
Abstract
While access to drug treatment has increased in recent years, there is still a shortage of substance use disorder (SUD) treatment counselors in the United States, especially in rural areas. This study examined recruitment and retention issues for counselors in rural substance use disorder treatment programs. Qualitative interviews were conducted with 26 program, clinical, and/or human resource directors of SUD treatment programs. Almost all interviewees had problems recruiting high-quality counselors although only a small number saw retention as a significant issue. Improving educational opportunities and training related to addictions counseling could result in more people entering the SUD treatment field. Strategies for improving retention of counselors include more supportive and inclusive management practices. The stigma of SUD also contributed to recruitment and retention problems.
Introduction
The Bureau of Labor Statistics (2019) predicts that the number of jobs related to behavioral health counseling, which includes substance use disorder (SUD) treatment, will increase by 23% by the year 2026, an increase higher than the average job growth. Yet, the per capita supply of behavioral health providers in non-metropolitan counties is significantly less than the supply in metropolitan counties (Larson, Patterson, Garberson, & Andrilla, 2016). Similarly, the Health Resources and Services Administration (2020) projects that the supply of addiction counselors is not sufficient to meet the future demand for substance use services in the United States.
A national sample of clinical directors in drug treatment programs found that almost half of the facilities surveyed had difficulty filling open positions, most often due to a lack of qualified applicants (Ryan, Murphy & Krom, 2012). Research suggests that recruitment problems for SUD treatment counselors are worse in rural areas. Challenges to recruiting SUD treatment staff in rural areas include low pay compared with their urban/suburban counterparts, social isolation, and fewer educational opportunities (SAMHSA, 2016; Snell-Rood, Pollini, & Willging, 2021). Given the shortage in mental health/SUD treatment providers in rural areas, some states have implemented programs to encourage college students to enter careers in behavioral health, including loan repayment programs and “pipeline” projects that educate rural students about related careers (Baum & King, 2020).
Because of this shortage, rural residents have less access to drug treatment services than people in urban areas (Borders & Booth, 2007). They also experience disparities in mental health outcomes even though rates of mental illness are similar in rural and metropolitan areas (Morales, Barksdale & Beckel-Mitchener, 2020). The recruitment and retention of high-quality counselors is important to improve rural mental health and SUD treatment.
Substance Use Disorder Treatment Turnover
In addition to a shortage of workers, the SUD treatment field faces the additional challenge of high turnover among clinical staff. Research consistently shows high voluntary turnover rates among counselors, typically ranging from 25 to 35%, with some studies showing rates as high as 50% (Eby, & Rothrauff-Laschober, 2012; Gallon, Gabriel & Knudsen, 2003; Garner, Hunter, Modisette, Ihnes, & Godley, 2012; Garner & Hunter, 2013, 2014; McLellan, Carise & Kleber, 2003; McNulty, Oser, Aaron Johnson, Knudsen & Roman, 2007). SAMHSA estimates that the annual turnover rate is about 33% (Sherman, Lynch, Greeno & Hoeffel, 2017), although these rates have likely increased since the beginning of the COVID-19 pandemic (Akinyooye & Nezamis, 2021). Turnover rates are also high for clinical supervisors (Eby, Burk & Maher, 2010; Knight, Broome, Edwards & Flynn, 2011). These rates are substantially higher than the annual turnover rate for all health and human services occupations reported by the Bureau of Labor Statistics (White & Garner, 2011).
High turnover rates are problematic because they can have negative impacts on the organization as well as those receiving treatment (Hyde, 2013). One issue is financial; it costs more to recruit and hire a new employee than to retain an existing one (Cascio, 2000). Programs with high turnover rates also show low employee morale and increased work demands (Johnson & Roman, 2002; Knight et al., 2012). Counselor turnover can also be disruptive to the treatment process. Research has found that clients stay in treatment longer and do better when they remain in contact with the same therapist (McCarty, Greenlick, & Lamb, 1998; McCaul & Svikis, 1991). There is a general lack of research, however, on the direct impacts of turnover on treatment outcomes. One study found that counselor and clinical supervisor turnover actually had positive impacts on treatment outcomes, such as reduced illegal activity (Garner et al., 2012). Another study linked poor job performance ratings to future turnover, suggesting that those who voluntarily leave their counseling positions might not be the highest quality (Laschober, & de Tormes Eby, 2013).
Some research suggests that facilities in rural areas may experience greater retention issues than urban facilities. For example, a study of treatment providers in Tennessee found that rural programs had higher turnover rates (Knudsen, Williams, & Perry, 2005). Other research on mental health providers finds higher rates of burnout and exhaustion in rural areas, suggesting that SUD treatment staff in rural areas might also experience higher stress and turnover than their urban counterparts (Hargrove & Curtin, 2012; Kee, Johnson & Hunt, 2002). A recent study examining physician bias toward people with opioid use disorder found higher levels of bias in rural areas (Franz, Dhanani, & Miller, 2021). Clearly, more research is needed to better understand the recruitment and retention issues for rural treatment workers and the impact they have on treatment.
Reasons for Turnover
One of the most consistent predictors of turnover is job satisfaction (Eby & Rothrauff-Laschober, 2012; Garner & Hunter, 2014; Kulesza, Hunter, Shearer, & Booth, 2017; Knight et al., 2012; Young, 2015). Secondary traumatic stress (the emotional toll of listening to another person’s trauma) can also predict job satisfaction, which often impacts intent to quit (Bride & Kintzle, 2011). Other characteristics of the organization, including perceived support, salary, level of clinical supervision, perception of fairness, and leadership effectiveness have been shown to relate to job satisfaction and predict turnover rates (Eby & Rothrauff-Laschober, 2012; Garner & Hunter, 2014; Rothrauff, Abraham, Bride & Roman, 2011; Tsounis, Niakas & Sarafis, 2017).
Research on turnover among SUD counselors suggests that management can adopt practices to increase retention. Counselors with higher organizational commitment are less likely to leave their position (Knudsen, Johnson & Roman, 2003; McNulty et al., 2007). Counselors who perceive their workplace to exhibit distributive justice (perceived fairness of how benefits and costs are distributed among staff) and who feel they are included in major workplace decisions also show lower intent to quit (Knudsen, Ducharme & Roman, 2006; Rothrauff et al., 2011). Facilities that use participatory management structures, where employees feel they are part of the decision-making process, experience lower turnover (Knudsen et al., 2006; McNulty et al., 2007). Counselors who reported higher levels of job autonomy also showed lower turnover intention (Ducharme, Knudsen & Roman, 2007; Knudsen et al., 2003). Given the importance of organizational structure and culture on turnover, more research is needed on strategies that programs have implemented to increase job satisfaction and reduce turnover.
Counselor stress and exhaustion (“burnout”) has been consistently linked to increased turnover intention (Garner & Hunter, 2013; Knudsen, Ducharme & Roman, 2008; Landrum, Knight & Flynn, 2012; O’Connor, Neff & Pitman, 2018). Burnout is most often associated with job-related demands, such as workload (Beitel et al., 2018; Landrum, Knight & Flynn, 2012). Counselors who report higher self-efficacy and control over their job show lower levels of burnout (Shoptaw , Stein & Rawson, 2000; Vilardaga et al., 2011. Most research findings agree that coworker support, increased clinical supervision, and self-care were important strategies for managing emotional exhaustion and improving job satisfaction (Beitel et al., 2018; Ducharme, Knudsen & Roman, 2007; Fukui, Wu & Salyers, 2019; Oberleitner et al., 2021; Oser et al., 2013; Shoptaw et al., 2000;Skinner & Roche, 2021; Vilardaga et al., 2011). Vilardaga et al. (2011) also found that negative attitude toward clients (SUD stigma) was related to higher levels of burnout.
Current Study and Context
Despite the large number of research studies on counselor turnover, more research is needed to understand recruitment and retention issues in rural SUD treatment programs. Almost all the research has examined retention issues through surveys of counselors so it is not entirely clear what organizations can do to improve job satisfaction and lower turnover rates. For instance, if coworker support and perceived justice is shown to improve retention, what specifically occurs in the work environment to encourage such outcomes? Because very little research has examined how clinical supervisors and program directors view recruitment and retention issues, this study utilizes qualitative interviews with these administrative staff to explore organizational strategies associated with recruitment and retention. This qualitative strategy allows for an in-depth exploration of practices that are occurring in these treatment programs, which could also lead to future quantitative research based on the themes discovered. The main research questions are: How do program and clinical directors perceive recruitment and retention issues in their facility? What strategies do these administrators cite as effective in improving recruitment and retention of quality counselors?
This study focuses on administrators in rural treatment programs in Pennsylvania, one of the hardest hit states by the opioid crisis. Pennsylvania had the fifth-highest death rate from drug overdoses in the United States in 2019, according to the Centers for Disease Control (Centers for Disease Control and Prevention CDCP, 2019). While overdose death rates declined in Pennsylvania from 2017 to 2019, preliminary data for 2020 shows an increase (Open Data PA, 2021). Rural counties in Pennsylvania have been particularly impacted; in 2018, 6 of the 10 counties with the highest opioid overdose death rates in Pennsylvania were rural, including the county with the highest overdose death rate that year (Overdose Free PA, 2019). In response to the overdose crisis, the governor has signed multiple “opioid disaster declarations,” including the 14th renewal in May 2021 (PA Governor’s Office, 2019). As a result, state and federal funding for drug treatment has expanded, especially for medication for addiction treatment and county funding to support treatment access for the uninsured or underinsured. These initiatives have assisted more people in Pennsylvania to access SUD treatment. Since 2015, there has been a steady increase in the number of Medicaid recipients receiving medication for addiction treatment (Open Data PA, 2021). Data from the Substance Abuse and Mental Health Services Administration (2021) indicate that admissions into drug treatment programs in Pennsylvania increased by 5% between 2016 and 2019 (from 27,494 to 28,871 admissions).
Given the increase in people accessing treatment for a SUD, it is important that treatment programs have the required staff to meet that demand. If opioid overdose death rates are an indicator of the need for drug treatment, we can expect that the highest growth in treatment demand in Pennsylvania will be in rural counties.
Methods
Sampling Frame
A list of all SUD treatment facilities licensed by the Pennsylvania Department of Drug and Alcohol Programs was obtained and sorted to exclude urban counties (per the urban/rural definition provided by the Center for Rural Pennsylvania 1 ). Two hundred forty facilities, located in 48 rural counties, were included in the sampling frame. From this list, 30 facilities were randomly selected to contact for a qualitative interview. Random selection was used because the master list of programs did not include many characteristics of each treatment program, such as staff size, number of admissions, or special populations served (i.e., pregnant women or adolescents). Therefore, purposive sampling was not possible.
The principal investigator emailed and called each prospective participant to explain the purpose of the research, which was part of a larger grant project examining counselor recruitment and retention issues in rural Pennsylvania counties. After reaching out via phone and email to the initial 30 facilities selected, 14 interviews with clinical supervisors/program directors were scheduled. Four facilities’ staff declined to be interviewed. The remaining facilities were contacted multiple times and received multiple messages about the project. After two weeks of no response from the facilities, an additional 30 facilities were randomly selected to contact. From this list, the facilities were first sorted by county and attempts were made to reach facilities located in counties where no treatment program had yet been contacted. All the facilities were contacted multiple times, resulting in the scheduling of eleven more interviews. The program director for one additional facility declined to be interviewed due to not having the time but agreed to answer questions via email 2 . An undergraduate research assistant assisted with contacting the selected treatment facilities.
Interviews
These efforts resulted in 26 completed interviews, including the one via email. The principal investigator, who has extensive experience with interview research, conducted and analyzed all interviews. The principal investigator has conducted research in substance use disorder (SUD) treatment facilities for over 20 years and has broad knowledge about different treatment types, structures, and the various staff roles in these facilities. Twenty-three interviews occurred in April and May, 2020. These interviews were then analyzed for themes. Two additional interviews occurred in September, 2020 to investigate whether any additional themes emerged. No new themes emerged from the additional interviews, so the investigator determined that saturation was reached, and no additional interviewees needed to be recruited (Saunders et al., 2018). No financial incentives were offered to participants.
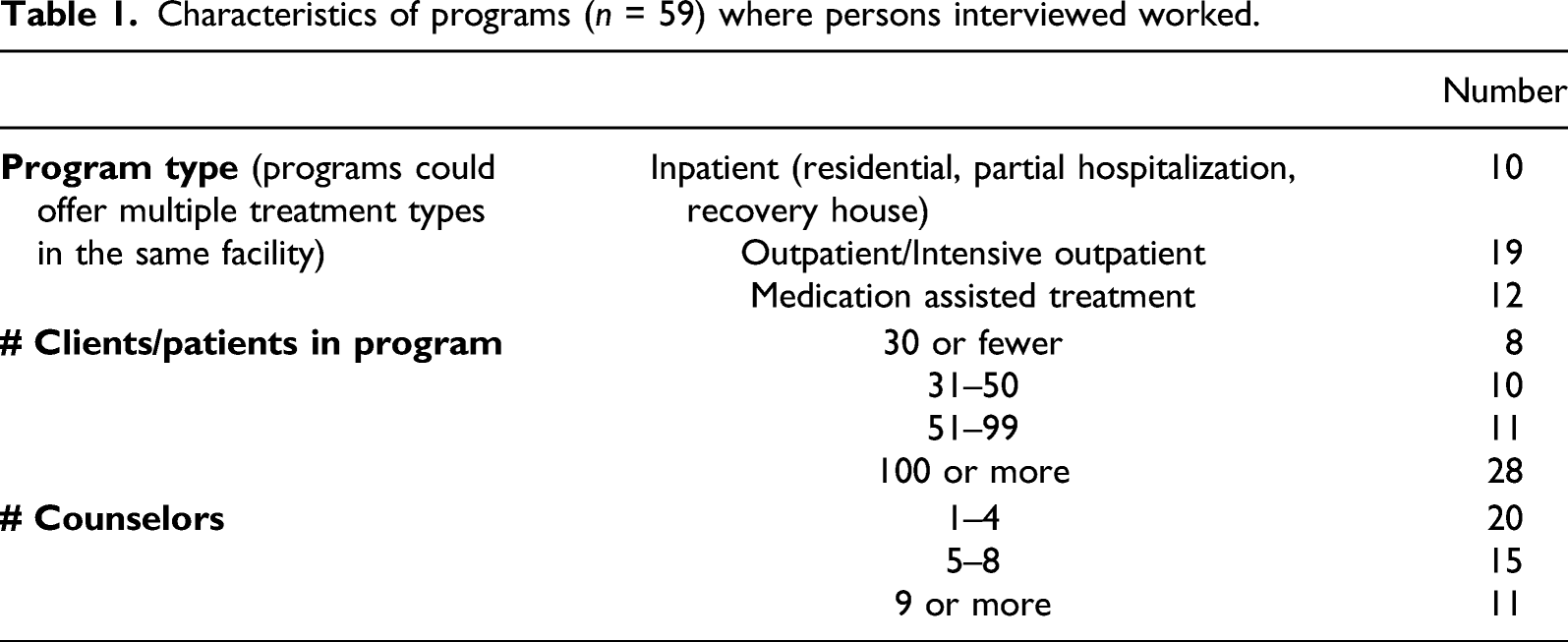
The purpose of these interviews was to gather information about recruitment and retention issues within the facility so the person who would be most knowledgeable about these issues was asked to participate in the interview. For some programs, especially smaller ones, the program director was the appropriate person to interview (several interviewees served as both the program director and clinical supervisor). For other programs, especially larger ones, the clinical supervisor was asked to participate. Some programs did not have a clinical supervisor position so the person who had experience hiring and supervising clinical treatment staff was asked to participate. Of the 26 interviewees, 10 held the role of clinical supervisor and 12 were considered the program or facility director. Two interviewees were both the program and clinical director. The other two interviewees were the human resources director for the organization. Seventeen interviewees (65%) were female; nine were male. All interviewees identified as white, which was not surprising given that all rural counties in Pennsylvania are overwhelmingly white 3 . The people interviewed had extensive experience in the drug and alcohol field; most held master’s degrees in counseling and had spent several years as a counselor before being promoted to their current position. The median number of years of experience a person had in the field was 15.
Characteristics of programs (n = 59) where persons interviewed worked.
Each interview was done via phone and recorded via a call recorder app (except for the one via email). The interviews were semi-structured and included questions about the structure of the facility, the process for hiring new counselors, recruitment and retention strategies, and perspectives about recruitment and retention issues. Interviewees were asked directly if they thought recruiting high-quality counselors was a problem for their facility, and if it was, why that might be. They were asked similar questions about how long the current counseling staff had been working and why staff may have left in the previous 2 years. While the interviews took place at the start of the COVID-19 pandemic, and many programs had to make major adjustments to the structure of treatment and counselor’s work, interviewees were asked to reflect on these issues pre-pandemic. Interviews typically lasted between 35 and 45 minutes and were transcribed verbatim by a research assistant. The Institutional Review Board of the investigator’s university approved all research protocols.
The interviews were systematically coded for themes using conventional content analysis (Hsieh & Shannon, 2005). This method was chosen because it can utilize a grounded theory approach, where codes emerge from the data rather than are predetermined and applied (Glaser & Strauss, 2017). The principal investigator first did open coding on all the interviews because of the exploratory nature of the research. Codes were grouped into similar categories to create themes and subthemes. Once a preliminary list of themes was created, the principal investigator re-analyzed all the interviews to document how prevalent the themes were and to ensure no other themes were overlooked.
Results
Perspectives on Recruitment
“It’s not like there’s a lot of positive energy out there in the news that’s saying, hey, don’t you want to be a drug and alcohol counselor?” (Facility Director, Inpatient Treatment Program)
Almost all interviewees (n = 21, or 81%) indicated that recruiting high-quality counselors was a significant problem for their program. One additional interviewee (a clinical director) indicated that while recruitment was not currently an issue, it had been at the facility where she worked previously. For the interviewees who indicated recruitment was not a problem (n = 5), three indicated that they had a good pool of candidates for the last positions they hired. Two also attributed their facility’s positive reputation as helping with recruitment. Two programs also had a very small staff (one program employed only one full-time counselor) and had not hired recently.
For those with recruitment problems, the main issue was that not enough qualified people would apply when these programs had open positions. Several interviewees related this issue to there not being enough new people entering the field. As one clinical director explained: “A lot of times we’re just recycling people…It’s not like we’re bringing new blood in from out of the area…We’re hiring somebody that’s working in a different clinic down the road…”
Given that a lack of qualified candidates was the major hindrance for recruiting, follow-up questions probed about why they felt recruitment was an issue and what could be done to improve the candidate pool. Five themes emerged in these areas, including low salary, stigma, fit/experience, rural location, and state requirements.
Low Salary
When asked why they thought recruiting was a problem, one reason offered was the salary. Eighteen interviewees (86%) mentioned low salary or unrealistic salary expectations as a major recruitment problem. While several interviewees felt that they offered a good benefits package, they did not see it as sufficient to compensate for low pay.
Low salary was a function of the low rates of reimbursement that drug and alcohol programs received from the state and insurance companies. Many of the interviewees lamented how poorly drug and alcohol services were reimbursed and found a general lack of respect toward the field. As one clinical director said: “Drug and Alcohol is often the redheaded stepchild of social services. And we don’t get respect from the insurance companies or the state or the legislature. It’s everyone’s dirty little secret.”
The program/clinical directors associated the lower reimbursement rates compared to other mental health services because of the lower status held by the drug and alcohol treatment field. Thus, the low salary they would offer new counselors was related to the next theme that emerged, the stigma of SUD treatment.
Stigma
Stigma emerged as a theme, both in how public stigma inhibited recruitment and the stigma perpetuated by clinical/program directors. Four interviewees (19%) who saw recruitment as a problem discussed the public stigma associated with SUD specifically. As one program director explained: “I think that a lot of it has to do with the stigma that’s still out there… The stigma that the media portrays, that society portrays… Who wants to go into a field where you’re not going to get any praise, you’re not going to feel like you’re doing something good?”
This program director sees stigma as discouraging potential counselors from entering the field because of the public perception that working in the field is not considered worthwhile. Another program director explained this public perception well: “Every time somebody asked me where I work and I say [Treatment Center], they’re like, ‘oh my gosh, how do you do that?’ And I always respond super positive and I say, ‘you know what, I love it. I can’t imagine doing something else… I love the people that I work with, I love the patients that I work with, and I enjoy everything about it.’ I think if people are able to portray that more than it would be a different story but that’s just not how it is.”
These are examples of how stigma could extend to those working in SUD treatment. Even though these individuals have professional jobs and advanced degrees, they could be stigmatized for working with what many consider to be an undesirable population.
Additional interviewees discussed stigma but indirectly. One program director saw stigma toward medication as part of treatment (MAT) as a barrier for recruiting counselors: “Some people are very opposed to MAT…so that would impact some facilities.”
While only one interviewee mentioned this as a potential problem, it relates to the stigma that is associated with SUD treatment more generally and shows that opioid use disorders could be more stigmatizing than other types of treatment.
While these program directors viewed public stigma as part of the problem for recruiting counselors, other program/clinical directors held stigmatizing views of the clients in their programs. For example, six interviewees (26%) mentioned that clients in drug and alcohol treatment are not the most desirable population to work with, which could impact recruitment. One facility director referred to clients as “difficult,” implying that they are a harder group to work with than in other types of mental health treatment. Similarly, another program director referred to their clients as “manipulative” which could impact both recruitment and retention. Here, a program director relates these unappealing characteristics of people in SUD treatment as barriers to recruiting counselors: “I think some people go to counseling and they think that they’re going to change the world and they’re going to have doctors and lawyers and like these upper-class people that are coming to see them in an office with a couch and that kind of stuff... And drug and alcohol is not that. You’re going to have the roughest of the rough coming in. So I think that’s a big barrier.”
While the facility where this program director worked might not attract upper class professionals for treatment, such individuals certainly experience addiction and need treatment. Her statement perpetuates the stereotype that people with SUD are lower class and uneducated. While she attributes recruitment problems to unrealistic expectations about clients, one wonders how her own perspective might get communicated to potential applicants and those going through the interview process. Her own biases toward the people in the treatment program might influence whether a counselor would want to work there. This idea that applicants have unrealistic expectations associated with the job relates to the next theme that emerged from the interviews, that those who are applying are not a “good fit” for SUD treatment.
Fit/Experience
When the interviewees were asked what was lacking in the candidate pool for open counseling positions, a common response was that the applicant was “not a good fit” for the position. Further analysis in this area revealed that being a good fit for the position meant that the person had training and direct experience counseling people with SUD as well as a passion/commitment for the field. Almost all the interviewees who had recruitment problems (n = 19, 90.5%), mentioned that candidates lacked training, experience, and/or commitment.
Part of a lack of experience was a lack of education about drug and alcohol issues in undergraduate and graduate programs related to counseling. For example, a clinical director of a residential facility felt that the education of potential applicants might not have kept up with changes in the field: “From where I started in the field, in the mid-80s, to where we are today, there’s just a different level of sophistication that a clinician needs. The significance of trauma… The understanding of what medication assisted therapy is and how to determine who is best for that angle of care… So it’s been very challenging [finding counselors].”
Many of those interviewed thought that undergraduate and graduate programs should offer more courses and internships related to SUD treatment. Several also suggested that programs offer certificates in Addiction Studies.
While applicants might have experience counseling in the mental health field, the interviewees did not view that experience as adequate preparation for the field of SUD treatment. This relates to the previous theme of stigma, that is, the perception that clients in SUD treatment are more challenging than those in other mental health treatment settings. It is concerning that interviewees did not think that the techniques that master’s level students learned and practiced would apply to people in SUD treatment programs; this perpetuates the stigma that they are more difficult to treat than other mental health patients.
In addition to having direct experience with alcohol and drug issues, the interviewees felt that candidates should be better prepared more generally for the counseling profession. As two clinical directors below explained: “A lot of it needs to start in undergrad… Making sure that students getting ready for their senior internship have a logical and reasonable goal for when they graduate. They’re not going to be making $100,000 a year with a Bachelor’s… This is very rewarding work, and you can get to a point where you make a good living…So, just making sure people really know what they’re getting into so you’re not surprised when you’re offered a certain salary.” “The students coming out of [Master’s programs] are…I don’t know what they’re being taught…They lack professionalism and they lack people skills. They lack compassion and clinical skills as well.”
These two program directors saw a lack of proper training to be a larger educational issue that included the need for better socialization into the profession. Both discussed shortcomings with individuals graduating from bachelor’s and master’s programs but believed the institutions from where they graduated could teach them the skills they needed and to be realistic about their expectations.
Related to this sense of lacking education and professionalism, three interviewees (14%) mentioned that more recent applicants did not have a passion for the field, which they viewed as necessary for success. As one facility director put it: “I don’t know where the people are anymore that really care to come in and help people instead of being out for the money.”
Another facility director shared this perspective: “And I want people that are called to counseling. I don’t want anybody working for me that does it for a job. They’re not going to last long in the field and their clients will pay for that.”
This perspective about the need for commitment to the field could be due to the extensive experience that all the clinical/program/human resource directors interviewed had. Most of them started their career as a counselor and later moved into administrative positions. Having spent so many years in the SUD treatment field, they interpreted their professional trajectories as the result of their own passion and commitment to working with people with SUD. Below are two statements that illustrate their own passion and commitment for the work: “I feel like once you get in drug and alcohol and you know that that’s your niche, that you couldn’t go anywhere else. I can’t imagine working with a different population.” (Clinical Director) “It’s a mission that I have. It is not a job for me, this is not employment... I would do it for money or I would do it voluntarily.” (Program Director)
The lack of passion cited by the interviewees was also related to the problem of salary. In their view, a counselor should have a level of commitment to the field that makes up for low salary. Given that many applicants for counseling positions are recent college graduates, with significant student loan debt, it may be unrealistic to expect such a high level of commitment to a field that does not pay as highly as others.
One strategy for addressing this lack of experience/commitment was to accept interns in their programs. Almost all the programs (n = 21, 81%) utilized interns and had at least one intern work for the facility after their graduation. One program was strategic about using interns to train for open positions, as the program director here explained: “We’ve had a heck of a time getting qualified people to respond to ads. And that’s why we take on interns, which is a good way to get someone in. That’s what we did with the one we have now. Brought him in as an intern, he was doing a great job, hired him and then we’ll see how he does and then he can go full time if the supervisor decides that he’s doing well enough.”
Having interns was also mentioned as important for exposing potential counselors to the field. One program director mentioned that she did an undergraduate internship in a drug treatment facility and fell in love with the field. Another clinical director had a similar experience: “So many people I know that have stayed with drug and alcohol treatment started off interning and worked their way up throughout the system… So I think establishing healthy programs with colleges and educators, that back and forth, would be really crucial.”
The few facilities that did not offer internships usually cited the work involved mentoring interns as being too great, especially if they had a small staff. Two interviewees mentioned that they would like to have interns but had not had anyone contact them in recent years. Cultivating internship opportunities could help improve the pipeline of future SUD counselors and give them the required training they would need to be hired, but it appeared that the programs that had successfully hired interns put a lot of work into mentoring interns and maintaining relationships with local universities.
Rural Location
Recruitment problems were also attributed to the rural location of the facility; 52% of interviewees who viewed recruitment as a problem discussed this barrier. Being in a rural location led to recruitment issues because people might have to commute to a more remote area and because not enough people lived nearby with the required higher education and experience for the position. Two interviewees mentioned the population decline in their rural areas and the migration of educated people to other parts of the state. Related to this problem was the lack of higher educational institutions in some of the rural areas where these programs were located. One clinical director who said recruitment was not a problem said that she saw a good “pipeline” of applicants from two universities located within 20 miles of her facility. Having such a pipeline, however, was the exception as most directors discussed the lack of educational programs in their rural counties.
State Requirements
Given that these directors worked in state-licensed treatment programs, they had to follow the state requirements for hiring new counselors, which required significant education and experience. These requirements were overall seen as necessary to ensure a quality workforce. However, six interviewees (29%) indicated that the requirements in certain areas were too strict and inhibited hiring. For example, one clinical supervisor mentioned that the state only permitted certain fields of study for a counseling position but that she had considered candidates to be qualified who had a degree in another field. While the state agency had a process where facilities could petition for an exception to the degree requirement, it created an extra barrier in the hiring process. Several other directors thought that the state should count time in recovery toward the required experience.
If a candidate did not meet the experience requirements that the state authorized for the position, programs could hire the individual as a “counselor assistant” until they achieved the required experience while working. However, it was unrealistic for many programs to hire counselor assistants because these individuals could not carry a client caseload on their own, and therefore none of their work would get reimbursed. This was not a viable option for most programs because they relied on reimbursements to fund their counselor’s salaries.
Perspectives on Retention
In contrast to the difficulty in recruiting qualified counselors, only six interviewees (23%) reported that turnover was a major problem in their rural facility. Two said that it could sometimes be an issue and five indicated they had experienced retention problems in other facilities where they worked. Most, however, (n = 18, 69%) were confident that it was not a problem at all in their current programs. Considering their extensive experience in the field, all interviewees were asked to reflect on the reasons for turnover either in their programs or in the SUD treatment field more generally. Six themes emerged about turnover/retention, including burnout/stress, workload, private practice, management support, professional development, and teamwork.
Burnout/Stress
All of those who viewed retention as an issue in their program, or in programs they worked for in the past (n = 13), mentioned counselor burnout or stress as a major reason. All but one interviewee who discussed burnout/stress elaborated how stress was worse for counselors who treat SUD. That is, their explanations for burnout and stress implied that SUD clients cause more stress. As one program director explained,
“I think it’s a super rewarding profession. It’s just, it’s very stressful, too. I had a colleague one time saying we deal in people’s pain and misery. That’s our business.”
Related to burnout and stress was the frustration counselors could feel when their clients relapsed. Those interviewed perceived a client’s relapse to be a major cause of burnout and stress for counselors: “It’s stressful, it’s tiring. Sometimes you get stuck in feeling like you’re fighting a losing battle… If you have a bunch of clients that relapsed at the same time… Just seeing the opioid epidemic in the news and still seeing people dying… It feels like it just never changes, and you’re doing the same thing over and over again.” (Clinical Director)
“It’s a very difficult field. A lot of times our therapists can feel defeated because if somebody relapses or passes away or gets arrested again. Like all that hard work, they feel like they failed.” (Program Director)
As these statements show, program/clinical directors viewed counselor burnout as worse for the SUD treatment field because of the likelihood of relapse, even though other mental health professionals must confront a client’s relapse (i.e., for depression or an eating disorder). Similar to their view that recruiting counselors is harder in the SUD treatment field, they view retention as worse because of their perception that people in SUD treatment have worse problems or are more emotionally difficult to work with. While only one interviewee mentioned the larger opioid crisis as a factor for burnout, the extensive media coverage of overdoses and addiction likely impacts how counselors process their work.
While all the program/clinical/human resource directors interviewed appeared to have empathy for the emotional well-being of their counselors, several of them still placed some of the blame for burnout or stress on the counselors themselves. Below are a couple of examples: “Some therapists aren’t the best at self-care.” (Human Resources Director) “When you can’t separate yourself from the client, emotionally, then you kind of get very burned out very quickly.” (Program Director)
While self-care and learning how to deal with secondary trauma would be important skills for dealing with stress, it is noteworthy that these interviewees do not see it as the responsibility of the program’s management to create such opportunities. On the other hand, many of the program/clinical directors who did not have retention problems in their programs cited specific initiatives they used to help monitor and alleviate counselor burnout and stress. One strategy was to encourage counselors to take a paid day off that was unplanned, as one program director explained: “I want them to take care of themselves and I told them that from the jump. Like, please, please, please take care of yourself. Our jobs are intense and so hard but you have to be able to balance that…You earn your time and take it off… Because, some days, you just, you wake up and you’re just like ‘f’ this, I’m not doing it today.”
This program director also mentioned that her previous employer would make counselors feel guilty for taking a day off, which she said led to low morale and higher turnover. A clinical director in another facility had a similar perspective: “I try to make sure it’s clear to my therapists that I’m here for you if you need to just come in my office and vent or cry about something, let me know. If you need a day off for self-care, we’ll make it happen, we’ll figure things out.”
This same interviewee said that it was company practice to discuss self-care with counselors during weekly supervision sessions. Similarly, another facility director mentioned using the “Sanctuary Model” during counselor staff meetings, where counselors would “check in” at the beginning of their weekly meetings to discuss their own emotional issues. While only one interviewee mentioned this sanctuary model specifically, others appeared to be using some of the elements, by encouraging counselors to express their own emotions and recognize when they are feeling stressed out.
Counselor burnout and stress are common in the SUD treatment field; these interviews show that programs with low turnover have taken measures to proactively deal with those issues by encouraging paid time off and regularly discussing emotional issues with counselors. An additional strategy for monitoring and treating counselor stress would be administering the Professional Quality of Life (ProQOL) measure. Only one program director mentioned that they used this tool twice each year but it was a deliberate effort to monitor the emotional needs of their counselors and to create opportunities to deal with that stress.
Workload
Seven interviewees (27%) discussed high workload as a contributor to counselor turnover. Workload issues included high caseloads and the amount of paperwork that the job required. Two of those interviewed blamed state requirements specifically for causing these workload issues because of their reporting requirements. For example: “[State Licensing Agency] is always putting in some kind of new program, and staff need to be trained, and then it lasts for a little bit and then it’s not good anymore. It’s a real problem.” (Facility Director)
While others did not mention the state specifically, they implied that high caseloads were a result of inadequate reimbursement for treatment from the state. These programs depended on state funding, so their counselors had high caseloads to cover the costs of running the program. Workload also tied to the previous theme because counselors who felt overwhelmed by paperwork or a high caseload would likely experience burnout and stress, which could lead to them leaving their job.
Private Practice
A considerable number of interviewees (n = 6, 23%) experienced turnover when a counselor left their position to pursue private practice. As one program director explained: “I’m seeing a trend where people will graduate, they’ll do their two years and get supervision and get licensed and go into private practice. And my mind says, I don’t think you know enough to go into private practice.”
Going into private practice appeared to be related to job dissatisfaction, although it was only an option for counselors with a master’s degree. Several interviewees implied that counselors who pursued private practice were attempting to work with a more “desirable” population by not working exclusively with clients in need of SUD treatment. Money appeared to also be related to pursuing private practice, as counselors could bill private insurance once they were licensed.
Management Support
Half of all interviewees (n = 13) viewed management support as a key element in successful retention. For those who had worked in facilities with high turnover, they often cited poor support and leadership by management as a main cause. For example, one clinical director discussed resignations by counselors that occurred within the past year: “The three most recent ones were just poor support from corporate. Yeah, when they leave, they’re like, oh I hope you can stick it out.”
As one facility director said:
“I think the retention really falls on the leadership of the center… If you treat your employees well, and they feel that support from each other…then they’ll stay. I want people to come and I want them to stay because I know that’s going to be good for the client.”
This facility director saw management support as key to retaining good counselors, which would have positive effects on clients. They saw their own role in making sure clients were receiving quality care in the facility.
Management support was also seen as one way to combat the high stress involved in the field: “We had a [client] leave here and then he died two days later from an overdose. That really affects a person. So, it would be nice to have support.” (Clinical Director)
This clinical director viewed management support as a way to mitigate the stress counselors felt that led to burnout, which all interviewees discussed as the chief reason counselors quit.
One element of management support was good communication with counselors. This meant having opportunities for counselors to communicate their feelings and opinions about their work environment. One Human Resource Director cited the management style of having an open-door policy to promote good communication: “Truly listening and hearing people’s feedback.”
Open communication could also relate to counselors feeling like they have a say in major decisions within the organization: “We’re cohesive, engaged in open communication... [Counselors’] voices are heard, it’s not run as a dictatorship; it’s run more of a democracy.” (Program Director/Clinical Supervisor)
Having management committed to these forms of open communication could create an overall culture of inclusion at the facility: “The turnover issue in my previous facility ended up being culture. The culture at times did not end up making you feel included or a part of the solution. You didn’t have an opportunity for input… We felt dictated to… I think that employees will have resiliency as long as they feel a part of, listened to, and have an opportunity to be about the solution.” (Clinical Director)
This quote shows how making counselors feel like they are an important part of the organization could improve their morale and mitigate against the stress they feel in the job. Open communication could create a positive work culture where staff felt valued and supported. One clinical supervisor related how management support and open communication could create a feeling of safety for counselors: “I have been here a long time so people feel safe. They feel this sense, they know what’s expected of them. They know they can come to me. They know they don’t have to be perfect… You stay where you feel safe.”
While this was the only interviewee to explain management support as creating an atmosphere where counselors felt “safe,” it relates to open communication and a sense that management is “taking care” of the staff, which was mentioned by other interviewees.
Another characteristic of management support was supervisor involvement, where clinical and program directors frequently interacted with counselors by offering supervision, covering when counselors were out, or carrying their own caseload of clients. These efforts were seen as creating an atmosphere that everyone was working together and experiencing the same difficulties. Here are two examples from the interviews: “[The staff] say to me how happy they are all the time. And I think it’s, I’m very positive. And I’m there all the time and they’ve said to me that other places they’ve worked, most owners aren’t there… If you’re telling people what to do and you’re not there, I think that impacts the morale of your staff.” (Clinical Supervisor/Owner) “I am on the front lines with them, not just dictating what to do but I actually get in the nitty gritty with them. That may help up morale… I can better understand what they are going through and experiencing.” (Program director/clinical supervisor)
The interviewee above also carried a caseload of 15 and felt that it made him more accessible to the counseling staff he oversaw. Two other clinical directors mentioned carrying a small caseload or helping their counseling staff by taking on clients perceived to be more difficult. Even those who did not individually counsel clients in treatment discussed strategies for staying involved with the day-to-day operations of the facility to demonstrate support for their counselors.
Professional Development
Nine interviewees (35%) discussed how relevant and accessible professional development opportunities could improve retention. This theme related to burnout/stress, in that several clinical/program directors mentioned trainings as a way to learn strategies for handling secondary trauma and self-care to alleviate burnout. The theme also related to management support because interviewees who were more involved with their staff saw it as their responsibility to help counselors get the required trainings completed as well as offered trainings in-house on issues that were relevant to their counselors.
As one clinical director explained: “As far as the professional development goes, management staff are expected to put on webinars and trainings and things like that. So the therapists here find it to be very beneficial because they can continue to grow within their careers.”
This quote shows how management can be actively involved in the professional development of the counselors in their facility. The state requires and offers certain trainings but programs with supportive and involved supervisors saw professional development as something to cultivate for better retention and worked more closely with their counselors to offer them the trainings they wanted.
The rural location of facilities could be an impediment for professional development, especially for programs that were too small to coordinate their own trainings or for new counselors who had to attend the state-sponsored trainings during their first year. Many interviewees complained that the locations for the state-sponsored trainings were far away and required significant travel expenses, which was a financial burden for some facilities. One clinical director suggested that the state could also offer more updated and contemporary topics in their trainings, especially for counselors who had been in the field for many years.
Professional development was also used as a retention strategy by covering the costs associated with state certification. Three programs paid for all or part of counselor certification; one paid to have it renewed every 2 years. An additional facility would not pay for the certification but gave counselors a 5% raise once they achieved certification. The interviewees saw certification as a way to promote retention and improve the quality of care in the facility. While covering some or all of the $300 cost associated with certification was not a huge financial incentive, it communicated the importance of professional development to the counseling staff.
Teamwork
Another theme that related to management support was the sense of camaraderie or “teamwork” present in facilities with low turnover. Thirteen (50%) interviewees described their counseling staff as a “team” or “family” and indicated that this dynamic was essential to creating a good workplace environment. These interviewees described counselors supporting each other, as well as receiving support from management, as another way to alleviate stress/burnout. As one facility director said, “It’s a very stressful job… And the counselors need support themselves, from other staff.”
Another program director described the collaborative environment as everyone taking care of each other: “Because we’re small…because our owner’s a social worker…we are focused on taking care of each other.”
Creating a work environment where people felt like they were part of a family or team was likely the result of positive management involvement and support.
About one-third of the interviewees mentioned having team-building events with their staff. These included lunch or dinner events, retreats, coordinating fundraisers together, and other social events (such as a “Paint Night”). One program mentioned having a yearly “Staff Appreciation Day” that included food and games. Another went offsite once a year for “Vision Day” where the staff worked collaboratively on the program’s strategic plan. These activities helped promote a work culture where employees felt valued and appreciated. Counseling staff working well together, or as a “team,” was likely the result of these efforts.
Discussion
Recruitment
Recruiting high-quality counselors was a problem for most of the programs in this study. Figure 1 illustrates how the various themes that emerged from the interviews impacted recruitment and how the themes related to each other. Thematic schema of recruitment problems.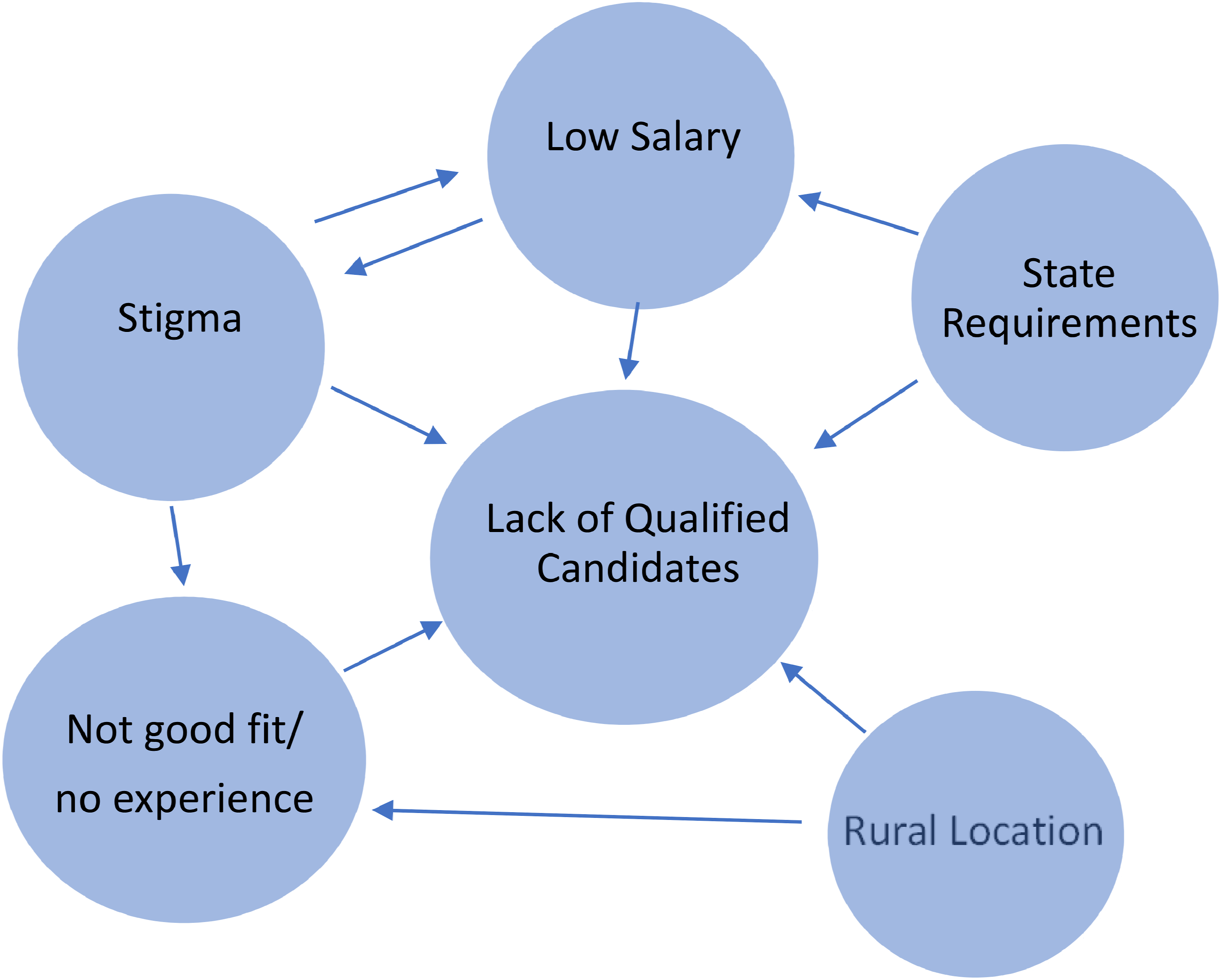
The primary reason offered for recruitment problems was low salary. Considering lower salary has been shown to negatively relate to job satisfaction and increase turnover intentions among counselors (Knudsen et al., 2003; Tsounis et al., 2017), it is likely that a low starting salary would also limit the candidate pool. Interviewees lamented that they found recent applicants were overly concerned with pay and lacked a commitment to helping others. This relates to recent research that revealed how SUD counselors choose their profession because of intrinsic rewards and interest rather than the salary (Oberleitner et al., 2021). The interviewees in this study had similar commitments to the field when they started working so they expected new counselors to have that same passion. However, those expectations might be unrealistic if the starting salary in other fields is higher, considering the amount of student loan debt new graduates might be carrying. Pennsylvania college graduates currently have the third highest average student loan debt in the United States (Balentine, 2021).
This study revealed how inadequate salary could be tied to stigma and the lower status of the addiction treatment field compared to other areas of mental health. Low salary resulted in fewer qualified candidates applying but it also related to the stigma of SUD because other types of mental health treatment paid their counselors higher and received higher reimbursements for services.
Another common theme related to recruitment was that candidates were not the right “fit” for the position and/or lacked clinical experience in SUD treatment. As Figure 1 shows, this theme related to stigma as well because students in counseling programs might choose other fields for internships and practicums due to the negative perception of SUD clients. These negative stereotypes were reinforced by the interviewees, in that they viewed the SUD treatment population as more difficult or emotionally draining than clients with other mental health problems. People with SUD already experience a great deal of public stigma; this research suggests they may also be experiencing stigma within the treatment program (Luoma et al., 2007). In addition, research does not confirm the interviewees’ perceptions about SUD clients. In a recent review of research on burnout among mental health professionals, Yang and Hayes (2020) found that characteristics within the work environment were better predictors of burnout than the types of treatment programs where the counselors worked. The perception that SUD clients are more difficult to counsel, however, may impact recruitment because new counselors are less likely to apply for positions in SUD treatment if they think the job will be more stressful and less rewarding. They may also fear being stigmatized themselves due to their association with such a highly stigmatized group (Madden, 2019; Oberleitner et al., 2021).
Being in a rural location exacerbated these recruitment problems, which have been discussed in other research on SUD counselor recruitment in rural areas (SAMHSA, 2016; Snell-Rood et al., 2021). Many of the counties where these facilities were located experienced population declines and few had higher education opportunities nearby that could provide a “pipeline” of potential counselors. To meet the demand for high-quality counselors, educational programs at the bachelor’s and master’s levels should offer more courses in SUD and more exposure to the SUD treatment field. Education and experience working in SUD treatment could also help combat the public stigma toward people with SUD (Livingston et al., 2012).
The state requirements for hiring counselors also inhibited recruitment both directly and as a contributor to low salary (Figure 1). Previous research on this topic has overlooked the role that the state plays in helping or hindering recruitment in rural areas. Given the education and experience requirements necessary to work as a counselor in a state-licensed facility, the agency that mandates these requirements should work more closely with other state agencies (including the department of education) to ensure that an educated, experienced workforce is available in rural areas. This could include student loan forgiveness for SUD treatment staff, which would be an incentive for recruitment. They could also lead anti-stigma campaigns to help combat the negative perceptions of clients in SUD treatment. With the influx of money from opioid-related lawsuits, the state should consider funding initiatives that could help counselor recruitment.
Retention
While counselor recruitment was a major challenge, turnover was not viewed as a problem in most treatment programs. Still, interviewees felt that the SUD treatment field lost a lot of counselors due to stress and burnout, which is well documented in the literature on counselor turnover (Garner and Hunter, 2013; Knudsen et al., 2008; Landrum et al., 2012; O’Connor et al., 2018). While counselor burnout is an established cause of turnover, these interviews revealed that program/clinical directors often perceived burnout to be worse for counselors in SUD treatment programs. The stigma of SUD was reinforced by the notion that clients in SUD treatment are more difficult to work with, less likely to change their behaviors, and create more emotional stress. However, research on burnout in other counseling areas, such as social workers and school counselors, suggests that all counseling fields experience high levels of burnout and turnover (Dreison et al., 2018; Kim & Stoner, 2008; Kim & Lambie, 2018; Wardle & Mayorga, 2016). The interviewees may view the SUD treatment field as more difficult, but emotional stress and burnout are pervasive in all counseling fields.
The programs that did not have turnover problems appeared to have organizational practices that facilitated management support and involvement. These were deliberate efforts to improve counselor retention. Management support included being involved in the day-to-day operations of the program, sometimes even carrying their own caseload of clients. These programs created a positive working environment where clinical staff and management worked as a team. Management cultivated this teamwork by organizing team-building activities, like group meals, strategic planning retreats, and other outings. They also promoted professional development opportunities for the staff, which were seen to improve morale. Research has shown that organizational factors like perceived fairness, communication, and support can alleviate counselor burnout and improve job satisfaction, possibly reducing turnover intention (Beitel et al., 2018; Ducharme et al., 2007; Fukui et al., 2019; Knudsen et al., 2003; McNulty et al., 2007; Oberleitner et al., 2021; Oser et al., 2013; Shoptaw et al., 2000; Skinner & Roche, 2021). This study revealed specific practices that could lead to these counselor perceptions which could improve retention.
A related strategy that clinical and program directors cited to improve retention was promoting self-care among the clinical staff. Supportive management emphasized that counselors should be able to use paid time off to help alleviate their stress. Programs that have had high turnover should consider implementing some of these strategies to monitor counselor’s emotional exhaustion and burnout, as well as offer trainings and resources to alleviate the stress and trauma of counseling clients in SUD treatment. Interviewees suggested that dealing with a client’s relapse could increase stress and burnout; counselors need more education and training in understanding relapse as part of the recovery process and how to manage their stress in dealing with setbacks.
While many of these issues (such as burnout, management support, and training) are important to the operation of both urban and rural treatment programs, the rural location of programs could exacerbate problems or make solutions more difficult. For example, those working in rural programs are more isolated from the professional development opportunities that could help them manage the stress associated with their job. Counselors could also face difficulties accessing mental health services for themselves, given the lower availability in rural areas (Kirby et al., 2019). State agencies should consider ways to make training more accessible to people in rural areas, possibly by increasing the availability of virtual trainings.
Conclusion
Counselor recruitment is a major problem for SUD treatment programs in rural Pennsylvania counties. Interviews with program and clinical directors revealed their concerns about the number of qualified applicants for open positions and uncovered strategies that could improve recruitment and retention. Given the increased demand for SUD treatment in Pennsylvania, as well as other states impacted by the opioid crisis, it is crucial to fully staff programs with counselors who can offer high-quality treatment.
The research has several limitations. One is that the actual turnover rates of facilities were not collected; program/clinical directors who reported high retention may have been overstating the benefits of their organizational practices. Future research could examine treatment programs more closely, possibly through participant observation, to get a fuller picture of the organizational dynamics that contribute to the retention of high-quality counselors. Additional qualitative and quantitative research with counselors about management practices would help identify the specific factors that contribute to job satisfaction and turnover intentions. The large number of program/clinical directors who did not respond to the interview request is also concerning, although the interview sample obtained oversaw 25% of all rural programs in Pennsylvania and these programs varied in size, structure, and location. This research began early in the COVID-19 pandemic, which likely impacted the response rate.
Despite the limitations, this research is noteworthy because there is a lack of qualitative research on this topic. The qualitative approach provided an in-depth examination of how SUD treatment programs’ administrators perceive recruitment and retention issues and how they are responding to the demand for more counselors. The focus on program and clinical directors also adds a new perspective to much of the research on this topic, which tends to be at the counselor level. Future research, both qualitative and quantitative, could elaborate on the specific practices that are used to create a sense of management support and involvement.
While the research focused on rural treatment programs, the strategies that emerged for improving recruitment and retention could be implemented in urban and suburban settings as well. Rural programs deserve special consideration, however, given their unique constraints for recruiting and retaining high-quality counselors and the impact that the opioid crisis has had on rural communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was made possible, in part, by a grant from the Center for Rural Pennsylvania, a legislative agency of the Pennsylvania General Assembly.