
Abstract
Groups with low socioeconomic status are less likely to make planned dental visits even though routine attenders have fewer caries and less tooth loss. Because behavioral interventions positioned in urgent dental care may improve health and inequalities, RETURN, which involved a nurse conversation supported by videos, booklets, and goal/action-plan setting, was developed. The objective of this study was to investigate the effectiveness of the RETURN intervention at increasing planned dental visits and lessening the oral health impact. Adults attending 14 National Health Service urgent dental services were recruited to a randomized controlled trial and followed up after 6, 12, and 18 mo. Co-primary outcomes were (1) planned visits at 12 mo as measured by Business Services Authority (BSA) data and (2) Oral Health Impact Profile (OHIP) summary score at 12 mo adjusted for baseline. Of the 1,176 consenting adults who were randomized, 591 were allocated to the RETURN group. More than half (55.2%, 315 intervention; 54.7%, 310 control) lived in the lowest Index Multiple Deprivation decile. RETURN participants had a 20% greater odds of planned care as recorded by the BSA at 12 mo (odds ratio [OR] = 1.21; 97.5% confidence interval [CI] = 0.86, 1.70; P = 0.217). There was a reduction (improvement) in OHIP scores at 12 mo in both groups (RETURN group, mean = −7.4, standard deviation [SD] = 12.9; control group, mean = −6.2, SD = 12.9). The least squares mean of the RETURN Modified Dental Anxiety Score decreased with time (anxiety improved) whereas it increased (worsened) in the control group (Modified Dental Anxiety Scale time and treatment group interaction = −0.01; CI = −0.03, 0.00; P = 0.027). RETURN participants had a more than 3 times greater odds of attempting to make an appointment, with the treatment effect increasing with time (at 18 mo: OR = 3.39; 95% CI = 1.83, 6.27; P = 0.0001). We are moderately certain RETURN produced small, consistently favorable effects on routine visits, oral health impact, and dental anxiety despite limited-service availability. RETURN also significantly increased attempts to make routine appointments even in a disadvantaged cohort. This supports integrating behavioral support alongside service reforms to support the transition into continuing care and the optimum use of resources.
Keywords
Introduction
Adult users of dental services can be categorized into routine attenders who attend to preempt problems and problem-oriented attenders who rely on urgent dental care (Gilbert et al 2000). Multiple studies, including longitudinal studies in several countries, show that routine dental visits are associated with fewer caries and less tooth loss and better oral health–related quality of life (Mohd Khairuddin et al 2024). For example, episodic dental attenders in New Zealand had 3 times higher odds of losing a tooth than their routine visiting counterparts did (Thomson et al 2000). Analyses support the conclusion that routine dental visits are beneficial because they allow increased oral health knowledge, prevention, and early intervention rather than being merely a “healthy user effect.” Indeed, the longer routine attendance is maintained, the stronger the effect (Thomson et al 2010).
Interventions targeting problem-oriented attenders are therefore an important tool for improving oral health. Surprisingly, given how significant the issue is, and pertinent to almost all health systems, evidence in this area is scarce (Currie et al 2021). Since dental visiting is a complex behavior nested in a web of causation, prioritizing addressing factors most amenable to “practical” intervention is advised (Krieger 1994; Harris et al 2017). Positioning interventions in urgent dental care therefore seems reasonable, especially since opportunistic interventions during illness visits have been shown to harness a “teachable moment” when advice is most persuasive and relevant to patients’ needs (Cohen et al 2004). Although brief preventive interventions (eg, smoking cessation) delivered in emergency departments have been shown to be effective (Pope et al 2024), this approach has never been used in dentistry.
RETURN (InteRvention to rEduce inequaliTies in the Uptake of Routine deNtal care) is a brief intervention derived from a synthesis of theory (Harris et al 2017), with mapping of behavioral determinants to behavior change techniques. It was designed involving target users from disadvantaged groups (Harris et al 2023). Its aim was to increase planned dental visiting and, through care received, reduce poor oral health impacts. The intervention involves a conversation based on motivational interviewing principles leading to goal and action planning, supported by short videos, a booklet pack, and follow-up text (Harris et al 2022, 2023, 2024). The aim of the RETURN randomized controlled trial was to establish the effectiveness and cost-effectiveness of the RETURN intervention delivered in urgent dental care. The trial was powered on 2 primary outcomes: first, on the record of planned visits within 12 mo of baseline as measured by centrally held (Business Services Authority [BSA]) data, and second, using summary scores at 12 mo adjusted for baseline of self-reported oral health–related quality of life. This article reports the primary and secondary outcomes (SOs). The analysis of socioeconomic effects, health economic evaluation, patient and public involvement and engagement, and embedded qualitative work will be published separately.
Methods
The trial protocol has been published (Harris et al 2022) and is reported here in summary, in line with CONSORT guidelines (Hopewell et al 2025). See Appendix 1 for further details.
Trial Design
This was a 2-arm randomized, parallel-group, open-label, superiority study. The allocation ratio between the intervention and control (standard care) was 1:1. The trial was registered at isrctn.com (ISRCTN84666712). Ethical approval was obtained (21/LO/0059). Intervention delivery took place after trial randomization and during the urgent care appointment - either before or after dental treatment, depending on clinic flow. Follow-up was 6, 12, and 18 mo after randomization by telephone, email, or post.
Participants
Adults aged 18 y or older attending urgent dental care in 13 dental practices or Liverpool Dental Hospital (LDH) in Merseyside and Cheshire, North-West England, were approached to take part. Eligibility criteria were those who had not visited a National Health Service (NHS) or private dentist for a non-emergency appointment for 2 y or more and who did not have a dentist for routine care, were able to provide contact details for follow-up, had adequate English language to participate, and were responsible for making their own dental appointments. Exclusion criteria were previous participation in the RETURN feasibility study or being related to/living with a participant. Although the intervention was designed to be especially relevant to urgent care users from disadvantaged groups and to reflect their social identity, we did not limit or weight recruitment according to socioeconomic factors.
Recruitment, Randomization, and Blinding
The unit of randomization was individual patients. Following screening for eligibility, informed consent was sought, eligibility confirmed, and then pre - randomization questionnaires completed. A trials center web-based program generated randomization lists using block randomization with random variable block length, stratified by site. Randomization lists were produced by a statistician independent of the trial. Patient allocations were irrevocably generated upon completion of the web-based randomization form by trained dental staff at sites. Allocation concealment was ensured as the system did not release the randomization code until the patient was consented and the prerandomization questionnaire completed. Due to the nature of the intervention, it was not possible to blind participants, interventionists, or researchers administering follow-up.
Intervention
Trained dental nurses elicited participants’ perceived barriers to routine dental care and helped identify relevant material from a set of short videos and booklets about overcoming barriers to routine care. Participants then set a routine dental visit goal and action plan. Details of intervention development and intervention components are published elsewhere (Harris et al 2022, 2023) and summarized in Appendix 1. Intervention delivery took on average 15.8 min (Lowers et al 2025a, 2025b). The control group received usual care and a video thanking them for participating.
Outcome Measures
The co-primary outcomes were primary outcome 1 (PO1): attendance for a routine appointment within 12 mo in an NHS dental practice as recorded in BSA data; and primary outcome 2 (PO2): oral health–related quality of life (OHRQoL) measured by the summary score of the Oral Health Impact Profile (OHIP-14) at 12 mo after adjusting for the baseline value (Slade 1997). OHIP-14 measured self-reported oral health symptoms experienced over the previous 6 mo. Summary scores ranged between 0 and 56, with worsening OHRQoL indicated by higher scores. PO1 required a match between participant identifiers collected at baseline (date of birth, sex, surname, and first initial) and BSA data. This was for all participants including those recruited in LDH who subsequently received care in an NHS dental practice.
SOs covered care received in the hospital and private practice not captured by BSA data and various data at the 6-, 12-, and 18-mo time points. Information on LDH post-randomization visits was collected by an audit of the LDH clinical records. SOs included self-reported attempts to make routine appointments, self-reported attendance (NHS or private) for routine dental care, BSA record of routine care at a dental practice within 18 mo, change in the OHIP-14 summary score from baseline to 6 mo and OHIP-14 baseline to 18 mo, urgent dental care attendance, antibiotic prescription by dentists, antibiotic prescription by non-dentists (general practitioner/accident and emergency/walk-in center), analgesic prescription, halitosis and bad taste, dental treatment (recorded from BSA data, LDH audit, and self-report at 6, 12, and 18 mo), and dental anxiety measured by the change in the continuous score of the Modified Dental Anxiety Scale (MDAS) (Humphris et al 2009). The protocol details all SO measures (Harris et al 2022).
Sample Size
The sample size calculations are detailed elsewhere (Harris et al 2022). Briefly, a sample size of 559 per group was calculated to give 80% power at α = 0.025 to detect a 9% improvement in the intervention group for PO1. Allowing for 5% loss to follow-up gave a target sample size of 590 per group. For PO2, a 20% loss to follow-up at 12 mo was assumed, so a sample size of 1,180 gave 80% power to detect a minimum clinically important OHIP-14 difference of 2.25 points, with α = 0.025.
Safety Assessment
Active monitoring of safety events included exacerbation of dental anxiety and any adverse events related to the trial.
Statistical Methods
Analysis was according to intention to treat. To allow for co-primary outcomes, the type I error rate was controlled by setting α = 0.025 and confidence intervals at 97.5% for both primary outcomes. PO1 was analyzed using logistic regression models, adjusted for the stratification factor site as a random effect (random intercept only). Sensitivity analyses looked at different levels of BSA data matching and a model that adjusted for any baseline covariates (education level, Index of Multiple Deprivation [IMD], receiving welfare/state benefit, MDAS) previously identified as independent of each other using chi-squared tests for independence. PO2 was analyzed using linear regression adjusted for the baseline value of OHIP-14 and recruitment site as a random effect.
All SO analyses used a 5% significance level. Binary SOs were analyzed using logistic regression models adjusted for site as a random effect (for most outcomes). Continuous SOs were analyzed using repeated-measures mixed-effects linear regression adjusted for the baseline value, the time of follow-up completion, and site. Models also explored the interaction between follow-up time and treatment group. For primary and key SOs, sensitivity analyses included models using multiple imputation for missing follow-up data and models adjusting for baseline covariates. While the trial was powered on co-primary outcomes, whether there was any differential intervention effect by socioeconomic status is of interest. However, equity analyses are reported separately.
Results
Recruitment was between August 2021 and September 2022 and follow-up from January 2022 to April 2024. Figure 1 shows the flow of participants. Of 1,176 consenting participants recruited, 591 were allocated to receive the intervention and 585 to standard care. Intervention compliance was 95.5% with 557 receiving the intervention (n = 8 intervention engagement missing). Reasons for not receiving the intervention were the participant wanting to leave (n = 15), not wanting to receive the intervention (n = 9), and withdrawal of consent (n = 2). Retention was 72% (n = 851) at 6 mo, 67% (n = 785) at 12 mo, and 59% (n = 691) at 18 mo.

CONSORT flow diagram.
Baseline characteristics (Table 1) were similar. The mean age of the intervention participants was 38.5 (SD = 13.8) y, whereas that of the control group was 38.4 (SD = 14.1) y. Just more than half of the intervention participants were female (52.2%, n = 304 intervention; 54.2%, n = 313 control). Most were of White ethnicity (88.7%, n = 518 intervention; 91.9%, n = 531 control). More than half lived in areas with the lowest IMD decile (55.2%, n = 315 intervention; 54.7%, n = 310 control). About 38% of participants were currently unemployed in both the intervention and control groups. Between 37% (intervention) and 25% (control) of these were unable to work because of mental and/or physical disabilities, although the numbers were relatively small in this subgroup and insufficient to conclude an imbalance existed.
Characteristics at Baseline of the 1,176 Adults Consented and Randomized to Participate in the Trial.
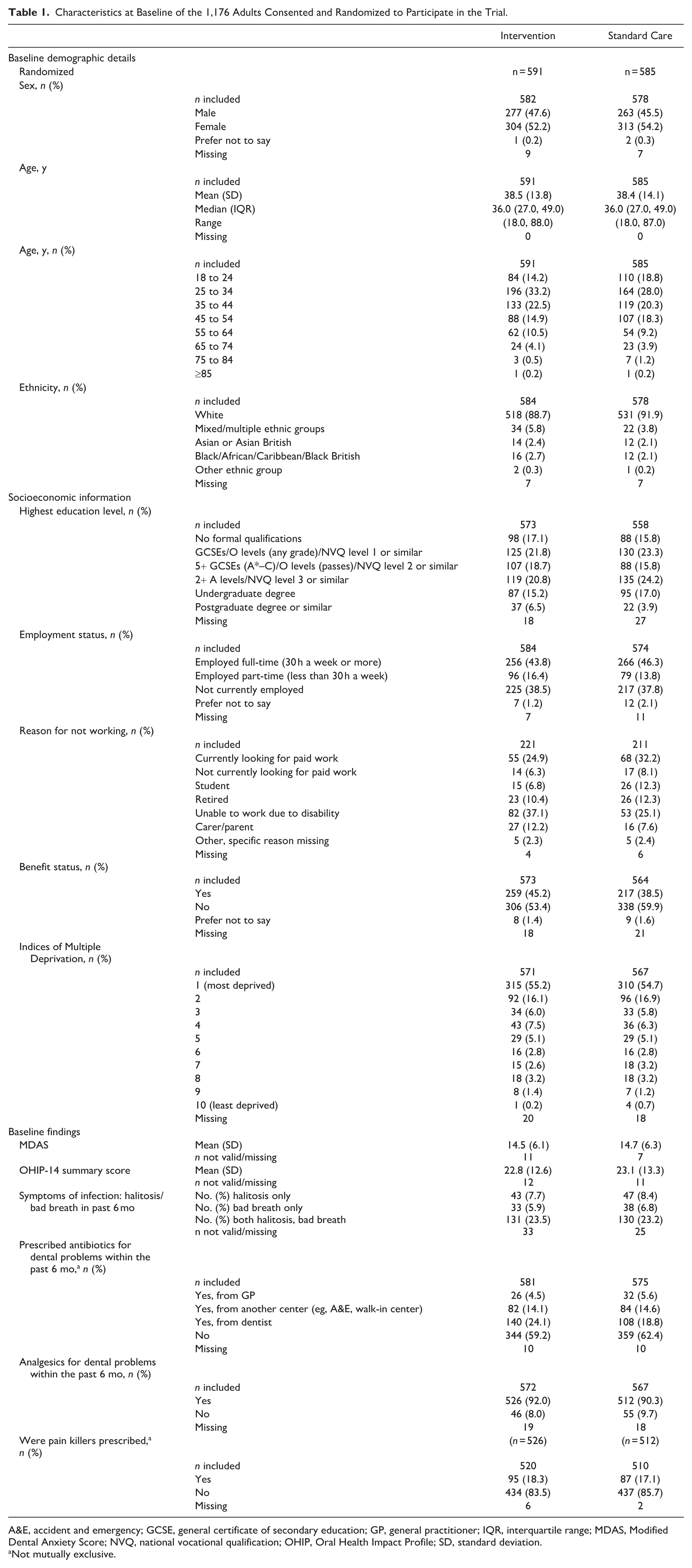
A&E, accident and emergency; GCSE, general certificate of secondary education; GP, general practitioner; IQR, interquartile range; MDAS, Modified Dental Anxiety Score; NVQ, national vocational qualification; OHIP, Oral Health Impact Profile; SD, standard deviation.
Not mutually exclusive.
Routine Attendance Outcomes
PO1 required matching participant identifiers collected at enrollment to BSA patient data, so this analysis involved 85.1% (n = 1,001) of participants, although the baseline characteristics for those matched versus not matched were similar (Appendix Table 1). Results showed a 21% increased odds of intervention participants having an NHS routine appointment within 12 mo, although a 14% decrease to 70% increase are also compatible with data (odds ratio [OR] = 1.21; 97.5% confidence interval [CI] = 0.86, 1.70; P = 0.217; Table 2). Sensitivity analyses produced similar results: extending BSA matching criteria to matching postcodes at follow-up (OR = 1.11; CI = 0.76, 1.60) and including all participants irrespective of BSA data matching (OR = 1.13; CI = 0.82, 1.55). A sensitivity analysis adjusted for baseline covariates, MDAS, and whether receiving benefits also gave similar results (OR = 1.21; CI = 0.85, 1.72).
Mixed-Effects Logistic Regression Model: Attendance for Planned Care within 12 mo (Participants with Matched Baseline Business Services Authority Records and Those Randomized at the Dental Hospital).

CI, confidence interval; RETURN, InteRvention to rEduce inequaliTies in the Uptake of Routine deNtal care.
The SO of routine attendance using BSA data but over a longer time frame (up to 18 mo) showed a slightly greater odds of intervention participants receiving an NHS routine appointment (OR = 1.27; CI = 0.95, 1.68). SOs of self-reported routine attendance showed similar findings of slightly higher odds in favor of the intervention group at each time point, with the highest odds at 18 mo: at 6 mo, OR = 1.11, CI = 0.82, 1.49; 12 mo, OR = 1.16, CI = 0.87, 1.55; and 18 mo, OR = 1.32, CI = 0.97, 1.79. Sensitivity analyses on self-reported routine attendance up to 18 mo adjusting for the baseline covariates education, IMD, and MDAS showed similar findings (OR = 1.33, CI = 0.96, 1.85), as did using multiple imputation, which showed a similar pattern, all favoring the intervention group (OR = 1.20; CI = 0.91, 1.57). All of these SO and sensitivity analyses had the same interpretation as PO1.
Self-Reported Attempts to Make a Routine Appointment
Intervention participants were significantly more likely to report attempting to make a routine appointment than control at 6, 12, and 18 mo (OR = 1.89, CI = 1.36, 2.63; OR = 3.08, CI = 1.88, 5.06; OR = 3.39, CI = 1.83, 6.27, respectively; Table 3). The odds increased over time: at 18 mo, intervention participants had between about 2 and 6 times greater odds of attempting to make an appointment. Sensitivity analyses involving multiple imputation and adjusting for baseline covariates did not change this interpretation.
Mixed Effects Logistic Regression Model Attempts to Make an Appointment within 6, a 12, and 18 mo (Self-Reported).
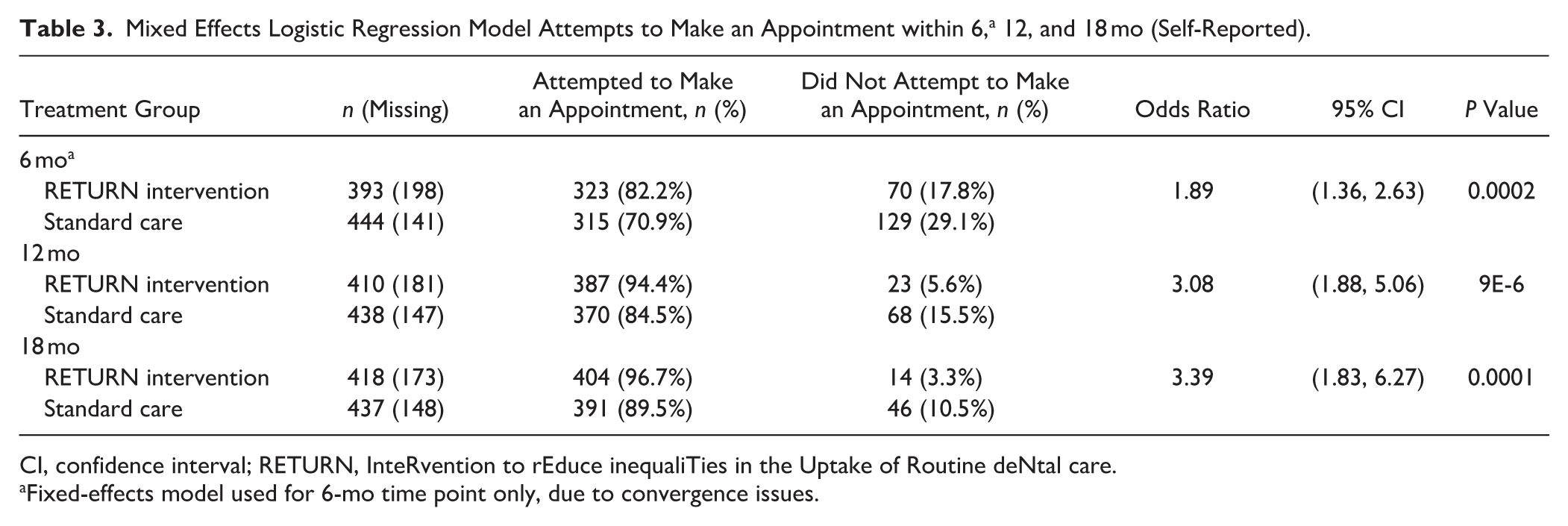
CI, confidence interval; RETURN, InteRvention to rEduce inequaliTies in the Uptake of Routine deNtal care.
Fixed-effects model used for 6-mo time point only, due to convergence issues.
OHRQoL
PO2 found intervention participants had slightly greater improved OHIP-14 scores (mean = −7.4, SD = 12.9) than control participants did (mean = −6.2, SD = 12.9) at 12 mo. Although OHIP-14 scores for intervention participants were slightly lower than for control participants at baseline (Table 1), this was more pronounced at 12 mo (mean = 15.0, SD = 13.6 intervention; mean = 16.0, SD = 14.4 control). Mixed-effect linear regression model estimates showed a treatment effect of −1.12 (on average, intervention participants had better OHRQoL), although an effect of −3.08 and +0.83 are also compatible with findings (97.5% CI = −3.08, 0.83; P = 0.197). While only 50.7% (596) participants responded at all follow-ups (6, 12, and 18 mo), multiple imputation and sensitivity analyses for PO1 did not change the interpretation of results. Figure 2 shows that the distribution curve of change in the OHIP-14 scores between baseline and 12 mo tended more toward lower scores (improved OHRQoL) for intervention participants than for controls, although the differences were relatively small.
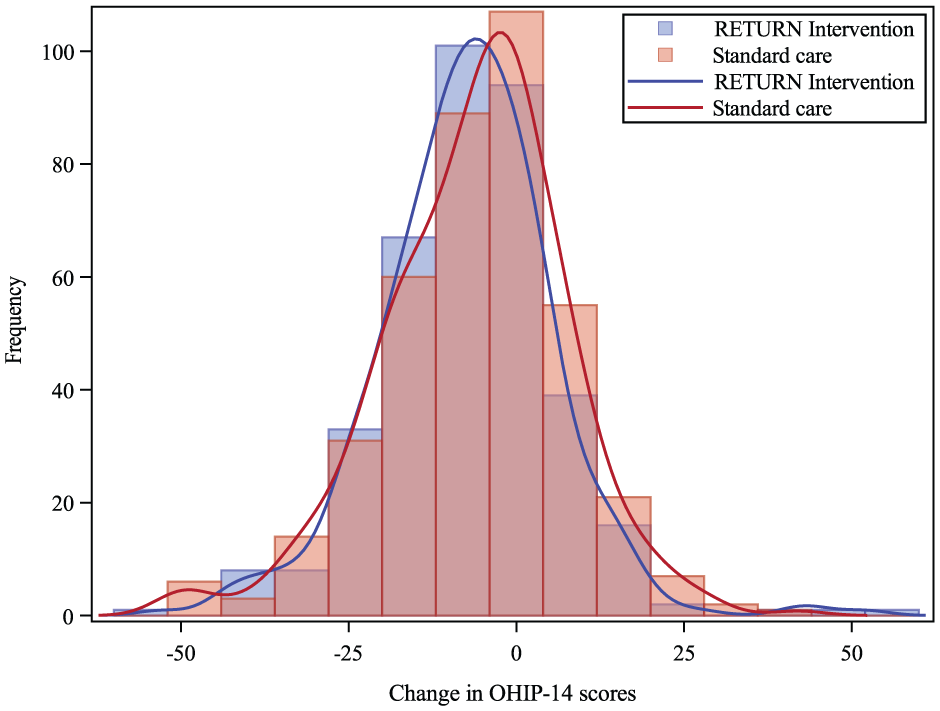
Histogram showing the change in Oral Health Impact Profile (OHIP)–14 scores.
The difference in OHIP-14 between intervention and control was greatest at 6 mo (mean = 16.5, SD = 14.0 intervention; mean = 17.7, SD = 14.8 control) and least at 18 mo (mean = 14.7, SD = 14.5 intervention; mean = 14.6, SD = 13.9 control). A repeated-measures mixed-effects model found the least squares mean was lower for intervention participants than for controls at each time point (better OHRQoL; Appendix Table 2). At 6 mo, the difference in least squares mean was −1.49 (CI = −2.92, −0.05), which was below the 2.25 minimum clinically important difference set in the PO2 sample size calculation. The least square means in both groups decreased, showing the OHRQoL in both groups improved over time and the difference between groups reduced. The time–treatment group interaction estimate of 0.01 (CI = −0.03, 0.04) was not statistically significant.
Other SOs
Dental anxiety scores at baseline were moderately high in both intervention and control groups (Table 1). Mean (SD) MDAS scores reduced over time in both groups at 6, 12, and 18 mo, respectively: intervention (13.4 [SD = 6.0]; 13.6 [SD = 6.2]; 13.0 [SD = 5.9]) and control (13.6 [SD = 6.0]; 13.5 [SD = 6.0]; 13.6 [SD = 6.2]). A repeated-measures mixed-effects model found the least squares mean was lower for RETURN at each time point (lower anxiety). At 18 mo, the difference in MDAS least squares means was −0.74 (CI = −1.39, −0.09), indicating a statistically significant, albeit small difference. The least squares mean for the intervention group decreased with time (anxiety improved), while it increased (anxiety worsened) in the control (Appendix Table 3). The time–treatment group interaction was statistically significant (−0.01; CI = −0.03, 0.00; P = 0.027).
The BSA payment data for bands of activity showed intervention participants had increased odds of receiving band 1 (checkup/prevention only, OR = 1.14, CI = 0.70, 1.86), band 2 (including fillings, extractions, etc, OR = 1.32, CI = 0.91, 1.92), and band 3 (including complex care, OR = 1.52, CI = 0.73, 3.20). The pattern was consistent at 6 and 12 mo and tended to increase with time, although this was not statistically significant (Appendix Table 4). When different data sources for treatment received were combined (BSA, LDH audit, and self-report [if reported in any source then recorded but not counted twice]), there were no statistically significant differences in the proportions of intervention versus control participants receiving different treatment types, at any time point.
Using combined data sources, intervention participants had a slightly reduced odds of receiving urgent dental care within 18 mo (OR = 0.86; CI = 0.68, 1.09) and a 20% lower odds of being prescribed antibiotics by a dentist at 6 mo (OR = 0.79; CI = 0.57, 1.09), increasing at 12 mo (OR = 0.89; CI = 0.67, 1.19) and 18 mo (OR = 0.95; CI = 0.73, 1.25), although no time point was statistically significant (Appendix Table 5). There was no significant difference by treatment group in the odds of self-reported antibiotic prescriptions by non-dental services (Appendix Table 6) or self-reported symptoms of infection at any time point (Appendix Table 7). Self-reported prescriptions of analgesics for dental problems tended to be slightly higher for the intervention group at each time point: at 18 mo 29.3% (n = 85) intervention versus 26.3% (n = 88) control (OR = 1.14; CI = 0.80, 1.64), but no time point was statistically significant (Appendix Table 8). Appendix Tables 9 to 11 contain additional analyses.
Discussion
Strengths and Limitations
While descriptive studies of barriers to dental care are numerous, intervention studies are few. This is the first large-scale trial anywhere in the world involving an intervention targeting dental visiting behavior for adults in general. Previous, much smaller-scale work has been limited to certain groups such as pregnant women (Riedy et al 2015), in which situational cues may be specific and influence how individuals respond (Papies 2016). While inclusion was not limited by socioeconomic status, more than half of trial participants lived in the lowest IMD decile areas. Follow-up was 6 monthly for 18 mo, and so the study not only investigates intervention effectiveness but also any maintenance of effect. The latter is especially important when considering intervention sustainability and its feasibility of adoption in the longer term.
While a strength of the study lies in this being a pragmatic trial delivered mainly in NHS dental practices, COVID-19 significantly affected this setting during the study period (O’Connor et al 2023). Service capacity shrank because of increased infection prevention control procedures, staff illness, and retention issues, with widespread media attention around this. Recovery of dental access remained at about 75% to 80% of pre-pandemic levels in mid-2022 (part-way through the follow-up period), with some areas especially affected (Joseph 2023). Access to appointments for new patients was monitored throughout by monthly telephone calls to all practices in the recruitment area. In September 2019, we identified 122 NHS practices accepting new patients, but this fell to <15 practices in July 2022. Between August 2022 and August 2023, this fell further to <5 practices, recovering slightly to <20 practices between September 2023 and the end of the trial. Interpretation of results should therefore take account of the difficulty of participants being successful in obtaining NHS dental care at that time. Taking account of local differences and temporal variation are common challenges when attempting to target health inequalities by addressing dental visiting behavior (Semprini 2024). Nevertheless, a trial design with long follow-up contributes valuable insights to understanding outcomes in contexts in which publicly funded service availability is limited.
Multiple primary outcomes are sometimes needed to assess treatment efficacy where no single variable is sufficient to reflect overall benefit (International Council for Harmonisation [ICH] 1998). Co-primary outcomes can “offset” each other; when taken together, they provide a fuller picture of efficacy (Pocock et al 1987). PO1 provided an objective, verifiable indicator of routine dental visiting immune from recall and social desirability bias, which can be a problem with self-reported data such as that from the OHIP-14 (Adams et al 2005). However, PO1 BSA data did not capture private, hospital, or other dental sector services. Moreover, the sample size for PO1 was reduced by 15% where trial records were unmatched with participant identifiers obtained on enrollment, although sensitivity analyses were undertaken which produced similar results and baseline characteristics of matched and unmatched participants were similar. In contrast, PO2 represents an outcome especially meaningful for patients and commissioners, and in the absence of outcomes measured by clinical examinations, it is important. Clinical outcomes (eg, decayed, missing, and filled teeth) were not feasible because follow-up visits to participants’ homes or to a dental service would have conflicted with trial design and confounded any intervention effect. While PO2 reflected the effects of, for example, private care, being reliant on self-report data made it more subject to attrition bias, which is a key downside. PO2 retention was lower (65% of participants included in the analysis at 12 mo) than planned in the power calculation, which assumed 80% retention at this point. Thus, PO2 nonsignificant findings should be interpreted with caution as the study may have been underpowered to detect modest effects. The ICH (1998) distinguishes POs (the most clinically relevant evidence of benefit) from SOs (outcomes that are supportive and help interpret and explain the main effect). Since POs were affected by limited-service availability, SOs became especially important in enabling a fuller understanding of intervention effectiveness: for example, the use of the private sector became more important as the availability of NHS services reduced, as did measuring the effect over time.
The latest advice is to summarize according to the level of certainty of evidence, rather than focusing on cutoff points for statistical significance (Amrhein et al 2019). Outcomes were consistently favorable to the intervention group, so taken as a whole, we are moderately certain of a small positive effect despite very limited service availability. This terminology is taken from the GRADE approach, which stipulates that while randomized controlled trials begin with a high certainty rating, they should be downgraded where important imprecision exists (Schünemann et al 2024). In line with GRADE guidance, imprecision was evaluated by comparing CIs with prespecified thresholds for a minimally important difference and by considering the optimal information size for each primary outcome. For PO2 (OHIP minimally important difference 2.25 points), the CI (−3.08 – 0.83) crossed the line of no effect and included the clinically important improvement without clinically important harms. For PO1, with OR = 1.21 and CI 0.86 to 1.70, the CI crossed the line of no effect, including effects consistent with the prespecified effect size. Accordingly, the certainty of evidence for both POs was downgraded by 1 level (moderate certainty) because of serious imprecision. The reduced effective sample size (through PO1 unmatched participants and PO2 attrition) was considered as supporting evidence for imprecision. The GRADE rating of moderate certainty of effect also indicates that further research may affect the confidence on the estimate of effect and may change the estimate. SOs were not used to determine certainty because of multiplicity, although they were directionally consistent.
The intervention also had an unambiguous effect on increasing attempts to obtain a routine appointment. Even though RETURN was a one-off, 15-min intervention, for most outcomes, differences between treatment groups increased over time, consistent with maintaining attempts to get care and a strong maintenance of intervention effect. Dental anxiety reduced over time for RETURN participants, whereas it tended to grow for the control group. It is also worth noting that findings reflect the behavior of those recruited and retained in a clinical trial, and wider implementation presents a slightly different context, since those compliant with trial procedures may have been more motivated to seek routine care, making differences between intervention and control harder to detect. That a relatively high proportion of control participants attempted to seek care despite their sociodemographic characteristics being typical of low users is perhaps indicative of this. So, the intervention effect may conceivably be stronger in “real-world” settings outside a trial context.
Policy Implications and Further Work
Trial findings indicating that routine visiting behavior is malleable, even in disadvantaged populations, has policy implications (see Appendix 1, discussion). In health systems where there is limited availability of a range of dental care for all, services prioritizing the stabilization of oral health, as a first step after urgent care, have been prioritized. This still requires return visits by urgent care users, so RETURN may have a role in supporting stabilization care uptake. However, evaluating its effect in this context and any economic benefits of reducing missed appointments and the revolving door of urgent care is needed. Further studies are also needed involving other populations (eg, diverse ethnicity) and health systems.
Conclusion
In this large, pragmatic trial, a brief, nurse-delivered behavioral intervention in urgent care consistently shifted behavior toward routine care with small, favorable differences in routine attendance, OHRQoL, and reduced dental anxiety over time. Taken together and adopting a certainty-of-evidence lens rather than a dichotomous focus on statistical significance, we judge the overall effect to be small and positive with moderate certainty. This was within a context of reduced effective sample size and very limited routine care availability. These findings support positioning behavioral support at the point of urgent care as a practical complement to, not a substitute for, structural reforms that address availability and affordability. Future research should test effectiveness and cost-effectiveness where routine services are more readily available and in other health systems and more diverse populations, as well as evaluate the effects on uptake and adherence to stabilization appointments to inform scalable implementation.
Author Contributions
R.V. Harris, led conception and design and contributed todata acquistion, data analysis and interpretation, and drafted the manuscript; V. Lowers, contributed to design, data acquisition, analysis, and interpretation, critically revised the manuscript; J. Green, led data analysis contributed to interpretation and critically revised the manuscript; R. Kirby, J. Hennessy, contributed to acquisition and interpretation and critically revised the manuscript; J.E. Clarkson, contributed to design, data interpretation and critically revised the manuscript; G. Burnside, contributed to design, data analysis and interpretation and critically revised the manuscript. All authors gave their final approval to this manuscript and agree to be accountable for all aspects of this work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261425929 – Supplemental material for RETURN Randomized Controlled Trial to Increase Adult Routine Dental Visits
Supplemental material, sj-docx-1-jdr-10.1177_00220345261425929 for RETURN Randomized Controlled Trial to Increase Adult Routine Dental Visits by R.V. Harris, V. Lowers, J. Green, R. Kirby, J. Hennessy, J.E. Clarkson and G. Burnside in Journal of Dental Research
Footnotes
Acknowledgements
We sincerely thank the patients who volunteered their time to participate in this trial. We are also grateful to the dental teams who delivered the intervention within their clinical and hospital settings, particularly the dental nurses whose dedication was crucial to its success. We acknowledge Professor Pauline Adair for her assistance in developing the training for dental teams, Professor Richard Cooke for his early contributions to the intervention design, and the patient and public advisors who helped shape participant-facing materials. Finally, we thank Michelle Girvan, Ashley Best, Emma Bedson, and other Liverpool Clinical Trials Centre staff for their support throughout the trial.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rebecca Harris is employed as a UK government advisor on NHS dentistry. Other authors have no conflicts of interests to report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project is funded by the National Institute for Health Research (NIHR) (PGfAR project reference RP-PG-0616-20004). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. All authors gave their final approval and agree to be accountable for all aspects of the work.
Data Availability Statement
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.