
Abstract
Timely dental care is essential for children’s health and development, yet disparities persist, particularly among immigrants and children of immigrants. This study examined how children’s and their parents’ immigration status affects dental care utilization, considering social capital and material hardship as mediators. Using 8 waves of the National Survey of Children’s Health from 2016 through 2023, we analyzed a nationally representative, pooled, cross-sectional survey sample of 274,302 children in the United States aged 2 to 17 y. Latent variables for social capital, material hardship, and socioeconomic status (SES) were constructed from factor analysis of observable indicators. Multivariable structural equation models simultaneously included child and parental immigration status as exposures to assess pathways linking immigration to dental attendance and receipt of preventive dental care. We compared models with mediation versus confounding by SES. Results indicate that social capital is a primary pathway through which immigration status reduces dental attendance. Social capital mediated the effect of being a foreign-born child in both the mediation-by-SES and confounding-by-SES models (odds ratio [OR], 0.74; 95% confidence intervals [CI], 0.64–0.86). Similarly, social capital mediated the effect of having foreign-born parents in both models (OR, 0.59; 95% CI, 0.46–0.76). Comparing the pathways of the 2 exposures revealed heterogeneity: direct effects (i.e., those not mediated by social capital or material hardship) were stronger than mediated effects for the child’s immigrant status, whereas mediated effects were stronger for parental immigrant status. Our findings remained consistent when assessing receipt of preventive care as an outcome and also when carrying out sensitivity analyses comparing the pre- and post-COVID-19 periods. These results highlight social capital as a potential target for future research into reducing dental care disparities among immigrant children. Improving social networks, community engagement, and access to supportive resources may potentially be a viable way to promote equitable utilization of dental care.
Keywords
Introduction
Dental caries is the most common chronic disease affecting children and adults in the United States (National Institute of Dental and Craniofacial Research 2022). Major dental and public health associations advocate that children visit a dentist within the first year of life, with the American Academy of Pediatric Dentistry maintaining that early dental visits form the best strategy for reducing rates of disease (Pediatric Oral Health Research and Policy Center, American Academy of Pediatric Dentistry 2014). Early preventive dental visits are associated with greater use of subsequent preventive services, lower prevalence of dental caries, and reduced expenditure (Savage et al 2004; Qu et al 2022). Disparities in the utilization of dental care, which represents the receipt of dental care services, remain a significant public health concern in the United States (Zhang et al 2019; Northridge et al 2020). This is particularly true for immigrant populations, with data from the Medical Expenditure Panel Survey indicating that US-born adults are more likely to have visited a dentist than noncitizens or naturalized citizens (Wilson et al 2016). Patterns among children are more complex; compared to US-born children with US-born parents, those born in the United States to immigrant parents are more likely to have received preventive dental care, whereas children born outside the United States are less likely (Okunseri et al 2021). Moreover, immigrant children experience higher rates of dental caries (Luo et al 2024).
Several factors have been identified as facilitators of dental service utilization among immigrant populations, including perceived oral health needs, education, and income (Wu et al 2005; Mao et al 2023). Social capital, encompassing neighborhood cohesion and trust, social networks, and social support, is another key determinant of health behavior and has been linked with increased use of preventive services (Nieminen et al 2013; Peng and Lin 2018; Knorst et al 2022b). In the context of pediatric oral health, higher social capital is associated with improved dental outcomes, and dental service utilization is posited as a mediator of this relationship (Knorst et al 2022a, 2022b). Conversely, material hardship, reflecting economic and resource constraints such as difficulty paying household bills or experiencing food insecurity, may hinder access to dental care (Rodems and Shaefer 2020). Indeed, cost remains the most frequently cited barrier to dental service use, with financial barriers representing a more pervasive obstacle than for any other type of health care (Vujicic et al 2016).
This study explores how social capital, material hardship, and socioeconomic factors influence utilization of dental care among children in the United States to better understand how oral health disparities arise in immigrant populations.
Materials and Methods
Data Source
We extracted data from the National Survey of Children’s Health (NSCH) studies, which are conducted by the US Census Bureau. These are multistage cross-sectional surveys that take a weighted sample representative of noninstitutionalized children in the US population. They are the largest national surveys on the health and health needs of children aged 0 through 17 y. The methodology involves sampling households, sampling children within households, and then selecting respondents who are parents or guardians of the sampled child. Respondents complete web-based or self-administered questionnaires, and response rates ranged from 35.8% (2023) to 43.1% (2018). We pooled data across 8 annual survey waves, NSCH 2016 through 2023, including all participants aged 2 y and older.
Outcomes
We evaluated 2 binary outcomes:
Measures
The population characteristics were as follows: age (2 to 5 y, 6 to 11 y, 12 to 17 y); sex (boys or girls); race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic Asian, other); household education according to the highest level of education reported among the primary caregiver adults (below, at, and above high school); household income/poverty ratio, defined as the ratio between household income and the federal poverty threshold (i.e., a value <100% indicates that a family is living in poverty; <100%, 100% to <250%, ≥250%); and 2-parent household (yes or no) according to whether the child lived with 2 primary caregivers who were biological/adoptive parents or step-parents. Children were defined as foreign-born if their place of birth was abroad and as having foreign-born parent(s) if at least 1 biological/adoptive parent was born abroad. When referring to the specific exposure of interest in this study, we use the term foreign-born, and when generally discussing groups of people who were born abroad, we use the term immigrants.
Material hardship was measured by 4 binary variables, according to whether 1) the household had ever found it hard to cover basics such as food or housing since the child was born and whether, in the past 12 mo, they 2) had received cash assistance from the government, 3) had received food stamps or supplemental nutrition assistance program benefits, or 4) had received free or reduced-cost meals at school.
Social capital, defined as the “features of social organization such as networks, norms, and social trust that facilitate coordination and cooperation for mutual benefit,” cannot be directly quantified but is inferred from indicators or proxies (Putnam 1995; Knorst et al 2022b). Typically, these are measures of social support, social networks, and community trust (Tang 2015; Knorst et al 2022a, 2022b; Chan et al 2025). In the present study, social capital was measured by 5 binary variables that act as proxies for previously established metrics (Appendix Table 1): 1) whether the respondent adult felt that people in the neighborhood helped each other out, 2) whether they felt that people in the neighborhood watch out for one another’s children, 3) whether they felt the child was safe in the neighborhood, 4) whether they had someone to turn to for emotional support, and 5) language acculturation, which was measured by whether the primary household language is English. Language acculturation is included for its pivotal role in the formation of social ties and community support in immigrant populations (Valdez et al 2013).
Statistical Analysis
We computed summary statistics for the analytic sample, followed by bivariate tests of the association between the exposures and participant characteristics. We then used structural equation models (SEMs) to explore pathways mediating immigration and utilization of dental care (Fig. 1). First, key indicator variables were combined into underlying constructs—material hardship, social support, and socioeconomic status (SES). We then assessed how these factors mediated the relationship between immigration status and dental visits or preventive care, while also accounting for other direct pathways not captured by these constructs. All models simultaneously included child and parental place of birth as exposures, while adjusting for age, sex, race and ethnicity, and survey year. Regression coefficients were converted to odds ratios (ORs) with 95% confidence intervals (CIs), to give a familiar measure of effect size, and model fit was evaluated using standard criteria. Given the large number of estimates, ORs are reported in full in the tables and summarized in the Results in terms of percentage changes in odds. For example, an OR of 0.70 corresponds to a 30% reduction in odds, while an OR of 1.50 corresponds to a 50% increase in odds, conveying the same information in a more interpretable format. The US Census Bureau imputed missing data on sociodemographics and income, and we fitted the models by pooling across multiple imputations. All analyses were adjusted for the sampling weights.
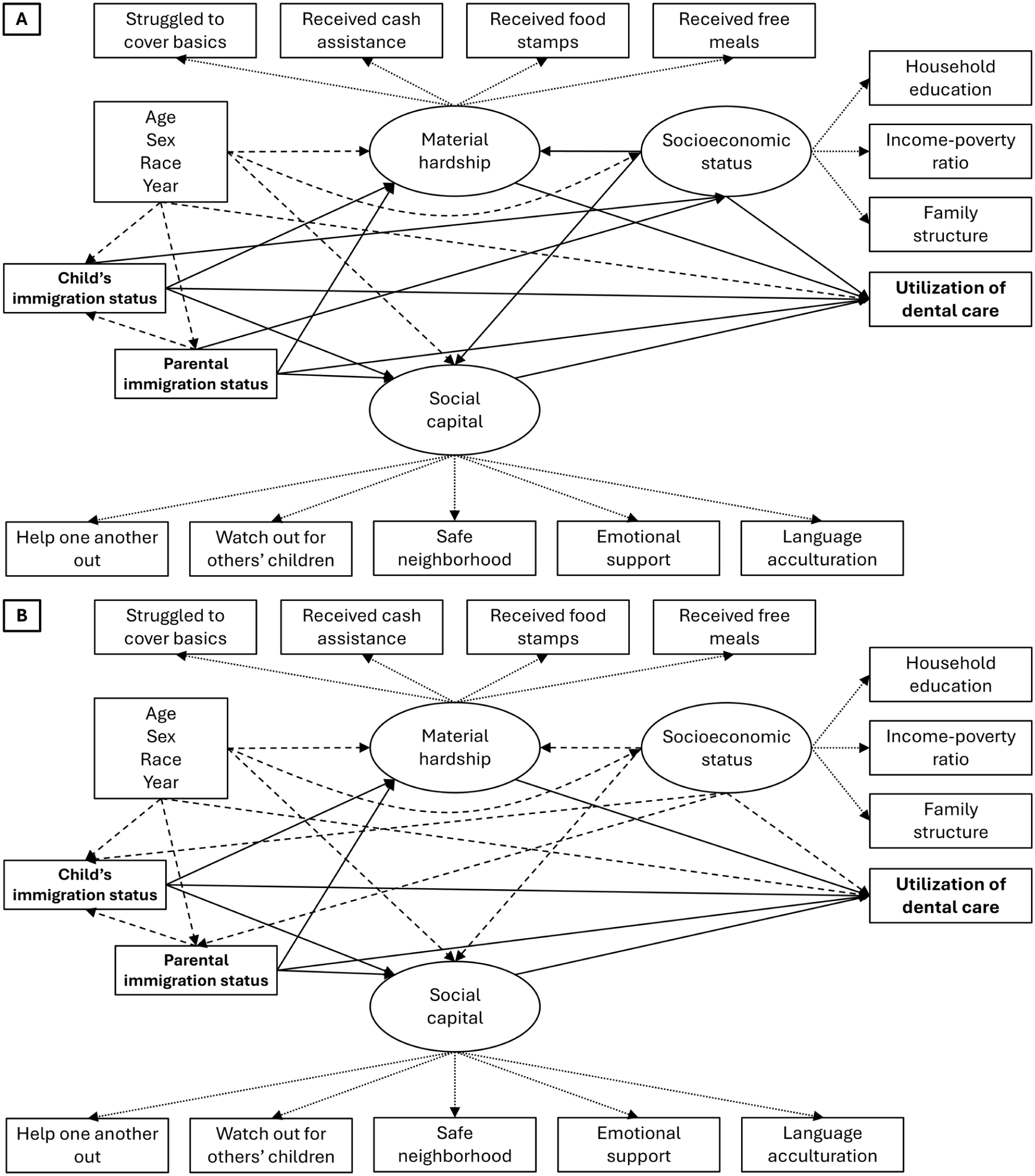
Directed acyclic graph for the conceptual framework linking child and parental immigration status with utilization of dental care. Rectangles represent observed variables, and ovals represent latent variables. Dotted arrows (⤑) represent pathways between latent variables to the indicators used in the measurement models. Dashed arrows (⇢) represent confounding pathways that were controlled for in analyses. Solid arrows (→) represent direct and mediating pathways of interest. (
We repeated the above twice: once for an SEM, in which socioeconomic status (SES) was treated as a mediator (Fig. 1A), and once in which it was treated as a confounder (Fig. 1B). Technical details of the modeling approach are presented in the Appendix Methods. We carried out sensitivity analyses, modeling the 2016 to 2019 datasets versus the 2020 to 2023 datasets separately, to evaluate effect modification by pre- versus post-COVID-19 periods. We reported the study according to Strengthening the Reporting of Observational Studies in Epidemiology guidelines (von Elm et al 2008).
Results
The characteristics of the participants are presented in Table 1, and a flowchart summarizing the selection procedure is presented in Figure 2. The study sample comprised 274,302 children, of whom 9,118 (4.6%) were foreign-born and 51,154 had foreign-born parent(s) (28.0%). Children who are foreign-born and children with foreign-born parent(s) are more likely to be older; of an ethnic minority; from a lower education household; from a poorer household; from a household that has received cash assistance, food stamps, or free or reduced-cost meals; from a household experiencing all indicators of lower social capital; not have visited the dentist in the past 12 mo; and not have received preventive dental care in the past 12 mo. Conversely, they were less likely to be from a household that had ever struggled to cover basics. Children with foreign-born parent(s) were also more likely to come from a 2-parent household. The factor loadings for the latent variables of material hardship, social capital, and SES are presented in Appendix Table 2. The observed variables are reliable indicators of these latent variables, supporting their construct validity. All SEMs exhibited good fit, with no rejection of the null hypothesis of close fit.
Characteristics of the Included Participants from the National Survey of Children’s Health, 2016 to 2023 (N = 274,302).
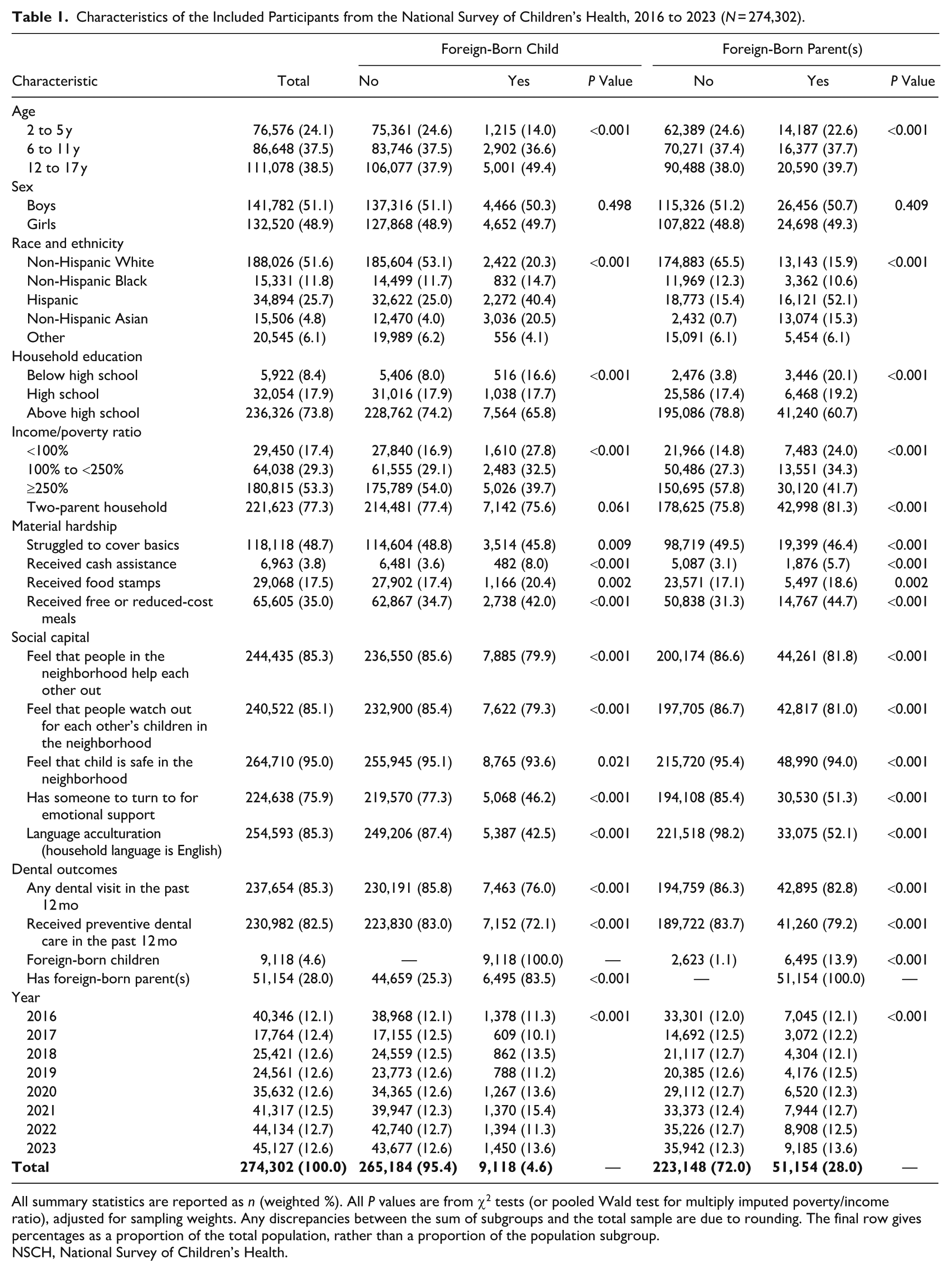
All summary statistics are reported as n (weighted %). All P values are from χ2 tests (or pooled Wald test for multiply imputed poverty/income ratio), adjusted for sampling weights. Any discrepancies between the sum of subgroups and the total sample are due to rounding. The final row gives percentages as a proportion of the total population, rather than a proportion of the population subgroup.
NSCH, National Survey of Children’s Health.
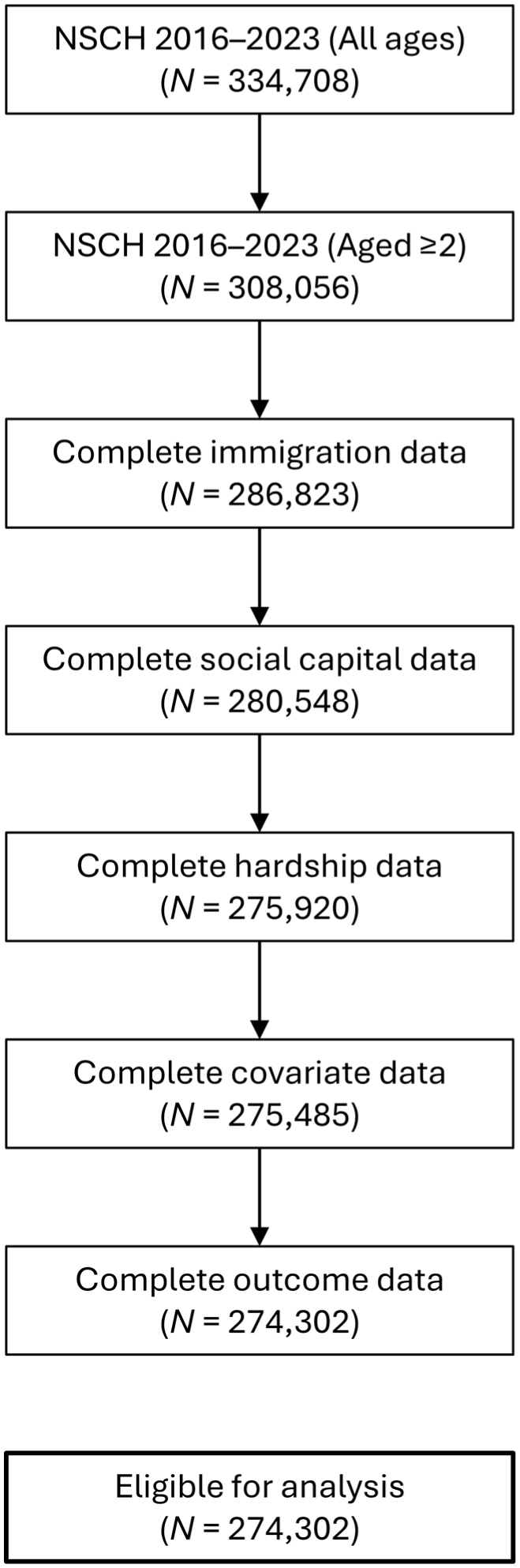
Participant selection flowchart showing selection for children in the National Survey of Children’s Health 2016 to 2023 datasets. Illustrates the steps leading to the number of participants retained for each set of variables, leading to the final analytic sample of children aged 2 through 17 y.
Outcome: Any Dental Visits
Mediating models
Results from the SEMs, which assumed SES to be a mediator, are presented in Table 2.
Results from the Structural Equation Models Where Socioeconomic Status Is Modeled as a Mediator, from the National Survey of Children’s Health, 2016 to 2023 (N = 274,302).
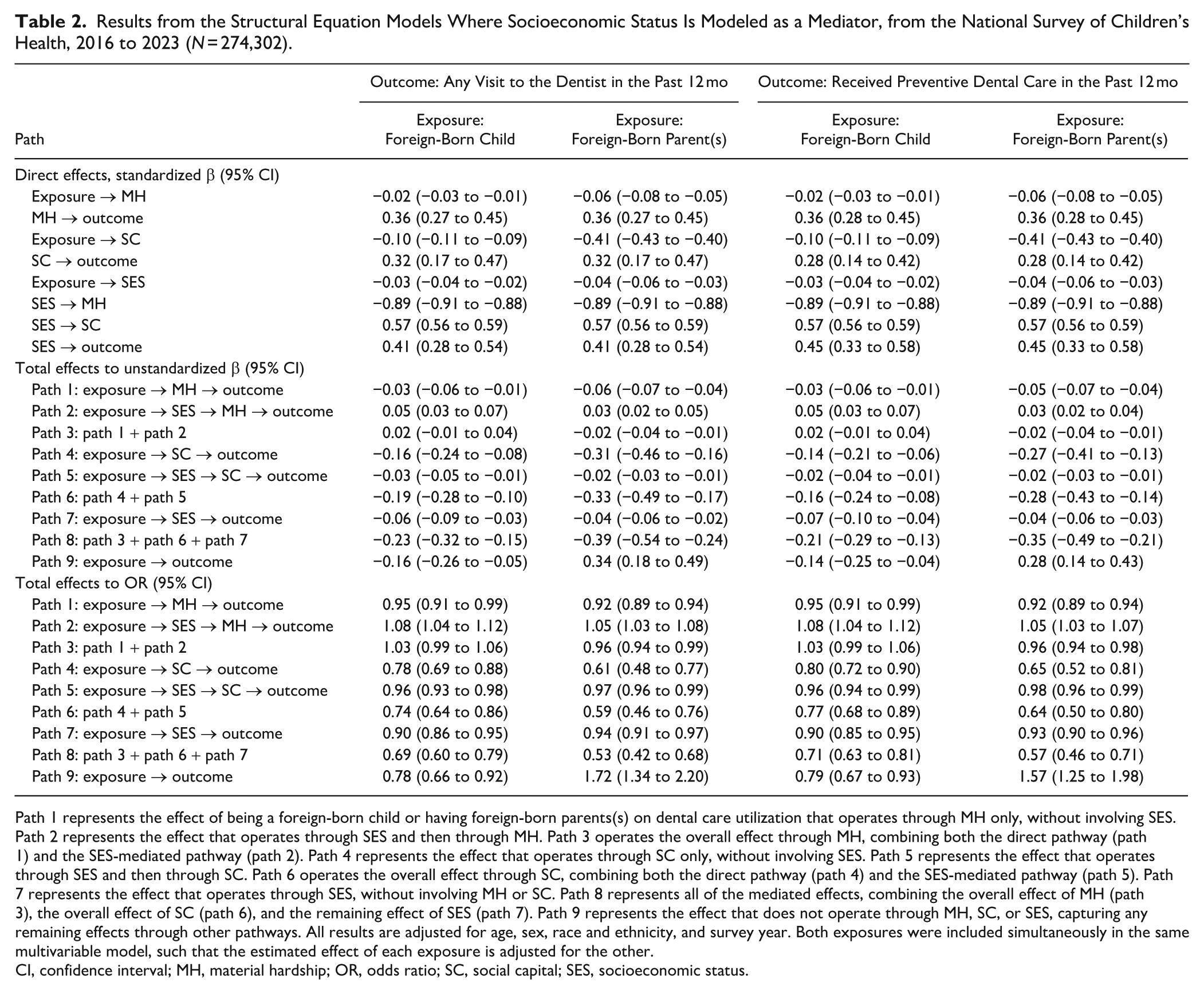
Path 1 represents the effect of being a foreign-born child or having foreign-born parents(s) on dental care utilization that operates through MH only, without involving SES. Path 2 represents the effect that operates through SES and then through MH. Path 3 operates the overall effect through MH, combining both the direct pathway (path 1) and the SES-mediated pathway (path 2). Path 4 represents the effect that operates through SC only, without involving SES. Path 5 represents the effect that operates through SES and then through SC. Path 6 operates the overall effect through SC, combining both the direct pathway (path 4) and the SES-mediated pathway (path 5). Path 7 represents the effect that operates through SES, without involving MH or SC. Path 8 represents all of the mediated effects, combining the overall effect of MH (path 3), the overall effect of SC (path 6), and the remaining effect of SES (path 7). Path 9 represents the effect that does not operate through MH, SC, or SES, capturing any remaining effects through other pathways. All results are adjusted for age, sex, race and ethnicity, and survey year. Both exposures were included simultaneously in the same multivariable model, such that the estimated effect of each exposure is adjusted for the other.
CI, confidence interval; MH, material hardship; OR, odds ratio; SC, social capital; SES, socioeconomic status.
Being foreign-born had a negligible effect on dental visits through the material hardship pathway (path 3) but a 26% reduction in odds of visiting the dentist through the social capital pathway (path 6). Even after accounting for material hardship and social capital, being a foreign-born child reduced the odds of dental visits by a further 10% through the direct effect of SES (path 7). Therefore, the total mediated effect of being a foreign-born child was a 31% reduction in the odds of visiting the dentist (path 8). The remaining pathway captured effects that were not mediated by material hardship, social capital, or SES, and this pathway comprised a further 22% reduction in the odds of visiting the dentist (path 9).
Having foreign-born parent(s) had a small effect on dental visits through the material hardship pathway (path 3) but a 41% reduction in odds of visiting the dentist through the social capital pathway (path 6). Even after accounting for material hardship and social capital, having foreign-born parents(s) reduced the odds of dental visits by a further 6% through the direct effect of SES (path 7). Therefore, the total mediated effect of being a foreign-born child was a 47% reduction in the odds of visiting the dentist (path 8). The remaining pathway captured the effect that was not mediated by material hardship, social capital, or SES, and this pathway comprised a further 72% increase in the odds of visiting the dentist (path 9).
Confounding models
Results from the SEMs that assumed SES to be a confounder are presented in Table 3.
Results from the Structural Equation Models Where Socioeconomic Status Is Modeled as a Confounder, from the National Survey of Children’s Health, 2016 to 2023 (N = 274,302).
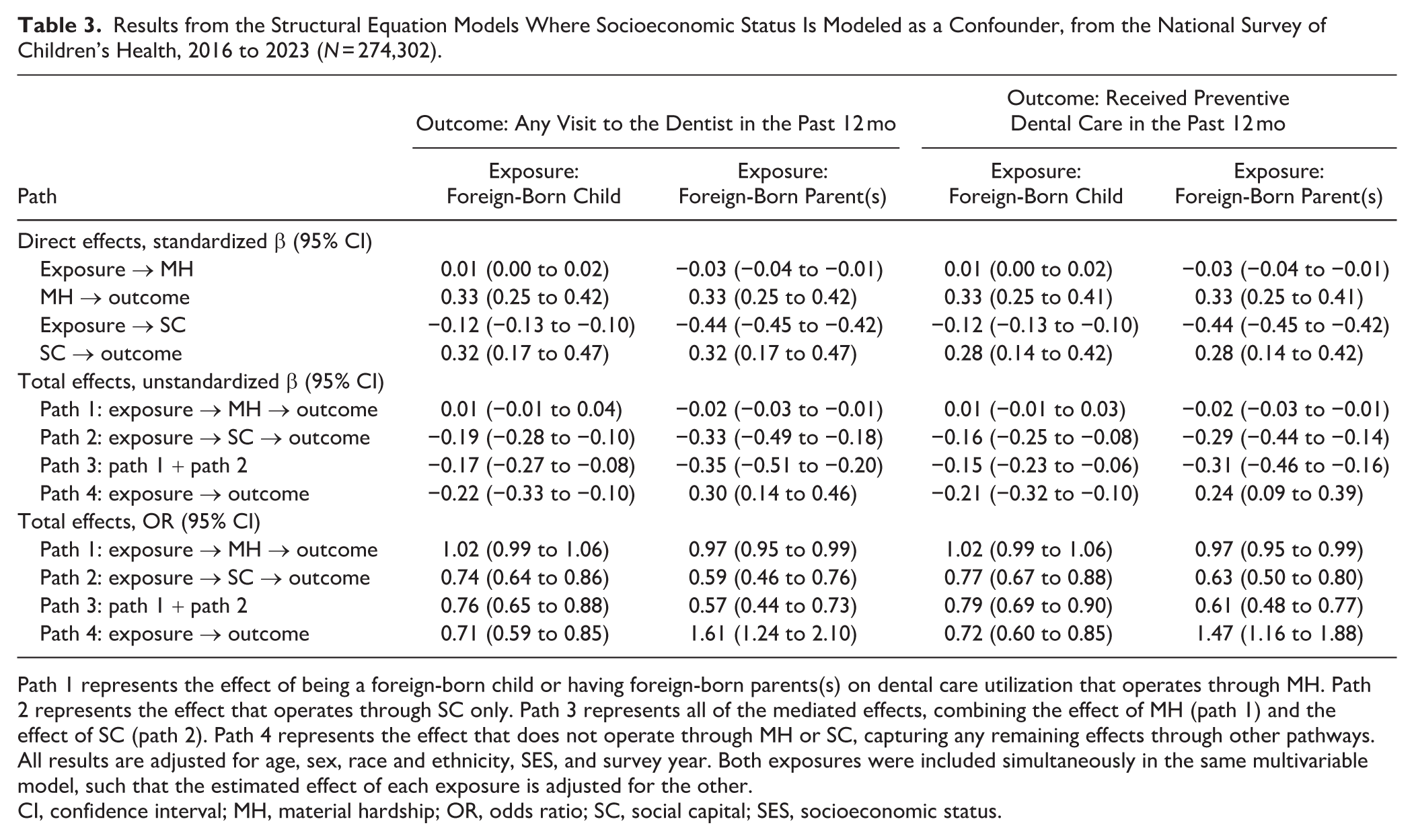
Path 1 represents the effect of being a foreign-born child or having foreign-born parents(s) on dental care utilization that operates through MH. Path 2 represents the effect that operates through SC only. Path 3 represents all of the mediated effects, combining the effect of MH (path 1) and the effect of SC (path 2). Path 4 represents the effect that does not operate through MH or SC, capturing any remaining effects through other pathways. All results are adjusted for age, sex, race and ethnicity, SES, and survey year. Both exposures were included simultaneously in the same multivariable model, such that the estimated effect of each exposure is adjusted for the other.
CI, confidence interval; MH, material hardship; OR, odds ratio; SC, social capital; SES, socioeconomic status.
Being foreign-born had a negligible effect on dental visits through the material hardship pathway (path 1) but a 26% reduction in odds of visiting the dentist through the social capital pathway (path 2). Therefore, the total mediated effect of being a foreign-born child was a 24% reduction in the odds of visiting the dentist (path 3). The remaining pathway captured effects that were not mediated by material hardship or social capital, and this pathway comprised a further 29% reduction in the odds of visiting the dentist (path 4).
Having foreign-born parent(s) had a small effect on dental visits through the material hardship pathway (path 1) but a 41% reduction in odds of visiting the dentist through the social capital pathway (path 2). Therefore, the total mediated effect of foreign-born parent(s) was a 43% reduction in the odds of visiting the dentist (path 3). The remaining pathway captured the effect that was not mediated by material hardship, social capital, or SES, and this pathway comprised a further 61% increase in the odds of visiting the dentist (path 4).
Outcome: Receipt of Preventive Care
There were small quantitative differences, but the qualitative conclusions were unchanged when analyzing receipt of preventive care as the outcome.
Sensitivity Analyses
The magnitude of effects tended to be slightly greater in the pre-COVID-19 period (Appendix Tables 3–6), but the overall qualitative interpretation of the results remained unchanged.
Discussion
In this study, we used SEMs to explore the mediating pathways between child and parental immigration status, as well as utilization of dental care. We found that these associations were largely mediated by social capital and, to a lesser extent, by material hardship. Furthermore, the direct pathway (path 9) indicates that being a foreign-born child has additional negative influences on utilization of dental care, while having foreign-born parent(s) positively influenced utilization of dental care, indicating that factors beyond material hardship, social capital, and SES may protect or facilitate dental attendance in this group. For example, their higher engagement with dental services may be linked to the well-established “healthy immigrant” phenomenon, which posits that immigrants tend to be healthier and more health-conscious upon arrival due to selection biases (Hamilton 2015; Elshahat et al 2022). Additionally, families with foreign-born parents who have resided longer in the United States may have had more opportunity to adapt to and navigate the health care system. Previous studies have similarly noted a greater receipt of preventive dental care in US-born children of immigrant families (Yun et al 2014; Okunseri et al 2021).
Our analyses indicate a positive direct effect of material hardship on utilization of dental care; while this may initially appear counterintuitive, there is a coherent explanation. Individuals experiencing material hardship are known to have higher prevalence of oral disease—a recent systematic review revealed a higher prevalence of dental caries among children and adolescents experiencing food insecurity (Sabbagh et al 2023). However, they also disproportionately belong to lower socioeconomic groups, where limited income and lower educational attainment act as major barriers to dental attendance (Provart and Carmichael 1995; Östberg et al 2017). In the present study, we have controlled for SES, so the residual association likely reflects the greater clinical need for dental care among individuals experiencing hardship, which may prompt more frequent attendance when socioeconomic differences are controlled for. Programs alleviating financial strain may further facilitate this utilization. For example, it has been shown that participation in the Supplemental Nutrition Assistance Program reduces the likelihood of not being able to afford dental care (Miller and Morrissey 2021).
Our findings are consistent with the literature that documents disparities in the utilization of oral health care among immigrant populations, particularly children (Okunseri et al 2021; Luo et al 2024). We extend these findings by quantifying the role of mediating pathways within a robust statistical framework. Through this, we confirm that social capital is a particularly strong mediator. Living in a safe neighborhood and being part of a community that offers reciprocal support fosters trust and cooperation. These social bonds can provide encouragement and practical assistance in seeking dental services and engaging in health-promoting behaviors (Chan et al 2024). Evidence suggests that social networks and practical or emotional support from family and friends are associated with increased use of dental care in immigrants (Dahlan et al 2019). Among Mexican immigrants in the United States, more frequent discussion of dental problems within social networks has been linked with higher utilization, possibly through information sharing about where and how to access care (Pullen et al 2018).
Our definition of social capital is innovative as it explicitly includes a measure of language acculturation. Language proficiency has been shown to play a crucial role in developing social connections and accessing resources among immigrant populations (Twersky et al 2024). Trust, mutual expectations, and shared values are closely intertwined with language; parents who are proficient in the dominant language of the culture often feel more supported and find it easier to communicate their children’s needs (Valdez et al 2013). In the context of dental care, language acculturation can enhance communication with health care providers, improve understanding of available services, and reduce misunderstandings that may prevent dental attendance. Previous systematic reviews have found a positive association between acculturation, which includes language competency or preference, and the utilization of dental services (Gao and McGrath 2011).
The contrasting directions of the direct effects for foreign-born children versus those with foreign-born parents highlight the heterogeneity of effects that are likely at play within immigrant populations and support findings that generational differences influence health service utilization (Calvo and Hawkins 2015; Evensen et al 2024). Child and parental immigration may operate through distinct social, cultural, and resource-related pathways. We conjecture that parental immigration potentially reflects accumulated familiarity with the health care system, as well as greater cultural acceptance and prioritization of dental care, while child immigration may capture more immediate barriers or adaptation challenges.
The strengths of this study lie in its large sample size, robust sampling design, and rigorous statistical methodology. However, limitations also should be noted. First, the measures used in this study are from questionnaire-based data, which could result in recall bias, as well as the possibility of differential response rates to the survey. Second, as with all epidemiological studies, our findings are susceptible to residual confounding, model misspecification, and measurement error. This includes the fact that the definition of immigration status was based solely on birthplace, and other unmeasured factors, such as duration of residence in the United States, severity of disease, and occurrence of pain, may also be important to account for. In addition, our SEMs included the placement of language acculturation within social capital, but there may be other theoretically justified model specifications; this is inherently subjective, and different decisions about the positioning of variables could yield different estimates. By incorporating sampling weights, our point estimates are generalizable to the US population, but variance estimates may not be, as it is computationally intractable to also account for the strata and sampling units in such models. In addition, it is unclear how our results generalize to time periods outside 2016 to 2023, non-US populations, and nonpediatric populations.
Future research may focus on developing policies that not only improve material resources but also enhance neighborhood support, trust, and social networks, as these may be a viable pathway to reduce disparities in dental care utilization. However, the persistence of a negative direct effect of being a foreign-born child suggests that this exposure may reflect additional barriers, potentially stemming from immigration policies, limited familiarity with the US health care system, or ineligibility for dental insurance coverage. Conversely, the positive direct effect of having foreign-born parents suggests that protective cultural or familial factors may offset some structural disadvantages, warranting further investigation. It is also important to note that these additional direct pathways had effect sizes that were comparable in size or larger than the mediated pathways. This indicates that they may be of even greater importance than social capital or material hardship.
Conclusion
Social capital, as measured by social support, neighborhood cohesion and trust, and language acculturation, appears to be a key mediator linking immigration to utilization of dental care among children. The contrasting effects observed between children and their parents’ immigration status suggest that pathways beyond material hardship and social capital likely influence dental service use, in quite distinct manners. Addressing inequities may require multifaceted strategies that not only improve economic resources but also strengthen social networks and support systems.
Author Contributions
N.Z. Bashir, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; C.C.K. Chan, C. McGrath, contributed to conception and design, data interpretation, drafted and critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261416826 – Supplemental material for Pathways Mediating Immigration and Utilization of Dental Care in Children
Supplemental material, sj-docx-1-jdr-10.1177_00220345261416826 for Pathways Mediating Immigration and Utilization of Dental Care in Children by N.Z. Bashir, C.C.K. Chan and C. McGrath in Journal of Dental Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: N.Z.B. is supported by the Wellcome Trust (322777/Z/24/Z). N.Z.B. is a member of the Medical Research Council Biostatistics Unit (MC_UU_00040/01).
A supplemental appendix to this article is available online.