
Abstract
In 2019, France implemented a large-scale reform aimed at reducing out-of-pocket health care expenditures, with the objective of preventing the forgoing of dental care for financial reasons. The aim of this study was to assess the impacts of this reform on dental care utilization, with a focus on full dentures as prosthetic care, which was the main target of the reform. The study was based on analyses of large-volume administrative data from the French social health insurance funds and comprised >1 billion dental treatments encountered in the years 2014 to 2023. Drawing from a quasi-experimental research design and segmented negative binomial regression, controlled interrupted time series analyses were conducted with a “control outcome” approach. Controlled interrupted time series analyses compared utilization rates for various types of care whose coverage was differentially affected by the reform. Models were adjusted for COVID-19 and seasonality covariates and stratified by socioeconomic status. Following the removal of out-of-pocket payments for resin-based full dentures, their utilization was 58.85% higher (95% CI, 37.18% to 83.95%) as compared with the control scenario. The utilization of other types of dental care, largely unaffected by the reform, remained unchanged. Prophylactic care use increased only slightly during the study period. These findings suggest that the removal of out-of-pocket expenditures through the French 100% santé reform led to higher utilization of full dentures. However, as the reform focuses on specific treatment items and mainly concerns patients with voluntary health insurance, the impacts of the reform should be carefully monitored in the future, particularly its effects on vulnerable populations.
Keywords
Introduction
Scarcity in public financing poses challenges for expanding coverage in disciplines such as oral health care, which are mainly privately financed, with a high proportion of out-of-pocket (OOP) payments. These costs are a major driver in catastrophic health expenditures and represent financial barriers in accessing dental care. While the urgency of achieving universal health coverage for oral health care is emphasized (United Nations 2019), there are still few attempts to extend oral health care coverage. Most reforms are limited to expanding public funding for narrowly defined treatment items or specific patient groups. To this end, understanding the impacts of broader changes in oral health care coverage, such as the French reform examined in this study, is particularly relevant.
Following the 2017 presidential campaign that highlighted the need for better dental prostheses coverage, the 100% santé reform was implemented in 2019. In France, dental care is usually provided by private dentists who receive fee-for-service payments. At that time, 70% of primary dental care costs were covered by social health insurance (SHI) (Or et al. 2023), and the remaining 30% were covered via private voluntary health insurance (VHI), half of which provided by employers. Low-income individuals had 100% coverage through publicly funded programs (Pegon-Machat et al. 2016). However, 5% of the population lacked additional VHI insurance. Before the reform, dentists could set prosthetic treatment fees freely, leading to high OOP costs for patients without adequate supplementary coverage. In 2019, the reform introduced several changes. Full coverage with no OOP costs was introduced for VHI holders and for prosthetic care such as resin-based full dentures, implementing price ceilings and full coverage commitments from VHI insurers. The reform also increased progressively fixed fees for primary care (endodontics, oral surgery, restorative & prophylactic treatments). Moreover, various already-existing public assistance programs were merged to provide single 100% public coverage (Complémentaire Santé Solidaire [CSS] 2023) for low-income individuals.
For people affected by severe tooth loss, access to full dentures is essential. Indeed, full edentulism is the final end point of oral diseases, with major detrimental impacts on quality of life (Felton 2016). In France, the prevalence of edentulism for those 65 to 74 y old was 9.2% in 2016, representing a high number of patients for whom access to full dentures is essential (Stock et al. 2016). Previous literature suggests associations between the level of OOP and difficulties in gaining access to dental care (Bas et al. 2020; Bas and Azogui-Lévy 2022).
The aim of this study was to assess the impacts of the 100% santé reform on the utilization of dental care in France, with a focus on full dentures as prosthetic care. The study was based on the analyses of dental claims data from SHI funds before and after implementation of the 100% santé reform (2014 to 2023), while considering the effects of the COVID-19 pandemic.
Methods
Study Design
Drawing from state-of-the-art methods for evaluating the impact of population-wide policy reforms, a quasi-experimental research design was chosen (Kim and Steiner 2016; Lopez Bernal et al. 2018; Coopersmith et al. 2022; Listl et al. 2022). We followed the STROBE-RECORD checklist (Benchimol et al. 2015) and conducted controlled interrupted time series analyses (CITSAs) based on multiple observations of an outcome at several consecutive time points. CITSAs allow one to consider confounding factors such as temporal changes during a study period (Linden 2015; Lopez Bernal et al. 2018).
Data Source
The data source was the SNDS database (Système National des Données de Santé), which gathers data on health claims paid or reimbursed by SHI for the whole French population (Bezin et al. 2017; Tuppin et al. 2017). Dental treatments delivered by a dentist between June 30, 2014, and September 30, 2023, were included in this study. Orthodontic treatments, treatments not covered by SHI such as implants, and dental care delivered by medical doctors or in public hospitals were excluded. Irrelevant extra fees or periods for which data were insufficiently complete were excluded. The selection process is described in Appendix Figure 1.
Examined Coverage Changes
During the study period (January 2015 to June 2023, 443 wk), the reform was characterized by different intervention time points depending on the type of treatment considered or the patients’ profile (Table 1, Appendix 1, Appendix Table 1). Specifically, 100% coverage for resin-based full dentures was implemented in January 2021 for patients with SHI and VHI. Moreover, the new CSS scheme for low-income earners, merging 2 former schemes, was implemented in November 2019.
Time Frame for the 100% Santé Interventions during the Study.
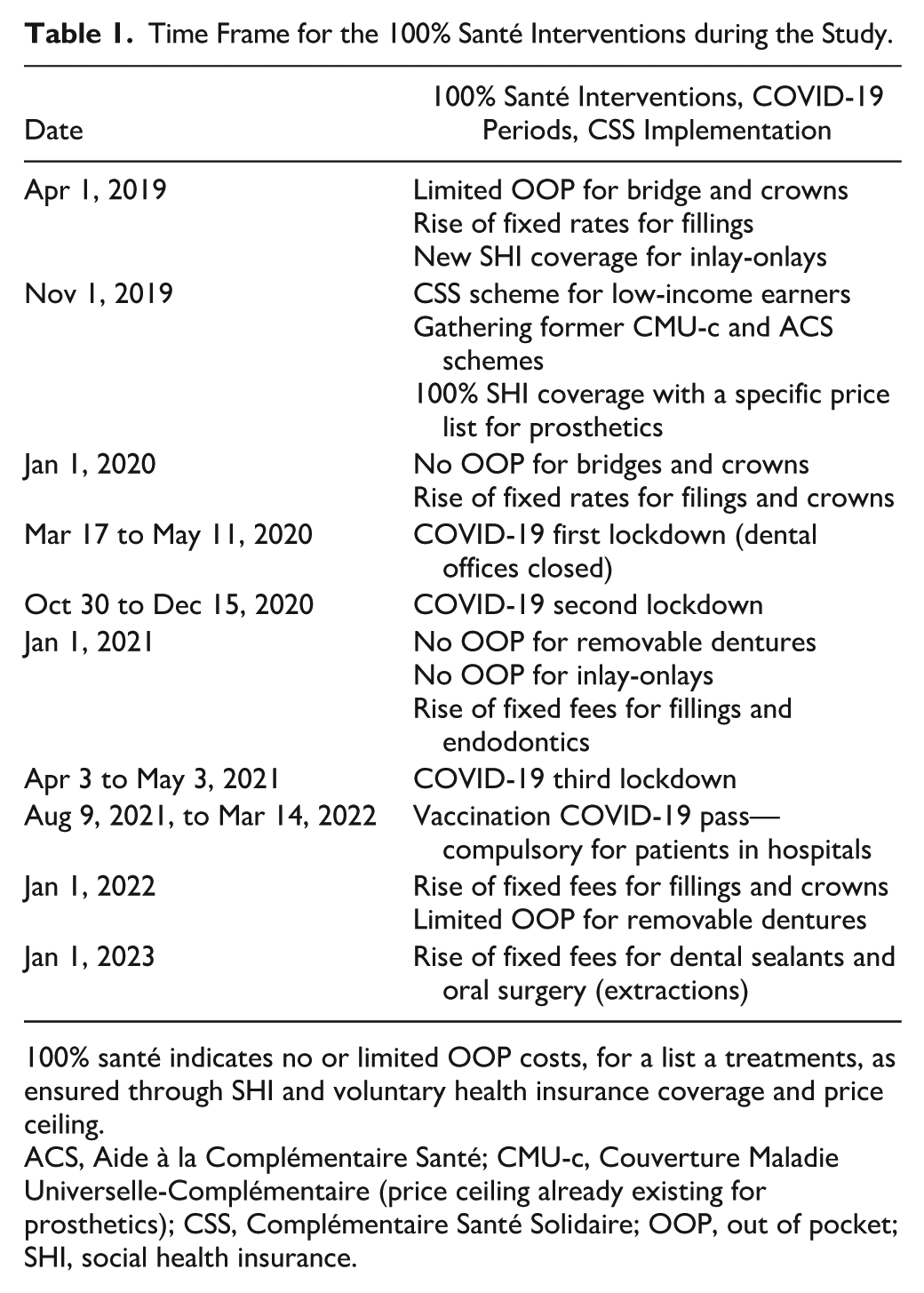
100% santé indicates no or limited OOP costs, for a list a treatments, as ensured through SHI and voluntary health insurance coverage and price ceiling.
ACS, Aide à la Complémentaire Santé; CMU-c, Couverture Maladie Universelle-Complémentaire (price ceiling already existing for prosthetics); CSS, Complémentaire Santé Solidaire; OOP, out of pocket; SHI, social health insurance.
Primary Outcome Variable
The primary outcome of interest was the weekly number of full dentures in the upper and lower jaws. For descriptive analyses, the weekly utilization rate was calculated by dividing the number of such treatments per week by the population size in the same year. The rate was expressed per 100,000 inhabitants (INSEE 2024).
CITSA Approach with Comparison of Primary vs Control Outcomes
CITSA usually explores changes in the level or trend of a single outcome, assessed before and after a defined intervention point, for an intervention group (affected by the reform) as compared with a control group (not affected). The 100% santé reform was implemented nationwide for the entire population; therefore, no population- or location-based control groups were available. In the absence of other applicable control groups, a “control outcome” approach was followed, as described by Lopez Bernal et al. (2018): the utilization of full dentures (primary outcome; intervention group) was compared with the utilization of oral surgery (control outcome; control group), as oral surgery was not subject to the 100% santé reform until 2023.
An immediate and persistent change in the utilization of full dentures was hypothesized at the intervention time point (i.e., the first week of January 2021), dividing the study period into 313 points before the intervention and 130 points after.
Statistical Approach
The characteristics of the population and the numbers and rates of utilization of different types of dental treatments were first described: dental visits, restorative treatments, and prophylactic care, along with full dentures and oral surgery (Appendix 2).
CITSAs were conducted via segmented negative binomial regression to account for overdispersion, drawing from the following general equation (Huitema and McKean 2000):

with Yt as the number of treatments per week at time point t and with Z as a binary variable indicating outcome status (primary outcome; i.e., intervention group vs control). The parameters β0 to β3 refer to the differences for the control outcome: β1 slope (preintervention), β2 level (intervention), and β3 slope (pre- to postintervention). The parameters β4 to β7 refer to differences between intervention and control outcomes: β4 levels (baseline), β5 slopes (preintervention), β6 levels (intervention), and β7 slopes (postintervention). We included the offset term ln(Pa), where Pa represents the annual population, to model the utilization rate and take into account changes in population size. A detailed description of the model specifications (relevant parameters, alternative specifications for robustness checks) are provided in Appendix Table 2 and Appendix 3.
Residual autocorrelation of multiple order was assessed by generalized Durbin-Watson tests and heteroscedasticity of residuals by Breusch-Pagan tests. Newey-West standard errors with automatic lag selection consistent, in case of autocorrelation and heteroscedasticity, were computed (Newey and West 1994; Zeileis 2004). As dentist’s activity is affected by seasonality (Christmas, summer), the number of bank holidays in a week and the week effects during holiday periods were considered in the models.
Two-sided tests were performed and P values interpreted considering the size of the differences based on clinical interpretation. Results are reported with rate ratios (RR = eβi) and 95% CIs, which indicate the relative change in the weekly rates between outcomes or periods. All the analyses were realized within the SNDS environment, using SAS (Guide version 8.3) and RStudio (version 4.1.2).
Stratified Analyses
Differential effects in the trends of full denture utilization between CSS and non-CSS patients were supposed. The impact of the reform was assessed via a CITSA stratified on CSS status after November 2019. Indeed, CSS patients were not directly concerned by the implementation of the “no OOP” measure for prosthetic treatments in January 2021. The annual number of CSS beneficiaries and the annual French population minus the number of CSS beneficiaries (= non-CSS beneficiaries), were considered as offsets in stratified models (CSS 2023). Another stratified CITSA was conducted to explore differential evolutions related to 2 time points: November 1, 2019 (time point for CSS), and January 1, 2021 (time point for non-CSS). To do so, the beneficiaries of former public supplementary coverage were grouped as CSS users before November 2019.
Robustness Checks
A dummy variable was added, identifying the first COVID-19 lockdown during which dental offices were closed and distinguishing the first week partly affected, from the remaining weeks of the lockdown. Other analyses were conducted that omitted the 8 wk of the first lockdown and 41 wk in 2020 from the first lockdown. The interactions between outcomes and COVID-19 variables were integrated in the models when significant. We also checked the intervention effects depending on age by conducting a CITSA limited to older adults (aged ≥60 y; Appendix Table 2).
Ethics and Data Protection
Access to the database was managed through the Clermont-Ferrand Hospital, which has permanent access to the SNDS. The study was approved by the local ethics committee (IRB00013412) and validated for its compliance with the French individual data protection policy.
Results
The study population is described in Appendix Table 3. Around 10% of the French population benefited from the CSS coverage, with a slight increase with time. This proportion was lower for dental care users (8% to 9%) and higher for complete denture users (19% to 28%), with a large decrease from 2021 on. The mean (SD) age of dental care users increased with time and varied in 2022 from 50.83 y (23.2) for oral surgery to 69.62 (12.4) for full dentures.
Figure 1 shows the trends in dental care utilization per type of treatment. The utilization for restorative and oral surgery care was stable during the study period. Prophylactic care tended to increase with time. A net increase in the level of utilization for full dentures can be noticed in January 2021.
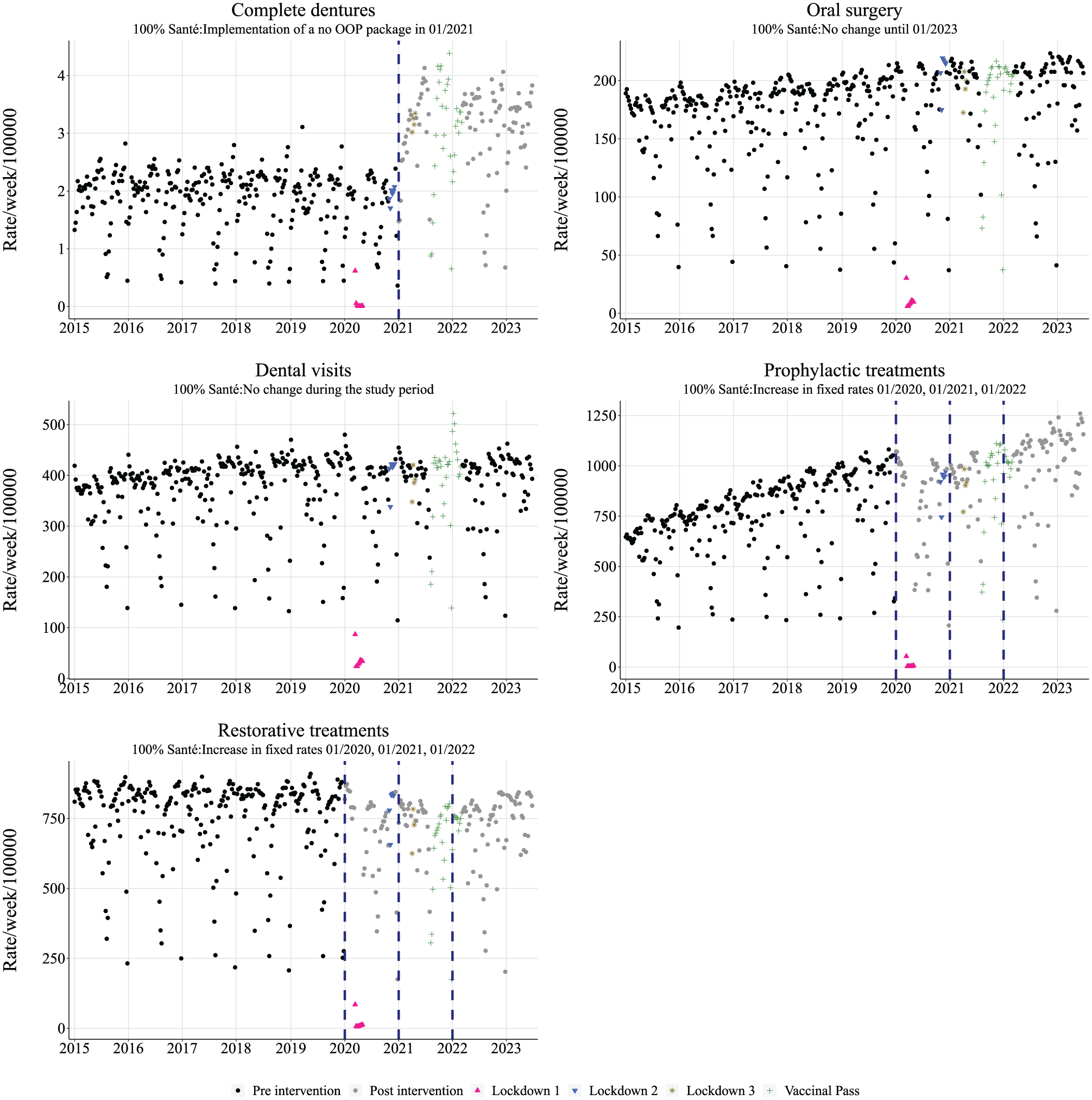
Rate of dental care utilization per type of treatment. OOP, out of pocket.
Table 2 presents the CITSA for the 2015–2023 period. There was a slight increase in the utilization of oral surgery and a slight decrease for complete dentures during the preintervention period, with a difference of trend between the outcomes. When no OOP on dentures was implemented, an additional 58.85% increase (95% CI, 37.18% to 83.95%) in their utilization was observed as compared with oral surgery utilization, which remained stable. No difference in trends was observed between the outcomes in the postintervention period. The model adjusted with the first COVID-19 lockdown periods, integrating interactions between outcomes and COVID-19 variables, was chosen for all CITSAs (Appendix Table 4).
Controlled Interrupted Times Series Analysis Comparing Primary Outcome (Intervention Group; Full Dentures) vs Control Outcome (Oral Surgery) for the 2015–2023 Period: Segmented Negative Binomial Regression.
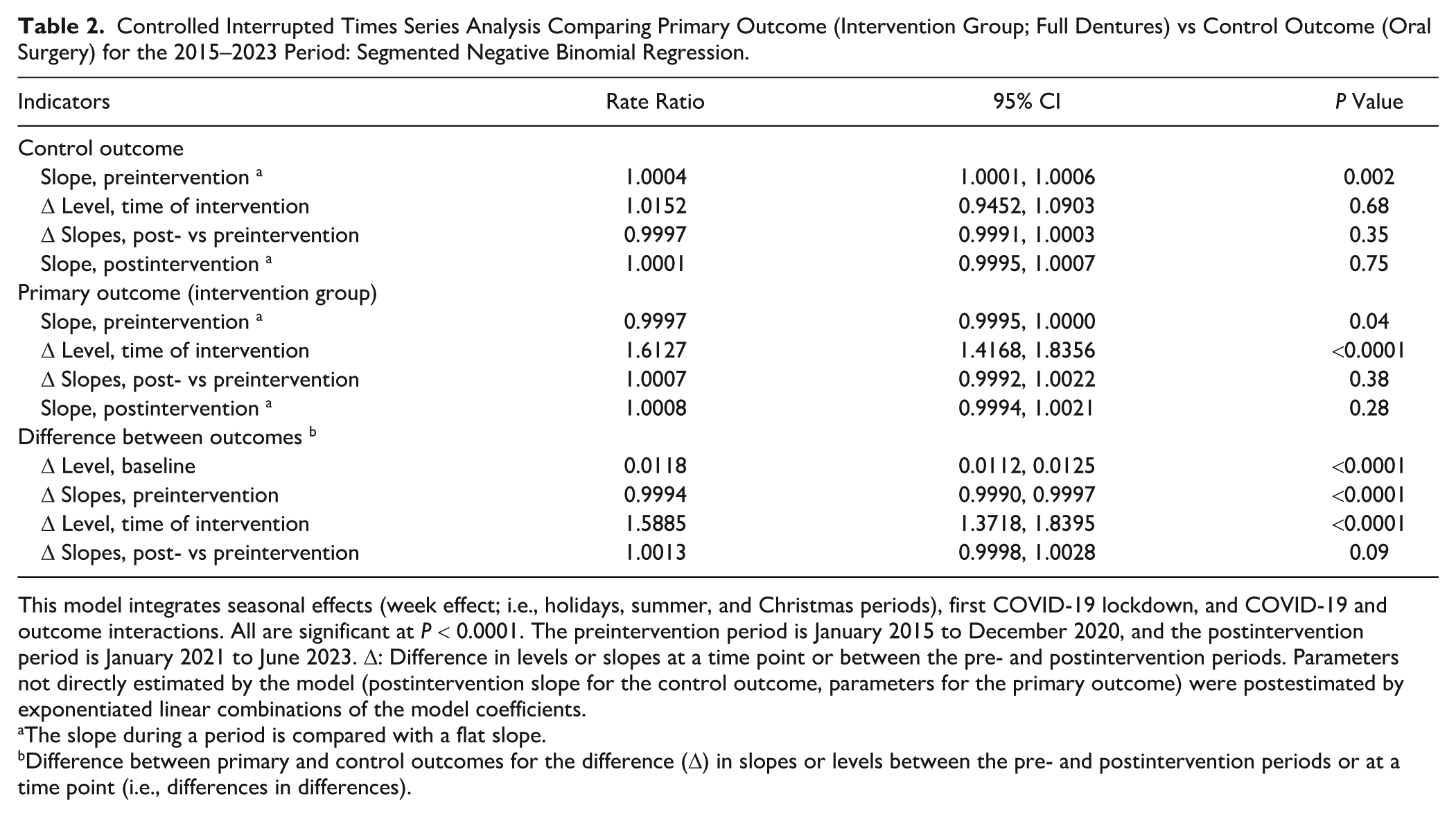
This model integrates seasonal effects (week effect; i.e., holidays, summer, and Christmas periods), first COVID-19 lockdown, and COVID-19 and outcome interactions. All are significant at P < 0.0001. The preintervention period is January 2015 to December 2020, and the postintervention period is January 2021 to June 2023. Δ: Difference in levels or slopes at a time point or between the pre- and postintervention periods. Parameters not directly estimated by the model (postintervention slope for the control outcome, parameters for the primary outcome) were postestimated by exponentiated linear combinations of the model coefficients.
The slope during a period is compared with a flat slope.
Difference between primary and control outcomes for the difference (Δ) in slopes or levels between the pre- and postintervention periods or at a time point (i.e., differences in differences).
Figure 2 shows results of stratified CITSA on CSS status for the 2019–2023 period (Appendix Table 5). No change was observed in the utilization of oral surgery for CSS and non-CSS patients. During the preintervention period, parallel slopes were observed for oral surgery and complete dentures for non-CSS and CSS patients. For non-CSS patients at the time of intervention (no OOP), a significant difference in levels of 85% was observed between outcome groups. There was no difference in slopes between the outcomes in the postintervention period.
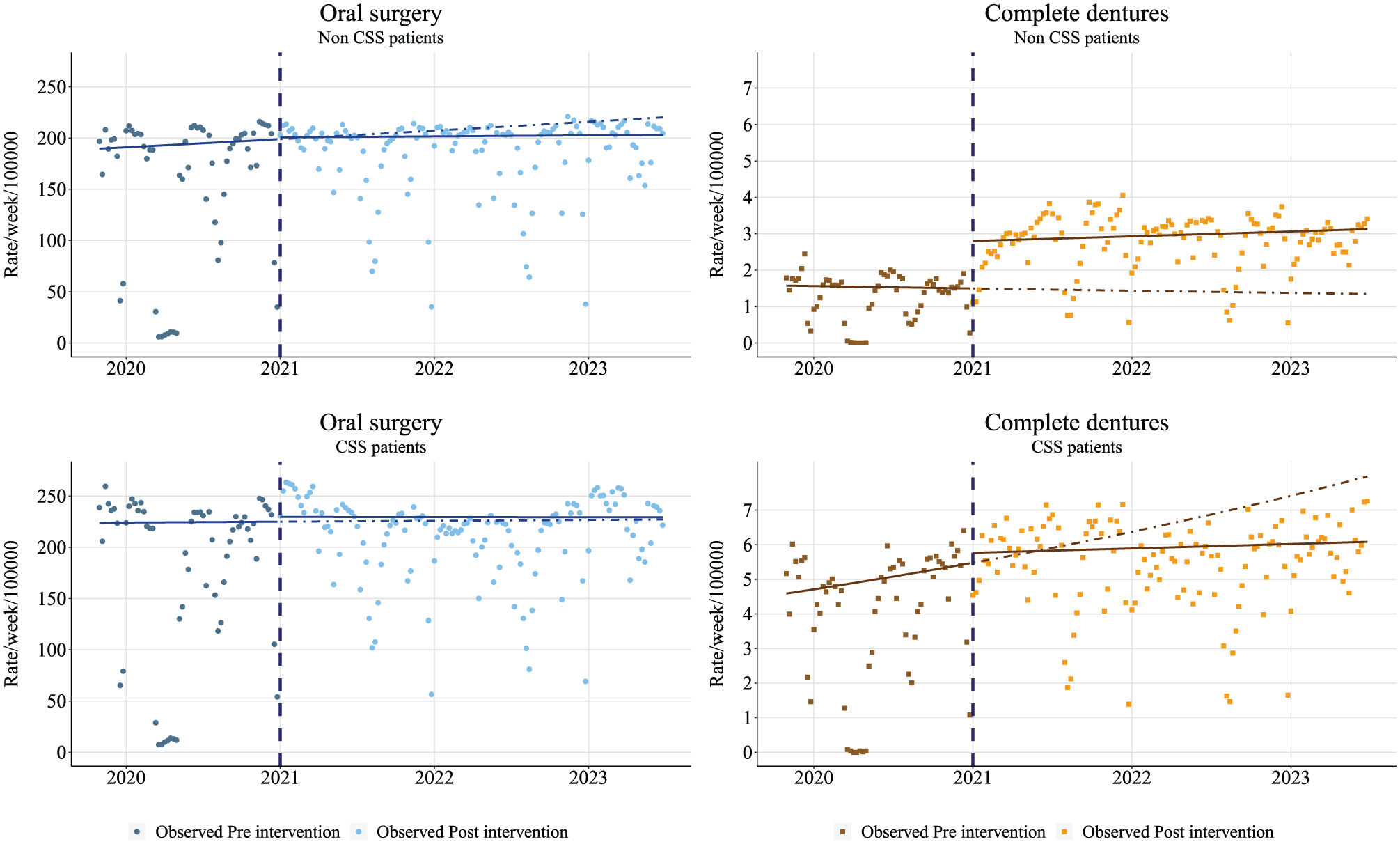
Stratified controlled interrupted time series analysis comparing primary outcome (i.e., intervention group; full dentures) vs control outcome (oral surgery) for the 2019–2023 period for CSS and non-CSS patients. Segmented negative binomial regression. Dot, observed rate; solid line, estimated deseasonalized trend; dotted line, estimated deseasonalized trend without intervention (i.e., counterfactual). CSS, Complémentaire Santé Solidaire.
Stratified CITSA on CSS status with 2 intervention points (November 2019, January 2021) is presented in Table 3. During the 2015–2019 period, there was a significant increase in the utilization of oral surgery and complete dentures for CSS patients, with no difference in trends between the outcomes. For non-CSS patients, a slight decrease in prosthetic care consumption was observed (RR, 0.999; 95% CI, 0.996 to 1.002). The difference between intervention and control slopes was significant but with a small variation. In November 2019 (implementation of the CSS scheme), no change was observed in non-CSS patients, while a decrease in the level of utilization of oral surgery (significant) and prosthetic care was observed for CSS patients. During the 2019–2023 period, the trends remained stable for oral surgery and prosthetic care in CSS and non-CSS patients. An increase in the level of utilization was observed after the second time point (no-OOP option) for prosthetic care: this increase is significant for non-CSS patients (+88%). The slopes for prosthetic care were stable in the postintervention period for CSS and non-CSS patients.
Stratified Controlled Interrupted Times Series Analysis Comparing Primary Outcome (Intervention Group; Full Dentures) vs Control Outcome (Oral Surgery) for the 2015–2023 Period for CSS and Non-CSS Patients: Segmented Negative Binomial Regression.
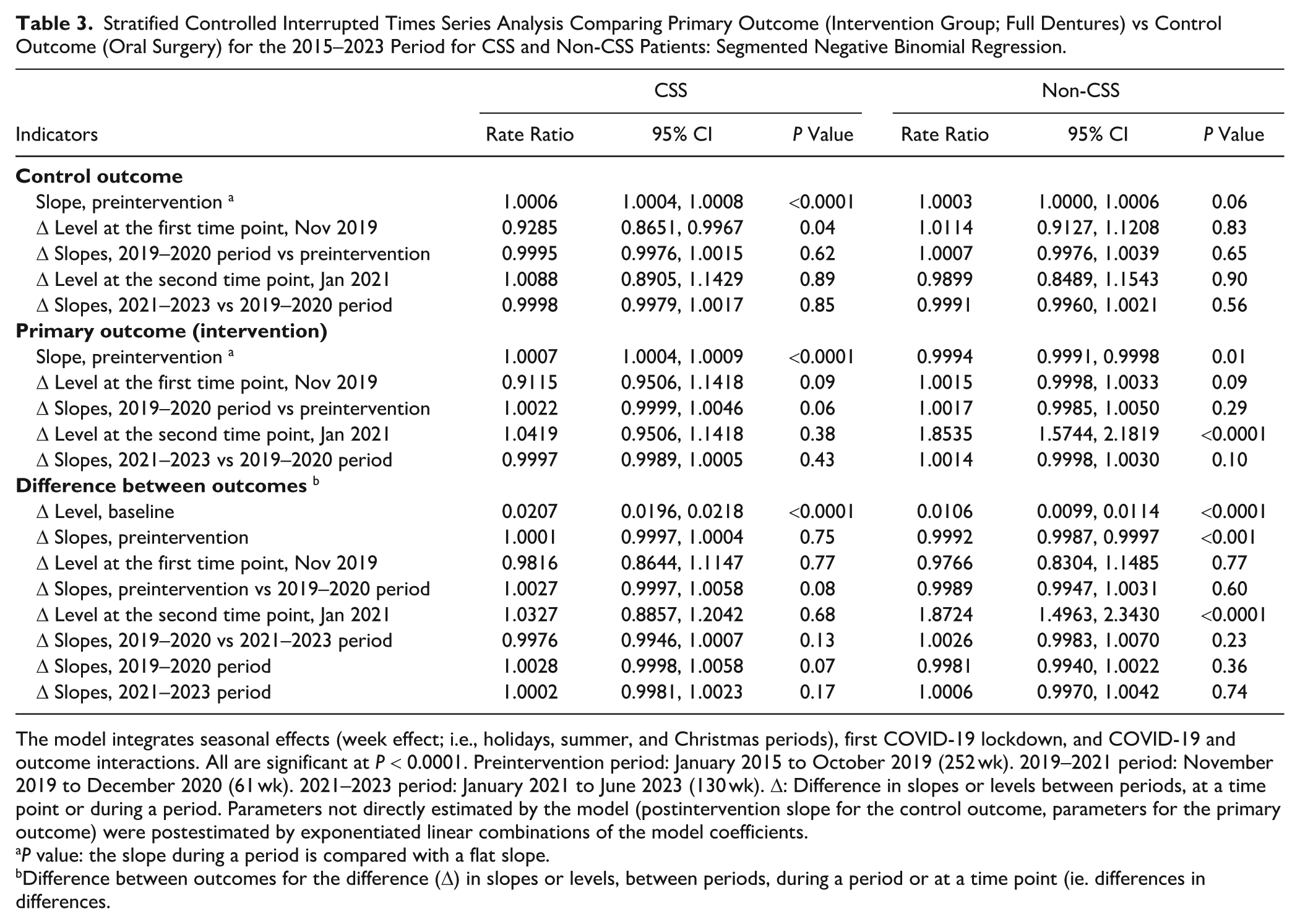
The model integrates seasonal effects (week effect; i.e., holidays, summer, and Christmas periods), first COVID-19 lockdown, and COVID-19 and outcome interactions. All are significant at P < 0.0001. Preintervention period: January 2015 to October 2019 (252 wk). 2019–2021 period: November 2019 to December 2020 (61 wk). 2021–2023 period: January 2021 to June 2023 (130 wk). Δ: Difference in slopes or levels between periods, at a time point or during a period. Parameters not directly estimated by the model (postintervention slope for the control outcome, parameters for the primary outcome) were postestimated by exponentiated linear combinations of the model coefficients.
P value: the slope during a period is compared with a flat slope.
Difference between outcomes for the difference (Δ) in slopes or levels, between periods, during a period or at a time point (ie. differences in differences.
A summary of main results for robustness analyses is presented Appendix Table 2.
Discussion
This study assessed the impact of a health care financing reform on the utilization of dental care in France. The reduction in OOP expenditures led to an increase in the utilization of full dentures as compared with the control scenario. The effect was smaller for low-income individuals with public supplementary coverage (CSS), as primary targets of the reform were patients with private VHI. Considering other types of dental treatments for which fixed tariffs have been revalued during the study period, their utilization rates remained largely unchanged. However, prophylactic care utilization increased slightly during the study period.
Our study is consistent with previous findings suggesting that lower copayments are associated with an increased utilization of dental care (Park et al. 2018). Insurance expansion by alleviating the cost burden of dental treatments tends to improve dental attendance and self-reported oral health with potentially lower unmet needs for older adults. However, there are inconsistent findings regarding the impact of insurance expansion on socioeconomic health inequalities (Kim et al. 2021). Moreover, increasing the utilization of dentures is not systematically related to improving chewing ability in the long term (Kim et al. 2022).
In this study, utilization rates for primary dental care (visits, restorative care, oral surgery) did not change much apart from a slight increase in prophylactic treatments. This trend aligns with findings showing that when prophylactic services are affordable, patients are more likely to engage in regular oral health practices (Lau et al. 2014). Financial incentives such as increased fees may also support practitioners’ utilization of prophylactic treatments. However, in this case, CITSA-type explanatory analyses should be conducted to assess the reasons for these trends.
In 2014, approximately 16% of French people reported skipping dental care due to cost, with disparities based on income level (Winkelmann et al. 2022). Before the reform, copayments for prosthetic care posed a major financial barrier, particularly for patients with limited VHI, due to the absence of price regulation. To address this, the reform for prosthetic coverage focused on capping prices and strengthening private VHI coverage. In France, VHI plays a significant role in health care financing, a trend reinforced by the reform; by 2022, VHI covered 45.1% of dental care fees (Unocam 2024). As a result, dental care remains one of the least publicly funded health services (Waitzberg et al. 2024).
The observed increase in prosthetic utilization following the reform does not necessarily indicate a reduction in the number of patients forgoing treatment due to financial constraints. While the number of patients receiving prosthetic treatments increased by 9% between 2019 and 2021, 92% of those treated in 2021 had already been patients between 2017 and 2020, suggesting that accessibility for individuals outside the health care system remained largely unchanged (Cour des comptes 2022). Additionally, limited information dissemination may have hindered vulnerable patients with poor health literacy from fully understanding the reform. Furthermore, an “anticipation effect” may have contributed to the rise in utilization, as some patients might have postponed prosthetic care until the reform took effect. This delay could have negatively affected their quality of life and masticatory function (Alpert 2016).
The 100% santé reform was introduced alongside a new plan aimed at low-income earners, known as CSS. While prosthetic prices for CSS patients were revised upward in November 2019, they remained below the capped prices set for non-CSS patients in January 2021. Consequently, utilization rates among CSS patients showed little change, whereas they increased for non-CSS patients. The higher average utilization among CSS beneficiaries can be attributed to income-based disparities in oral health, as individuals with higher socioeconomic status generally exhibit better oral health (Borg-Bartolo et al. 2022). Individuals without VHI did not benefit at all from the 100% santé. Likewise, it should be noted that the reform did not change much the level of coverage for low income patients with CSS. Thus, the reform might have exacerbated social inequalities and limited access to dental care for the most disadvantaged (Winkelmann et al. 2022). Although prosthetic prices for CSS and non-CSS patients are now gradually converging (by 2028), challenges remain for individuals without VHI.
The increase in dental care expenses since 2019 is often attributed to the reform, with expenditures reaching €15.5 billion in 2023, 46% of which was allocated to prosthetics. However, this trend could also be influenced by factors such as the rising incidence of noncommunicable diseases, population aging, and the impact of the COVID-19 pandemic (DREES 2024). To offset additional costs, the government decided in October 2023 to reduce SHI coverage for dental care from 70% to 60%. This policy reversal raises concerns about the sustainability of oral health care reforms, as inconsistent changes in coverage levels can disrupt consumption patterns and hinder access to dental care (Ranade et al. 2020).
Financial hardship is not the only barrier to dental care access; the availability of oral health care services also poses significant challenges, particularly for vulnerable populations. In 2021, the density of dentists in France was 62 per 100,000 inhabitants, with lower rates in underserved areas. Shortages in dental services were exacerbated by the COVID-19 pandemic, as dental care was interrupted in 2020, leading to cumulative delays in health care access from 2021 to 2022. Additionally, increased demand for prosthetics following the 100% santé reform further strained available resources (L’Assurance Maladie 2022). Robustness analyses in this study confirmed these COVID-19–related impacts, with trends varying by the inclusion of COVID-19 factors.
This study is not without limitations. A quasi-experimental design drawing from CITSA with a control outcome approach served to evaluate the impacts of the population-wide 100% santé reform. While utilization trends for primary vs control outcomes were compared in the sense of a “natural experiment,” this might not be considered equivalent to random assignment of persons to a treatment or control group. Utilization patterns between the compared outcomes were not following fully parallel trends in the preintervention period. Nevertheless, in the absence of better alternatives, the applied design can be considered the best possible identification strategy, especially since models gave consistent results (Lopez Bernal et al. 2019). Another limitation was the absence of data on oral health as SNDS compiles only claims information. Furthermore, the content of the SNDS database does not include dental treatments not covered by SHI funds or information about patients’ status for private VHI coverage. The postimplementation analysis period was short and did not allow exploring the long-term impact of the reform.
This study highlighted the significant impact of the reform on the utilization of full dentures, linked to a potential improvement in their affordability for patients with VHIs. However, it remains difficult to determine whether this trend reflects a catch-up effect for patients already well integrated into the health care system or whether the reform has enabled new patients to access previously unaffordable care.
Author Contributions
S. Tubert-Jeannin, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; L. Bénézet, contributed to design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; A. Mulliez, contributed to design, contributed to analysis, drafted manuscript, critically revised manuscript; S. Listl, contributed to conception, contributed to interpretation, drafted manuscript, critically revised manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345251364167 – Supplemental material for The French 100% Santé Reform: Impacts on Dental Care Utilization
Supplemental material, sj-docx-1-jdr-10.1177_00220345251364167 for The French 100% Santé Reform: Impacts on Dental Care Utilization by S. Tubert-Jeannin, L. Bénézet, A. Mulliez and S. Listl in Journal of Dental Research
Footnotes
Acknowledgements
The authors thank the Clinical Research and Innovation Direction team from the Clermont-Ferrand Hospital, which provided the support for access to the SNDS database, as well as Caroline Eschevins for helping in formatting the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has received funding from the European Union’s Horizon Europe research and innovation program under grant agreement 101094366: ![]() . The funder of the study had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
. The funder of the study had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.