
Abstract
This article presents a summary of the third American Association for Dental, Oral, and Craniofacial Research Meeting within a Meeting, which was held during the 2024 annual meeting in New Orleans, Louisiana. Speakers were challenged to reflect on how women are differentially affected by health and societal issues by factors that go beyond biology. The goal was to promote current research on women’s issues that are relevant to dental, oral, and craniofacial scientists.
Background of the American Association for Dental, Oral, and Craniofacial Research Meeting within a Meeting
As part of the American Association for Dental, Oral, and Craniofacial Research (AADOCR) science-first initiative to bring new opportunities for membership, professional development, and program growth, the AADOCR initiated a Meeting within a Meeting (MwM) featuring cutting-edge presentations on broader themes in dental, oral, and craniofacial (DOC) science. The first MwM in March 2022 in Atlanta featured Contemporary Artificial Intelligence Applications in Dental Research, oriented toward both dental researchers and clinicians to build a shared terminology for contemporary research and to welcome researchers new to DOC science. The second MwM in March 2023 in Portland was on the topic of Geroscience: Aging and Oral Health Research (Weintraub et al. 2023),which was based on a trans–National Institutes of Health (NIH) research initiative and was also partly inspired by the United Nations declaration of 2021 to 2030 as the “UN Decade of Healthy Ageing” (United Nations General Assembly 2020). The third MwM was on the topic of Women in Dental Clinical Translational Research and was held during the annual session of the AADOCR and the Canadian Association for Dental Research in conjunction with the International Association for Dental, Oral, and Craniofacial Research in New Orleans, Louisiana, March 14 and 15, 2024. Over the 2 d, speakers were challenged to think about how women are differentially affected by health issues beyond their biology and spoke on a spectrum including autoimmune diseases, mental health, chronic pain, and cardiovascular risks. Further, social determinants of health and clinical and translational training were discussed. The goal was to bring to light current research on women’s issues, display areas of interest and potential synergism, and identify current gaps in knowledge. To address these gaps and promote DOC research, we will require a deliberate plan that weaves concepts on basic genetics, cellular and molecular physiology, epidemiology, and pharmacology into dental research.
Origin of Sex Disparities: Summary of Alexandre R. Vieira’s Remarks
It is generally accepted that differences exist in all facets of health care and disease related to sex and gender. These differences are the result of several aspects related to social, behavioral, and biological determinants of health. These differences may be perceived as not very dramatic, depending on the conditions being assessed (Table 1).
Relative Frequency (%) of the Leading Causes of Death in the United States (Mauvais-Jarvis et al. 2020) by Sex.
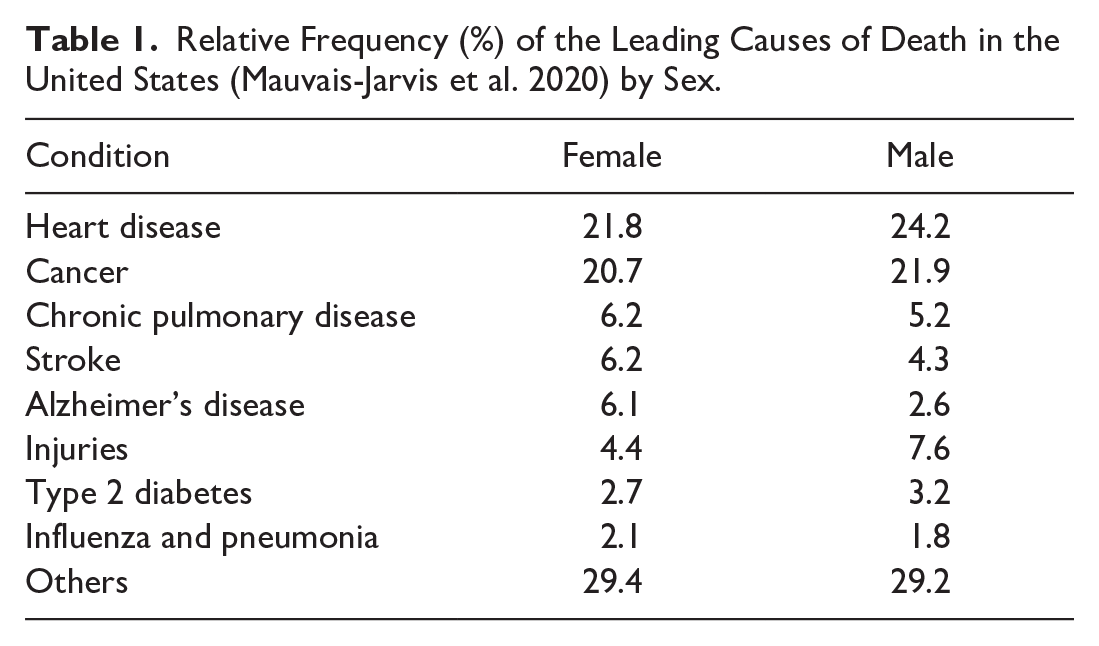
However, certain disabling conditions, such as autoimmune disorders, neurodegenerative and neuropsychiatric illnesses, and painful and socially disabling ailments, show important differences in prevalence, with women being significantly more affected by Sjögren’s disease, systemic lupus erythematosus, primary biliary cholangitis, thyroid disease, scleroderma, myasthenia gravis, rheumatoid arthritis, eating disorders, anxiety, inflammatory bowel disease, migraine, fibromyalgia, and chronic fatigue syndrome (Mauvais-Jarvis et al. 2020).
Sex differences can also be seen in normal trait variation, and one of the best examples is intelligence. When intelligence was measured by IQ at 11 y of age in more than 80,000 children born in Scotland in 1921, girls outnumbered boys for IQs between 90 and 115, whereas boys outnumbered girls at IQ scores lower than 90 (59% versus 41%) and higher than 115 (58% versus 42%) (Deary et al. 2003).
Sex differences are the consequence of 2 main components. Biology determines disease and disease risks, pathophysiology, disease manifestation, and responses to treatments. The environment (meaning society, gender constructs, lifestyle, nutritional habits, exercise, perceived stress, and smoking) determines disease perception, help-seeking behavior, use of health care, decision making, and therapeutic responses (Mauvais-Jarvis et al. 2020). We also know that biology further influences at least some of these components such as behavior and decision making (Vieira 2019).
The origin of societal contributions to today’s sex differences can be dated at least back to the Neolithic, for which evidence shows women and children were less likely to receive a formal burial, men were more likely to be buried with arrowheads and women with ceramics, and men were overrepresented in cave art (Peña and Sanjuán 2019). The perpetuation of these gender role patterns is responsible for current patterns in which women, in comparison with men, are less likely to be employed full-time; more likely to be attuned to caring roles; more likely to have their working life interrupted by pregnancy and caring responsibilities; more likely to work in lower-paid jobs and exercise less control in those jobs; more likely to have their views devalued; less likely to occupy top positions in society; more likely to be seen as irrational, emotional, and unsuited for responsible positions; and more likely to have lower self-esteem and to be concerned about body image (Walters 2004).
Dental and medical training achieved equity among graduates, but women are still underrepresented in senior faculty and leadership roles in their professions and face more challenges in research careers. Implicit bias is not consciously appreciated and persists from early in training, playing a role in disparities in hiring, advancement, and pay as careers progress (Hui et al. 2020).
Culture constructs promote disparities (Forman-Rabinovici and Sommer 2018), and studies on sex disparities tend to focus on the biological component. Addressing how the environment interacts with biological factors and leads to sex disparities is necessary, and research designs should account for as many aspects related to the environment (society, gender constructs, lifestyle, nutritional habits, exercise, perceived stress, and smoking) as possible. It is understandable that biology is an easier problem to study, but biological-cultural interactions should be the center of the current effort to close the gaps in the understanding of sex disparities in health.
Burnout and Women Health Care Providers: Summary of Karen G. Martinez-Gonzalez’s Remarks
The definition of well-being could include myriad concepts, including hope, optimism, resiliency, self-acceptance, self-esteem, work-life integration, personal and/or professional growth, meaningful social support, and sense of purpose. Absence of well-being is a leading cause of burnout. Health care professionals must continuously respond to the needs of patients and families and expend their own emotional resources to provide care and caring to others. Health care encounters are often stressful, and the professional must continuously adapt to the ever-changing demands of the profession. Patient and societal expectations demand certainty from the medical health professions, while scientific knowledge includes limitations and uncertainties. Everyday health care professionals are called to cope and adapt with these stressors, which are characteristic of their role. To perform our jobs, we are called to suppress the emotional toil of these stressors. For some, coping capabilities prove insufficient, and emotional reserves become depleted. For these individuals, burnout becomes reality (Lönn et al. 2023).
Three degrees of burnout have been suggested. First-degree burnout is characterized by a failure to keep up, complacency regarding the status quo, and a gradual loss of reality. Second-degree burnout is accompanied by accelerated deterioration, where individuals have sleep problems and little energy. They may gain or lose weight. Third-degree burnout involves major physical and/or psychological breakdown (could include complications such as cardiovascular and gastrointestinal disease as well as mental illness, such as anxiety and depression (Simmendinger and Moore 1985)).
Rapidly increasing medical knowledge and technology make it difficult to keep up to date, and there is an increasing pressure to focus on the disease rather than the patient. Health care professionals are confronted daily with death and are thus focused on dealing with the issue of their own mortality and the purpose and meaning of life. Many, unfortunately, begin to view death and disease as well as life in general as a battle. Some see the battle as already lost and develop a sense of hopelessness and powerlessness (Williams and Doolittle 2022).
Health care professionals might try to cope with demands of their practice by working harder and longer, which can lead to inefficiency, psychological impairment, and poor patient care. İt is often difficult for health care professionals to acknowledge that they are having trouble in coping with stress. This frequently stems from a sense of entitlement and a sense of being immune to stressors (West et al. 2018). Health care workers’ own expectations are often their greatest source of stress. Few spend time in self-reflection or in attending their own needs. Professional training reinforces false beliefs in one’s immunity to difficulties and prevents self-recognition of serious psychological problems (Williams and Doolittle 2022).
Another cause of burnout in health care professionals is that they often isolate themselves from their support groups. Three primary explanations for alienating family members and friends have been proposed (West et al. 2018):
anger and frustration are vented to family and friends in the belief it is safer to express these negative feelings to family members and friends than toward patients and coworkers;
fearing a breach of confidentiality, physicians may feel unable to share troublesome experiences with others; and
family and friends may be perceived as another source of potential demands.
With regard to women, 60% of female physicians experience burnout compared with 40% of male physicians. Women in health professionals have an increased risk of burnout beginning early in their careers (graduate studies), and the increased risk of burnout in women in the health professions is associated with poor work-life integration, sex inequity in the workplace, and lack of workplace autonomy (Karakcheyeva et al. 2024). It has been suggested that supportive and flexible work environments as well as access to professional development, including mentoring, supportive personal relationships, and intentional mindful practice, can help increase the well-being of women in the health care professions (Karakcheyeva et al. 2024).
To promote well-being, women can pay attention to lifestyle choices, negative self-talk, mind traps, personality traits, and coping styles. The acronym SPIRE (Fig.) addresses aspects that can help to prevent burnout.

SPIRE mindset to prevent burnout.
Health care professionals can also prevent negative consequences of stress by engaging in recovery strategies. Some examples of burnout recovery strategies include sleep, mindfulness, prayer, screen-free hours, unplugging, hugs, healthy eating, music, nature, and spending time with those you love. Exercising self-compassion (monitoring language used to talk to self, expectations, and making sure to take time to take care of self), exercising kindness to others, and prioritizing social connections are ways to decrease the probability of burnout.
Decoding the Impact of Sex and Gender on the Temporomandibular Disorder/Orofacial Pain Process in the Brain: Summary of Alexandre F. DaSilva’s Remarks
There is evidence of different influences of sex and gender on health outcomes and pain outcomes (Boemer et al. 2024). Gender here is defined as socially constructed roles, behaviors, expressions, and identities of girls, women, boys, men, and gender-diverse people, whereas sex is biological attributes of humans and animals, including physical features, chromosomes, gene expression, hormones, and anatomy.
Female and male brains are different, and these differences are expressed both in the functional brain organization and other brain features and cognitive profiles. One recent study used artificial intelligence to analyze brain features and found consistent significant sex differences across sessions and independent cohorts associated with the default mode network (DMN), striatum, and limbic network (Ryali et al. 2024), which accurately predicted sex-specific cognitive profiles. For example, the DMN influences various cognitive and social behaviors and plays a significant role in integrating self-referential information processing and monitoring of the internal mental landscape. In addition, the striatum and limbic networks have great association with reinforcement, learning, and reward sensitivity. These findings highlight the importance of understanding sex-specific differences in brain functionality and their impact on cognitive and social behaviors (Ryali et al. 2024).
It comes as no surprise that in the case of chronic pain, more specifically migraine, there are differences between females and males across their lives (Borsook et al. 2014). Migraine prevalence in boys and girls is similar until puberty, after which it diverges (at approximately 10 to 11 y of age). Hormonal changes during development increase the probability of migraines, particularly in young females between puberty and early adulthood. The prevalence is approximately 6% in men and 15% to 17% in women and normally decreases some years after menopause (Faria et al. 2015). In part, the sex hormones have a great influence on pain perception and suffering. Testosterone has been found to have an analgesic effect, whereas estrogen and progesterone can have both pain-inhibiting and pain-promoting effects. Female sex hormones are associated with pain regulation and response to therapies, and they may influence pain-related signaling pathways and immune modulation (Boemer et al. 2024).
In the brain, estrogen levels affect µ-opioid receptor levels and activation in response to sustained pain in young, healthy males and females (Jassar et al. 2019). High estrogen states were associated with increased baseline µ-opioid receptor availability and greater activation of endogenous opioid neurotransmission during pain in the brain. Conversely, low estrogen states were linked to reductions in endogenous opioid tone and hyperalgesic responses. The variations in µ-opioid neurotransmission correlated with individual ratings of pain perception and recall. Overall, the study showed that estrogen plays a significant role in modulating endogenous opioid neurotransmission and psychophysical responses to pain in male and females (Smith et al. 2006). At a structural level, the average parahippocampal volume of males is significantly decreased in individuals affected by migraine when compared with healthy males. Both healthy and migraine-affected females have higher average parahippocampal volumes when compared with males. However, the average parahippocampal volumes of healthy females do not differ from the average volumes of females affected by migraine (Maleki et al. 2012).
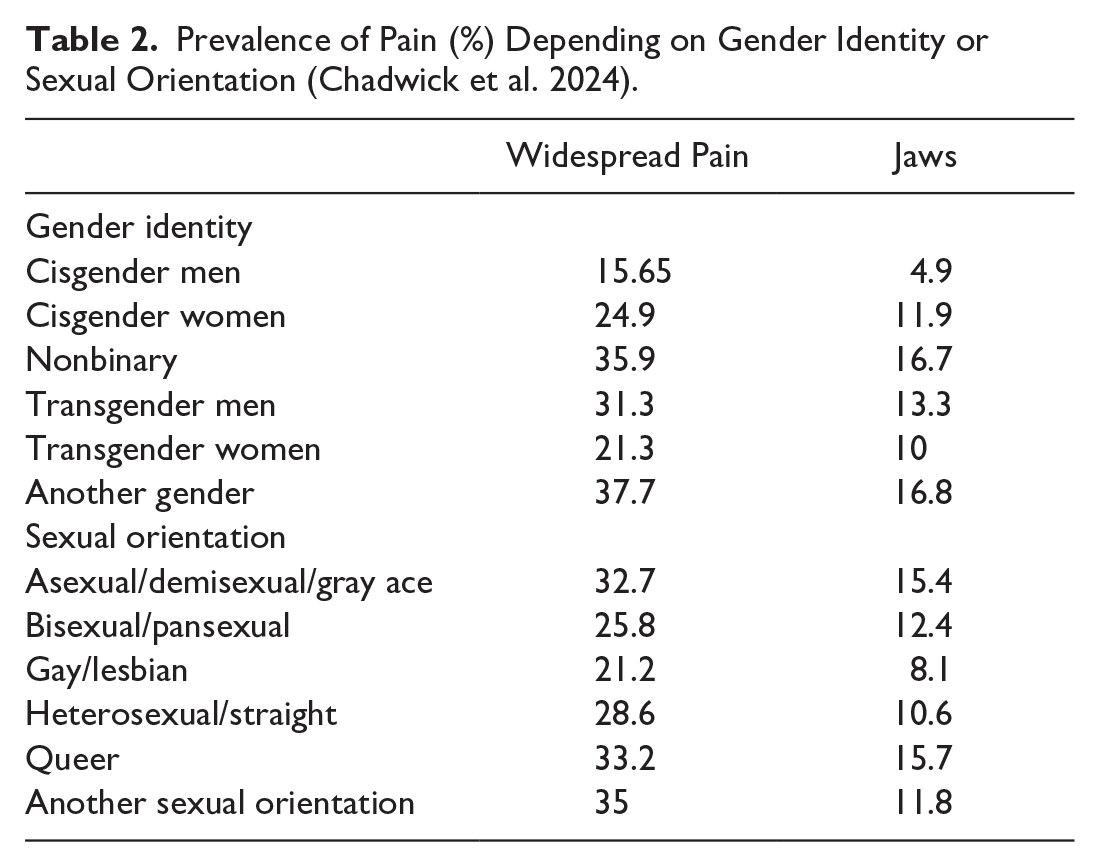
Finally, widespread headache and orofacial pain frequency differ depending on gender (Table 2) (Chadwick et al. 2024). Hormone therapy appears to be, at least in part, responsible for that variation (Aloisi et al. 2007). A study looking into gender diversity and the effects of cross-sex hormone administration in transsexuals on chronic pain demonstrated that sex steroid hormones have sex-specific effects on pain (Aloisi et al. 2007). Male-to-female transsexual subjects develop chronic pain, mainly headaches and musculoskeletal pain, with estrogen/antiandrogen treatment, whereas female-to-male transsexuals report improvement in chronic pain with testosterone treatment. The findings above suggest that sex steroid hormones play a crucial role in pain (van Lohuizen et al. 2023).
Prevalence of Pain (%) Depending on Gender Identity or Sexual Orientation (Chadwick et al. 2024).
Incorporating Sex as a Biological Variable into Clinical and Translational Training: Summary of Stacey J. Winham’s Remarks
Most education on women’s health has historically focused on the reproductive system only. To change this scenario, a goal of engaging the learner in curriculum across the full spectrum of clinical and translational science training with individualized components is desirable, by combining the right content with the right learner at the right time through the right modality. In addition to traditional lectures and coursework, this can include case-based approaches, journal clubs, seminars, workshops, and mentoring (Kantarci et al. 2020). Given NIH mandates for including sex and gender in research studies (Clayton and Collins 2014), these education and dissemination efforts should include the promotion of standards and policy for incorporating sex as a biological variable (Kantarci et al. 2020). Dissemination through symposiums, workshops, video tutorials, and other resources for learning about how to incorporate sex and gender into clinical and translational research were also discussed.
In addition to didactic educational content, resources should be created purposefully to address the career enhancement needs of the next generation of basic, clinical, and translational scientists in the study of sex differences. This should include leadership training, career enrichment, and research stimulus through funding mechanisms such as career development awards and pilot grants. Career development and mentoring are critical to training and may have a multipronged approach that includes group mentoring (e.g., germination meetings, mentoring committees, and giving feedback on grant writing) and individualized mentoring (e.g., lectures and workshops, executive coaching). An important component of career development is leadership development. Important themes and topics for leadership development include communication skills for sticky situations, building self-efficacy, and intentionality in making and holding boundaries, and delivering these topics using an individualized format may be particularly beneficial (Morrow et al. 2023).
The importance of incorporating sex and gender into research design and analysis was also emphasized. In general, studies should be “sex aware,” representing both females and males, and it is recommended that sex-specific data are reported. This requires that data be disaggregated by sex, that sex-aware descriptions be included throughout the text (in the Methods and Results sections) and data presentation (label “sex” in tables and figures) of scientific manuscripts, and that data be shared publicly in such a way that promotes future sex-specific analysis (Rich-Edwards et al. 2018; Winham and Mielke 2021). The presentation of results is important and should avoid bar and line graphs that hide the distribution of continuous data, since the actual data may suggest different conclusions from the summary statistics alone; figures that show individual data points and the full data distribution, separately in males and females, should be used instead (Weissgerber et al. 2015). Sex-aware analyses should also be conducted, including analyses that not only are adjusted by sex but also distinguish between confounding by sex versus sex differences (i.e., interactions). Differences between sex-pooled, sex-stratified, and sex interaction analyses were discussed (Winham and Mielke 2021). Special consideration should also be made for genomic studies that tend to not report data on the X and Y chromosomes. Genomic studies should also have a sex-aware design, sex-aware quality control for both autosomes and sex chromosomes (X and Y), sex-aware data visualization, and sex-aware analysis (sex-combined and sex-stratified, X and Y chromosome data should be always included, and gene-sex interactions should be evaluated; Khramtsova et al. 2023).
In summary, understanding of sex and gender have evolved and will continue to evolve, which may lead to future changes related to research recommendations. But it will continue to be critical for clinical and translational research studies to include both females and males with data disaggregated by sex.
Health Promotion for Underserved Populations: Summary of Vanessa Pardi’s Remarks
Health promotion is the process of empowering individuals and communities to address negative influences of determinants of health. Segments of the population are affected differently by determinants of health and can be underserved, vulnerable, or both. Underserved communities have limited access to health care services. Vulnerable communities tend to experience additional barriers to getting care (Caron et al. 2024). Women, in particular, experience many unique health issues, such as pregnancy, childbirth, and menopause. Also, some health issues that affect both men and women pose unique challenges for women.
Underserved communities share 1 or more of the following characteristics: they receive fewer heath care services, face barriers (economic, cultural, linguistic) to accessing primary health care services, are not familiar with the health care delivery system, and face a shortage of readily available providers (Lazo-Porras and Penniecook 2023).
Vulnerable communities have a high risk for multiple health problems or preexisting conditions, have limited options (financial, educational, housing), display fear and distrust, have a limited ability to understand or give informed consent, have mobility impairments, lack access to transportation services, have a lowered capacity to communicate effectively, and face many types of discrimination (US Department of Health & Human Services 2014).
The underserved communities are Black/African Americans, Latinos, Native Americans, Asian Americans and Pacific Islanders, other persons of color, members of religious minorities, members of the LGBTQI+ community, individuals with disabilities, rural dwellers, and groups affected by persistent poverty and inequality. Table 3 shows how they are affected over their life course. In the case of women, one should ensure that plans account for the unique perspectives, strengths, and challenges as well (National Institute on Minority Health and Disparities 2017).
National Institute on Minority Health and Health Disparities Research Framework (National Institute on Minority Health and Health Disparities 2017). a

The framework reflects an evolving conceptualization of factors relevant to understanding and promoting minority health and to understanding and reducing health disparities.
Improving access to oral health care is a crucial first step in improving oral health outcomes and reducing disparities. Achieving this improvement will necessarily require multiple solutions involving a range of providers across various settings. Potential strategies include integrating oral health into overall health care, promoting legislation that supports access to care, improving education and training for dental professionals, reducing barriers to care, promoting research, and increasing capacity at state and local levels (Institute of Medicine and National Research Council of the National Academies 2011). Some initiatives already underway include the dental home concept, colocation of dental care and primary care services, diversifying workforce models, loan repayment/tuition off-set incentives, and teledentistry.
Women’s oral health promotion and prevention strategies need to consider sex and gender differences in attitudes and behaviors toward oral health throughout their life course. Women generally have more positive attitudes toward dental visits, greater oral health literacy, and better oral health behaviors compared with men (Lipsky et al. 2021). Underserved women include those with low income, racial and ethnic minorities, rural dwellers, women with disabilities, LGBTQ+ members, elderly, homeless, incarcerated, immigrants and refugees, pregnant and parenting women, and victims of domestic violence or sexual assault. One aggravating factor is bias and stereotyping in health care and medical research, which is further compounded by the social positions of women, their experience of burnout, and economic inequality.
Community-based participatory research has been instrumental in understanding barriers and facilitators to health promotion interventions among underserved populations (Wang et al. 2020). Approaches suggested to reach communities have included community-based education programs, mobile dental clinics, partnerships with community organizations, integration with primary health care, targeted outreach for pregnant women, peer support programs, culturally competent outreach, financial assistance programs, and policy advocacy.
In conclusion, health promotion for underserved women should encompass gender and health equity and include access to dental care, oral health education, oral health promotion during pregnancy, and cultural competency. It should also address intersectionality to target oral health disparities, incorporate community-based interventions, policy, and advocacy. Collaborative partnerships, preventive care and early intervention, and the empowerment and self-care of women are essential components in this comprehensive approach.
Authors’ Contributions
A.R. Vieira, conceptualized and designed the section and article, data, contributed with content, wrote the draft; K.G. Martinez Gonzalez, A.F. DaSilva, S.J. Winham, V. Pardi, contributed to content, critically revised the manuscript. All authors gave final approval for the submission of the manuscript and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The session also included Lindsey A. Criswell presenting Why Women Are More Affected by Autoimmune Diseases and Mariana Bezamat presenting Heart Disease: A Leading Cause of Death for Women.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.