
Abstract
Although the association between type 2 diabetes mellitus (T2DM) and oral disease has been widely investigated, little is known about long-term dental care patterns before T2DM diagnosis. This study therefore described dental service utilization up to 30 y prior to the incidence of a T2DM, compared with age- and sex-matched controls. This matched cohort study used nationwide Danish registry data on individuals born between 1950 and 1970 who maintained permanent residency from 1990 to 2021. For each person with incident T2DM in 2021, 4 age- and sex-matched controls were selected. Incident T2DM was identified based on the purchases of glucose-lowering medication or a hospital diagnosis. Dental service utilization included receipt of any dental care, periodontal, endodontic, restorative, and extraction treatments. Time trends were analyzed using logistic and Poisson regression models. Among 1,231,846 eligible individuals, 10,205 had incident T2DM in 2021 and were matched to 40,820 controls. The incident T2DM population was less likely to receive dental care in a calendar year than the controls and had 2.4 (95% confidence interval [CI]: 2.2 to 2.6) fewer years with a dental visit in the years preceding the diagnosis. The individuals with incident T2DM were more likely to have received periodontal (risk ratio: 1.08, 95% CI 1.05 to 1.12) and endodontic treatments (risk ratio: 1.14, 95% CI: 1.11 to 1.17), and they had received more extractions (rate ratio: 1.32, 95% CI: 1.29 to 1.36) and slightly more restorative treatments (rate ratio: 1.02, 95% CI: 1.00 to 1.04) during a calendar year over the period preceding the T2DM diagnosis than did the controls. More than 30 y prior to diagnosis, individuals who developed T2DM were less likely to attend dental care, but when they did attend, they underwent more complex and invasive procedures. These findings support a common risk factor approach to prevent T2DM and oral diseases at the clinical, health system, and policy levels.
Introduction
Type 2 diabetes mellitus (T2DM) develops over a long preclinical phase marked by metabolic dysregulation and low‑grade systemic inflammation (Kyrou et al 2020; Sanches et al 2023; Cifuentes et al 2025). Previous studies have suggested that T2DM is associated with periodontitis and other oral conditions, such as dental caries, endodontic lesions, and tooth loss (Wu et al 2020; Bitencourt et al 2023; Chung et al 2025; Alves-Costa et al 2025). These oral conditions have also been found to be associated with incident T2DM (Stohr et al 2021; Heikkila et al 2022; Nygaard et al 2025). Patterns of dental service utilization (eg, frequency of preventive visits versus need for periodontal, restorative, or extraction services) reflect both oral disease burden and health‑seeking behaviors shaped by complex biopsychosocial factors that are themselves linked to T2DM risk (Agardh et al 2011; Kolb and Martin 2017; Pronk et al 2024).
Earlier studies have indicated that individuals with or developing T2DM are less likely to visit dental services and more likely to receive more invasive treatments, suggesting poorer oral disease status (Tomar and Lester 2000; Macek et al 2008; Zhang et al 2021; Aldosari et al 2022; Nurminen and Rättö 2023; Raittio et al 2024). However, it remains unclear how far back in time dental care utilization patterns begin to diverge between individuals who eventually develop T2DM and those who do not. Scarce prior research on dental service utilization prior to T2DM diagnosis has focused on relatively short, 7 y (Raittio et al 2024) or 1 y (Nurminen and Rättö 2023) preceding T2DM onset. The diagnosis itself may be insufficient to produce a rapid or sizable change in T2DM patients’ dental service utilization patterns (Nurminen and Rättö 2023; Raittio et al 2024).
In this context, strong confounding between prior dental utilization and incident T2DM is likely. Both are shaped by shared determinants that influence both dental care use and future T2DM risk, such as health behaviors and socioeconomic conditions. Many of these determinants vary over time and can themselves be affected by oral health and dental care. For example, smoking and diet affect oral health and are the targets of, and thus potentially modified by, dental care, just as they may influence T2DM risk and later socioeconomic status, which in turn may affect subsequent oral health and dental care. Extensive adjustment for this time‑varying confounding can attenuate associations and may obscure where, in the observed population, higher dental needs and future T2DM co‑occur due to shared time‑varying causes. Yet it is precisely this unadjusted co‑occurrence that clinicians and health systems encounter in practice, rather than the model‑dependent, adjusted association between oral health or dental care utilization and incident T2DM (Fox et al 2022). Moreover, many prior studies are constrained by selection bias from conditioning on voluntary participation, insurance status, or specific providers, producing nonrepresentative samples and biased causal estimates (Wong et al 2026).
Taken together, these considerations support a descriptive, population‑focused approach as more informative for clinical, health, system and policy planning than weak etiologic, risk‑factor analyses (Fox et al 2022). Accordingly, our focus is descriptive rather than causal: we examine dental service use by eventual T2DM status, with comparisons matched on age and sex. Using nationwide Danish registries that provide practically complete population coverage, long-term follow-up, and provider-recorded dental procedure codes, this study aimed to investigate the use of dental services up to 30 y preceding incident T2DM diagnosis, compared with age- and sex-matched individuals who did not develop T2DM. We also investigated these patterns in selected demographic and socioeconomic subgroups.
Materials and Methods
This study used data from a nationwide Danish register-based prospective cohort. In Denmark, every resident is assigned a unique civil registration number linked to the Danish Civil Registration System, which tracks vital status, migration, and emigration. The data include all Danish residents aged 20 y and older between 1990 and 2021. Individuals entered the cohort by immigration or when turning 20 y of age. Participants remained in the cohort as long as they lived and retained permanent residency in Denmark.
Via pseudonymized civil registration numbers assigned to all residents of Denmark in the Civil Registration System, we linked information from the National Health Service Register, the Register for Selected Chronic Diseases, the Educational Register, and the Income Statistics Register.
The study was registered with the Danish Data Protection Agency (2015-57-0002) and Aarhus University (2016-051-000001-914). According to Danish legal regulation, registry-based studies like this do not require individual informed consent. The RECORD checklist for reporting observational studies using routinely collected health data was followed.
Incident T2DM
In the Register for Selected Chronic Diseases (Danish Health Data Authority 2024), the incident date of T2DM was defined as the time point when an individual met 1 of the 2 criteria for the first time: (1) had at least 2 purchases of glucose-lowering medication in the Danish National Prescription Registry and (2) had a relevant primary or secondary diagnosis (ICD-10 code E11) or any of its subcategories (e.g., complications or manifestations) recorded during any inpatient, emergency, or outpatient hospital visits in the Danish National Patient Registry. Individuals who likely had type 1 diabetes, polycystic ovary syndrome, or gestational diabetes were excluded (Appendix). A validation study showed that this method of identifying T2DM in the Register for Selected Chronic Diseases had a sensitivity of 0.91 (95% confidence interval [CI]: 0.89 to 0.92), specificity of 0.99 (95% CI: 0.99 to 0.99), and positive predictive value of 0.90 (0.88 to 0.91) when compared with self-reported T2DM status (Isaksen et al 2023).
Final Sample Selection and Follow-Up
From the nationwide cohort, we defined a source population of individuals born from 1950 to 1970 who had continuous permanent residency in Denmark from January 1, 1990, to December 31, 2021. Incident T2DM cases were those with a first T2DM registration (as per the registry definition above) during 2021 (index year). For each case, 4 sex- and exact birth year–matched comparators were randomly selected among persons who were alive and resident in Denmark on January 1, 2021, and free of registered incident T2DM during 1995 to 2021. Restricting the study population to the 1950 to 1970 birth cohorts minimized the misclassification of unrecorded pre‑1995 T2DM because the prevalence in these cohorts was low before 1995, <1% (Carstensen et al 2020).
Dental Care Utilization
Adult dental services in Denmark are delivered by private practitioners under a universal publicly subsidized scheme that covers diagnostic, preventive, and basic restorative and surgical treatments (excluding prosthetic rehabilitation), with all subsidized services for residents recorded in the National Health Service Register since 1990 (Andersen et al 2011). Using the subsidized service codes, the following 3 binary outcome variables (yes/no) representing the care received during a calendar year were formed: (1) any dental service, (2) periodontal care services (subgingival scaling or periodontal surgery), and (3) endodontic treatments (Appendix). In addition, the annual numbers of restorations and extractions were used as count outcome variables.
Demographic and Socioeconomic Covariates
Information regarding the highest educational attainment, income percentile, main source of income, region, and country of birth were obtained from the national Danish registers (details in the Appendix).
Statistical Analysis
We summed outcomes across years to compare total dental service use between the incident T2DM and comparison populations over the entire period (1990 to 2021).
Trends in dental service utilization in the incident T2DM and comparison populations were investigated using logistic regression for the binary outcomes and Poisson regression for the count outcomes. These models included an interaction term between the incident T2DM/comparison status and a natural cubic spline transformation of calendar year (1990 to 2021) with 4 knots.
Findings from these models are reported as (1) average annual predictions by the incident T2DM and comparison status, (2) risk/rate ratios of these average annual predictions, and (3) average predictions aggregated (pooled) over the period preceding the T2DM diagnosis. Confidence intervals (95%) for the average prediction and risk/rate ratios were generated using cluster-robust standard errors.
We also investigated whether the incident T2DM and comparison populations had different dental service utilization patterns over the follow-up across the year of birth (1950 to 1970), gender, demographic, and socioeconomic groups. We thus included an interaction of the incident T2DM/comparison status, a natural cubic spline transformation of calendar year (1990 to 2021) with 4 knots, and 1 covariate at the time to the logistic regression and Poisson regression models (Appendix).
As sensitivity analyses, we applied a similar sample selection and analytical strategy to investigate differences in dental service utilization between the incident T2DM and comparison populations among individuals born between 1971 and 2000, with follow-up starting in the year they turned 20 y and incident T2DM occurring in 2021.
All analyses were conducted in R (v. 4.5.1).
Results
Among 1,231,846 individuals born between 1950 and 1970, who maintained permanent residency in Denmark from 1990 to 2021 and had not developed T2DM between 1995 and 2020 (Fig 1), a total of 10,205 (0.8%) developed incident T2DM in 2021. For each of these individuals, 4 age- and sex-matched comparisons were selected (n = 40,820). Of the selected population, 58% were men, and the median age was 61 y (Q1 = 56, Q3 = 66) in 2021, while it was 30 y (Q1 = 25, Q3 = 35) in 1990. People who developed incident T2DM were more likely to have been born outside Denmark, to have only a primary school education, to have a lower income, and to be unemployed or receiving social assistance, sickness benefits, or disability pensions in 2021 (Table 1). Differences in income percentile and source of income between the incident T2DM and comparison populations were smaller in 1990 and 2005 than in 2021 (Table 1).

Sample selection process.
Descriptive Statistics of the Incident Type 2 Diabetes Mellitus (T2DM, n = 10,205) and Comparison Populations (n = 40,820) in 1990, 2005, and 2021.

Median (Q1, Q3).
Over the period preceding the diagnosis, people who developed T2DM had, on average, 2.4 (95% CI: 2.2 to 2.6) fewer years with any dental care visit between 1990 and 2021 than the comparison population (mean ± SD: 21 ± 10 vs 24 ± 9 y; P < 0.001) (Table 2). The incident T2DM population also had a slightly higher number of years with periodontal and endodontic care and on average had 1 more extraction over the follow-up period than the comparison population.
Total Number of Years with Any Dental Care, Periodontal Care, or Endodontic Treatment and Total Number of Restorations and Extractions Received in the Incident Type 2 Diabetes Mellitus (T2DM, n = 10,205) and Comparison Populations (n = 40,820) from 1990 to 2021.
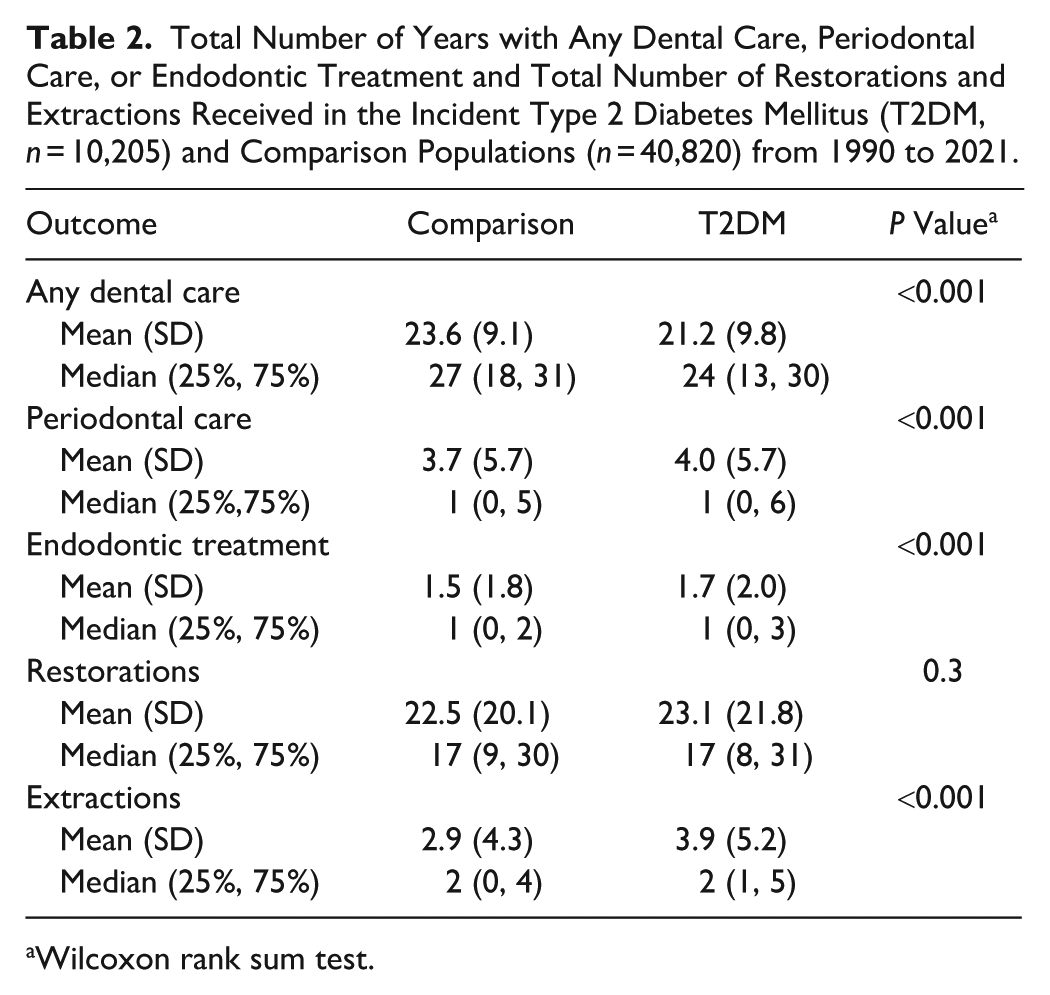
Wilcoxon rank sum test.
In 1990, the comparison population had a 6.4 (95% CI: 5.5 to 7.3) percentage point higher probability of receiving any dental care than those who developed T2DM in 2021. By the end of the follow-up, this difference had increased to 8.3 (95% CI: 7.4 to 9.3) percentage points (Fig 2A). In relative terms, the incident T2DM population had 0.92 (risk ratio, 95% CI: 0.91 to 0.93) times lower probability of receiving any dental care in 1990 and 0.88 (risk ratio, 95% CI: 0.87 to 0.89) times lower probability in 2021 (Fig 3A). Already in the early 1990s, the incident T2DM population had a slightly higher probability of receiving periodontal treatment, endodontic treatment, and a higher number of extractions and restorations compared with the comparison population (Figs 2B–E and 3B–E). These differences narrowed toward the end of the follow-up period, except for the number of extractions (Figs 2B–E and 3B–E).

Estimated average probabilities or counts of dental care received during a calendar year in the incident type 2 diabetes mellitus (T2DM) and comparison populations from 1990 to 2021. Shaded areas represent 95% confidence intervals. (

Rate or risk ratios of the estimated average probability or count of dental care received during a calendar year between the incident type 2 diabetes mellitus (T2DM) and comparison populations from 1990 to 2021. Shaded areas represent 95% confidence intervals. (
Pooled across all follow-up years, the incident T2DM population was less likely to receive any dental care in a calendar year (risk ratio 0.90, 95% CI: 0.89 to 0.91), more likely to receive periodontal (risk ratio 1.08, 95% CI: 1.05 to 1.12) and endodontic treatments (1.14, 95% CI: 1.11 to 1.17) in a calendar year, and they received more extractions (1.32, 95% CI: 1.29 to 1.36) and slightly more restorations (1.02, 95% CI: 1.00 to 1.04) per year than the comparison population did.
Differences in dental care utilization over the follow-up between the incident T2DM and comparison populations were of similar magnitude across most demographic and socioeconomic subgroups (Appendix Table S1). Some noteworthy exceptions were as follows: differences in the probability of receiving periodontal and endodontic treatments and in the number of restorative treatments between the incident T2DM and comparison populations were smaller in the older cohorts (born early 1950s) than in the younger cohorts (born late 1960s). In the lower income and education groups, differences in the predicted annual probability of receiving periodontal and endodontic treatments between the incident T2DM and comparison populations were minimal but more pronounced in the higher income and higher educational attainment groups.
In sensitivity analyses of individuals born from 1971 to 2000 (Appendix Figs S1 and S2), patterns of dental service utilization were similar to those in the main analyses. However, the difference in the number of restorative treatments between the incident T2DM and comparison populations was larger (rate ratios around 1.1 to 1.2 annually) than in the 1950 to 1970 cohorts.
Discussion
This nationwide population-based study has revealed that individuals who developed incident T2DM in 2021 were consistently less likely to utilize dental services than their age- and sex-matched counterparts over many years preceding the diagnosis, with this disparity evident as early as the 1990s and widening over time. Over the 3-decade observation period, the incident T2DM group had, on average, 2.4 fewer years of use of any dental care compared with the comparison group. Despite lower overall utilization, the incident T2DM population had undergone more invasive procedures, such as periodontal and endodontic treatments, restorations, and extractions, highlighting that individuals on a trajectory toward T2DM were already experiencing a greater oral disease burden decades long before their T2DM diagnosis.
As a limitation, it should be noted that information on T2DM incidence was restricted to individuals who maintained permanent residency in Denmark from 1990 to 2021. As a result, only individuals who were alive at the index date (2021) were included, and dental care utilization among those who died during the study period was not captured. Given the approximately 90% sensitivity of T2DM detection (Isaksen et al 2023) and lacking pre-1995 incident T2DM data, some people with T2DM may have been misclassified into the comparison population. This misclassification, however, seems minor relative to the general underdiagnosis of T2DM reported in Denmark (Jorgensen et al 2020). While we were unable to account for clinical measures of oral disease severity, the wide range of dental procedures investigated, from restorations to extractions, can be used as proxies for oral health status. Finally, as Denmark is a high-income country with universal health coverage and a relatively low national burden of diabetes compared with other lower-income countries (Ong et al 2023), the worldwide generalizability of these findings may be limited.
Notwithstanding these limitations, this study was able to address limitations common in other studies, including self-reported dental or T2DM status (Stohr et al 2021), potential selection bias from baseline nonparticipation and subsequent sample attrition in cohort studies (Stohr et al 2021), or related to the use of information available to only a small part of the population of interest (Heikkila et al 2022; Nygaard et al 2025). Our findings also extend previous research by demonstrating that differences in dental service utilization among people with T2DM is a phenomenon that stretches way beyond the previously reported 7 y before or after the diagnosis (Raittio et al 2024). Moreover, to avoid the interpretational ambiguity that can arise from partial or excessive adjustment for potentially confounders, colliders and mediators, as often done in the earlier studies, we adjusted only for age and sex while intentionally not adjusting for variables likely to be shared causal factors or potentially lie on a causal pathway from oral diseases to incidence of T2DM. This approach aligns with calls to revitalize descriptive epidemiology by prioritizing transparent and population‑relevant contrasts over weak etiological, risk factor analyses (Fox et al 2022), which also plague the oral-systemic research (Raittio and Farmer 2021; Schuch et al 2023).
In line with earlier research, the observed inverse relationship between lower routine dental attendance and higher rates of restorative, periodontal, extraction, and endodontic treatments suggest a predominantly reactive, symptom‑driven model of dental care utilization in those who later develop T2DM. Their oral conditions appear to progress until they are more likely to require irreversible or complex interventions when accessing dental care. These trends, detectable even decades before the incidence of T2DM, indicate that deterioration in oral health may manifest in parallel with other diabetes risk factors long before metabolic dysfunction becomes clinically or diagnostically evident (Tabak et al 2012; Kyrou et al 2020; Sanches et al 2023; Cifuentes et al 2025). In line with this, it has also been reported that individuals who develop T2DM exhibit approximately double the cardiovascular disease event risk up to 30 y before diagnosis compared with those who do not, with the difference being highest closer to the onset of T2DM (Gyldenkerne et al 2024). The relative increases in invasive dental treatments we observed were clearly less than the double. Interestingly, relative differences in the probability of receiving periodontal and endodontic treatments were larger decades before than closer to the onset of T2DM. However, these findings are difficult to interpret, as they are likely to reflect a complex mix of higher disease activity and treatment needs, different patient preferences/values, lower utilization, and a higher number of extracted teeth over the life course. Nevertheless, these findings highlight how oral diseases and dental care utilization are likely associated with conditions such as T2DM through a complex network of upstream determinants including lifestyle factors such as unhealthy diet, smoking, body fat composition, and physical inactivity, in addition to genetic and perinatal factors and childhood, socioeconomic, and mental health adversities (Dalene et al 2023; Pronk et al 2024; Alves-Costa et al 2025). Therefore, a common risk factor approach (Sheiham and Watt 2000), which targets these shared, frequently clustered determinants (Birch et al 2019; Dalene et al 2023) should be the approach promoted to tackle the noncommunicable disease burden. This aligns with World Health Organization priorities to integrate oral health within broader noncommunicable disease prevention (World Health Organization 2024).
Even though the population-wide reduction of shared clustered risk exposures remains the cornerstone of preventing T2DM and oral diseases, our findings also indicate a need to revise national dental prevention strategies for high-risk or disadvantaged groups to strengthen oral health promotion as a goal in its own right. Moreover, dental services may positively influence some shared determinants, such as smoking and healthy diet and drinking habits, particularly when integrated into universal and coordinated multisectoral prevention actions (Watt and Sheiham 2012). In our view, any potential beneficial effects of dental care on systemic inflammation and T2DM risk should be regarded as an additional advantage, complementing its primary role in promoting oral health and modifying shared behavioral and social determinants of health.
Although all Danish adults are entitled to subsidized fee-for-service dental care provided by private practitioners, barriers persist for disadvantaged populations (Hede et al 2019; Skov Kristensen et al 2024; Baelum et al 2025). Our finding that differences in receipt of periodontal and endodontic treatments between the incident T2DM and comparison populations were minimal in the lower income and education groups may reflect such barriers to obtaining needed care. Municipalities are mandated to arrange care for adults unable to use private clinics because of mental or physical impairments, yet many eligible individuals remain unreached, likely due to bureaucratic hurdles in the enrolment process (Hede et al 2019; Skov Kristensen et al 2024). Streamlining enrollment; proactively identifying eligible individuals; revisiting and, where appropriate, expanding eligibility criteria for higher subsidization programs; and enabling earlier preventive engagement may help narrow these disparities in access to dental care and oral health.
To conclude, over a period of up to 3 decades preceding the incident T2DM diagnosis, individuals who developed T2DM were less likely to use dental services than their age- and sex-matched comparators and, when attending, received more complex and invasive procedures. These findings support a common risk factor approach to prevent T2DM and oral diseases at the clinical, health system, and policy levels.
Author Contributions
E. Raittio, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; F.V. Bitencourt, contributed to conception and design, data interpretation, drafted and critically revised the manuscript; V. Baelum, contributed to conception and design, data acquisition and interpretation, critically revised the manuscript; R. Lopez, contributed to conception and design, data interpretation, critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261432661 – Supplemental material for Dental Service Use during the 30 Years before Type 2 Diabetes Onset
Supplemental material, sj-docx-1-jdr-10.1177_00220345261432661 for Dental Service Use during the 30 Years before Type 2 Diabetes Onset by E. Raittio, F.V. Bitencourt, V. Baelum and R. Lopez in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Danish Rheumatism Association (Gigtforeningen, #R171-A5894) for the financial support for the project database. FVB is supported by a research grant from the Danish Diabetes and Endocrine Academy, which is funded by the Novo Nordisk Foundation (grant NNF22SA0079901).
Data Availability Statement
The data that support the findings of this study are available from Statistics Denmark. Restrictions apply to the availability of these data, which were used under license for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.