
Abstract
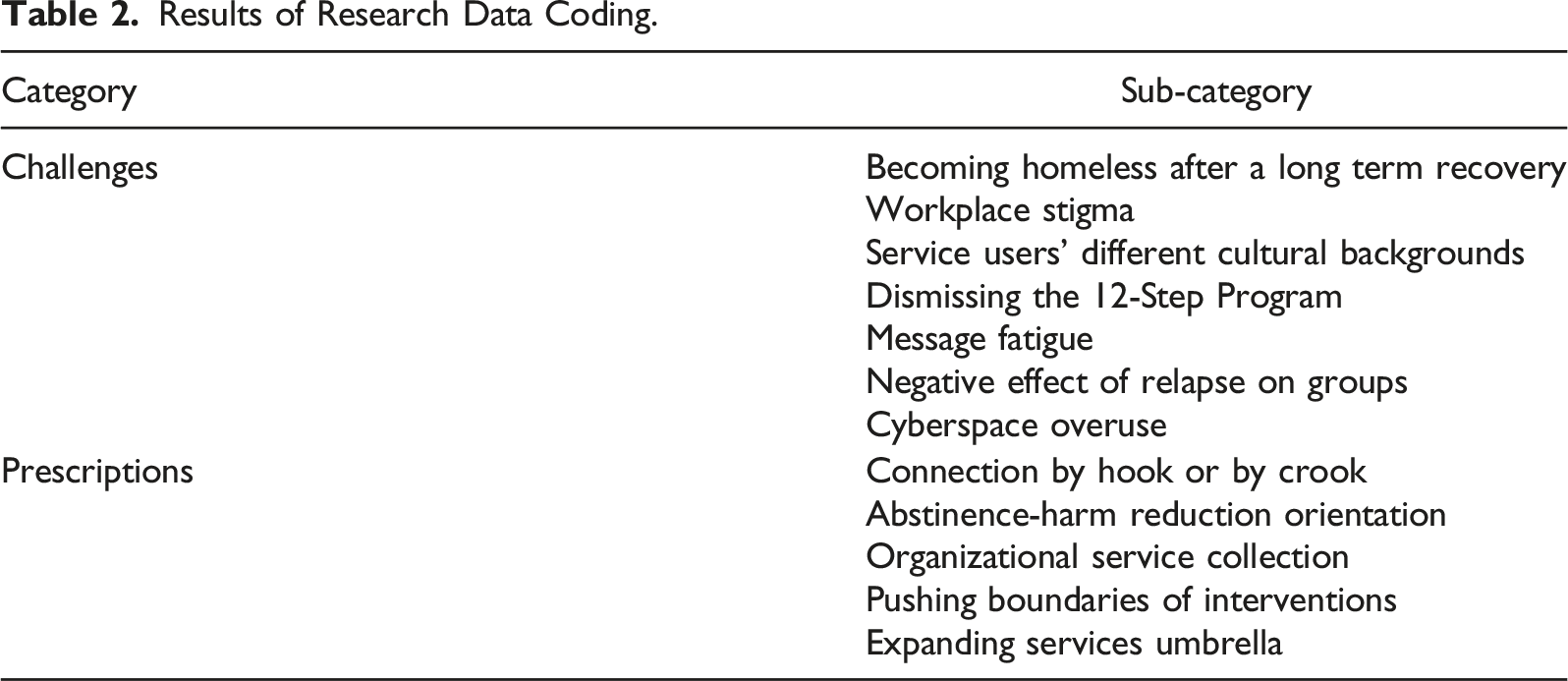
The research addressed challenges and prescriptions for reintegration of homeless people who use drugs. Data were collected through conducting semi-structured interviews. Twenty-nine participants were recruited. The primary codes were extracted and divided into two main categories of challenges and prescriptions; the former included becoming homeless after a long term recovery, workplace stigma, service users’ different cultural backgrounds, dismissing the 12-Step Program, message fatigue, negative effect of relapse on groups and cyberspace overuse; and the latter included connection by hook or by crook, abstinence-harm reduction orientation, organizational service collection, pushing boundaries of interventions, and expanding services umbrella.
Introduction
Homelessness is a global phenomenon which has affected many individuals, families, societies and governments (Amin-Esmaeili, Rahimi-Movaghar, Gholamrezaei, & Razaghi, 2016; Sleet & Francescutti, 2021; Tsai, O’Toole, and Kearney, 2017). In Iran, there is a lack of official and accurate statistics on the number of people living in homelessness. Yet, evidence indicates the rate is increasing, especially among substance users, and unofficial statistics estimate there are between 70,000 and 150,000 homeless people who use drugs (HPWUD) (Akbari et al., 2019; Noroozi et al., 2020; Rafiei, Alipour, Madani, & Narenjiha, 2019; Roshanpajouh, Mirkazemi, Asadi, & Hedayati, 2019). They are in Iran generally known as “cardboard sleepers,” “displaced,” or “visible addicts.”
There is a mutual relationship between substance use and homelessness that creates a vicious cycle (Nilsson, Nordentoft, & Hjorthøj, 2019). On one hand, substance use and/or addictive disorders break down relationships with family and friends and often lead to financial crisis due to unemployment. For people who struggle to make ends meet, the onset or exacerbation of drug use may result in loss of accommodation (Anker, 2008; Booth, Sullivan, Koegel, & Burnam, 2002; National Coalition for the Homeless, 2009). On the other hand, substance use in some cases is caused by homelessness itself. To cope with the situation and to temporarily alleviate problems, people in homelessness may consume drugs and alcohol. But in reality, substance use instead exacerbates their problems and reduces their possibilities to find stability in employment and leave street based environment. In addition, some individuals may find drug and alcohol use necessary to be accepted among the homeless community (Cheng et al., 2014; Didenko & Pankratz, 2007).
Problems with substance use, relationships with relatives, and mental health problems are associated with a reduced chance of leaving homelessness (Nilsson, Nordentoft, & Hjorthøj, 2019). Additionally, comorbidities such as HIV/AIDS, hepatitis B and C, dental problems, and diabetes are more common among HPWUD than among those with shelter (Center for Substance Abuse Treatment, 2013).
Classifying homelessness is done by dividing it into three categories, including: transitional homelessness (experiencing homelessness for a few weeks up to a few months, however less than a year, this includes people who have recently been released from jail); periodic homelessness (refers to a period in which people frequently move in and out of homelessness, this is common among individuals with unstable shelter); and chronic homelessness (a period of homelessness which lasts at least a year or occurs frequently while struggling with a debilitating illness such as substance use disorder, chronic illness or physical disability) (U.S. Department of Housing and Urban Development, 2015).
In general, HPWUD face many barriers to treatment. Due to their living situation and stigmatization, the group is less likely to have access to treatment and more likely to drop out of treatment (Luchenski et al., 2018). A study conducted on the perspective of HPWUD has identified five effective treatment factors including: facilitating service environments, compassionate and non-judgmental support, the importance of time, the right to choose, and opportunities to relearn life (Carver, Ring, Miler, & Parkes, 2020). Sosin and Bruni (2000) reflect on three factors that HPWUD do not undergo treatment including disconnection with family and community, isolation and lack of social support, and financial inability (Sosin & Bruni, 2000).
The United Nations Office on Drugs and Crime (UNODC) asserts the importance of access to and retention in treatment for the people in recovery from substance use who are homeless. Social reinsertion should be seen as an integral part of the treatment process to improve treatment results, prevent relapse, and ensure successful reintegration into society (UNODC, 2008). Social reintegration is defined as “any social intervention aimed at integrating former or current drug users into society.” The three pivots of social reintegration encompass (a) housing, (b) education, and (c) employment (including vocational training). Other measures, such as counseling and leisure activities, may be used (Souza, Silva, Batista, & Almeida, 2016; Sumnall & Brotherhood, 2012).
David Best (2019) believes that the integral part of all recovery journeys is the effective reintegration of the person into community, therefore to support recovery paths, structural and contextual efforts are needed to complement individual-based interventions and programs. He introduces five components of connectedness and social cohesion, hope about the future, promoting a recovery identity around social inclusion and social participation, meaning, empowerment and strength-based (Best & Colman, 2019).
In the Tripler R report, the main challenge addressed by various organizations for reinserting substance users has been job finding, especially in the economic crises Europe has faced over the past decade which has affected employment conditions and clients’ income generation (Tripler R Rehabilitation for Recovery and Reinsertion, 2017).
Most studies conducted on HPWUD have only addressed homelessness reasons and process, demographic characteristics, problems and barriers etc and less attention has been paid to their empowerment. Thus, the realization of the learned lessons service providers face to provide quality reintegration services to homeless drug users is crucial because knowledge update of the challenges and best practices may lead to proper, cost-effective, efficient and timely planning and policy-making.
This research has been conducted based on an action co-funded by European Union and Rebirth Charity Society through forming partnerships with well-known network of European NGOs for more than 2 years to ensure and utilize international best practices and quality standards on serving HPWUD in Iran. In fact, we intended to respond to two questions of: (a) what are the main challenges faced by service providers in reintegration of HPWHD? and (b) what are the main prescriptions for reintegration of HPWUD?
Methodology
Design and Sampling
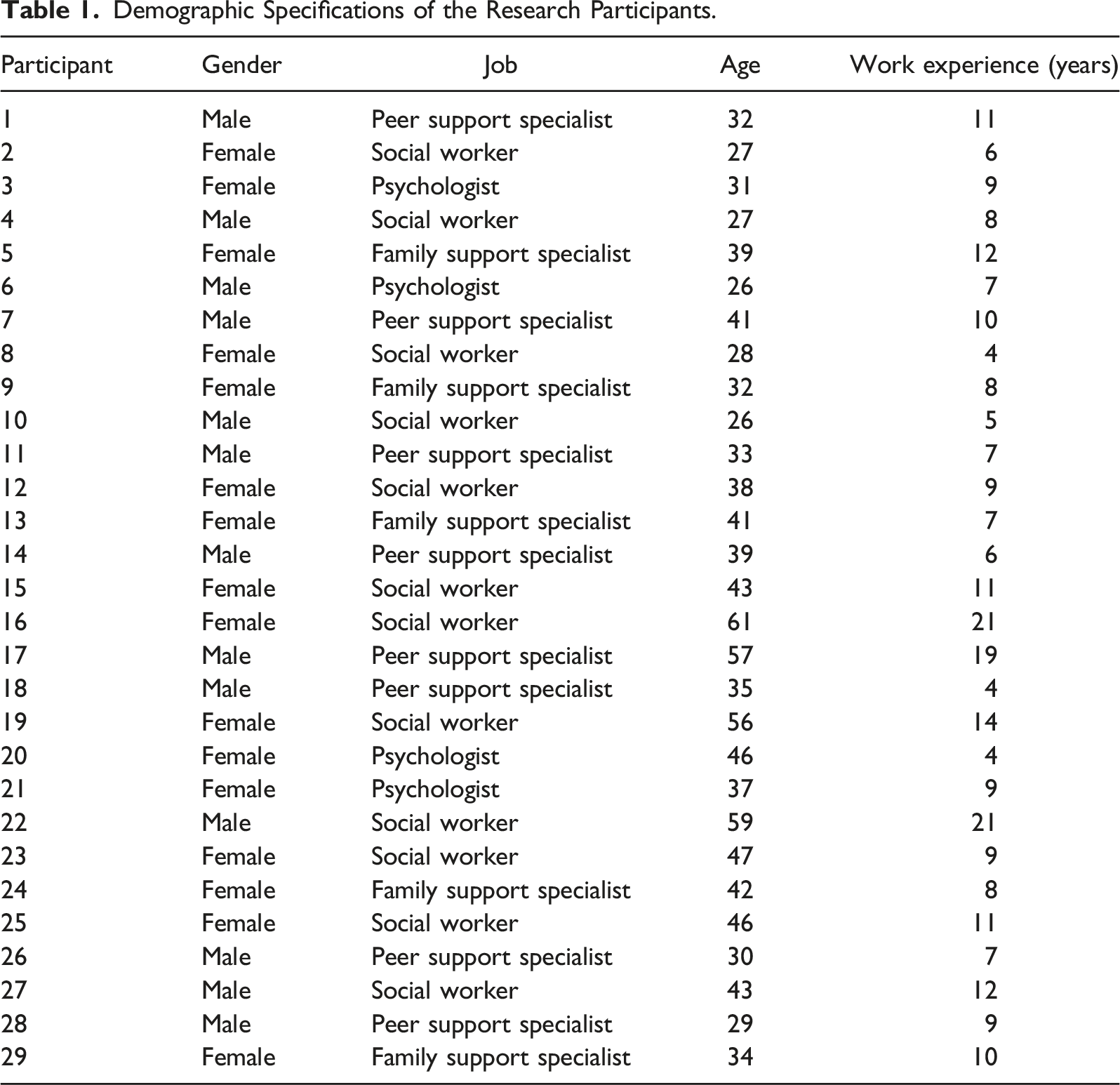
This research has been conducted through a qualitative method of content analysis based on the 18-month experiences (July 2020–December 2021) of the service providers of a project implemented with the aim of reintegration of HPWHD in the six provinces of Iran including Tehran, Alborz, Fars, Qom. Kerman and East Azerbaijan.
Demographic Specifications of the Research Participants.
Settings and Intervention
The participants were trained in one month (32 hr) in the areas of homelessness, substance abuse, comorbidities, family training, case management, relapse prevention, income generation, and more.
The intervention the participants provided for HPWUD was based on the Assertive Community Treatment and Intensive Case Management approach (Vanderplasschen, Wolf, Rapp, & Broekaert, 2007). The service provision covered treatment, accommodation, relapse prevention and life skills training, sanitary packages for the clients and incentive packages for families, screening and treatment of comorbidities, peer and family support counseling for clients and families, seeking advocacy for tracking identity documents, vocational training and job creation/finding.
The inclusion criteria for service users consisted of the people: who (a) had no permanent or temporary residence, (b) used drugs/were in recovery, and (c) were volunteers willing to use services.
Data Collection
All interviews were carried out by the first and eighth authors who are social workers in Ph.D. and bachelor respectively with quality interview experiences. Due to Covid-19 conditions and the distance between the provinces, semi-structured interviews were conducted in a hybrid format (face to face for some and video call for some others). All the interviews were audio-recorded and each interview lasted between 60 and 90 min, seven of which repeated for long interviews, concepts clarification and probing.
An interview guide was employed which was piloted with the first two participants and the required modifications were made. It began with an open-ended question such as “What challenges have you faced on providing reintegration services to HPWUD?” Or “Please describe the successful experiences you have had in the process of returning HPWUD to society.” Where the answers needed to be clarified and deepened, more detailed questions were asked, such as “Can you talk more about what you said” or “Can you explain more?”
The data collection process was saturated after interviewing 26 participants, which continued with three others to ensure its saturation. Prior to each interview, the partakers received an explanation of the purpose of the interview and their written informed consent was obtained prior to their participation.
Data Coding and Analysis
To analyze the data, the audio files recorded by the interviewers were transcribed verbatim and returned to the participants for any probable comment or correction. They entered into a MAXQDA 2020 software after each interview. After, the two members of the research team read and re-read the files to determine the meaning units and initial codes. Next, the meaning units and initial codes were extracted and the same initial codes were divided into sorting codes. Then, the codes were compared with each other, the pivots were determined, and their similarities and differences were classified into more abstract subcategories. Finally, the findings were shared with the participants and their feedback was considered.
Trustworthiness
To assure rigorous data, the criteria introduced by Guba and Lincoln (1994) was applied (Guba & Lincoln, 1994). For the purpose of credibility, the researchers had a long-term engagement in the research scope. Peer debriefing was also used with data sharing between the research team. The extracted data was shared and reviewed with the participants for their feedback through the process of member checking.
In terms of data conformity, the process of undertaking interviews, data analysis and extraction of codes and concepts were reviewed by the research team and shared with the field experts. Prior to the interviews, the interviewers’ assumptions and judgments on the subjects were recorded.
Findings
Results of Research Data Coding.
Challenges
Given the participants’ experiences, the following issues have been identified and extracted as the most important challenges encountered in the empowerment of HPWUD:
Becoming Homeless After a Long Course of Recovery.
One of the challenges come across by the participants was the referral of people who relapsed after several years of long-term recovery (more than 5 years) and due to the significance of the abstinence sanctity, their relapse have created conditions that led to self-isolation.
One of the social workers (p16) said, “I recently had a case who fell into drug take after 6 years of recovery. It was very difficult to work with him, he was disappointed, especially since he had several years of recovery experience and it was very difficult for him to start over. He said he had lost his whole life and no one trusted him anymore.”
A peer support specialist (p7) said of his experience working with multiple cases: “The problem of working with these people is that they consider themselves to be a know-it-all and resist learning and re-learning. It seems that their load is heavier to continue the path because they both consider themselves guilty and are not looked at well by others. Finally, until some time ago, he was a mentor, felt important, but now his clients are ahead of him. Well, this makes theپ work harder.”
Workplace Stigma.
The return of the people in recovery who are homeless into society requires a change in people’s attitude and trust. Employers’ distrust, abuse and discrimination against this particular group make up some of the challenges raised by the participants.
A peer support specialist (p11) said, “Society has negative views to drug users, even the recovered, e.g. a Mr. engineer, who we introduced a number of our clients, said he wouldn’t pay their salaries for the first three months because no one would employ them, this is a kind of guarantee because they may damage and leave.”
A social worker (p23) said, “Society rejects these people. I sent someone to work but was fired as soon as they found out he was recovered and where he lived while he had potential skills and talents. It seems he was rejected. The worst feeling is this feeling. Neither family nor community wants you. We’re trying to make them feel socially secure. For example, I’ve to say I am his sister! I really wish the conditions were suitable so that we could very easily say that this ex-drug user has recovered and society will give them a chance to change. That’s why I see some of the relapse which occur, well, the person says what else I can do. I lost things I can’t get back and I can’t skip them. These are people who come ahead up to at some point of recovery and regularly attend classes, but get engaged in drugs again.”
Service Users’ Different Cultural Backgrounds.
The partakers’ experiences showcase a percentage of HPWUD, especially in large cities, were migrants from other provinces with different cultures and ethnicities, therefore this cultural diversity has been challenging to work with them and their families.
One of the psychologists (p27) noted, “When we have a rehabilitation center or a clinic, people who belong to that area usually get the services; in Chitgar, the service receivers are often from the middle class. But, there is a great gap in social class and cultural differences between clients in the residential and empowerment centers for homeless drug users. For example, concerning religion or language, issues like these sometimes cause fights or annoyances and cliquish behavior among clients in their accommodation. Meanwhile, to work with each of them, we need to be very familiar with their culture.”
A family support specialist (p5) also shared her experience: “I hold group training classes to connect and encourage families to accept their members. Usually, because these families are mostly from different cities and different cultures, group work with them is difficult and therefore mostly individual counseling works.”
Dismissing 12-Step Program.
The participants encountered clients who did not believe in the 12-Step Program for the purpose of relapse prevention. A psychologist (p21) stated, “I had a few clients who said Narcotic Anonymous (NA) did not work for them. Group participation, the expression of past feelings and experiences in the crowd made them feel bad and that was why they ignored meetings.”
“Stimulant users and younger people are less committed to NA sessions and these sessions don’t work well for them. For these people, specialized programs work better such as matrix – a psycho behavioral and outpatient intervention,” another participant said (p18).
Message Fatigue.
HPWUD have had various experiences of recovery. The different recovery models available may be a reason to become tired of and distrust the empowerment program. One participant (p10) stated, “They have a particular distrust of themselves and us because of the various recovery programs they have been engaged in as well as their ineffectiveness since they say they have been treated several times, but no result.”
“Some cases have very low motivation and have heard so many promises not kept from various governmental sources, therapists and philanthropists about employment and support, so they do not hope to improve their condition.” another participant (p28) pointed out.
Negative Effect of Relapse on Groups.
Since homeless clients reside in groups in a place, one person’s lapse or relapse may affect others, and his or her return can break the indecency of consumption and adversely affect the recovery of others.
“The return of those who relapse and return to their place of residence after treatment weakens the belief of others in recovery and gives a message to them if they consume nothing will take place.”, one of the participants (p1) mentioned, Or the other participant (p25) said, “When one client takes drugs, the others become dizzy and tempted. You see, someone goes to the center and slips and comes back again, he/she is told you are not allowed to come to this center for six months because it becomes a habit and everyone else repeats it.”
Cyberspace Overuse.
Due to Covid-19 restrictions and the closure of NA sessions, the presence of individuals in cyberspace has increased. Despite the benefits of cyberspace, especially its helpfulness during the pandemic, for some clients who had a smartphone and without the necessary skills, their presence in cyberspace might be challenging. A participant (p6) said, “When one of my cases came to the virtual group, totally withdrew from people because she was always active on Instagram or WhatsApp groups. Her depression also made her isolated.”
“One of the other harms the Internet may cause is the social class differences. It means that one compares oneself with others, and this makes it impossible for one to have proper financial management. Sometimes drugs are promoted, which may be tempting, or a person wastes a lot of time there” Another partaker (p20) stated.
Prescriptions
According to the experiences of the research participants, the prescriptions for empowering HPWUD include the following:
Connection by Hook or by Crook.
One of the most important criteria for the recovery among the clients is their connection with the support system. One partaker (p14) believes, “providing an empathetic, intimate, yet engaging atmosphere for clients brings a situation in which even if clients take drugs because they know they are behaved well, they’d go to social workers and talk about their problems.”
“Because the main criteria for our service provision is the individual’s willingness and we aren’t supposed to confine them in a closed space, so it’s very important that they’re linked to us. If the linkage is lost because they don’t have a fixed location and most of them don’t have phones, we can’t find them and it gets very difficult”, a social worker (p12) shared her experience.
Abstinence-Harm Reduction Orientation.
Since lapse and relapse are very likely in the empowerment process, the boundaries defined need to be very flexible. If abstinence from illicit drugs becomes sacred, lapse or relapse rejects the person (both through external pressure and internal shame) and results in re-homelessness, while substance use and homelessness are equally important.
The other participant (p4) noted, “I had a case and found that he hadn’t been to the accommodation center for several days. I told myself that he went and wouldn’t come here again. After a few days, he came to me in a state of confusion which was clear he had taken drugs and had slept outside for a few nights and asked for help. It made me feel very good. But, when I asked him if he could go for treatment, he said no, I can’t do it now. I said no problem, you can go to the Qiam harm reduction center. If there’s no harm reduction center, we can do nothing for them, because all our accommodation centers offer services to the recovered.”
“One of my clients after 4 months of recovery took some pills. She took a drug addiction test and it was positive. I told her she couldn’t go to the accommodation center and she’d to go to the harm reduction center and didn’t take any illegal substances there for a week, then she could go back to the accommodation center. A week passed, and she kept his promise”, one of the participants (p8) stated.”
Organizational Service Collection.
The HPWUD have a variety of needs that should be responded to and met through different service centers and institutions. Having a set of services in an organization that meets their minimum needs and does not require bureaucratic and inter-organizational mechanisms can facilitate the empowerment process.
One of the participants (p22) said, “We have a number of services and service centers which are all work for the organization. Now, people benefit from the service delivery depending on the stage they are at, the extent of their progress, their recovery conditions and the need they have.”
“That the main services the majority of clients need are covered in the organization has made our work much easier and increased our maneuverability to help clients. For example, if I want to refer a case, who has relapsed and wants to be treated again in the treatment center, it gets easy because we’ve the center,” another partaker said (p16).
Pushing Boundaries of Interventions.
Homelessness does not take place in a certain and definite point rather it is a phenomenon which occurs within a process. According to the experiences of the research participants, drug users who live in families facing poverty, due to financial inability and/or not being aware of the services, cannot be engaged in recovery despite their desire, hence it seems they should be considered as the target group of the homeless.
One of the partakers said (p15), “In the office, we work with clients in one of the poor and vulnerable neighborhoods of Tehran (Harandi), families also come to us to receive the services. As their drug-using member lived with them as the head of the family without an income, family members were at risk of losing their shelter. We started working with these clients and families since if we didn’t work with them, soon they would become future cases.”
The other participant said (p12), “One of my clients lives with his family, but spends most of his daytime in the spots of Harandi neighborhood. When he is with the family, they always argue, so the family don’t want him. He also has got a brother who takes drugs and they’re user mates. … I found them at risk of homelessness.”
Expanding Services Umbrella.
Many years of experience living in a situation where access to health, treatment, and social services has been very limited and lack of financial resources and attention to these issues have all aggravated the reason for the accumulation of physical, psychological, and family problems of homeless substance users which appear on the road to empowerment.
One of the partakers (p27) expressed “physical illnesses are common among these people because they’ve lived in very bad conditions. I’d a case who had an infection from a leg plate. The doctor said it needed surgery. It cost a lot. He was hospitalized for about 90 days and got several operations on his leg.”
Another partaker (p29) emphasized “The basic needs of these people need to be addressed, from clothes and food to transportation money. Because we provide them with these facilities, a very good linkage has been formed between us and they seem to have found an identity.”
Discussion
The conduct of this study aimed at addressing the issues and suggestions on service provision to HPWUD from service providers’ perspective. It found the issues as becoming homeless after a long term recovery, workplace stigma, service users’ different cultural backgrounds, dismissing the 12-Step Program, message fatigue, negative effect of relapse on groups and cyberspace overuse; and the recommended interventions as connection by hook or by crook, abstinence-harm reduction orientation, organizational service collection, pushing boundaries of interventions, and expanding services umbrella.
Despite the novelty of the research topic, relatively high experience, and geographical diversity of the participants as the strengths of this research, there have been some limitations in generalizing the findings since it was carried out qualitatively and from the service providers’ experiences of working with HPWUD. Besides this, for the findings application, it needs to be considered that they were obtained based on the work experience of the participants at the time of the outbreak of Covid-19. Some studies suggest that virtual groups may act as a supportive factor in the recovery. This seems to have been especially helpful during the Covid-19 pandemic, as at times when restrictions were tightened, NA and counseling sessions were virtually held (Bliuc, Doan, & Best, 2019; Dugdale, Elison, Davies, Ward, & Jones, 2016). However, this research has considered excessive presence in cyberspace as a challenge.
The experiences of Dianova – a NGO working on the development of people, communities and organizations in different parts of the world - indicate it is very difficult to achieve social resettlement without family support, and even in the absence of family, it offers the option of an alternative family (Tripler R Rehabilitation for Recovery and Reinsertion, 2017). This study has addressed cultural differences between families as one of the reintegration challenges, which becomes more outstanding in training and group meetings, especially in Tehran where the target group have migrated from across the country.
Most HPWUD experience lapses and relapses, and the prerequisite for any intervention is the availability of support professionals since access to them and continued connection with service users are essential. Based on the experiences of the partakers, the disconnection of the clients from the support system puts all the assistance ways in a deadlock. As in the CHIME model, connectedness is an integral part of recovery, the prerequisite for supporting this group is their connection and the continuity within the support system (Leamy, Bird, Le Boutillier, Williams, & Slade, 2011).
Interventions for substance use and homelessness should be carried out such that the former does not lead to the latter recurrence, since if there is no realization of harm reduction in this process, the empowerment process itself will reproduce the stigma and reject those who slip into this cycle. Therefore, the existence of combined harm reduction-empowerment interventions assures the prevention of recurrence of homelessness.
Following the findings, other studies conducted on empowerment and rehabilitation of similar target groups suggest many of their participants had, for the purpose of recovery, preferred interventions such as meeting their basic needs, harm reduction approach, participation in social activities and building positive social relations (Collins et al., 2016; Pleace & Lloyd, 2020).
Research suggests working with HPWUD is challenging since they have different needs and the response to these requirements needs to be addressed through many different centers (Moghanibashi-Mansourieh et al., 2022; Pleace & Lloyd, 2020; Rafiey, Alipour, Moghanibashi-Mansourieh, & Mardani, 2019). One of the findings of this study is that there should be organizations with different centers offering a collection of various services instead of leaving clients between different organizations to get involved in administrative procedures. This model can be especially effective in countries such as Iran, where there is no coordinated, structured and systematically institutionalized inter-organizational social support system to offer services to HPWUD. As David Best addresses inclusive cities/communities for the reintegration, thus this procedure should not lead to the responsible institutions shirking their duties, as eventually some of the services, such as issuing identity cards and employment, etc., require the coordination and cooperation of other bodies (Best & Colman, 2019).
Studies conducted in various countries conclude that while the visible form of homelessness appears as people reach adulthood, a large proportion of them have had severe social harms and traumatic experiences in their childhood such as poverty, housing problems, educational disruption, lack of social and psychological support, the experience of physical, sexual and emotional abuse, family relationship breakdown, and family structure instability all of which enhance the likelihood of homelessness (Grinman et al., 2010; Mabhala, Yohannes, & Griffith, 2017; Priester et al., 2016; Rafiey et al., 2019; Thompson, Wall, Greenstein, Grant, & Hasin, 2013). Accordingly, this study found that for HPWUD empowerment, there is a need to expand the services umbrella in the domains of family livelihood, mental and physical health, dental services, income generation, legal issues etc.
The findings remind the policy and decision makers that the ruling spirit on the policies for HPWUD should concentrate on an abstinence-harm reduction approach. In terms of practice, the scope of interventions should not merely be constrained to substance use, but they should be undertaken as comprehensive interventions. In addition, more research on the efficiency and effectiveness of the interventions through group control and/or longitudinal studies in future is recommended.
Footnotes
Acknowledgments
The research was conducted on the experiences of the service providers of the project of social support for homeless drug users in Iran co-funded by the European Commission and Rebirth Charity Society. The partners included World Federation Against Drugs (WFAD), European Treatment Centers For Drug Addiction (euro-TC), Therapiesalon im Wald, and Society for Recovery Support. We would also like to express our special thanks to the research participants who shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The authors declare that they have obtained ethics approval from an appropriately constituted ethics committee/institutional review board where the research entailed animal or human participation.
Prior to each interview, the partakers received an explanation of the purpose of the interview and their written informed consent was obtained prior to their participation.