
Abstract
Drug consumption rooms are one of the harm reduction interventions to handle complex social problems. The Helsinki city initiative puts drug consumption room (DCR) on a government agenda in Finland, which has also triggered a broader discussion. This study presents how stakeholders problematise and what solutions they propose for DCRs. The research is based on in-depth interviews of 23 stakeholders and the theoretical perspective of Bacchi’s approach – ‘What’s the problem represented to be?’ (WPR).
The results show that while stakeholders’ solutions resemble each other on the core DCR functions, the variations are found mainly in the introduction of extended services, policy development strategy, types of drug allowance in DCRs, and drug testing options. Stigmatisation of PWUDs still leads the harm reduction services to be considered from a moral framework. Stakeholders tend to take their positions according to strategic considerations related to electoral politics, expedience and the symbolic role of policies.
Introduction
Wherever proposed or established, drug consumption rooms (DCRs) have become a matter of public concern and have led to intensive political and professional debates (Fitzgerald, 2013). DCRs, also known as ‘medically supervised injecting centres’ or ‘safe injecting facilities/sites’ are places where illicit drugs can be used under hygienic and safe conditions, supervised by a professional staff. DCRs aim to reduce health problems caused by problematic drug use, improve access to social and health services for people who use drugs and decrease the nuisance associated with drug use in public spaces. DCRs have been operating in Europe, Australia and Canada over the last three decades. The first facility was legally established in Bern, Switzerland, in 1986. Currently, there are over 100 DCRs globally (Belackova et al., 2019; Kennedy et al., 2017; The International Network of Drug Consumption Rooms, 2021).
Controversies around DCRs involve complex interactions between different actors, such as harm reduction and drug treatment professionals, politicians and other policymakers at the local and national levels, law enforcement, local residents and people who use drugs (PWUD) as well as their friends and families (Jauffret-Roustide & Cailbault, 2018). Similar progress was initiated in Finland, where a more restrictive drug policy approach is adopted than many European counterparts, even the Nordic countries.
Until the 1990’s, drug policy in Finland was a minor issue and it was concentrated on reducing drug-related crime. Law enforcement and the Ministry of the Interior played key roles in both policy and practice. Nevertheless, the policy changed when there was a major increase in drug usage and accompanying problems in the second half of the 1990’s. These circumstances forced authorities and politicians to reconsider national drug strategies and policies, resulting in the formation of a Drug Policy Committee and, eventually, the adoption of Finland’s first and only national drug policy strategy in 1997. There were disagreements on this drug policy committee about how to define drug issues. The two main opposing camps were the law enforcement authorities, who advocated for a drug-free society and insisted on strict control policies, and the social welfare, health and criminal policy alliance, which favoured a harm reduction approach. Harm reduction at the time referred to two contentious issues: opioid substitution treatment and needle exchange programs. The end result – the drug strategy’s goals and metrics – was a compromise between the two logics, which has since paved the way for further elaboration of the harm reduction policy as well as stricter criminal controls on drug users. This drug policy model and the actions that follow it have been prevalent throughout the 21st century. Both repression and harm reduction activities have grown side by side without challenging each other much (Tammi, 2007).
Concerns on high-risk PWUDs enforce municipality to find a local solution, which contradicts the national drug approach that frames drug use within prohibition regime (Unlu et al., 2021). Hence, city-level initiative triggers a discussion not only among residents but also experts, politicians and civic communities since it requires a law change to establish a DCR. The city council proposed legislative change from the government but it is still waiting at the ministry’s desk without further progress.
Even in countries implementing decriminalization policies (such as Portugal), DCR establishment remains slow (Pinto de Oliveiraa et al., 2020). Particularly in countries where drug possession is illegal and drug use is stigmatised such as Finland, launching a DCR is a challenging policy initiative. Thus, opening a space where drug use is allowed (within harm reduction principles) might be controversial and even in breach of existing laws. Fueling the intense political debates, DCRs tend to be discussed beyond their expected health outcomes. This is the first research that aims to evaluate the current DCR policy progress from stakeholders’ points of view in Finland. More specifically, by using Bacchi’s WPR framework, the paper focuses on how stakeholders problematize the DCRs and formulate solutions different from the current approach, and to what extent and in which areas their problematisation resemble each other and vary among them.
Framework
Post-structural approaches have been widely used in the drug field, which mainly discusses why policies, strategies and interventions bring problems into specific frame to define the solutions (Duke, 2013; 2020; Kammersgaard, 2020; Lancaster et al., 2015; 2020; 2020; Lancaster & Ritter, 2014; Moore & Fraser, 2013). In other words, problematisation refers to how certain things become the objects of government and what ‘solutions’ are posed for these emerging ‘problems’ through policy and proposals for change (Bacchi, 2009, 2012).
Bacchi’s ‘What’s the problem represented to be?’ (WPR) approach aims to reflect ‘how we are governed and the material-discursive effects of such practices’ (Lancaster et al., 2020, p. 3). The analysis includes day-to-day policy practices and how problematisation is constructed and presented (problematised) (Berends, 2020; Lancaster & Ritter, 2014). Thus, WPR focuses on ‘problem questioning’ instead of the conventional means of policy analysis, ‘problem solving’ (Bacchi, 2009). This entails a new approach to consider drug policy within power and contestation contexts (Bacchi & Goodwin, 2016). Thus, the new way of thinking requires incorporating the roles of multiple actors, such as stakeholders, politics, ideas and values (Berends, 2020). By focussing on discourse in action, WPR enables us not only to identify the representation of problems but also to trace their development and evaluate their effects on the operations of government (K. Brown & Wincup, 2020).
While most of the studies employ policy documents for analysis, this study is made through discourse analysis of interviews with stakeholders. Bacchi (2012) suggests that interview data requires a particular approach to analysis, as interviews do not advance proposals in the same way as policy documents. She suggests the examination of interview texts with attention to what it was possible to say in the circumstances. For this study, professional stakeholders are representing their sector’s position in the way that problems are understood. Thus, for example, solutions put forward by those in criminal justice may be about the perceived ‘problem’ of public safety posed by PWUDs.
Power and knowledge play an essential role in the study of problematisation (Houborg et al., 2020), where stakeholders have a greater influence on problem construction and framing, such in this case that the progress is tied to legislative change. In the previous harm reduction reform (needle exchange points) in 2000’s, experts played an essential role by building a network, leading the public discussions and pressuring the government (Tammi, 2005; Unlu et al., 2021).
A local DCR initiative was filed in March 2018 by a Green Party city councillor in Helsinki. The city initiative does not propose a detailed plan for DCRs, instead, as the name suggests, it is about ‘to explore the possibility to establish a space for supervised injecting’ (Helsingin kaupunginvaltuusto, 2018). The initiative offers a new approach (without specifying any services but a space/room) when dealing with PWUDs who injects drugs. Thus, the participants were asked more about how current policy formulates drug issues, what kind of problems PWUDs are experiencing in this system and how this initiative would be relevant to solve these problems. By examining the ideas of stakeholders, we could observe how a certain way of thinking about problems could reflect specific institutional and cultural contexts (Lancaster et al., 2015; Small, 2016). Understanding the political and governmental rationalities shows us ‘how governing takes place’ and ‘what it is possible for us to become’ (Bacchi & Goodwin, 2016, p. 43).
Bacchi (2009) outlines a series of key methodological questions to make problematisation more visible in policy analysis and suggests that ‘every question need not always be addressed in every analysis, although it is useful to keep the full set of questions in mind’ (p. 111). Thus, we structured our analysis based on two main questions within the WPR framework: (1) How are DCRs framed as a policy problem by stakeholders, that is, ‘what’s the problem represented to be?’, and (2) How do the opinions of stakeholders represent the causes of and solutions to drug problems, and what are the values and assumptions which underlie these claims? The results section of the paper explores these two questions and examines how the ‘problem’ of DCRs is represented in the various strands of the response and the assumptions underpinning these representations. The discussion section also takes up the question of the silences (what is left unproblematic in the problem representations) and suggests alternative ways of thinking about the DCR ‘problem’.
Method and Analysis
Qualitative interviews began after approval by the THL Ethics Committee 1 in February 2020. Correspondingly, some participants were also obligated to get ethical approval from their institutions. The participants were asked 12 main questions (15 more sub-questions depending on their responses) about how they describe the drug problem in Helsinki, how they conceptualise DCRs and their relevance to the Finnish context, what do they think about services that could be provided in DCRs, how do they frame their justifications about the location, restrictions and house of rules in DCRs, types of drug administration, drug testing and management of DCRs and finally how PWUDs are served within this current system. The interviews were conducted in English, which is widely used in the public and private sectors in Finland. All the interviews were recorded with a written consent form and then transcribed. To reduce potential language limitations, the transcripts were available to participants for clarification and corrections upon request. During the research, the Covid-19 pandemic spread, which affected the study period and interview settings. Although we initially set aside 4 months for data collection, the unexpected circumstances extended the process to 8 months. Thus, the data was gathered between February and November 2020.
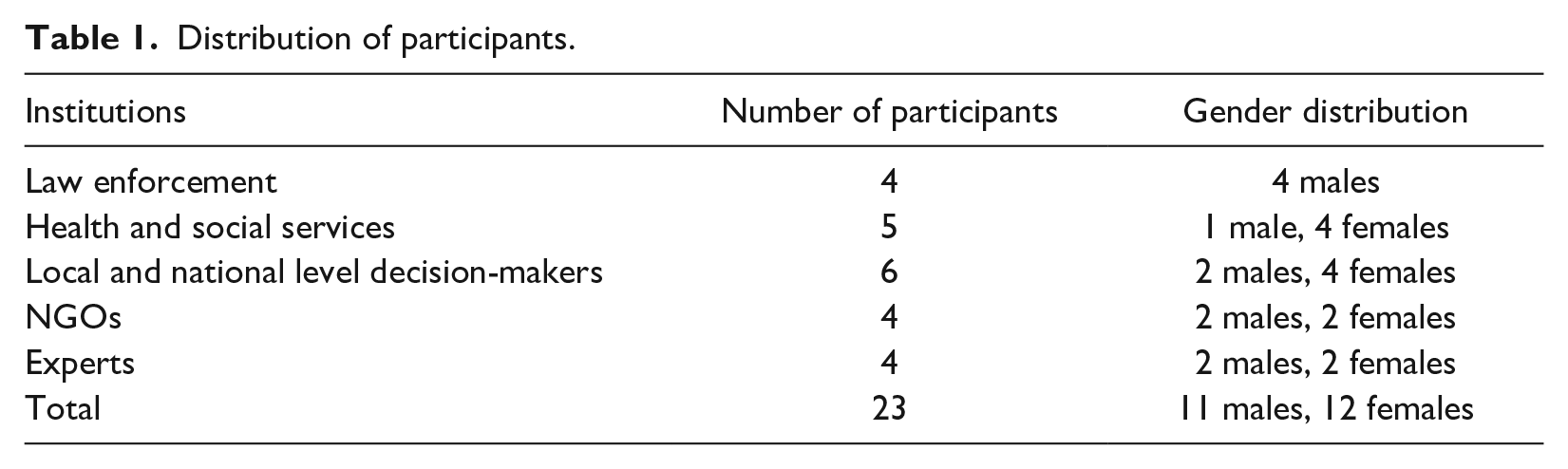
We initially used purposive sampling to reach key actors from stakeholders. Research participants were identified among professional networks, the Helsinki City Council and ministries. Each actor was selected based on their role in harm reduction centres, administrative roles in public institutions or NGOs, professional expertise, stance on DCR voting in the city council, statements and media appearances. Participants were invited through e-mail, and then the sample size was expanded through the snowballing technique. Seven candidates explicitly declined to participate in the study, while 12 candidates never responded to invitations; these were mostly from political parties opposing the DCR initiative. Overall, while 71 % of the invitees responded to invitations, 54% of them participated in the research. We conducted interviews with 23 people (each lasting an average of 1 hour) – 11 males and 12 females (Table 1). While 12 of the semi-structured interviews were conducted in face-to-face settings, online meeting platforms were used for the rest. The participants represent five different sectors: four key actors from law enforcement (police officers of different ranks and positions), five from health and social service providers (nurses and health specialists from low-threshold centres, including public and private organisations), six from decision-makers (including bureaucrats from ministries, local administrators and politicians), four from NGOs (administrators, field and health experts and activists) and four from policy expert networks (academics and researchers) (Table 1).
Distribution of participants.
Some of the interviewees work at the various facilities that offer services to the most marginalised PWUD. As ‘key informants’, these experts provided a depth of information about the current drug situation, harm reduction services and public order problems related to PWUD (Bryman, 2015). Besides, local and national-level politicians representing different political views were invited to take part in the research after establishing the DCRs tied to legislation. To have the voices of opponents and proponents, invitations were deliberately sent to members of political parties and public figures whose positions on issues were known.
Data were analysed using the Structured Framework Analysis technique (Spencer & Ritchie, 2002), which involves a sequential step process of reading and re-reading interview transcripts until the researcher becomes familiar with the content. Data were then analysed using the NVivo software package (version 12) through line-by-line manual coding of meaning units to create themes in an inductive process. After subsequent iterative rounds, themes were merged into the larger parent codes when patterns and links were identified (Evans & Lewis, 2018). The thematic analysis enabled us to identify patterns and themes within the data.
Within each topic, discourse analysis was also used to convey the meaning of the language participants used in the interviews. The analysis enables the identification of the way concepts are expressed and an examination of the actual words used (G. Brown & Yule, 1983). The process aims to reveal socio-psychological characteristics of the speaker rather than the structure of the text, which will guide us in interpreting participants’ words within the WPR approach used here. Validity checks were done by authors sequentially (Cho & Trent, 2006). Finally, the participants’ anonymity was assured by removing personal identifiers (such as their roles and positions) but kept their sectoral-level information to shed light on their professions.
Results
Conceptualisation of the Drug Problem
One of the functions of DCRs is to decrease overdose drug deaths (Elliott, 2014; Kennedy et al., 2017; Kimber et al., 2005; Small, 2016). Nevertheless, field experts assert that DCRs would not serve as a direct intervention in overdose deaths in Finland since buprenorphine constitutes the leading substance for drug deaths, where overdosing immediately after injection is unlikely. Still, the alarming progress in overall drug deaths among the young population alters the views of more conservative groups and opens room for alternative solutions. For instance, a police officer explains how law enforcement views the DCR as an option: ‘Maybe it's time to look at it the other way around. . . treat people better …I think the police organisation is always very against that kind of policy. But I believe that now in Helsinki, we are changing to thinking. . . because we see that this war is lost.’ The majority of the study participants interpret ongoing increase in drug-related deaths is primarily related to a prohibition drug regime, which inhibits PWUDs from getting timely health support when needed. Thus, DCRs are seen as a pathway change since the current approach fails to save those lives.
There is almost a consensus among study participants that the primary function of a DCR is to connect isolated and marginalised groups to the health and social care services. Although needle exchange service points have been serving a similar function for two decades, their impact is limited to stopping the spread of the HIV epidemic and other infectious diseases but still unable to reach the most marginalised PWUDs. According to a harm reduction expert, ‘There are a lot of persons outside of the services, even though we have quite a good network of low threshold health service centres. But we estimate that they can reach like 50 to 60% of injecting drug users in Finland’.
Furthermore, the drug treatment policy is criticised for not functioning effectively in providing accessible and inclusive services to high-risk PWUDs. Treatment limitations of stimulant users, long queues, insufficient public resources and high standards of treatment entry (such as full sobriety) are seen as the primary barriers for PWUDs. For instance, a harm reduction expert in an NGO says that ‘when people want to go to rehabilitation, they have to prove that they earn it. They have to take enough points from the evaluation forms or scales. Do you sweat? Or does your heart go up quickly? They (the nurses) ask all these kinds of things, and if you have too few points, then you are not sick enough. So, you can go home or you can go with your friends and everybody hopes that you are doing okay’.
Another problematisation pushing the DCR in the policy agenda as a potential solution is based on the perspective of human and social rights. According to a policy expert, ‘DCRs are not solving all the problems, but it’s much better than the current situation! DCRs are for the people who are not using the current services…DCRs could reach so-called ‘hard to reach and hard to treat people’ who may not use other health services’.
In this conception, the focus is not on the authorities’ ability to control the drug situation but on the needs and rights of PWUDs to appropriate services. As a result, DCR is more likely conceptualised from a human rights framework that basically aims to eliminate stigma and discrimination toward PWUDs and address substance use disorders as public health problems instead of criminal justice issues (UNGASS, 2016). A more inclusive approach recognises PWUDs as members of the society and offers services with equity principles. Stakeholders’ perspectives reveal that DCRs symbolise more than a room or space, instead a desire to change the current approaches. Prohibition, stigma and discrimination leave high-risk PWUDs behind the social and health services.
A DCR model and services
The majority of the participants defined DCR as more likely an integrated facility that targets hard-to-reach and hard-to-treat people, tailored to Finnish settings, similar to those in other European countries, which is believed to serve the sort of most vulnerable subgroups of PWUDs. Particularly, DCR implementations in other Nordic countries (Denmark and Norway) and western European countries like Germany and the Netherlands constitute a convincing reference for DCR accomplishment (Hedrich et al., 2010). For instance, a field expert in municipality says that, ‘there has been a lot of studies. . .made on DCRs around Europe and how they’ve been very successful in contacting and getting people into services, and then and cleaning up the indictment. I think in Denmark, they’ve been doing it good’.
Tested and evaluated long-term outcomes makes DCR a good alternative policy intervention. Thus, the expected DCR structure significantly differs from the standalone models developed in Canada or Australia (O’Shea, 2007). Furthermore, some participants infer that the DCRs are the only solution to solve complex drug problems, and they might be part of the answer, but a more cohesive approach is necessary to respond to the problem properly, such as improving treatment services and introducing, a take-home naloxone prescription.
Since Finland does not have such a vast PWUD subgroup, participants articulated that running an integrated facility would not put a heavy burden on public resources. Based on budget constraints, even extended services like sheltering, washing machines and food services are inferred, but essential health and social services that ease PWUD daily life were mentioned as the core functions. They conceptualised the DCR as an inclusive institution to reach marginalised people who are out of the current programme’s reach. In principle, participants supported DCRs regardless of which one of the two different problematisations they were referring to. However, when the components of DCRs were asked in more detail, the diversity of the responses becomes more evident among participants and reflects the personal preferences and sectoral division. For example, participants from law enforcement put more emphasis on the management of the drug situation and the public health benefits of DCRs, such as providing a safe place and clean equipment services. On the other hand, experts from health and social services listed a wide range of DCR benefits, including, but not limited to, providing data to allow authorities to monitor drug trends, informing the PWUDs and the general public about drugs, teaching safe drug use and preventing infectious diseases. Nevertheless, drug-related deaths and improving the health status of PWUDs constitute the primary common ground across sectors for the benefits of DCRs.
Policy Development Strategy
Our study participants have a variety of views on strategies to establish DCRs. While some believe that the problematisation of DCRs from a public order and nuisance perspective would be substantial leverage – since it may increase the likelihood of getting public support – others think that it should be discussed within the public health framework. Since most ordinary people’s knowledge about DCR and drug problems is generally limited to newspaper articles and media streams, experts point out that public interest tends to concentrate on security concerns. Literature shows that emphasising public nuisance contributes to the involvement of local stakeholders and residents in DCR process (Smith et al., 2019). For instance, a stabbing case between PWUDs in the Oodi library downtown brought a lot of public attention and even opened rooms for DCR discussions (Sinisalo, 2020). People would consider alternative solutions to make public spaces safer and cleaner when it could possibly affect their daily lives.
Although this type of generalisation reduces the comprehension of complex issues (Bjerge et al., 2020), the DCR policy is too specific to enlighten the general public. According to a policy expert in a ministry, ‘Finland doesn't have an opinion because not all, maybe only 10% knows that the whole thing exists. But I would say that. . . it has to come from the angle of street security and general security. I think this is the way to buy or sell this to people. . . While it’s a human rights issue. . .it is like a duty to help people. . .it’s kind of a form of harm reduction…but sorry, that doesn't fly with most people in Finland, I would use this security, safety, cleanliness path and path to treatment’.
On the other hand, some of the participants insist that it should be discussed within the public health framework. To discuss the problem within this framework, experts utilised statistics to create its rationale. Statistics, in terms of ‘institutionalised numbering’, is another tool for problem presentation or being critical of the policies (Lancaster et al., 2020). While drug-related deaths among the younger population are higher than the average in Europe and still rising in Finland, DCRs could provide an inclusive health approach to alleviate the problem (The European Monitoring Centre for Drugs and Drug Addiction, 2020).
According to a national policy expert, ‘it’s always this one time a year when they publish EMCDDA data about drug overdose deaths, and Finland has 3 years in a row of such casualties rising. And it’s looked a little bit bad because we are nearly the only country in Europe, apart from Estonia and Sweden, where the deaths of under 25-year-olds have risen in recent years. . .this is about what we want to show the public and about showing the users that we care’.
In drug and mental health policy, PWUDs are experiencing problems not only because of their inability to use health care services but also due to systematic errors that hinder their access to these services (Bjerge et al., 2020). Since PWUDs are part of society and they deserve to be treated with the respect of ‘human dignity’ as a requirement of the welfare state and democratic society, the importance of an inclusive policy should be acknowledged by combining two perspectives.
According to a municipality health expert working in the field, ‘Yes, safety is one framework and I can see it as something that would possibly work for people to understand the importance of a DCR who don't use drugs. And then money always talks, we need to talk about. . .HIV costs to the country a lot of money. One diagnosis of HIV costs a lot of money to take care of. . .treatment in hospitals is expensive. Prison days are expensive to taxpayers. That is one way of explaining to people who don't use drugs why we need DCRs but also that humanity is one entity. I think we need a wider-level discussion of how we treat others. People need to discuss openly about…values. . .we also need to treat each other with respect and humanely and I think it needs to come from that’.
According to this notion, while public order and nuisance framework, economic costs of treatment, HIV and prosecution provide a common ground for people who do not use drugs, it is not fair to restrict the discussion only in one dimension. Discussions should include alternative approaches and respecting others’ values and preferences when considering a human being.
Three different problematisations – public order and nuisance, public health and human rights – are used in strategic thinking about how to make policy viable. Except for health and social workers, no one emphasised putting the human rights theme into the policy strategy. Most of the participants think that the drug problem is not very visible to the public, and they are only interested in it if the event distracts from their daily life by public drug use, such as the littering from drug use and the public nuisance. Nevertheless, this type of disturbance currently can be perceived only in some parts of Helsinki, but for the DCR establishment, support from parliament is needed. When considering overall public attitudes toward drug use in Finland, which is still framed from a moral perspective, decision-makers and politicians most likely consider framing DCR within a public order and nuisance framework.
Extended services in DCRs
While the main expectation from DCRs is to reach isolated and marginalised PWUDs, several extended services (doctor visits, prescription services, food, shelters, lockers, washing machines, weekend and evening services, etc.) are offered to attract them in several countries. Nevertheless, stakeholders have different reference points on the range of services and operating hours. According to a policy expert in the ministry, who is ‘…a little bit concerned that it cannot be like really full house services or something like that. I mean, then people get a little bit jealous. . .(because) normal people need to queue for 6 hours to get treatment at healthcare centres and drug users can get full services. . . it could stir up a little bit of opposition’.
Likewise, a police officer said, ‘It’s fine for 24 hours a day 7 days a week, it is the best service. But do we have any services here? Except for hospitals and police?’ Similarly, a CEO of an NGO in the field said, ‘We have a social service for everybody. What I’m not sure about. . .is whether it is a wise policy to make separate services for (these) people. . . Perhaps normalisation would be more…profitable than integration with the services’.
On the other hand, a harm reduction field expert working in an NGO said that a separate facility with extensive services will inevitably reach these people. Otherwise, it would not be realistic to offer public services to this group. She said ‘if we have a Kela [the Social Insurance Institution of Finland] worker there once a week. . .the clients could also go to Kela, but they never go, and if they go and talk too loud, they would be kicked out. The point is that we will gather these sorts of ‘problem makers’ into one place and give them their services there because it’s good for these marginalised people. But on other hand, it’s also good for the general population because these types of people would not be sitting beside normal people in the Kela rooms. So, we can at least . . .play this way’.
Since drug use is still stigmatised behaviour, experts are concerned with justifying public concerns. According to a municipality health expert, ‘We need to discuss it more openly in the media as well as people who use drugs or who are homeless. It’s not something to be envious of . . .this is not a great lifestyle. . ..It’s not something that you would want yourself. . .we need humanity, and it would be inhumane…to not give certain services to people who are already on the streets living off . . .possibly prostitution and . . .not eating every day’.
The polarisation of views shows that the key question of what services should be provided is contingent on how much do PWUDs deserve, which is the ‘problem’ with scarce resources. Participants seem to be unconvinced to allocate these scarce recourses to PWUDs and they are looking for stronger justifications for public approval. If drug use is more likely framed within moral values, a kind of normality principle tends to be the more prevailing argument, and only basic health services are considered as an appropriate intervention to reduce drug-related deaths and harm, and this may alleviate the main public concern. On the other hand, problematisation from the harm reduction and human rights points of view hold that high-risk PWUDs deserve extra care and extensive services that may ease their daily life.
Route of Drug Administration
The conceptualisation of drug allowance in DCRs rests on diverse lines of reasoning. The first one is to provide service only to the high-risk PWUDs who are mostly injecting drugs in Finland. For instance, a harm reduction expert pointed out that ‘because there are a lot of injecting drug users in the Nordic countries, especially in Finland. And this is one kind of service we are missing. . .If you try include everything in the pilot, it never starts. . .maybe you should just concentrate on the injecting drugs component in the beginning’.
The second problematisation is more likely based on the strategic planning of the pilot project. According to a university professor, ‘this entire concept is something that is really for those people who are really, let’s say, severely addicted to injecting. . . like heavy drugs and or so. So, I think we should, by all means. . . really try to avoid the picture that it's a sort of fun facility where you go to entertain yourself by using drugs. . .I think it should be tailored to a point toward people who are in a very bad situation and have pretty much already gone down the road in their drug use’.
This framing is also linked to moral values and a distinction between different routes of administration. Using drugs by smoking is portrayed as a recreational form of drug use compared to injecting. This also reflects the local drug situation since heroin smoking and crack cocaine are almost non-existent in Finland.
Likewise, prevention efforts, particularly focussing on infectious diseases, are considered the main targets of DCRs. Thus, a DCR is conceptualised as a facility to protect public health to a greater extent. The injecting use of drugs at the ‘harder end of the continuum’ seems to be an acceptable form of consumption in DCRs (Seear & Fraser, 2014). A police officer said, ‘to address the healthcare issue, it has to be connected to needle exchanges. So, I think injections, if we have the public health factor included. . .It’s not just a facility to pop into, have fun at and smoke and inject with people’.
A young politician reflected on the public perception of drug use and PWUDs who need help. According to him, a deprived image of PWUDs constitutes a reference for the justification of services: ‘that’s the group like the injection drug users, they need more help than these. . .if you call it ecstasy, and cannabis in which the users may be like normal. I mean, normal that they go to work, and you cannot say that they’re drug users’.
On the other hand, one policy expert suggests that the availability of a smoking room enables new opportunities to reach a wider group of customers.’ For instance, including a smoking room might have the potential to alter PWUDs’ behaviour in countries where the injection rate is high. A policy expert in a ministry said, ‘they (Norway) still have a heroin problem. So, they’ve tried to change their way of using from needles to inhaling because of safety considerations’. Likewise, a medical doctor in the private sector of the field said, ‘if there would be a facility for smoking, maybe some injection users would move on to smoking when they see some peers smoking…which may be less harmful’.
The majority of the participants are in favour of limiting DCRs to only drug injection, based on a variety of reasons. It shows that the harms from drugs are more likely problematised from a stigmatised perception of drug use rather than the effects of the substance itself.
Drug Testing
Since the discussion is mostly concentrated on the policy dimension, participants do not have detailed technical information about the drug testing procedures within DCRs. Thus, some participants pointed out the feasibility of the drug testing service. For instance, a policy analyst expressed her doubts about its practicality in the daily life routines of PWUDs: ‘I’m not so in favour of this drug testing. But maybe. . .we should have this option that if there is going to be some major problem with Fentanyl or some new . . .very dangerous, NPS . . .there could be some opportunities for fast tests. But otherwise, it’s such a dangerous thing that if you are not certain that those tests are going to yield the right result. . .if you have one dose and you have decided to use it, and then the test result is uncertain. Are you really going to . . .not use it?’
Another concern is the legislative and administrative dimensions of its operationality. One of the local politicians explained, ‘we have discussed a lot about this testing. . . but there we saw that the city’s general responsibilities are very far from the city’s role. . .If there is a need for that, is it going to be some national . . .body taking charge of that element? Or if it’s something that we just aren't capable of testing? So. . .we realised that may not be the main focus of the city’s responsibilities’.
Our results show that stakeholders generally support the idea of drug testing opportunities in DCRs. Nevertheless, participants generally agree that it is too early to include it in the DCR discussion at first. Likewise, a separate legislative change is required for drug testing, and pushing all this at the same time would not be the right step strategically.
For instance, a CEO of an NGO organisation said, ‘(it) would be wise if we could do drug testing before the use of the drugs. . .(but) if we take the drug sample. . .we are committing a crime’. Likewise, a field expert in the municipality said, ‘it would be good to have drug testing in the DCR. It would be important, and they’ve managed to do it in Denmark. It’s just a machine. But I understand that there is also legislation that is against it and that makes it very difficult. That would be ideal if we would have drug testing, but I think we need to start slowly. And probably if a DCR would be established. . .if we can just get the DCR first and then bring into the discussion . . .the drug testing’.
Defining the boundary of harm reduction services is a difficult task. For instance, a young politician explained the weakness of any intervention while drug accessibility is still a criminal act. ‘From a legal perspective, if we have DCRs, and then. . .if it happens there or not, I think. . .it will happen. . .sooner or later. . .that someone gets killed…by overdosing or using the wrong substance. . .it will happen that the workers and the user won't know that this stuff is different from what it should be, and then we have this discussion, okay, how can we avoid this. Then someone …suggests that okay, maybe . . .we should test the materials beforehand, and this discussion will eventually lead to that discussion on. . .should we have a legal market for substances. . .narcotics that are sold in places where. . .we can guarantee that it’s the government that sells the substance. We will eventually make stock for the black market, where you can sell anything – almost anything – as narcotics, and there is no liability or any judicial tools to solve the problems, wherein if the substance is something other than what you’ve been promised, you then have some legal rights’.
Although this notion discusses the different dimension of harm reduction perspective, it is important to keep in mind that DCRs have a significant impact on fatal overdose among PWUDs who use the facilities. No fatal overdose has recorded in any DCRs around the world (Potier et al., 2014), instead, there was a reduction in neighbourhood and city. For instance, 35% reduction in overdose deaths in the vicinity of the DCR (Insite) and a 9% reduction in the city of Vancouver (Kennedy et al., 2017).
The discussion shows that drug testing tends to be problematised in varying dimensions, including but not limited to technical, administrative, legal and strategic concerns. But the underlying theme shows that in the long run, the introduction of drug testing service requires extensive discussion. At the current stage, problematisation of the drug testing service is far beyond the harm reduction framework, which makes it less likely to be an option. Even if the technical administration and barriers were removed, it might be stuck in the limits of a moralistic approach.
Discussions
According to the WPR approach, the policy is a productive process. It not only constitutes but gives shape and meaning to the problem instead of merely addressing it (Bacchi, 2009; 2012; Lancaster et al., 2015). This makes an analysis of the policy discussions at different stages of the process important. Since the city initiative does not infer a specific model and services, uncertainties lead study participants to discuss the DCR in a wider context, such as general attitudes to drug use and PWUDs, political environment and perception of harm reduction programs in society. Besides, level of knowledge about the evidence of DCR(s), its effects on society and businesses, its overall cost-efficiency vary across individuals, which bring ambivalences in formulating a DCR in new settings (Strike et al., 2015).
Although DCRs are one of the harm reduction interventions, public attitudes led stakeholders to consider alternative presentations of DCRs. This notion also supports the previous findings in the literature. For instance, Jauffret-Roustide et al. (2013) observe how consecutive surveys, framing the issue in different ways, showed differing levels of the social acceptability of DCRs among the general public in France. When a drug problem is seen as a public rather than a personal problem, a policy transformation could be achieved more easily (Small, 2016). Nevertheless, the policy preference still matters to prioritise focus groups. For example, a similar study in Canada has shown that although the primary objective of the DCRs is to improve the health outcomes of PWUDs, the public is more likely to be in favour of DCRs when they are presented as an effective tool to reduce problems tied to public order and nuisances (Kolla et al., 2017). As such, re-openings of DCRs in Amsterdam in 1990s were in response to public nuisances and their establishment in Frankfurt were in response to the widespread visible ‘open scene’ of drug users in the city (O’Shea, 2007).
If the main aim of the public policy is to generalise the problem and discuss it more broadly (which is useful to formulate such societal interventions (Bjerge et al., 2020), public order and nuisance framework still ensure the moral expectations of society. Nevertheless, in this problematisation, the main focus here is the wellbeing of society, not to prioritise PWUD. The establishment of DCR will better serve society, which improves the sense of amenity, provides more protection and diminishes the fear of crimes that might be committed by PWUDs (Fitzgerald, 2013). This paternalistic notion problematizes these groups as addicts or criminals who are in need of either treatment or punishment (Hathaway & Tousaw, 2008). Thus, the aim of DCR is to clean up the inner-city with a policing focus such as removing public disorder and public drug use (Elliott, 2014). For instance, Watson et al. (2018), found that law enforcement in Canada expects from an intervention on illicit drug use to lead PWUDs to the treatment and rehabilitation when DCRs are considered. Participants from law enforcement in our study sample similarly problematised DCR from the health framework, but they do not consider it as a threat to weakening their role in keeping the community safe (Watson et al., 2018).
The only element included from the health perspective is the drug-related deaths that public concerns. By its establishment, DCR(s) would sustain this goal by reaching and including high-risk PWUDs in health and social care services. Over the last 5 years, the proportion of under-30 s in drug-related deaths has risen from 33% to 49%, and drug-related deaths have increased in the last consecutive years, which is clearly above the European average (The European Monitoring Centre for Drugs and Drug Addiction, 2020). These rates make drug death a sensitive issue not only among study participants but also for society. For example, in May 2021, two MPs posed an interrogatory in the Parliament asking what the government will do for the prevention of drug deaths among young people and if the Ministry of Social Affairs and Health will prepare new legislation needed for consumption rooms (Outi Alanko-Kahiluoto, 2021). Furthermore, in August 2021, Helsingin Sanomat (the leading newspaper in Finland) published an editorial on drug deaths that also referred to consumption rooms as a means for preventing drug deaths (Pääkirjoitus, 2021).
On the other hand, extensive services in DCR(s) are less likely supported even by most of our study participants. DCRs, as a harm reduction intervention, aim to reduce the harms of all sorts of drug use, which necessitates a non-judgemental, non-coercive provision of services and resources. This framework safeguards PWUDs’ sense of dignity and self-worth without necessarily stopping their drug use (Hawk et al., 2017). Nevertheless, participants restrict the services according to their perceived image of drugs. While people who inject drugs are more likely problematised as the most deserving group to get help, others are conceptualised as recreational drug users who do not need support. These concerns point out that stigma associated with drug use obscures the aims of harm reduction, which infers ‘weak rights’ to the PWUDs and prioritises public health over users’ rights or changes in their legal status (Hunt, 2004). Nevertheless, it is argued that legalisation debates and advocating ‘strong rights’ in the name of harm reduction policy could easily subvert this type of initiative (Hathaway & Tousaw, 2008; Hunt, 2004). These underlining factors may lead stakeholders to pay more attention to political aspects of the process.
Participants largely agreed on the benefits, models and basic services, locations, anonymity procedures and opening hours of the DCR. Nevertheless, there were also different opinions and disagreements about numerous details. Interestingly, a key point of departure for all of them seems to be to put a lot of emphasis on considerations of what would be acceptable for ordinary people, who more likely consider the issue from a moralistic approach. This kind of political realism also seems to leave more principal-based issues like the human rights of PWUDs in its shadow. Most probably, it also tells us that most of our participants think that opposition to DCRs among national politicians is prevalent, and showing a sympathetic attitude towards PWUDs would not be of great help when arguing for DCRs.
Thus, the problematisation of DCRs is similar and varies among the study participants, depending on contextual factors such as political environment, public support and legislation. Our results show that sectoral differentiation slightly appears with some levels of personal preferences. For instance, similar to the literature findings (Philbin et al., 2009), participants from the health sector have more supportive views on harm reduction and public health frameworks; their conceptualisation more likely merges with the rest on age and drug administration issues, which mostly reflects the moral boundaries of society. In addition, the capacity and power of actors formulating the potential measures for this problem also affects their problematization (Smith et al., 2019). For instance, while local authorities have more responsibility for providing health services, they tend to frame it within the health approach. Similarly, national authorities have more responsibility and power to formulate penal law, they tend to consider other dimensions.
Indeed, silence on the human rights issues indicates that in Finland, drug problems are mostly defined in terms of law and order or the public health perspective but not from the perspective of human and basic rights (Hakkarainen, 2021). However, according to the Constitution of Finland, the state should safeguard satisfactory social and health services for each citizen equally and without discrimination. These issues now are snowed in beneath the call for political realism. Instead of a human rights argument, stakeholders are divided regarding the public health framework and public safety/security framework.
While participants from law enforcement and some policy experts are more likely to problematise DCR as a potentially successful strategy within the public health framework, a policy expert in a ministry, as well as some health and social service experts from the field, thought that it would be a better strategy to discuss DCRs within the public order and nuisance framework. Experience of other countries shows that involvement of police voices in health policy, particularly in DCR establishment, is essential and productive since they represent the symbolic role of law-and-order responses. Law enforcement may offer an unambiguous moral direction that could justify the state endorsed moral ambivalence (Fitzgerald, 2013). Our participants from police reflect the main theme of the law enforcement statement on DCR that they are not against it, instead, looking for regulations in laws (Helsinki Police Department, 2018; Unlu et al., 2021).
The literature shows that despite scientific evidence and international legislation support, social and structural barriers inhibit the establishment of DCRs in many countries (Smith et al., 2019). Likewise, our results show that DCR represents one of the most value-attached harm reduction services. Even some field experts who are supposed to be behind this type of intervention seem to be somewhat sensitive to services provided in DCRs if they include extra benefits for PWUDs. It shows that stigmatisation constitutes ‘a potential subjectification effect of the production of the vulnerable subject’ (K. Brown & Wincup, 2020, p. 5) in determining what kind of services PWUDs can access and which type of drugs they are allowed to consume in DCRs. For instance, providing extended services in DCRs or allowing minors to use these facilities have the potential to trigger public discussions. Nevertheless, if their establishment is more likely structured within public health frameworks, such as stopping infectious diseases, reducing overdose deaths or public order problems, a consensus can be reached more easily. This coincides with the Smith et al. (2019) findings that when DCR is framed in a health policy as sufficiently severe to deserve attention, it is more likely to attract political support in Belgium. Seeing drug consumption as an individual responsibility constitutes one of the underlining factors in this rationale (Duke, 2013; Fraser, 2004). Thus, the solution of an individualised problem is more likely to be framed in the self-management of the cases, such as recovery.
Second, although the main expectations of DCRs are to improve the health conditions and daily life of PWUDs, framing the issue within the public order and nuisance framework is popular among the experts. It is interesting to find out that experts tend to conceptualise DCRs out of their sectors as a strategy for their establishment. For instance, participants from law enforcement define DCRs within the health framework, whereas health experts argue that framing the DCR within the public order and nuisance path would be a better strategy to get public approval. However, in spite of their supportive stances, the study participants do not seem to seek any common understanding or propose any collaboration between different actors or build up alliances to promote DCRs together. Indeed, in the interviews, their answers about leadership of the process were unclear and confused, most probably also reflecting a challenging situation in the administration created by the novel Covid-19 pandemic.
Another silenced area not talked about in the interviews was the role of PWUDs in the process. According to the guidelines of the Ministry of Justice, people who will be influenced by legislation should be heard and called upon to participate in the planning of statutes and services. In the interviews, no one took this up, which tells us how easily ‘silent groups’ like PWUDs are excluded from these kinds of societal processes, even when special services for them are being set up (Ritter et al., 2018). Thus, seeing PWUDs as passive policy subjects results in solutions that reflect a morally superior way of dealing with them (Bjerge et al., 2020).
Our results indicate that most of the participants tend to justify their problematization based on gaining public support. The literature shows that community members are concerned with the establishment of DCR(s) because it is a common belief that it would devastate their neighbourhood and harm reduction programs cause more harm rather than reduce it (Philbin et al., 2009; Wenger et al., 2011) but researches also indicate that insufficient information is the main source of public fear to harm reduction programs and when they have enough knowledge, they are also open for discussion (Smith et al., 2019; Wenger et al., 2011). The current level of public support does not get the attention that one deserves. For instance, the latest national drug survey from 2018 in Finland shows that 50% of the Finns totally or partially approve of DCRs, 36% are against and the other 13% answered that they don’t know (Karjalainen et al., 2020). We interpret this result as indicating that our study participants may be underestimating current public support for DCRs. In fact, instead of resistance, they might get support from the public. Hence, an active expansion of public debate would be a workable strategy for getting DCRs into use. Our study shows that based on different problematisations, stakeholders from different branches of Finnish society have several arguments for DCRs.
Culture is one of the principal barriers to DCR establishment in many countries since it constitutes the main source of political decisions and personal actions (Philbin et al., 2009). Particularly in countries where legalistic culture is eminent, people may insist that government is the sole authority to take responsibility and actions on these issues. Local attempts and community actions to improve environmental settings may face resistance or hesitation. Involvement and support of institutions, academics, bureaucrats, religious authorities, progressive politicians, community drug user groups and service providers are driving forces of cultural change regarding attitudes on drug policy (Hathaway & Tousaw, 2008; Philbin et al., 2009). On the other hand, well-organised civil disobedience is also another way of forcing the government to remove legal barriers in front of the DCRs, such as in Denmark. Local activists and organisations demanded DCR from the grass-roots level and insisted on solutions rather than problems to improve the conditions of PWUDs (Ankjærgaard et al., 2015). Civil disobedience, such as using a mobile DCR vehicle named Fixelance, was used as a form of engagement with politicians since they believed that the barriers rise not from laws but the politics (Ankjærgaard et al., 2015). Legalistic culture in Finland leads the initiation to start at the municipality level by progressive politicians but our results show that a multi-pronged alliance of actors is inevitable to put the DCR(s) on the government agenda.
Limitations
Although PWUDs are the natural stakeholders of this policy, they were not included in this study because broader research was planned to conduct need assessment and their DCR problematization. It is expected that their DCR problematization would differ to some extent from experts and decision-makers since they will infer the contribution of DCR in their daily life. Particularly, their problematization on extended services, drug testing and potential effects on reaching isolated PWUDs would provide better insight into the problems they faced and how DCR could improve their health and wellbeing.
Our data were limited mostly to the debaters who were in favour of piloting DCRs in Finland. As stated, with one exception, politicians who voted against DCRs in the Helsinki City Council were more likely to refrain from expressing an opinion on this subject. Their problematization would contribute us to comprehend to what extent moral values and stigma are attached to drug use and DCR in the Finnish context. Politicians prefer to voice their displeasure but are unwilling to go into detail about it. They may take into account more factors than the possible advantages or disadvantages of DCRs. Their opinion may change in response to changing political realities, but they may be hesitant to take a position while there is no active discussion in parliament. Nevertheless, this reservation and their arguments were also asked to other participants to reveal the underlining concerns and disagreements of the opposition groups.
Conclusion
By applying the WPR approach, we have identified different problematisations and solutions that show similarities and important distinctions within the DCR issue. The problematisation of the problem varies, reflecting either stakeholders’ personal preferences, professional cultures or special issues in question and political context. Stakeholders tend to take their positions according to strategic considerations related to electoral politics, expedience and the symbolic role of policies.
Our results show that the expectations of study participants from DCR(s) are to serve basic functions more likely from the public health framework, targeting high-risk PWUDs and connecting them to the social and health services, which in turn reduces drug-related deaths. Nevertheless, when extended services, drug testing and allowance of drug inhalation are considered, the harm reduction principles left their place to the stigmatisation and moral values. The public order and nuisance framework constitute the prevailing argument to shape the overall DCR policy process. Our results also indicate that the design of DCRs varies in different countries and is firmly attached to the socio-political culture of the society. Without changing ambivalent opinions and stigma/discrimination toward PWUDs, aversion to harm reduction services will remain persistent. That makes the human rights perspective important. Thus, besides awareness of harm reduction programs, a broader and open discussion is inevitable to alter public attitudes on drug use. Nevertheless, our study participants point out alternative framing strategies for policymakers to better address public concerns and design more favourable policies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research and/or authorship of this article. The first author received financial support for the research from the Kone Foundation [Grant No. 201906595].