
Abstract
This study described cannabis use behavior among college students in Berlin, in particular, differences in use motives between subjects with frequent use and those with signs of cannabis use disorder (CUD). Cross-sectional data were collected via an online survey among Berlin college students (N=9350; 50.7% women; Mage=24.4). Motivation scales were computed based on an exploratory factor analysis. Effects of these motive scales were compared using multivariate regression models, where the dependent variable was use intensity (ordinal), frequent use (twice or more per week, binary) or a positive substance use disorder screening test (binary). Cannabis use is known to be particularly prevalent among Berlin college students, which was confirmed by our data. The most frequent use motive was enhancement, which, however, was not associated with frequent use or CUD. The motives predicting frequent use (sociability) are different from motives predicting CUD (coping), even when controlling for a wide array of covariates.
Introduction
Cannabis is the most commonly used illicit substance worldwide (European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), 2020). Lifetime prevalence of cannabis consumption in the general population is estimated at 27.2% in the European Union (EU), while past-year prevalence is 15.0% for young adults (15–24 years; EMCDDA, 2020). Young adults are more likely to consume cannabis heavily and experience adverse effects of cannabis use (Hall & Degenhardt, 2009; Johnston et al., 2019), in particular, in Berlin (Jochmann et al., 2019). The reputation of Berlin as the capital of European nightlife and techno scene particularly attracts students interested in a lifestyle that is often related to drug use and substance use disorders (Ding, He, Shoptaw, Gao, & Detels, 2014; Kelly, Parsons, & Wells, 2006; Palamar, Griffin-Tomas, & Ompad, 2015). As a consequence, Berlin college students are particularly likely to use cannabis (Viohl et al., 2019) and might therefore be at high risk for CUD and use-related problems (Helmer et al., 2021).
While cannabis use prevalence has remained stable over the past decade, the demand for treatment for cannabis-related problems has increased by 76% between 2006 and 2017 in the EU (EMCDDA, 2019; Manthey, 2019). A likely explanation is the increase in cannabis use disorder (CUD) prevalence (Manthey, 2019). In Germany, cannabis use prevalence has increased seemingly without such an accompanying increase in cannabis-related disorders (Seitz et al., 2019). Frequent cannabis use increases the risk of dependence, nevertheless most subjects using cannabis frequently are not dependent (Foster, Arterberry, Iacono, McGue, & Hicks, 2018; Van Der Pol et al., 2013). Foster et al. (2018) show that subjects using cannabis frequently (weekly and more) reported more substance use problems and externalizing behavior than subjects not using cannabis; at the same time, subjects using cannabis frequently without signs of CUD have significantly less psychiatric comorbidity and psychosocial impairment than subjects with CUD. These findings highlight the importance of differentiating between cannabis use, frequent use, and CUD, where arguably the latter deserves the main weight in counseling and prevention targeting. As only a fraction of subjects with CUD seek treatment (Specht, Dauber, Künzel, & Schwarzkopf, 2020), the prevalence of CUD among Berlin college students was unknown prior to this study, even though this population with high prevalence of cannabis consumption may be at high risk of CUD.
Substance use motives may be seen as the final pathway through which more distal factors, both external (availability, use context) and internal (traits, affect, expectancies), influence use behavior (Buckner, Zvolensky, Farris, & Hogan., 2014; J. S. Simons, Gaher, Correia, Hansen, & Christopher, 2005; Vangsness, Bry, & LaBouvie, 2005). Recent literature gives an increasing importance to cannabis use motives, measured typically with one of several different motive questionnaires. Drawing on interviews with “young poly-substance users,” Boys, Marsden, and Strang. (2001) identify a series of use motives, giving rise to an 18-item questionnaire. The Marijuana Motives Measure (MMM) has been derived from models of alcohol motives and is characterized in five scales: enhancement, coping, social, expansion, and conformity (Simons, Correia, Carey, & Borsari, 1998). The Comprehensive Marijuana Motives Questionnaire (CMMQ, Lee, Neighbors, Hendershot, & Grossbard, 2009) identifies as many as 12 motive scales for use, including boredom, social anxiety, and sleep.
Subjects using cannabis frequent generally score higher on all motives (Beck et al., 2009; Bonar et al., 2017; Pearson, Bravo, Conner, & Parnes, 2019). The literature finds that coping motives are associated with more frequent cannabis use (Bonar et al., 2017; Mader, Smith, Afzal, Szeto, & Winters, 2019) and correlate with mental health problems and CUD (Beck et al., 2009; Phillips, Lalonde, Phillips, & Schneider, 2017). Subjects using cannabis stating social and conformity motives generally experience less psychopathologies (Bonar et al., 2017; Schultz, Bassett, Messina, & Correia, 2019). While we know that Berlin college students have a high prevalence of cannabis consumption, we know little about the use motives in this high-risk population.
Aside socio-demographic characteristics and use motives, certain personality characteristics are associated with more frequent cannabis use. Individuals with external locus of control (LOC)—defined as believing in a weak effect of their behavior on their future life events—are more likely to use cannabis (Heckman, Stixrud, & Urzua, 2006; Mendolia & Walker, 2014). Likewise, high impulsivity—defined as a tendency to show “rapid, unplanned actions regardless of possible negative consequences” (Meule, Vögele, & Kübler, 2011)—has been shown to predict substance use and use disorder (Acton, 2003). Hecimovic, Barrett, Darredeau and Stewart. (2014) that the literature has largely failed to provide a consistent pattern of personality traits among subjects using cannabis within the classical five factor model. They attribute this failure to the heterogeneity of cannabis use contexts and motives: Cannabis seems to differ from other substances, in the sense that it fulfills a wider array of different functions in subjects’ lives than other substances (O’Hara, Armeli, & Tennen, 2016), for example, ecstasy or cocaine.
The purpose of this study was twofold. First, this study aims at quantifying cannabis use and CUD among college students in Berlin. Further, the study examines the correlation between use motives and cannabis use and CUD in this population, controlling for personality traits and other factors in a multivariate analysis. Based on the literature, we hypothesize that (a) Berlin students have a higher use intensity and a high rate of CUD compared to similar age groups in other cities and compared to other population groups in Berlin, (b) the main use motive scales include enhancement, sociability and coping, (c) motive scales have significant impact on use intensity and CUD even when controlling for other covariates, (d) coping motives are positively associated with CUD, and (e) high BIS and external LOC are associated with CUD.
Materials and Methods
Sample and procedure
The cross-sectional data were gathered as part of the Student Drug Survey among students of 17 institutions of higher education in Berlin, conducted online between 11/2016 and 09/2017. Invitation was sent by the university via email to all students in public colleges in Berlin. Participation was incentivized with a lottery to win 100 Euro once or five Amazon vouchers worth 20 Euros each. Please refer to Viohl et al. (2019) for more details and the original version of the survey, as well as the full questionnaire. The study was approved by the Ethics Committee (application number: EA1/258/16) and commissioner of data privacy of the Charité University Medicine Berlin.
Questionnaire
Primary outcomes: Cannabis use and CUD
Cannabis use prevalence, excluding prescribed medical use, was assessed by self-report over the past month, past year, and lifetime. Respondents who indicated any use were further asked to report frequency (never, < monthly, monthly, 2–4/month, 2–3/week, >3/week). Interacting prevalence and frequency answers, a 9-level measure of use intensity was constructed similarly to Simons et al. (1998): 8 (>3/week), 7 (2–3/week), 6 (2–4/month), 5 (monthly), 4 (less than monthly, but within past month), 3 (less than monthly, but within last 12 months), 2 (less than monthly, but not in past 12 months), 1 (never, but has tried), 0 (never tried). Moreover, the four-item “Cutting down, Annoyance by criticism, Guilty feeling, and Eye-opener” Adapted to Include Drugs (CAGE-AID) screening test (Brown & Rounds, 1995) was used to screen for alcohol and substance use disorder (positive if two or more “yes” answers).
Primary predictor of interest: Cannabis use motives
Use motives were assessed using an adapted version of the questionnaire by Boys et al. (2001). Boys’ questionnaire assesses use motives for several substances, this study concentrates on cannabis. Therefore, we dismissed the item “keep going” which applied mostly to amphetamines and ecstasy. Inspired by the literature (Lee et al., 2009; J. Simons et al., 1998), we added three items (“to be creative”, “to reduce my fears” and “to understand others’ points of view”). This resulted in a use motive questionnaire with 20 items (5-point Likert scale).
Covariates: Socio-demographics and psychosocial factors
Information was collected about socio-demographic information, such as gender (woman, man, or free text input), age, and sexual orientation (heterosexual, homosexual, bisexual, or free text input). The level of religiosity was assessed (5-point Likert scale). Participants further indicated any diagnosis of psychiatric disorder. Academic outcomes were self-assessed by the participants with average grade (German grades from 1=very good to 5=fail). Personality was assessed along the dimensions of impulsivity and LOC. Impulsivity was measured using a short form of the Barratt Impulsivity Scale (BIS-15) (Meule et al., 2011), with total scores ranging from 16 (low impulsivity) to 54 (high impulsivity). LOC was measured using the questionnaire from the German socioeconomic-panel (Richter et al., 2017), with a final score ranging from 1 (external) to 7 (internal).
The raw data may be available to interested researchers on request.
Statistical methods
Data was analyzed using Stata 15. We excluded respondents who had too many missing answers (max. 20%), incomplete questionnaires, and implausibly short overall response time; for more details, please refer to Viohl et al. (2019).
We provided descriptive statistics on cannabis use prevalence, frequency and CAGE-AID screening test. A descriptive analysis showed overall means and frequencies of socio-demographic covariates. We provided a comparison (a) between the frequent use group and other subjects and (b) between CAGE-AID positive and negative groups, testing for equality using Student’s t-test for ordinal/continuous variables and a chi-square test for categorical variables. Across the study, our threshold for significance lies at 5% and we applied Bonferroni corrections for multiple testing.
We performed an exploratory factor analysis using the principal factor method. The number of factors was determined using parallel analysis (Horn, 1965), as implemented in Stata (Dinno, 2009). In order to reduce the number of items needed to explain each factor, we applied a promax oblique rotation, allowing the factors to correlate; scales were constructed based on items loading >.40 and excluding cross-loading items (procedure similar to Simons et al., 1998, or Grilo et al., 2010). Factors were labeled based on face validity. We computed the correlations and internal consistency (α after Cronbach, 1951) of the resulting motive scales; we consider α above 0.75 satisfactory and above 0.65 acceptable (Cortina, 1993; Taber, 2018). Only participants who indicated having used cannabis ever were included in the factor and subsequent regression analysis (N=4102) because use motives were considered interpretable only for those who actually use cannabis.
We performed linear ordinary-least-squares regressions predicting use intensity, both using only cannabis use motives (“unconditional”) and use motives combined with known cannabis use covariates from the literature (“conditional”). Graphical analysis was performed to check the distribution of the residuals for bias and heteroskedasticity. Further, we provided the results of unconditional and conditional binary logistic regressions, both on the outcome of frequent use and positive CAGE-AID, indicating potential CUD. We compared the results of unconditional and conditional regressions in order to assess whether use motives provide an explanatory advantage over more standard cannabis use covariates. The covariates included are: socio-demographic variables age, gender, and sexuality (Hemsing & Greaves, 2020; Vangsness et al., 2005); religiosity (Mader et al., 2019; Pinchevsky et al., 2012); LOC and BIS as known personality correlates of cannabis use/initiation (Acton, 2003; Helmer, Krämer, & Mikolajczyk, 2012; Mendolia & Walker, 2014; Vangsness et al., 2005); and an existing psychiatric diagnosis (Mader et al., 2019; Schlossarek, Kempkensteffen, Reimer, & Verthein, 2016). Grades were considered but not included in the regression because the descriptive statistics indicated that they were not linked to frequent use or CUD.
Results
Sample
Socio-demographic variables for total sample and subject with frequent use (cannabis use twice or more per week).
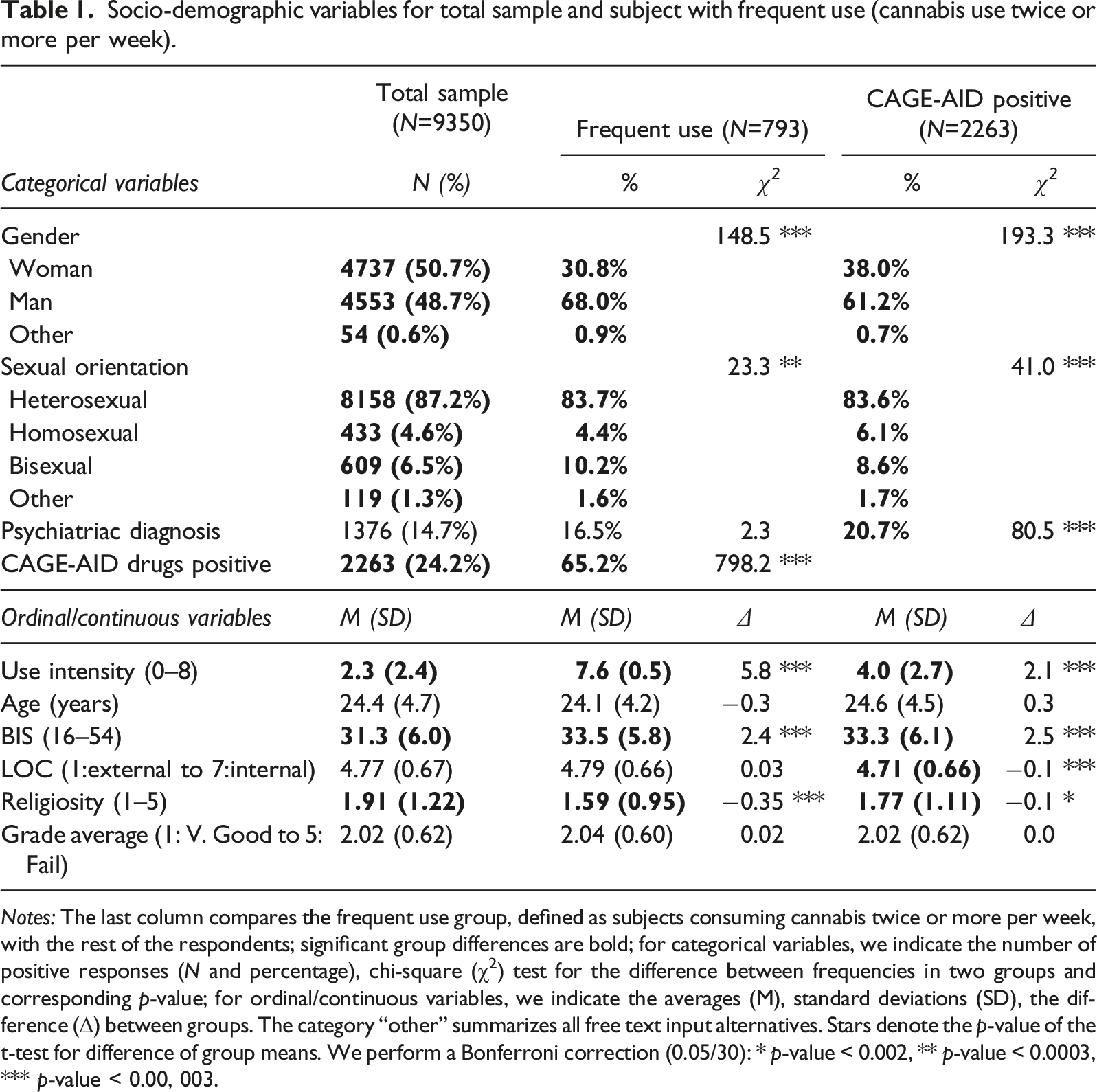
Notes: The last column compares the frequent use group, defined as subjects consuming cannabis twice or more per week, with the rest of the respondents; significant group differences are bold; for categorical variables, we indicate the number of positive responses (N and percentage), chi-square (χ2) test for the difference between frequencies in two groups and corresponding p-value; for ordinal/continuous variables, we indicate the averages (M), standard deviations (SD), the difference (Δ) between groups. The category “other” summarizes all free text input alternatives. Stars denote the p-value of the t-test for difference of group means. We perform a Bonferroni correction (0.05/30): * p-value < 0.002, ** p-value < 0.0003, *** p-value < 0.00, 003.
Cannabis use prevalence and risk factors
Cannabis use prevalence over the past month was 23.9%, over the past year 41.5% and lifetime prevalence was 67.1% (as in Viohl et al., 2019). Among those indicating having used cannabis in their lifetime, the majority (70.1%) used it less than monthly, while 8.3% consumed cannabis monthly, 9.0% 2–4 times a month, 5.4% 2–3 times a week and 7.3% more than 3 time per week.
Figure 1 shows the distribution of subjects across use intensity (yellow bars). The largest group is the subjects who never used cannabis. Figure 1 also shows the share of subjects with a positive CAGE-AID test within each use intensity level (blue dots). Overall, 24.2% of the respondents had a positive CAGE-AID screening test, and Figure 1 shows that positive CAGE-AID was more frequent in respondent groups consuming more cannabis. In this study, we will focus in particular on the group of subjects with use intensity of 7 or 8, that is, subjects consuming cannabis twice or more per week. In this group with frequent use, the share of subjects with a positive CAGE-AID test is over 50%, so that we considered them a group at high risk of CUD. Histogram of use intensity (left axis) and share of respondents with a positive CAGE-AID screening test, indicating potential CUD (right axis).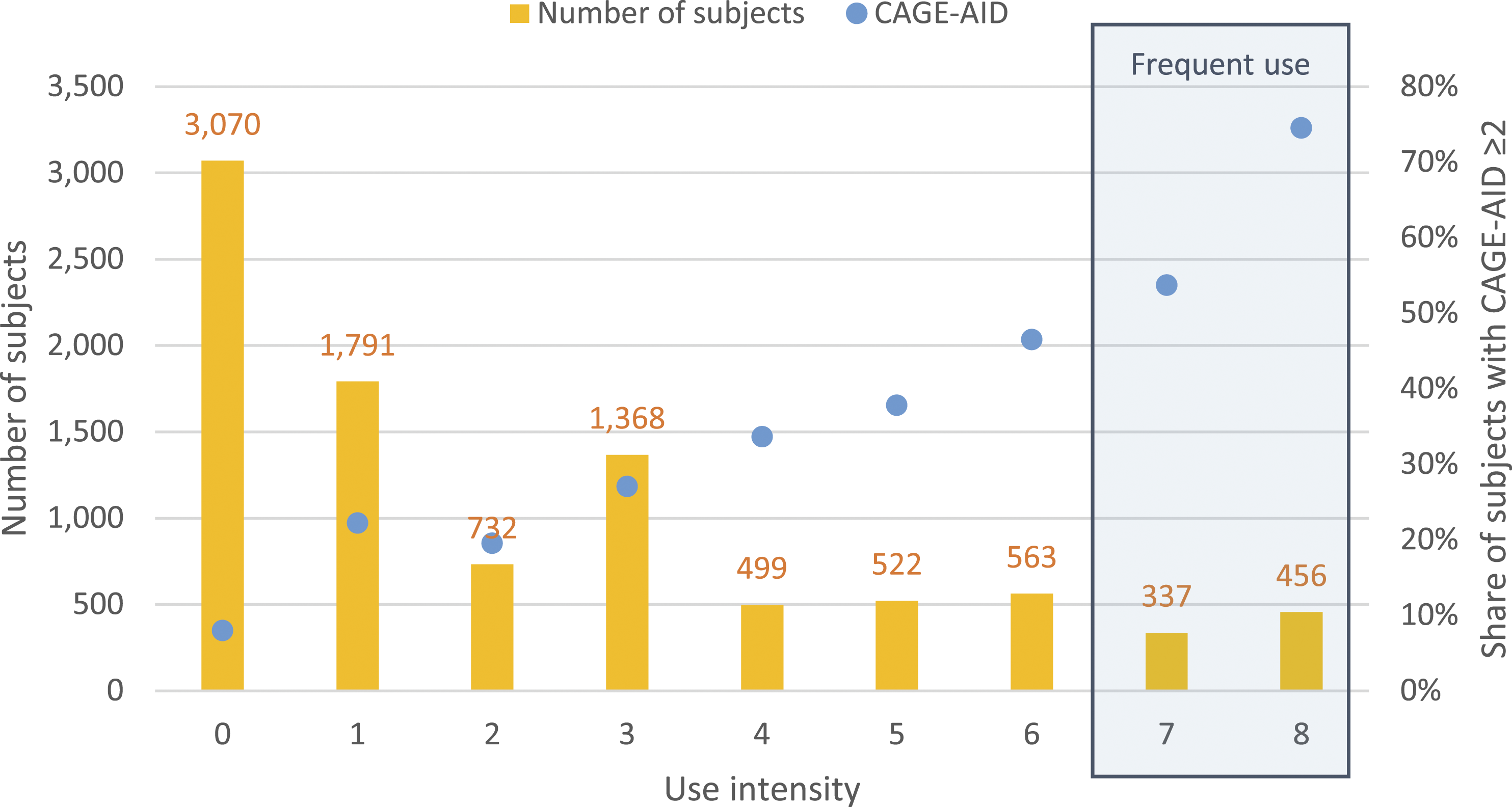
Subjects with frequent cannabis use indicated more often men and “other” gender. Respondents with frequent use were also more impulsive and less religious. The distribution of sexual preferences was significantly different with less respondents identifying as heterosexual and homosexual and more as bisexual or selecting the free text input. Differences in age, LOC and psychiatric diagnosis were not statistically significant.
The CAGE-AID screening test for CUD was significantly more often positive for subjects with frequent use. Women had significantly less often a positive CAGE-AID than men and “other” gender. Respondents with positive CAGE-AID indicated less often heterosexual preferences. Moreover, subjects with a positive CAGE-AID had significantly higher BIS, more external LOC and lower religiosity. Average grades did not differ significantly between subjects with frequent use or positive CAGE-AID and other respondents.
Cannabis use motives
The average scores (5-point Likert scale) of the 20 motive items are shown on Figure 2 for those who consume cannabis, as use motives are not applicable to those not using cannabis. The motives yielding the highest agreement among respondents were euphoria, relaxation, and inebriety (Figure 2). However, the overall agreement was generally low with even the most popular items scoring on average around 2.5 (middle of the scale). Motives for cannabis consumption, average of 5-point Likert scale (1= does not apply, 5= fully applies, N = 4102).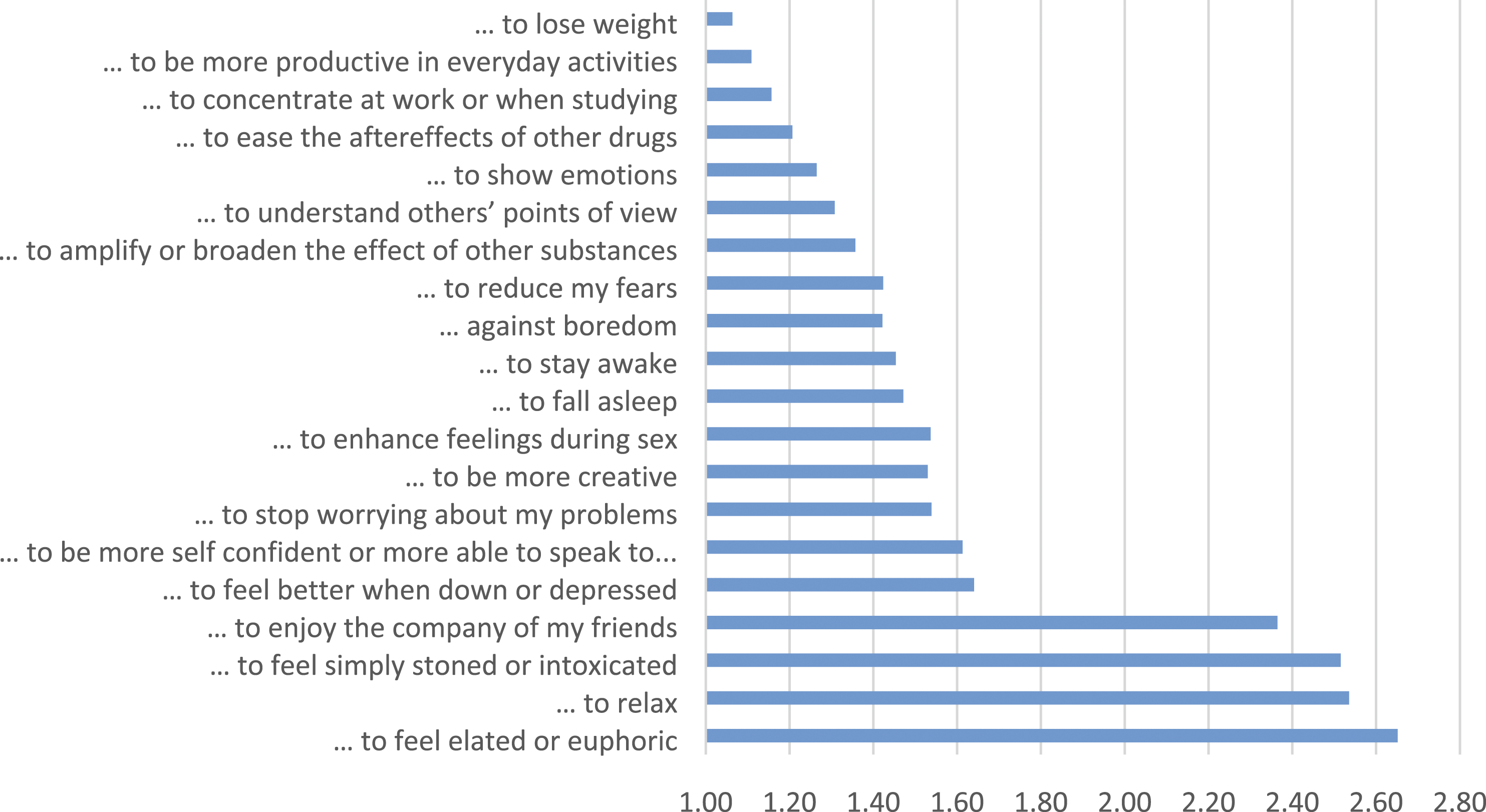
Standardized factor loadings of the 20 motive items for the five factor model (N = 4102).
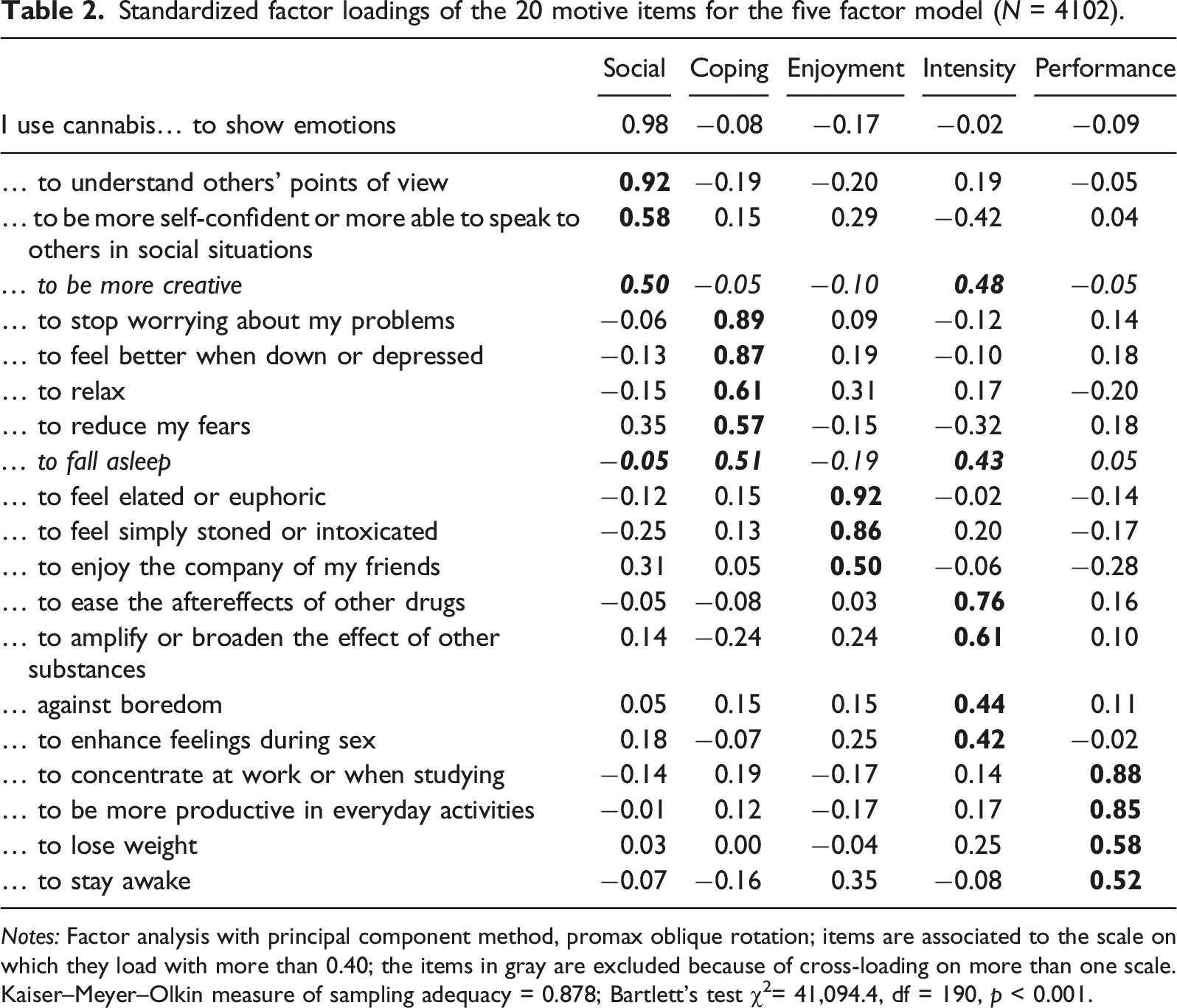
Notes: Factor analysis with principal component method, promax oblique rotation; items are associated to the scale on which they load with more than 0.40; the items in gray are excluded because of cross-loading on more than one scale. Kaiser–Meyer–Olkin measure of sampling adequacy = 0.878; Bartlett’s test χ2= 41,094.4, df = 190, p < 0.001.
Pairwise Pearson’s correlation, Cronbach’s alpha (α), means (M), and standard deviations (SD) of motive scales (N = 4102).
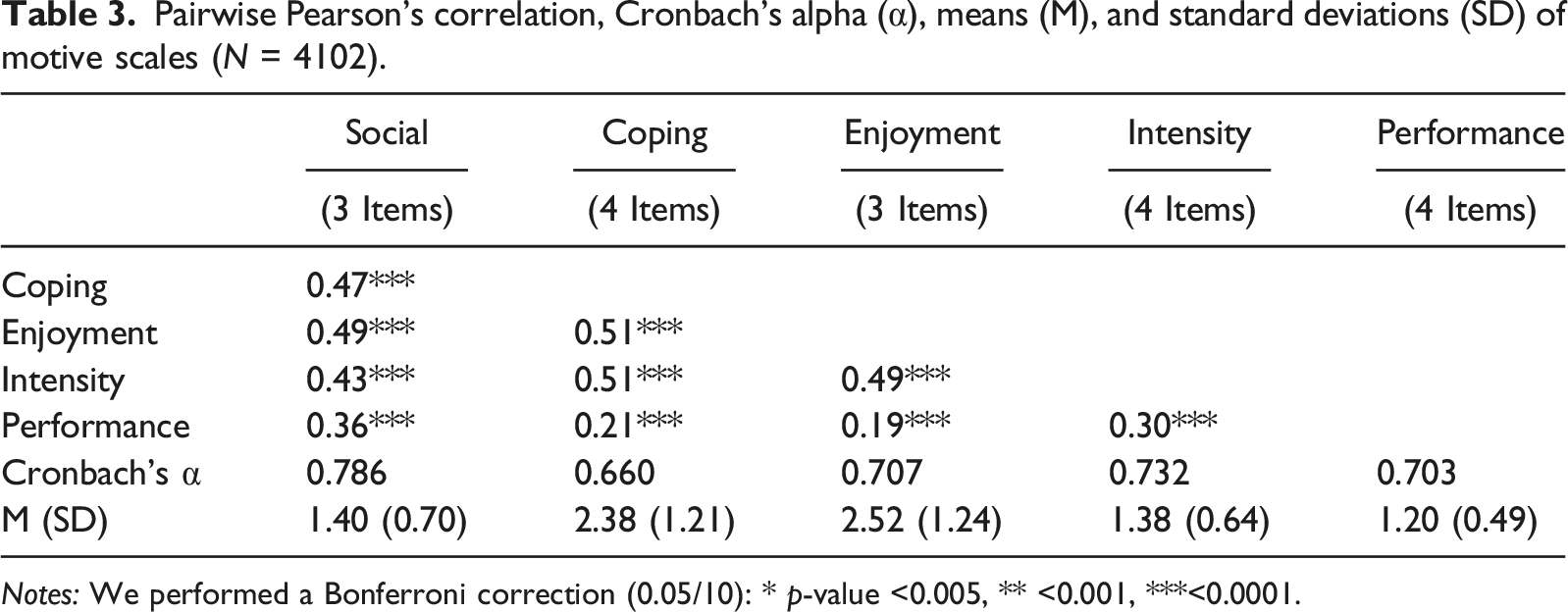
Notes: We performed a Bonferroni correction (0.05/10): * p-value <0.005, ** <0.001, ***<0.0001.
Motive scales for all respondents, and for subjects with heavy use and CAGE-AID.
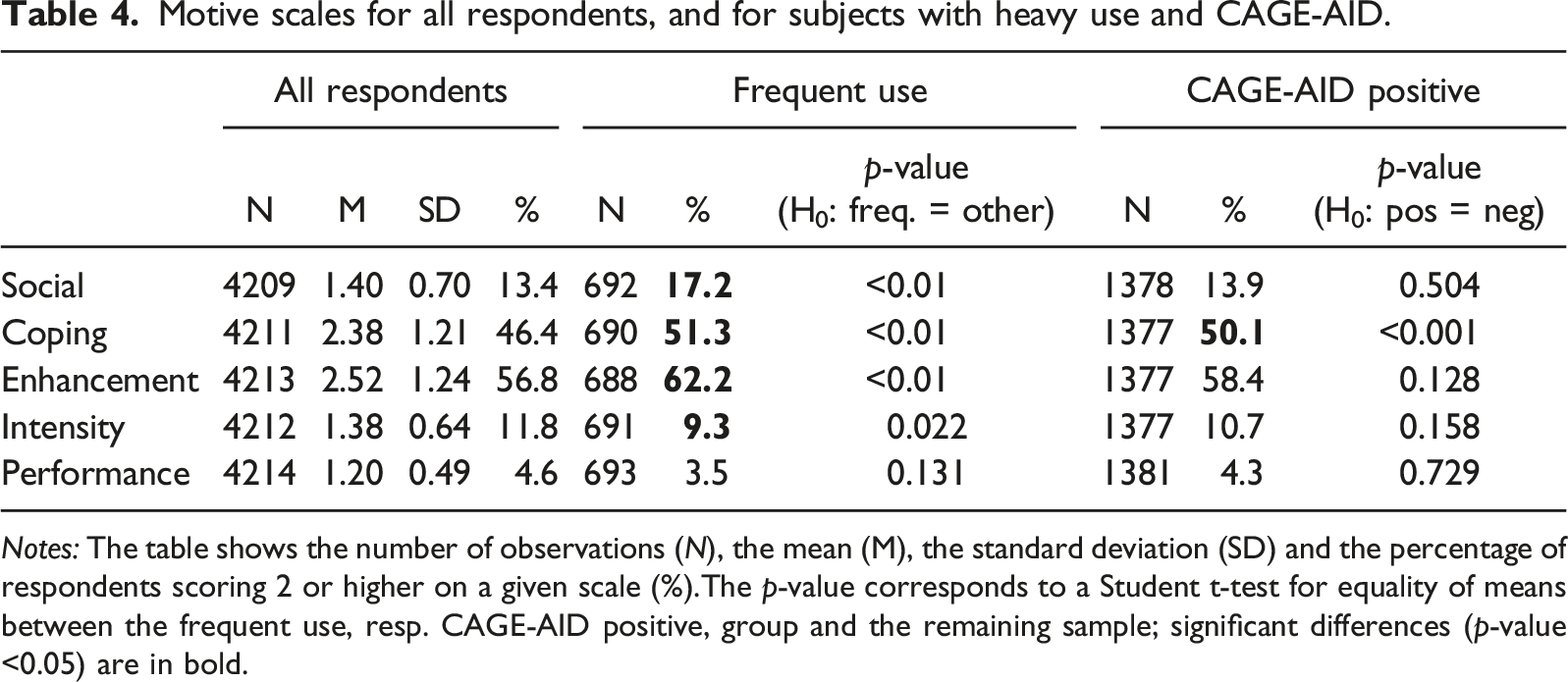
Notes: The table shows the number of observations (N), the mean (M), the standard deviation (SD) and the percentage of respondents scoring 2 or higher on a given scale (%).The p-value corresponds to a Student t-test for equality of means between the frequent use, resp. CAGE-AID positive, group and the remaining sample; significant differences (p-value <0.05) are in bold.
Linear regression model predicting use intensity, and logistic regression predicting frequent use and positive CAGE-AID; each with and without covariates.
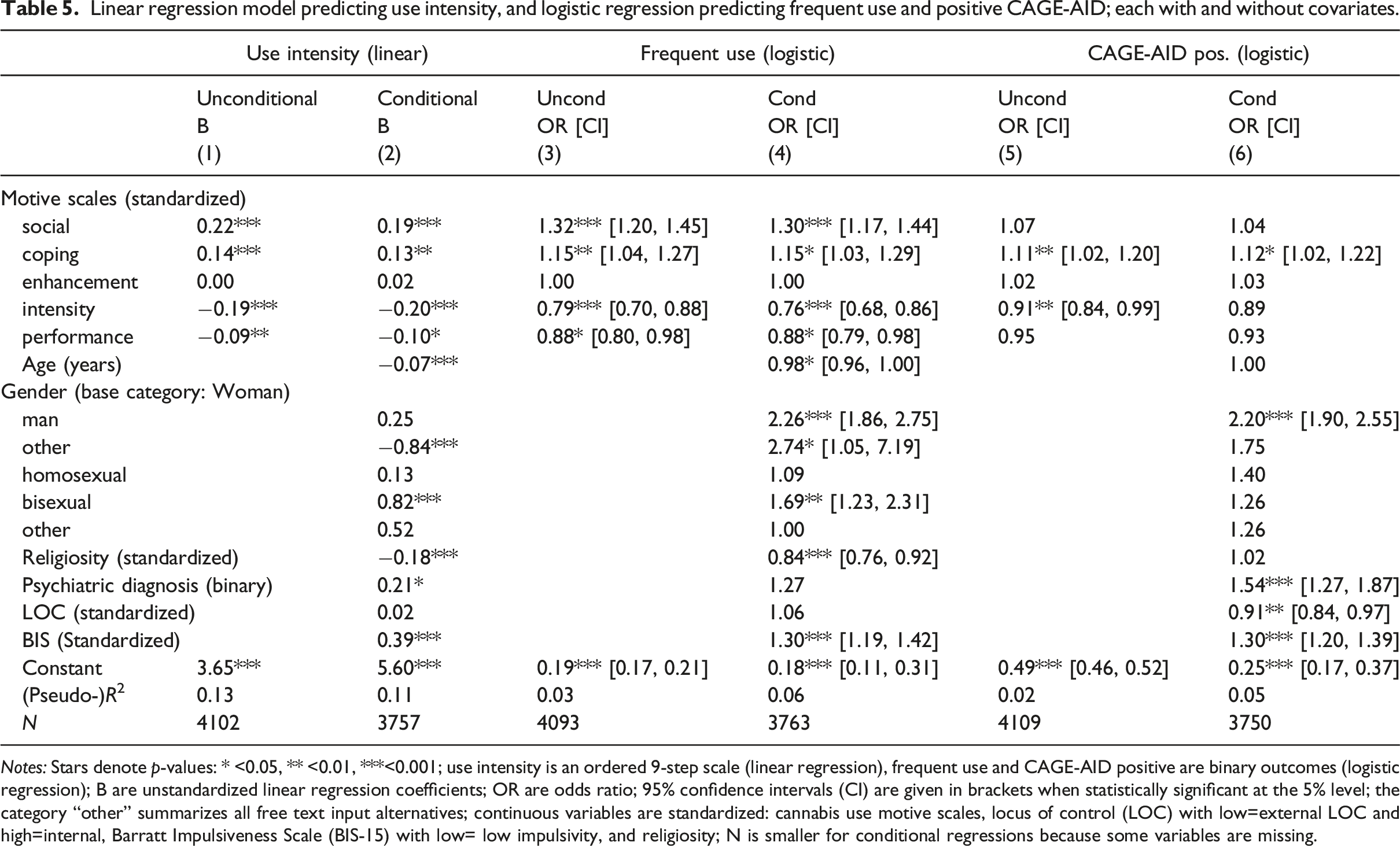
Notes: Stars denote p-values: * <0.05, ** <0.01, ***<0.001; use intensity is an ordered 9-step scale (linear regression), frequent use and CAGE-AID positive are binary outcomes (logistic regression); B are unstandardized linear regression coefficients; OR are odds ratio; 95% confidence intervals (CI) are given in brackets when statistically significant at the 5% level; the category “other” summarizes all free text input alternatives; continuous variables are standardized: cannabis use motive scales, locus of control (LOC) with low=external LOC and high=internal, Barratt Impulsiveness Scale (BIS-15) with low= low impulsivity, and religiosity; N is smaller for conditional regressions because some variables are missing.
A binary logistic regression predicting the probability of frequent use showed a similar pattern (column (3) and (4) of Table 5): social and coping had odds ratios above one, signifying a higher probability of frequent use, while intensity and performance had odds ratios below one, meaning that subjects scoring high on these scales have a lower probability of frequent use. Endorsing social motives more by one standard deviation increased the likelihood of frequent use by 30%, all else equal. These effects remained statistically significant after controlling for covariates.
A binary logistic regression predicting the probability to score positive in the CAGE-AID screening test for substance use disorder showed that coping significantly increased the risk to have a positive CAGE-AID and intensity significantly decreased the risk (column (5) and (6) of Table 5). The effect of coping motives remained after controlling for covariates, whereas the effect of intensity was not significant anymore. One standard deviation higher endorsement of coping motives increased the likelihood of a positive CAGE-AID by 12%.
Age decreased the likelihood of frequent cannabis use (column (2) and (4) of Table 5). Controlling for other factors, men were more than twice as likely as women to show frequent use (column (4)) and a positive CAGE-AID (column (6)); other gender (49 respondents) were significantly more likely to show frequent use. All else equal, bisexual preferences increased the probability to show frequent cannabis use, while CAGE-AID was not significantly related to sexual preferences. Religiosity was negatively correlated to use intensity, but not likelihood of potential CUD. Impulsivity was positively correlated to use intensity and a positive CAGE-AID. An internal LOC had no impact on use intensity, but decreased the likelihood of a positive CAGE-AID. An existing psychiatric diagnosis increased use intensity and the likelihood to have a positive CAGE-AID.
Discussion
The cannabis use prevalence found in our sample is consistent with the literature on Berlin college students, albeit moderately higher than the prevalence found in a similar sample by Jochmann et al. (2019): we found a 30 day prevalence (30Dp) of 24% versus 17% in their sample, a past year prevalence (12Mp) of 41%, and lifetime prevalence (Lp) of 68% versus 63%. As hypothesized, these prevalences were higher than in similar age groups in Germany (Orth & Merkel, 2018: 30Dp=10%, 12Mp=23%, Lp=423%; Seitz, Böttcher, Atzendorf, Rauschert, & Kraus, 2021: 30Dp=9%, 12Mp=30%, Lp=43%) or the US (SAMHSA, 2020: 12Mp=35%). The prevalences of this study were about twice as high as the general population in Berlin (Kraus, Seitz, & Rauschert, 2020: 30Dp=8%, 12Mp=17%, Lp=48%), and much higher than Germany (Seitz et al., 2021: 30Dp=3%, 12Mp=7%, Lp=28%) or the US (SAMHSA, 2020: 12Mp=18%). The hypothesis that Berlin as the “party capital of Europe” shows higher prevalences of substance use seemed thus supported by our data set.
With 24.2% of respondents scoring positive on the CAGE-AID, lifetime incidence of CUD appeared higher in our sample than 9.4% found in an American sample of first-year college students by Caldeira, Arria, O’Grady, Vincent, & Wish (2008). Compared to yearly diagnosed CUD incidences in Berlin in general (Kraus et al., 2020: 1.8%) or the European Union (EMCDDA, 2020: 1%) or the US (SAMHSA, 2020: 5.1%), our findings are high, but one may expect most CUD to be never clinically diagnosed (Caldeira et al., 2008).
The 20-item questionnaire on cannabis use motives gave rise to five motive scales, which were similar to other scales used within the literature (Lee et al., 2009; Schnell, Gliese, Schröter, Kasten, & Gouzoulis-Mayfrank, 2017; J. Simons et al., 1998): coping, social, enhancement, intensity, and performance. Our empirically determined structure of the scales showed only moderate overlap with the scales postulated ex ante by Boys et al. (2001), except for our coping scale which represents their “changing mood” scale; we believe this difference stemmed from different methodologies applied.
In our data, the highest scoring scale was enhancement of positive affect, similar to MMM (J. Simons et al., 1998). However, previous literature found that social reasons were the second most common motive (Glodosky & Cuttler, 2020; Norberg, Olivier, Schmidt, & Zvolensky, 2014; J. Simons et al., 1998), while in our data coping (endorsed by 46.4%) was much more common than social (endorsed by 13.4% of all respondents, 17.2% of subjects using cannabis frequently). Social motives were associated with less intense and less problematic cannabis use in the literature (Glodosky & Cuttler, 2020). This work at hand was the first study on cannabis use motives focusing on students in Berlin. The unusually high share of respondents indicating coping motives could explain the high levels of frequent use and CUD in this population, as coping is known to be associated with frequent use and CUD (Lee et al., 2009; Phillips et al., 2017; Schultz et al., 2019). At this stage, it remained unclear whether this was a selection effect stemming from the attractiveness of Berlin’s nightlife for students interested in a substance-affine lifestyle or whether the living conditions in Berlin induced these coping motives.
We found that high scores on the coping (forgetting problems, avoiding sadness) and social (showing emotions, increasing empathy) motive scales significantly predicted higher use intensity (similar to Bonar et al., 2017; Norberg et al., 2014), while intensity and performance were associated with lower use intensity. Despite being the most common cannabis use motive, enhancement had no significant impact on use intensity in a regression including all five motive scales: this motive seemed to be shared equally among respondents with frequent and not so frequent cannabis use. Across the three outcomes of this study, we saw that motive scales had a significant impact even when controlling for other covariates.
Coping motives were the only significant motives scale for predicting a positive CAGE-AID and thus a potential CUD, after controlling for a list of potential confounding factors. This strengthened the finding from previous literature that coping was associated with more cannabis use, dependence and other negative outcomes (Lee et al., 2009; Phillips et al., 2017; Schultz et al., 2019). However, previous literature had found differences between subjects using cannabis with and without signs of CUD in other motive scales, like enhancement, social and expansion (Bonn-Miller & Zvolensky, 2009; Patterson, Vu, Haardörfer, Windle, & Berg, 2020; Pearson et al., 2019), which could not be confirmed in our data.
The literature has hypothesized that coping motives mediate the relationship between previous vulnerability and CUD: subjects suffering from psychiatric symptoms could develop coping motives, and these coping motives could increase the likelihood of developing a CUD (Bujarski, Norberg, & Copeland, 2012; Fox, Towe, Stephens, Walker, & Roffman, 2011; Johnson, Mullin, Marshall, Bonn-Miller, & Zvolensky, 2010; Vangsness et al., 2005). Indeed, a psychiatric diagnosis had no direct significant impact on the probability of frequent use, but showed a significant association with potential CUD. There remained a significant impact of coping motives on the probability of CUD in our data, even when controlling for psychiatric diagnosis.
The impact of socio-demographic characteristics in our sample was similar to other studies. As in many studies, men had higher levels of use intensity and CUD than women: Hemsing & Greaves (2020) provide an interesting discussion on how this finding may be explained by “‘male-typical or masculine’ identity.” Similar to Mader et al. (2019), religiosity decreased the risk of frequent use in our sample, but not CUD: another instance where a nuanced inspection of use frequency and CUD appeared adequate. Age had a small impact on use frequency and no impact on CUD; this would be consistent with the pattern documented by Caldeira, O’Grady, Vincent and Arria (2012) that cannabis use by university students is “typically heaviest in the first year of study and tends to reduce over the course of academic studies.” Strong associations had been found previously between frequency of cannabis use and psychiatric disorders (Caldeira et al., 2008). In our data, frequent use was not significantly correlated to psychiatric diagnosis, while potential CUD was correlated with a psychiatric diagnosis as in previous studies (Chabrol, Ducongé, Casas, Roura, & Carey, 2005; Schlossarek et al., 2016).
LOC did not impact cannabis use frequency in our sample, which is consistent with Mendolia & Walker (2014). Although internal LOC is known to impact a variety of health behaviors, the impact on substance use seems minor (Helmer et al., 2012). However, respondents with more internal LOC showed significantly less CUD in our sample. This is consistent with the idea, that internal LOC is a protective factor on many life outcomes (Heckman et al., 2006). Similar to the literature, impulsivity, as measured by BIS in our sample, increased both use intensity and CUD rates. Vangsness et al. (2005) shows that impulsivity both directly impacts the frequency of cannabis use and indirectly via less negative cannabis use expectancies. Hecimovic et al. (2014) explain that “impulsive individuals are marked by their inability to weigh immediate reward against long term consequences […] and might use cannabis […] as a short term solution to problems,” which might induce subsequent CUD.
Sample selection among the overall college student population of Berlin (N= 111,007, estimated response rate=11.6%) was difficult to assess, although the sample gender distribution matched roughly the overall gender distribution of the population (Viohl et al., 2019). Subjects using alcohol and other substances have generally higher response rate and the monetary incentive may cause a further bias toward higher substance use (Betzler, Viohl, & Romanczuk-Seiferth, 2017).
Usual limitations for self-report based data apply: socio-demographic data could not be verified, information may have been subject to desirability bias and memory faults (Parra, O’Neill, & Sher, 2003; Williams & Nowatzki, 2005). Nevertheless, self-report is a well-validated (Harrison & Hughes, 1997) and widely used substance use measurement technique. Cross-sectional studies cannot provide causal analysis and the timing of events remains unclear; longitudinal studies, prospective and interventional, would be needed for more clarity on the mechanisms. This study presented the results of exploratory analysis on use motives, and the replicability of exploratory analysis needs to be confirmed in further research.
A core hypothesis of this study was that a positive CAGE-AID captures potential CUD. Although no simple screening tool could replace the diagnosis of CUD by a clinician, this measure has performed reasonably well in other studies (Brown, Leonard, Saunders, & Papasouliotis, 1998; Couwenbergh, Van Der Gaag, Koeter, De Ruiter, & Van den Brink, 2009). In Germany, collecting data on race and ethnicity is highly problematic (Balestra & Fleischer, 2018), so that we could not control for these factors despite their known impact on cannabis use patterns (e.g. Pacek, Mauro, & Martins, 2015).
Conclusion
This study has shown that Berlin college students use cannabis frequently and are at high risk for CUD. In our sample, we confirm the known link between coping motives and CUD and show that coping motives are highly prevalent in this sample. Further research is needed to understand why Berlin college students endorse coping use motives more than other samples in the literature.
We believe that coping motives could be useful for identifying subjects with problematic use (Fox et al., 2011), as they may be potentially less subject to social desirability than CAGE-AID items in non-anonymous surveys. Moreover, knowing about the high rates of coping motives may be useful to primary and secondary prevention campaigns in Berlin. Following the classification of Foxcroft (2014), such campaigns may cover informational functions aiming at showing that cannabis use is a maladaptive coping mechanism (Glodosky & Cuttler, 2020) and developmental functions aiming at teaching vulnerable subject groups other coping strategies. Clinically, further research should elaborate more in detail what problems college students are trying to cope with by using cannabis and what would be more helpful alternative coping strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.