
Abstract
Introduction
Substance misuse relapse – commonly understood as the resumption of drug using behavior after sustained periods of abstinence - has been found to increase the risk for overdose death by 80% (Sureshkumar et al., 2021). As drug overdose deaths have, worldwide, significantly increased in recent years (United Nations Office on Drugs and Crime [UNODC], 2021), relapse is an important aspect for relevant scientists, practitioners, and policymakers to consider. Nevertheless, relapse remains a relatively misunderstood aspect of addiction in both, its conceptualization and in how it is approached in treatment.
Historically, relapse has been conceptualized within a biomedical perspective of addiction, as part of the addiction disease. Since 1997, the National Institute on Drug Abuse (NIDA) has been promoting the ‘scientific’ perspective of addiction as a chronic relapsing brain disease, with the aim to counter the then widely accepted, and highly stigmatizing, view of addiction as being the result of people’s poor choices or moral failures (Kuorikoski & Uusitalo, 2018). Although this perspective has been invaluable for service users to gain better access to, and insurance cover for, treatment, it has also been constructing individuals seeking help for their addiction as 'sick' and 'in need of a cure'. This perspective has been endorsed through the dynamic relapse prevention model, one of the earliest relapse theories developed and refined by Marlatt and colleagues (see Marlatt & Donovan, 2005; Marlatt & Gordon, 1985; Witkiewitz & Marlatt, 2004). This theory forms the basis of relapse prevention strategies for identifying relapse risk and protective indicators. The theory holds that relapse occurs in situations where a person is at risk of violating their promise to maintain abstinence (i.e., abstinence violation effect). Relapse prevention strategies have since been developed using mindfulness, in the form of mindfulness-based relapse prevention strategies (Bowen et al., 2021). Here, mindfulness is used to help individuals become aware of, and cope with, their relapse risk factors. More recently, scientists have argued for the notion that addiction, and therefore recovery from addiction, is an ongoing process, which may or may not include periods of abstinence (Ashford et al., 2019; Best et al., 2021; Heather et al., 2022). This understanding has been conceptualized through recovery capital theory (Cloud & Granfield, 2008; Granfield & Cloud, 1999), which holds that recovery from addiction is a process which depends on a combination of someone’s available resources for recovery (i.e., recovery capital) - on a personal, social and community level. This theory has been further developed into the REC-CAP measure (Cano et al., 2017), which accounts for various recovery pathways and can be applied in treatment as well as recovery support services to track someone’s development of their recovery capital. It is therefore considered as a fundamentally strength-based approach to addiction recovery. As such, relapse is not seen as something which must be prevented because it violates recovery goals, but as something which can both decrease or increase someone’s recovery capital.
These theoretical perspectives of relapse have an impact on how relapse is being approached in treatment. Although the current UK drug policy “From Harm to Hope” (HM Government, 2022) fails to recognize relapse, it emphasizes that recovery can be a process which involves various strategies to reduce the harmful effects of addictions. This is however not reflected in clinical treatment service settings; treatment for people with substance use and addiction issues in the UK remains predominantly focused on the biomedical model of addiction, with treatment providers offering services in line with the view that recovery equals the absence of addiction symptoms (i.e., abstinence). As such, relapse is seen as negatively impacting treatment outcomes. This understanding is based on the ‘revolving door phenomenon’, meaning that people who relapse back into misuse and re-present to a service are not considered as effectively recovered; repeated admission into a drug service is being considered as a ‘poor treatment outcome’ which diminishes the service’s treatment outcome ratings data, and therefore (often) also their chances of receiving further funding from local authorities (Di Martino, 2022).
In addition to this, relapse puts additional stressors on specialist addiction services. For instance, when service users relapse and want to re-present back to the service, they have fewer chances of being seen and receiving timely treatment due to (sometimes year-long) waiting lists, understaffed services and higher caseloads, especially after the onset of COVID-19 (see Ali et al., 2021; Zastepa et al., 2020). In this sense, relapse has also a direct impact on treatment staff and the quality of their service provision. The ability of the counsellor or psychotherapist, who works within addiction treatment settings (henceforth, addiction therapist), to create and maintain a strong therapeutic alliance with their client, has been deemed as one of the defining factors which influences a client’s wellbeing and overall treatment outcome (Cook et al., 2015; Knock et al., 2021; Pettersen et al., 2019). Accordingly, the Substance Abuse and Mental Health Services Administration (SAMHSA) has established that addiction therapy competencies emphasize affect regulation as well as management of transference and countertransference (SAMHSA, 2006). However, within the context of increasing pressures to produce certain recovery/treatment targets as well as the increase in relapses and re-presentation of service users, addiction therapists are faced with relatively high risk of burnout; understood as a combination of emotional exhaustion, feelings of cynicism, and a sense of ineffectiveness (Leiter et al., 2014). As such, client relapses can be seen as not only compromising a service’s sustainability (i.e., through poor/incomplete treatment outcome data) but also a therapist’s sense of wellbeing and professional efficacy, which can impact on their ability to sustain a therapeutic alliance with their clients.
However, the wider addiction literature lacks an understanding of these tensions, specifically from a lived experience perspective of relevant stakeholders (e.g., addiction therapists). Our recent study on repeated relapse into substance misuse has demonstrated the importance of understanding relapse from a lived experience perspective (see Klein, 2021; Klein et al., 2022); the study highlighted important nuances of relapse, including that service users often identify relapse as crucial motivators for their recovery. However, this understanding will go relatively unnoticed in a treatment system in which relapse is demonized. In fact, the scientific debates on addiction recovery and relapse are seen as limiting and as lacking clinical utility. For example, Moe and colleagues (2022) found that relapse studies, historically, have lacked consensus on relapse definitions within a ‘disease’ perspective of addiction, while more recent studies have lacked consensus on how relapse can be operationalized within a more holistic perspective of recovery (i.e., when accounting for the varying phases of recovery). Therefore, it is invaluable to add the perspectives of those most closely linked to relapse – such as addiction therapists, as to gain a more accurate understanding of effectively supporting those who relapse, and those who support those who relapse. Whilst there is a handful of research on addiction therapists’ accounts of working with addicted individuals (see Najavits et al., 1995; Shinebourne & Adams, 2007) or their perspectives on various assessments (see Brewer & Tidy, 2019; Ekendahl & Karlsson, 2021; Tauscher et al., 2021), a gap remains in understanding relapse from their perspectives.
Given these limitations and the above-mentioned context, we propose that understanding what it is like for addiction therapists to experience their clients relapse and how this impacts therapists’ personally and professionally, is timely. Therefore, our study seeks to address two central questions: 1. What are addiction therapists’ lived experiences of supporting clients through relapse from substance misuse? 2. How do these experiences impact addiction therapists personally, and how do therapists make sense of these experiences within the context of their therapeutic work?
By addressing these questions, the study aims to generate an in-depth, and novel understanding around the impact of supporting clients through relapse on addiction therapists’ psychological wellbeing, treatment approaches, and therapeutic relationships, all of which will be invaluable for the development of appropriate and effective support strategies for addiction therapists and, consequently, their clients.
Methodology
Design
To address the questions and aims, we employed interpretative phenomenological analysis ([IPA], Smith et al., 2009, 2021). IPA is both a methodology and method of analysis for interpreting the in-depth lived experiences, specifically emphasizing the particular over the generic. This means that the IPA analyst seeks to highlight the part (i.e., each individual case) to generate a better understanding of the experiences on a whole (i.e., hermeneutic circle). IPA is grounded in three philosophical traditions: hermeneutics, phenomenology and idiography, all of which underpin the interpretations and overall data analysis (Nizza & Smith, 2021). Additionally, IPA analysts are provided with an opportunity to involve their background knowledge on the topic and utilize their own interpretations to further explore their case’s interpretations (i.e., double hermeneutics; Larkin et al., 2006). Given these methodological principles, as well as our aim of understanding how therapists experience and make sense of supporting their clients through relapse, we deemed IPA as most suitable for this study.
Sample
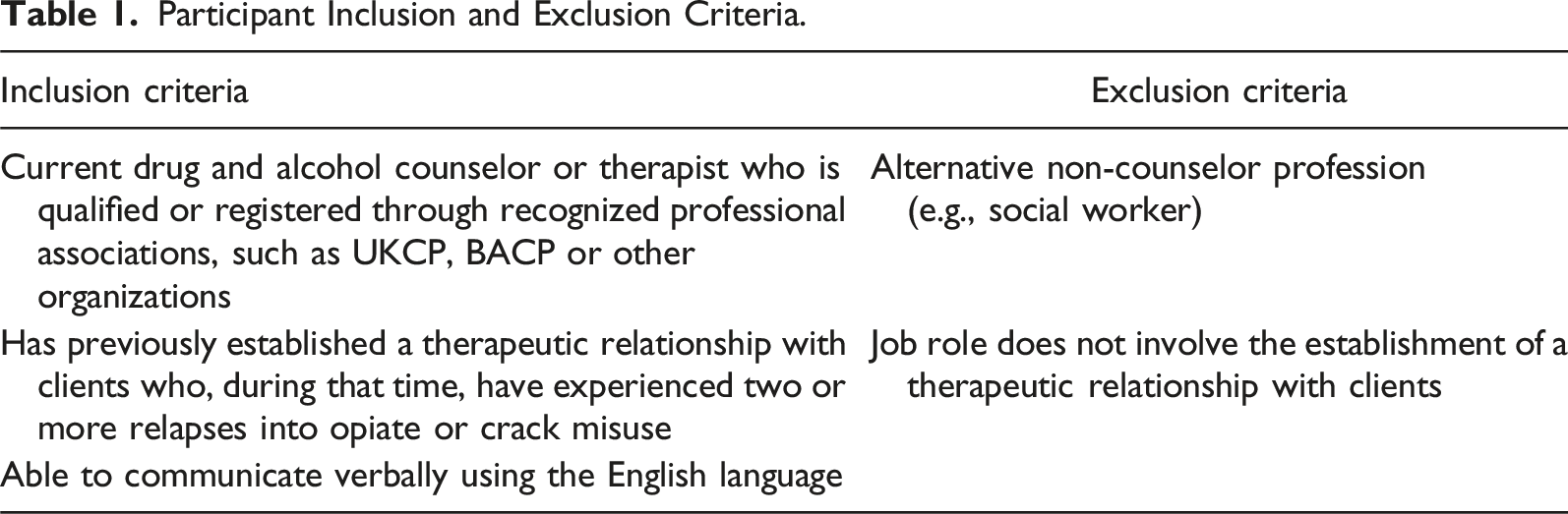
Participant Inclusion and Exclusion Criteria.
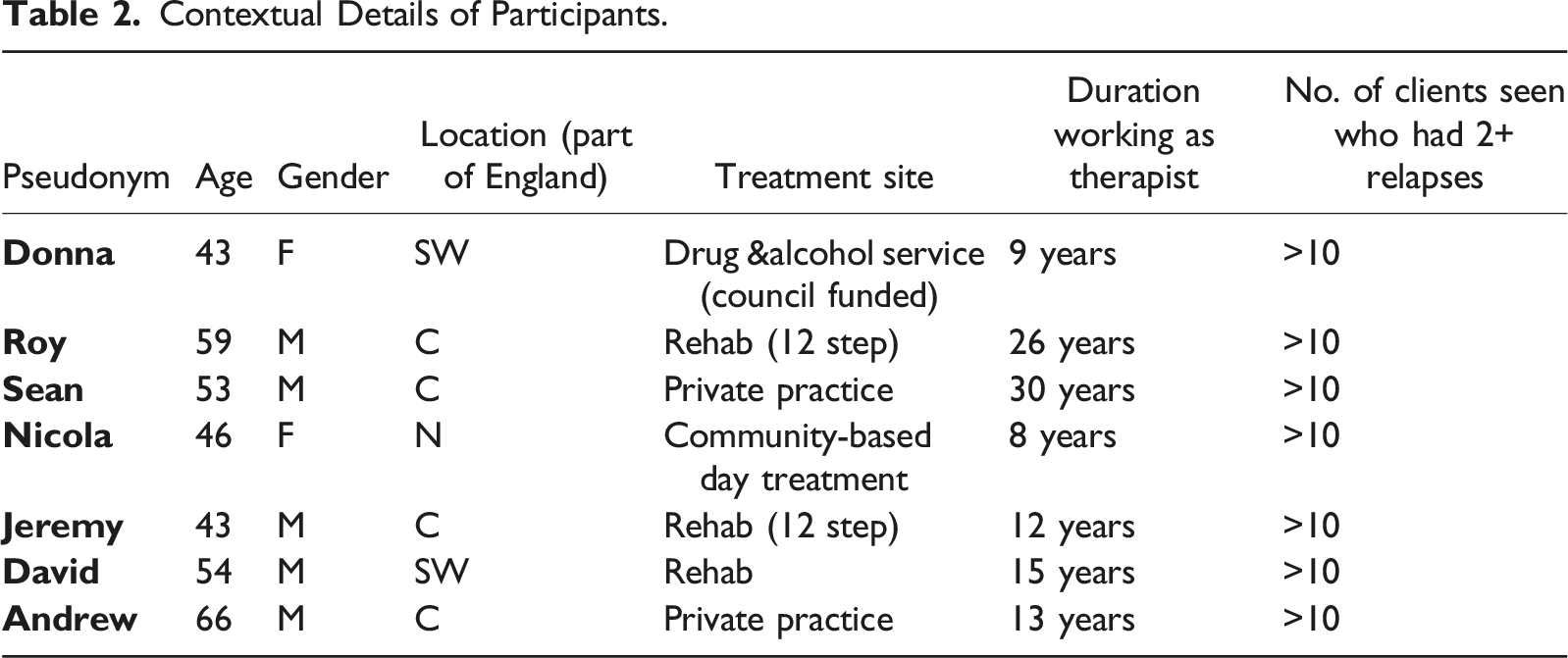
Contextual Details of Participants.
Data Generation
Data were generated via individual, semi-structured interviews which were held virtually, via Microsoft Teams, due to the COVID-19 restrictions at the time. Following Smith and Osborn’s (2015) guidance for interviewing in IPA, a semi-structured interview guide was developed and piloted prior to commencing the interviews. Questions focused on therapists’ feelings, thought patterns and physical sensations when witnessing a client relapse, as well as how this impacted their approach to supporting clients in their recovery. Interviews lasted between 1.5 and 2 hours. Ethical approval for the project was granted from the host university’s Research Ethics Committee (S18-017). All participants gave informed consent, which the first author noted on a separate consent form. Each interview was then recorded and subsequently transcribed by the first author.
Data Analysis
IPA offers a protocol with analytical steps for inductively generating a thematic account, which was adopted in this study. These steps are applied to each individual transcript and include 1) reading the transcript, 2) initial coding, 3) transforming codes into interpretations, 4) reflecting and interrogating the interpretations, 5) developing themes from interpretations and, 6) moving on to the next transcript, repeating each step (Smith et al., 2021). During the first step, the transcript was read and any initial thoughts, assumptions or points of interest to the author were noted on the side. This ‘bracketing’ process was important so that any preconceived ideas about the data could be ‘parked’, to prevent this from clouding the overall analytical judgment. In line with Larkin and colleagues’ (2006) suggestion, the next step required careful line-by-line coding of each individual transcript. This involved coding of descriptive, linguistic, and contextual elements in each transcript, to identify things that mattered to the participant (objects of concern), the meaning that participants attributed to these things (experiential claims), and participants’ stances in relation to these things (dispositions). These steps were repeated for each individual transcript before a thematic account was developed across the whole sample set.
The first author was responsible for all analysis steps whilst authors two and three conducted independent credibility checks; they reviewed the codes and themes to ensure coding validity and to identify any biases about the data. This was because authors two and three were the research supervisors and also practitioners in the field, who had methodological and practical expertise and could identify any themes that may have been influenced by the first author’s biases and assumptions. After independently checking, all authors critically discussed the development of themes, with authors two and three highlighting any issues and providing the first author with recommendations for areas for development. These critical discussions were engaged with frequently, throughout the course of the study, as is good practice in IPA research. Amongst other things, this involved frequent critical discussions about how our own values, assumptions and biases could impact our interpretation of the data. Additionally, the first author kept a research diary to record her thoughts and reflections throughout the study. Notes from this diary were also recorded on an audit trail, which the first author kept throughout the data generation process. This audit trail consisted of researcher comments, reflections, codes and theme spreadsheets (Morrow, 2005). The data that support the findings of this study are openly available in the host University’s Research Data Archive.
Findings
Three superordinate themes were identified during the data analysis: “Therapeutic view of relapse”, “Relapse de-powers therapeutic work” and “Therapist role after relapse”. Each superordinate theme also encompasses several individual subthemes, which highlight the nuances of participants’ lived experiences. We now present each superordinate theme, using verbatim quotes from the text as a guide.
Superordinate Theme One: Therapeutic View of Relapse
Participants offered various perceptions of relapse in relation to recovery from substance misuse. This first superordinate theme was collectively shared by all participants and presented itself in two sub-themes.
Relapse as Multidimensional and Multifunctional
Most therapists conceptualized relapse as multidimensional; as having multiple parts. For instance, Roy mentioned that there is “(…) an element of relapse”, indicating that he saw relapse as being made up of multiple parts. Multiple dimensions of relapse were evident in accounts of both, unsuccessful and successful recovery as indicated by Sean: “It’s not particularly (…) at the failure side of it only; it could be part of the successful kind of journey”. Both Roy and Sean allude to the perceived complexity of relapse and that there is also a dimension of relapse which is neither considered as setback nor as hindering the individual from recovering, but as a dimension which marks growth or a desired outcome. However, there was also an interpretation of relapse which reflects the medical model of addiction as it results in only one outcome, as highlighted by David: “(…) relapse is the process that leads up to you starting to use your substance again” and by Nicola: “The substance or the action is always the last thing to happen”. Here, relapse is interpreted as something with multiple parts (i.e., “process that leads up to”) as well as being part of something (i.e., “last thing”). These statements highlight that therapists hold a multifaceted and complex perception of relapse.
Another way in which therapists perceived relapse was as multifunctional; in other words, as something which served a useful function for themselves as well as their clients. For instance, several participants recognized a client’s relapse as a humbling experience for them; in that it helped them to remember their own limits and to appreciate clients’ experiences, as highlighted by Sean: “Relapse is a very loud way of teaching us to actually respect our clients”. Here, Sean emphasizes his client’s autonomy and recognizes that he cannot make his clients engage (or not engage) in a certain behavior, but that his client has choice. Viewing relapse as a reminder to stay grounded was also shared by David: It's a reminder of how difficult it is to work with addiction. How challenging it is. But it is also a reminder of how difficult it is for people in their positions.
Here, David revealed that relapse enabled him to maintain an empathetic and compassionate view towards himself, his colleagues, and his clients. In addition, some therapists understood relapse as protecting, empowering, regulating and motivating clients. Relapse was understood by some as a protective strategy which service users developed to help them cope with painful experiences, as Andrew indicated: “(…) they’re revisiting their pain, the emotional pain, and they’re revisiting it in the most secure way they feel able to deal with”. Additionally, therapists viewed relapse as having other useful functions. For instance, Donna expressed relapse to be a learning opportunity for clients: “(…) people that will have one or two relapses, will use those as a learning process. And they will move forward and move forward strongly”. This interpretation implied that relapse could empower clients by enabling them to build stamina which would then facilitate self-discovery. In addition, relapse was conceptualized as providing clients with the motivation which they may have lacked previously, as indicated by Jeremy: “(…) quite often, somebody who has had a serious relapse, they are so much more motivated.” This relapse ‘function’ was seen to be providing some individuals with more drive/motivation to pursue recovery again. A last way in which relapse was conceptualized as serving a function was captured by Roy: He’d done what he needed to survive. And the relapse had given him the voice (…); him returning to the cocaine wasn’t about relapsing. It was about him using that to regulate his emotions.
Here, Roy acknowledged that relapse helped the individual to regain agency and to regulate his emotions by turning the reaction inward, towards himself (i.e., using drugs) rather than reacting outwardly towards someone or something else.
Relapse as Responsibility
Some therapists explained relapse as either independent of, or dependent on, their therapeutic efforts. Where therapists alluded to relapse as being independent of their therapeutic work, the responsibility for relapse was put on the client. For instance, David states: “Sometimes you have to question whether they want to survive (…) are they able and willing to use [their relapse] to make changes that need to happen?“. Here, David explains his client’s relapse as their willingness, or unwillingness, to live and learn, rather than blaming his own therapeutic efforts. This, more or less, boundaried understanding of what the therapist’s responsibility is, has also been shared by Sean: “(…) this is their success, not mine”. And I’m respecting their decision, even though I don’t approve that.” This statement was relating to Sean’s attitude towards his clients’ recovery; neither successful nor unsuccessful recovery, including relapse, are the responsibility of his therapeutic work. In fact, Sean highlights that these are but mere decisions of his clients, which he respects. Similarly, assigning responsibility for relapse to the client was expressed by Donna: “(…) just because you’ve decided that you want to relapse, why do I have to drop everything?“. Here, Donna expresses her reluctancy to re-engage with her client who has relapsed, after conceptualizing relapse as her client’s decision. This conceptualization may have been particularly emphasized as she was recalling this client to request urgent support after they had relapsed, whilst Donna was experiencing increasing caseloads at her service, and therefore felt she had very limited time available.
However, blaming the client for their relapse and conceptualizing relapse as their choice or decision shifted when relapse ended in death, in which case relapse was viewed as being the result of therapists’ own therapeutic failures. For instance, Jeremy shares: “When the guy died (…) it made me really evaluate how I did the work”. Similarly, Andrew highlights: “I’m thinking, ‘oh, I caused you to relapse!’ So there’s a bit of self-punishment”. Additionally, Sean explains: “Their failure is my failure; my failure is their failure, and I’m connected to the setbacks”. Together, these statements reiterate that there is an emotional self-blaming or self-burdening when clients of therapists experience a fatal relapse. It is also striking that when relapses are fatal, they are thought of as “failures” rather than bad “choices” or “decisions”, which were the explanations used in the above cases. Overall, there seems to be an increased risk of blurring professional boundaries (i.e., what therapists are responsible for and what they are not) when relapses are fatal. David offers insights into his thought process after experiencing fatal relapse: I was numbed. And the reason being is the night that she relapsed, she rang me, and I didn't take the call. So, I was left in quite a numb position. I just felt awful in that instance.
In this excerpt, David’s immediate thought was to blame himself for his client’s relapse. His repeated use of the word “numb” also illuminates a sense of guilt around his internal blame-taking, which left him in shock.
Taken together, this first theme revealed that therapists varied in how they therapeutically perceived relapse. Some understood relapse as multidimensional whilst others as multifunctional. Additionally, therapists viewed relapse as either being the responsibility of the client (i.e., the client’s decision) or as consequence of their own therapeutic efforts (i.e., how well they have engaged with their clients). The accounts further highlighted that this process of assigning responsibility is influenced by the intensity of the relapse experience (i.e., relapse vs. fatal relapse).
Superordinate Theme Two: Relapse De-Powers Therapeutic Work
This second superordinate theme highlights what it felt like for participants to experience their clients relapse repeatedly and was reflected in two sub-themes.
Towards Disempowerment
The first subtheme refers to a process which was shared by all therapists; a process in which participants moved from feeling intense loss to gradually feeling disempowered. When reflecting on the emotions and feelings in response to a client’s relapse, therapists’ accounts focused largely on fatal relapses and how this experience transformed their ability to empathize. First, relapses, especially those that ended in death, resulted in participants feelings shock and loss. This was especially the case when relapses were unexpected or sudden, as explained by Jeremy: “I think it’s the fact that he’s been here one day and the next day he was dead (…) it was quite traumatic”. Similarly, Sean alludes to a spiritual level of loss: “It [relapse] takes something out of us [therapists], something of me goes with the person”. Another, more somatic, level of loss was expressed by Nicola: There is definitely a sinking feeling and that can be like, you know, something just kind of drops in your spirit. And you can feel it, definitely, there is a tangible kind of disappointment on their behalf.
Nicola’s statement indicates the intensity with which she empathizes with her relapsing clients. Therapists’ accounts further highlighted that this empathic ability, over time and with each added relapse, develops either into self-doubt or emotional detachment. For example, Andrew shared that he feels “(…) not good enough” after his client relapsed multiple times. However, Donna highlights that she felt “emotionally tougher” with each relapse experience. Similarly, Jeremy explains: “I’m more philosophical now than I was (…) slightly desensitized, I would say, because I’ve seen it so much”. Although the ability to empathize on different levels is usually perceived as a gift in therapeutic work, these statements illuminate that numerous relapse encounters can lead to intense loss and even emotional numbness. This emotional desensitization gradually develops therapists to feel “powerless” (Jeremy), as was captured well by David: “[Witnessing relapse] it’s frustrating…there’s nothing you can do”. These statements demonstrate the long-term psychological effects of multiple relapses on therapists. The repeated element of relapse numbs therapists’ unique empathic abilities and develops within them a feeling of powerlessness over their supportive work.
Factors Impacting Emotional Responses
The second subtheme reflects a more nuanced position. Participants expressed that their emotional responses also depended on other variables, including the strength of the therapeutic connection, the client’s attitude toward relapse and the frequency of relapse. For example, Sean highlighted that the therapeutic alliance with his client determined how relapse impacted him psychologically: It feels to me [with] some people you are close enough to have some sort of connection and when those [clients] relapse, it cuts deeper…it's different degrees of sadness when [those] people relapse.
By referring to his sadness in “different degrees”, he emphasized that not all clients’ relapses impacted him deeply. Rather, an increased sense of loss was felt when his emotional connection, or therapeutic alliance, with the client was strong. This emotional experiencing was shared by Roy: “(…) when you do have that connection with someone, you are inclined to be more sympathetic to their arguments [for relapse]”. Additionally, some therapists shared that their emotional responses varied with their clients’ attitudes towards their relapses. For instance, Donna shares: If they’re self-reflecting of what they can do differently next time, then there’s a practical ‘what can we do’ [but] if they come in and they are just a welter of self-pity…I will be thinking ‘oh for goodness’ sake! You idiot!’.
Here, Donna seems to experience a mirroring of emotional responses; whenever her clients return with enthusiasm, she feels enthusiastic but when clients return in a state of “self-pity”, Donna seems to become judgmental and accusatory. Donna’s case, in particular, has demonstrated her levels of emotional detachment from her clients, which may contribute to her choice of blaming language. On the other hand, when clients were actively working on their recovery post-relapse, therapists felt more positive. This was supported by Sean, who shared: “Even though I heard that he was kind of relapsing…it wasn't very heavy because I heard it and he's trying to do something about it (…). It was more hopeful because he's trying to pull his life together”. It seems that clients’ attitudes towards their relapse, whether they become hopeless or motivated to do better, have an effect on how therapists feel about the relapse. Taken together, these emotional responses link to the ways in which therapists assign responsibility for relapse
Thirdly, therapists expressed that their emotional response depends on the number of relapses a client experienced, with each relapse having a culminative impact. This emotional process was explained in more detail by Roy: If it gets to the fourth time, then then there's been a massive investment…you’re having worked for someone for a fairly long period of time. I think it does have a cumulative effect, so the more times it happens…it wrecks me, you know, I feel like I could cry.
Here, Roy highlights that the more a client relapses, the more he feels emotionally attached to, and ‘invested’ in, his client’s progress. As such, Roy’s emotional experience is more intense when relapses accumulate, which seems to stand in contrast to the theme above, in which some of the therapists felt desensitized to their clients’ relapses, the more often these occurred. The quote may also speak to the strength of their therapeutic bond, where strong levels of empathy and commitment to the client’s process have been developed. However, this has an even greater effect on Roy’s emotional processing as the number of relapses increases. Roy’s use of the word “wrecked” signifies this; the level of pain which he experiences on behalf of his client’s relapse and a sense of devastation over the loss he feels for the work he has done with this client, including his hopes for this client and their achievements made, up to that point. Lastly, this demonstrates that Roy, regardless of the number of relapses, keeps up expectations and hope for his clients. This was not the case for other therapists, as expressed by Donna: “(…) once you start coming into three or four lapses, four or five…pretty much on a bit of a ‘merry go around’. And I think perhaps my expectation of them lowers as well”.
In summary, therapists’ emotional responses (when working with the same client throughout multiple relapse experiences) seemed to transform, over time and with each added relapse, from intense empathy to feelings of disempowerment. The accounts varied around what factors influenced therapists’ emotional responses, including their therapeutic relationship to that client, the client’s personal attitude towards their relapse and the number of relapses.
Superordinate Theme Three: Therapists Role After Relapse
A third theme identified how experiences of relapse shaped therapists’ positionality towards recovery, or, how they formulated their therapeutic role in supporting clients. The theme highlights how therapists, after having supported their clients through relapses, saw themselves as a travel companion on their client’s recovery journey and as someone who must maintain a balance between hope and caution. Words like “together” (Andrew) or “along” (Sean) were used to suggest that their role as travel companions was proactive, ongoing, and involved persistence. For example, Sean made a clear distinction in his therapeutic role by stating: “I’m a fellow traveler. I’m not their therapist…deep down I’m actually travelling alongside another human being in his journey in life”. As a travel companion, therapists understood themselves as providing clients with ongoing, non-judgmental support throughout any uncertainties or challenges. This included being available to support their clients even after they have achieved their recovery goals. In addition, therapists understood their role as travel companion to involve maintaining hope. For example, Andrew shared that he “always feel[s] very disappointed (…) and deflated when a client relapses, but there’s a joy”. Here, Andrew reflects that remaining hopeful when faced with a potentially fatal relapse (i.e., when a relapse results in death, often through overdose), involved remembering the positives and possibilities that relapse can bring. Nicola shared this view, and expounded further on how she practices this internal balance between hope and caution around the risks of potential harm/death of relapse: [Relapse] it'’s about the middle road. So, there is still hope if you do relapse even if it’s multiple times. And there is also a real kind of seriousness to be had with it because you just never know whether that relapse could potentially be the last as well. So, I suppose it gives me the balance of recognizing that there’s hope, but there’s also an urgency and a seriousness to it as well.
Nicola revealed that her role involves regulating her emotions, even when faced with the possibility of a client experiencing a fatal relapse. As such, it illustrates a rather jarring position for therapists; although their very work is dependent on empathy and therapeutic connection with a client, this does develop into a more cautious and detached attitude towards recovery goals, as there is a real risk of harm and death from relapse. In summary, this last superordinate theme provided insights into the impact of relapse on therapists’ perception of their therapeutic roles. All participants shared the view that their therapeutic role includes offering consistent yet flexible support while maintaining an attitude of hope for themselves as well as for their clients. This theme also offered insights into how therapists, who have experienced some of their clients relapse repeatedly, are conceptualizing recovery. They understand recovery to be a pathway, a journey, a process; something that is non-linear, rather than a binary treatment outcome, such as ‘not using drugs’. Within this conceptualization, their roles as therapists seem more accepting, tolerant and compassionate towards relapse rather than as rigid prescribers of how recovery should look like and of treatments (e.g., steps to follow for achieving abstinence) in which relapse has no value.
Discussion
This study is the first to use a phenomenological, hermeneutic, and idiographic design to elucidate the issues and experiences of seven addiction therapists who have supported clients through relapses from opiates and crack cocaine in UK based addiction treatment facilities. Findings demonstrated that therapists identify relapse as a multi-factorial, and sometimes positive, phenomenon. This interpretation is in line with Witkiewitz & Marlatt’s (2004) dynamic relapse prevention model, which has established relapse as a dynamic process of maladaptive responses to internal and external stressors, ultimately leading the individual to resume their substance use. What was striking in therapists’ accounts was their conceptualization of relapse as multifunctional; that is, as serving a useful function for both, themselves, and their clients. As our findings indicate that some therapists find value in relapse (e.g., to be reminded of the limitations in their work), it demonstrates a relative split from the (still) dominant scientific understanding that relapse is part of a medical model of addiction, and a chronic indicator of illness, of failure or ineffectiveness in treatment (Gutman, 2006; Slomski, 2014). With that, our findings support the notion that recovery is not a linear pathway (White, 2007), but a spectrum of pathways which are fluid and co-exist (Ashford et al., 2019; Heather et al., 2022). This aligns with recovery capital theory (Cano et al., 2017; Cloud & Granfield, 2008) which understands substance use recovery as simultaneously happening on various life spheres (personal, social, community). As became clear in the findings, therapists justify relapse in one of two ways: as either being the client’s choice or, especially after fatal relapse experiences, as the responsibility of their own therapeutic work, or perceived lack thereof. This aligns with previous research which found that treatment providers often combined models of addiction (i.e., disease, choice, moral behavior models) to understand clients, thereby leading therapists to perceiving them as both, disordered and in control (Ekendahl & Karlsson, 2021). This finding is significant because the change between the above-mentioned justifications occurred more often with clients who relapsed multiple times versus only one, or two times. As such, the prevalence of relapse is an important factor which influences therapists’ clinical views on, and subsequent delivery of treatment for, relapse.
Additionally, our findings demonstrated that addiction therapists experience relapse intensely, psychologically and emotionally, which manifests in internalized loss, emotional numbness, and feelings of disempowerment. Such feelings can also have consequences for the quality of therapeutic work. As Pettersen and colleagues (2019) have pointed out, therapists’ emotions can be perceived by their clients and, if the therapist feels hopeless for the client, this can create mixed messages for the aims of treatment. Therapists in this study expressed that they became more emotionally detached from their work with clients in general, the more they experienced their clients relapsing, which resulted in a sense of powerlessness over their therapeutic abilities. Reasons for this indicate a self-protective strategy, during which therapists protect themselves from feeling like a failure and remain in a more objective, detached, therapeutic role. As such, this indicates that relapse seems to adversely affect the therapeutic relationship as a result of therapists’ emotional withdrawal, and thereby further develops Van der Merve’s (2019) conclusions that psychologists’ unwanted emotions in a therapeutic relationship affect their self-concept and professional identity. In summary, therapists who have supported many clients through their multiple relapses seem to be at significant higher risk of experiencing compassion fatigue, which could also have a knock-on effect on their therapeutic effectiveness.
Lastly, our findings revealed how therapists who support someone through repeated relapses can shift their perception and formulation of their therapeutic roles. Findings of this study imply that therapeutic competencies, when supporting clients through multiple relapses, reach far beyond attitude and knowledge, which the leading international regulators consider as most important competencies (SAMHSA, 2006). Participants in this study reformulated their therapeutic role as offering consistent encouragement, guidance, and companionship, like a travel companion. Additionally, therapists highlighted a sense of duty to maintain an attitude of hope, specifically in the face of fatal relapse. This is consistent with Rosenberg, Arnold, and Schenker (2021) who argued that “holding complex, flexible, and diverse hopes enables patients to believe in the unlikely while simultaneously accepting the inevitable. The role of clinicians is to support both.” (p. 1260). These shifts in role perspective may need to be openly communicated to any addiction therapists, and specifically to beginners, via clinical trainings or supervisions, to minimize the risk for therapists to overstep their boundaries and subsequently feel overworked.
In summary, and perhaps most importantly, these findings have unearthed the links between definitions/perspectives of, and therapeutic practice approaches to, relapse; the ways in which addiction therapists in this study have conceptually understood relapse has had a direct impact on how they have emotionally experienced their clients’ relapses, all of which has had an impact on the ways in which these therapists conceptualized their therapeutic role in further supporting their clients’ recovery. This interplay between understanding, experiencing, and sense-making (i.e., therapeutic identity) among addiction therapists has several important implications for future practice and policy.
Implications
Supporting a client through relapse can impact therapists’ emotional wellbeing and foster a sense of emotional detachment from clients and their treatment goals. This was mainly reflected in a change in therapists’ expectations of treatment outcomes after multiple relapses. As such, this finding has clinical relevance and adds to Spagnolo et al.’s (2015) research which has shown that therapists’ expectations (positive and negative) can influence the expectations of clients, and thereby impact therapeutic outcomes. In other words, relapse diminishes both the therapeutic relationship and therapeutic goals/expectations, including therapists’ perceived professional efficacy, and can lead to a mirrored sense of powerlessness which can affect a client’s belief that recovery is a realistic goal. On a conceptual level, this evidence adds an important dimension to Marlatt’s dynamic relapse prevention model (Witkiewitz & Marlatt, 2004), which emphasizes the abstinence violation effect as one of the main contributing factors for relapse. The relapse prevention model must consider the interplay between relapse and the therapeutic relationship, all of which has a considerable impact on the client’s self-efficacy and motivation for recovery. In addition, this finding could be conceptualized within the recovery capital model (Cano et al., 2017), which should account for the therapeutic alliance (particularly long-term) as an important resource for, as well as barrier to, recovery. Additionally, new evidence was generated on therapists’ perceptions of their therapeutic roles after supporting clients through relapses, and therefore warrants further research. This could, for instance, include a longitudinal design to better understand the transition process and nuances in perception change over time. This also suggests frequent reviewing (and potentially redrafting) of practice guidelines around the impact of relapse on treatment retention as well as on staff turnover from specialist addiction services, for which findings of this study could be useful.
On a practical level, the findings imply that therapists must be provided with appropriate strategies for upkeeping levels of empathy whilst remaining pragmatic about the real risks (and potential death) of relapse. As such, psychoeducation about approaches to recovery as well as understandings of what constitutes recovery must consider relapse as a pathway, rather than a roadblock to, recovery. Additionally, and within the harm reduction notion of addiction recovery, the use of naloxone may need to be more widely promoted as a form of preventing fatal relapses. Lastly, practitioners may need to engage in practices which support their self-concept as a therapist and their ability to empathize with, attach and commit to their clients. This could be done through the implementation of Compassionate Mind Training ([CMT], Beaumont & Martin, 2016), which is useful for supporting individuals who suffer from self-criticism, or via regular peer supervision, so as to foster a sense of community and a ‘me too’ mentality. If left unsupported, these effects can contribute to therapist burnout. Given that burnout rates remain a prevalent issue among addiction therapists, this is important to consider. For instance, Vilardaga and colleagues’ (2011) study evidenced that up to 50% of addiction therapists suffer at least one episode of burnout during their career. They also highlighted three factors to correlate with burnout risk in addiction therapists: experiential avoidance (i.e., the unwillingness to stay connected to certain thoughts or feelings), cognitive fusion (i.e., the ability to see thoughts as ‘just thoughts’) and values commitment (i.e., engaging in behavior which aligns with certain values). As such, therapists with less relapse experiences, or beginners who are starting out in the field, must be made aware of, and prepared for, these risks. To preserve the quality of therapeutic support to clients as well as therapists’ own wellbeing, future practice guidelines may need to consider more frequent and focused supervisory care for therapists who re-engage with clients who have relapsed extensively.
Limitations and Strengths
The current study must be considered in the light of some limitations. Firstly, given the COVID-19 restrictions at the time, interviews were held virtually. Historically, the use of telephone or other non-face-to-face methods to qualitative interviewing has been considered inferior to face-to-face interviews, because the interviewer would have less scope to build rapport or to gauge participants’ non-verbal cues, thereby limiting the data (Novick, 2008). However, the interviewer was, at the time, offering therapy sessions over video chat and therefore familiar with building rapport this way. Additionally, we believe that there were no issues around generating good, appropriate interview data from the use of video chat. Secondly, interviewing virtually meant the sample was limited to participants who had access to such options (i.e., stable Wi-Fi, video-chat function). We acknowledge this as something which must be considered in additional research of this nature. However, we believe this to be a strength of this study, given that remote interviewing seemed to widen the reach for potential participants and was even perceived as a comfortable solution for those who, due to local lockdown restrictions, could otherwise not have participated. Thirdly, the sample consisted of psychotherapists belonging to a professional association in the UK, thereby limiting generalizability of other addiction professionals, such as social workers or psychologists. More research which considers the lived experiences of other addiction professionals is now warranted. Lastly, the sample was predominantly male, which may have been due to the recruitment network and/or the recruitment sites that were chosen. As such, to provide a more comprehensive picture of the effects of these experiences, more research of how female addiction therapists experience clients relapsing should be conducted.
Limitations notwithstanding, the current study offers important insights into addiction therapists’ lived experiences of supporting clients through relapses, an area which was significantly understudied. Therefore, the use of IPA was seen as a strength. Second, it should be noted that the first author works as an addiction therapist. Given that IPA is compatible with the researcher having awareness of the phenomenon of interest, this was believed to be a strength of the present study. Lastly, findings of this study do not only support existing literature but also offer additional important considerations as scope for developing future practice and research.
Conclusion
This was the first study to explore addiction therapists’ lived experience perspectives of working with service users who have repeatedly relapsed. Substance misuse relapse can significantly impact the therapist’s therapeutic connection with a client, their expectations about clients, and, ultimately, their recovery pathways. This is because working with individuals who relapse often, particularly for longer periods of time, may lead therapeutic professionals to become desensitized to their therapeutic work, which clients can perceive as ambivalence or lack of optimism about the treatment they are being provided. As such, relapse not only risks the wellbeing of therapists but also the outcome of their therapeutic work with clients. These complex risks, for therapeutic professionals as well as service users, must be considered in future research, policies and practice initiatives. Perhaps most importantly, future practice approaches must address relapse as a concept integrated in, not separated from, addiction recovery, so as to promote a non-judgmental and compassionate-informed recovery pathway.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council, Society for the Study of Addictions.