
Abstract
Associations between tooth loss and frailty have been reported, but longitudinal evidence on directionality and pathways of this association is lacking. We examined the direction and pathways of the association between edentulousness and frailty among older adults in England using a nationally representative sample of 6,800 adults aged ≥50 y who participated in the English Longitudinal Study of Ageing (ELSA) at wave 3. Edentulousness and frailty (determined using the Frailty Index) were assessed at waves 3 (2006/7), 5 (2010/11), and 7 (2014/15). The following mediators were assessed at waves 4 (2008/9) and 6 (2012/13): loneliness (UCLA Loneliness Scale), C-reactive protein (CRP), and consumption of fruit and vegetables. A cross-lagged longitudinal structural equation model with a Bayesian estimator using probit regression assessed the direction and pathways of the association between edentulousness and frailty at 2 time points (i.e., wave 3 to wave 5 and wave 5 to wave 7), after adjusting for sociodemographic factors and smoking. Being edentate at wave 3 was associated with an increased probability of frailty at wave 5, but the path was not significant between waves 5 and 7 (probit regression coefficient 0.05; 95% CI, −0.02 to 0.13). The paths from frailty to edentulousness were not significant at either time point (probit regression coefficients 0.09 [95% CI, −0.10 to 0.279] and 0.14 [95% CI, −0.03 to 0.31] for waves 3-5 and waves 5-7, respectively). The estimates of indirect paths via loneliness and CRP were of small magnitude but significant at both time points. No significant mediation was observed via the consumption of fruit and vegetables. Health promotion strategies aimed at preserving natural teeth and tackling loneliness in older people may have the potential to prevent frailty.
Keywords
Introduction
Societies worldwide are experiencing a rapid trend toward aging populations (WHO 2024a). A major public health concern related to population aging is frailty, described as a state of vulnerability to unfavorable health outcomes, such as falls, incident disability, hospitalization, and mortality (Clegg et al 2013). Poor oral health, including loss of natural teeth, is associated with an increased risk of incident frailty in older adults (Hakeem et al 2019; Huang et al 2025). The association between oral health and frailty is potentially bidirectional. Poor oral health might increase the risk of incident frailty, while frailty may also affect oral health status (Hakeem et al 2019), as physical impairment and reduced mobility may lead to lower dental service use (Janssens et al 2023) and lower ability to perform sufficient oral self-care (MacEntee et al 2010). However, bidirectional associations between oral health and frailty remain underexplored.
In terms of pathways, there is some cross-sectional evidence that the association between tooth loss and frailty may be mediated by nutrition (Hakeem et al 2020, 2021; Xia et al 2024). A nutritional pathway is plausible given that edentulous individuals or those without a functional dentition have an increased risk of malnutrition (Zelig et al 2022), an established risk factor for frailty (Lorenzo-López et al 2017). However, relevant evidence from longitudinal studies supporting a nutritional pathway is scarce (Xu et al 2023).
Second, it has been suggested that negative social consequences of poor oral health may link oral health and frailty (Hakeem et al 2019). Associations between tooth loss and loneliness, a risk factor for frailty (Kojima et al 2022), have been documented in several cross-sectional studies (Olofsson et al 2018; Singh et al 2020; Koyama et al 2021). However, to our knowledge, evidence for this mediating pathway from longitudinal data is absent.
Third, edentulousness (Kotronia et al 2020) has also been associated with higher levels of C-reactive protein (CRP) in older adults, and chronic systemic inflammation is a risk factor of frailty (Clegg et al 2013). All in all, potential nutritional, psychosocial, and inflammation pathways linking poor oral health and frailty have been proposed (Hakeem et al 2019), but empirical evidence from relevant longitudinal studies is lacking.
Therefore, this study aimed to assess the potential bidirectionality in the longitudinal association between edentulousness and frailty in a national sample of older adults in England, hypothesizing that associations exist in both directions. In addition, mediating pathways via nutrition, loneliness, and inflammation that may link edentulousness to frailty were explored.
Materials and Methods
This is a secondary analysis from the English Longitudinal Study of Ageing (ELSA). Wave 3 (2006/7) was used as baseline data, since this was when oral health was first assessed in ELSA with follow-up data up to wave 7 (2014/15). The analytical sample consisted of 1) wave 3 core members, 2) not residing at an institution, and 3) eligible to provide blood samples. This study was reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines (Appendix Table 1).
The English Longitudinal Study of Ageing
ELSA is a nationally representative cohort study of community-dwelling English adults aged 50 y and older (Steptoe et al 2013). The initial study sample was drawn from households that participated in the Health Survey for England (HSE) between 1998 and 2001. All age-eligible people in the household who responded to HSE and also conducted an ELSA interview became ELSA “core members”. Baseline ELSA data (wave 1) were collected from 2002 to 2003. The ELSA cohort has been followed biannually through face-to-face computer-assisted personal interviews and self-completion questionnaires, with additional nurse visits, including blood sample collection, conducted every 4 y. In ELSA, participants with clotting or bleeding disorders, a history of fits or convulsions, or taking anticoagulant medicine were not eligible for blood sample collection. Ethical approval for the ELSA was granted by the London Multi-Centre Research Ethics Committee, and all individuals provided written informed consent. Further details on data and sampling are available at http://www.elsa-project.ac.uk/.
Edentulousness and Frailty Index
Edentulousness was self-reported and differentiated between dentate (having at least 1 natural tooth) and edentate (having no natural teeth) participants.
A dichotomous (frail vs. nonfrail) Frailty Index variable in line with criteria proposed by Rockwood and colleagues (Searle et al 2008) was constructed following the protocol previously used in ELSA (Rogers et al 2017). Respondents were considered frail if their Frailty Index score was greater than 0.25. Variables used to create the Frailty Index are displayed in Appendix Table 2.
Covariates
Potential covariates were selected based on the literature and measured at baseline: age (in years), sex (male vs. female), cohabitation status (married or cohabiting vs. neither married nor cohabiting), wealth (quintiles of total nonpension wealth, a composite measure of financial wealth, physical wealth including land, business worth, and jewelry, as well as housing wealth), education (degree or equivalent, secondary qualification, or no qualifications), and current cigarette smoking (yes/no).
Potential Mediating Variables
To assess nutrition, a binary variable (yes/no) was derived indicating reported consumption of at least 5 fruit and vegetable servings in the past day. This threshold has been linked to a lower risk of incident frailty in older adults (Kojima et al 2020). Further details on the construction of the nutrition variable are presented in the Appendix section 1.1, Appendix Figure 1, and Appendix Table 3.
Loneliness was assessed through the 3-item short form of the Revised UCLA loneliness scale (Hughes et al 2004), which is a validated measure of loneliness in ELSA (Office for National Statistics 2018). Each of the 3 questions (i.e., How often do you feel you lack companionship? How often do you feel left out? How often do you feel isolated from others?) included 3 potential answers: “Hardly ever or never,” “Some of the time,” and “Often.” Answers were summed up to create a loneliness score ranging from 3 to 9. A dichotomous variable (“not lonely” vs. “lonely”) was created, classifying individuals scoring 3 to 5 as “not lonely” and individuals scoring ≥6 as “lonely” (Rouxel et al 2017).
Inflammation was assessed by high-sensitivity serum CRP (mg/L) using the N Latex CRP mono Immunoassay on the Behring Nephelometer II Analyzer (Dade Behring). It was measured from blood samples of nurse visits at waves 4 and 6 (ranging from 0.2 to 190 mg/L at wave 4 and from 0.1 to 392.7 mg/L at wave 6). CRP was used as a continuous variable, and participants with CRP >10 mg/L were excluded, as higher CRP values may indicate acute inflammation and present infection rather than chronic inflammation (Lassale et al 2019).
Data Analysis
The analytical study sample was based on data from waves 3 to 7 of ELSA. Edentulousness and frailty variables were available at waves 3, 5, and 7, whereas all 3 mediator variables were assessed at both waves 4 and 6. To address missing data, the full information maximum likelihood (FIML) method was applied (Muthén et al 2016). Namely, full information from participants who had nonmissing data in at least 1 time point of the study was used to estimate the structural equation model (SEM).
Descriptive analyses examined frequency distributions of edentulousness, frailty, and sociodemographic, behavioral, and mediator variables on the full analytic sample with cross-sectional nonresponse weights applied. An autoregressive cross-lagged longitudinal SEM with a Bayesian estimator (Rosel and Plewis 2008) using probit regression was used to assess the direction and pathways of an association between edentulousness and frailty. The term autoregressive refers to the fact that each value of the variable depends on the value of that same variable in the previous measurement. This model also assumed initial covariance between baseline edentulousness and frailty. As the same edentulousness and frailty variables were measured in waves 3, 5, and 7, it was possible to study the directional effect of one variable on the other. Namely, these analyses examined the edentulism–frailty direction using incident frailty and the frailty–edentulism direction using incident cases of edentulism. Indirect pathways via nutrition, loneliness, and inflammation, which were measured at waves 4 and 6, were also tested. Analysis was adjusted for baseline (wave 3) sociodemographic factors and smoking. The sign of the probit regression coefficients in this model can be interpreted as follows: a positive coefficient indicates that an increase in the independent variable results in an increase in the predicted probability of an outcome variable, whereas a negative coefficient corresponds to a decrease in this probability. It is also possible to compare the relative strength of the paths (i.e., higher coefficients indicating stronger associations and coefficients closer to zero meaning weaker associations). The proposed SEM was assessed following the Bayesian analysis methodology by Muthén et al (2016). The convergence and quality of the posterior distribution for each model parameter were confirmed by inspecting the model plots, as well as the potential scale reduction criterion. Further details on the choice and assessment of the SEM are provided in the Appendix section 1.2 and Appendix Figure 2.
STATA SE 15.1 software was used for descriptive analysis, whereas SEM was completed using MPlus 8.
Results
Figure 1 shows how the analytical sample was derived, resulting in a baseline analytical sample of 6,800 individuals. Of these, 3,521 individuals were followed up until wave 7. The SEM analysis was conducted for all 6,800 baseline sample participants, using the FIML method to handle missing data.
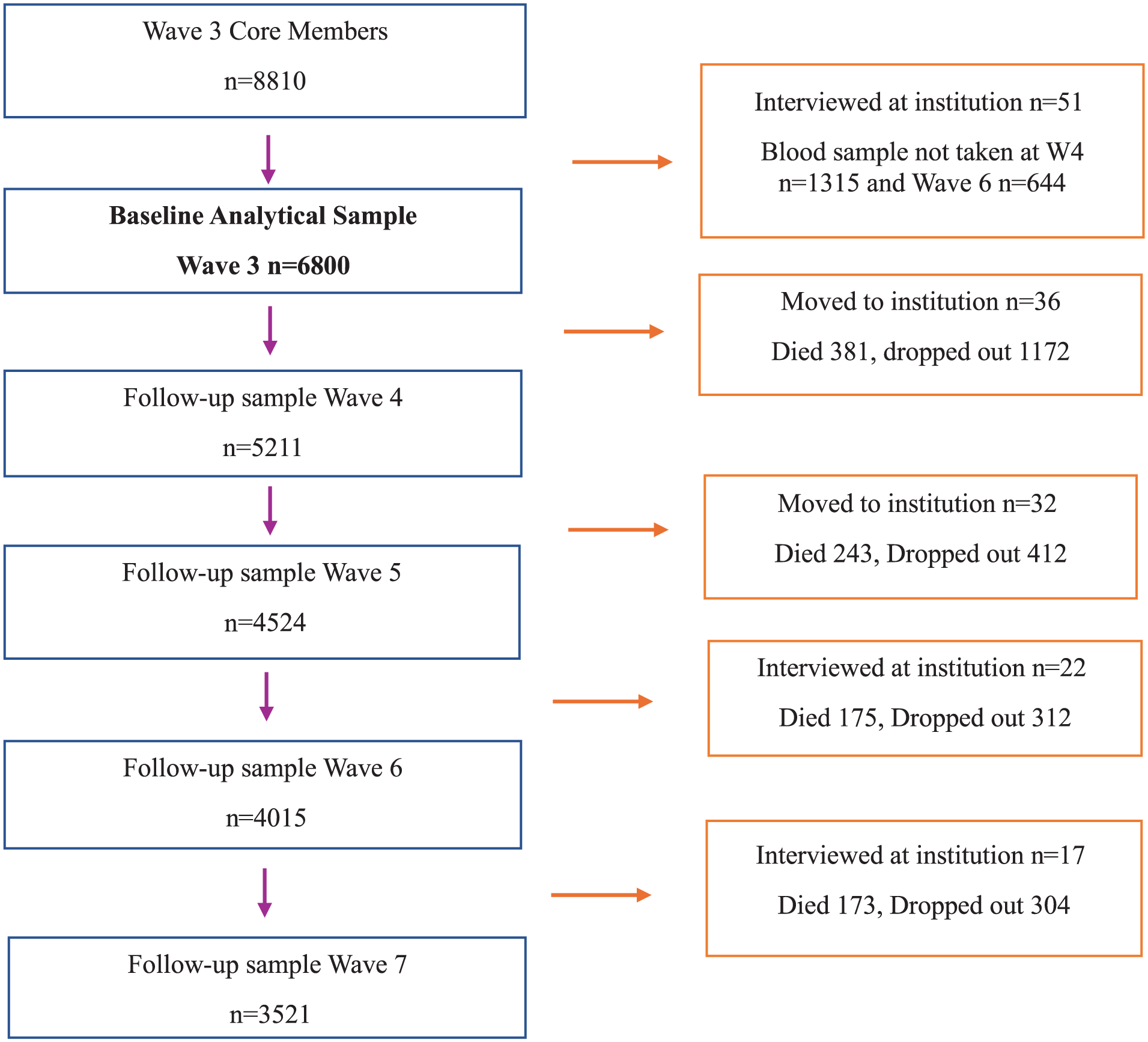
The construction process of the analytical sample for SEM analysis.
Table 1 displays the frequency distribution of edentulousness, covariate, and frailty variables in waves 3, 5 and 7. At baseline (wave 3), 52.8% of the sample were female, and the mean age was 65.5 (SD 10.9) y. In terms of tooth loss, 17.6% were edentate at baseline, 12.1% at wave 5, and 10.3% at wave 7. At baseline, 18.2% of the participants were frail, but the proportion of frail respondents halved in subsequent waves to 9.4% and 10.8% at waves 5 and 7, respectively.
Frequency Distribution of Edentulousness, Frailty, and Sociodemographic and Behavioral Variables in Waves 3, 5, and 7.
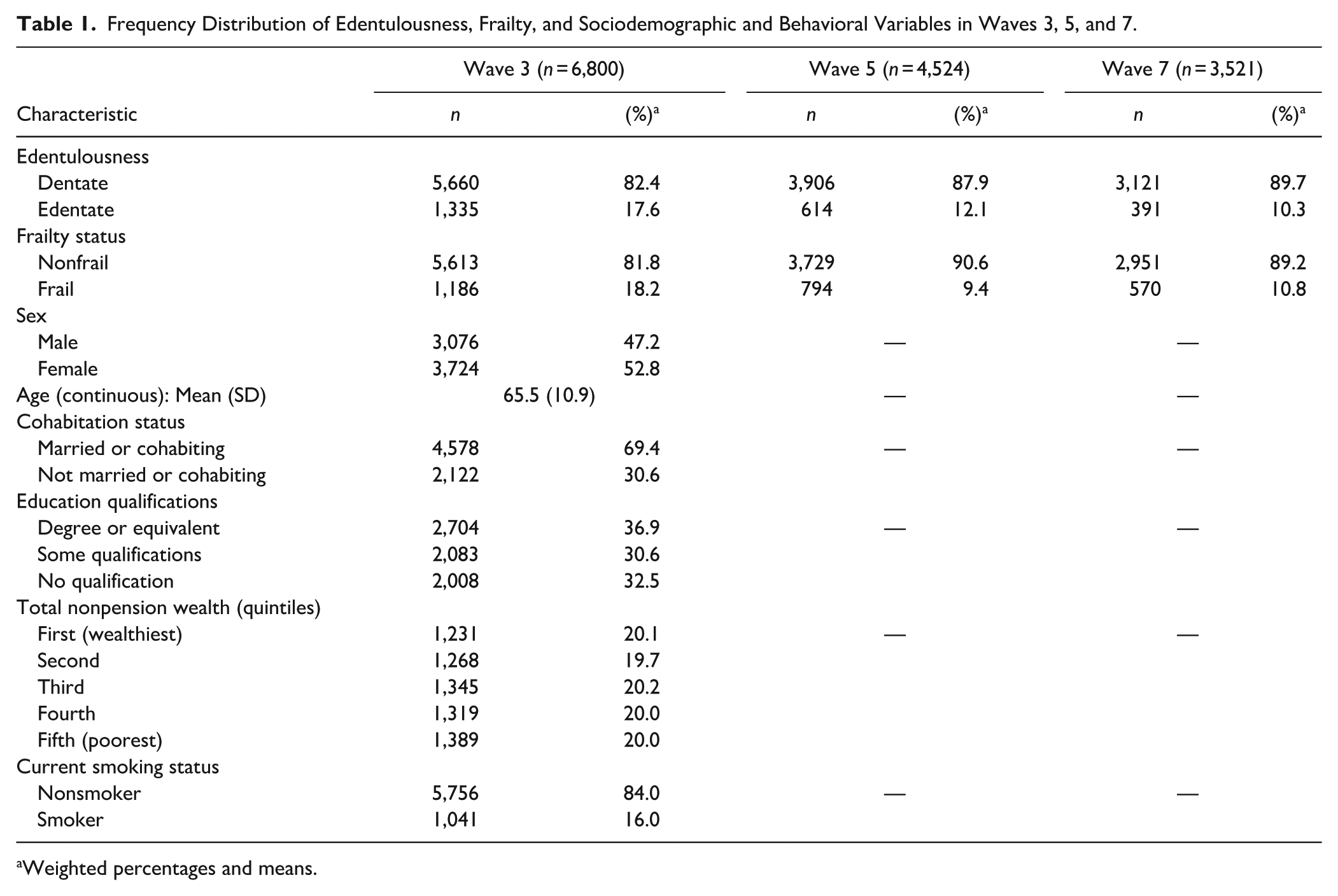
Weighted percentages and means.
Table 2 shows that daily consumption of 5 or more portions of fruit and vegetables was reported by 43.4% of participants at wave 4 and 62.1% at wave 6. At waves 4 and 6, just below one-fifth of the respondents reported being lonely (17.1% and 17.3%, respectively). The mean CRP level was 2.4 (SD 0.04) at wave 4, with a similar value of 2.1 (SD 0.04) observed at wave 6. The proportions of missing data are displayed in Appendix Tables 4 and 5.
Frequency Distribution of Mediator Variables in Waves 4 and 6.
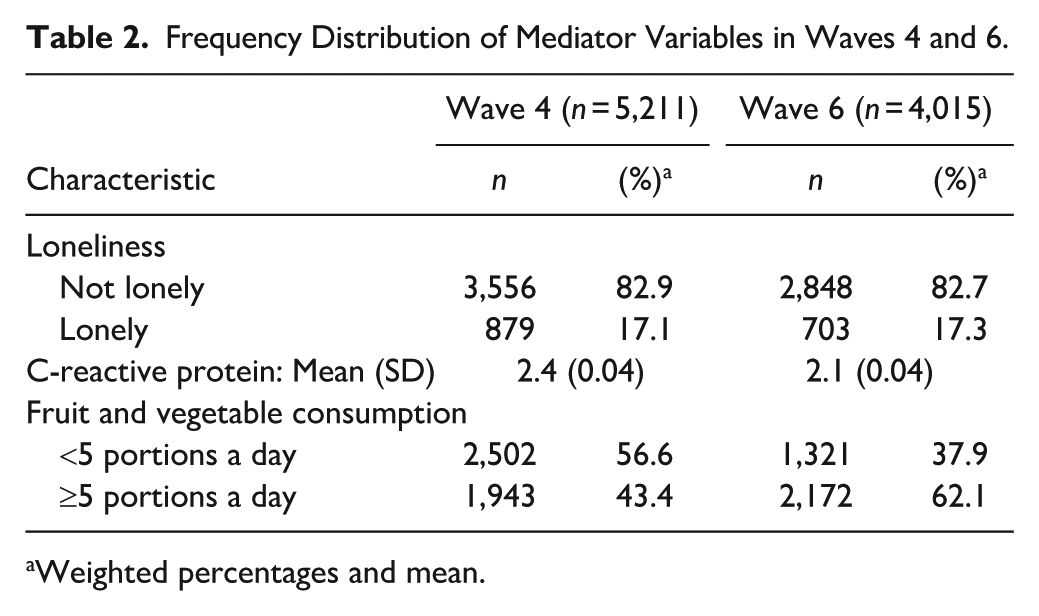
Weighted percentages and mean.
Table 3 and Figure 2 present the results of the SEM analysis. In the adjusted model, the direct paths from edentulousness to frailty indicated that being edentate at wave 3 was associated with a higher probability of incident frailty at wave 5, but there was no association between edentulousness at wave 5 and frailty at wave 7. The adjusted paths in the opposite direction (from frailty to edentulousness) were not statistically significant at both waves 3 to 5 and waves 5 to 7. Direct cross-lagged effects between edentulousness and frailty were attenuated following adjustment for sociodemographic characteristics and smoking. However, the indirect paths did not attenuate throughout the adjustment process.
Cross-Lagged Model for Bidirectionality and Pathways of an Association between Edentulousness and Frailty, Waves 3 to 7 (Total N = 6,800).
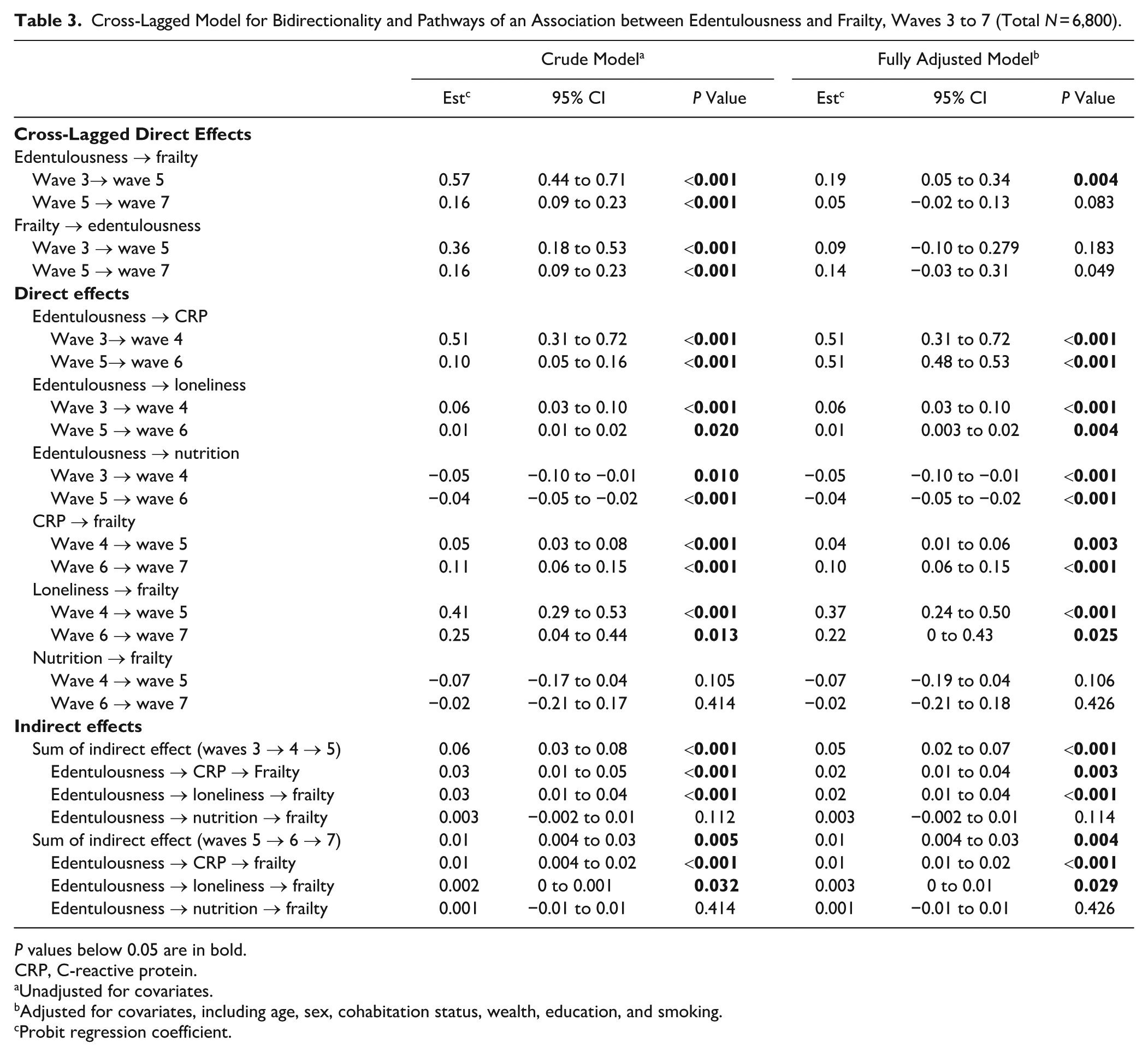
P values below 0.05 are in bold.
CRP, C-reactive protein.
Unadjusted for covariates.
Adjusted for covariates, including age, sex, cohabitation status, wealth, education, and smoking.
Probit regression coefficient.
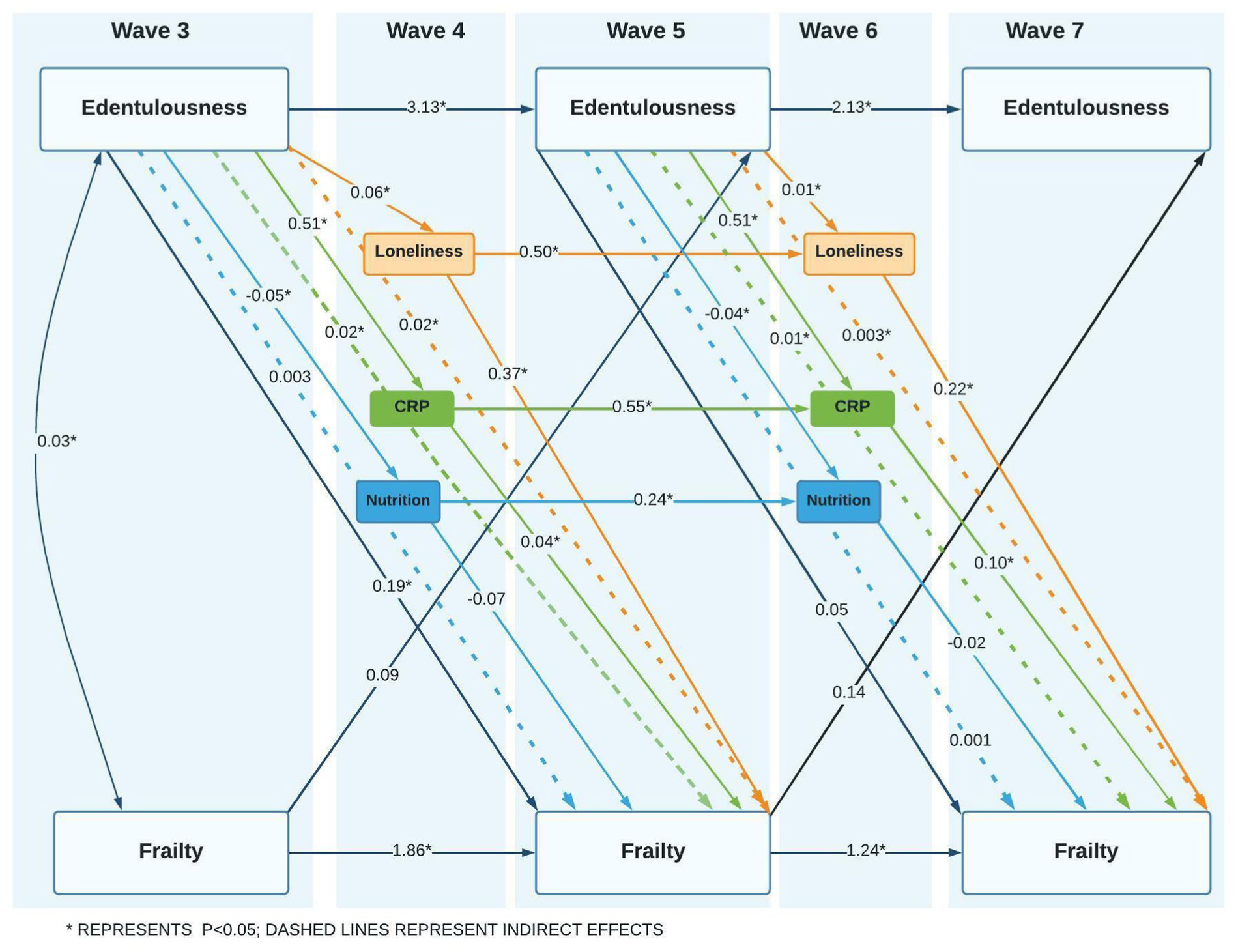
Cross-lagged model for bidirectionality and pathways of an association between edentulousness and frailty. Estimates adjusted for covariates, including age, sex, cohabitation status, wealth, education, and smoking.
Looking at the mediation analysis, no significant mediation via consumption of fruit and vegetables was observed. On the other hand, there was a small but significant mediation via loneliness at both waves 3-4-5 and waves 5-6-7. The estimates for indirect paths via CRP were also small but significant at both time points. The estimates for the respective indirect and direct paths from edentulousness to mediators and from mediators to frailty are presented in Table 3 and Figure 2.
Discussion
In this representative sample of older adults in England, the main findings of this study were that edentulousness had a significant effect on later frailty, while frailty was not associated with later edentulousness. Loneliness and CRP mediated the association between edentulousness and frailty to a small extent, whereas no mediation was observed via fruit and vegetable consumption. The adjustment for sociodemographic characteristics and smoking showed an attenuation of the direct associations between edentulousness and frailty, suggesting their potential confounding role.
This study corroborates evidence from previous longitudinal studies, which showed that having fewer teeth (Castrejón-Pérez et al 2017; Kimble et al 2023; Xu et al 2023; Komiyama et al 2024; Lin et al 2024) and being edentulous (Ramsay et al 2017; Velázquez-Olmedo et al 2021; Kimble et al 2023) were associated with a higher risk of incident frailty after adjustments for a range of covariates, including sociodemographics, general health characteristics, and smoking, with follow-up periods spanning from 1 to 16 y. Although the effect sizes observed in this study are not directly comparable to those reported by previous studies due to the heterogeneity of the measures used, our study further supports evidence for an association between edentulousness and later frailty. On the other hand, we found no evidence to support a path in the opposite direction (from frailty to edentulousness). Several potential explanations can be postulated for the lack of an association. First, in ELSA, the exact timing of becoming edentate is unknown, and participants may have been edentate for a long time. Second, the time lag between frailty and edentulousness in this analysis (i.e., 4 y) might have been too short to show an impact on the incidence of edentulism. Finally, we also note that while a bidirectional association between edentulousness and frailty has been postulated in the literature, it has also been argued that this association may be due to comorbidities related to common risk factors (Hakeem et al 2019).
Previous cross-sectional studies indicated potential mediation effects via nutritional status in the association between the number of teeth and frailty (Hakeem et al 2020, 2021; Xia et al 2024). Small yet significant mediation effects through nutrition on the relationship between tooth loss and frailty were also demonstrated in the longitudinal study by Xu et al (2023). Those studies assessed nutrition through composite variables, including nutritional intake based on micronutrients from the dietary assessment (Hakeem et al 2021), the Mini Nutritional Assessment (Hakeem et al 2020, Xia et al 2024), and the dietary diversity score assessed by a food frequency questionnaire (Xu et al 2023). The lack of mediation via fruit and vegetable consumption in our longitudinal study may be due to the limitations of the dietary data available in ELSA, where a single question on fruit and vegetable portion consumption cannot comprehensively assess nutritional status.
This study found a small but significant mediation effect through loneliness, an established risk factor for frailty (Kojima et al 2022). While adverse psychosocial consequences of poor oral health have been hypothesized to link oral health and frailty (Hakeem et al 2019), to our knowledge, this is the first study that provided longitudinal empirical evidence for the role of this mediating pathway in the association between edentulousness and frailty. Our findings build upon evidence from a longitudinal study among Chinese older adults (Ma et al 2023), which showed that social relationships play a partial mediating role in the association between tooth loss and instrumental activities of daily living, which are also part of the frailty index assessed in our study.
The finding of a small but significant mediation pathway via inflammation in the association between edentulousness and frailty builds upon previous research suggesting that edentulousness (Kotronia et al 2020) is associated with increased plasma CRP levels in older adults. A previous longitudinal study from Sweden (Welmer et al 2017) also showed that adjustment for CRP explained the association between tooth loss and accelerated decline in walking speed, a component of the frailty phenotype. Cross-sectional data from another study in China (Lin et al 2024) also indicated that higher levels of CRP explained 5% to 6% of the association between dentition status, assessed as having 20 or more natural teeth, and frailty. Our study, therefore, further expands existing evidence by documenting the longitudinal mediation role of the inflammation pathway. A potential explanation for the mediation path of edentulousness-CRP-frailty could be that tooth loss is a consequence of periodontal diseases and that inflammation in the periodontal tissue is associated with general health (Castrejón-Pérez et al 2017; Sabbah et al 2018). Moreover, edentulousness has been associated with multiple chronic conditions in older adults (Hag Mohamed and Sabbah 2023), which can lead to frailty (Villacampa-Fernández et al 2017). Similarly, tooth loss has been linked to an increased risk of cognitive and physical decline (Tsakos et al 2015), which are also key frailty components involving inflammatory mechanisms (Sanada et al 2018) and, therefore, may underpin the edentulousness-inflammation-frailty pathway.
This study added to the evidence base of directionality and pathways of the longitudinal association between edentulousness and frailty. The strengths include analysis of a large, nationally representative sample of adults aged 50 y and older living in England and the use of SEM, which enabled the analysis of several potential mediating factors and direction of associations between edentulousness and frailty. Analyses also adjusted for a set of relevant potential confounding factors.
We also acknowledge a number of limitations. This analysis used edentulousness as the oral health variable because information on the number of remaining teeth, a more refined measure of oral function, was not available. In addition, although missing data and sample attrition were addressed through the FIML method, individuals who did not have blood tests taken due to general health problems cannot be considered missing at random, thereby likely violating a key assumption of the method. Also, considering the high proportion of sample attrition during the study follow-up and the reduction of the prevalence of frailty, particularly between waves 3 and 5, it is possible that frail individuals were more likely to die or drop out of the study. Therefore, this analysis may have excluded individuals with less favorable health characteristics and, consequently, may have underestimated the strength of associations between oral health and frailty. On the other hand, mortality can also be a competing outcome in the relationship between edentulism and frailty; therefore, future research focusing on competing-risk analysis is required. We also acknowledge that, while we have explored independent indirect effects of loneliness, inflammation, and nutrition in the association between edentulousness and frailty, it is possible that there is mutual influence between the different pathways, and this is an important implication for future research. Similarly, edentulism, its psychosocial consequences such as loneliness, and subsequent progression to frailty may occur over differing time scales, which may not be fully captured within the available fixed time intervals in this study. Also, given that frailty is a potentially reversible dynamic condition, and considering that becoming edentate may require longer follow-up than available in our study, future research should examine their association, considering dynamic trajectories of frailty and edentulousness over longer follow-up periods. Moreover, while our analysis using the SEM Bayesian estimator with the probit regression coefficients allowed us to estimate the direction and significance of the associations, it was not possible to fully quantify the magnitude of an association.
Our study highlighted that edentulousness is associated with frailty in older adults, and this happens partly through psychosocial and inflammatory pathways. In the context of global population aging, this evidence supports the integration of oral health care into general health care systems, aligned with the WHO Global Oral Health Action Plan (WHO, 2024b). From a public health and policy perspective, the findings of this study suggest that retaining natural teeth into later life may reduce the risk of frailty and need for long-term care, lowering the burden on health care systems. Health promotion strategies across the life course to maintain good oral health into older adulthood, as well as health promotion initiatives to tackle loneliness in older people, may help prevent frailty. Future research should evaluate the role of such policies in lowering the risk of frailty in older adults.
Conclusion
This longitudinal study used a novel approach by comprehensively exploring directionality and pathways of the association between edentulousness and frailty among older adults in England. Edentulousness was associated with a higher probability of frailty over time, with some evidence for mediation via loneliness and inflammation, but frailty did not predict later edentulousness. The findings of this study can inform future health promotion strategies aimed at frailty prevention.
Author Contributions
E. Petrauskiene, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; P. Zaninotto, A. Heilmann, A. Peasey, G. Tsakos, contributed to conception and design, data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345251414409 – Supplemental material for Edentulousness and Frailty: A Study of Directionality and Pathways
Supplemental material, sj-docx-1-jdr-10.1177_00220345251414409 for Edentulousness and Frailty: A Study of Directionality and Pathways by E. Petrauskiene, P. Zaninotto, A. Heilmann, A. Peasey and G. Tsakos in Journal of Dental Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the PhD studentship through the MRC grant MR/N013867/1. The English Longitudinal Study of Ageing is funded by the National Institute on Aging (Ref: R01AG017644) and by a consortium of UK government departments: Department for Health and Social Care, Department for Transport, and Department for Work and Pensions, which is coordinated by the National Institute for Health Research (NIHR, Ref: 198-1074). Funding has also been provided by the Economic and Social Research Council (ESRC).
A supplemental appendix to this article is available online.