
Abstract
The aim of this study was to understand caregivers of individuals with dementia attitudes toward CBD oil. Thematic analysis was conducted with 67 posts (570 comments) about CBD oil selected from a Polish online support forum for caregivers. We identified caregivers’ expectations, motivations, and practices of using CBD oil. Caregivers expected CBD to improve the behavior, cognition, communication, and daily activities of their loved ones. They motivated each other by sharing experiences about the positive effects of CBD oil and claimed to be administering CBD oil without medical advice, which led to dangerous practices such as an overnight withdrawal of all drugs or experimenting with CBD oil dosage. Caregivers perceive CBD oil as a safer and more effective treatment for those with dementia than the conventional methods. We recommend healthcare professionals inquire about possible CBD oil usage during follow-up visits and thoroughly explain what to expect from prescribed medications.
Introduction
Dementia is a syndrome characterized by a decline in cognition to such an extent that it impairs independent living and functioning range (Rehm et al., 2019). Current estimates indicate that approximately 55 million individuals worldwide suffer from dementia and it is predicted that by 2050 this number may exceed 152 million (Nichols et al., 2022). Dementia poses considerable challenges for an increasing number of individuals and their family members who often become their caregivers. Caregiving involves a continual adaptation to decline in functioning and may have a detrimental impact on caregivers’ health and well-being (Del-Pino-Casado, Priego-Cubero, López-Martínez, & Orgeta, 2021; Sörensen & Conwell, 2011).
Current treatments available to individuals with dementia are limited and can neither cure nor alter the progression of the most common forms of dementia but only temporarily reduce certain symptoms. Additionally, there are conflicting findings regarding the effectiveness and safety of commonly recommended medications like donepezil or rivastigmine (Lanctôt, Rajaram, & Herrmann, 2009; Li, Zhang, Zhang, & Zhao, 2019; Tricco et al., 2018). Furthermore, they are associated with a range of side effects such as nausea, confusion, fatigue, or dizziness (Briggs, Kennelly, & O’Neill, 2016; Buckley & Salpeter, 2015). While pharmacotherapy can be useful in stabilizing or slowing the progression of the disease, the clinical evidence demonstrates that they are most effective only during the early stages of the disease (Dou et al., 2018; Knight, Khondoker, Magill, Stewart, & Landau, 2018).
A growing body of research shows that caregivers of individuals with dementia experience greater levels of strain due to the difficulty in dealing with the behavioral and psychological symptoms of dementia (BPSD). The BPSD occur in more than 90% of people with dementia (Cerejeira, Lagarto, & Mukaetova-Ladinska, 2012; Kim, Noh, & Kim, 2021). These symptoms include a range of behaviors such as social withdrawal, agitation, anxiety, wandering, sleep disruption, disinhibition, irritability, appetite changes, and outbursts of aggressive behavior and can present a significant burden for individuals with dementia and their caregivers (Deardorff & Grossberg, 2019; Kales, Lyketsos, Miller, & Ballard, 2019). Due to the BPSD’s unpredictable nature, they may lead to detrimental outcomes in providing care, including poor quality of life, depression, caregiver burden, and a higher risk of substance abuse and mortality (Cerejeira et al., 2012). They are also associated with an increased use of medications, frequent hospitalization, and an earlier nursing home placement of the individual with dementia (Hessler et al., 2018).
Since the BPSD represent a heterogeneous group of non-cognitive symptoms and behaviors, their management depends on the symptom and its severity. The conventional treatment to lessen the symptoms often includes antidepressants, benzodiazepines, and antipsychotics. However, the administration of these drugs is associated with a range of adverse side effects such as increased fall risk and mortality risk (Ettcheto et al., 2019; Rochon, Vozoris, & Gill, 2017). Although non-pharmacological interventions (e.g., reminiscence therapy, music therapy) are recommended as the first line of treatment and have been shown to benefit individuals with dementia by improving their subjective well-being, communication skills, and decreasing depressive symptoms, their effectiveness is limited (Wang, Pei, Zhan, & Cai, 2020). Additionally, considering the demands associated with attending to the needs of an individual with dementia, caregivers often do not have the time, energy, or finances to comply with the recommended activities for the intervention to be successful (Kales et al., 2019).
A lack of effective treatments for the most common symptoms of dementia and the stressful nature of caregiving have prompted caregivers to investigate alternative therapies for symptoms of dementia, including cannabidiol oil (Peprah & McCormack, 2019). Cannabidiol (CBD) is one of more than a hundred cannabinoids found in Cannabis sativa L. Unlike Δ9-tetrahydrocannabinol (Δ9-THC), cannabidiol (CBD) is a non-psychoactive component of cannabis. CBD is most often inhaled, consumed in edibles, or immersed in oil (Outen et al., 2021). Contrary to THC, CBD does not change heart rate or blood pressure, does not induce catalepsy, nor does it have detrimental effects on psychomotor or psychological functions and is generally well tolerated (Maroon & Bost, 2018). This favorable safety profile of CBD oil has led to its increasing popularity. CBD oil has been extensively used for a wide range of medical conditions and is easily accessible to the public online or as an over-the-counter supplement as long as it does not exceed .2% THC (Hughes, Vandam, Mounteney, & Griffiths, 2022).
Numerous studies have demonstrated the therapeutic potential of CBD and its effectiveness in conditions such as anxiety, insomnia, nausea, epilepsy, and chronic pain (Beedham, Sbai, Allison, Coary, & Shipway, 2020; Crippa et al., 2021; Larsen & Shahinas, 2020). Even though the effects of CBD are not yet supported by clinical data, there has been an increase in use of CBD among dementia caregivers (Leszko & Meenrajan, 2021). The interest in using cannabinoids in dementia was motivated by the preliminary trials suggesting a therapeutic potential of CBD oil in neurodegenerative diseases such as vascular dementia, Huntington’s disease, Parkinson’s disease, and Alzheimer’s disease in vitro and animal studies (Ahmed, van der Marck, van den Elsen, & Olde Rikkert, 2015; Aso & Ferrer, 2014; Walther & Halpern, 2010). Although research into the effects of CBD is rapidly increasing, in a recently conducted systematic review of randomized controlled trials investigating the effectiveness of cannabinoids for the treatment of dementia, the authors concluded that the available evidence is limited and requires further investigation due to some methodological deficiencies such as small sample sizes, short-lasting treatment, and inadequate controls (Charernboon, Lerthattasilp, & Supasitthumrong, 2021).
Considering the limited treatment options for dementia, CBD oil has become an attractive therapeutic option. Yet, little is known about the experiences of family caregivers of individuals with dementia. This is of particular concern given that previous preliminary findings indicate that caregivers are reluctant to consult with their primary healthcare professional about using CBD oil and experiment with a dosage (Leszko & Meenrajan, 2021). Although it has been marketed as a natural remedy in alleviating many symptoms, in many countries, including Poland, CBD oil is not classified as a drug but as a dietary supplement. This means its quality is not controlled nor regulated by the government and therefore raises concerns about the accuracy of the labeling, safe dosage, harmful contaminants, and potential harm. Producers often use unproven health claims (McGregor et al., 2020). Add to this, we know even less about the long-term effects of CBD oil usage. This becomes problematic when CBD oil of unknown quality is administered to vulnerable individuals and when caregivers choose to substitute medications for CBD oil without consulting a healthcare professional.
To the best of our knowledge, there are no qualitative studies on CBD oil among caregivers of individuals with dementia. To fill this gap in knowledge, the aim of this study is to understand caregivers’ beliefs and practices related to CBD oil. The current analysis draws on online support group posts and synthesizes the evidence utilizing thematic analysis by addressing the three following research questions: 1. What are the caregivers’ experiences with using CBD oil? 2. What kind of information do caregivers look for regarding CBD oil? 3. What motivates informal caregivers to start using CBD oil?
Method
Study Design and Sample
We conducted a thematic analysis of caregiver’s discussions related to CBD oil in one of the largest Polish online support forums for caregivers with dementia. This online support forum consists of members who identify themselves as informal caregivers of individuals with dementia. In order to become a member of the forum, an individual uses his or her Facebook account and accepts the rules and regulations. The participants in this study are the members who wrote the messages selected for analysis. The total number of forum participants during the study period was 2497, and 955 of them actively participated in content creation. The average number of posts published per day is 3 (39 comments), and per month is 100 (1192 comments). This online group was established in 2016 as a platform to promote good practices in dementia care. The purpose of it was to create a place where receiving support and sharing experiences would be possible, as in Poland the number of stationary support groups and dementia centers is scant.
Data Collection
All posts about CBD oil published between 09/2019 and 11/2021 were included for analysis. Within the forum, the search function was used to identify all user posts relating to CBD oil. The posts were identified using search queries with “CBD oil,” “CBD,” “oil,” “marijuana,” “CBD drops,” and “cannabis.” For the purpose of this study we focused only on the content of the posts, threads and messages visible to each member of the discussion forum. When a list of potential posts was created, each post, threads and its messages were examined to assess whether they were suitable for analysis. We gathered a total number of 67 posts that contained: 570 threads, 1757 messages, and 2509 likes. This content was created by 405 forum members (16.21% among all forum members and 42.40% of all active members). Of those, 221 of them (54.57%) actively posted on the topic of CBD oil, while 184 people (45.43%) limited their reactions only to liking the content appearing on the forum. Female avatars were utilized by 381 of them (94.07%) and only 24 (5.93%) had adopted male ones. Among the users, 246 of them (60.74%) declared to be middle-aged women who are informal caregivers to a close family member: a parent, a grandparent, or a spouse. This is consistent with previous studies as, across the world, women are the predominant providers of informal care for older adults (Mucha, Leszko, & Potemkowski, 2021; Sharma, Chakrabarti, & Grover, 2016). The quotes were translated from Polish into English separately by both authors and checked by a professional English native speaker. The translation is as close as possible to the original Polish version, to reflect both lexical and syntactic aspects of utterances. It occasionally may result in ‘disjointed’ English, used also to represent incorrect grammatical structures of the original Polish utterances. In the quoted fragments, trade names of drugs were changed into generic ones.
We collected only retrospective and public data, thus we did not obtain informed consent. However, following ethical guidelines published by the British Sociological Association Digital Sociology (2016), we removed all sensitive information which could lead to revealing the identity of the group members. We also obtained approval from the Ethical Review Board for the research procedure. To allow identification of quotes created by the same forum member, we marked them with a single letter placed in the upper index behind the extract number.
Data Analysis
Thematic analysis was chosen to analyze the gathered material as it allowed us to identify patterns within the dataset. It is a popular methodological approach in clinical psychology, which allows the researcher to identify themes in personal experiences and provides a procedure to analyze qualitative material (Braun & Clarke, 2006; Clarke & Braun, 2018). In our study, we implemented social constructionism as a theoretical background. Constructionism assumes that people constitute social realities through and within language (Barker & Galasiński, 2001).
In our study, we utilized Braun and Clark’s (Braun & Clarke, 2006) six-step guide to reflexive thematic analysis. First, both authors (UK and ML) have immersed themselves in the data that involves repeated reading, writing down insights, and identifying initial data patterns. At the beginning of the analysis, we had no theoretical assumptions towards the data. In the next step, the first author (UK) started an inductive coding process to organize the data into meaningful clusters and to reduce the amount of analytical material. We adapted semantic meaning as a unit of coding because it reflects the best core concept assigned to the code extracts. A professional qualified in linguistic analysis was consulted about the codes. The data were coded with the use of MaxQDA software (ver. 20.4.1). In the third step, the first author (UK) sorted codes into initial themes, checking if they fulfilled the internal homogeneity and the external heterogeneity criteria. Then, both authors together reviewed all those initial themes to identify overarching themes and sub-themes. At this point of the analysis, we distinguished semantic and latent themes. Finally, we defined and named the themes and prepared the final report that we have presented in the results section.
Credibility Checks
To enhance the reliability of the analysis, we used investigator triangulation, reflexivity, and an audit trail of the study (Merriam & Tisdell, 2016). We have reached the level of data saturation with 18 analyzed posts, which means that no relevant themes have emerged from the data set since that point. To enhance the transferability of our findings, we provided a rich, thick description (Merriam & Tisdell, 2016) of the study’s context, support forum, study participants, and available support to family caregivers in Poland. We also decided to exemplify our findings with original quotes from the forum users.
Results
Main Themes and Sub-themes Identified During the Analysis.
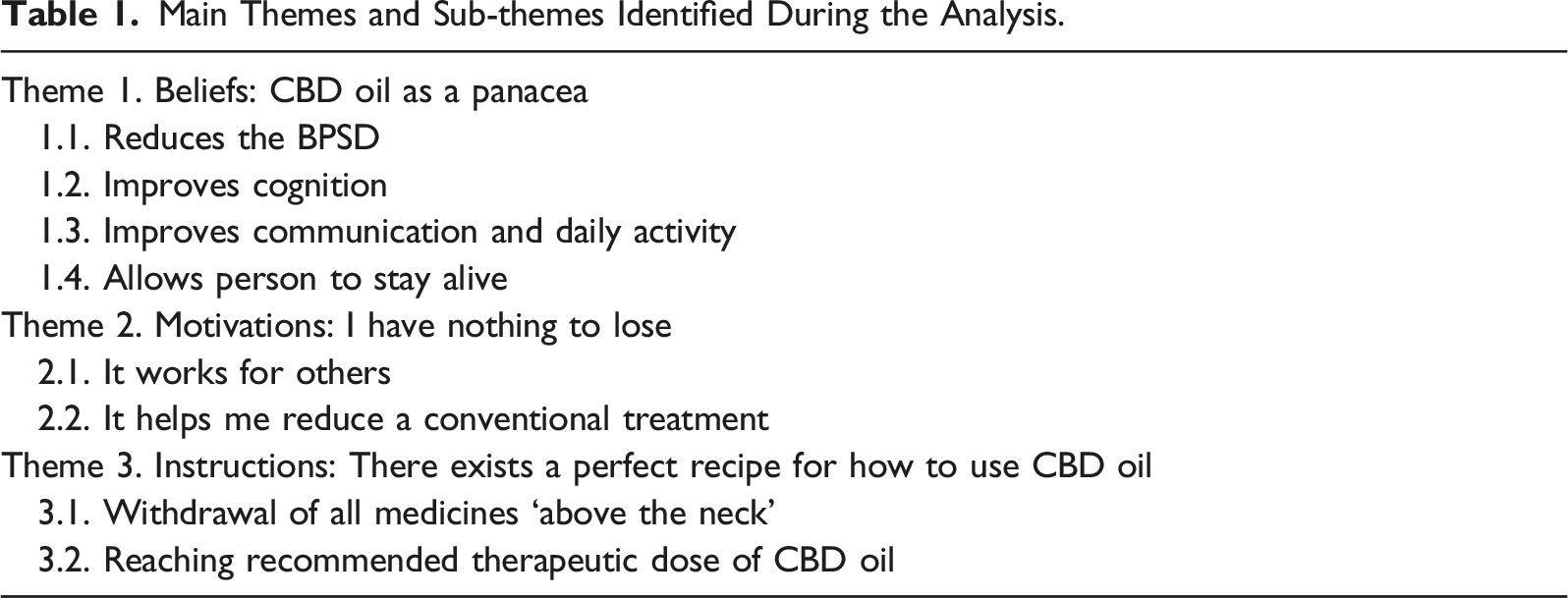
Theme 1. Beliefs: CBD OIL as a Panacea
In the gathered material, we found different expectations towards the CBD oil that were revealed by caregivers. In this topic we want to discuss four of the most popular intentions. We will start by showing what effect they believe the CBD oil has on reducing difficult behaviors. Then we discussed its impact on cognitive function, communication, and everyday activity. Finally, we show caregivers hope that the CBD oil might bring back a pre-disease state for a while and determine why it is important for them.
Reduces the BPSD
As we expected based on previous research (Deardorff & Grossberg, 2019; Kales et al., 2019), caregivers emphasized how much of a burden dealing with the BPSD are for them. They anticipated the CBD oil would reduce different difficult behaviors in those they care for. Consider the following examples: Extract 1. I’m going to, for the first time, buy CBD drops. For Mom, [who is] 92 years old. [She suffers from] increasingly frequent dementia attacks, auditory hallucinations, conspiracy theories, and very severe agitation near aggression. Extract 2a. She has ghastly hallucinations, everywhere she sees her friend that she was with two years ago and she thinks he still lives with us. When she starts walking back and forth, she repeats the same thing over and over. She doesn’t want to clean herself… I have to promise her something sweet to get her into the shower. She won't handle herself on the toilet either… although it’s been slightly better recently as she’s going there and not pooping in her pants. Mom will only be 65 in June, she’s still a young woman… and I think the oil might be able to help her. Extract 3. I’m staying alone with my grandma for a week, my parents are finally going on a holiday. I’m afraid of the night, because that’s when she has nothing to do, she thinks and speaks. Can this oil help?
Caregivers in those extracts perceived CBD oil as a remedy for such challenging behaviors as hallucinations, delusions, and agitation with aggression. They also expressed hope that it would reduce sleeping-disturbance, calling out, repetition and wandering. Interestingly, in presented extracts CBD oil was seen as an effective remedy for the BPSD both in young and late onsets of dementia. This conviction was also expressed by other caregivers who expected that it would be effective in all types and stages of dementia.
Improves Cognition
Caregivers also presumed that the CBD oil could improve cognition. However, they assumed this positive effect will be achieved indirectly by improving the mood of the individual with dementia. They want the CBD oil to specifically reduce anxiety and anger, which occurs when their loved ones notice memory difficulties and thus worse cognitive functioning. Extract 4. I think about this oil mainly because of the emotional state [of my dad], as it also impacts his cognition - as soon as he gets nervous, he can’t remember or understand anything. (…) [I consider] the oil as a supplement, because dad can’t handle himself, his emotions, not remembering, and all that gets him upset, then, we can’t handle anything anymore and he gets even more touchy and explosive.
In the gathered material, group members agreed that it was impossible to reverse neurodegeneration and there is no cure for brain damage. However, we were surprised that in their opinions this didn’t apply to vascular dementia caused by a stroke. Some have suggested that the CBD oil may help to regenerate the cerebral blood vessels, and thereby restore cognitive function. Extract 5. I’m totally convinced as to the use of the oil (…). My husband has had the onset of vascular dementia since a micro-stroke. (…) I am very hopeful that there will be regeneration of the ischemic lesions.
Improves Communication and Increased Activity
Caregivers considered administering CBD oil also to those who were calm and did not present any BPSD. They want the oil to improve language skills and reduce aphasia in those they care for. In their expectations, CBD oil would make it easier for them to speak and would increase their ability to retrieve words. Extract 6. I thought maybe after the oil he would start talking. Sometimes he utters a single word, but usually he just gestures. Extract 7b. My dad doesn’t have any problems like aggression, he “only” can’t express himself, laughs at everything, doesn’t recognize who is who, but is sure that he knows them (e.g., his kids). My dad generally has this emptiness in his eyes that scares me, everything has to be explained to him, he needs to be guided everywhere, etc.
In the utterances of caregivers, the CBD oil could cure not only aphasia, but also apathy. Some of them described their loved ones as overly withdrawn, too calm, and having difficulty in carrying out everyday activities. They wanted the CBD oil to help them in daily life functioning by improving their mobility and boosting energy. Extract 8c. My mom is very calm, rather I hope the oil will bring her back some of her functional realm. I wouldn’t want it to give her an unhealthy arousal and rattle her… Extract 9. [M]y mom is getting weaker and weaker; I noticed that what she was doing yesterday is already difficult for her today so I thought maybe things would improve [with the oil]. Her walking is getting worse and worse and she is losing her balance and becoming more and more like a rag doll. I wish she had a bit more energy but I don’t know if that is possible.
In all the extracts above, caregivers stressed the experience of their loved ones’ alienation due to their difficulties in expressing needs, understanding others, and progressive inertia. In extracts 9 and 10 caregivers use metaphors - ‘to be like a rag doll’ and ‘have empty eyes’ - to emphasize the objectification of their loved ones. In this context, they expressed their hopes that the CBD oil could make them more present.
Allows Person to Stay Alive
Caregivers had one more expectation, a result of the long-standing contact with a loved one in cognitive and functional deterioration. They have expressed an impossible desire to stop death and be with their loved one as before the disease one last time. In contrast to previously discussed arguments, that expectation was expressed indirectly with metaphors, like in the extracts below. Extract 10c. Actually I have mommy under control, I wanted to give her back some of her life. Extract 11a. I’ve decided to try CBD oil as well, it is my last hope… I have to do something before the disease completely takes my mom away… Besides, I’m already on the brink of exhaustion… Extract 12. CBD won’t fix if the lesions are very large, but often in severe stages it increases life comfort. (…) Well, there are many cases like that. And there you have nothing to lose.
The speakers use idioms – ‘give her back her life’ and ‘the disease takes her away’ to stress the economy of life and death. Dementia is an agent that slowly leads to death. It is also a disease and caregivers use the same heuristic as Western culture proposes in thinking about disease as something that can be cured. Also, in extracts 10 and 11 they position themselves as an agent, which suggests that they feel responsible for keeping their loved ones alive. This unfeasible task makes them exhausted, as they are failing again and again in finding a cure for dementia. In these extracts, the CBD oil is described as ‘the last hope’ that might keep their loved ones alive.
Those extracts show one more thing. It is characteristic that speakers decided to use omissions in their utterances. They dont explicitly say what their last hope is, what they can lose, what life they want to give back to their loved ones, and finally, what the disease has taken away. In this way, they are trying to mark linguistically something important to them that is difficult to name and articulate. The metaphors they use can suggest that they refuse to accept the progressive deterioration and eventual death of the one they love. Even if they mention the inevitability of death, they wished to stop its progression and return some of the life known pre-disease. As speakers discussed in extract 12, the purpose of it is to increase life comfort, but whose is unclear – the caregivers or those who live with dementia. Finally, they use a formula in that they ‘have nothing to lose’ to stress their determination in finding a cure and that they will not suffer if their actions are unsuccessful.
Theme 2. Motivations: I Have Nothing to Lose
Previously, we have described four different caregivers’ assumptions on how CBD oil works. In this part of our article, we have illustrated two factors that motivate caregivers to give the CBD oil to their loved ones. We start with discussing how sharing positive experiences by other group members affects their decision-making. In the second part of this section, we show their reluctance toward antipsychotic drugs and their search for an alternative to complementary treatment in the CBD oil.
IT Works for Others
Group members motivated themselves to start administering the CBD oil by sharing detailed stories about its effectiveness. Those who have been giving it to their loved ones for some time emphasized the many benefits from using it and pointed out that CBD oil ‘ended their nightmares’ and returned ‘more or less a normal life.’ For example, they described that the CBD oil was able to successfully manage the BPSD so they want ‘to do a lot around their loved ones again’. According to the caregivers, the CBD oil also improved communication as their loved ones with dementia were more talkative, ‘compliant,’ and less ‘offensive’. The caregivers mentioned the CBD oil improved the thinking and understanding of those with dementia, and made them happier, more ‘relaxed,’ and less ‘freaked out’. They also shared videos to prove that the CBD oil has improved movement, eating, and involvement in daily activities of those they care for. They stressed that, although the CBD oil didn’t stop the progression of dementia, the cannabis made it ‘tamed and silenced.’ One caregiver has summed it up as follows: Extract 13d. Loved ones - with the oil it’s good, calm, cheerful - today I am happy that I am in this Group - I have put my trust in you - with the CBD oil - because our everyday life is easier and nights are peaceful – I’ll also add that Mom speaks better, and cognizes well, also helps in her own way – she simply lives again.
The posts and videos mentioned above clearly inspired caregivers to administer the CBD oil to those they care for. They have stressed that this opportunity to read about the positive experiences from group members gave them hope in improving their life situation and encouraged them to try CBD oil. Extract 14b. I have been reading with passion, analyzing what you write and show and I have decided! I will try the CBD oil with my dad.
Making decisions about administering the CBD oil was not easy for the caregivers. It was mostly because they anticipated being mocked and rejected by others. That is why they declared their initial reservations towards ‘the miracle drug’, like in the extract below: Extract 15d. I also spent a lot of time thinking, reading, and analyzing [posts], because I’m a person who doesn’t believe in various quacks’ miracles - but I decided - and today it seems to me that I made the right decision - because it’s better. Mom sleeps better at night and is happier. We are at the beginning of the oil route because it has only been 26 days.
IT Helps me Reduce a Conventional Treatment
Besides the encouraging positive experiences of others, caregivers also declared that they started giving the CBD oil to their loved ones to avoid new medications. Group members have been aware that conventional treatment in dementia not only will not stop the progression of the neurodegeneration, but could also cause adverse effects. Thus, they have come to the conclusion that the conventional treatment is ineffective, overly burdensome, and potentially harmful. As a result, they sought to administer as few medications as possible, or even to completely abandon conventional treatments. Extract 16. I’ve been using the oil for almost a year right now for my father [who is] 90 years old and diagnosed with moderate dementia. Since I’ve been administering the 10% CBD oil to him, apart from standard medications such as donepezil, I don’t have to use any sedatives drugs such as tiapride, dad is cheerful and non-aggressive.
Even if they had been reduced or had to forgo conventional treatment, the caregivers still faced many challenging behaviors in their loved ones and have tried to manage BPSD desperately. In spite of their conviction that dementia is a disease, they have been looking for ‘a safer remedy’ that would help them to manage the dementia and its challenges, as illustrated in the example below: Extract 17. Going to the doctor we are hoping for help, but how can they help us if nothing works for this “trash”. Looking for help we try everything. (…) [P]lease don't be surprised by all those who are looking for help everywhere. We will be understood only by a person who will have been through this ‘hell’.
The CBD oil was described by the group members as a ‘safer remedy’ than a conventional treatment. They argue, as quoted previously in extract 16, that the CBD oil can be viewed as a form of complementary treatment that could replace more ‘dangerous’ medications. They also have revealed a belief that the CBD oil would help to revoke the side effects of previously administered medications. Extract 18c. I’m trying to make a somber assessment of the CBD oil’s effectiveness. I shall argue that they will “turnaround” the psychotropics effects. My mom was muddled twice: by progressive dementia and by drugs. Since she has been taking them, the progression of the disease has been frightful. I know I can’t cure dementia with the CBD oil, but maybe I can at least undo the damage done by the psychotropics? What do you think?
In particular, antipsychotic medications were considered to be overly burdening by group members. At the same time, antipsychotic medications are those medicines which are frequently prescribed to manage BPSD. Caregivers stressed that its prolonged administering caused significant harm to their loved ones and triggered new problems, such as: tremors, falling, or immobility. Consider the following examples: Extract 19. Dear Friends, Mom came home with her aortic valve replaced after 4 weeks in cardiology. It was a real rollercoaster but it worked out. Unfortunately, they have been giving her quetiapine, haloperidol, and oxazepam at the hospital for sleep. The side effects are visible. Her legs, hands and mouth are shaking. I decided to follow through with it and immediately administered her only 10% CBD oil. Extract 20. On January 12, a month has passed since the psychiatrist chained my mom to bed for good by prescribing lorazepam, after which she fell over in the night and I don't know how long she laid there. The first two weeks were a nightmare involving bedwetting, an anti-decubitus mattress and other things - my mom’s condition was such that I was already saying goodbye to her. And now the positives: the CBD oil, 3 drops till noon, 2 in the afternoon, awesome today as she tried getting up on her own in the morning, for several days now I’ve been seeing a significant improvement, I can sit her on the bed every 2 days, and even in a wheelchair.
In extracts 19 and 20, the caregivers communicate that they had decided to withdraw antipsychotic drugs as soon as they noticed their side effects (which is a medically recommended procedure). However, they have not only discontinued antipsychotic drugs, but exchanged them with the CBD oil, as well. One might hypothesize that their behavior displays a presupposition that dealing with dementia and the BPSD is impossible without any medication. The caregivers have decided to replace drugs with the CBD oil because they consider it a herbal medicine that should not cause any adverse effects. Here we can see a second presupposition, that the CBD oil is a safer alternative to conventional, ‘chemical’ treatments prescribed by physicians because it is ‘natural’. See a fragment of the discussion in the extract below: Extract 21. - Meds prescribed for dementia that our loved ones are taking are so strong that any herbal med won’t help. The CBD oil may have an impact on somebody who is not taking any chemical meds for brain stimulation. - It’s not true. There is a lot of literature that contradicts what you wrote. The thing is to replace these meds with the oil.
Theme 3. Instructions: There Exists a Perfect Recipe for HOW to Use CBD OIL
Since caregivers decided to start administering the CBD oil to their loved ones, they have been looking for instructions on how to use it effectively. In this part of our article, we will discuss the issues related to an unsupervised discontinuation of conventional medications by caregivers and their debates concerning dosage recommendations. In particular, we will highlight those aspects of caregivers’ beliefs which may be potentially harmful for people living with dementia.
Withdrawal of all Medicines ‘ABOVE the NECK’
The group members have revealed a belief that stopping the administering of antipsychotics to their loved ones is necessary for the CBD oil to work effectively. They have been actively discussing the rate at which antipsychotic medications should be reduced to minimize withdrawal side effects. Some of the caregivers declared that they have been minimizing dosages gradually, sometimes even for a few months. Others claimed that they resigned from administering all antipsychotic drugs overnight and then waited for at least 2 days to start giving the CBD oil to their loved ones. Regardless of which layoff method they have chosen, the CBD oil could only be administered once their loved ones were “cleared” from all antipsychotic medication. Otherwise, they shared a conviction that the CBD oil would not only be ineffective, but could also cause a myriad of adverse effects. Extract 22c. I know from my first trial that it is definitely a mistake to administer the oil at the same time as psychotropics. My mom was unhealthily agitated at that time and the caregiver couldn’t handle her.
Given caregivers’ aversion to antipsychotics, which was described in detail in Theme 2, we were not surprised that they conditioned the effectiveness of the CBD oil with complete withdrawal of antipsychotic medications. Some of them also declared withdrawal from procognitive, antidepressants, or even antiparkinsonian drugs. The caregivers have pointed out that these drugs can interact harmfully with the CBD oil by weakening or completely nullifying its beneficial effects. Moreover, some caregivers have admitted to discontinuing those medications overnight and substituting them with the CBD oil after 2 days. Some caregivers have also recommended resigning from antihypertensive medications after a month of using the CBD oil. In their opinion cannabidiol stabilized blood pressure and made these medications redundant. All those beliefs are expressed in a manifesto we present below: Extract 23e. YOU BLAST OUT EVERYTHING ABOVE THE NECK. ANYTHING BELOW THE NECK: ORGANS. YOU LEAVE THOSE DRUGS. Oil doesn’t kill… you won’t poison. And the psychotropics you give… they kill little by little… maybe not literally because some people will lynch me right away… but they’re slowly taking away a lot of functions… speech, movement, the sense of peeing, etc. Thanks to the oil, you’ll withdraw the blood pressure drugs later because dad’s blood pressure will be exemplary healed by the oil, like in a 20-year-old.
In essence, caregivers have chosen to discontinue medications on their own. They declared not consulting about their decision with any physicians as they presumed doctors would not approve their abandonment of the conventional treatment and its substitution with the CBD oil. In effect, they were looking for other group members’ assistance in deciding which medications should be withdrawn, as presented in extract 24: Extract 24b. My dad is taking memantine under two different names, I don’t know why, and also bisoprolol, salicylic acid, valsartan, trazodone, and donepezil. From my understanding, I should withdraw trazodone and donepezil for sure. I’ve read that donepezil can be discontinued without any problem and there will be no side effects. It seems to me that I should also stop giving him memantine1 and memantine2, or at least limit treatment to one of them. I’ll still try talking to a neurologist, but I want to have a wider recon. Can you advise me on the topic of medication?
The caregivers have warned one another about the difficulties of the withdrawal period. They pointed out that during this time, their loved one’s body would ‘demand psychotropics’ and they would present a range of difficult behaviors - from increased agitation, aggression, to blood pressure dysregulation, excessive sweating, or even deterioration of communication skills. These difficulties were supposed to be temporary and last a maximum of 1 month. After having waited out this period, the caregivers were supposed to be rewarded because their loved ones would be ‘clean of drugs’ and they could finally start administering the CBD oil. See the extract below: Extract 25e. The oil has no side effects, but the body reacts differently to taking away the psychotropics. The oil is herbal and it’s hard for it to break through the chemistry, that is, neuroleptics, the organism reacts differently to the gradual lack of psychoactive substances. [I]t looks like a drug addict on a hunger strike. (…) It is easy to give psychotropics but harder get it out… unfortunately.
Reaching Recommended Therapeutic Dose of CBD OIL
The caregivers claimed that in order for the CBD oil to work effectively, it was necessary to administer a correct dose of the drops. Similar to issues with withdrawing medicines, the caregivers were looking for advice from other group members in this matter. The most recommended therapeutic dosage in the group was administering 4 drops of 10% CBD oil 4 times per day. This was the recommended dosage for people with any kind of dementia at any stage. The exception was increased BPSD severity, when they recommended the daily dose be elevated even twice. Extract 26e. The minimum dose for dementia is 4 drops of 10% oil every 6 hours… and with 5% oil you need to give a minimum of 8 drops every 6 hours. If the condition is worse, 6–8 drops every 6 hours-10%. When Senior is back in shape… then give 4 drops (10%) every 6 hr. to maintain the condition.
The important issue for the caregivers was reaching a proper level of cannabidiol saturation, which was expected to last for a minimum of 2 weeks. If a caregiver has not withdrawn medication “above the neck”, the group advised that this period could be extended. The group shared a belief that during this transition period, the therapeutic effects of the CBD oil may not have been visible. The caregivers presented two different approaches to reaching the recommended level of saturation. The first consisted of giving a higher number of CBD drops for the first 2 weeks to gradually reduce them to the recommended dose. The second represented the ‘start slow, go slow’ approach, starting with small doses of the CBD oil and gradually increasing the amount of drops until the desired state was achieved. Extract 27. We have been using [the CBD oil] for a year and a half on my dad, who is 82 and has advanced Alzheimer’s. We administer the oil at a concentration of 15%, 4 drops every 8 hours, so that the body is saturated all day. Of course, we reached this dose in small steps, starting with a single drop and observing what was happening. At the same time, we were slowly getting off psychotropics.
The caregivers have mentioned that besides the positive experience of other group members, they have been gaining knowledge about CBD and its dosing from: CBD oil sellers, pharmacists, doctors ‘from the family’, popular non-scientific articles written in English, popular science books, dementia trainers, professional caregivers, and paramedics. It is important to stress that none of them confirm consulting on the dosages of the CBD oil with physicians who routinely provide dementia care. Instead of highly trained and specialized medical personnel, they decided to look for other sources of knowledge about the CBD oil and instructions on its usage.
Discussion
In the present study, we wanted to understand caregivers’ attitudes towards cannabidiol (CBD) by describing their expectations, underlying motivations, and its application methods. Our purpose was to understand their reasons behind administering CBD to those they care for. Given that caregivers are responsible for the care arrangements, it is crucial to acquire information about this unique group. To our knowledge, this is the first study that has analyzed CBD trends among caregivers using thematic analysis.
We discovered that during the last 2 years topics concerning CBD have been vividly discussed in the largest online Polish support forum for caregivers. Our findings revealed that group members who identify as family caregivers were convinced that CBD can be helpful in treating the symptoms of dementia, regardless of its stages or etiology. They expect CBD to: reduce the BPSD of their loved ones, improve their cognition by reducing anxiety and anger, increase their daily activity, and finally, stop dementia and coming death. In that way, they share a belief that CBD is a panacea for the difficulties they have been facing which are well identified in the literature as the main causes of caregiver burden (Isik, Soysal, Solmi, & Veronese, 2019; Kim & Park, 2019; van den Kieboom, Snaphaan, Mark, & Bongers, 2020).
The tendency to use CBD for medical purposes is not exclusively specific to caregivers of people with dementia. As shown by Corroon and Phillips (Corroon & Phillips, 2018) most of the CBD users treat it as a form of self-therapy for multiple diverse medical conditions, among which the top three are: chronic pain, arthritis, and anxiety. Self-treatment with cannabidiol has also recently been reported by patients with eczema (Whiting, Duan, & Friedman, 2022) or depression (Wieckiewicz, Stokłosa, Stokłosa, Gorczyca, & Pudlo, 2022).
In this study, family caregivers have revealed a shared presupposition that CBD is an actual medicine. They were convinced that CBD is a safer alternative to conventional treatments because of its herbal origin which, in their opinion, guarantees no side effects. As they were dissatisfied with conventional treatments, which were perceived as being overutilized by physicians and burdensome to individuals with dementia, they turned to CBD oil instead. Caregivers have also felt encouraged about using CBD oil because of the positive reports shared by other forum members. These two motivations were similar to. (Welz, Emberger-Klein, & Menrad, 2018) who stipulated four reasons that people use herbal medicine: dissatisfaction with conventional treatment, past good experiences, positive aspects associated with herbal medicine, and family traditions. This is also aligned with the findings of Jolly, Tamir, Burum, & Mitchell, (2019) and Leszko (2020) who demonstrated that the desire to share experiences with others gave individuals a sense of belonging to a group, enabling them to find information about the disease and receive peer advice. In that context, it is worth noting that almost two-thirds of family caregivers reported being lonely, which is one of the main risk factors for caregivers’ burden (Victor et al., 2021). Thus, reading about the positive experiences of others serves as an encouragement to use CBD oil. Moreover, sharing positive experiences provides caregivers with a sense of belonging and prevents loneliness.
Our findings also raise some concerns about making healthcare decisions without consulting a healthcare professional beforehand. The participants in the. (Welz et al., 2018) study reported using herbal medicine without medical advice in cases of mild to moderate diseases and as an initial stage before applying conventional treatment. Similar statements were made by forum members in our study. Most often caregivers described administering CBD to individuals with dementia without any medical advice and relying solely on information obtained from non-expert group members. Therefore, individuals in our study operated contrarily to the ones in. (Welz et al., 2018) as they were convinced that CBD oil can be effective in severe stages of dementia and cannabidiol can successfully replace conventional medicines.
Caregivers in our study believed that CBD should be used under certain conditions to be effective. That is why they were looking for specific information about CBD oil sellers and producers, methods of CBD administration, dosage, CBD interactions with other drugs. Based only on the non-expert advice, they declared an overnight discontinuation of all medications ‘from the neck up’ or experimenting with CBD and conventional medicine dosages. Some caregivers reported that they did not consult with doctors about medicine withdrawal in favor of CBD oil, as they were afraid of being negatively judged. These findings are related to the widespread crisis of trust in healthcare professionals (Lewandowski, Goncharuk, & Cirella, 2021). As shown by Lu et al. (Lu et al., 2018), people who spend more time on Internet searches are more skeptical of doctors, unwillingly discuss their health conditions with them, and rarely follow their instructions. As a result, the positive effects of medical treatment are limited. Our study shows this problem to be of great importance for individuals with dementia who depend on the decisions of their relatives. Caregivers’ choices about self-treatment, even made in good faith, may be harmful for them. Prospective research should explore these issues further by focusing on communication between healthcare professionals and caregivers. Studies that identify barriers in communication about CBD and self-discontinuation of treatment are warranted.
Limitations
Although the study enabled us to explore caregivers’ behavior and attitudes toward CBD oil, a few limitations should be addressed. First, this study employed qualitative analysis, which describe that people do certain things but cannot show trends, such as how many caregivers administer CBD to their loved ones or how many of them engage in the dangerous practice of drug withdrawal overnight. Further quantitative studies in this field are required. Secondly, we rely on self-reports and we are not sure if caregivers truly have done what they claimed. Therefore, the findings should be treated with caution. Another limitation is that the study focuses on web users and they are considered to be a subpopulation of caregivers. Previous studies have demonstrated that caregivers who were younger, non-Hispanic white, and well-educated are more likely to use the Internet (Gell et al., 2015). Additionally, users who are literate online are able to successfully navigate online discussion groups. Therefore, our study population is not representative of the Polish general population of caregivers. Finally, due to the nature of the online forum for caregivers, where often sensitive topics are discussed, many forum users prefer not to reveal their true identity. Therefore, we did not collect sufficient sociodemographic characteristics of the forum users. Acknowledging that does not invalidate the results of our study, as our purpose was to shed light on possible caregivers’ reasons behind CBD oil’s use and growing popularity. Despite the limitations, results from this study are valuable and offer important insights into caregivers’ behavior.
Implications
Our findings have implications for healthcare professionals. Caregivers may use alternative therapies such as CBD oil because they are frustrated with available treatments. However, being classified as both a medicine and a supplement in some forms, CBD oil leads to caregivers’ confusion and potential frustration regarding its effectiveness, doses, and purity of content (Corroon & Phillips, 2018). Caregivers may also be unaware of potential interactions and side effects.
Healthcare professionals should be aware of the increasing popularity of CBD oil among caregivers and understand caregivers’ motivations. The present study highlights the need for an open, non-judgmental communication between healthcare professionals and caregivers. When healthcare professionals criticize caregivers’ decisions, they create barriers to communication. Lack of communication with a healthcare professional may lead to dangerous consequences including a decreased adherence to treatment, health complications, and a diminished quality of care (Tiwary, Rimal, Paudyal, Sigdel, & Basnyat, 2019). By listening to caregivers’ concerns, hopes, and providing education regarding dosage and potential drug interactions, healthcare professionals might be able to help them navigate through any confusing information about the disease and treatment.
The findings highlight the need for more studies regarding the therapeutic effects and safe delivery of CBD oil. Healthcare professionals need to acknowledge that online support groups play a significant role in developing decision making and they should learn more about how to support caregivers who may be struggling with assessing the reliability of information available online.
Conclusion
CBD oil is increasing in popularity among caregivers of individuals with dementia. Frustrated with a lack of effectiveness and the side effects of commonly prescribed medications for dementia, caregivers are looking for other therapeutic options that could help them to cope with the most common symptoms of dementia. This study contributes to our understanding of how caregivers navigate through treatment options and how they consult with each other and acquire knowledge about CBD using an online support forum. Although participating in the online forum may give caregivers a sense of belonging to a group, making healthcare decisions by consulting with other caregivers instead of discussing it with a healthcare professional can lead to negative health outcomes. Such practices promote dangerous self-treatment practices and reduce trust in healthcare professionals.
Footnotes
Authorship Contribution Statement
Kłosińska, Urszula Kłosińska: Conceptualization, Formal analysis, Methodology, Project administration, Writing - original draft, Writing - review and editing.
Leszko, Magdalena Leszko: Conceptualization, Data curation, Investigation, Project administration, Writing - original draft, Writing - review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The project was approved by the Ethical Review Board at the SWPS University of Social Sciences and Humanities in Poland (No. 09/P/04/2022) on April 28, 2022.