
Abstract
Numerous studies have shown that education correlates with tooth loss and dental services use, but whether expanding educational opportunities would reduce tooth loss and improve dental attendance remains unclear given that prior studies lacked a study design to assess causality. We leveraged a policy reform, raising the school leaving age, as an instrumental variable (IV) to estimate the effect of education on edentulism and dental visits in the United States using the repeated cross-sectional data from the Behavioral Risk Factor Surveillance System (BRFSS; N = 463,878). We additionally examined the effect of education on dental visits using longitudinal data from the Survey of Health, Aging and Retirement in Europe (SHARE; N = 69,929). Applying IV probit models, we found 1 extra year of schooling reduced edentulism likelihood by 2.9 percentage points (95% confidence interval [CI]: −0.041; −0.017) and increased dental visit likelihood by 1.2 percentage points (95% CI: 0.01; 0.024) in the United States, with similar effects on dental visits in Europe. Estimates were robust to different model specifications and plausible amounts of imperfect exogeneity. Negative control analysis supported the validity of our findings. This study provides consistent evidence that extended schooling reduces edentulism risk and increases regular dental attendance.
Keywords
Introduction
Education strongly correlates with health outcomes in Western countries, with less educated individuals experiencing higher morbidity and mortality rates (Mackenbach et al. 2016). The putative causal effect of education on morbidity and mortality has been corroborated by twin, quasi-experimental, and experimental studies (Bann et al. 2024). However, the link between education and oral health, including how often people visit the dentist, is less clear. Tooth loss and untreated dental diseases contribute significantly to the occurrence and progression of chronic diseases and have been associated with physical frailty and poor health-related quality of life among older people (Matsuyama et al. 2023; Allen and Tsakos 2024). Behaviors such as managing sugar intake and avoiding smoking, which are more common among those with higher education, are crucial factors in preventing dental caries and periodontitis, the main causes of tooth loss. Hence, education seems to play a role in preventing these diseases. Educated people tend to have more teeth and attend dental care more regularly for checkups and dental treatments, but it is unclear whether raising education would induce changes in oral health and dental service use (Elani et al. 2017; Reda et al. 2018).
Observational studies on education’s impact on oral health and dental service use are often limited by confounding and selection bias. Quasi-experiments, such as policies to raise the school leaving age, can serve as potential instrumental variables (IVs) for educational attainment (Bann et al. 2024). Several studies have exploited changes in the legally mandated years of schooling as an IV for the effect of education on health (Lleras-Muney 2005; Stephens and Yang 2014; Yue et al. 2023; Bann et al. 2024). Taking the United States as an example, although all states had compulsory schooling laws in place by 1918, states varied substantially with respect to the number of years required, and states changed their schooling laws repeatedly (Lleras-Muney 2005). As a result, some older U.S. residents were born in states that required only a few years in school before a child could drop out or obtain work permits. Schooling law changes allocated people a longer education based on an arbitrary threshold (year of birth). Such analysis compares educational attainment and health outcomes of adjacent cohorts just affected and not affected by changes in the schooling laws. The IV-based approach to estimate causal effects is compelling because there are many unmeasured confounders of the relationship between education and oral health. Identifying, measuring, and adjusting for these confounders is challenging. In contrast, the IV approach does not require correct specification of the exposure–outcome association but relies on an IV that affects the outcome only through the exposure and shares no confounders with the outcome. An IV design takes advantage of the quasi-randomness that occurs in exposure assignment to help address imbalances in confounders (Bann et al. 2024). It assumes that, conditional on covariates, changes in schooling laws are independent of other variables influencing oral health and dental services use. In the present study, we apply IV models using the population-based Behavioral Risk Factor Surveillance Survey (BRFSS) to estimate the effects of schooling on tooth loss and dental services use in the United States. The Survey of Health and Retirement in Europe (SHARE) is used to examine the effect of education on dental visits across 25 European countries.
Methods
Study Design
The BRFSS is a state-based cross-sectional survey covering all 50 U.S. states, the District of Columbia, and 3 U.S. territories. For this study, we used BRFSS data from 1995 to 2006, 2008, 2010, and 2012, focusing on tooth loss and dental service use. The analysis was restricted to participants born between 1896 and 1950 due to available data on compulsory schooling laws. Since these laws primarily affect lower-educated individuals (Fletcher 2015; Yue et al. 2023), we limited the sample to those with a high school diploma or less, resulting in a pooled sample of 463,878 participants (Table 1). SHARE is a cross-national cohort study of adults aged 50+ y across 29 countries, conducted biannually since 2004 (8 waves). We restricted our sample to participants born between 1901 and 1979 in 1 of 25 countries with available schooling law data, excluding foreign-born individuals. All education levels were included, creating a panel dataset of 124,687 observations from 69,929 individuals across up to 8 waves (Table 2). In addition, descriptive statistics for SHARE wave 1 and 2 participants (N = 14,471) reporting on curative and preventive dental visits are in Appendix Table 1. All studies received ethics approval, and informed consent was obtained from participants.
Descriptive Statistics of the Behavioral Risk Factor Surveillance Surveys.

Entries are mean (standard deviation) for continuous variable and number of observations (%) for categorical variables.
Descriptive Statistics of Survey of Health, Aging and Retirement in Europe.

Entries are mean (standard deviation) for continuous variable and number of observations (%) for categorical variables.
Study Variables
The BRFSS included questions on tooth loss due to decay and gum disease, categorized as none, 1 to 5, 6+ but not all, or all. We derived 2 binary outcomes: edentulism (complete tooth loss) and loss of 6+ teeth, following the Centers for Disease Control and Prevention (CDC) Oral Health Indicators. Both BRFSS and SHARE assessed dental visits within the past year, with SHARE waves 1 and 2 distinguishing between treatment and prevention visits. Educational attainment was quantified as years of schooling. We used datasets from 48 U.S. states (excluding Alaska, Hawaii, and Washington, DC) and followed the approach of previous studies to construct IVs based on school attendance and labor laws at age 14 y (Lleras-Muney 2005; Stephens and Yang 2014). Hofmarcher (2021) constructed a history of compulsory schooling laws for 25 European countries included in SHARE. We computed years of required schooling and used dummy variables (≥7, ≥8, ≥9, ≥10 y) to capture nonlinear effects (Yue et al. 2023). Covariates included sex, age, birth year category interacted with state/country fixed effects, and additional controls specific to each dataset (race/ethnicity for BRFSS, father’s education for SHARE). Potential mediators such as income, dental insurance, and health behaviors were not adjusted for to avoid bias in effect estimates.
Statistical Analyses
We used an IV probit model to estimate the effect of educational attainment on tooth loss and dental visits. The endogenous exposure years of schooling were regressed on the IVs and other exogenous covariates (including birth year × country fixed effects), and fitted exposure values were entered into a second-stage probit model for tooth loss and dental visits (Wooldridge 2010). Risk differences were derived from model-adjusted predicted average probabilities. Control function IV Poisson models provided relative risks (Wooldridge 2015). Standard errors were clustered at the state/country-by-birth cohort level. IV isolates the variation in the exposure caused by the instrument and uses only this variation to estimate the causal effect. The IV strategy relies on 3 conditions (Fig.): relevance (schooling laws affect education), testable by the first-stage F statistic; (2) conditional exchangeability (no uncontrolled IV-outcome confounding); and (3) exclusion restriction (the IV affects outcomes only through schooling). Only relevance is empirically testable, while exchangeability and exclusion restriction can be supported by sensitivity analyses. In our first sensitivity analysis, we examined robustness to uncontrolled confounders (conditional exchangeability) using a partial identification strategy (Nevo and Rosen 2012), bounding the 2-stage least-squares estimate under 2 assumptions regarding correlations between the exposure, IV, and residual error. Second, we assessed exclusion restriction using a negative control population approach (Davies et al. 2017), applying IV probit models to a BRFSS subsample of college graduates. To address potential survivor bias in SHARE, we weighted IV models using stabilized inverse probability of attrition weights (Weuve et al. 2012). Reporting followed STROBE (STrengthening the Reporting of OBservational studies in Epidemiology).
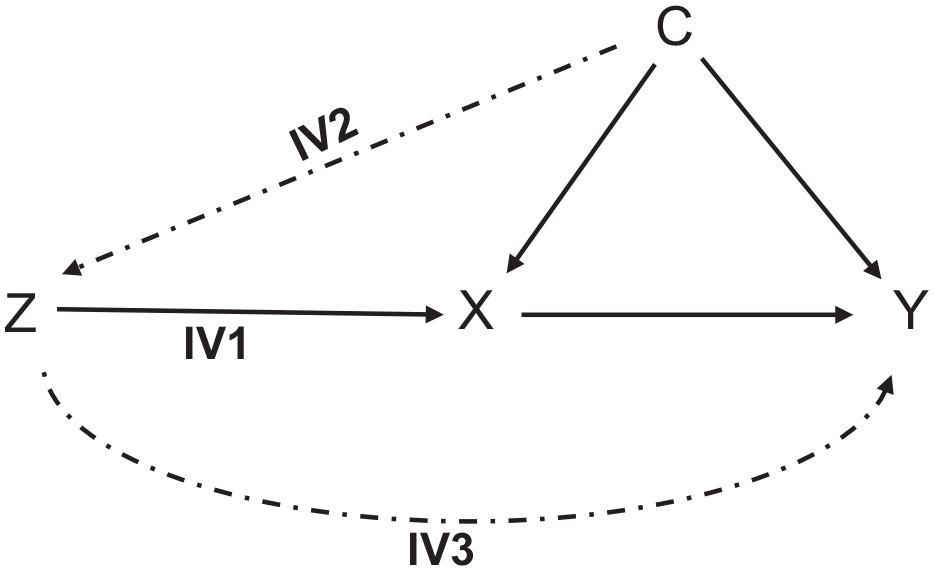
Instrumental variable assumptions diagram.
Results
In the BRFSS, each additional year of schooling reduced the likelihood of edentulism by 2.9 percentage points (pp) (95% confidence interval [CI]: −0.041; −0.017) and the risk of losing 6 or more teeth by 4.9 pp (95% CI: −0.058; −0.039) (Table 3). Schooling increased the likelihood of dental visits by 1.2 pp (95% CI: 0.01; 0.024), with stronger effects in women (1.9 pp) than in men (−0.4 pp, P value for interaction <0.01). Stratified by race/ethnicity, schooling’s impact on edentulism was stronger among White participants, while the positive effect on dental visits was more pronounced among Black individuals (Appendix Tables 3 and 5). SHARE results corroborated the positive effect of schooling on dental visits (5.0 pp increase, 95% CI: 0.037; 0.063) (Table 4). The SHARE waves 1 and 2 distinguished between dental visits for treatment and prevention. We found stronger effects for preventive (9.4 pp increase, 95% CI: 0.077; 0.111) than for curative visits (3.4 pp increase, 95% CI: 0.023; 0.045) (Table 4, Appendix Table 6). The effect on preventive treatment was also stronger in women than in men. First-stage F statistics were strong (>40), confirming IV relevance. Sensitivity analyses supported the IV assumptions: bounds for 2-stage least-squares estimates consistently excluded the null (Appendix Table 7), and IV models among BRFSS college graduates showed nonsignificant associations, supporting the exclusion restriction (Appendix Table 8). Inverse probability weighting in SHARE revealed larger effects for dental visits, suggesting attrition may have attenuated the unweighted results (Appendix Table 9).
Effect of Education on Tooth Loss and Dental Services Use in the Behavioral Risk Factor Surveillance Survey.

The instrumental variable probit model was adjusted for (sex), age, age², race/ethnicity, and birth year category × state fixed effects.
CI, confidence interval.
Effect of Education on Dental Services Use in the Survey of Health, Aging and Retirement in Europe.

The instrumental variable probit model was adjusted for (sex), age, age², and father’s education, and birth year category × country fixed effects.
CI, confidence interval.
Discussion
Our findings suggest that additional schooling reduces the likelihood of tooth loss and increases the probability of dental visits among low-education older adults born between 1896 and 1950 in the United States. Similarly, additional schooling raises dental attendance among older adults born between 1901 and 1979 in 25 European countries. Our findings are in line with the literature on education and oral health in Western countries. Several studies conducted cross-country comparisons of education-based inequalities in tooth loss. Elani et al. (2017) used cross-sectional data from Australia, Canada, Chile, New Zealand, and the United States and found that the United States had the widest absolute and relative inequality in tooth loss. Existing research further suggests cross-country variations in education-related inequalities in dental care use. A meta-analysis of 25 studies found that dental services use was lower among those with lower educational attainment (Reda et al. 2018). Inequality gradients were larger in the United States and Asian countries than in Europe, North Africa, the Middle East, and Scandinavia. An analysis comparing several European countries and the United States demonstrated that, in Europe, the association of education and income with dental visits was stronger than the association between dental coverage and dental visits (Manski et al. 2016).
Existing research on the association of education with oral health and dental care use typically attempted to draw inferences from observational studies by adjusting for confounders of the exposure–outcome relationship using regression adjustment, standardization, or matching. This approach produces unbiased estimates when all relevant confounders are measured and adjusted for. Confounder–control methods do not address non-exchangeability due to unobserved confounders. Many of the previous studies adjusted for a range of socioeconomic and behavioral covariates but lacked adjustment for genetic predisposition, innate intelligence, motivation, or parental background. A strength of IV analyses is that violations of the no unmeasured exposure–outcome confounding underlying conventional observational studies using confounder–control methods do not compromise IV estimates and allow causality assessment in non-experimental data. Few studies made use of IV or other quasi-experimental designs. Matsuyama et al. (2019) leveraged compulsory schooling law reforms in 1947 and 1972 and found that an additional year of schooling reduced the likelihood of edentulism by 9.1 pp in the English Longitudinal Study of Aging. Baumeister et al. (2022) instrumented education using genetic variation in European ancestry individuals and found an inverse effect of education on periodontitis (odds ratio per standard deviation increment = 0.78). Grytten and Skau (2018) exploited schooling law reforms in Norway as IVs and found that additional schooling increased the probability of subsidized dental care use (2 pp).
Our findings further suggest that the effect of education on dental services use is stronger in women than in men in the United States and Europe. A meta-analysis of 10 European studies and 23 studies conducted in North America found that the odds of dental visits were lower in men compared with women (Reda et al. 2018). Other studies have shown a higher likelihood of dental visits and a higher amount of dental care received among older women and a longer period of nonutilization as well as a higher likelihood of nonattendance in the last year among older men (Holm-Pedersen et al. 2005; Manski and Moeller 2017). Gender disparities persist, with women using dental care more frequently than men, driven by greater health literacy, caregiving roles, and societal expectations, while men exhibit slower gains from education due to entrenched norms of health-seeking behavior (Lipsky et al. 2021; Su et al. 2022). Cultural contexts play a crucial role: in the United States, structural barriers such as income and insurance gaps mediate education’s impact, whereas in Europe, broader health coverage reduces financial barriers, shifting the role of education to psychosocial mechanisms such as health literacy and attitudes toward preventive care. These gendered patterns are stronger in culturally traditional regions, such as Southern Europe, and less pronounced in egalitarian welfare regimes such as Scandinavia (Guarnizo-Herreño et al. 2019; Bastos et al. 2023). Intersectional frameworks reveal that overlapping identities, such as gender, race, and socioeconomic status, exacerbate disparities, particularly among marginalized groups in the United States (Bastos et al. 2023; Madera et al. 2023). Educational disparities often emerge early and persist across the life course, despite regional variations in welfare systems and cultural norms. In the United States, the effect of education on edentulism was more pronounced in non-Hispanic Whites, while the effect on dental visits was stronger among Black individuals. Individuals from ethnic minority groups, particularly Blacks and Hispanics, generally experience higher levels of untreated dental decay, periodontal disease, and tooth loss than Whites do (CDC 2019). A similar stronger positive association between education and regular dental visits among Blacks compared with other ethnicities was found in the National Health and Nutrition Examination Survey (Han 2019).
The present study has limitations. First, we cannot fully rule out the possibility of IV exchangeability violations by unadjusted confounders of the IV-outcome association. Such confounders include economic shocks or co-occurring policies (tobacco or sugar, access to care). We included state/country-by-birth cohort fixed effects, which account for such unobserved confounders varying across state/country and birth cohorts. In addition, our first sensitivity analysis found that the associations of such state- or country-level confounders would need to be stronger than the association of schooling with tooth loss and dental attendance, which is unlikely. Also, previous studies tested the robustness of IV exogeneity of the compulsory schooling reforms-IV in different samples and did not reject its validity (Brunello et al. 2013; Bolzern and Huber 2017). Second, tooth loss, dental visits, and years of schooling were self-reported. It is possible that misclassification of tooth loss and dental visits varies by education level. In BRFSS, we restricted our analysis to individuals with a lower level of education, and it is unlikely that misclassification differs by years of schooling in this subgroup. Unfortunately, the BRFSS did not allow the categorization of important tooth loss indicators, such as functional dentition. However, one might speculate that the category “6 or more, but not all” could be taken as a proxy for functional dentition, given the likelihood of underreporting tooth loss, especially among low-educated people. Also, it is important to emphasize that one of our aims was to replicate the study conducted by Matsuyama et al. (2019) in the United Kingdom and generalize those findings to the United States and several European countries. Equivalent to our study, Matsuyama et al. (2019) also used edentulism as a primary outcome. Third, our U.S.-based findings should apply to low-education community-dwelling individuals, while the estimates from SHARE should also be generalizable to individuals with upper-secondary and tertiary education. In addition, the schooling policy affects only those who would have otherwise left school earlier, meaning that we estimate a local effect among compliers in this context. Due to the SHARE sample selection, our estimate of education on dental visits for Europe should be generalized only to those who survive to middle age. We do not know whether findings translate to other countries and institutionalized older adults.
In conclusion, our study adds to the evidence that education has a causal impact on oral health and dental care use in Western countries. Reducing disparities in oral health requires universal and targeted interventions and the integration of oral care into broader preventive strategies, especially within universal health coverage frameworks. The World Health Organization (WHO) Global Health Action Plan 2023–2030 and the 2024 WHO global oral health meeting include several key objectives related to equitable access to dental care, including coverage of essential oral health care, ensuring related financial protection, and reorientation toward preventive care. Increasing diversity in the dental profession and promoting cultural competence will be crucial as the U.S. population continues to diversify.
Author Contributions
S.-E. Baumeister, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; S. Listl, G.G. Nascimento, M. Nolde, contributed to conception, design, data interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345251316815 – Supplemental material for Education, Tooth Loss, and Dental Visits: Evidence from Schooling Reforms
Supplemental material, sj-docx-1-jdr-10.1177_00220345251316815 for Education, Tooth Loss, and Dental Visits: Evidence from Schooling Reforms by S.-E. Baumeister, S. Listl, G.G. Nascimento and M. Nolde in Journal of Dental Research
Supplemental Material
sj-docx-2-jdr-10.1177_00220345251316815 – Supplemental material for Education, Tooth Loss, and Dental Visits: Evidence from Schooling Reforms
Supplemental material, sj-docx-2-jdr-10.1177_00220345251316815 for Education, Tooth Loss, and Dental Visits: Evidence from Schooling Reforms by S.-E. Baumeister, S. Listl, G.G. Nascimento and M. Nolde in Journal of Dental Research
Footnotes
A supplemental appendix to this article is available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The BRFFS data are accessible at https://www.cdc.gov/brfss/. The harmonized SHARE datasets are available through the Gateway to Global Aging website (https://g2aging.org/). Compulsory school laws, compiled by Lleras-Muney, Stephens, and Yang for U.S. states and by Hofmarcher for European countries, can be downloaded at https://adriana-llerasmuney.squarespace.com/data (access date March 25, 2024), https://www.openicpsr.org/openicpsr/project/112828/version/V1/view?path=/openicpsr/112828/fcr:versions/V1/data_programs_AER-2012-1082&type=folder (access date March 27, 2024), and ![]() (access date March 27, 2024).
(access date March 27, 2024).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.