
Abstract
The overall aim of the present study is to examine the utility of the DSM OUD Checklist and the NM-ASSIST screening tools to identify symptoms consistent with OUD among incarcerated women in county jails. This study contributes to the existing literature because research on screening and assessment approaches for incarcerated women has been limited. The focus of the current study is to describe the screening procedures and study recruitment for a larger parent study focused on increasing treatment linkages. Study findings indicate a positive correlation between indicators of OUD using the two screening tools, as well as a high degree of correlation between street opioid misuse and other high-risk drug indicators (overdose and injection practices). These findings underscore the importance of outreach, screening, and intervention in real-world settings, including jails, in order to increase access to OUD treatment among this vulnerable sample of women.
Introduction
Recent U.S. data indicate that the number of incarcerated women in 2020 was nearly five times the number of incarcerated women in 1980 (The Sentencing Project, 2022). From 1980 to 2020, the number of incarcerated women increased by about 475%, a rate nearly twice that of male incarceration. The high rate of incarceration for women is largely driven by drug-related charges, which have increased 216% for women in the past 35 years (Herring, 2020). This trend is consistent in Kentucky which ranks sixth in the nation for the highest rate of female incarceration (The Sentencing Project, 2022), primarily attributed to the opioid epidemic (Cheves, 2017).
Kentucky is an epicenter of the opioid crisis, and despite a number of policy changes in the last decade to curtail illicit distribution and misuse of prescription opioids, nearly 2000 Kentuckians died of an overdose in 2020 – a 49% increase over 2019 (Kentucky Office of Drug Control Policy [KYODCP], 2021). The drug overdose death rate in Kentucky is 57% higher than the national average (National Center for Drug Abuse Statistics [NCDAS], 2022), and death rates for Kentucky women (28.1%) are also considerably higher than the national average (14.4%; Akers & Ward, 2018). Amid the opioid crisis, the criminal justice system, both in Kentucky and nationally, has experienced tremendous growth and depleted resources due to opioid-related arrests (Caulkins, Gould, Pardo, Reuter, & Stein, 2020). Justice-involved individuals have significantly higher rates of opioid use disorder (OUD) than individuals in the general population (8.5% vs. .8%; Substance Abuse and Mental Health Services Administration [SAMHSA], 2017). One study found that the likelihood of justice system involvement increases along a continuum of opioid use severity (Winkelman, Chang, & Binswanger, 2018). Incarceration significantly increases the risk for opioid overdose deaths due to loss of tolerance, limited access to medications to treat OUD, and disruptions to social support networks (Joudrey et al., 2019; Sinkman & Dorchak, 2022).
Considering these risks for justice-involved individuals in general, it is critical to focus research efforts on OUD screening among incarcerated women. The opioid overdose death rate among women increased 492% from 1999 (2.6/100,000) to 2017 (15.5/100,000; VanHouten, Rudd, Ballesteros, & Mack, 2019). During this time, the most dramatic increases in opioid overdose deaths among women were attributed to synthetic opioids (1643% increase), heroin (915% increase), and prescription opioids (485% increase). Data from national samples have indicated that a greater percentage of women demonstrate a need for opioid treatment compared to men, yet fewer receive it (Martin, Parlier-Ahmad, Beck, Scialli, & Terplan, 2021). Women have been significantly affected by the opioid crisis due in large part to self-medication, often related to experiences of chronic pain (Goetz, Becker, & Mazure, 2021), physician prescribing practices and self-medication (Mazure & Fiellin, 2018; McHugh et al., 2013), as well as a faster trajectory from opioid exposure to the development of OUD (Greenfield, Back, Lawson, & Brady, 2010; Kay, Taylor, Barthwell, Wichelecki, & Leopold, 2010).
U.S. jail data indicate that 72% of incarcerated women met diagnostic criteria for substance use disorder (compared to 62% of men), and 60% reported active drug use in the month before arrest (compared to 54% of men; Bronson, Stroop, Zimmer, & Berzofsky, 2017). One study found that 97% of women randomly selected from three Kentucky jails reported illicit drug use, primarily opioids, in the year before incarceration (Staton et al., 2018). Treatment opportunities (including medications to treat opioid use disorder) are limited in correctional settings, particularly jails, despite the growing evidence base in recent years on sustaining recovery (Moore et al., 2019) and reducing the risk of overdose (Malta et al., 2019) following release from custody. Yet, women with OUD often attain and sustain sobriety during periods of incarceration but, in the absence of effective treatment, there is substantial risk for relapse and overdose during community re-entry. Thus, there is significant need to increase research on screening and assessment for OUD among incarcerated women in order to more effectively target treatment during incarceration, as well as during the transition to the community.
OUD treatment during re-entry is critical considering the risk for relapse and overdose following a long period of abstinence during incarceration (Binswanger, Blatchford, Mueller, & Stern, 2013). In addition to overdose risk, women with OUD experience a number of health and social challenges including high-risk pregnancies and fertility complications (Corsi & Murphy, 2021; Pentecost, Latendresse, & Smid, 2021), mental health issues including depression and PTSD (McHugh et al., 2013), and higher rates of interpersonal conflicts and intimate partner violence (Gilbert, El-Bassel, Chang, Wu, & Roy, 2012; Smith, Homish, Leonard, & Cornelius, 2012; van Reekum et al., 2020). Women who inject opioids are disproportionately vulnerable to infectious disease transmission (including HIV) due to unprotected heterosexual contact with risky partners, impaired condom use judgement, lack of agency for negotiating safer sex behaviors with partners, and being in violent and abusive relationships (Wechsberg et al., 2015).
Despite significant health risks and unique vulnerabilities for women with OUD, screening and assessment approaches in jails have been limited. One recent study found that OUD screening was reported as part of standard intake procedures in less than half of prisons surveyed (Scott, Dennis, Grella, Mischel, & Carnevale, 2021). Research on the prevalence for OUD screening in jails is even more limited (Zaller, Donadeo, Coffey, Zielinski, & Brinkley-Rubinstein, 2019), with no clear evidence to suggest universal screening procedures are in place for OUD specifically nor SUD more generally. Jails are often managed at the local level (compared to prisons which are managed at the larger state level), which often may result in less resources for health and behavioral health care – such as OUD screening and medications. Considering the high rates of individuals with OUD in county jails and the risks associated with OUD relapse upon release, jails provide critical venues for screening and assessment of OUD and subsequent treatment linkage. Evidence-based screening approaches have been successful in other settings (such as health care settings and pharmacies) to identify individuals at high risk for OUD, which may have application within criminal justice settings. For example, the Alcohol Smoking Substance Involved Screening Test (ASSIST) was developed and validated by the World Health Organization ([WHO]; Humeniuk & Ali, 2006; WHO ASSIST Working Group, 2002) to detect substance use risk in health care settings, and further modified by the National Institute on Drug Abuse (NIDA) to separate specific categories of prescription/street opioids and stimulant use (NIDA modified-ASSIST [NM-ASSIST]; Pagliaro & Pagliaro, 2012). The NM-ASSIST takes 5–10 min to administer, yields a substance use severity score which can be indicative of intervention need (4+), and has been validated as an effective screening tool for substance use in criminal justice settings (Holmwood, Marriott, & Humeniuk, 2008; Staton et al., 2018; Wolff & Shi, 2015).
Another screening tool is the Diagnostic and Statistical Manual (DSM) of Mental Disorders-5 OUD Checklist (American Psychiatric Association [APA], 2013). The DSM OUD Checklist includes a list of 11 symptoms associated with opioid misuse in a 12 months period. The total number of reported symptoms is calculated, and severity is assessed along a continuum of endorsed symptoms ranging from mild, moderate, and severe (Centers for Disease Control and Prevention, 2021; SAMHSA, 2018) with a score of two or higher being consistent with the presence of an OUD. While used widely as a clinical tool, the DSM OUD Checklist has received less attention in the empirical research on OUD screening. One study found that the DSM OUD Checklist was a critical component of symptom tracking among buprenorphine patients in primary care (dela Cruz, Walker, Pipes, Wakhlu, & Trivedi, 2021). Another study reported the DSM OUD Checklist as part of a screening package for patient-centered opioid tapering in outpatient settings (You et al., 2021). To our knowledge, the DSM OUD Checklist has not been used as a screening tool in a justice setting.
The overall aim of the present study is to examine the utility of the DSM OUD Checklist and the NM-ASSIST screening tools to identify symptoms consistent with OUD among incarcerated women in county jails. This study contributes to the literature because research on screening and assessment approaches for incarcerated women has been limited. The focus of the current study is to describe the screening procedures and study recruitment for a larger parent study focused on increasing treatment linkages. Specific study objectives are to: (1) profile opioid use and self-reported criteria associated with OUD using the two screening tools; (2) examine bivariate relationships between OUD screening criteria, high risk drug use indicators (non-fatal overdose, injection drug use), and criminal justice involvement; and (3) examine high-risk drug use indicators and criminal justice involvement as independent correlates of OUD screening criteria among this sample of incarcerated women.
Methods
Overview
The current study focuses on data collected during the screening process and baseline interviews for a larger parent project funded under the NIH/NIDA Justice Community Opioid Innovation Network (JCOIN, UG1DA050069; Staton et al., 2021) between December 2020 and June 2022. This paper describes the overall OUD screening process, which was used as a critical factor for larger study eligibility. Women who were eligible for the study also completed a more detailed baseline interview, allowing for analysis to also examine other high-risk drug use factors and criminal history as related to criteria consistent with OUD.
Participants and Procedure
We used random sampling to recruit adult (aged 18 and older) incarcerated women with a history of symptoms consistent with OUD who were not currently in treatment in order to engage them in a larger trial focused on intervention linkages to treatment. Study recruitment took place on targeted days in each of five jails, all located in non-urban areas of Kentucky. Each of these jails had existing substance use disorder treatment programs on site, but only for men. Male participants in those programs who met OUD criteria had access to extended-release naltrexone (the only form of medications for OUD provided) through the contracted medical provider at the jail prior to their release. These jails were selected for inclusion in the study because they had the administrative and medical infrastructure for treatment, but were not currently providing services for women. In fact, OUD screening for women was not standard practice in any of the facilities. The daily female population at the five facilities ranged from 40 to 125, and on average women accounted for about 20% of the total inmate population in these jails. The broader parent study is focused on increasing access to treatment through linkages to providers using telehealth prior to release. The current analysis focuses only on the screening protocol and study recruitment during this phase of the trial.
Recruitment procedures were initiated by the study director who obtained a list of women housed at each jail on the day of study recruitment. The list was provided either by the jail staff or downloaded from the jail’s online tracking system, depending on the facility. We included potential participants in the sampling frame if they had an anticipated release date from the jail within 7–60 days. Recognizing that release dates may not always be accurate (especially for women serving time for county charges), we verified dates with the jail records, as well as included in self-report screening measures. While not relevant for the present analysis, release dates were critical for re-entry intervention activities for the larger JCOIN study.
All women included in the initial sampling frame had an equal opportunity of being selected for study screening. For each screening session, approximately 10–20 women (depending on the size of the jail facility) were randomly selected from the full list of women using Research Randomizer (www.randomizer.org). Randomly selected women were invited to participate in a screening session with one female member of the research staff. Research staff lived in the local areas of the state close to the targeted jails. Study screening sessions were private with no jail staff or criminal justice representatives present. In March 2020, COVID-19 restrictions closed jails in Kentucky. The study team implemented screening and data collection procedures in December 2020 with collaborative planning between the research team and participating jails to best accommodate their COVID-19 protocols. This meant that face-to-face data collection occurred in person, behind a visitation glass, or via videoconference, depending on the jail’s protocol.
Each individual screening session included an overview of the study, informed consent procedures, and screening data collection. Interested participants (who confirmed opioid use during the year before incarceration and had anticipated release dates within 7–60 days) then responded to questions from the screening tools (NM-ASSIST opioid scales and DSM OUD Checklist). Screening procedures were used to determine study eligibility criteria which included: (1) endorsing symptoms consistent with OUD, including a score of 2 + on the DSM OUD Checklist or 4 + on the NM-ASSIST; (2) anticipated release date within 7–60 days to participate in a re-entry intervention; (3) no evidence of serious mental illness or hallucinations; (4) cognitively able to provide informed consent; and (5) willingness to participate. Women who met all study eligibility completed a face-to-face baseline interview for the larger JCOIN trial during the same session. All study procedures were approved by the University Institutional Review Board (IRB) and the Certificate of Confidentiality covered all procedures.
Measures
Demographics
Participants self-reported age (a continuous measure of self-reported age at the time of study screening), race (dichotomously coded as non-Hispanic White vs. other non-White, Hispanic, or multiracial categories), marital status (dichotomously coded as “never married” vs. other), education level (dichotomously coded as “received a high school diploma or GED” vs. not), and employment (percentage reporting any full-time or part-time work prior to incarceration vs. not working).
OUD Screening
Study screening included one initial question to assess opioid use, “Did you use any opioids in the year before you were incarcerated?” Women were informed that “opioids” includes prescription drugs like Lortab, Oxycodone or Percocet used other than as prescribed, or other opioids like heroin, fentanyl, codeine, or morphine. Women were reminded that this did not include Neurontin/gabapentin, or sedative or anti-anxiety medications like Xanax or Valium. Women who said “yes” to this question proceeded with completing the OUD screening tools.
Participants completed the NIDA-modified version of the Alcohol, Smoking and Substance Involvement Screening Test (NM-ASSIST; Pagliaro & Pagliaro, 2012) and the DSM OUD Checklist (APA, 2013) to assess for presence of OUD symptoms and the range of symptom severity. For the NM-ASSIST, the timeframe for data collection is typically focused on the past 3 months, but was modified for this study to the 3 months before incarceration. Participants also completed two scales of the NM-ASSIST for the current study screening including the Prescription Opioids scale and the Street Opioid (heroin, fentanyl) scale. Items are scored using categorical responses to assess frequency of the occurrence of problematic opioid use. Each scale is easily scored and yields a Substance Involvement (SI) score ranging from 0 to 39, with higher scores being indicative of higher degree of drug use severity (scores 4+ used for study eligibility indicate moderate need for intervention).
The DSM OUD Checklist includes 11 symptoms associated with problematic opioid use leading to clinically significant impairment or distress (American Psychiatric Association, 2013). The checklist is usually administered to assess a 12 month period of time, but was modified for the current study to the 12 months prior to incarceration. If women endorsed any criteria for that 12 month period of time, they reported whether it was present during the 30 days before incarceration. Endorsed criteria were summed for both the 12 months and the 30 days time frames, and an endorsement of 2–3 items was considered consistent with meeting criteria for mild OUD, 4–5 symptoms consistent with moderate OUD, and 6+ symptoms consistent with severe OUD.
High Risk Drug Use Indicators
To assess high risk drug use, women were asked to report if they had (ever and in the 90 days before jail) - (1) experienced a nonfatal overdose and (2) injected any illicit drugs.
History of Justice Involvement
Participants answered four self-reported continuous variables including the age of first arrest, number of lifetime arrests, number of lifetime convictions, and total number of lifetime months incarcerated to assess history of justice involvement.
Analytic Plan
Study recruitment for the trial is on-going. To meet the first study objective, we calculated descriptive statistics (e.g., means and proportions) for all variables of interest including any opioid use in the year prior to incarceration and scores on the NM-ASSIST and DSM OUD Checklist.
To meet the second study objective, we examined bivariate relationships between opioid screening tool scores (NM-ASSIST Street Opioid scale, NM-ASSIST Prescription Opioid scale, and DSM OUD Checklist 12-month as dependent variables) and independent variables including high risk drug use indicators (non-fatal overdose, injection drug use) and criminal justice involvement. Specifically, we used a series of t-tests when the independent variables were dichotomous (i.e., high risk drug use indicators). We used nonparametric correlational analysis (Spearman’s rho) to examine relationships between opioid screening tools and criminal justice system involvement variables, both continuous variables with skewed distributions.
Finally, we used a series of three multivariable ordinary least squares regression analyses to examine criminal justice factors and high-risk drug use as independent correlates of OUD screening criteria. Each model included a different OUD screening tool as the dependent variable of interest (i.e., NM-ASSIST Street Opioids, NM-ASSIST Prescription Opioids, and DSM OUD Checklist 12-month), and independent variables of interest included all criminal justice variables, 90-day pre-incarceration overdose, injection drug use (IDU), and sociodemographics. We also assessed for multicollinearity using variance inflation factors, none of which were greater than 2.13. Influential cases were examined by calculating Cook’s Distance, a measure which accounts for both leverage and standardized residuals of individual cases, with higher values (relative to sample size) indicating potential risk for inaccurate results in OLS regression. Removal of influential cases (i.e., Cook’s D values greater than 4/N) for each model resulted in an increased R2 value and were thus excluded from the final models. We used Huber-White robust standard errors to address heteroskedasticity of residuals. All analyses were conducted using Stata 15, with the exception of a post hoc power analysis, conducted using G*Power version 3.1.9.7 (Faul, Erdfelder, Lang, & Buchner, 2007). Using a significance criterion of α = .05, final linear regression sample size (n = 171), number of independent variables in the model (11), and model effect size (Cohen’s f 2 = .32), we calculated a power level of 99%, which is appropriately powered to conduct these preliminary interim analyses for screening procedures for the larger parent trial.
Results
Study recruitment for the trial is on-going. Since implementation of the study in December 2020, 556 women have been randomly selected from five Kentucky jails. As shown in Figure 1, 279 women did not participate (50.2%) because 200 were released between random selection and screening, 33 declined to participate, 26 were transferred to another facility between random selection and screening, and 20 had release dates outside the window of 7–60 days. Of the 277 (49.8%) women who did participate in screening, 76 (27.4%) did not meet study eligibility criteria, most commonly because they reported no opioid use in the year before incarceration (n = 61), reported opioid use but did not meet OUD screening criteria (n = 1), or anticipated a release date outside of the 7–60 days window (n = 14). One additional woman was released after screening eligible but prior to completing enrollment and a baseline interview. Thus, the current analysis focuses on the 200 women who met study eligibility criteria, including scores on the NM-ASSIST and/or DSM OUD Checklist, were enrolled in the study, and completed a baseline interview with research staff. Screening and baseline enrollment.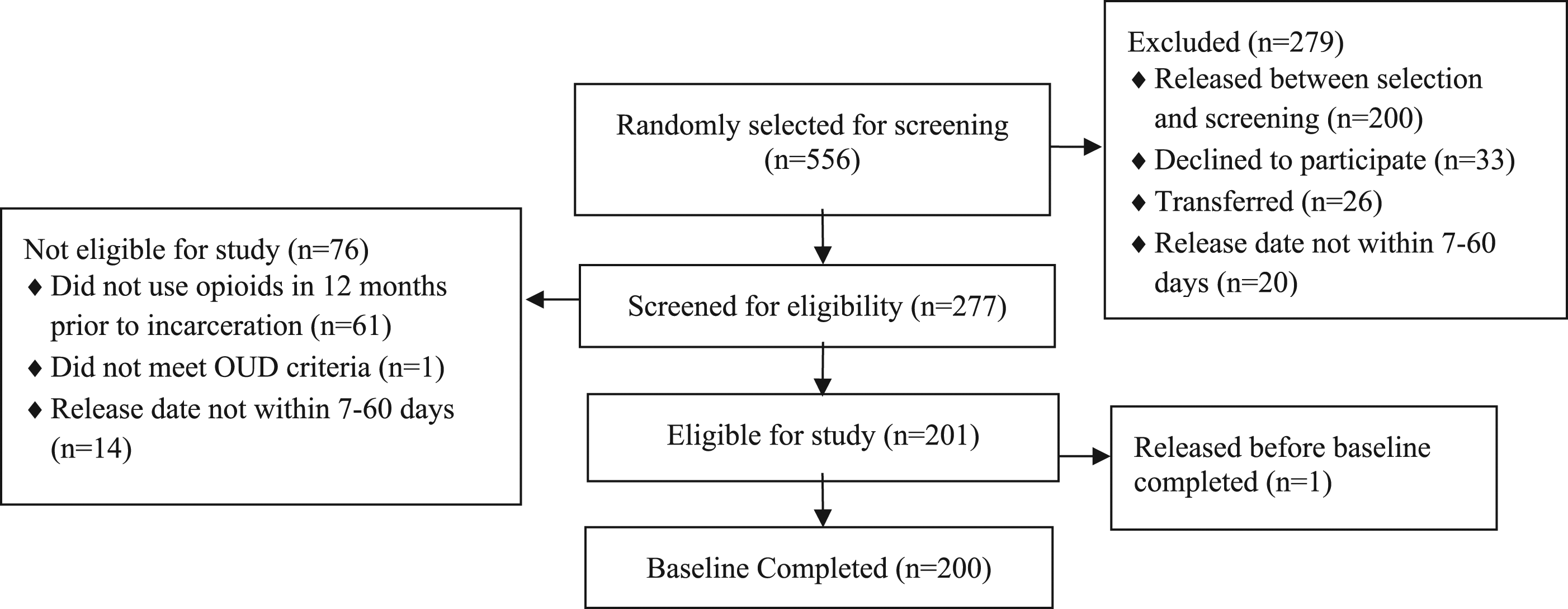
Demographics
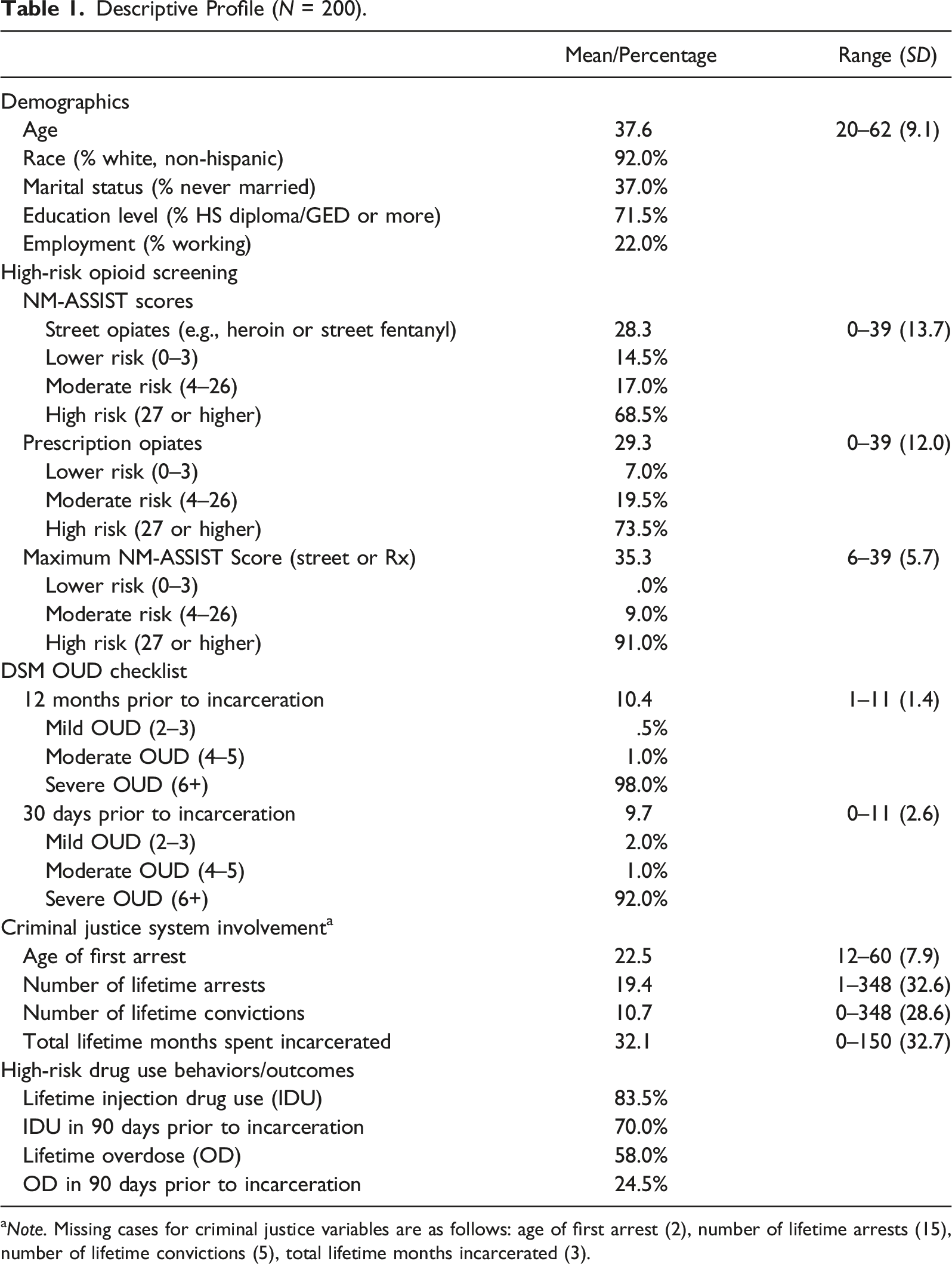
Descriptive Profile (N = 200).
aNote. Missing cases for criminal justice variables are as follows: age of first arrest (2), number of lifetime arrests (15), number of lifetime convictions (5), total lifetime months incarcerated (3).
Opioid Use and OUD Criteria
Of the women who were randomly selected and participated in the study screening session, 61 women (22% of the total 277) did not report any opioid use. However, only one woman reported using opioids in the 12 months before incarceration but did not meet OUD criteria on either the NM-ASSIST or DSM OUD Checklist. Findings on self-reported criteria associated with OUD among eligible women who enrolled in the study are presented in Table 1. Women reported an average score of 28.3 for street opioids (heroin, fentanyl; range 0–39, SD = 13.7) and the majority of women (68.5%) scored in the “high-risk” category of use (27+). In addition, women scored an average of 29.3 (range 0–39, SD = 12.0) for misuse of prescription opioids, with the majority (73.5%) scoring in the high-risk category. Because a number of women reported high scores on either/or the street and prescription opioid use categories (51.0% of women scored as “high-risk” for both), a maximum criteria score was also computed for use of either street or prescription opioids. As shown in Table 1, the average maximum NM-ASSIST score for either opioid category was 35.3 (range 6–39, SD = 5.7). With study entry criteria set at 4+ (indicative of a moderate need for substance use intervention), the minimum NM-ASSIST score reported by any participant for opioid use was a six, but 92.0% of study participants scored in the high-risk category for either or both NM-ASSIST scales.
Findings for the NM-ASSIST were consistent with the DSM OUD Checklist, in that women reported an average of 10.4 symptoms endorsed for the 12 months prior to incarceration (range 1–11, SD = 1.4), and the majority (98.0%) scoring in the severe OUD category. During the 30 days prior to incarceration, women scored an average of 9.7 symptoms (range 0–11, SD = 2.6), with 92.0% scoring in the high-risk category. Concordance between the DSM OUD Checklist and maximum NM-ASSIST score for either opioid category was high, with 99.5% of participants meeting the inclusion criteria threshold on both instruments (2+ on the DSM OUD Checklist, 4+ on either NM-ASSIST scale). Furthermore, 90.5% of participants scored both as “severe” on the DSM OUD Checklist and “high-risk” on either NM-ASSIST scale, the highest categories for each instrument.
Women reported an average age of first arrest of 22.5 (range 12–60, SD = 7.9). They also reported being arrested an average of 19.4 times (range 1–348, SD = 32.6), with 10.7 convictions (range 0–348, SD = 28.6), and 32.1 total lifetime months spent incarcerated (range 0–150, SD = 32.7). The majority of women reported lifetime drug injection (83.5%), as well as recent injection during the 90 days prior to incarceration (70.0%). Lastly, although more than half of women reported a lifetime non-fatal overdose (58.0%), about a quarter (24.5%) had experienced an overdose in the 90 days before jail.
Factors Associated With OUD Screening Criteria
Correlation Matrix of Opioid Screening Tools and Criminal Justice Involvement (N = 200).
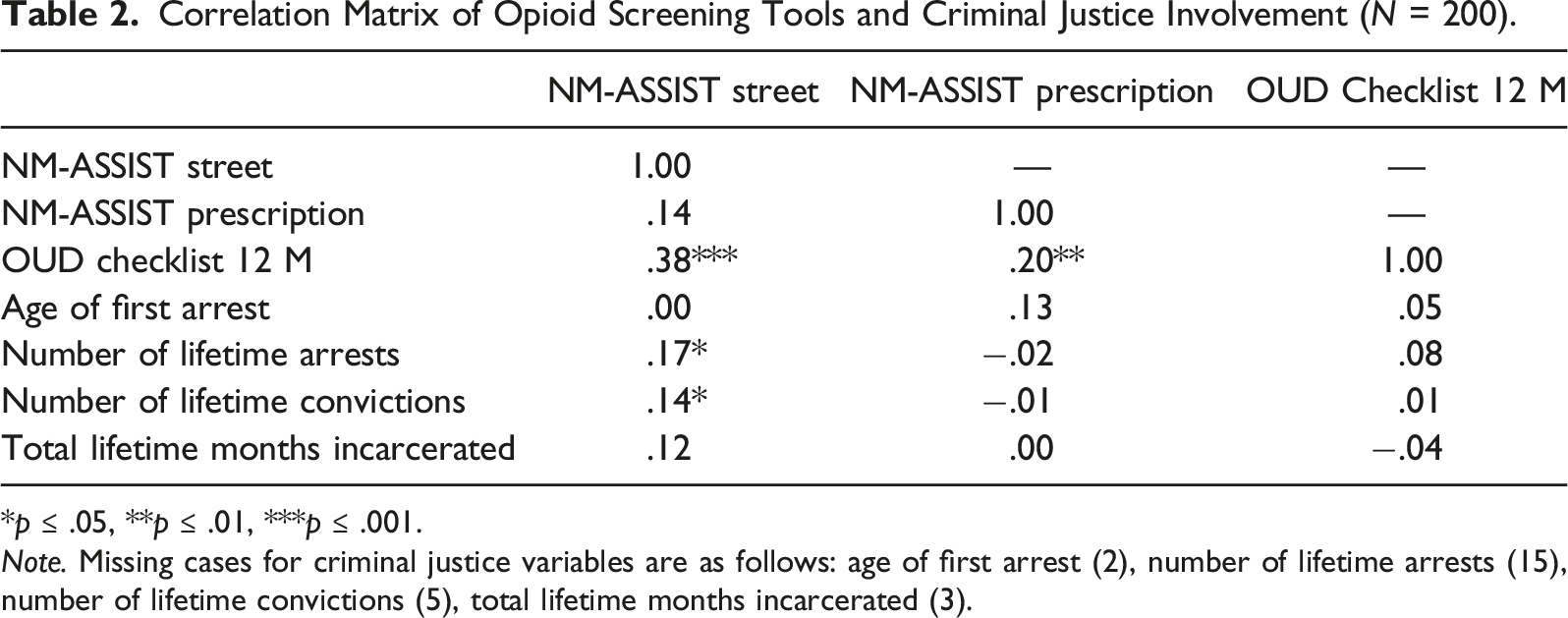
*p ≤ .05, **p ≤ .01, ***p ≤ .001.
Note. Missing cases for criminal justice variables are as follows: age of first arrest (2), number of lifetime arrests (15), number of lifetime convictions (5), total lifetime months incarcerated (3).
Bivariate Associations Between Opioid Screening Tools and High Risk Drug Use Indicators (N = 200).
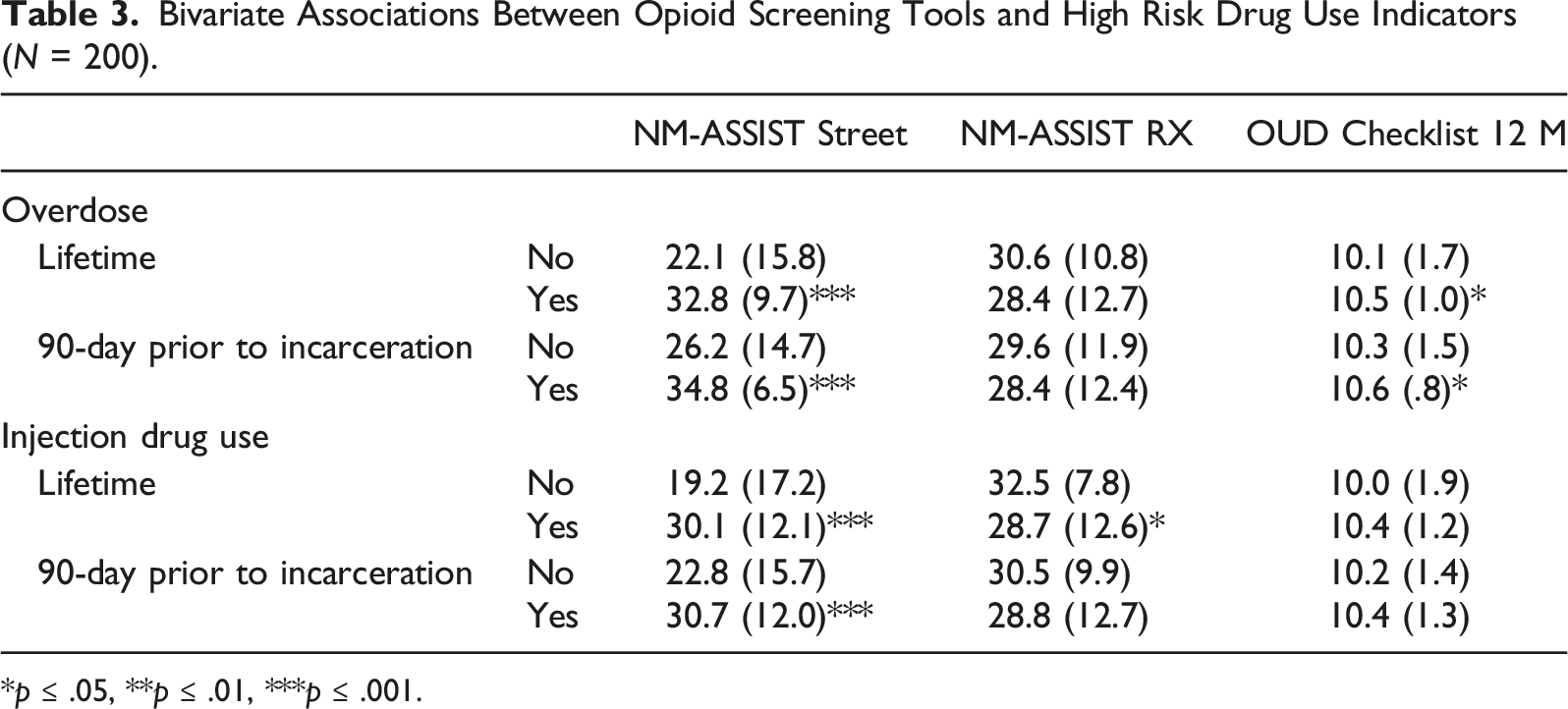
*p ≤ .05, **p ≤ .01, ***p ≤ .001.
Independent Correlates of OUD Criteria Screening Scores
Regression Analysis of Criminal Justice Factors and High-Risk Drug Use as Independent Correlates of NM-ASSIST Street Opioid Screening Scores (N = 171).
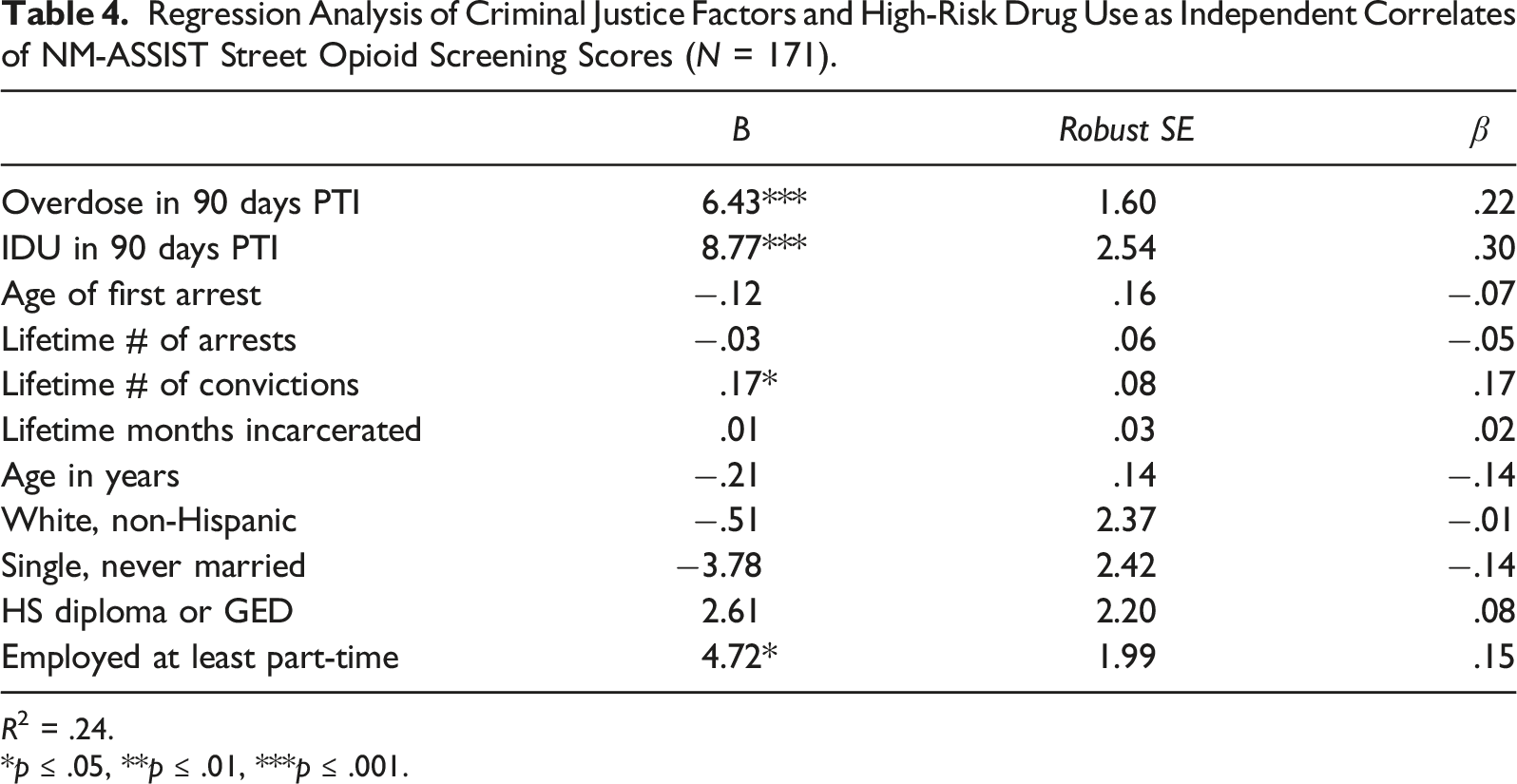
R2 = .24.
*p ≤ .05, **p ≤ .01, ***p ≤ .001.
Discussion
The overall aim study was to examine the utility of the DSM OUD Checklist and the NM-ASSIST screening tools to identify symptoms consistent with OUD among incarcerated women in jails. This study makes an important contribution to the literature because, despite significant health risks and unique vulnerabilities for women with OUD, research on screening and assessment approaches for incarcerated women has been limited. These study findings suggest high rates of OUD related risks among this sample of women. Considering the high rates of OUD in county jails and the risks associated with OUD relapse during the transition to the community, jails provide an important opportunity to identify and screen for OUD, engage in treatment planning while incarcerated, and develop plans for overdose prevention and treatment upon release.
The first study objective was to describe opioid use and self-reported criteria associated with OUD using two screening tools (NM-ASSIST and DSM OUD Checklist). In order to proceed with study screening, women were asked an initial question about any opioid use during the 12 months before incarceration. It is important to note that of the 277 women who were randomly selected and participated in the study screening session, 22% of women reported no opioid use during the year before incarceration. However, only one woman who reported using opioids in the 12 months before incarceration did not meet study inclusion criteria on either the NM-ASSIST (4+) or DSM OUD Checklist (2+). This finding is consistent with other studies which suggest a single item indicator of use can be informative in identifying individuals who misuse substances (Hearon et al., 2015; McNeely et al., 2015; Smith et al., 2010). However, our literature review did not yield any studies which examined the relationship between a single item indicator of opioid use and subsequently meeting screening criteria for OUD. These findings suggest that justice-involved women who use opioids are likely using them at levels indicative of a need for intervention. Thus, a single item indicator of opioid use may be critical at the time of jail entry in order to plan appropriately for treatment during incarceration (if available), as well as assessment at the time of release for re-entry treatment planning.
Women’s substance involvement (SI) scores on the opioid scales of the NM-ASSIST were considerably high in this study compared to other research. Specifically, women reported an average SI score of 28.3 for street opioids (heroin, fentanyl) and an average SI score of 29.3 for misuse of prescription opioids. In addition, for both street opioids and for prescription opioids, the majority of women fell into the “high risk” category of use (68.5% and 73.5% respectively). These average NM-ASSIST scores are higher than other samples of individuals in general who use drugs (Dawson-Rose et al., 2020; Shuper et al., 2020), as well as higher than other samples of incarcerated women (Staton et al., 2018). Specifically, among a randomly selected sample of women from three jails in rural Appalachia (Staton et al., 2018), mean scores for prescription opioids (26.5) and categorical risk indicators (62.4% high risk) were lower than those reported in this study. While the NM-ASSIST has been questioned as a valid screening tool for cocaine, benzodiazepines, and opioid use among pregnant women in urban communities (Oga, Mark, Peters, & Coleman-Cowger, 2020), these findings suggest that it may be a credible tool for assessment of severity of opioid use patterns among justice-involved women.
This is the first study to examine both the NM-ASSIST and the DSM OUD Checklist as screening tools to identify indicators consistent with OUD in a non-treatment seeking sample of women. In order to meet criteria to enter this trial, women had to endorse two or more criteria on the DSM OUD Checklist. Women in this sample endorsed an average of 10.4 symptoms during the 12 months prior to incarceration, and the majority (98.0%) scoring in the severe OUD category. Findings were similar during the 30 days before incarceration. While more commonly used as a tool to assess OUD in clinical settings, the DSM OUD Checklist has also been used to assess OUD severity in other research studies (e.g., Dunn, Barrett, Fingerhood, & Bigelow, 2017). However, scores among this sample of justice-involved women are considerably higher than observed in other samples of individuals who misuse substances (Dunn et al., 2017). While cut-off scores were consistent with how the tool is used clinically, future research should examine whether cut-off scores are low for samples of justice-involved women who use opioids. These findings suggest that the DSM OUD Checklist is a resource for OUD screening and can be administered in a research capacity in diverse settings to identify individuals who may be at high risk.
The second study objective was to examine bivariate relationships between OUD screening criteria, high risk drug use indicators (non-fatal overdose, injection drug use), and criminal justice involvement among this sample of women, as previous studies have shown that criminal justice involvement is associated with high risk drug use and risky sexual behavior among women (Jones et al., 2019). These findings indicated that both of the NM-ASSIST opioid scales were significantly and positively correlated with the DSM OUD Checklist. To our knowledge, this is the first study to examine the correlations between these tools among a justice-involved sample of women. In addition, the NM-ASSIST Street Opioids scale was also significantly and positively correlated with criminal justice involvement and other high risk drug use including non-fatal overdoses and injection. DSM OUD Checklist criteria also significantly and positively associated with non-fatal overdose, which corroborates prior research that has indicated that an increase in endorsement of DSM-5 OUD symptom criteria is associated with higher rates of lifetime overdoses (Dunn et al., 2017). These findings suggest that alone, and in combination, these screening tools may be viable indicators of high-risk drug use among justice-involved women and critical indicators of the need for treatment intervention planning – both during incarceration and during the transition to the community.
The final study objective was to examine criminal justice factors and high-risk drug use as independent correlates of OUD screening criteria. Findings indicated that, even when controlling for demographics, high risk drug use indicators including injection and non-fatal overdose were independent correlates of the NM-ASSIST Street Opioid scale, but not for the Prescription Opioid scale or the DSM OUD Checklist. These findings may be explained by data that demonstrates that street opioids, such as heroin, have higher rates of injection than prescription opioids (Jones, 2018). Street opioids may also be more likely to be contaminated with other substances than prescription opioids (Singh, Browne, & Montgomery, 2020), leading to an increased risk of overdose. In addition, a common trajectory of opioid use includes transitioning from prescription opioids to street opioids as tolerance increases (Compton, Jones, & Baldwin, 2016); thus, women with higher NM-ASSIST Street Opioid scores may be at a more advanced, high-risk stage of opioid use severity, which is often characterized by injection practices and non-fatal overdoses (Gicquelais et al., 2019; Staton et al., 2018) compared to those with only high scores on the NM-ASSIST Prescription opioid scale. Finally, polysubstance use may also be an important indicator of risk which should be examined in future research – particularly the co-use of opioids with stimulants, benzodiazepines, and alcohol, all of which increase overdose risk.
Interpretation of study findings should be considered with limitations. Women were randomly selected and recruited for the study from five purposefully selected jails in non-urban areas of Kentucky. While the random selection process should increase generalizability of study findings, it should be noted that findings may not be applicable for other justice-involved women who use drugs in larger, urban areas. Data included in this analysis was also self-reported by women while they were incarcerated. While self-report is common in social and behavioral research and has been shown to be valid for substance use (Del Boca & Noll, 2000; Rutherford, Cacciola, Alterman, McKay, & Cook, 2000), it is possible that self-report of sensitive information like drug use and criminal activities may be limited. In addition, while no criminal justice staff were present during any of the interviews, it is possible that women could have had concerns about study confidentiality. Each participant was provided informed consent prior to any research activities, which also covered the study Certificate of Confidentiality. However, despite these protections, it is still possible that being in a correctional facility may influence women’s perceptions of confidentiality. Finally, study analysis focused on data collected during the screening session and the baseline interview, and because of the variation in time for some of the measures (lifetime, year before incarceration, 3 months before incarceration), time spent incarcerated may have impacted memory recall.
Despite limitations, this study makes an important contribution to understanding the use of evidence-based screening tools for OUD among a sample of justice-involved women. The opioid epidemic continues to ravage rural and suburban areas, and with the explosion of high grade, synthetic opioids into the drug supply, the risk for opioid overdose following release from jail is of critical concern. For women in particular, the risks associated with opioid misuse can be even more concerning considering the increase in opioid overdoses among women compared to men in recent years. Although the use of a single-item measure in the present study was informative for screening the majority of incarcerated women for OUD, implementation of OUD screening in real-world contexts must be paired both with expanded services and with a treatment-centered, rather than carceral, response to substance use. Given the prevalence of OUD documented in the present study, the need for these expanded services is clear. Study findings indicate a positive correlation between indicators of OUD using two screening tools, as well as a high degree of correlation between street opioid misuse in particular and other high-risk drug indicators such as overdose and injection practices. Identification of indicators consistent with OUD during incarceration creates the opportunity for treatment assessment and planning, as well as during the transition to the community after release. These findings underscore the importance of integrating evidence-based screening approaches into routine intake procedures for carceral health providers, as well as increasing efforts to ensure access to OUD treatment among this vulnerable sample of women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (UG1-DA050069).