
Abstract
Contrasting widespread speculation in the media and public debate about spiking (administration of a substance to a person without their knowledge/consent), empirical evidence on the subject is lacking. This study aimed to investigate the assumed prevalence, perceived likelihood, and fear of drink-versus needle-spiking, and associated mental strain. Data from a cross-sectional online-survey (November 2022 – January 2023) of 1916 adults connected to Berlin’s nightlife-scene were analyzed. Almost a quarter reported having experienced drink-spiking, but only a small fraction sought medical or police attention; about 1% suspected needle-spiking. Presumptive victims of drink-spiking rated the likelihood and fear of spiking significantly higher and exhibited more symptoms of depression and anxiety. Considering toxicological and police findings, the reported prevalence and perceived likelihood of spiking seem to be highly overestimated. This, in conjunction with associated mental strain, highlights the importance of adequately addressing the issue of spiking through psychoeducation, prevention, and interprofessional investigation.
Introduction
Concerns regarding “spiking attacks”, so-called “knockout drops”, “date-rape drugs”, and related issues have been present for many years and periodically received pronounced attention (Blandamer et al., 2023; Sheard, 2011; Taylor et al., 2004). The discussion of this topic in media and society has intensified in 2021 and 2022 due to the (re-)emergence of the phenomenon “needle spiking” (Blandamer et al., 2023; Campion-Vincent, 2022; Home Affairs Committee, 2022).
Spiking is an umbrella term for the intentional administration of a substance to a person without their knowledge or consent; often with the goal of rendering the intended recipient unconscious or incapacitated. Drink spiking qualifies as a possible modality and refers to the addition of alcohol, illegal substances, or prescription drugs (e.g., tranquilizers, sedatives, opioids) to non-alcoholic or alcoholic drinks. Needle spiking (injection spiking, syringe spiking) denotes the administering of a substance by injecting a needle. Further methods of spiking are conceivable, including the intentional mislabelling of optically indistinguishable substances (e.g., labelling ketamine as amphetamine).
Whereas mainstream media pays great attention to spiking and cites vast numbers of spiking incidents, even calling out a “spiking epidemic” (Weaver, 2022), the empirical evidence regarding spiking is scarce. Of the few existing studies, most concern drink spiking in the context of drug-facilitated sexual assault (DFSA) whereas other conceivable motives and outcomes of spiking, such as robbery, are understudied (Sheard, 2011; Swan et al., 2017).
To date, it remains elusive to accurately estimate the prevalence of spiking (Blandamer et al., 2023; Sheard, 2011). Many individuals seem reluctant to seek medical and/or police services to investigate suspected spiking – probably due to stigma, shame, insecurity, and other barriers associated with such incidents (Busardò et al., 2019; Taylor et al., 2004). Further, even among those who do seek professional investigation, the suspicion of spiking is often not confirmed: In the vast majority of cases, involuntarily consumed substances are not detected or their pharmacological profiles do not align with spiking (Greene et al., 2007; Hughes et al., 2007; Quigley et al., 2009). Contrary to the widespread populistic assumption that gamma-Hydroxybutyric acid (GHB) / gamma-Butyrolactone (GBL) is frequently used in drink spiking, this substance is seldomly detected in toxicological analyses. Instead, high levels of alcohol intoxications seem to play a much more prominent role than often expected (Anderson et al., 2019; Bühler et al., 2019; Fiorentin & Logan, 2019; Greene et al., 2007; Hughes et al., 2007; Quigley et al., 2009). In a prospective observational case series, Greene et al. (2007) investigated urine and blood samples from 78 adults (mean age = 24 years; 82% women, 18% men) who presented to an emergency department in London within 12 hours of allegedly having consumed a spiked drink. Ethanol was detected in 90% of participants. The mean serum ethanol concentration was 1.65 g/L (range: 0.04–3.10 g/L) and 60% exhibited a concentration associated with significant intoxication (>1.5 g/L). Whether these levels of intoxication were voluntary or (in part) due to spiking with alcohol remains indistinguishable. Illicit drugs were detected in 12 (15%) participants, prescription drugs in 13 (16.7%). Illicit or medicinal substances of unexplained origin (with denied intentional exposure) were detected in eight participants (10%). Three of these cases exhibited methylenedioxymethamphetamine (MDMA), three cannabis, and two (3%) unexplained sedative drug exposure (one case GHB/GBL; one case benzodiazepine) (Greene et al., 2007). In a prospective observational study of 97 individuals with suspected drink spiking within the previous 12 hours at an emergency department in Australia, nine cases appeared to be clinically plausible and in four of those cases unexpected substances were detected (Quigley et al., 2009). In a descriptive toxicological analysis of urine and blood samples of 264 females aged ≥12 years who sought consultation at a Sexual Assault Center in Trondheim (Norway) between 2003 and 2010, Ethanol was again the most prevalent substance, with high concentrations frequently observed (estimated median serum ethanol concentration at the time of assault: 1.87 g/L) (Hagemann et al., 2013). A total of 19% screened positive for drugs; 62% of these with benzodiazepines/benzodiazepine-like-drugs, 28% central stimulants (MDMA, amphetamine, methamphetamine), 26% cannabinoids, and 18% opioids; no one tested positive for GHB/GBL. A total of 57 females (22%) suspected proactive DFSA, but only seven (12%) of these individuals tested positive for substances not voluntarily ingested (benzodiazepines, opioids, cannabis, and amphetamines). Toxicological results from a study in Wales (UK) (Hughes et al., 2007) as well as a Canadian study of 882 alleged victims of DFSA (mean age = 26 years; 96.2% women, 3.8% males; Du Mont et al., 2010) aligned with these findings. In 87 (10%) cases, unexpected drugs were found, and again, most of them were not typically expected “spiking drugs”: 40% cannabinoids, 32% cocaine, 14% amphetamines, 9% MDMA, 2% ketamine, and 1% GHB/GBL (Du Mont et al., 2010).
The prevalence of spiking suspicions seems to mirror the topic’s media presence and awareness campaigns (Sheard, 2011; Taylor et al., 2004). This trend was evident for decades for drink spiking suspicions and skyrocketed in the past two years regarding needle spiking (Blandamer et al., 2023; Campion-Vincent, 2022; Home Affairs Committee, 2022). For example, the UK National Police Chiefs’ Council recorded 1,032 suspected needle spiking incidents between September 2021 and December 2022 (Home Affairs Committee, 2022). In France, the Netherlands, Germany, and various other countries, this trend has persisted (Blandamer et al., 2023; Koppen et al., 2023). To date, none of the suspected cases have been definitively verified, neither in police investigations nor the very few medical/toxicological case reports concerning needle spiking (Koppen et al., 2023). Further, no study so far has directly compared subjective experiences, risk perceptions, and fears of drink versus needle spiking.
It can be assumed that the salience of the topic, biases in its perceived likelihood, and fear processes are connected to the high rates of unconfirmed spiking suspicions (Campion-Vincent, 2022). Theoretical frameworks (Figure 1) and empirical findings on fear of crime suggest that demographic variables, such as gender, may be directly and indirectly related to perceived risk and fear of spiking (Gainey et al., 2011). Specifically, individuals who perceive themselves as more vulnerable to spiking (e.g., females) regard spiking as likelier and experience more fear as a result (Brooks, 2014; Gainey et al., 2011). Evidence on the link between experiences as a victim and fear of crime is sparse and inconsistent but it can be assumed that having been (allegedly) subjected to a spiking incident in the past is associated with a higher perceived risk and fear of spiking (Gainey et al., 2011). Further, indirect information about crime from media coverage and word of mouth seemed to influence risk perception and fear in previous studies (Chiricos et al., 2000; Gainey et al., 2011; Weiss & Colyer, 2010). These effects may also be applicable to spiking. However, research that specifically examines the connections between sociodemographic characteristics, previous alleged spiking incidents, subjective risk perception, and fear associated with drink versus needle spiking is currently absent. The present study addresses this research gap. In addition, the study aimed to investigate associations of depressive and anxiety symptoms with spiking-related experiences, perceptions, and fears, as psychological distress could be a consequence of alleged spiking incidents as well as a pre-existing vulnerability factor (Anderson et al., 2017). Adapted and expanded theoretical model of fear of crime hypothesizing factors associated with the perceived risk and fear of spiking (modified from Gainey et al., 2011).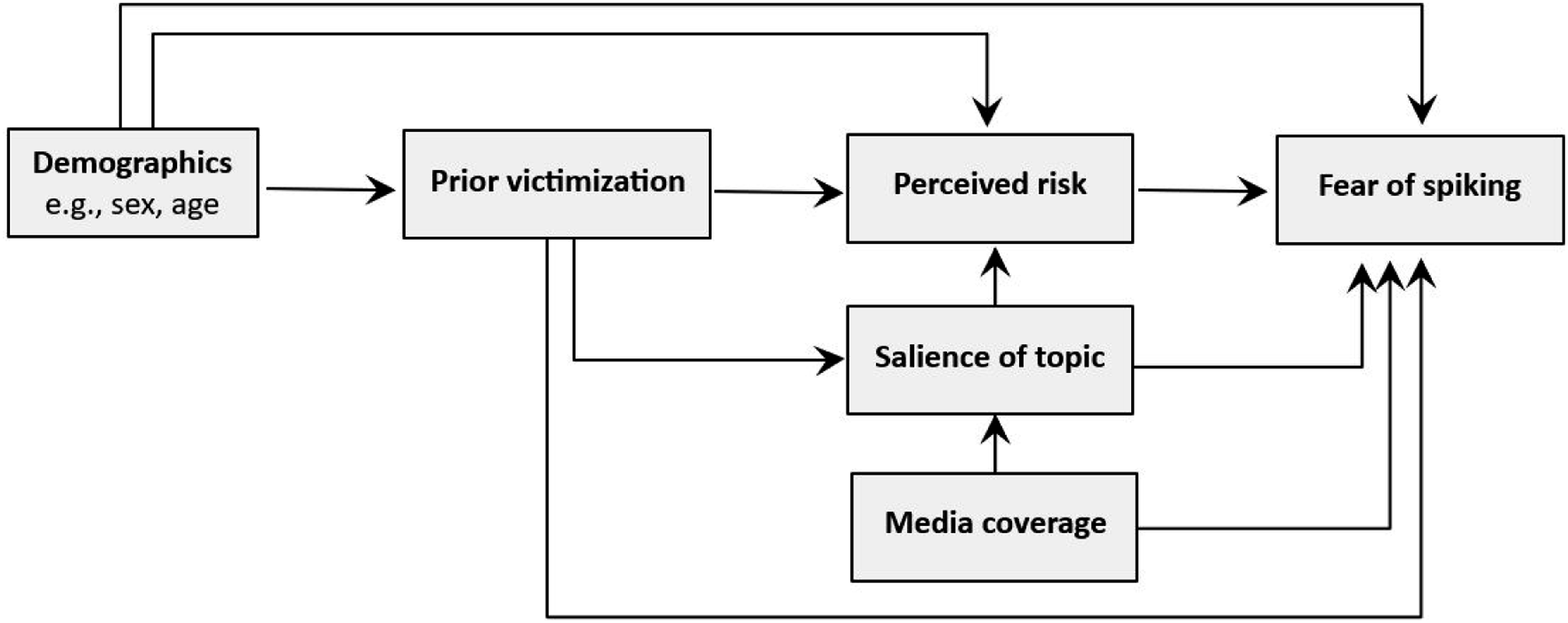
Methods
Study Design
The data were collected within the framework of a larger cross-sectional research project focusing on the perception, consumption, and risk mitigation of GHB/GBL. The survey was conducted online via the platform SoSci Survey from November 19, 2022 to January 16, 2023.
Participants were recruited via non-probability convenience sampling; primarily through social media channels (Instagram, Facebook) of institutions, organizations, and associations within the Berlin nightlife scene, as well as prevention and counselling services in Berlin. The inclusion criteria were a minimum age of 18 years and sufficient language proficiency to complete the questionnaire in German or English. Written informed consent was obtained from all participants before participation. Monetary or material incentives were not offered in exchange for participation. The study was granted ethical approval by the Ethics Committee of Charité – Universitätsmedizin Berlin and pre-registered at Deutsches Register Klinischer Studien (https://drks.de/search/de/trial/DRKS00030608).
The questionnaire was accessed 4155 times; 2668 individuals completed (at least distinct parts of) the questionnaire and a final sample of 1916 participants completed the items regarding drink and needle spiking.
Assessment
The online survey captured sociodemographic information (e.g., gender, age). Past suspicions of drink or needle spiking occurrences among themselves or their social contacts were assessed with two dichotomous items (yes/no). The perceived likelihood of becoming subjected to drink or needle spiking, respectively, was rated on a 5-point Likert-scale from 1 (very unlikely) to 5 (very likely). The fear of becoming a victim of drink or needle spiking, respectively, was also answered on a 5-point Likert-scale from 1 (very low) to 5 (very high).
The two subscales of the well-established Patient Health Questionnaire-4 (PHQ-4, (Löwe et al., 2010) were used to assess the dimensional presence of core symptoms of depression (PHQ-2) and generalized anxiety (GAD-2). The PHQ-2 and GAD-2 subscales comprise two items each, which rate the intensity of the symptoms on 4-point Likert-scales ranging from 0 (not at all) to 3 (nearly every day). A subscale sum score of ≥3, and a total score of ≥6, are indicative of high symptom severity and are considered alarming.
Analyses
Statistical analyses were performed with IBM SPSS Statistics Version 29. The significance level was set at .05 (two-tailed). Descriptive statistics were utilized to examine the prevalence of spiking occurrences and the levels of perceived likelihood and fear of spiking; Odds Ratios were calculated to quantify gender-based differences in the rates of spiking incidents. ANOVAs were used to analyze differences in perceived likelihood and fear based on spiking modalities (drink vs. needle), gender, sexual orientation, and past suspicion of spiking. The association of perceived likelihood and fear with age were tested with Pearson’s correlations. ANOVAs, controlling for age and gender, were carried out to determine differences in mental strain based on past suspicion of having been subjected to spiking. Partial Pearson’s correlations (controlling for age, gender, and past suspicion of spiking) were used to explore the relationship of depressive and anxiety symptoms with perceived likelihood and fear of spiking.
Results
Sample Characteristics
Of the final sample of N = 1916 individuals, 48.7% (n = 933) reported identifying as male, 43.5% (n = 833) as female, 5.3% (n = 101) as diverse, and 1.8% (n = 34) as other (e.g., non-binary, agender); 0.8% (n = 15) of participants did not indicate their gender. The mean age was 29.23 years (SD = 6.82; range: 18 – 62). About half (51.3%, n = 983) of the sample was employed, 14.9% (n = 286) self-employed, 4.6% (n = 88) unemployed/work-seeking, 21.7% (n = 416) enrolled at university, 5.2% (n = 99) in vocational training, and 1.3% (n = 24) in school. Sexual orientation was heterosexual for 45.1% (n = 865), homosexual for 27.0% (n = 518), bisexual for 21.3% (n = 408), and other for 5.4% (n = 103) (e.g., pansexual, asexual).
Subjective Experiences With Spiking
Figure 2 depicts the percentage of respondents who suspected that they or others in their social environment had been previously subjected to drink or needle spiking. About half (53.3%, n = 1021) of the participants reported that someone in their social environment had been subjected to drink spiking, almost a fifth (18.2%, n = 348) indicated knowing someone who was affected by needle spiking, but only a fraction subsequently underwent a medical or police examination. Almost a quarter (22.2%, n = 425) of the sample reported that drink spiking happened to them, but again only a negligible fraction sought medical examination (2.7%) or initiated police investigation (0.9%) concerning this matter. Only a few individuals (1.3%, n = 25) suspected themselves to have been victims of needle spiking and even fewer have had this inspected by medicals and/or the police. Percentage of participants who expressed suspicion of having been a victim of spiking themselves or knowing someone in their social environment who had experienced spiking.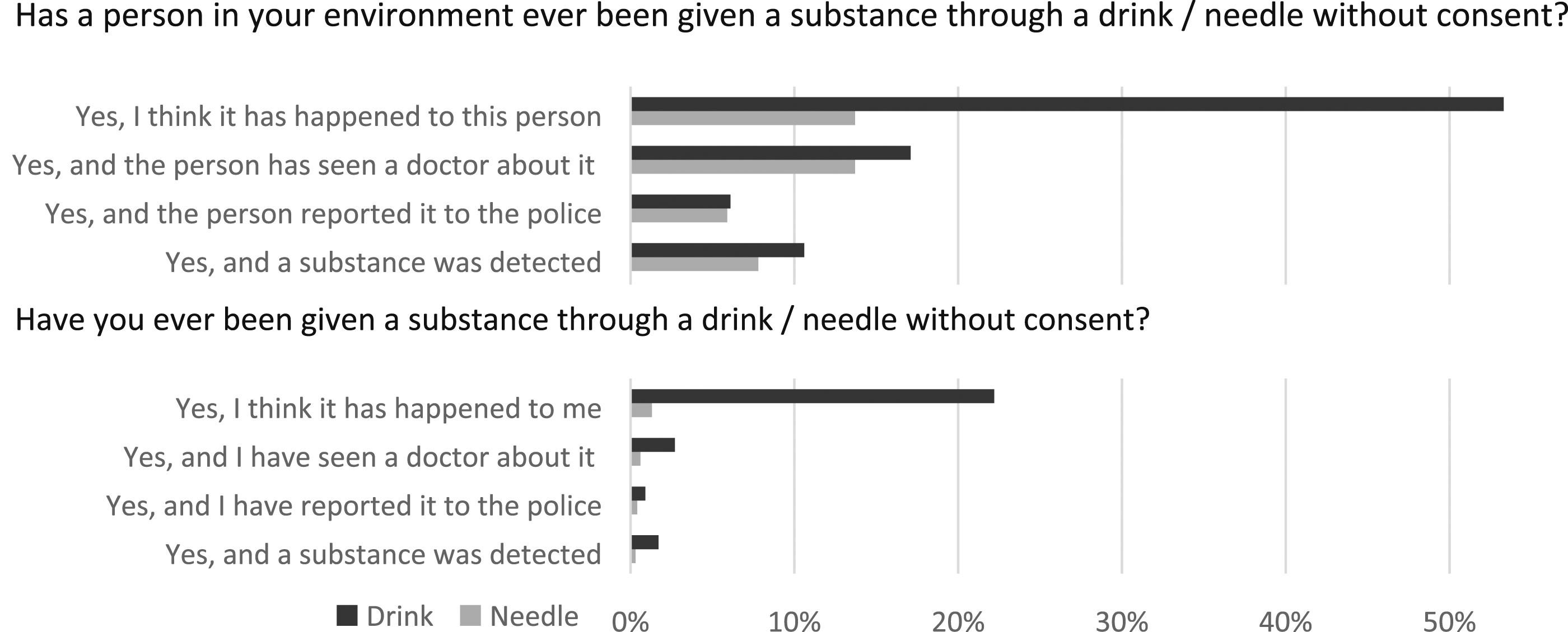
Participants identifying as females most frequently reported the suspicion of having experienced drink spiking (26.5% of female participants), followed by diverse (25.7%), others (23.5%), and males (18.1%). The Odds Ratio (OR) between females and males was 1.63 (95% confidence interval (95%-CI): 1.3, 2.05; p < .001). Regarding needle spiking, again the percentage in females was higher than in males (2.2% vs. .6%; OR = 3.41, 95%-CI: 1.35, 8.64); in the smaller subsamples of individuals identifying as diverse or other, no one reported a needle spiking suspicion.
Perceived Likelihood and Fear of Spiking
Figure 3 and Table 1 present the perceived likelihood and fear of becoming subjected to drink spiking (for the total sample and, in Table 1, divided by gender, sexual orientation, and previous presumptive experience with drink spiking). The likelihood of drink spiking was rated substantially higher than the likelihood of needle spiking (repeated measures ANOVA: F (1,1804) = 454.702, p < .001; η2 = .201), whereas fear of drink over needle spiking was higher with a very small effect size (F (1,1829) = 10.146, p < .001; η2 = .006). Perceived likelihood and fear of a spiking incident in the future. Perceived Likelihood and Fear of Becoming Subjected to Spiking – As a Function of Age, Gender, Sexual Orientation, Self-Reported Suspicion of Having Been a Victim of Drink Spiking in the Past, and Mental Strain. Note. The perceived likelihood of becoming subjected to spiking was rated on a 5-point Likert-scale from 1 (very unlikely) to 5 (very likely). The fear of becoming subjected to spiking was rated on a 5-point Likert-scale from 1 (very low) to 5 (very high). For categorial data, between-subjects ANOVAs were conducted; for quantitative data, (partial) Pearson’s correlations were calculated (controlling for age, gender, and past suspicion of spiking when analyzing correlations with mental strain). Bold formatting to visually distinguish M & SD from the median.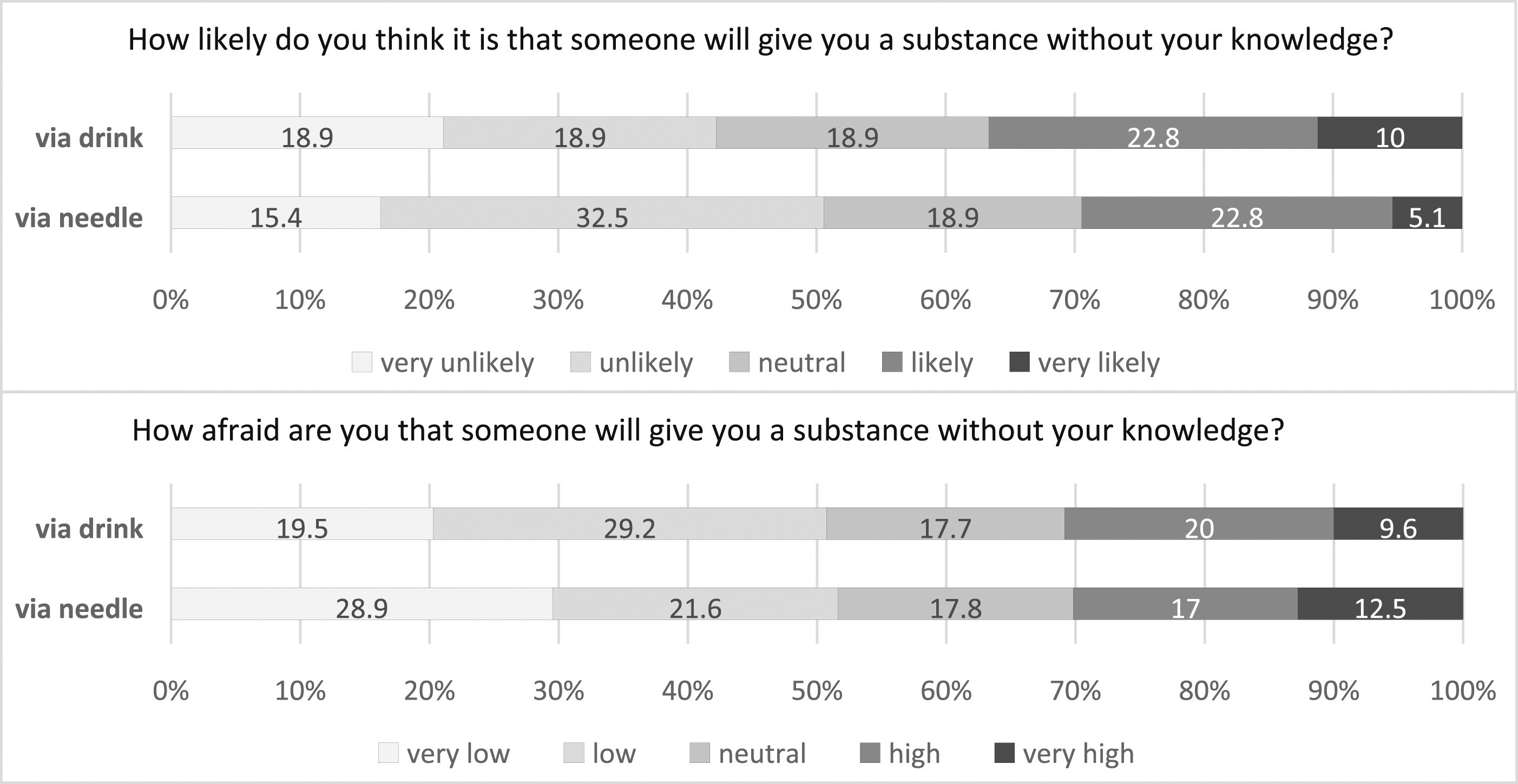
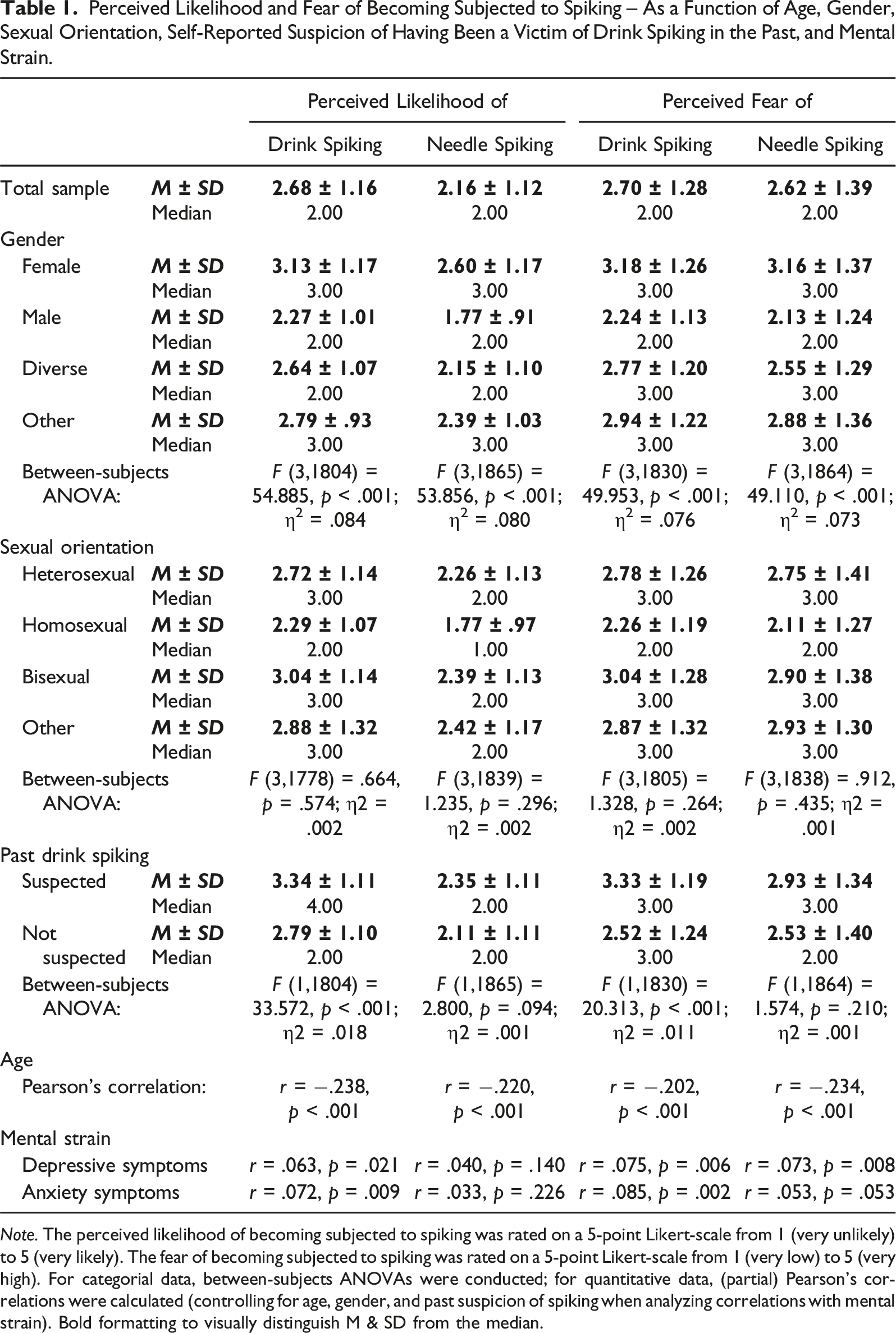
Higher age was associated with a lower perceived likelihood and fear of spiking (see Table 1). Significant gender differences were observed in the perceived likelihood and fear of becoming subjected to drink and needle spiking, respectively. On average, females reported the highest perceived likelihood and fear, males the lowest.
The differences in the perceived likelihood and fear of spiking among individuals of different sexual orientations (see Table 1) might partly be accounted for by unequal gender distributions. For instance, the majority of homosexual participants indicated male gender (84.7% male, 6.9% female, 7.5% diverse, 0.8% other), while the majority of bisexual participants was female (68.1% female, 20.6% male, 8.3% diverse, 2.9% other). Upon controlling for the effect of gender, none of the mean differences between sexual orientations were significant.
Individuals with assumed past exposure to drink spiking rated the likelihood of drink spiking, but not needle spiking, significantly higher than those unexposed (see Table 1). Participants’ fear of spiking followed a similar pattern.
Mental Strain and Spiking
Symptoms of depression were higher in individuals who reported alleged drink spiking in the past (M = 1.99, SD = 1.68) compared to those who did not (M = 1.68, SD = 1.53) (between subjects ANOVA controlled for age and gender: F (3,1391) = 8.412, p = .004; η2 = .006). A similar finding occurred with regard to symptoms of generalized anxiety: M = 2.00 (SD = 1.72) versus M = 1.56 (SD = 1.52), F (3,1391) = 17.534, p < .001; η2 = .012.
Higher symptoms of depression were associated with a higher perceived likelihood of drink (r = .063, p = .021) but not needle spiking (r = .040, p = .140) as well as a more pronounced fear of becoming subjected to drink (r = .075, p = .006) and needle spiking (r = .073, p = .008). A corresponding pattern of results was evident for anxiety symptoms (see Table 1).
Discussion
Summary and Interpretation of the Results
The study investigated alleged victimization, perceived likelihood, and fear of drink versus needle spiking, and its associations with mental strain. Results indicate that a substantial percentage of the sample suspected having been subjected to drink spiking themselves (22%) or knowing an alleged victim (53%), but only a negligible fraction sought medical attention or initiated police investigation. This corresponds to the finding of Hughes et al. (2007) that only 14% of the patients presenting to an emergency department in the UK with alleged drink spiking informed the police about their drink spiking suspicion. Thus, the barriers to medical examination seem very high and those to police investigation even higher. Reasons for reluctance to report alleged incidents may include a perceived or actual difficulty in accessing appropriate services, feared harsh treatment in emergency departments and police stations, stigmatization, shame, guilt, and blurred memories (Busardò et al., 2019; Dinis-Oliveira & Magalhães, 2013). Therefore, efforts should be aspired to reduce the barriers in a transdisciplinary manner. For example, by providing services specialized in spiking suspicions and being particularly sensitive with potentially affected individuals (Blandamer et al., 2023). Significantly fewer participants reported being subjected to needle spiking compared to drink spiking. However, the percentage of 1% (and 18% reportedly knowing an alleged victim of needle spiking) is still remarkably high, considering that not a single case of needle spiking has been undoubtedly proven so far (and taking into account that the subcutaneous or intramuscular injection of an effective dose of a sedative substance is unlikely to happen completely unnoticed). That actual medical or police evidence is not always decisive with regard to the conviction of having been spiked, was previously implied by findings of Hughes et al. (2007): Irrespective of the negative toxicology results, 35% of the individuals still believed that they had been subjected to drink spiking. Commonly expressed reasons are the limited detectability of certain substances due to rapid metabolization and the presumed involvement of unknown/untested substances (Busardò et al., 2019; Morgillo et al., 2023). These arguments cannot be entirely dismissed. However, it can be assumed that toxicological studies with a narrow time window (e.g., max. 12 hours) between alleged substance intake and sample extraction, and a comprehensive composition of toxicological tests, have very high detection rates (Bühler et al., 2019; Greene et al., 2007; Quigley et al., 2009).
Females reported the suspicion of having experienced drink and needle spiking significantly more frequently than males. This is congruent with findings from previous studies (Anderson et al., 2019; Busardò et al., 2019; Fiorentin & Logan, 2019). For example, in an observational study of 6064 university students in the US, 10% of females and 4% of males reported having been drink spiked (Swan et al., 2017). Outcomes after (alleged) drink spiking also differed with female victims experiencing more negative outcomes such as sexual assault and blacking out, while male victims were more likely to have been physically hurt by others (Swan et al., 2017). In our study, females reported the highest levels of perceived likelihood and fear of drink and needle spiking, compared to other genders. This is in line with the assumption that (subjective) vulnerability is associated with higher risk perception and fear (Figure 1). Age also appears to play a part, with younger individuals rating risk and fear of spiking higher. Beyond actual differences in the risk of becoming subjected to spiking, this might be attributed to a tendency of younger individuals to consume more media coverage on this topic, leading to a stronger salience of this subjective threat. It should be noted, nonetheless, that the magnitude of the differences and correlations, albeit statistically significant, was relatively small.
The fear of drink versus needle spiking was similar, whereas the perceived likelihood of drink spiking was rated higher than needle spiking. About a third of the sample thought it likely or very likely they would become subject to drink spiking (33.8%), and more than a quarter thought the same for needle spiking (27.9%). Considering the very small percentage of actually confirmed drink spiking cases (Greene et al., 2007; Hughes et al., 2007; Quigley et al., 2009) and no confirmed case of needle spiking (Koppen et al., 2023), this subjectively perceived likelihood of spiking, particularly of needle spiking, seems to be highly overestimated (Campion-Vincent, 2022; Colyer & Weiss, 2018; Weiss & Colyer, 2010). This may be attributable to the extensive media coverage and public debate, particularly with a focus on needle spiking, resulting in increased salience of the perceived threat (Figure 1) and the emergence of processes of social panic (Campion-Vincent, 2022; Sheard, 2011). High or very high fear of drink (29.5%) and needle spiking (29.6%) was very prevalent in the study sample, which emphasizes the need to address these concerns with appropriate measures (e.g., taking this aspect of distorted risk perception into account in information campaigns by counselling services, feeding this information on social media channels that relate to nightlife etc.).
Individuals who reported to have putatively been victims of drink spiking rated the likelihood and fear of drink and needle spiking, respectively, significantly higher than those who did not suspect they had been previously affected. Further, allegedly affected individuals reported higher symptoms of depression and generalized anxiety. In addition, a higher perceived likelihood and fear of becoming subjected to drink and needle spiking was associated with more symptoms of depression and anxiety. This underscores the importance of taking mental health into consideration in the context of (alleged) spiking incidents. Psychological distress may arise as a consequence of such incidents, which could be regarded as traumatic or distressing events. At the same time, higher state anxiety, rumination, and riskier substance use may be linked to a higher (perceived) probability and fear of spiking. In a study by Anderson et al. (2019), alleged victims of spiking (in the context of DFSA) exhibited a four times higher prevalence of self-reported premorbid depression (12-month prevalence: 21%) and a two times higher prevalence of drug and alcohol abuse (10%) than the general population (Anderson et al., 2019).
It seems to be relevant to consider voluntary substance use as a vulnerability factor for actual spiking incidents as well as unconfirmed suspicions. The vast majority of alleged victims voluntarily consumed psychoactive substances; alcohol emerged as the most commonly consumed substance, whereas concomitant use of alcohol, prescription drugs, and illicit drugs was also frequently reported (Anderson et al., 2017, 2019; Greene et al., 2007; Hagemann et al., 2013; Hughes et al., 2007; Quigley et al., 2009). In addition, there appears to be a tendency among potential victims to underreport drug use (Juhascik et al., 2007), possibly due to memory errors, response biases (such as social desirability), and concerns about stigmatization. In fact, victim-blaming occurs more frequently in DFSA-cases with intentional substance use (Clough, 2019; Girard & Senn, 2008; Thompson, 2021). This emphasizes the importance of reducing stigma and provide adequate care for potential victims. Further, preventive efforts often solely focus on the behavior of potentially affected individuals (e.g., watching drinks, using protective devices), which is problematic because it places the responsibility on the potential victims and, additionally, self-administered devices to detect spiked drinks often fail in providing valid and reliable results (Quest & Horsley, 2007). As a side effect of prevention messages and devices it should be noted that their amplified presence in specific environments (e.g., clubs) may engender a perception of spiking as a ubiquitous or selectively prevalent phenomenon (Sheard, 2011; Taylor et al., 2004). In addition, extensive campaigns concerning spiking may potentially deflect attention and resources from other (more prevalent) risks, such as harmful excessive alcohol consumption.
Preventive efforts should also educate about the effects of alcohol and other substances, as well as various physiological and psychological processes. For example, hypoglycemia, dehydration, or sleep deprivation can trigger physiological sensations similar to those of being spiked with a sedative substance (Zucker et al., 2022). Additionally, even if individuals are familiar with specific substances, they do not always have the same effect and can sometimes trigger unexpected symptoms. Moreover, unclear somatic sensations can exacerbate into severe panic symptoms (which again correspond to possible spiking symptoms), especially when combined with anxiety processes - for example, due to high salience and social panic regarding spiking. Notably, the surge in suspected needle spiking incidents coincided with the reopening of nightlife venues in different countries (Blandamer et al., 2023); a prolonged hiatus and pandemic-related strains may have fostered a sense of unfamiliarity or estrangement within the party context, leading individuals to be more susceptible to misperceptions.
While previous awareness campaigns focused mainly on spiking in public spaces (e.g., bars and clubs) and anonymous perpetrators, it is important not to lose sight of private settings. In an Australian study, half of the examined alleged DFSA-cases occurred in private residences, and in half of the incidents, the perpetrators were known to the complainant (Anderson et al., 2019). This is not only pertinent in the context of DFSA, but also spiking incidents with other motives, such as enhancing social enjoyment among friends during a home-based gathering (Swan et al., 2017). Even though participants in our study were primarily recruited from nightlife-associated settings, it is plausible that some of the suspected spiking incidents have occurred in private settings or the context of intimate encounters (as the questionnaire was not specifically about spiking in nightlife-related situations). Future research should endeavor to differentiate more clearly between different contexts.
In the future, preventive attention should also be extended to (potential) perpetrators and their motives (Costello & Blyth, 2004). Yet, no empirical data on needle spiking addresses this and only scattered findings exist regarding drink spiking. In a survey by Swan et al. (2017), 1.4% (83 students; 1.2% of female students and 1.8% of male students) indicated that they or someone they know had purposefully drink-spiked someone. Participants' views on motives for drink spiking varied by gender, with women being more likely to assume sex or sexual assault as a motive, while men were more likely to mention having fun (Swan et al., 2017). Other motives reported or assumed by participants included getting others more intoxicated or relaxed.
Limitations
Our sample was recruited through convenience sampling, which may limit its representativeness. For instance, individuals with an interest in the topic and those more proficient with online media may have been more likely to participate. All outcome measures were obtained through self-report, which can be susceptible to deliberate as well as unaware biases such as retrospective memory and response biases. So as not to overwhelm participants and minimize dropout rates, we used primarily brief instruments in our investigation. This may have reduced the overall conclusiveness and reliability of our results compared to more extensive instruments, and the complex topic of spiking may not have been encompassed in all relevant dimensions. Future research should strive to comprehensively assess spiking in more detail, potentially incorporating alternative modalities of spiking, such as intentional mislabelling of substances, and investigate a broader range of related variables. Whenever possible, subjective self-report information should be complemented with objective data (e.g., toxicological findings). Due to the cross-sectional observational study design, the effects of unconsidered third variables cannot be ruled out and no causal conclusions can be drawn. Thus, future longitudinal studies as well as randomized-controlled trials, if feasible, are desirable.
Conclusions
In summary, our findings suggest that the subjective threat of drink and needle spiking is high. Considering toxicological findings and police investigations, the reported prevalence and perceived likelihood of spiking seem highly overestimated – nevertheless, every allegedly affected individual must be taken seriously and treated sensitively and adaptively. The high perceived prevalence and subjective likelihood in combination with associated fear, anxiety, and depressive symptoms emphasizes the importance of adequately addressing the issue of spiking and associated fears in the society, explaining reasons for unconfirmed spiking-like symptoms, and improving awareness, prevention, and medical-toxicological as well as police-related investigation efforts.
Footnotes
Acknowledgments
We would like to thank Clubcommission e.V. Berlin, SONAR – Safer Nightlife Berlin, and Notdienst e.V. Berlin for the support in conceptualization and data collection. Further, we thank Lucie Schröder, Grace Viljoen, and Dr Helene Naegele for their support in designing and preparing the survey.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Felix Betzler received honoraria (consulting, lectures) from Takeda Pharmaceutical. All remaining authors declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Research Transparency Statement
The authors are willing to share their data, analytics methods, and study materials with other researchers. The material will be available upon request.
Design and Analysis Transparency
The STROBE checklist for observational studies served as reporting guideline for the study.