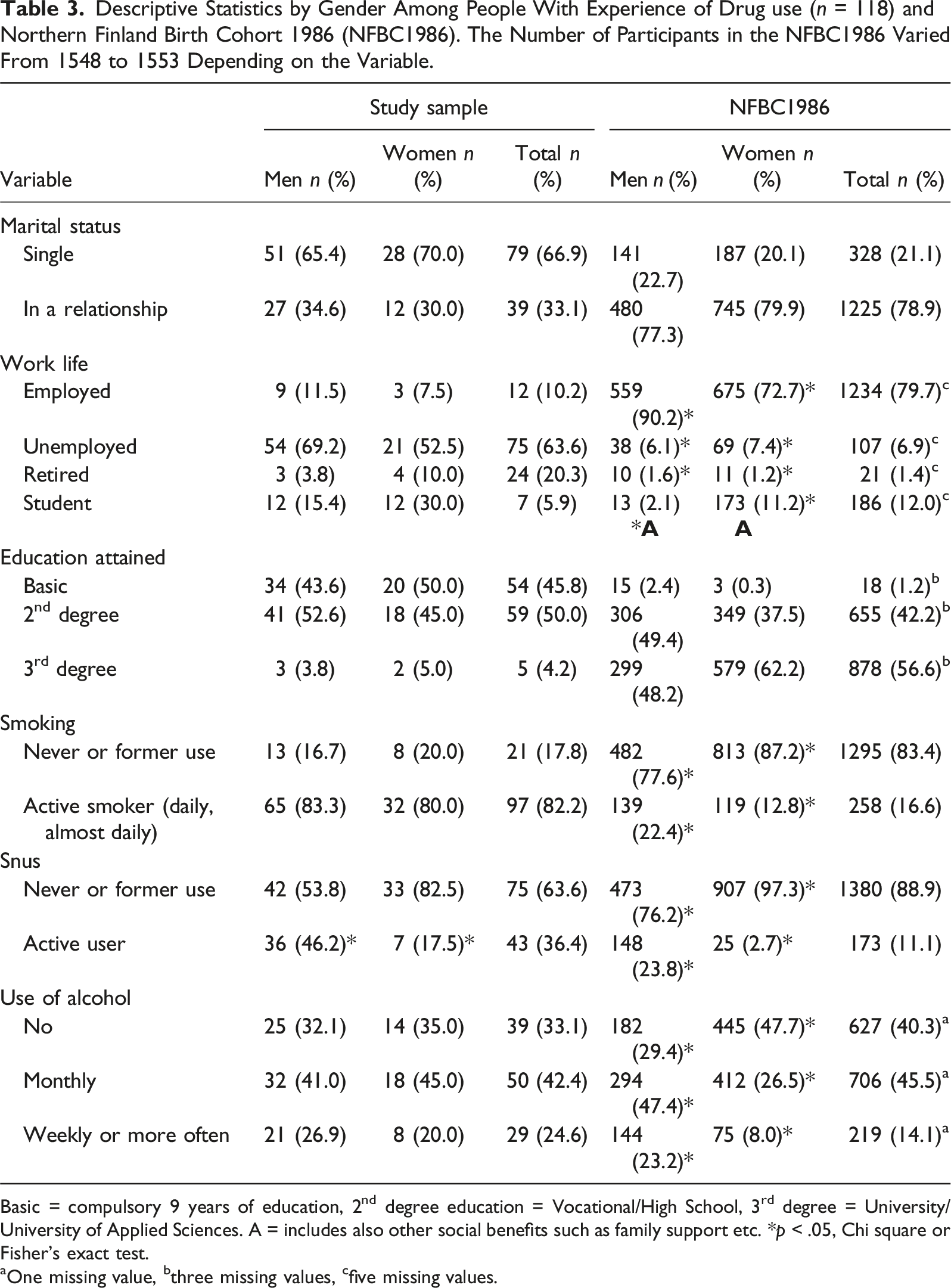
Basic = compulsory 9 years of education, 2nd degree education = Vocational/High School, 3rd degree = University/University of Applied Sciences. A = includes also other social benefits such as family support etc. *p < .05, Chi square or Fisher’s exact test.
aOne missing value, bthree missing values, cfive missing values.
Among the people who use drugs, the mean number of teeth was lower than in the age-matched reference population (NFBC1986). Almost all the people with experience of drug use (∼93%) had at least one decayed tooth (ICDAS ≥3+), whereas in the reference population approximately 60% had at least one decayed tooth. Majority of the study sample (65%) had more than four teeth in need of restorative treatment whereas the same was true only for 11% in the NFBC1986. The number of decayed teeth in the study sample was significantly higher among men (mean 8.3, SD 6.0) than among women (mean 4.9, SD 4.0) (t (-3.59) = 101, p = .001, independent t test). The same was true for the number of decayed root remnants (women: 0.3, SD 1.63; men: 1.6, SD 2.43, t (−2.04) = 102, p = .044, independent t test) and teeth with dental plaque (women: 10.5, SD 8.99; men: 14.5, SD 8.91, t (−2.23) = 105, p = .028, independent t test). In the study sample, mean numbers of teeth with dental erosion (BEWE), teeth with gingival bleeding, and teeth with deepened periodontal pockets (≥4 mm) were higher among men, but not significantly. Compared to the reference population, people who use drugs had more teeth with dental plaque (mean 13.1, SD 9.19 vs. mean 4.31, SD 5.04), but equal amount of dental erosion (BEWE) (mean 4.11, SD 4.17 vs. mean 4.14, SD 4.10). (Figure 2, Appendix Table 2). Mean values of oral health variables among people with experience of illicit drug use (n = 118) and Northern Finland Birth Cohort 1986 (NFBC1986, n = 1551) by gender.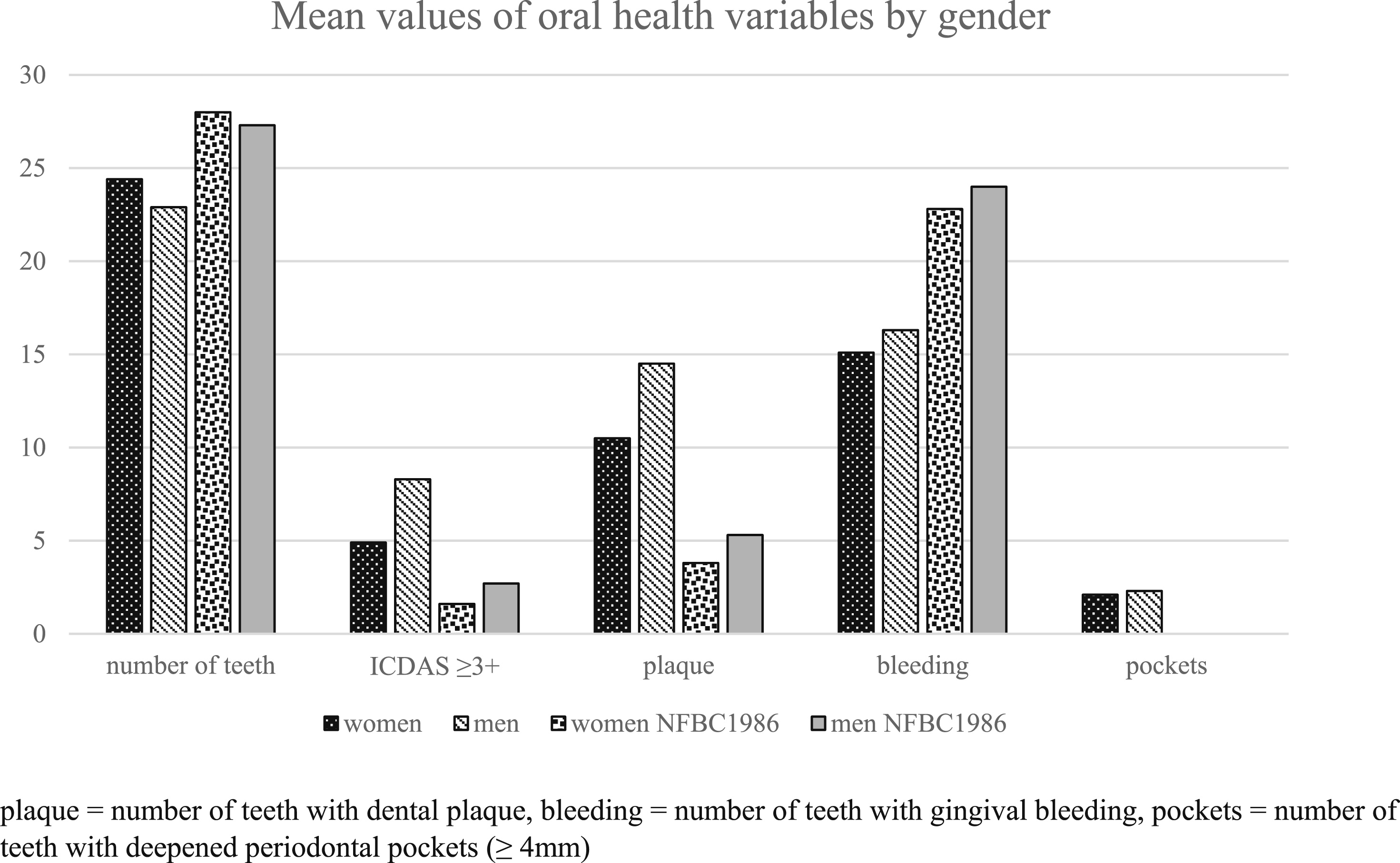
It the study sample, more than 10% had severe consequences of dental caries, or PUFA ≥1 and the highest PUFA value was 6. Among the people who use drugs, one in five of the women and one in four of the men had reduced salivary flow whereas the same was true for only 3% of the NFBC1986 participants. The mean pH value of saliva among the people who use drugs was 6.4 (SD 0.9, min 4, max 8). One fifth of the people who use drug had deepened periodontal pockets; seven percent even had deep periodontal pockets (≥6 mm), and 11% had teeth with increased mobility. Eight participants had either full or partial dentures.
Discussion
To our knowledge, the oral health among Finnish people using illicit drugs has not been previously studied with comparable study design. This cross-sectional study shows an association between a use of illicit drugs and poor oral health, which is in line with previous international studies (Mukhari-Baloyi et al., 2023; Rossow, 2020; Yazdanian et al., 2020). Here, as many as one in ten users had severe consequences of dental caries present in their dentition. In addition to poorer oral health, the people with experience of drug use exhibited a profile characterized by marginalization in many respects that is lower education, unemployment, early retirement, and often single marital status, compared to their counterparts of same age in general population.
Opioids were the most frequently used substances among the people who use drugs in the Oulu region, Finland, followed by amphetamine, a combination of amphetamine and opioids, and cannabis, which accounted for about 90% of the used illicit drugs. In the general population of the same age, less than one in ten used cannabis often or regularly and less than five percent had ever used hard drugs. Illicit drugs used in Finland differ from many Western and Central European countries, where heroin and cocaine are commonly used instead of buprenorphine and amphetamine. (EUDA, 2024)
According to the current data, the most typical Northern Finnish individual who use drugs is a single man in his 30s, with only a first or second-degree education, and is unemployed or retired. Our results are in line with previous literature on the sociodemographic characteristics of the people with experience of illicit drug use (Daniel et al., 2009; Onyeka et al., 2012). Peers of the same age in the NFBC1986 were cohabiting, educated with second or third-degree education, and working. Active smoking was common among the people who use drugs and a third of them used snus; both habits were more common than among the general population. Alcohol was used more often among the people who use drug than in the NFBC1986 group. All these unhealthy, harmful behaviours also have detrimental effects on oral health (Muthukrishnan & Warnakulasuriya, 2018; Priyanka et al., 2017; Tanner et al., 2015).
In Finland, as elsewhere, the people who use drugs often use several different drugs and their combinations, and the use of tobacco products and alcohol is often abundant (Baghaie et al., 2017; Chaparro-Gonzảlez et al., 2018). Therefore, it is challenging to study the direct effects of any specific illicit drug on oral health. However, a recent Swedish study (Rafat et al., 2020) found that people who use cannabis have fewer oral health problems than users of opioids or amphetamine and cocaine. Those who are on pharmaceutical substitution therapy might have poor oral health due to previously usage of illicit drugs but also due to ongoing opioid therapy (Nathwani & Gallagher, 2008). It may be that the indirect effects of the drug use plays an important role in oral health problems, especially among users of harder drugs, who are often marginalized and have problems in maintaining their oral health through oral hygiene and undergoing dental care. This assumption is supported by the poor dental status and high number of teeth with visible plaque in the current study. This study also showed the direct effect of illicit drug use on lowered salivary flow, which is a threat to oral health. Low salivary flow leads to lower buffering and lubricating as well as rinsing capacity (Pedersen et al., 2018).
Consistent with the current study, several previous studies have reported that the people with experience of drug use have poor oral health (Baghaie et al., 2017; Cossa et al., 2020; Mukhari- Baloyi et al., 2023; Paisi et al., 2021; Rafat et al., 2020; Teoh et al., 2019; Yazdanian et al., 2020). This is true especially for dental caries. Almost all the people who use drugs in this study had a need for restorative treatment and the number of decayed teeth was remarkably higher among the people who use drugs than in the aged-matched general population (NFBC1986). The existence of caries among the people with experience of drug use was shown to be polarized, too. The mean number of teeth was also lower in the group of people who use drugs than in the reference population (NFBC1986). In a previous study, almost none of the Finns aged 30–44 have removable dentures (Suominen et al., 2012), whereas in the current study, despite the mean age of 34 years, seven percent had either partial or full dentures.
Severe consequences of dental caries (PUFA-index) (Monse et al., 2011) have rarely been reported. However, those consequences were indeed present in this study, indicating a risk for oral systemic infections. One in seven (15%) subjects had a PUFA index ≥1. PUFA is often associated with dental pain. During responding structured questionnaires, some participants said that tooth pain had been treated with different medications and/or with illicit drugs, which act also as an analgesic agent. In a recent South African study (Mukhari-Baloyi et al., 2023), the PUFA prevalence was significantly lower, only 2.5%, indicating that toothaches of people who use drugs had probably been treated with tooth extractions. This was true here as well, as the average number of missing teeth was five, excluding wisdom teeth.
Surprisingly, there were no significant differences between the groups in the mean BEWE sum scores, or in the need for preventive erosion treatment. The reason for this can only be speculated. Most of the people who use illicit drugs in this study used opioids, and significantly less used cocaine or ecstasy. This may at least partly explain similar ETW states among both the people who use drugs and the reference group, because the use of cocaine, MDMA (‘ecstasy’) and amphetamine are known to be associated with erosive tooth wear (Nixon et al., 2002).
The city of Oulu was the most convenient and accessible location to conduct the study while it had substance abuse service units enough to reach voluntary participants. Comprehensive data was obtained in spite of the Covid 2019 pandemic, even though the number of participants ended up being somewhat lower than recommended by the power calculation. The availability of the NBFC1986 data (with its similar clinical setting and questionnaires) is a strength, even if a direct comparison of two data sets is not allowed (Ministry of Social Affairs and Health: The Act on Secondary Use of Health and Social Affairs and Health, 2019). Another strength was that the study among the people who use drugs could be conducted in places familiar and safe for them instead of dental clinics, which could have made data collection even more difficult. Instead of giving the questionnaires for the people who use drugs and asking them to respond to them, the structured questionnaires were carried out, which was a great benefit. One strength here is that for both study populations the questionnaires were similar and dental clinical examinations were done by trained and calibrated dentists, and the same modern criteria were used both among people who use drugs and NFBC1986. (Bartlett et al., 2008; Ismail et al., 2007; Monse et al., 2011).
Radiographic examinations were not possible due to the research locations, and this is one limitation of the study. Due to the limited sample size, grouping by age was not practicable and conclusions concerning oral health among different age groups could not be drawn. Also, it can be speculated that those individuals who were not able or interested to participate the study may have had even poorer oral health. Thus, the results should be interpreted with some caution. Further research on the topic is needed and especially intervention studies focusing to promote oral health of people who use drugs would be valuable.
Conclusions
The people who use drugs in northern Finland have poorer oral health in terms of dental caries and its severe consequences compared to their age-matched reference group. Additionally, users of illicit drugs have had teeth extracted, which has functional as well as social impacts. Compared to the general population of the same age, marginalization experienced by the people who use illicit drugs was shown in this study in many aspects of life. Consequently, they have neglected dental care amid the challenges and difficulties of their lives. Dental professionals play an important role in identifying this group of patients, detecting, and diagnosing oral changes caused by psychoactive substances. The staff of different substance abuse service units should also be involved and informed and educated about oral health, and how to refer patients to dental care.
Footnotes
Acknowledgements
The authors express their gratitude to all the participants and thank the personnel of the different substance abuse service units and their chief organizations. We wish to thank all cohort members, researchers and NFBC project center personnel who participated in the NFBC data collections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NFBC1986 33–35y follow-up study received financial support from University of Oulu (Strategic funding from donations) and Oulu University Hospital (K65760). The oral health study was supported in part by the Research Council of Finland former Academy of Finland, Grant no. (326189).
Appendix
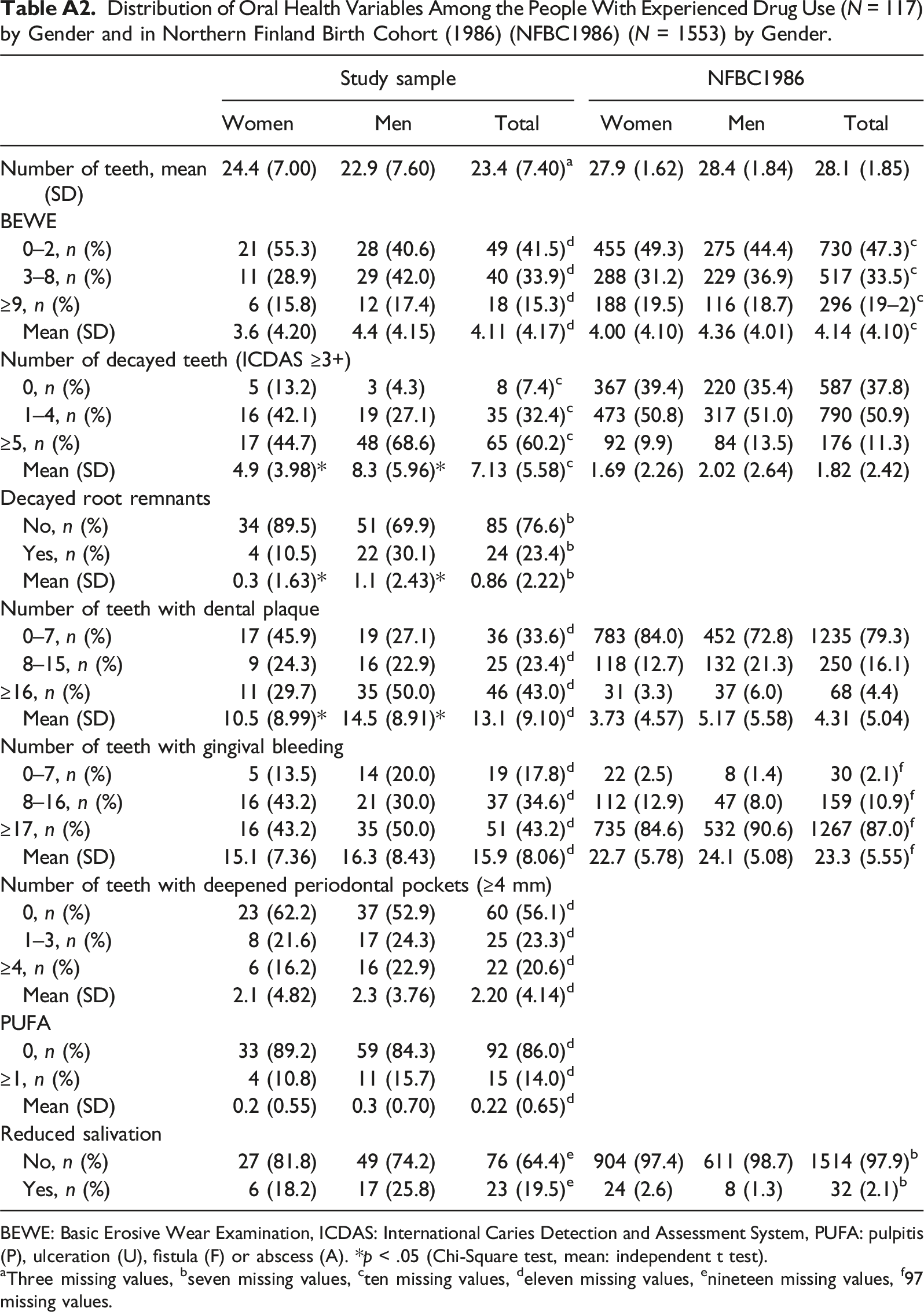
Self-reported Drugs Used among People with Experience of drug Use (Study Sample, n = 118) Distribution of Oral Health Variables Among the People With Experienced Drug Use (N = 117) by Gender and in Northern Finland Birth Cohort (1986) (NFBC1986) (N = 1553) by Gender. BEWE: Basic Erosive Wear Examination, ICDAS: International Caries Detection and Assessment System, PUFA: pulpitis (P), ulceration (U), fistula (F) or abscess (A). *p < .05 (Chi-Square test, mean: independent t test). aThree missing values, bseven missing values, cten missing values, deleven missing values, enineteen missing values, f97 missing values.
Drug
Hashish
Marijuana
Amphetamine
Methamphetamine
Heroin
Buprenorphine other than in replacement treatment
Methadone other than in replacement treatment
Other opioids (e.g., tramadol, fentanyl, codeine, oxycodone) morphine
Cocaine or crack
LSD
MDMA a.k.a. ecstasy
GHB (gammas-hydro butyrate) or GBL (gamma-butyrolactone)
MDPV (“baths salts”), alpha-PVP (flakka) or other synthetic cations
Synthetic cannabinoids e.g.”JWH”
Hallucinogenic mushrooms e.g. psilocybin
Study sample
NFBC1986
Women
Men
Total
Women
Men
Total
Number of teeth, mean (SD)
24.4 (7.00)
22.9 (7.60)
23.4 (7.40)
a
27.9 (1.62)
28.4 (1.84)
28.1 (1.85)
BEWE
0–2, n (%)
21 (55.3)
28 (40.6)
49 (41.5)
d
455 (49.3)
275 (44.4)
730 (47.3)
c
3–8, n (%)
11 (28.9)
29 (42.0)
40 (33.9)
d
288 (31.2)
229 (36.9)
517 (33.5)
c
≥9, n (%)
6 (15.8)
12 (17.4)
18 (15.3)
d
188 (19.5)
116 (18.7)
296 (19–2)
c
Mean (SD)
3.6 (4.20)
4.4 (4.15)
4.11 (4.17)
d
4.00 (4.10)
4.36 (4.01)
4.14 (4.10)
c
Number of decayed teeth (ICDAS ≥3+)
0, n (%)
5 (13.2)
3 (4.3)
8 (7.4)
c
367 (39.4)
220 (35.4)
587 (37.8)
1–4, n (%)
16 (42.1)
19 (27.1)
35 (32.4)
c
473 (50.8)
317 (51.0)
790 (50.9)
≥5, n (%)
17 (44.7)
48 (68.6)
65 (60.2)
c
92 (9.9)
84 (13.5)
176 (11.3)
Mean (SD)
4.9 (3.98)*
8.3 (5.96)*
7.13 (5.58)
c
1.69 (2.26)
2.02 (2.64)
1.82 (2.42)
Decayed root remnants
No, n (%)
34 (89.5)
51 (69.9)
85 (76.6)
b
Yes, n (%)
4 (10.5)
22 (30.1)
24 (23.4)
b
Mean (SD)
0.3 (1.63)*
1.1 (2.43)*
0.86 (2.22)
b
Number of teeth with dental plaque
0–7, n (%)
17 (45.9)
19 (27.1)
36 (33.6)
d
783 (84.0)
452 (72.8)
1235 (79.3)
8–15, n (%)
9 (24.3)
16 (22.9)
25 (23.4)
d
118 (12.7)
132 (21.3)
250 (16.1)
≥16, n (%)
11 (29.7)
35 (50.0)
46 (43.0)
d
31 (3.3)
37 (6.0)
68 (4.4)
Mean (SD)
10.5 (8.99)*
14.5 (8.91)*
13.1 (9.10)
d
3.73 (4.57)
5.17 (5.58)
4.31 (5.04)
Number of teeth with gingival bleeding
0–7, n (%)
5 (13.5)
14 (20.0)
19 (17.8)
d
22 (2.5)
8 (1.4)
30 (2.1)
f
8–16, n (%)
16 (43.2)
21 (30.0)
37 (34.6)
d
112 (12.9)
47 (8.0)
159 (10.9)
f
≥17, n (%)
16 (43.2)
35 (50.0)
51 (43.2)
d
735 (84.6)
532 (90.6)
1267 (87.0)
f
Mean (SD)
15.1 (7.36)
16.3 (8.43)
15.9 (8.06)
d
22.7 (5.78)
24.1 (5.08)
23.3 (5.55)
f
Number of teeth with deepened periodontal pockets (≥4 mm)
0, n (%)
23 (62.2)
37 (52.9)
60 (56.1)
d
1–3, n (%)
8 (21.6)
17 (24.3)
25 (23.3)
d
≥4, n (%)
6 (16.2)
16 (22.9)
22 (20.6)
d
Mean (SD)
2.1 (4.82)
2.3 (3.76)
2.20 (4.14)
d
PUFA
0, n (%)
33 (89.2)
59 (84.3)
92 (86.0)
d
≥1, n (%)
4 (10.8)
11 (15.7)
15 (14.0)
d
Mean (SD)
0.2 (0.55)
0.3 (0.70)
0.22 (0.65)
d
Reduced salivation
No, n (%)
27 (81.8)
49 (74.2)
76 (64.4)
e
904 (97.4)
611 (98.7)
1514 (97.9)
b
Yes, n (%)
6 (18.2)
17 (25.8)
23 (19.5)
e
24 (2.6)
8 (1.3)
32 (2.1)
b
Author Biographies