
Abstract
Clinicians have recommended, with no scientific evidence, increasing the application times of 38% silver diamine fluoride (SDF) to foster caries arrest. The current study determined the rate of carious lesion activity in response to topical 38% SDF with increasing treatment application time. A 6-mo, stratified-randomized, double-blind, active-controlled, parallel-group trial compared 9 treatment arms. The primary outcome was carious lesion activity at the tooth-surface level 6 mo after initial treatment. Participants included 665 children aged 3 to 4 y with 2,106 carious teeth (234 teeth/group) with 3,024 active carious tooth surfaces. The carious teeth were block randomized into 9 groups with SDF application times of 3, 5, 10, 15, 30, 45, 60, 120, and 180 s. The dose (SDF application time) and response (proportion of active carious tooth surfaces becoming arrested) were modeled using multiple dose-response models. At the 6-mo examination, 642 children with 2,038 SDF-treated carious teeth and 2,939 SDF-treated carious tooth surfaces were evaluated. The estimated proportion of inactive (arrested) lesions (%) increased over time from 75% at 4 s, to 80% at 16 s, and 84% at 60 s. Among the multiple dose-response models, the Emax model provided the best fit. The estimated rate of the proportion of arrested lesions (%s−1) reduced over time from 0.1%s−1 at 30 s to 0.05%s−1 at 43 s. An estimated 16-s application time was required to arrest 80% of caries lesions. The proportion of arrested lesions was associated with lesion-surface type (single/multiple) and tooth location (anterior/posterior). A 16-s application time was estimated to arrest 88% of single tooth-surface lesions in anterior teeth, compared with 66% of multiple tooth-surface lesions in posterior teeth. In conclusion, the trial found an increase in the proportion of arrested lesions with increasing SDF application time, although the rate of the proportion of arrested lesions decreased over application time. (ClinicalTrials.gov NCT04655430)
Introduction
The World Health Organization (WHO; 2022) recognizes the effectiveness of silver diamine fluoride (SDF) for caries control and recommends its use for primary teeth, permanent teeth, and root surfaces affected by dental caries. The SDF does not require the removal of carious tissue, making it a medically appropriate treatment option for all patients (Crystal and Niederman 2019). The WHO Collaborating Centre for Quality Improvement and Evidence-Based Dentistry proposed SDF as the first choice for carious lesion management during and emerging from the pandemic (Benzian and Niederman 2020).
Based on expert opinion, clinical investigators at the University of California, San Francisco (UCSF) published the widely cited UCSF Protocol for caries arrest using SDF (Horst et al. 2016). The protocol suggested isolating and drying the teeth to be treated and then allowing the applied SDF to absorb up to 60 s before rinsing with water. Rinsing was suggested to reduce the amount of SDF swallowed and thus increase safety. However, manufacturers and clinicians have recommended different clinical protocols (Yan et al. 2022a), suggesting an application time ranging from 10 to 240 s without scientific evidence (Yan et al. 2022b).
Clinicians generally consider a longer contact time with 38% SDF before washing with water favors arresting carious lesions. However, a prolonged application time makes it more difficult to maintain moisture control. Thus, a shorter application time is preferred, especially because SDF is commonly used on the teeth of young children who may have difficulty cooperating (Yan et al. 2022a). Often, multiple teeth are affected by carious lesions, which makes isolation and SDF application even more challenging. Therefore, the objective of the current clinical trial was to study the dental carious lesion activity response to topical application of 38% SDF solution with increasing treatment application time.
Methods
The Consolidated Standards of Reporting Trials (CONSORT) 2010 checklist was followed to report the current trial (Schulz et al. 2010). Figure 1 shows the study flow chart.
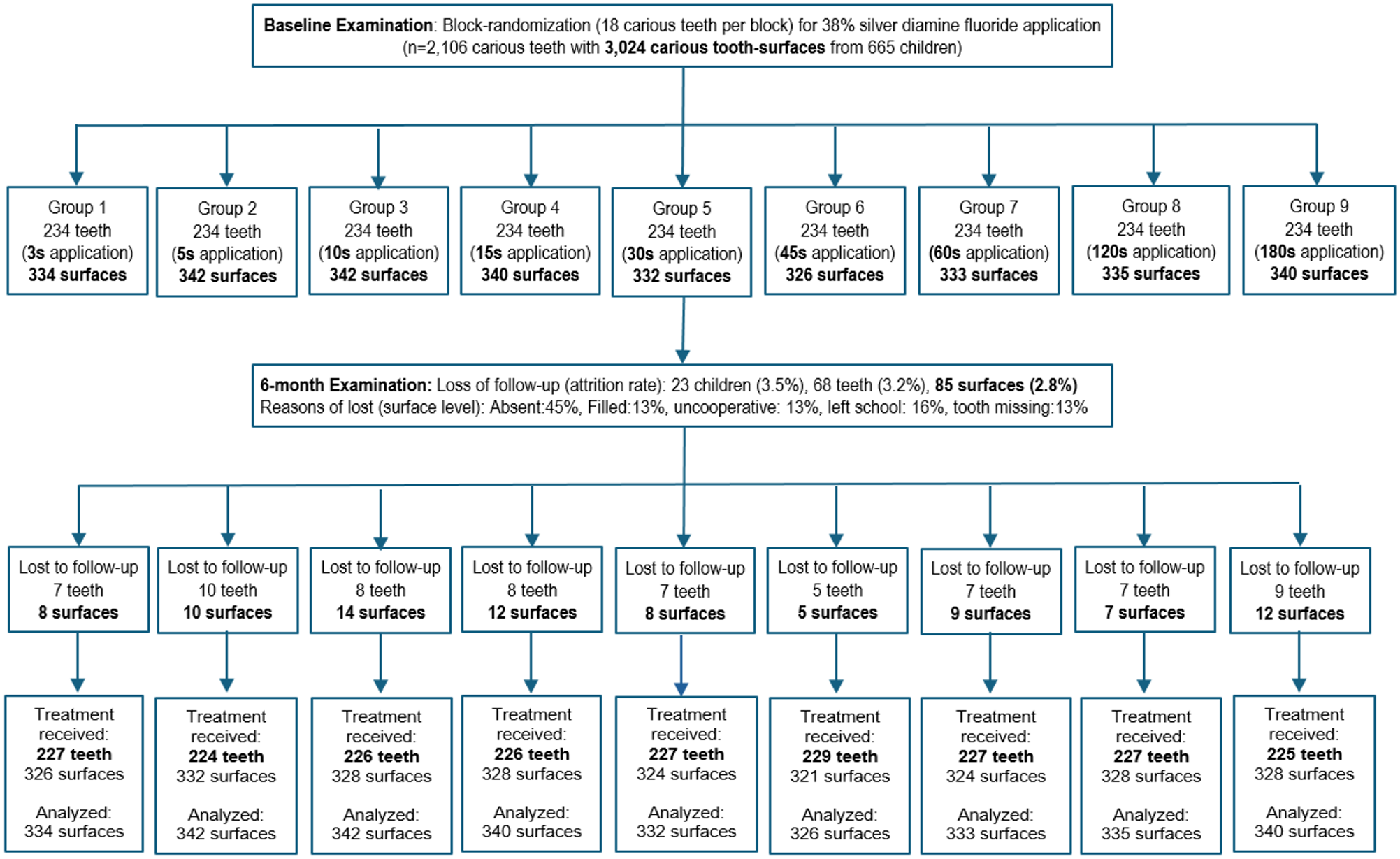
Flow chart of application time of 38% silver diamine fluoride (SDF) solution on arrested caries (intention-to-treat analysis).
Trial Design
This is a stratified-randomized, double-blind, active-controlled, parallel-group clinical trial with 1:1 allocation in 9 arms. Ethics approval was obtained from the local Institutional Review Board (IRB UW 20-737), and the trial was registered in ClinicalTrials.gov (NCT04655430). The trial protocol was published in an open-access peer-reviewed journal (Yan et al. 2022a).
Participants, Settings, and Location
Children who met the following criteria were recruited: (1) aged 3 to 4 y and attending kindergarten, (b) generally healthy by parental report, (c) had a parental consent, and (d) had at least 1 untreated cavitated active carious lesion extending into the dentin. Children who were uncooperative or who were on long-term medication were excluded. The setting was the kindergarten classroom. The first child was enrolled on October 1, 2021, and the last child was evaluated on July 31, 2022.
Questionnaire Survey
A validated Chinese- and English-language parental questionnaire was used (Yan et al. 2022a) at baseline to collect data on demographic information (sex, age, and family income) and the child’s health-related habits to describe the children and adjust for an imbalance in the randomization. The information collected included toothbrushing frequency, supervised (parent-assisted) toothbrushing, current bottle feeding, and daily snacking frequency.
Clinical Examination
One trained examiner performed the baseline and 6-mo examinations to evaluate caries experience using the dmft (decayed, missing, and filled teeth) and dmfs (decayed, missing, and filled tooth-surfaces) indices. Oral hygiene status was determined using the simplified version of the Visible Plaque Index (VPI) (Ainamo and Bay 1975). In carrying out the VPI, the examiner determined the presence of visible plaque (yes = 1, no = 0) on the buccal and lingual surfaces of 6 indexed teeth (55, 53, 51, 75, 73, and 71). The VPI score = (total score/12) × 100%. The VPI score can range from 0 (no visible plaque on all 12 tooth surfaces) to 100% (visible plaque on all 12 tooth surfaces).
Carious lesion activity was recorded as active or inactive (arrested) (Chu et al. 2002).The examiner used a WHO-standardized 0.5-mm ball-end probe with approximately 20 g of force to assess caries activity. Active caries was recorded when softness was detected in the carious dentin lesions of primary teeth (Chu et al. 2002). Arrested caries was recorded if the lesion was hard upon probing (Chu et al. 2002). The center of the carious lesion was probed. For larger lesions involving 2 or 3 surfaces, 2 or 3 test points were assessed to evaluate caries activity. The lesion was considered active if softness was detected on at least 1 of the test points. The examiner (Yan) completed 8 h of training including 30 calibration cases (κ > 0.8), supervised by the corresponding author (Chu).The examiner reexamined 10% of the children at each stage of the clinical trial to evaluate intraexaminer agreement on the VPI, dmfs score, and lesion activity. The kappa values for the baseline intraexaminer agreement on the VPI, dmfs score, and lesion activity were 0.84, 0.91, and 0.92, respectively. The kappa value for the 6-mo intraexaminer agreement on the lesion activity was 0.92.
Interventions
The 9 treatment arms were defined by SDF application times: 3, 5, 10, 15, 30, 45, 60, 120, and 180 s, as recommended by different clinicians (Yan et al. 2022b). One manufacturer recommended an application time of 240 s. However, 4 min was considered too long for young children to remain cooperative. An operator applied the 38% SDF solution (Advantage Arrest Silver Diamine Fluoride 38%, Lot No. 21109, Elevate Oral Care) with a microbrush (regular microbrush, Elevate Oral Care) with a applicator’s tip diameter of 2.5 mm. SDF was applied to the lesion using 3 agitation cycles then left on for the assigned application time. Each carious lesion received 1 application. A laboratory study found an application delivered a mean of 4.23 ± 0.69 mL SDF solution (Yan et al. 2022c).
Outcomes
The outcome measure was carious lesion activity (active/inactive) at the tooth-surface level 6 mo after initial treatment. This 6-mo time frame allowed a clinician to administer a second dose if necessary.
Posttreatment Instruction
An assistant provided a report on the child’s oral health status to the parents.
Concomitant Treatment
Children could attend dentists for dental care during the 6-mo study. All SDF-treated teeth that received a restoration were considered active carious lesion (failed to arrest) during follow-up.
Harms
The children’s parents were provided a 24-h mobile contact number to call if there were any problems or questions.
Randomization and Treatment Allocation
The children were examined and stratified by high or low caries severity and then allocated to 9 treatment groups by strata using a randomization method with a block size of 18. Children were categorized as having a high caries rate if they had more than 3 untreated carious tooth surfaces or a low caries rate if they had no more than 3 untreated carious tooth surfaces (Chou et al. 2021).
Allocation Concealment and Implementation
A statistician generated the randomization sequence. The random number sequence was maintained in opaque sealed envelopes to conceal the allocation sequence until the interventions were assigned. An assistant conducted the group allocation.
Blinding
The examiner and the child were blinded to the treatment group allocation. Another operator applied the 38% SDF solution after the examination.
Quality Control of Data Entry
A data management plan and a statistical analysis plan were developed for the current trial (Yan et al. 2022a). To minimize data entry errors, 2 assistants entered and compared the data. The investigators assessed intraexaminer agreement regarding caries diagnoses and the VPI at each time point using Cohen’s kappa statistics. They also performed continuous monitoring to ensure adherence to data entry protocols.
Sample Size and Power Calculation
The estimated sample size was based on a caries arrest rate of 70% (Gao et al. 2020) for a 60-s application time. A caries arrest rate of 65.3% for a 3-s application was used, and a monotonically increasing trend was assumed, reaching an 80% caries arrest rate for a 180-s application. To detect a proportional trend with 90% power and a 2-sided type I (α) error set at 0.05 required 104 SDF-treated carious tooth surfaces per group.
The mean number of carious tooth surfaces per child was estimated to be 4.75 and the mean number of carious teeth per child to be 3.69 at baseline (Fung et al. 2018). The anticipated intraclass correlation coefficient was 0.23 (Fung et al. 2018). The current trial needed 195 carious tooth surfaces from 152 teeth per group, calculated using the equation for a multilevel study (Twisk 2006).
The current trial was performed during the COVID-19 pandemic. Considering an anticipated dropout rate of 25% and a noncompliance rate of 10% due to the pandemic, at least 226 carious teeth per group for SDF application at baseline were needed. Stratified randomization with a block size of 18 was used to assign carious teeth for the 9 intervention groups. At baseline, 234 carious teeth per group (13 blocks) were recruited to achieve the required number of tooth surfaces for analysis at the tooth-surface level.
Statistical Analysis
Statistical analyses using IBM SPSS Statistics for Windows, version 28 (IBM Corp.), R-4.4.0 for Windows (The R Foundation SAS Institute), and R Studio were performed (Posit, PBC). An intention-to-treat analysis was used, with missing outcome data imputed as the worst-case scenario to handle missing data. Group comparison in baseline information at the tooth level was performed by generalized estimating equations (GEE) models adjusted for clustering effects.
For the primary analysis of caries arrest at 6 mo, the Multiple Comparison Procedure-Modeling (MCP-Mod) methodology was used (Pinheiro et al. 2014). In addition, the GEE model was used to compute the mean and variance–covariance matrix for each dose. To preserve the familywise error rate at a 1-sided significance level of 2.5%, the optimal contrasts derived from the prespecified model candidate set for each dosing regimen were individually compared with the critical value derived using a multiplicity adjustment. The model candidate set included Emax (maximal effect at high drug concentrations), sigmoid Emax, linear, lin-log (linear-logarithmic), and exponential models. This adjustment accounted for all tests comparing doses (SDF application times) across all regimens simultaneously.
The models were initially based on the estimated results of the different SDF application time groups (as a categorical variable) from GEE models, adjusted for intraclass correlation since multiple lesions could be found in a single child. The GEE model was used to adjust for the effect of correlation due to multiple lesions in a child. Confounding variables with a P value less than 0.05 in the bivariate GEE model were included in the base model. The corrected quasi-likelihood information criterion (QICC) of all potential subset models was compared. The multivariable GEE model containing all statistically significant variables with the smallest QICC was selected as the best-fit model. The significance level for all tests was set at 0.05.
Results
Baseline
The current clinical trial included in total 3,024 carious tooth surfaces on 2,106 teeth among 665 children aged 3 to 4 y (350 boys) at baseline (Fig. 1). Their dmft score (mean ± standard deviation) was 5.7 ± 3.5 teeth, and the dt score was 5.6 ± 3.5 teeth. The dmfs score was 9.0 ± 7.4 tooth surfaces, and the ds score was 8.8 ± 7.0 tooth surfaces. The VPI score was 34% ± 16%, with visible plaque found on 96% of the carious tooth surfaces. There were no significant differences in the children’s demographic background, oral health–related behavior, or clinical characteristics among the treatment arms (Table 1a).
(a) Baseline Variables and Silver Diamine Fluoride (SDF) Application Time. a
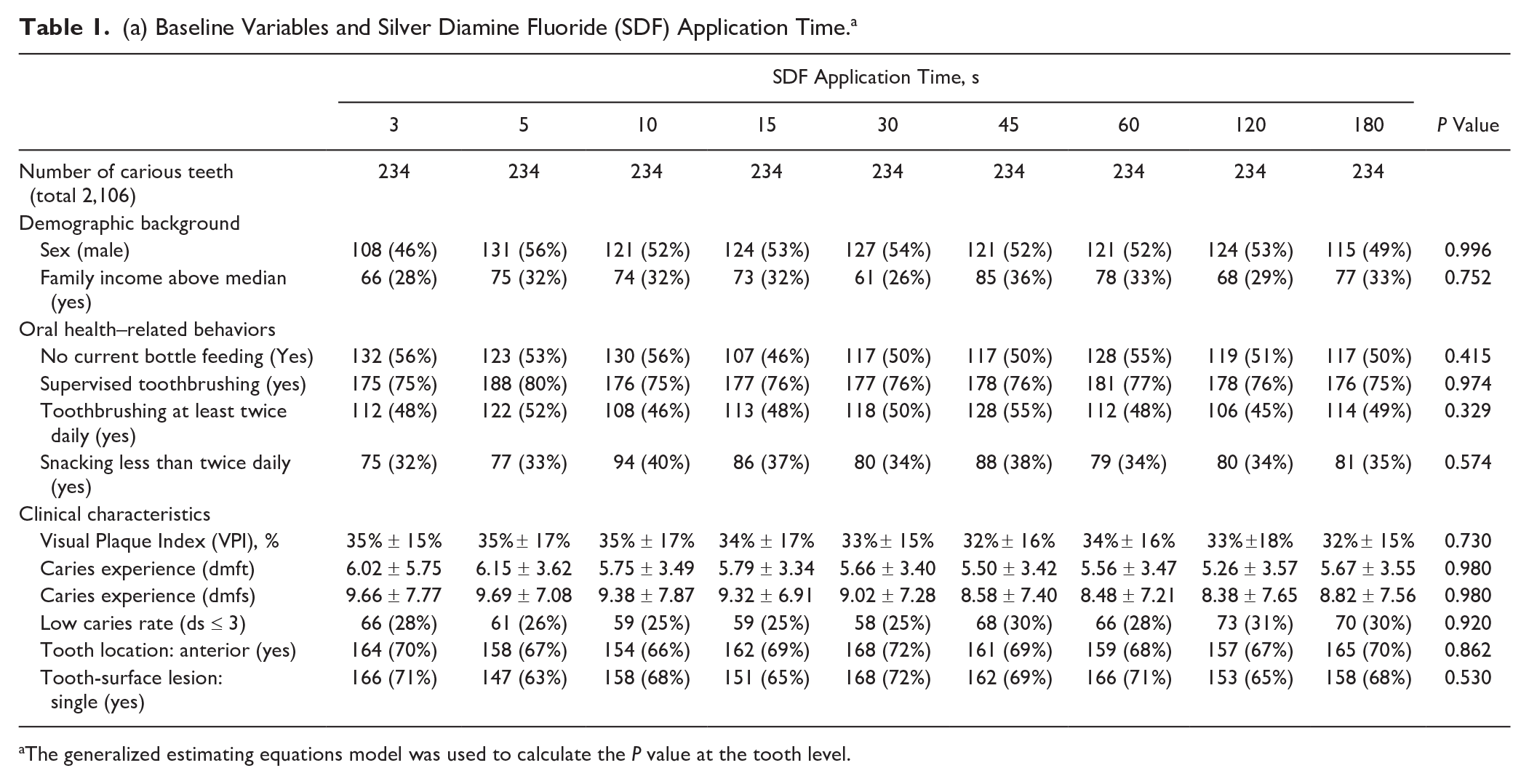
The generalized estimating equations model was used to calculate the P value at the tooth level.
(b) Baseline Variables and Unadjusted Odds Ratio for Arresting Caries. a
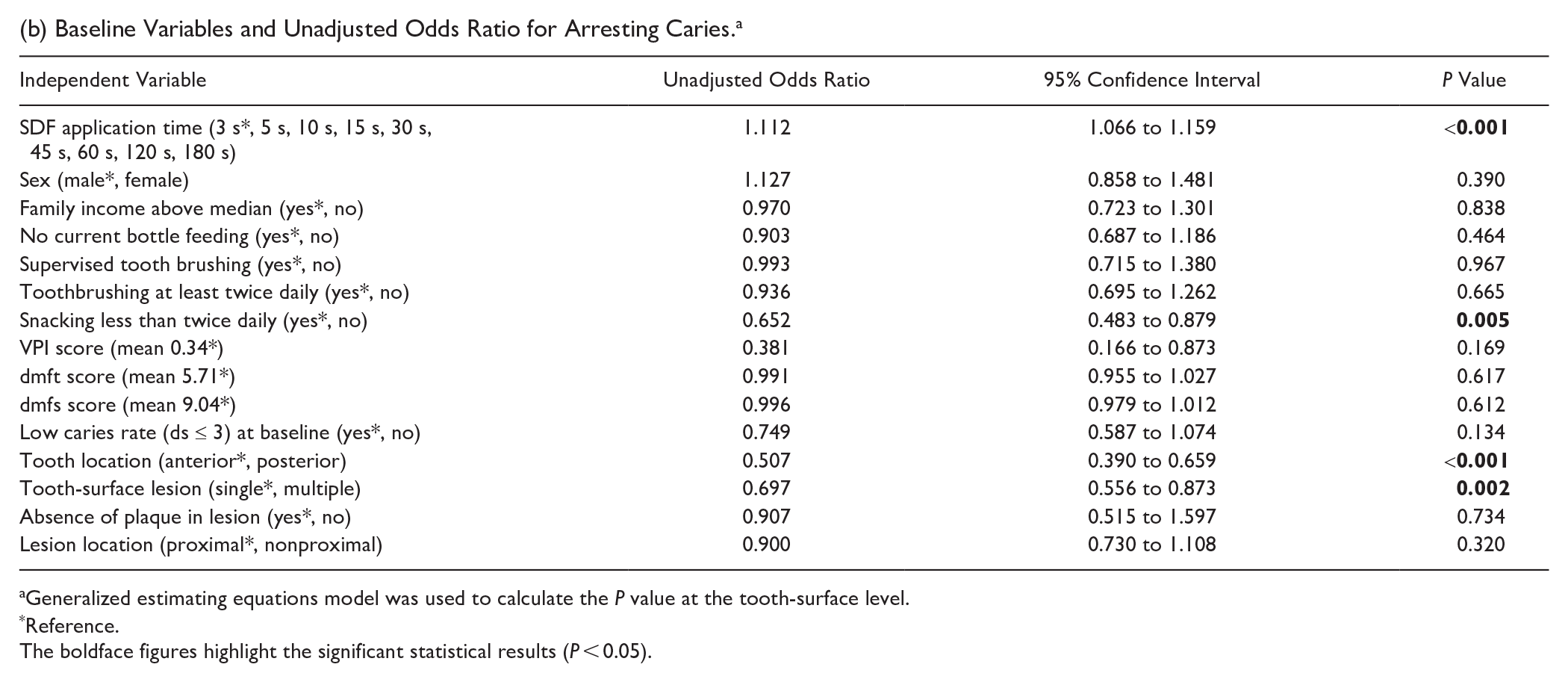
Generalized estimating equations model was used to calculate the P value at the tooth-surface level.
Reference.
The boldface figures highlight the significant statistical results (P < 0.05).
6-mo Follow-up
At the 6-mo follow-up, 2,939 carious tooth-surfaces on 2,038 carious teeth from 642 children were examined. The loss to follow-up rate was 3.5% (23/665) at the child level, 3.2% (68/2,106) at the tooth level, and 2.8% (85/3,024) at the tooth-surface level (Fig. 1). The mean dmft score was 6.3 ± 3.7 teeth, and the mean dt score was 6.1 ± 3.7 teeth. The mean dmfs score was 10.7 ± 8.4 surfaces, and the mean ds score was 10.4 ± 8.0 surfaces. The mean VPI score was 28% ± 16%, with visible plaque found on 98% of all the SDF-treated carious tooth surfaces.
Harms
No harms were observed or reported by the parents in the current study.
Effectiveness of SDF in Arresting Caries
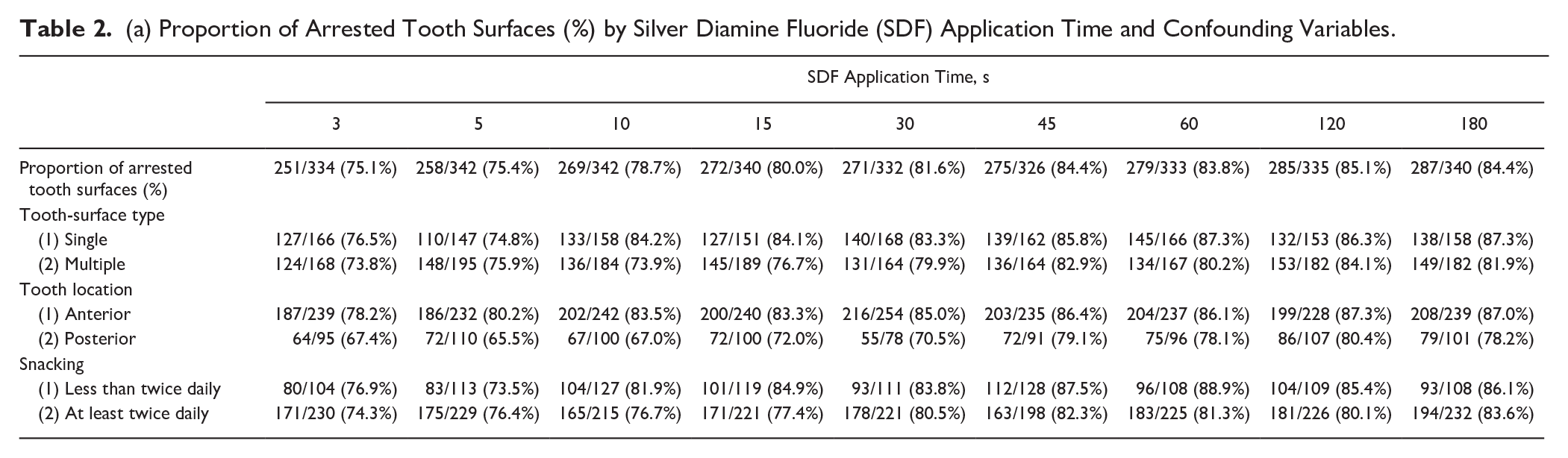
Table 2 summarizes the proportion of arrested tooth surfaces (%) by SDF application time and the GEE model of confounding variables. After intention-to-treat analysis with missing values imputation by the worst-case scenario, the proportion in each group was lower by 1.9% to 3.3%, with the range of the proportion of arrested tooth surfaces decreasing from 77.0%–87.5% to 75.1%–85.1%.
(a) Proportion of Arrested Tooth Surfaces (%) by Silver Diamine Fluoride (SDF) Application Time and Confounding Variables.
(b) Adjusted Odds Ratio for Caries Arrest by 38% SDF Application Time and Confounding Variables. a
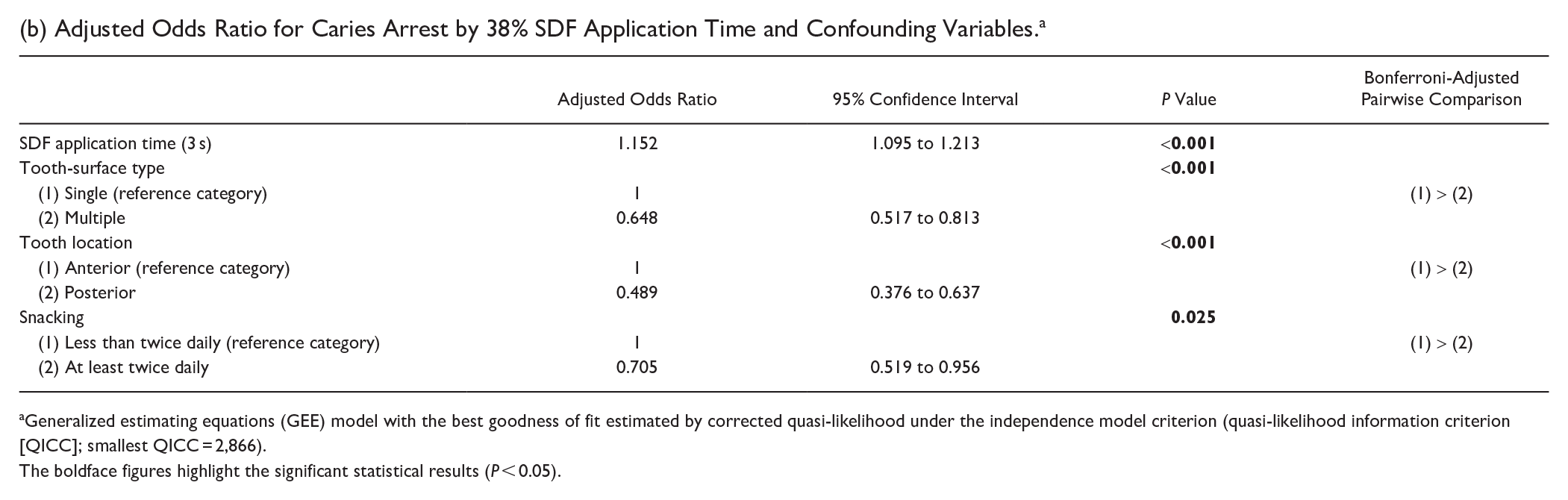
Generalized estimating equations (GEE) model with the best goodness of fit estimated by corrected quasi-likelihood under the independence model criterion (quasi-likelihood information criterion [QICC]; smallest QICC = 2,866).
The boldface figures highlight the significant statistical results (P < 0.05).
Potential Modifying Variables for SDF Application Time on Proportion of Arrested Lesions
Modifying potential confounding variables that could affect the proportion of arrested tooth surfaces due to the application time were identified. The GEE model results found the proportion of arrested tooth surfaces was associated with snacking habits, tooth location (anterior or posterior), tooth-surface lesion (single surface or multiple surfaces), and SDF application time (Table 1b). The multivariable GEE model with the smallest QICC (2,866) revealed that a higher proportion of arrested lesions was found on single tooth-surface lesions and on anterior teeth in children who snacked less than twice daily, compared with those with multiple tooth-surface lesions on posterior teeth in children who snacked at least twice daily (Table 2b).
Model Prediction: SDF Application Time on the Proportion of Arrested Lesions
An MCP-Mod was used to predict the 6-mo caries-arrest proportion at the tooth-surface level for the 9 treatment groups based on the results of the multivariable GEE model analysis (Table 2a). All candidate models for testing the dose-response signal were statistically significant (adjusted P < 0.001), with the Emax model being the best fit. The Emax model curve is well aligned with the GEE model-predicted curve for the effect of SDF application time on the proportion of arrested lesions.
Examining the proportion of arrested lesions with reference to SDF application time in the random effect term, the predicted proportion of arrested lesions ranged from 74.9% (3 s) to 84.8% (180 s) (Table 3). The Emax dose-response curve (application time on proportion of arrested lesions) demonstrated that the proportion of arrested lesions increased by more than 0.1% per second from 3 to 30 s of SDF application time. After 89 s, the caries-arrest rates exhibited an increase of less than 0.01% per second in the proportion of caries arrest.
Predicted Proportion of Arrested Lesions (%) and Application Time of 38% Silver Diamine Fluoride (SDF) Solution.
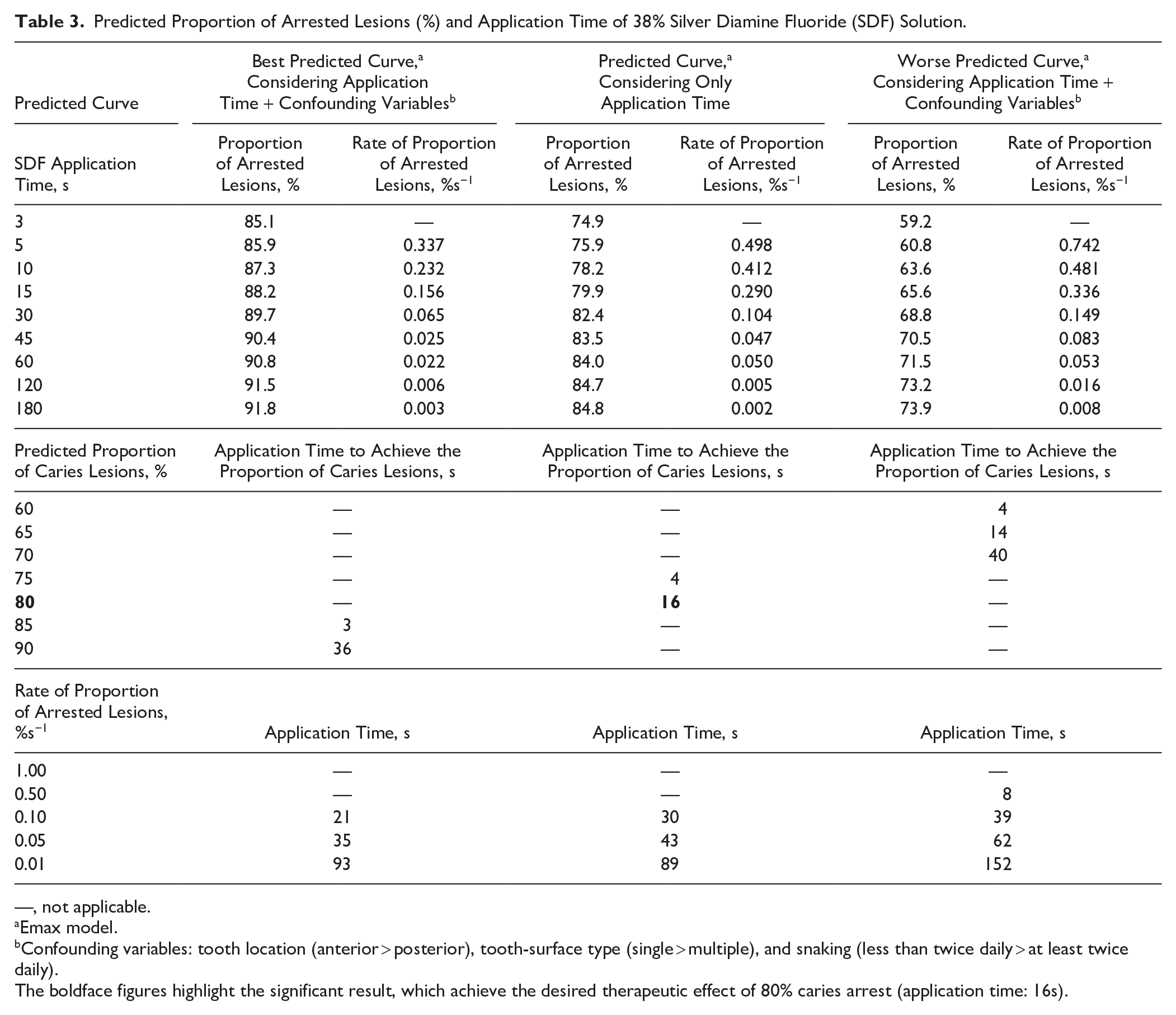
—, not applicable.
Emax model.
Confounding variables: tooth location (anterior > posterior), tooth-surface type (single > multiple), and snaking (less than twice daily > at least twice daily).
The boldface figures highlight the significant result, which achieve the desired therapeutic effect of 80% caries arrest (application time: 16s).
Figure 2 shows the predicted proportion of the arrested lesion curves for SDF application times ranging from 3 to 180 s. The SDF therapy was expected to result in a higher proportion of arrested lesions in single tooth-surface lesions or anterior teeth (85.1% to 91.8%) compared with multi-tooth-surface lesions or posterior teeth (59.2% to 73.9%). In addition, it was anticipated to be more effective in children who snacked less than twice daily (Table 3).
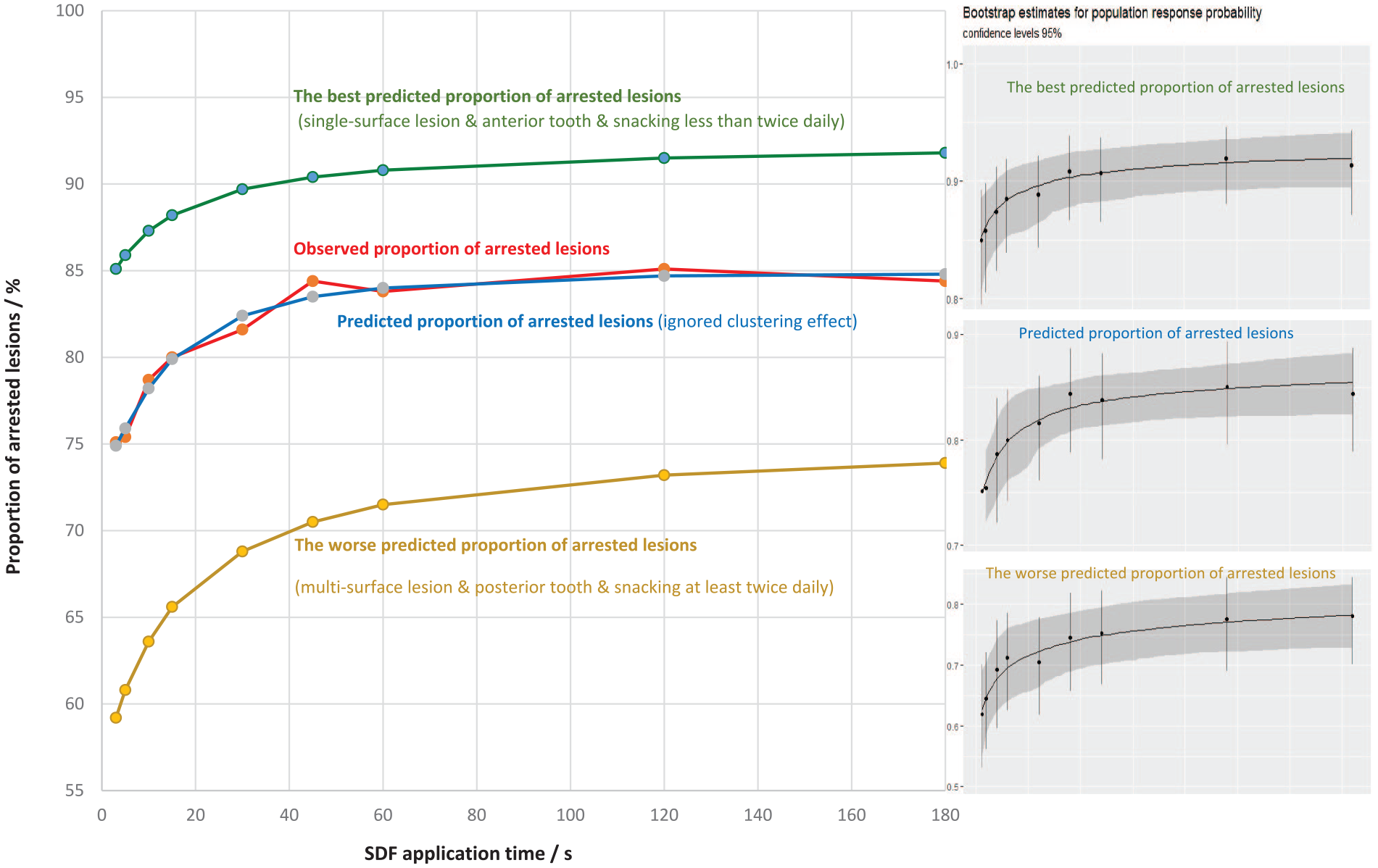
Predicted and observed proportion of arrested lesion curves of 38% silver diamine fluoride (SDF) solution from 3 to 180 s.
Discussion
A randomized clinical trial was conducted to determine the carious lesion activity response to SDF therapy with increasing treatment application times. The trial found a nonlinear relationship between the application time of 38% SDF solution and caries arrest. The results revealed an increase in the proportion of arrested lesions with increasing SDF application time, although the rate of increase decreased and eventually plateaued. Specifically, the observed proportion of arrested lesions was 75% with a 4-s application time, increasing to 80% with a 16-s application time. This additional 12 s of application time provided an additional 5% caries arrest proportion.
Clemens et al. (2018) studied 102 cavities in 32 children, aiming to apply SDF for 120 s per lesion. However, because some children did not cooperate fully, the application times varied. For 9 cavities, the application time was only 30 s, while for 36 cavities, it was the full 120 s. This variation made it difficult to determine if the length of SDF application duration affected caries arrest. A later study by Thakur et al. (2022) faced similar issues. They applied SDF for 30 s, 60 s, or 120 s to 154 carious lesions in 49 children. However, this sample size remained insufficient to draw definitive conclusions regarding the effect of SDF application duration on caries arrest.
In the present study, untreated caries were identified as a caries risk factor because more than 90% of Hong Kong preschool students with caries remain untreated (Zheng et al. 2021). However, we acknowledge that relying solely on cavitated lesions as an indicator of caries risk is a limitation of this study. The rate of increase in the proportion of caries arrest decreased over time and was estimated to be less than 0.05% per second after a 43-s application time, suggesting a clinically insignificant increase in caries arrest with prolonged application time. A laboratory study also found no significant difference in enamel remineralization with 60-s and 180-s application times (Punhagui et al. 2021). No laboratory studies reported on dentine caries. In the current clinical trial, a 16-s application time (minimum effective dose) was estimated to achieve the desired therapeutic effect of 80% caries arrest. The study design allows us to understand how different SDF application times (doses) affect caries arrest (responses). The efficacy of SDF was studied by observing and measuring the effect of SDF application time on caries arrest. In addition, the present study may provide insights for future research to explore the biological mechanisms of how SDF works and its interaction with carious lesions. While most child patients can tolerate a 4-s application time, clinicians should consider extending the application time to 16 s to optimize caries management. The current study provides data to develop appropriate dosing regimens for young children. It offers valuable information for clinicians to make informed decisions regarding the application time of 38% SDF solution in their clinical care.
The present study’s strengths include a large sample size, high retention rate, and good intraexaminer reliability. The study design allows for causal inferences, provides evidence of a treatment’s efficacy, and minimizes bias. An intention-to-treat analysis was performed with missing outcome data imputed as the worst-case scenario, which serves as an appropriate analysis to best align with our study objectives. The children might have received fillings from other dentists to restore caries. However, the number of these fillings was very small. As a result, any interaction effect from concurrent treatments was insignificant.
The parents and children were instructed to avoid eating or drinking for 30 min after treatment, but the children were not observed, and such recommendations are not always followed. However, our previous trial found no statistically significant difference in caries arrest between children who rinsed immediately and those who rinsed 30 min after SDF therapy (Sun et al. 2024). There is also a possibility of model overfitting, which can result in overly optimistic predictions of success rates that may not hold true in practice. Nevertheless, the MCP-Mod is not a complex model and is unlikely to overfit the data.
Conclusion
In the current randomized controlled trial, an increase in the proportion of lesions arrested with an increasing treatment application time of 38% SDF was determined. A 16-s SDF application time was required to achieve an 80% arrest of lesions. The increment rate of the proportion of lesions arrested reduced after 43 s. A higher proportion of lesions arrested is expected if SDF is applied to single tooth-surface lesions on anterior teeth in children. The current study aids clinicians in making informed decisions in their clinical care.
Author Contributions
I.G. Yan, data acquisition and analysis, drafted and critically revised the manuscript; F.M. Zheng, D. Duangthip, data analysis and interpretation, critically revised the manuscript; I.G. Sun, data acquisition, critically revised the manuscript; E.C.M. Lo, C.H. Chu, contributed to conception and design, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors thank Samantha K. Y. Li for her statistical advice. They also thank the kindergarten teachers, children, and parents for their support in the current study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received support from the Research Grant Council General Research Fund (17100421).